Embed Size (px)
DESCRIPTION
dentatl whitening
Citation preview
Navigating the “Whitening Maze” Assessment and Clinical Protocol
INTRODUCTION TO THE DENTAL PATIENT (IDP III)
Dorothy Vannah, M.Ed., RDH, CDA Director :The Simulation Learning Center
Associate Professor: Diagnosis & Health Promotion 2015
Return to Menu
At-Home Tooth Whitening
Also known as night guard bleaching, vital tooth whitening.
Noninvasive dental procedure that uses “bleaching” agents to whiten dark or discolored teeth with living pulp.
Most requested service
Opalescence PF 10% Lowest sensitivity whitening product on the market
Return to Menu
Dental Whitening Agents: Composition and Chemical Make-Up
Active ingredient common to ALL Whitening products: Carbamide peroxide or Hydrogen peroxide
Gel base: Propylene glycol/glycerin and water
Thickening agent: Carbopol
Additives: Potassium nitrate or Fluoride
Return to Menu
Hydrogen peroxide - Carbamide peroxide
Hydrogen peroxide –The ↑ the concentration the more rapid the lightening effect. Day-time , shorter wear time
Carbamide peroxide - Is weaker than hydrogen peroxide, added thickening to allow a prolonged exposure to the whitening agents. Night-time , longer wear time
Return to Menu
Composition cont.
Hydrogen Peroxide concentration is equivalent to three times the comparable Carbamide Peroxide concentration.
10% Carbamide peroxide ≈ 3% Hydrogen peroxide (H2O2)
Return to Menu
Dental Whitening Agents: Composition
Carbamide peroxide, the active ingredient most widely used is available in gel concentrations that range from 10% to 22%.
Having multiple concentrations from 10% to 22% allows you to customize the bleaching program to each patient’s specific needs.

Return to Menu
How Whitening Works
Oxidation is believed to be responsible for the observable whitening
In the presence of saliva, Carbamide peroxide breaks down into hydrogen peroxide and urea, which then degrades into water an oxygen; materials commonly found and readily disposed of in the body.
10% = 7% urea, 3% hydrogen peroxide 15% =10% urea, 5% hydrogen peroxide 20% = 13% urea, 7% hydrogen peroxide
2 H2O2 = 2 H2O + O2

Return to Menu
Oxygen enters the enamel and dentin and diffuses to areas containing the discolored substances.
The structure of the tooth is not altered; only the tooth is made lighter and whiter.
O2 O2 O2 O2 O2
Mode of Action
Return to Menu
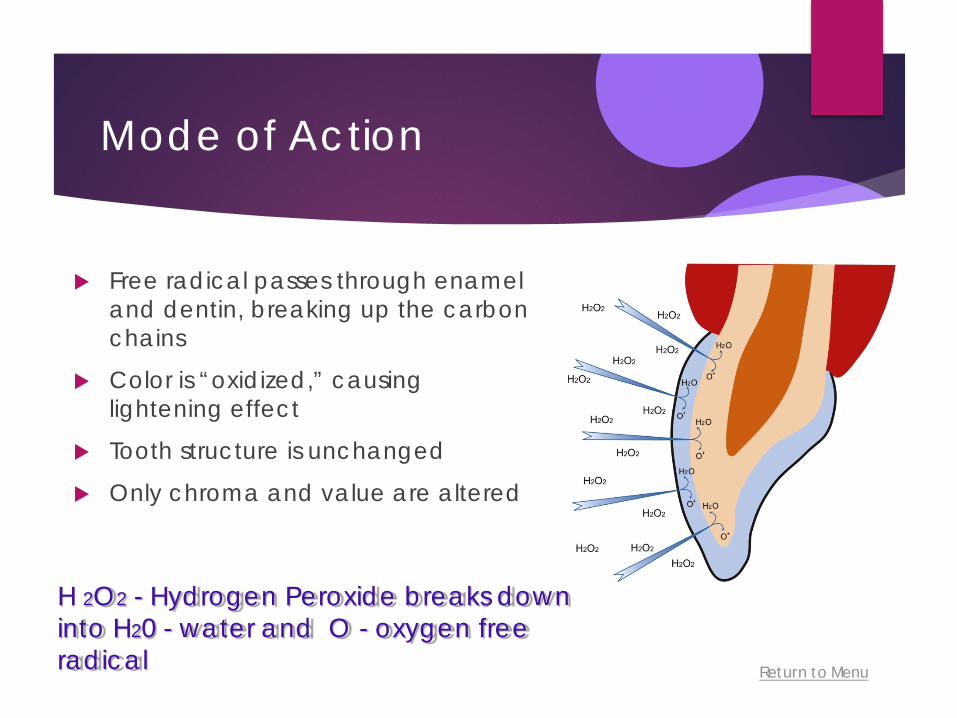
Mode of Action
Free radical passes through enamel and dentin, breaking up the carbon chains
Color is “oxidized,” causing lightening effect
Tooth structure is unchanged
Only chroma and value are altered
H 2O2 - Hydrogen Peroxide breaks down into H20 - water and O - oxygen free radical
Return to Menu
Why do we whiten?
To remove stains and discolorations due to:
Natural factors
Congenital factors
Systemic factors
Pharmalogical factors
Trauma factors, etc.
To make people feel better about themselves:
Look younger
Improve confidence
Smile more
Return to Menu
Types and Nature of Stains/Discolorations
External:
Ingestion of chromatogenic drinks (colas, coffee, tea, wine)
Tobacco (cigarettes, chewing)
Aging (thinning of enamel)
Micro cracks in the enamel, Internal
Drugs (tetracycline, fluoride)
Trauma Systemic conditions
Return to Menu
Types and Nature of Stains/Discolorations
Severe jaundice in infancy
Dental caries
Presence of Restorations / Endodontic treatment
Return to Menu
Types and Nature of Stains/Discolorations
Multiple variables affect the outcome of the whitening procedure. Dependent upon the following factors:
Cause or type of discoloration or stain
Brown stains response well 80%
Grey stains, less response
White stains behave differently – White “spot”cannot be removed, the background is lightened, white “spot” is less noticeable
Degree or intensity of the discoloration or stain
1 of 4
Return to Menu
Success Rates /Considerations
Multiple variables affect the outcome of the whitening procedure as well: Selection and strength of whitening agent Length of exposure of the teeth to the whitening
agent Selection of Whitening technique Cooperative/compliant patient
Return to Menu
Success Rates /Considerations
Mild cases of tetracycline staining and fluorosis have a higher success rate with whitening than do moderate to severe cases.
Yellow, orange or light brown stains are treated more successfully 80%
Blue-gray stains are more difficult to remove.

Return to Menu
Home Whitening
10% for 10 Nights
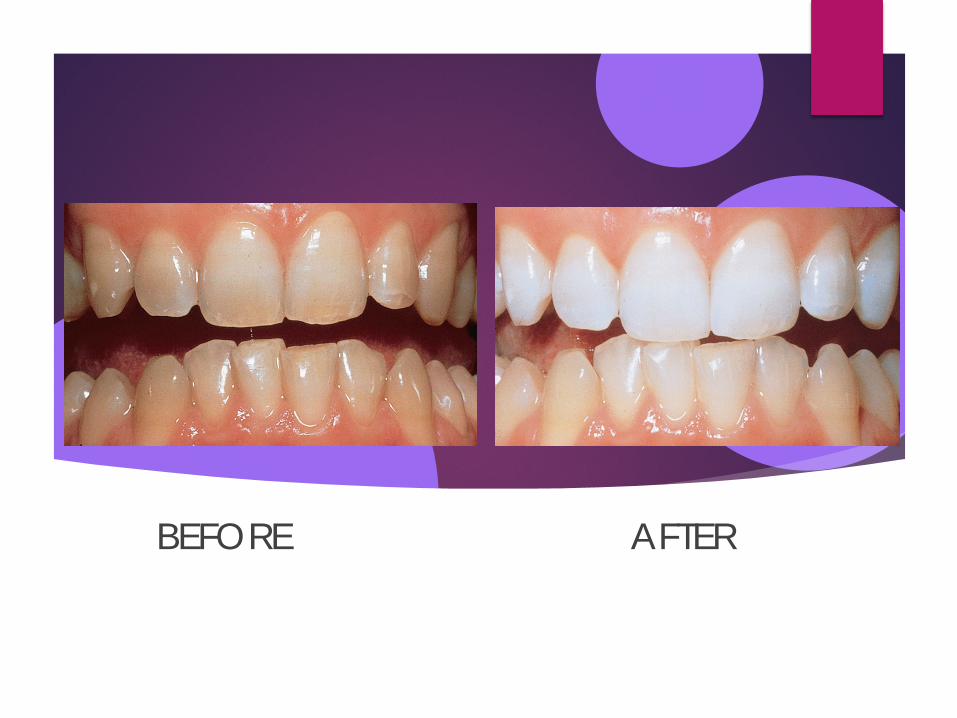
BEFORE AFTER

Return to Menu
Moderate to advanced tetracycline stains
Before

Return to Menu
Intrinsic/Extrinsic Staining
Return to Menu
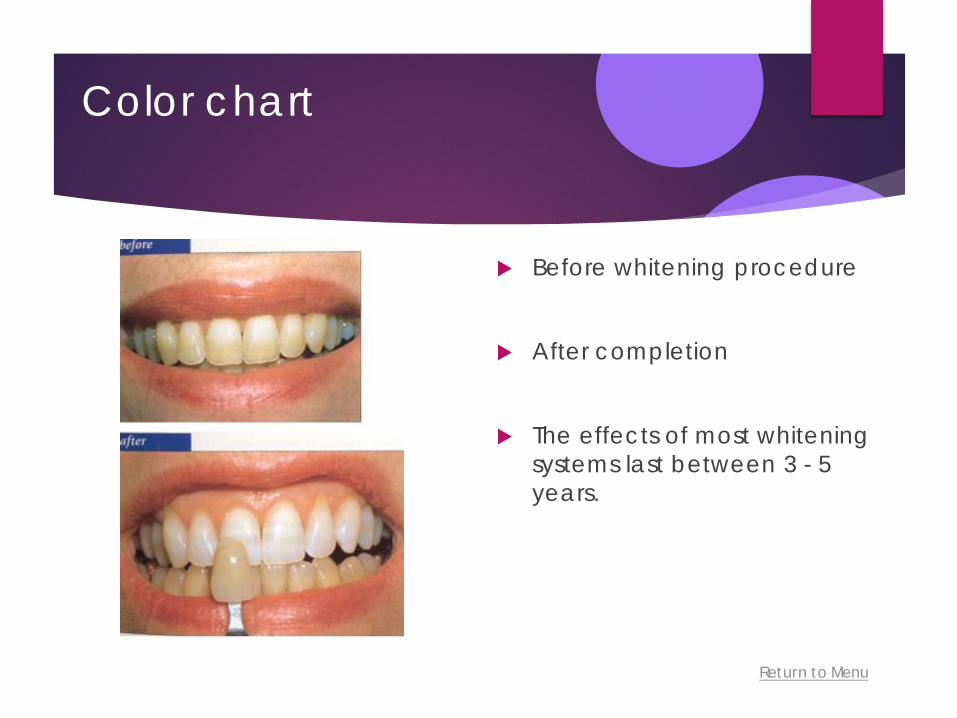
Color chart
Before whitening procedure
After completion
The effects of most whitening systems last between 3 - 5 years.

Return to Menu
Tooth Whitening -Intrinsic stains (From Roberson T, et al: Sturdevant’s art and science of operative dentistry, ed 4, St Louis, 2002, Mosby.)
Before After

Return to Menu
Composite Restoration
Before whitening procedure
After completion

Return to Menu
Tetracycline Staining
Before whitening procedure
After completion

Return to Menu
Moderate to advanced tetracycline stains
Before
After Treatment may take 2-6
months

Return to Menu
WHITE SPOTS
Possible causes:
Decalcification Excessive fluoride during tooth formation
Return to Menu
Contraindications to Tooth Whitening
Pregnant or lactating women
Children and Adolescents/ Judicious Use Only
- The American Academy of Pediatric Dentistry discourages:
full arch bleaching, mixed dentitions
– permanent teeth/single teeth
Restorations / Replacement
- Tooth colored
- Porcelain
- Planned restorative procedure within 2 weeks/ ↓ bonding strength, color match
Return to Menu
Contraindications cont.
Exposed root surfaces (may not have optimal results)
Hypersensitivity (Treat the sensitivity issues beforehand)
Sensitivity or allergy to components of the whitening agent
Unreasonable personal expectations
Return to Menu
How Long Will It Take?
Yellow/Brown 1-2 weeks
Blue/Grey twice as long
Tetracycline several months
(~ 5% of population will not whiten)
10% carbamide peroxide = 3% hydrogen peroxide 35% carbamide peroxide = 12% hydrogen peroxide
Return to Menu
Potential Side Effects of Tooth Whitening: Thermal hypersensitivity
To ↓ sensitivity while wearing the tray:
Shortening duration or frequency of treatment
↓The solution concentration
Alternate whitening solution with potassium nitrate or sodium fluoride, a desensitizing agent directly in the tray
Return to Menu
Assessing Sensitivity:
SOLUTION
trim tray off soft tissue, instruct patient proper dosage, discontinue bleaching until wounds heal.
Shortening duration or frequency of treatment
↓The solution concentration
Alternate whitening solution with potassium nitrate or sodium fluoride, a desensitizing agent directly in the tray
Return to Menu
Potential Side Effects of Tooth Whitening: Gingival Irritation
Strength of Whitening solution Due to contact with the whitening solution or an ill-
fitting tray. Trim the tray away from the gingival for a better fit Consider using a trayless whitening method
Return to Menu
What to look for in a Home Whitening System?
Sustained Released Formula Nighttime whitening - material stays active for 8-10 hours by adhering to
oral soft tissues, thereby permitting continued antimicrobial action resisting dilution by salivary action or gingival crevicular fluid.
Near Neutral pH (6.5)
Heavy, Viscous, Sticky Gel Tray containment of the material gingival irritation
Product Containing 20% Water Minimizes dehydration sensitivity
Product with Desensitizers
Reservoirs or No Reservoirs
Return to Menu
Opalescence Carbamide peroxide Tooth Whitening gels
Four concentrations – 10%, 15%, 20%, 35%
Allows clinician to customize a treatment for specific patient needs
All contain desensitizing agents
.3% potassium nitrate, 0.11% w/fluoride
Opalescence PF 10% Lowest sensitivity whitening product on the market
Patented, sustained-release formula
Return to Menu
Opalescence PF 10% (cont)
Sticky gel consistency- Gel holds tray in place
Less wasted gel, Limited material swallowed by patient
Three flavors - Encourages patient compliance
Soft tray with reservoirs
ADA accepted (10% original)
20% water content - Minimizes dehydration that can lead to sensitivity
Return to Menu
Frequently Asked Questions
Will my teeth lighten 8-12 shades?
Will my teeth be sensitive? How long does tooth
whitening last? Will tooth whitening affect
the enamel?
Studies on the Opalelsence PF product line show that use of TresWhite or Opalesence PF minimize sensitivity and provides anti-caries benefits as well as increases enamel microhardness. It improves the overall enamel health.
Return to Menu
Frequently Asked Questions
Will my teeth lighten 8-12 shades?
Will my teeth be sensitive? How long does tooth
whitening last? Will tooth whitening affect
the enamel?
Studies on the Opalelsence PF product line show that use of TresWhite or Opalesence PF minimize sensitivity and provides anti-caries benefits as well as increases enamel microhardness. It improves the overall enamel health.
Patient Preparation AXIUM – CASE NOTES
Return to Menu
Patient Preparation
Patient Assessment: Complete medical history, oral cancer screening, dental and
periodontal exam, FMX
Review current oral hygiene routine, note the surface of the tongue
CAMBRA- Caries Management by Risk Assessment
Occlusal evaluation
Evaluate the presence of existing hypersensitivity
Return to Menu
Patient Preparation (cont)
Develop a Treatment Plan
Identify existing restorations, crowns, bridges that need replacing
Select appropriate method of whitening and provide education on whitening product and procedure
Determine tooth shade guide and take photographs
Obtain Informed Consent
Return to Menu
Patient Preparation
Patient Instructions - Review Instructions for Use
Procedures Prior to Whitening - Photographs with shade guide - Scaling and Prophylaxis - Restorative procedures/removal of decay
Planning for Maintenance and Follow-Up
Return to Menu
Clinical Protocol
Eliminate extrinsic stain, plaque and calculus
Deplaque tongue
Evaluate for additional preventive and clinical treatment for sensitivity applying topical fluoride varnish to prevent sensitivity during whitening
Take impressions for custom whitening trays
Reappoint for: delivery or trays and follow-up for evaluation of whitening procedure
Documentation in AxiUM
Return to Menu
Screen Shot – AxiUm
Return to Menu
Screen Shot – AxiUm
Return to Menu
Screen Shot – AxiUm

PATIENT INSTRUCTIONS

Return to Menu
•Patients should be told beforehand: • Existing composites will not lighten • Limit intake of foods,beverages, and smoking that will stain the teeth during treatment
Restorative Considerations
Return to Menu
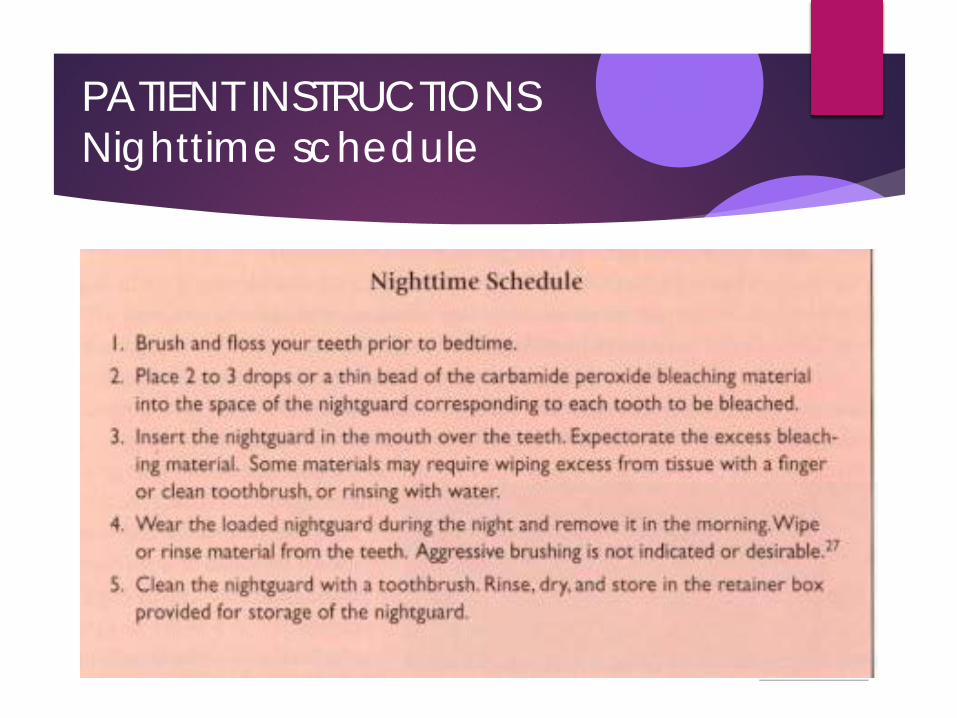
PATIENT INSTRUCTIONS Nighttime schedule
Return to Menu
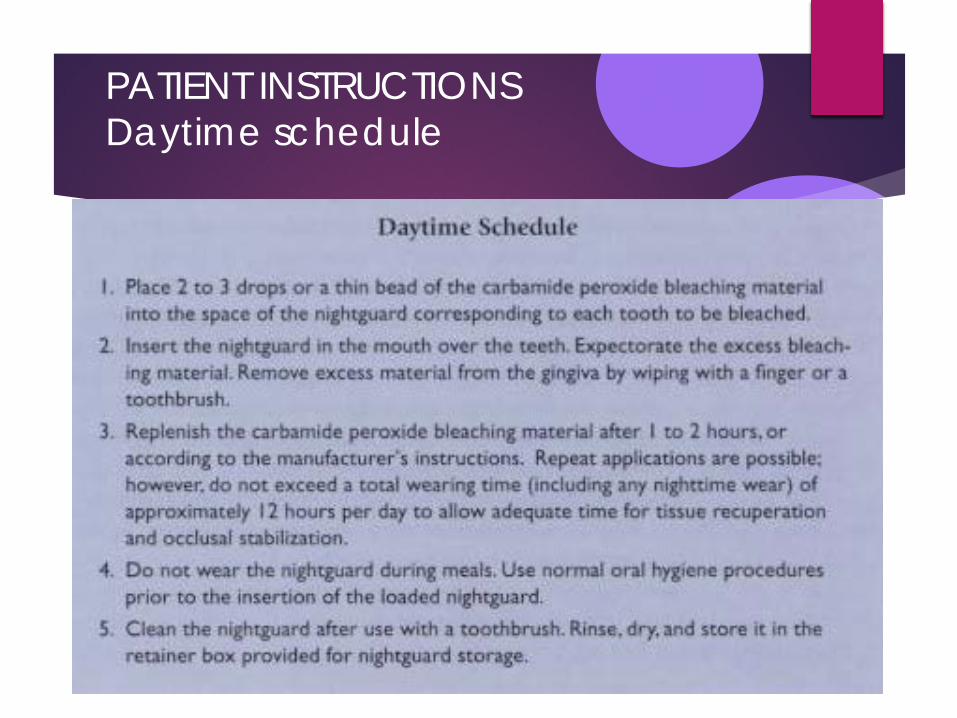
PATIENT INSTRUCTIONS Daytime schedule
Return to Menu
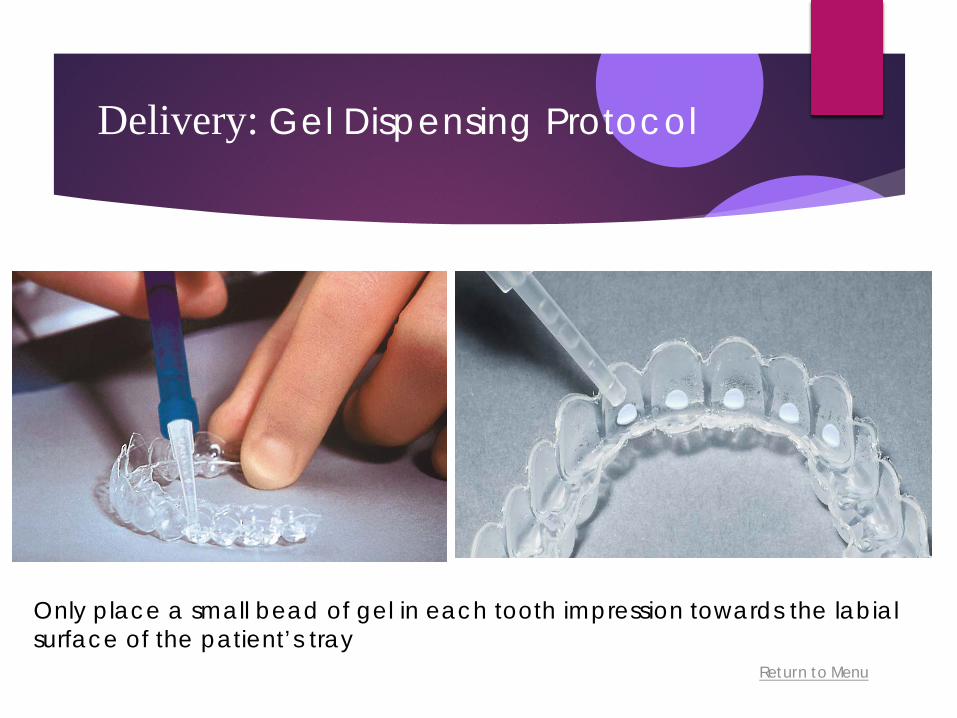
Only place a small bead of gel in each tooth impression towards the labial surface of the patient’s tray
Delivery: Gel Dispensing Protocol
Return to Menu
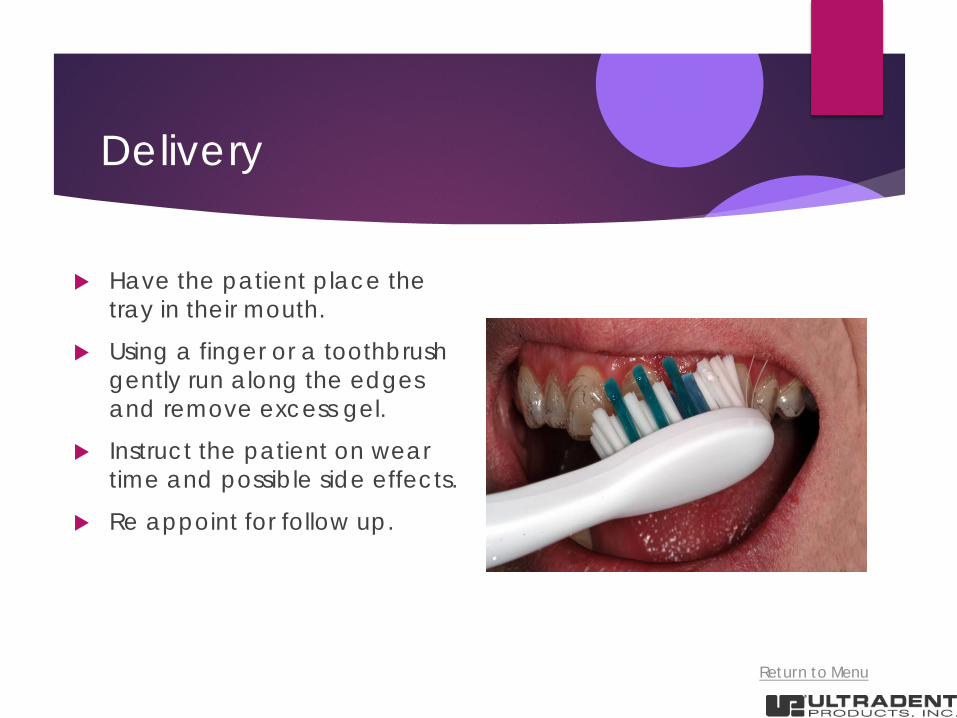
Delivery
Have the patient place the tray in their mouth.
Using a finger or a toothbrush gently run along the edges and remove excess gel.
Instruct the patient on wear time and possible side effects.
Re appoint for follow up.
Return to Menu
Delivery

Return to Menu
Custom Whitening Tray in Place
Return to Menu
If you are planning any cosmetic dentistry, it is strongly recommended that you start by whitening the teeth first. After all, why match a new smile to old coffee stains!
Return to Menu
Haywood V.B. Bleaching and Caries control in Elderly patients Aesthetic dentistry today October 2007 Volume1 Number 4 Haywood V.B. Bleaching and Caries control in Elderly patients Aesthetic Dentistry Today October 2007
Volume/ Number 4 Primarily the indication for caries control for ageing patients, those with physical handicaps or patients in nursing homes for which conventional brushing and flossing is not proving effective.
Return to Menu
Chemotherapeutic Approach Root Caries may be minimized by:
10% Carbamide Peroxide (preferred) in custom tray overnight Remove plaque
Elevate pH
Kills Lactobacillus bacteria
Used in combo with Chlorohexidine –Strep Mutans
Return to Menu
Rampart Root Surface Caries
Associated with ↓ in salivary flow due to both aging, ↑ side effects of medications
Decline in Health
Loss of manual dexterity
Side Effects of Whitening: Teeth become whiter, mismatched existing restorations
Technique to be used for the life of the patient
Return to Menu
Haywood V.B. Bleaching Children’s teeth: Questions and Answers The GAGD Explorer
(Georgia Academy of General Dentistry ) Summer 2006
Return to Menu
Bleaching Children’s Teeth
How young can the child be for bleaching? 10-14 year old range with permanent teeth present
Are there concerns for sensitivity in the young tooth? We know that peroxide goes through the enamel and
dentin to the pulp in 5-15 minutes, which is apparently the cause for sensitivity.
NO. possibly the good blood supply, large apices and resiliency of children allows sensitivity not to be a problem.
Return to Menu
Bleaching Children’s Teeth
What about safety to the child from swallowing the product? 10% carbamide peroxide is used in new born infants, 10
drops in their throat every two hours for 7-8 days, to treat candidias or thrush.
Urea peroxide used in 1800’s to stop caries in children with pitted teeth.
10% carbamide peroxide as a rinse,(Glyoxide0, in orthodontic patients during 3 years treatment to prevent white spot lesions.
Return to Menu
Bleaching Children’s Teeth
The strongest position for safety is that of the American Dental Association’s seal of approval.
4 have the ADA seal: Rembrandt by DenMat (Johnson & Johnson)
Platinum by Colgate Oral Pharmaceuticals
Opalescence by Ultradent Products Inc.
NiteWhite by Discus Dental.

Fabrication of a Custom Whitening Tray
Return to Menu
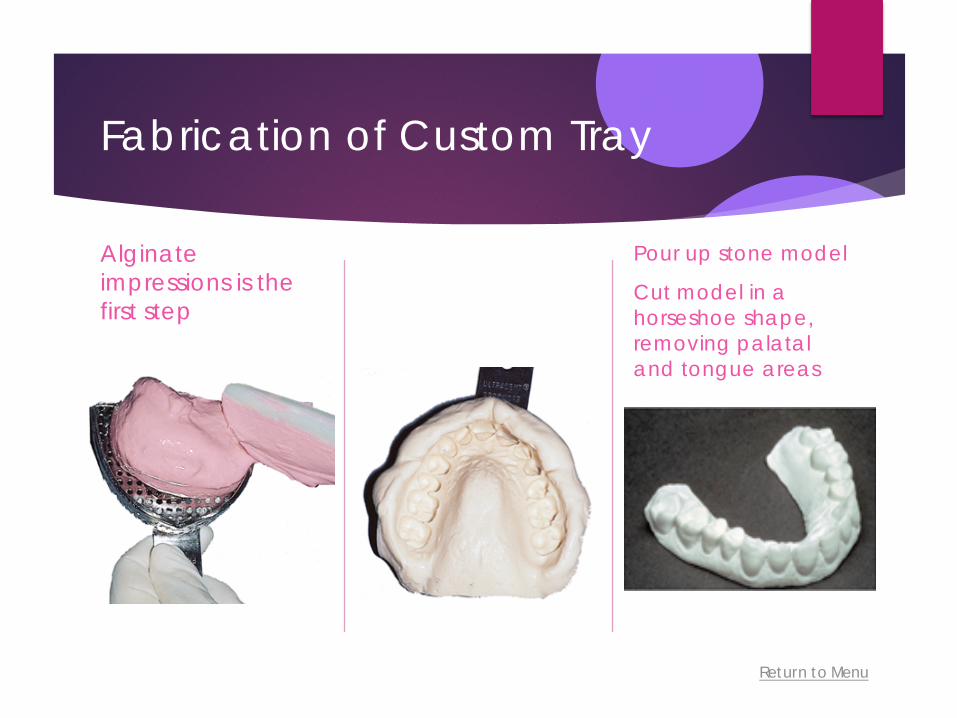
Fabrication of Custom Tray
Alginate impressions is the first step
Pour up stone model
Cut model in a horseshoe shape, removing palatal and tongue areas
Return to Menu
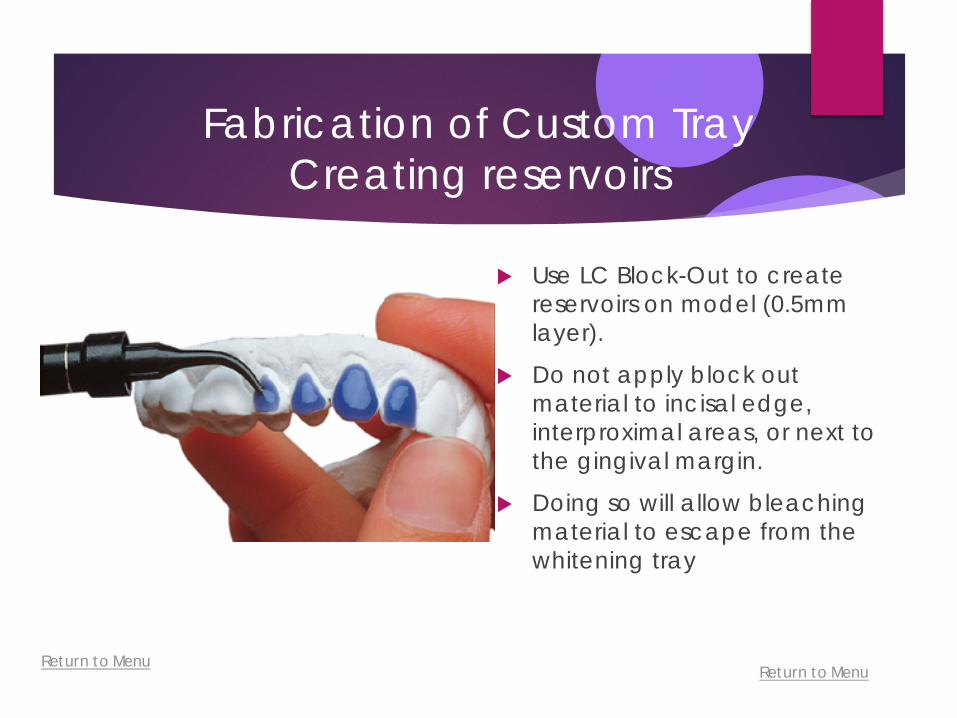
Fabrication of Custom Tray Creating reservoirs
Use LC Block-Out to create reservoirs on model (0.5mm layer).
Do not apply block out material to incisal edge, interproximal areas, or next to the gingival margin.
Doing so will allow bleaching material to escape from the whitening tray
Return to Menu

Return to Menu
Light cure block out material for 30 seconds
Fabrication of Custom Tray Creating reservoirs

Return to Menu
Fabrication of Custom Tray
Vacuum Former : heating element melts the plastic sheet and then suctions it to the stone model
Thermoplastic sheets .035 mm
Return to Menu
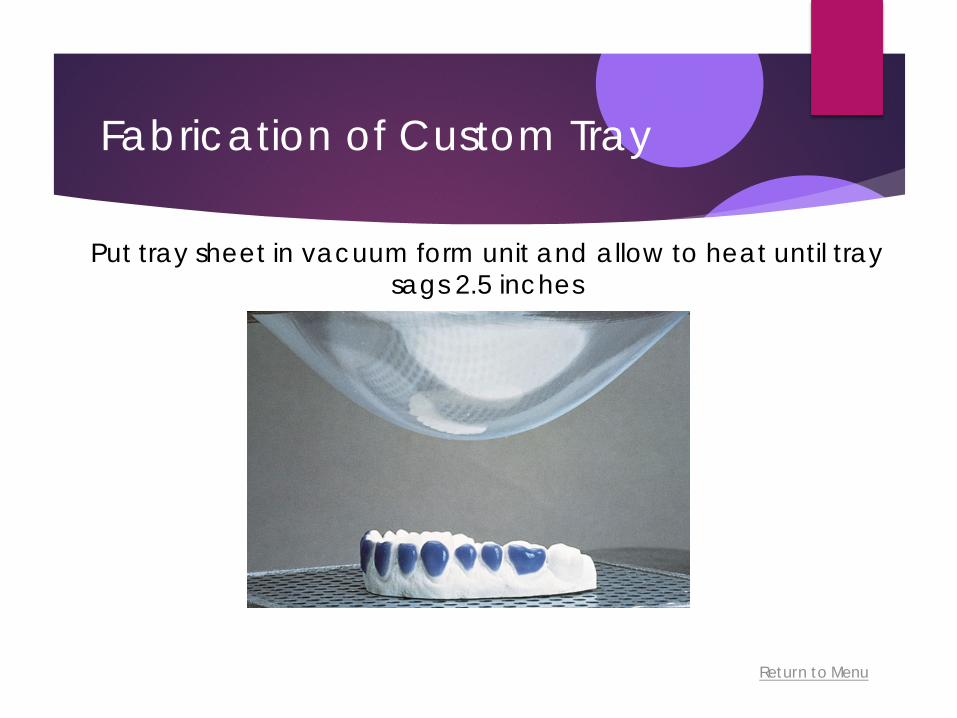
Fabrication of Custom Tray
Put tray sheet in vacuum form unit and allow to heat until tray sags 2.5 inches

Return to Menu
Trimming
Remove gross tray material with Utility Vinyl Cutters For detailed trimming, use the Ultra-Trim scissors
Return to Menu
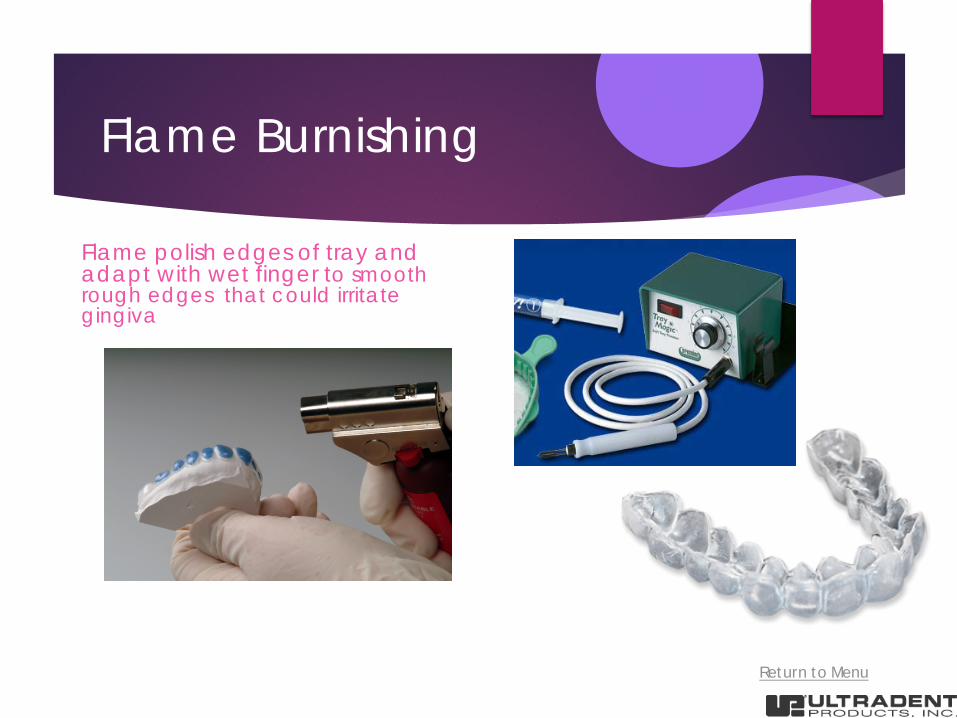
Flame Burnishing
Flame polish edges of tray and adapt with wet finger to smooth rough edges that could irritate gingiva