Embed Size (px)
Citation preview
W. Wayne Weston, MD Judith Belle Brown, MSW Moira A. Stewart, PhD
Patient-Centred InterviewingPart I: Understanding Patients' Experiences
SUMMARYEffective patient care requires attending asmuch to patients' personal experiences ofillnesses as to their diseases. Diseases areferreted out by using the conventionalmedical model, but understanding illnessesrequires a different approach. A patient-centred method focuses on four principaldimensions of patients' experiences: theirideas about what is wrong with them; theirfeelings about their illnesses, especially theirfears; the impact of their problems onfunctioning; and their expectations aboutwhat should be done. The key to thisapproach is attention to patients' cuesrelated to these dimensions; the goal is tofollow patients' leads, to understandpatients' experiences from their own pointof view. This method improves patientsatisfaction, compliance and outcome, andis applicable to the everyday work of familyphysicians with "ordinary" patients. (CanFam Physician 1989; 35:147-151.)
RESUMEL'efficacite des soins necessite qu'on s'occupe autantdes experiences personnelles du vecu entourant lamaladie que de la maladie elle-meme. Le modelemedical traditionnel sait comment rechercher lesmaladies, mais leur comprehension exige uneapproche differente. La methode centree sur lepatient met l'emphase sur quatre aspects importantsdes experiences vecues par les patients: leurperception de ce qui ne va pas; les sentiments qu'ilseprouvent face a leur maladie, en particulier leurscraintes; l'impact de ce probleme sur leurfonctionnement; et leurs attentes face ca ce qui devraitetre fait. La cle de cette approche est l'attentionportee aux indices donnes par le patient danschacune de ces quatre dimensions; l'objectif est desuivre les indices donnes par le patient, et de tenterde comprendre le vecu du patient a partir de sonpoint de vue a lui. Cette methode ameliore lasatisfation du patient, son niveau d'observance, et leresultat ultime peut s'appliquer a la pratiquequotidienne pour la majorite des soins de premiereligne.
Key words: interviewing, physician-patient relationships
The three authors of this paper holdappointments in the Department ofFamily Medicine of the University ofWestern Ontario, London. Dr.Weston is a Professor. Ms. Brown is aClinical Assistant Professor. Dr.Stewart is an Associate Professor.Requests for reprints to: Dr. WayneWeston, Byron Family MedicalCentre, 1228 Commissioners Road,West, London, Ont. N6K 1C7
OR SEVERAL YEARS our1 group at The University of West-ern Ontario has been developing amodel of family practice.14 This pa-per outlines some of the theoretical
CAN. FAM. PHYSICIAN Vol. 35: JANUARY 1989
background of this approach and pro-vides practical advice for implemen-tation.
Disease and IllnessThe basis of this conceptual model
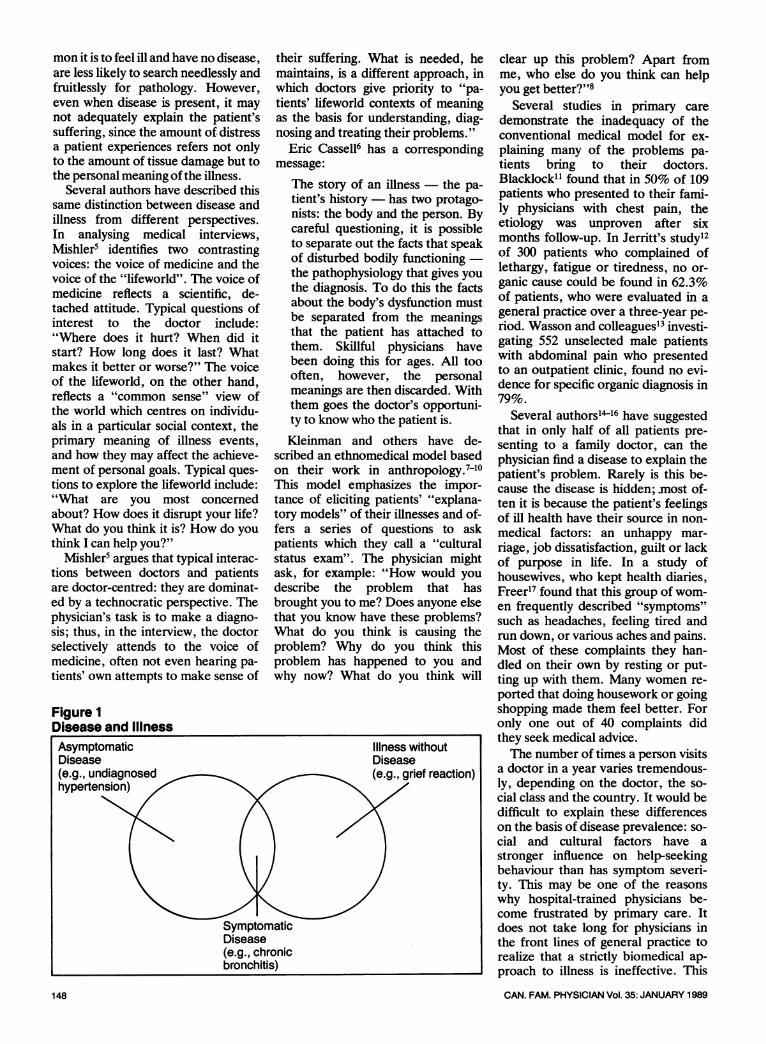
is a distinction between two modes ofill health: disease and illness. Diseaseis an abstraction: the "thing" that iswrong with the body-as-machine; ill-ness, on the other hand, is the pa-tient's personal experience of sick-ness: the thoughts, feelings, andaltered behaviour of someone whofeels sick (Figure 1).
In the biomedical model, sicknessis explained in terms of pathophysiol-
ogy: abnormal structure and functionof tissues and organs. This model is aconceptual framework for under-standing the biological dimensions ofsickness by reducing sickness to dis-ease. The focus is on the body, notthe person. A particular disease iswhat everyone with that disease hasin common, but the illness experi-ences of each person are unique. Dis-ease and illness do not always co-exist. Patients with undiagnosed a-symptomatic disease are not ill; peo-ple who are grieving or worried mayfeel ill but have no disease. Patientsand doctors who recognize this dis-tinction and who realize how com-
147
I
mon it is to feel ill and have no disease,are less likely to search needlessly andfruitlessly for pathology. However,even when disease is present, it maynot adequately explain the patient'ssuffering, since the amount of distressa patient experiences refers not onlyto the amount of tissue damage but tothe personal meaning ofthe illness.
Several authors have described thissame distinction between disease andillness from different perspectives.In analysing medical interviews,Mishlers identifies two contrastingvoices: the voice of medicine and thevoice of the "lifeworld". The voice ofmedicine reflects a scientific, de-tached attitude. Typical questions ofinterest to the doctor include:"Where does it hurt? When did itstart? How long does it last? Whatmakes it better or worse?" The voiceof the lifeworld, on the other hand,reflects a "common sense" view ofthe world which centres on individu-als in a particular social context, theprimary meaning of illness events,and how they may affect the achieve-ment of personal goals. Typical ques-tions to explore the lifeworld include:"What are you most concemedabout? How does it disrupt your life?What do you think it is? How do youthink I can help you?"
Mishler5 argues that typical interac-tions between doctors and patientsare doctor-centred: they are dominat-ed by a technocratic perspective. Thephysician's task is to make a diagno-sis; thus, in the interview, the doctorselectively attends to the voice ofmedicine, often not even hearing pa-tients' own attempts to make sense of
Figure 1Disease and Illness
148
their suffering. What is needed, hemaintains, is a different approach, inwhich doctors give priority to "pa-tients' lifeworld contexts of meaningas the basis for understanding, diag-nosing and treating their problems."
Eric Cassell6 has a correspondingmessage:
The story of an illness the pa-
tient's history has two protago-nists: the body and the person. Bycareful questioning, it is possibleto separate out the facts that speakof disturbed bodily functioningthe pathophysiology that gives youthe diagnosis. To do this the factsabout the body's dysfunction mustbe separated from the meaningsthat the patient has attached tothem. Skillful physicians havebeen doing this for ages. All toooften, however, the personalmeanings are then discarded. Withthem goes the doctor's opportuni-ty to know who the patient is.
Kleinman and others have de-scribed an ethnomedical model basedon their work in anthropology. 7-10This model emphasizes the impor-tance of eliciting patients' "explana-tory models" of their illnesses and of-fers a series of questions to askpatients which they call a "culturalstatus exam". The physician mightask, for example: "How would youdescribe the problem that hasbrought you to me? Does anyone elsethat you know have these problems?What do you think is causing theproblem? Why do you think thisproblem has happened to you andwhy now? What do you think will
clear up this problem? Apart fromme, who else do you think can helpyou get better?"8
Several studies in primary caredemonstrate the inadequacy of theconventional medical model for ex-plaining many of the problems pa-tients bring to their doctors.Blacklock11 found that in 50% of 109patients who presented to their fami-ly physicians with chest pain, theetiology was unproven after sixmonths follow-up. In Jerritt's study12of 300 patients who complained oflethargy, fatigue or tiredness, no or-ganic cause could be found in 62.3%of patients, who were evaluated in ageneral practice over a three-year pe-riod. Wasson and colleagues13 investi-gating 552 unselected male patientswith abdominal pain who presentedto an outpatient clinic, found no evi-dence for specific organic diagnosis in79%.
Several authors14'6 have suggestedthat in only half of all patients pre-senting to a family doctor, can thephysician find a disease to explain thepatient's problem. Rarely is this be-cause the disease is hidden; .most of-ten it is because the patient's feelingsof ill health have their source in non-medical factors: an unhappy mar-riage, job dissatisfaction, guilt or lackof purpose in life. In a study ofhousewives, who kept health diaries,Freer17 found that this group of wom-en frequently described "symptoms"such as headaches, feeling tired andrun down, or various aches and pains.Most of these complaints they han-dled on their own by resting or put-ting up with them. Many women re-ported that doing housework or goingshopping made them feel better. Foronly one out of 40 complaints didthey seek medical advice.The number of times a person visits
a doctor in a year varies tremendous-ly, depending on the doctor, the so-cial class and the country. It would bedifficult to explain these differenceson the basis of disease prevalence: so-cial and cultural factors have astronger influence on help-seekingbehaviour than has symptom severi-ty. This may be one of the reasonswhy hospital-trained physicians be-come frustrated by primary care. Itdoes not take long for physicians inthe front lines of general practice torealize that a strictly biomedical ap-proach to illness is ineffective. This
CAN. FAM. PHYSICIAN Vol. 35: JANUARY 1989
Illness withoutDisease(e.g., grief reaction)
(e.g., chronicbronchitis)
highlights the importance of havingadditional approaches to understand-ing human sickness.
Diagnostic Issues:Understanding theDimensions of IllnessThe reasons patients present them-
selves to their family doctors whenthey do are often more importantthan the diagnosis. Frequently the di-agnosis is obvious or is alreadyknown from previous contacts; oftenthere is no biomedical label to ex-plain the patient's problem. Thus, itis often more helpful to answer thequestion "Why now?" than the ques-tion "What's the diagnosis?" Inchronic illness, for example, a changein a social situation is a more com-mon reason for presenting than achange in the disease or the symp-toms.
Illness experience has many dimen-sions. Illness is often a painful crisisthat will overwhelm the coping abili-ties of some patients and challengeothers to increased personal growth.It is helpful to understand these reac-tions as part of a developmental pro-cess that has three stages: awareness,disorganization, and reorganization.18The first stage, awareness, is charac-terized by ambivalence about know-ing: on the one hand, wanting toknow the truth and to understand theillness and on the other, not wantingto admit that anything could bewrong. At the same time patients areoften struggling with conflictingwishes to remain independent and alonging to be taken care of. Eventual-ly, if the symptoms do not go away,the fact of the illness hits home andtheir sense of being in control of theirown lives is shattered.
This disrupts the universal defence- the magical belief that some-how we are immune from disease,injury and death...The patientwho has struggled to forestall hisawareness of serious illness andthen has finally recognized thetruth is one of the most fragile, de-fenseless, and exquisitely vulnera-ble people one can ever find. Thisis a time of terror and de-pression.18At this stage patients typically re-
gress to childhood defenses and reactto their caretakers as parents ratherthan as equals. They often become
self-centred and demanding, and al-though they may be aware of this re-action and embarrassed by it, theycannot seem to stop it. They maywithdraw from the external worldand become preoccupied with eachlittle change in their bodies. Theirsense of time becomes constrictedand the future seems uncertain; theymay lose a sense of continuity of self.They can no longer trust their bodies,and they feel diminished and out ofcontrol. Their whole sense of theirpersonal identities may be severelythreatened. One reaction to this stateof mind in some patients is rebellion:a desperate attempt to have at leastsome small measure of control overtheir lives even if it is self-destructivein the end.The third stage is reorganization.
In this stage patients call upon all oftheir inner strengths to find newmeaning in the face of illness and, ifpossible, to transcend their plight.Their degree of mastery will be af-fected, of course, by the nature andseverity of the illness. But in addi-tion, the outcome is profoundlyinfluenced by the patients' social sup-ports, especially loving relationshipswithin their families, and by the typeof support their physician can pro-vide.These stages of illness are part of a
normal human response to disasterand not another set of disease catego-ries or psychopathology. But this de-scription emphasizes how the human-ity of the ill person is compromisedand points to an added obligation ofphysicians to their wounded patients.
So great is the assault of illnessupon our being that "it is almost asif our natures themselves were ill,as if the strands or parts of us werebeing forced apart and we vergedon the loss of our own humanness.A phenomenon so great in its ef-fects that it can threaten us withthe loss of our fundamental hu-manness clearly requires morethan technical competence fromthose who would "treat" illness.19
Interviewing MethodsPatients often provide physicians
with cues and prompts about the rea-son they are presenting. These maybe verbal or non-verbal signals. Thepatient may look tearful, sigh deeply,or be short of breath. They may saydirectly, "I feel awful, Doctor. I
CAN. FAM. PHYSICIAN Vol. 35: JANUARY 1989
think this flu is going to kill me." Or,indirectly, they may present a varietyof vague symptoms that are maskinga more serious illness such as depres-sion. As physicians sit down with pa-tients and ask them, "What bringsyou in today?" they must ask them-selves, "Why did the patient comenow? What has precipitated this vis-it?"We propose four dimensions of ill-
ness experience that physiciansshould explore: patients' ideas aboutwhat is wrong; their feelings, espe-cially their fears, about their prob-lems; their expectations of the doc-tor; and the effect of the illness onfunctioning. When physicians addressthese aspects of illness, patients aremore likely to be satisfied with theirdoctors, more likely to comply withthe treatment recommendations, andalso more likely to recover.20What are the patient's ideas about
their illness? What meaning do theyattach to the illness experience?Many persons endure illness as an ir-reparable loss; others may view it asan opportunity to gain valuable in-sight into their life experience. Is theillness seen as a form of punishmentor as an opportunity for dependency?Whatever the illness, knowing itsmeaning is paramount for under-standing the patient.What are the patients' feelings? Do
they fear that the symptoms theypresent may be the precursor of amore serious problem such as cancer?Some patients may feel a sense of re-lief and view the illness as an oppor-tunity for respite from demands or re-sponsibilities. Patients often feelangry or guilty about being ill.What are their expectations of the
doctor? Does the presentation of asore throat carry with it an expecta-tion of penicillin? Do they want thedoctor to do something or just listen?What are the effects of the illness
on function? Does it limit patients'daily activities? Does it impair theirfamily relationships? Does it requirea change in lifestyle?The following examples of physi-
cian-patient dialogue contain specificquestions that physicians might ask toelicit this information.To the doctor's question, "What
brings you in today?", a patient re-sponds, "I've had these severe head-aches for the last few weeks. I'mwondering if there is something that I
149
can do about them." To examine thepatient's ideas about the headaches,the physician might ask (waiting aftereach question for the patient's reply):"What do you think is causing theheadaches? Have you any ideas ortheories about why you might be hav-ing them? Do you think there is anyrelationship between the headachesand current events in your life?"The patient's feelings about the
headaches can be elicited by ques-tions such as: "What are your con-cerns about the headache? Do youthink that something sinister is caus-ing them? Is there something particu-larly worrisome for you about theheadaches?"To determine how the headaches
may be impeding the patient's func-tion, the physician might ask: "Howare your headaches affecting yourday-to-day living? Are they stoppingyou from participating in any activi-ties? Is there any connection betweenthe headaches and the way your life isgoing?"
Finally, to identify the patient's ex-pectations of the physician at this vis-it, the doctor might enquire: "Whatdo you think would help you to dealwith these headaches? Is there somespecific management that you wantfor your headaches? In what way mayI help you? Have you a particular testin mind? What do you think wouldreassure you about these head-aches?"
Certain illnesses or events in thelives of individuals may cause themembarrassment or emotional discom-fort. As a result, patients may not al-ways feel at ease with themselves ortheir physician and may cloak theirprimary concerns by presenting mul-tiple symptoms. The doctor must, onoccasion, respond to each of thesesymptoms to create an environmentin which patients may feel more trust-ing and comfortable about exposingtheir concerns. Often, the physicianwill provide them with an avenue toexpress their feelings by commenting:"I sense that there is something trou-bling you or something more goingon. Can I help you with that?"The following case illustrates pa-
tient-centred interviewing in moredetail:
Case History: Mr. R.Mr. R. is a 58-year-old man who
has been a patient in the practice for
150
10 years. Until eight months ago,when he had a massive myocardial in-farction and required triple coronaryartery bypass surgery, he had been ahealthy man with few problems. He ismarried, with grown children and hasreturned to work as a plumber. Hehas come to the office for diet coun-selling about his elevated cholesterol.The interaction begins with the
doctor stating, "So, Mr. R., you're inabout your diet. Looks like your cho-lesterol levels are dropping nicely.""Yes," responds Mr. R. "That'sgood news and I'm feeling prettygood about my weight. I'm down fivemore pounds and almost at my goal."The doctor proceeds to explore Mr.R.'s diet in some detail.The interview then shifts to Mr.
R.'s weight-loss program, and hestates that he has been dutifully fol-lowing his exercise regimen through-out the summer months and is walk-ing up to four miles a day. The doctorasks, "Will you be able to continueyour walking during the winter?""Oh yes," says Mr. R., "I don't
mind walking in the winter. I quiteenjoy it. I just have to be careful onthose very cold days."
"Yes, you do need to be cautiousduring the severe weather," repliesthe doctor. Mr. R. looks away andappears sad. The doctor pauses andasks, "Is there something concerningyou, Mr. R.?""Oh well...no," says Mr. R. quick-
ly. "No, not really.""Not really?" says the doctor."Well," replies Mr. R., "I was just
thinking about the winter and...well-...no, I guess I'll be able to skidoo if Ijust keep warm.""Why are you concerned that you
won't be able to do that, Mr. R.?",says the doctor.
"Well, I don't know. I'd just miss itif I couldn't participate."
"It sounds as if that activity is im-portant to you," responds the doctor.
"Well, yes, it has been a very im-portant family activity. We havesome land and a little cabin up northof here, and it's really how we spendour winter weekends - the wholefamily together."
"It sounds as if not being able toparticipate in something that's beenan important family activity would bevery difficult for you," reflects thedoctor."Oh, yes it would be. I just feel
that so many things have been takenaway from me that I really wouldmiss not being able to do that."The doctor responds, "Mr. R., it
seems that in the last several months,you have experienced a lot of changesand a lot of losses. I sense it has beenvery difficult for you."
"Yes, Doc, it has. It's been tough.I've gone from being a man who is re-ally healthy and has no problems tohaving a bad heart attack and a bigoperation and being a real weightwatcher. It has been a big change,and it has had its tough moments, butI'm alive and I guess that is what mat-ters," answers Mr. R.
"It seems that you still have a lot offeelings surrounding your heart at-tack and the surgery and the changesthat have occurred," comments thedoctor. "Yes, I have," says Mr. R.,"...I have.""Would it be helpful at some time
for us to talk about that more, to setaside some time just to look at that?"asks the doctor.Mr. R. replies, "Yes it would. It's
hard to talk about, but it would behelpful."
"Just briefly, are you encounteringany problems with sleep or appetiteMr. R.?", inquires the doctor."No, none at all," replies Mr. R.The doctor asks a few more ques-
tions exploring possible symptoms ofdepression. Finding none, he againoffers to talk further with Mr. R. attheir next visit. Mr. R. answers af-firmatively.
In this example the patient's situa-tion can be summarized by using thepatient-centred model as a frame-work:
A) Disease1. Coronary artery disease with pre-vious MI2. Status post CABG3. Obesity4. Hypercholesterolemia
B) Illness1. Ideas:"No longer a healthy man."Seems to see himself as disabled.2. Feelings:Sad about his losses.Fears that he will not be able to par-ticipate in family activities. Perhaps
CAN. FAM. PHYSICIAN Vol. 35: JANUARY 1989
fears another NI or even death.3. Expectations:Co-operates with doctor re diet.Agrees that "talking it out" mighthelp.4. Function:Walks four miles a day.Sexual function should be explored onthe next visit.The doctor already knew the pa-
tient's disorders before the interviewbegan. He picked up on the patient'ssadness and his hesitancy in exploringhow he was experiencing his illness.At the same time, the doctor ruledout serious depression by asking afew diagnostic questions and offeredthe patient an opportunity to explorefurther his feelings about his illness.By considering the patient's illness
experience as a legitimate focus ofenquiry and management, the physi-cian has avoided two potential errors.First, if the conventional biomedicalmodel had been overused, by seekinga disease to explain the patient's dis-tress, the doctor might have labelledthe patient depressed and given himunnecessary and potentially hazard-ous medication. On the other hand,he might have decided the patientwas not depressed, that his distresswas normal and therefore not an is-sue to be discussed further.
This case also illustrates that doc-tors are often very limited in whatthey can do about a patient's disease.Lowering this man's cholesterol is un-likely to have a great effect on hishealth after his disease has pro-gressed so far. However, dealing withthis patient's experience of illnessmay be helpful by alleviating fears,correcting misconceptions, encourag-ing him to discuss his discourage-ment, or simply by "being there" andcaring what happens to him. At thevery least this compassionate concernis a testimony to the fundamentalworth and dignity of the patient: itmight help prevent him from becom-ing truly depressed; it might evenhelp him to live more fully. U
References1. McCracken EC, Stewart MA, BrownJB, McWhinney IR. Patient-centred care:the family practice model. Can FamPhysician 1983; 29:2313-6.
2. Levenstein JH, McCracken EC,McWhinney IR, Stewart MA, Brown JB.Patient-centred clinical method. 1. Amodel for the doctor-patient interaction
in family medicine. Fam Pract 1986;3(1):24-30.
3. Brown J, Stewart M, McCracken E,McWhinney I, Levenstein J. Patient-cen-tred clinical method. 2. Definition andApplication. Fam Pract 1986; 3(2):75-9.
4. Stewart M, Brown J, Levenstein J,McCracken E, McWhinney I. Patient-centred clinical method. 3. Changes inresidents' performance over two monthsof training. Fam Pract 1986; 3(3):164-7.
5. Mishler EG. Discourse ofmedicine: di-alectics of medical interviews. Norwood,NJ: Ablex Publishing, 1984.
6. Cassell EJ. Talking with patients. I.Clinical technique. Cambridge, MA.: TheMIT Press, 1985.
7. Kleinman AM, Eisenberg L, Good B.Culture, illness and care. Ann Int Med1978; 88:251-8.
8. Good BJ, Good M. Meaning of symp-toms: a cultural-hermeneutic model forclinical practice. In: Eisenberg L, Klein-man A, eds. Relevance of social sciencefor medicine. Boston: D. Reidel Publish-ing, 1981.
9. Galazka SS, Eckert JK. Clinically ap-plied anthropology: concepts for the fami-ly physician. J Fam Pract 1986; 22:159-65.
10. Katon W, Kleinman A. Doctor-pa-tient negotiation and other social sciencestrategies in patient care. In: Eisenberg L,Kleinman A, eds. Relevance of social sci-ence for medicine. Boston: D. ReidelPublishing, 1981.
11. Blacklock SM. Symptom of chestpain in family practice. J Fam Pract 1977;4:429-33.
12. Jerritt WA. Lethargy in general prac-tice. Practitioner 1981; 225:731-7.
13. Wasson JH, Sox HC, Sox CH. Diag-nosis of abdominal pain in ambulatorymale patients. Medical Decision Making1981; 1:215-24.
14. Morell DC. Symptom interpretationin general practice. J Royal Coll GenPractitioners 1972; 22:297.
15.Peabody FW. Care of the patient. JAm Med Assoc 1927; 88:877-82.
16. Research Committee of the Collegeof General Practitioners. Continuing ob-servation and recording of morbidity. JColl Gen Practitioners 1958; 1:107.
17. Freer CB. Self-care: a health diarystudy. Medical Care 1980; 18:853-61.
18. Reiser D, Schroder AK. Patient inter-viewing: the human dimension. Baltimore:Williams and Wilkins, 1980.
19. Kestenbaum V. Humanity of the ill:phenomenological perspectives. Knox-ville: University of Tennessee Press, 1982.
20. Stewart MA, Brown JB, WestonWW. Patient-centred interviewing. III.Five provocative questions about the pa-tient-centred approach. Can FainPhysician 1989; 35:159-161.
CAN. FAM. PHYSICIAN Vol. 35: JANUARY 1989
HypertensionDetection and Management
PROCEEDINGSNOW AVAILABLEThis important symposium-took place at the University ofCalgary in October 1984.Sponsored by the College ofFamily Physicians of Canada,the University of Calgary andthe Alberta HeritageFoundation for MedicalResearch, it brought togetherresearchers from cardiology,genetics, public health andfamily practice. Thesymposium produced threepolicy statements: a protocolfor initial assessment of highblood pressure, a protocol formanaging hypertension, anda screening policy for thefamily physician's office. The60-page proceedings are nowavailable, including all of thepolicy statements and the fulltexts of the 12 papers plus thesummnaries of discussion.
60 page proceedings:$3 per copy
Discount availablefor quantity
Order fromCanadian Family Physician1200 Sheppard Ave. E., #507Willowdale, Ont. M2K 2S5Make cheques payable toCanadian Family Physician.
151