Embed Size (px)
Citation preview

ISSN: 2220-7562
JBUMDCThe Journal of Bahria University Medical and Dental College
Bahria University Medical & Dental College,Adjacent PNS Shifa, DHA Phase II, Karachi.
Recognized by PMDC
Volume-6, Issue-2, April-June, 2016

Correspondence address:Editor, JBUMDC, Bahria University Medical & Dental College, Adjacent PNS Shifa,
DHA Phase II, Karachi, Pakistan.
Ph: +92-21-35319491-9
Website: http://jbumdc.bahria.edu.pk
JBUMDC Web Mail: [email protected]
Published by: Bahria University Medical & Dental College Karachi

JBUMDC ISSN 2220-7562
Vice Admiral (Retd) Tanveer Faiz HI (M)Rector Bahria University, Pakistan.
Patron-in-Chief
Vice Admiral (Retd) Tahseen Ullah Khan HI (M)Director General Bahria University Medical & Dental College, Karachi.
Patron
Fatema JawadHuma Qureshi
Kamran HameedKhalid Mehmood
Samad SheraSyed Tipu Sultan
Members Advisory Board
Aamir Omair (KSA)Ambreen Ahmed (USA)Farida Habib (KSA)
Irfanullah Siddiqi (KSA)Mukhtiar Baig (KSA)Raheela Hafeez (USA)
Sadiqa Syed (KSA)Shamaun Razi (KSA)S. Moazzam Zaidi (Newzealand)
Members Editorial Board - International
The Journal of Bahria University Medical and Dental CollegeKarachi, Pakistan
Indexed with PakMediNetPeer Reviewed Multidisciplinary Quaterly Published Journal
Asad Ullah Khan, Irfan Ali Mirza, Kulsoom FatimaAssistant Editors
Iqbal HussainAssociate Editor
Nasim KarimEditor
Shaheen MoinEditor-in-Chief
Members Editorial Board - National
Aafia Zafar (AKUH)Abid Azhar (KIBJE)Ahmed Danyal (NM&DC)Ambreen Usmani (BUMDC)Anis Jaffery (BUMDC)Hasan Ali (BUMDC)Imran Shaikh (BUMDC)Khalida Nasreen (BUMDC)Khalid Mustafa (BUMDC)
Masood Qureshi (DUHS)Mehreen Latif (BUMDC)Mohiuddin Alamgir (BUMDC)Munawar Ansari (LUMHS)Mushtaque Memon (BUMDC)Naheed Sultan (BUMDC)Nighat Huda (LNH)Nighat Rukhsana (BUMDC)Qamar Jamal (ZMU)
Razia Korego (BUMDC)Saeeda Baig (ZMU)Sameer Shahid Ameen (BUMDC)Sajid Abbas Jaffri (BUMDC)Shazia Shakoor (BUMDC)Shahid Noor (LNH)Shakeel Ahmed (BUMDC)Sher Shah Syed (AH)Zubair Ahmed Abbasi (BUMDC)
Editorial AssistantsArsalan AhmedTahira Zamir

67
69
76
81
84
88
92
97
101
106
121
124
127
130
131
CONTENTS Volume-6, Issue-2, April-June, 2016
EDITORIAL
REVIEW ARTICLE
ORIGINAL ARTICLES
COMMENTARY
STUDENT CORNER
CASE REPORT
LETTER TO EDITOR
JBUMDC INSTRUCTION TO AUTHORS
Stress and its AftermathsKhalid Mustafa
Lead and its Health HazardsSyed Sanowar Ali, Nasim Karim
1. Caries Experience and Oral Health Status among Disabled Individuals of Special School of Gadap Town Karachi
Asghar Ali, Muhammad Ali Leghari, Samreen Mazhar, Mahwish Bano2. Frequency of Neck Swellings in Patients Coming for Dental Check-up in a Sample of Pakistani
PopulationYousuf Lakdawala, Dawar Nadeem, Zeerak Jarrar, Syeda Maria Fakhar
3. Efficacy of Steroid Injection in the Treatment of Trigger FingerAdeel Ahmed Siddiqui, Farooq Mamji, Badaruddin Sahito, Syed Mohammad Tariq, Dileep Kumar ,Syed Itaat Hussain Zaidi
4. Comparison of Gonial Angle Determination from Cephalograms and Orthopantomogram ofPatients under Orthodontic TreatmentMansoor Majeed, Imtiaz Ahmed
5. Radial Head Fracture Mason Type III and IV Treated with K -wire FixationFarooq Mamji, Badaruddin Sahito, Adeel Ahmed Siddiqui, Syed Mohammad Tariq, Dileep Kumar,Syed Itaaat Hussain Zaidi
6. Assessment of Parents’ Attitude toward EPI (Expanded Program on Immunization) in TertiaryCare Hospitals of KarachiAbdul Qadir, Khola Noreen, Tahira Zamir, Muhammad Sajid Abbas Jaffri, Nazish Fatima, Rehana Khan, Sadia Atta
7. Leflunomide in Rheumatoid Arthritis: Effect on Laboratory ParametersFuad Shaikh, Shaikh Nadeem Ahmed, Shamaila Khalid, Nasim Karim
8. Frequency of Dental Caries and Status of Permanent Mandibular First Molar in Young AdultsSyed Ahmed Omer, Daud Mirza, Isra Ahmed, Omer Moosani, Syed Muzzamil Ali Shah
9. Comparison of Anticonvulsant Effects of Combined Regimens of Gabapentin and Verapamilwith their Individual EffectsItefaq Hussain Qureshi, Shahbana Usman Simjee
10.Socio Cultural Determinants of Low Contraceptive Use and High Unmet Needs in Married Females of Urban Karachi
Khaula Noreen, Nadia Khalid, Imran Shaikh, Tahira Zamir, , Marium Shoaib, Azka Shahab, Aisha Siddiqua,Osama Rehman
Spinal Cord Stroke: An Uncommon Diagnosis behind Common Symptoms!!Anoshia Afzal, Maria Shoaib
Cultural Day Celebration at Bahria University Medical & Dental CollegeSara Abbassi, Tahira Zamir, Hasan Ali
An Incidental Finding of Ovarian Brenner TumorNazish Jaffar, Noshaba Rahat, Saroona Haroon, Syed Mehmood Hasan
Personalized Medicine- A New Genomic EraMaria Shoaib
110
116

Stress is a normal psychological and physical reactionto increasing demands of our life. People experiencechallenges with stress at some point during their life.Our brain has an alarm system that provides us protection.When our brain perceives a threat, it signals the bodyto release a burst of hormones in order to generate theresponse. This is called the "fight-or-flight" response.Once such a situation is over the body returns to it`snormal state. However, today residing in a modernizedworld alarm bell scarcely is turned off rather we cansay the bell keeps on ringing off and on. Continuous orhigh levels of stress can have bad impact on our livesand therefore we should take care of it before it canprogress to point of no return.Thus stress can be definedas the brain's response to any demand. It can be stimulatedby various triggers that may be real or just the imaginationof a person such as daily routines as going to school orwork every day, looking after the matters of home,helping children in doing homework etc. and they couldbe more serious things like death, diseases, accidentsetc. Moreover it could be violence and unrest prevailingin the environment of our society leading to emotionaland physical trauma and distress.1
Stress is not always bad as it may be the sense ofresponsibility of any person to the assigned task andeagerness to accomplish the task within the specifiedperiod with dedication and elegance. So is the stressthat is rather involuntary and is associated with conditionsas examination, surgery etc. Stress is said to be trouble-some when it lingers on and affects the performance ofan individual on continuous basis. In short term whenwe face a dangerous situation our pulse quickens, breathbecomes faster, muscles become tense, our brain usesmore oxygen and increases activity which is beneficialbut if it becomes long term that is becomes persistenteven after the situation or task subsides then problemsarise.Thus chronic stress is the response to emotionalpressure suffered for a prolonged period over which anindividual perceives he or she has no control. It involvesan endocrine system response causing release ofcorticosteroids. While the immediate effects of stresshormones are beneficial in a particular situation, long-term exposure to stress creates a high level of thesehormones that remains constant. This may lead to highblood pressure and subsequently heart disease, damageto muscle tissue, inhibition of growth, suppression ofthe immune system and damage to mental health.2
Different types of stressors, the timing (duration) of thestressors, and personal characteristics all influence theresponse of the hypothalamic-pituitary adrenal axis,which is implicated in many theories and relate chronicstress with health morbidities. Symptoms of chronicstress can vary from anxiety, depression, social isolation,headache, abdominal pain or lack of sleep to backpainetc. Other symptoms include hypertension and cardio-vascular diseases, hemorrhoids,varicose veins, panicattacks or panic disorder.3,4,5 The signs and symptomsof stress are mainly categorized into(1) Common features such as sleep disturbances, clen-
ching of jaw, grinding of teeth, digestive upsets,feeling of lump in throat, difficulty in swallowing,agitated behavior, twiddling of fingers, playingwith hairs, increased heart rate, generalized restles-sness, sense of muscle tension in the body or actualmuscle twitching, non-cardiac chest pains,dizziness,light heartedness, hyperventilation, sweaty palms,nervousness, stumbling over words, high bloodpressure, lack of energy, fatigue etc.
(2) Cognitive features of stress such as mental slowness,confusion, general negative attitudes or thoughts,constant worry, difficulty in concentrating, forgetful-ness, difficulty in logical thinking, inability to solveproblems6
(3) Emotional features of stress such as irritation, nosense of humor, frustration, jumpiness, over-excita-bility, feeling overworked,sense of helplessness,apathy
(4) Behavioral features of stress such as decreasedcontact with family and friends, poor work relations,sense of loneliness, decreased sex drive, avoidingothers, failing to set aside times for relaxation thro-ugh activities such as hobbies, music, art or reading.7Thus stress makes it difficult to control our emotions,it bring out diseases, can ruin our teeth, heart andmental status, can make us fat and look older andcan weaken our immune system8
5 R'S OF STRESS REDUCTION:9
There are 5 core concepts which are used in the reductionof anxiety or stress:Recognition of the causes and sources of the threat ordistress; education and consciousness raisingRelationships identified for support, help, reassuranceRemoval from (or of) the threat or stressor; managingthe stimulusRelaxation through techniques such as meditation,massage, breathing exercises, or imageryRe-engagement through managed re-exposure anddesensitizationCOPING STEPS TO REDUCE STRESS:10,11
The effects of stress tend to build up over time. Beforeit may cause a vicious circle and compromise our lifeit should be disrupted through some coping steps:• Staying in touch with people who can provide
EDITORIAL
JBUMDC 2016; 6(2): 67-68 Page-67
Stress and its AftermathsKhalid Mustafa
Dr. Khalid MustafaProfessorDepartment of PharmacologyBahria University Medical & Dental CollegeKarachi.Email: [email protected]: 07-05-2016Accepted: 09-05-2016

emotional and other support like friends, family,and community or religious organizations to reducestress due to work burdens or family issues
• Recognizing signs of our body's response to stress,such as difficulty sleeping, being easily angered,feeling of depression, and having low energy
• Setting priorities and learn to say no to new tasksif they are overloading or burdening us
• Noting always accomplishments at the end of theday
• Trying always but avoiding guilty feeling for thingswe have been unable to do
• Avoiding lingering on with the problems.• Trying to get help from others in case of need• Switching to healthy life style changes such as 30
minutes gentle walking every day• Scheduling some time on daily basis for healthy
and relaxing activities• Exploring meditation, yoga, tai chi, or other gentle
exercises• Eating simple healthy preferably home-made food• Seeking help from a qualified mental health care
provider for psychotherapy and or medications
REFERENCES:1. The Effects of Stress on Your Body - Web MD
http://www.webmd.com/balance/stress-management/effects-of-stress-on-your-bodyJun24,2014 Accessed on03-05-2016
2. Neil C .Physiology of Behavior. Pearson. 2013 pp.602-
6. ISBN 97802052393993. Gregory EM, Edith C, Eric S Z. If it goes up, must
it come down? Chronic stress and the hypothalamicpituitary-adrenocortical axis in humans. PsychologicalBulletin 2007; 133 (1): 25-45. doi:10.1037/00332909.133.1.25.PMID 17201569
4. Cohen S, Janicki-Deverts D, Miller GE Psychologicalstress and disease. JAMA 2007; 298 (14):1685-7 doi:10.1001/jama.298.14.1685. PMID 17925521
5. Metcalfe C, Smith G D. Self-reported stress and subse-quent hospital admissions as a result of hypertension,varicose veins and haemorrhoids. Journal of Public Hea-lth Medicine 2003; 25 (1): 62-8.doi:10.1093/ pubmed/fdg013. PMID 12669921
6. The Impact of Stress | Psych Central http://psychcentral.com/lib/the-impact-of-stress/Oct 30,2015. Accessedon 03-05-2016
7. Benson H,Beary JF, Carol MP. The Relaxation Response.Psychiatry 1974;37:37-46
8. 8 Ways Stress Is More Dangerous Than You Think -Healthlinehttp://www.healthline.com/health news/mental-eight-ways-stress-harms-your-health 082713 Aug 27,2013. Accessed on 05-05-2016
9. Patricia P. Canadian Fundamentals of Nursing(5ed.). 2014 Toronto: Elsevier. pp. 472-88
10. Ruth C, Constance H,Sharon J. Fundatmentalsof Nursing: Human and Health Function (7 ed.).2013 Philadephia: Lippincott Williams & Wilkins. p.1319
11. NIMH » Fact Sheet on Stress - National Instituteof Mental Health https://www.nimh.nih.gov /health/publications/stress/Accessed on 05-05-2016
JBUMDC 2016; 6(2): 67-68 Page-68
Khalid Mustafa

INTRODUCTION:The use of metals like lead, mercury, cadmium, arsenicetc. has played a crucial role in the progress and successof present civilization. Metals are important source ofpollutant toxicants which are all naturally occurring inthe human environment. Now-a-days many metals havebecome essential to various biological processes andsome level of human exposure is therefore unavoidable.Thus essential metals are becoming toxic with increasingexposure. Worldwide toxic metals are being used fordifferent purposes since hundreds of years such as Lead(Pb) that is said to be in use for at least 5000 years. Itwas employed in building materials, glazing ceramicpigments, and water pipes. Lead acetate during theRoman times was used to sweeten old wine, and someRomans might have consumed large amount of lead asmuch as one gram per day. Use of lead by humanprobably started prior to 2000 BC, at that time abundantsupplies were obtained from minerals as a by-productof silver smelting. In 370 BC credit has been given toHippocrates for the first description of abdominal colicin a man who extracted metals.1
Lead is also known as the horror mineral because it isassociated with violence, lowered IQ, Attention DeficitDisorder, Attention Deficit Hyperactivity Disorder(ADHD) and other neurological diseases. It is acommonly distributed toxic metal with extensive usesin industry. Till 1970s lead was added to gasoline. Thenew gasoline has manganese in it instead of lead. It isalso present in paints, lubricants, medications, cosmetics(i.e. lipstick) and inks. Books have been written on thetoxicity of lead, which describe the lead related conditions
from anemia to death.2 The effects produced by the toxicmetals also depend upon the half-life and eliminationof the metals for example the biological half-life of leadin bone is 20-30 years. Thus continuous metal exposuremay follow retention kinetics .The blood lead level inpopulation of United States had elevated about 0.7-4.4µg/dl in both genders with age limit of >1 to >60.3 Themain analytical problem in determining trace metals inblood contains lead levels and the data pertaining tolead levels in the population of United States has beenreported by Center for Disease Control and Prevention(CDC). 4 This is clearly highlighting that the task is noteasy at the level of technically advance country and inlight of this one can think about the situation in our partof the world and in our country where heavy metalstheir toxicity and related complications are not addressedwith due attention and there is paucity of documentedliterature. Present review is therefore written to providecomprehensive awareness regarding the sources,exposure to humans, health hazards, analytical techniquesand measures to reduce if not prevent the problemscaused by lead.
METHODOLOGY:Articles were collected and identified by using electrondata bases Google Search, Google Scholar, Pubmedfrom 2000-2016. Keywords and phrases used were lead,heavy metals, toxic metal, lead toxicity, human exposureto lead, diseases caused by lead exposure. 200 articleswere selected. Inclusion criteria was review articles,original articles, CDC and WHO reports. Exclusioncriteria was articles related to animal studies, articleswith heavy metals other then lead. Filters used werehealth hazards and human dangers. A total of 60 articlesthat met the inclusion criteria were included in this writeup.
LITERATURE REVIEW:Lead (Pb) occurs naturally in the environment. Lead(Pb) has been used by humans for at least 7000 yearsalone and in combination with arsenic and antimony.Lead (Pb) is a highly toxic, ductile and malleable metalthat is easy to smelt. Lead occurs naturally in the earth’scrust. It is also called as plumbum derived from Latinand is designated as Pb. Metallic lead (Pb) is resistantto corrosion and can combine other metals to formvarious alloys. Organo-lead compounds are dominated
REVIEW ARTICLE
JBUMDC 2016; 6(2): 69-75 Page-69
ABSTRACT:Metals are important source of pollutant toxicants which occur naturally in the environment. Now-a-days many metals have becomeessential to various biological processes and some level of human exposure is therefore unavoidable. Lead has been used by humansfor at least 7000 years alone and in combination with other metals. It is highly toxic, ductile, malleable and easy to smelt. A widerange of adverse effects could be induced in human beings depending upon the dose and time period of lead exposure. Centralnervous system of children is the most sensitive to lead effects while peripheral neuropathy, chronic nephropathy, and hypertensionare the main concerns in adults. Other target tissues include the gastrointestinal, immune, skeletal, and reproductive systems. Effectson the heme biosynthesis provide a sensitive biochemical indicator even in the absence of other detectable effects. Present reviewis therefore written to provide comprehensive awareness regarding lead and its health hazards.Keywords: Heavy metals, Lead, Human exposure, Health hazards, Toxicity, Prevention
Lead and its Health HazardsSyed Sanowar Ali1, Nasim Karim2
Dr. Syed Sanowar AliAssociate ProfessorDepartment of Community Health SciencesUnited Medical & Dental CollegeKarachiEmail: [email protected]
Dr. Nasim KarimProfessor & HeadDepartment of PharmacologyBahria University Medical & Dental CollegeKarachiReceived: 02-04-2016Revised: 04-05-2016Accepted: 07-05-2016

JBUMDC 2016; 6(2): 69-75 Page-70
Syed Sanowar Ali1, Nasim Karim2
by Pb4+. Inorganic lead compounds are used as pigmentsin paints, dyes, and ceramic glazes. Organo-lead compou-nds were used as gasoline additives. Lead is primarilyderived from such human activities as mining, man-ufacturing, and burning fossil fuels that is found in allparts of the environment. Lead (Pb) has been a ubiquitousenvironmental pollutant, and is toxic even in low doses.Primary production and reprocessing of Pb is based onsmelting, with substantial emission of metal fumes.Lead (Pb) toxicity exert impact on the nervous system,both in adults and children.5 Lead alloys are used inbatteries, shields from radiation, water pipes, andammunition. Environmental lead comes mainly fromhuman activity and is listed as a top toxic substance.6
Lead toxicity problem has become more serious withthe industrial expansion in the last two centuries, asevident from the Antarctic and Arctic ice core datashowing presence of lead even in such far off places.The cognitive deficits, neurotoxicity, behavior disorders,growth problems, reduced heme synthesis and impairedhearing are reported as adverse effects of Pb. It has beenobserved that blood lead is associated with house dustconcentrations of lead, the duration of time spent workingin a closed workshop and the year in which the subjectmoved into that residence.7,8
Lead is not biodegradable and the concerns forecotoxicity of lead are increasing. For instance, theleaded fish sinkers or pellets lost in the bottom of lakesand river banks can be mistaken for stone and ingestedby birds causing adverse effects including death.9 Aprimary source of lead exposure in children is lead-containing paint however major environmental sourcesof lead exposure is hand-to-mouth transfer of leadcontaining paint chips or dust from floors of olderhousing or from neighborhood soil among infants andtoddlers up to 4 years of age.10,11
Pharmacokinetic characteristics: Lead absorptioncommonly occurs from lungs and depends upon vaporversus particle size and concentration. About 90% oflead particles are small and are readily absorbed throughalveoli into blood. 99% of lead in blood binds to hemog-lobin leaving only 1% for tissue distribution such askidney, liver, skeleton and hair. The fraction of lead inbone increases with age from 70% of body burden inchildhood to as much as 95% in adulthood, with a half-life of about 20 years however in blood lead half-life isabout 30 days. Lead in trabecular bone is more labileand has a shorter turnover time than cortical bone. Leadreleased from bones may contribute up to 50% of thelead in blood, and is a significant source of endogenousexposure. Bone lead release may be important in adultswith accumulated occupational exposure and in womendue to bone resorption during pregnancy, lactation,menopause, and from osteoporosis.12 Lead is eliminatedvia kidney and bile.Sources of lead: There are many sources of lead in ourenvironment.(1) Food SourcesAgriculture lands near the industries and highways areat a greater risk of becoming contaminated by toxic
metals. Even old house paint (Pb),sprays, insecticidesand processes that involved fruits refining predisposehuman beings to metal toxicities. The food sources oflead are rice, milk, carrot, wheat, potato, calcium supple-ment, eggs, cocoa powder, smoked food, wine, beer,raisons etc.(2) Drinking water: Contamination of water (wellsand municipal water) by toxic metals is an importantsource of affecting humans. Pipes made of plastic, lead,copper and galvanized pipes can be an important sourceof water contamination particularly soft watercontamination. The largest source of lead in drinkingwater occurs through leaching from lead-containingpipes, faucets, and solder, which can be found in plumb-ing of older buildings.13,14
(3) Lead paint: Lead carbonate [PbCO3/ Pb(OH)2)]was added to paints to speed drying, improve durability,and protect the surface from corrosion before 1978 whenit was banned. All those who are concerned frommanufacturing to use of lead containing paints are atincreased risk but children are at particular risk fromlead paints because they occasionally might eat paintchips. Lead paint can have a sweet taste, and babies andtoddlers will often lick or suck window sills, crib bars,and other objects that may be coated with lead paint.Leaded dust from peeling, chipping, cracking orotherwise deteriorating lead paint will collect onto floorsand other surfaces. Children touch the dust, and thenput their fingers in their mouths.(4) Imported candies: Lead has been found in candyand candy wrappers imported primarily from Mexicoand Asia.15
(5) Hobbies and art: Some art supplies, such as artists'paint, still have lead in them. Some hobbies require theuse of lead, such as stained glass, firing guns, makingammunition, and making fishing lures and sinkers.(6) Contaminated soil: Another common source oflead is contaminated soil. Two possible sources ofcontaminated soil are leaded gasoline and industrialoperations like smelters. While gasoline is generally nolonger a major source of lead, decades of leaded gasolineleft contamination in the soil next to roadways up toone-quarter of a mile from the road might be a sourceto expose children. They play on or near the floor andmake their hands dirty. Often they put their fingers intotheir mouths. In addition urban environments incomparison to rural receive higher depositions of leadfrom vehicular emissions and are therefore at a greaterrisk. Similarly smelter operations also contaminate thesoil and thereby expose the workers and the nearby landto a risk.(7) Jewelry: Some jewelry is made of lead and canpose a danger to children if they put the jewelry in theirmouths.(8) Lead at work: Adults who work in industries thatuse lead (battery manufacturing, pipe fitting, firingranges, demolition, glass production, smelting operations,etc.) should be careful not to bring lead home with them,shower and change clothes and shoes at work.(9) Dishware: Imported glazed pottery and leaded

JBUMDC 2016; 6(2): 69-75 Page-71
Lead and its Health Hazards
crystal may also be sources of lead.(10) Mini-blinds: Vinyl mini-blinds exported by China,Indonesia, Taiwan and Mexico before 1997 containedlead, which was used to make them less brittle. Leaddust forms on the blinds, particularly when the blindsare exposed to sun and heat.(11) Lunch boxes: There is evidence that some softvinyl lunch boxes may contain lead in the lining.16
(12) Herbal medicines: Lead poisoning is reported tobe caused by contaminated ayurvedic herbal products.Effect of lead on Human Health: The effects of leadon human health can be summarized as in:(A) Children: They may suffer from learning disabilit-ies resulting in a decreased intelligence (decreased IQ),attention deficit disorder, behavior issues, nervous systemdamage, speech and language impairment, decreasedmuscle growth, decreased bone growth, kidney damageetc. The neurotoxicity of lead is of particular concern,because evidence from prospective longitudinal studieshas shown that neurobehavioral effects, such as impairedacademic performance and deficits in motor skills, maypersist even after Pb blood levels have returned tonormal. Although no threshold level for these effectshas been established, the available evidence suggeststhat lead toxicity may occur at Pb blood levels of 10-15 mcg/dl or possibly less. High levels of lead are lifethreatening and can cause seizures, unconsciousness,and death.(B) Adults: Multiple problems are related to high levelsof lead in adults such as increase chance of illness duringpregnancy, harm to a fetus including brain damage ordeath, fertility problems in men as well as women, highblood pressure, digestive issues, nerve disorders, memoryand concentration problems, muscle and joint pain etc. Thus a wide range of adverse effects could be inducedin human beings depending upon the dose and timeperiod of lead exposure. The central nervous system ofchildren is the most sensitive to lead effects whileperipheral neuropathy, chronic nephropathy, andhypertension are the main concerns in adults. Othertarget tissues include the gastrointestinal, immune,skeletal, and reproductive systems. Effects on the hemebiosynthesis provide a sensitive biochemical indicatoreven in the absence of other detectable effects.Thepsychomotor tests or mental development indices, andbroad measures of IQ are found to be the most sensitiveindicators of adverse neurological outcomes and 2 to 4point IQ deficit for each µg/dL increase in BLL withinthe range of 5–35 µg/dL with deficits in cognitive andacademic skills could occur with BLL <5.0 µg/dL.17Allthese systems play a critical role in synaptic plasticityand cellular mechanisms for cognitive function, learning,and memory because lead affects virtually everyneurotransmitter system in the brain, includingglutaminergic, dopaminergic, and cholinergic systems.Diseases caused by lead are:(1) Anemia: There is a significant negative relationshippresent between blood lead levels and hemoglobinpercentage. Increased blood lead concentration maycause a decrease in hemoglobin percentage in some
individuals. Increased blood lead concentrations alsocause decrease in serum ferritin and body iron. It hasbeen found that high dietary ferrous intake is associatedwith decrease blood lead concentrations.18
(2) Heart diseases: Lead and various other metals arealso involved in producing an increase in cardiovasculardiseases.19 In this regard lead produced hypertension,coronary heart disease, stroke and peripheral arterialdiseases. Lustberg and Silbergeld 20 investigated thatthe accumulation of toxic metals such as Pb in adultsare associated with heart diseases, cancer and infertility.Further investigations about toxicity of these metalshave shown that they produce atherosclerosis byincreasing oxidative stress.21
(3) Hypertension: Lead cause hypertension.22,23 Oncethe arteries become inflamed and brittle they becomeliable to rupture.Ca and fatty plaques prevents thisrupture. The plaque in turn decreases the interior diameterof the arteries and increases blood pressure. The BLLand blood pressure has a weak, but significant association.The lead-induced hypertension and other cardiovasculardiseases, is multifactorial including the pathogenesis(1) The endogenous nitric oxide and cGMP inactivationpossibly through lead-induced reactive oxygen species;(2) The renin–angiotensin–aldosterone system changesand increases in sympathetic activity. (3) Alterations incalcium-activated functions of vascular smooth musclecells including contractility by decreasing Na+/K+ATPase activity and stimulation of the Na+/Ca++exchange pump (4) A possible rise in endothelin andthromboxane.24,25
(4) CNS diseases: Increases in peak blood leadconcentrations result in lower activity in the CNS. Theexistence of this effect is much greater than is currentlybelieved.26 A study has documented that Pb interactswith Ca-regulated enzymes such as protein Kinase Cand causes oxidative damage.27,28
(5) Reproductive diseases: The population of womenexposed to toxic metals either at work or in their homeenvironment showed a correlation between high toxicmetals levels in different biological specimen and thelow birth weight of their children. Toxic metals causepremature birth, congenital malformation and evendisturb production of chorionic gonadotrophin by theplacenta and impair development of the newborn vascularsystem. There is evidence that statistical differencebetween mothers of healthy children compared tomothers of children with locomotor system malformationregarding toxic metal concentrations in various biologicalsamples.29
(6) Kidney diseases: Lead can cause acute and chronicnephrotoxicity. The proximal tubular dysfunction causedby acute lead nephrotoxicity that could be reversed bytreatment with chelating agents. Acute and chronicnephrotoxicity results in a characteristic microscopicchange is the presence of intra-nuclear inclusion bodies(composed of a lead– protein complex) and appearedas a dense, homogeneous eosinophilic with hematoxylinand eosin staining. High level of lead in a relativelyinert, non-toxic state was found in inclusion bodies

JBUMDC 2016; 6(2): 69-75 Page-72
Syed Sanowar Ali1, Nasim Karim2
having acidic protein component composed of mainlywith aspartic and glutamic acid residues with littlecystine. Metallothionein is found on the outer surfaceof lead inclusion bodies and facilitates the transport ofmetal to the forming inclusion. Various heme containingenzymes are synthesized in the kidney. Their synthesisis affected by lead induced nephrotoxicity. This alsoaffects Vitamin D metabolism leading to effects onbones and uric acid metabolism thus causinghyperuricemia, gout etc.30,31
(7) Immunotoxicity: Lead immunotoxicity might bea risk factor for childhood asthma 32,33 because IgE levelwas increased and inflammatory cytokines were foundin lead-exposed neonatal rodents may be indicated anassociation between BLL and elevated IgE levels inchildren.34
(8) Bones and Teeth: Lead gets deposited in teeth andinhibits mineralization of enamel and dentine. It affectsosteoblasts, osteoclasts and chrondrocytes by producingosteoporosis and delays in fracture repair. 35,36
(9) Other diseases: Lead exposure increases the riskof various types of cancers including lung, brain, stomach,kidney, bladder cancers etc. 37,38,39 Severe deficiency andpresence of essential trace elements in excess amountsboth can affect the host response to combat pathogensespecially the former increases the incidence, durationand severity of microbial infections. 40,41,42
Analytical techniques for estimation of lead level:Biomedical analysis of toxic metals in biological sampleslike nails, blood, urine and hairs etc. is done becauseheavy metals concentration may give a picture fordiagnosis of diseases.43 Blood analysis give presentstatus of metals load of body and it is usually found tobe different than accumulation of metals in tissues.Whole blood analysis measures total metal levels thatis present in the intracellular (within circulating bloodcells) and extracellular (serum/plasma) fluids.44 Bloodcirculation of various elements particularly the toxicones is proportional to their depot-storage rangeproperties which can be met by urine and hair testing.45,46
Analysis of metals in urine is an important tool indiagnosis of various diseases and can be easily donealong with blood analysis, as toxic metals may bedeposited in various tissues like kidney, bone etc. withoutraising blood level. It has been observed that hair providesvital clues about body nutritional imbalances besideshair have simple matrix for analysis and almost tentimes higher concentration as compared to blood andurine sample. Hairs are easy to collect, transfer and forstorage in laboratory without any specific condition.Drug consumption and drug abuse and/or metaboliteanalysis in the hairs is commonly recommended.However hair cleaning before analysis is not an easytask because of endogenous and exogenous metal originand removal is significant before analysis. Hairs maybe contaminated by exogenous and endogenous sourcesof toxic metals. Human health research requires toxicmetals to be monitored in all biological matrices. Fororganic and inorganic matrices, samples are dissolvedand pretreated prior to instrumental analysis as in metal
determination by atomic absorption spectrometry (AAS)requires a preliminary sample treatment.47,48 In AASsample preparation involve digestion, extraction andcalibration by Certified Reference Material (CRMs ) ofanalytes before the analysis of samples. Conventionalsample preparation of organic materials for atomicabsorption spectrometric analysis involves solubulizationand or decomposition of the matrix typically achievedby wet digestion or dry ashing techniques using oxidativeacids.49 Different sample pre-treatments for metals havebeen developed for organic and biological samples. Thedirect sample introduction, as slurry sampling techniquehas also been used for pretreatment by avoiding the useof reagents and dilutions that can introduce contaminantbesides no losses of volatile elements, safety of operation,short time duration and small amount of sample.50
Biological samples: The human biological sampleswhich are used in analysis are blood, urine, nail andhair but estimation of lead in blood is the common one.Blood lead levels (BLL) test is used as a biomarker forhuman lead exposure 51
Hairs: The characteristics of hair make them an attractivebio-monitoring substrate52,53,54 Methods based on acidor alkaline digestion are commonly used. Samples aredigested by addition of concentrated nitric acid in abeaker heated on a hot plate, after which hydrogenperoxide and nitric acids is added.55
Nails: Estimating the levels of toxic metals in nails isa common method of biological monitoring, diagnosisand assessment of metal exposures and their risks.Determination of toxic metals in finger nails has beenassayed by atomic absorption spectrophotometry.56,57
Blood: Human Serum (5-10 ml) taken in a flask andadded with 10 ml of concentrated nitric acid withdigestion under gentle heating followed by cooling havebeen employed.58 The diagnosis of diseases, intoxicationand exposure to toxic metals is frequently evaluated bydetermining their concentrations in body fluids. Whenthe analyses of whole blood were performed withoutsample digestion, the carbonaceous residues weregenerated in the graphite tube after several heatingcycles.59
Urine: Determination of toxic metals in urine is usedcommonly in biological monitoring.60
PREVENTIVE MEASURES:(1) Clean and safe drinking wáter from wells and muni-
cipal supplies(2) Protect houses by avoiding lead containing paints
& reduce lead dust(3) Reduce dust levels in homes by:· Using a door mat to remove dirt from shoes before
taking them off. Clean dust from underneath thematt frequently.
· Taking off shoes before going into home. Evenafter scraping off dirt, shoes will track some dustand lead into home.
· Keeping play areas clean. Frequently wash toys,pacifiers, stuffed animals and other objects youngchildren put in their mouths.
· Damping dust and damping mop the house at least

JBUMDC 2016; 6(2): 69-75 Page-73
Lead and its Health Hazards
once a week as both are very effective at pickingup dust.
· Keeping sidewalks and porch free of dust and debrisby using a HEPA vacuum if possible or simply bya broom15
(4) Healthy eating:· Washing hands before every meal and snack· Keeping children away from eating and chewing
on non-food items such as paint chips, windowsills, and dirt
· Avoiding use of imported glazed pottery for food.· Eating foods high in calcium, vitamin C and iron.
All these discourage absorption of lead.· Avoiding eating of lead containing candies· Avoiding eating of contaminated sea foods as fish,
shrimps etc. being polluted by industrialized waste(5) Lead testing: In blood samples usually but if required
other samples as hairs, nails and urine may also beused to diagnose the features of toxicity.16
CONCLUSION:Lead is a naturally occurring heavy metal. A wide rangeof adverse effects could be induced in human beingsdepending upon the dose and time period of leadexposure. Central nervous system of children is mostsensitive to the effects of lead while peripheralneuropathy, chronic nephropathy, and hypertension aresome of the main concerns in adults. Awareness regardingit`s exposure, health hazards and preventive measuresshould be disseminated through print and electronicmedia.Government alone and or with NGOs should takemeasures to provide safe water supply for drinking,improve the hygienic practices in the living environme-ntal conditions, ensure safety and control marinepollution, present industrial waste should be treatedbefore drainage into sea, provide contaminant free fishery,utilize mass, print and electronic media to educatepeople regarding healthy living, report to health officialsin case of acute and chronic lead toxicity, monitor healthparameters by employing health visitors etc.
REFERENCES:1. Liu J, Goyer RA, Waalkes MP. Toxic effects of Metals.
In: Klaassen CD, Editor. Casarett and Doull’s Toxicology-The Basic Science of Poisons.7th ed. New York: McGrawHill Companies.2008 p. 932-4
2. Wilson L. Toxic metals & Human health. 2013. Availableat: http://www.healingaia.com/blog-resources/whats-new/toxic-metals-and-human-health/ Accessed on 29th
December 20143. CDC (Center for Disease Control and Prevention) Blood
lead levels-United States, 1999–2002. MMWR MorbMortal Wkly Rep. 2005;54:513-6
4. CDC (Center for Disease Control and Prevention) SecondNational Report on Human Exposure to EnvironmentalChemicals. Atlanta: U.S. Department of Health andHuman, Services, 2003. NCEH Pub. No. 02-0716. Available at http://www.cdc.gov/exposurereport/2nd/pdf/secondner .pdf
5. Sanders T, Liu Y, Buchner V, Tchounwou PB. Neurotoxic
Effects and Biomarkers of Lead Exposure. Rev EnvironHealth. 2009;24(1):15-45
6. ATSDR: Toxicological Profile for Lead (update). (2005c)Agency for Toxic Substances and Disease Registry,Atlanta, Georgia, pp. 1-577
7. Roy A, Georgopoulos PG, Ouyang M, Freeman N, LioyPJ. Environmental, dietary, demographic, and activityvariables associated with biomarkers of exposure forbenzene and lead. J Expo Anal Environ Epidemiol 2003;13(6):417-26. [PubMed: 14603342]
8. Bergdahl IA, Skerfving S. Biomonitoring of lead expos-ure-alternatives to blood. J Toxicol Environ. Health2008;71(18):1235-43. [PubMed: 18654894]
9. De Francisco N, Ruiz Troya JD, Aguera EI. Lead andlead toxicity in domestic and free living birds. AvianPathol 2003; 32:3-13
10. Manton WI, Angle CR, Stanek KL. Acquisition andretention of lead by Young children. Environ Res2000;82:60-80
11. Von Lindren IH, Spalinger SM, Bero BN. The influenceof soil remediation on lead in house dust. Sci Total Env-iron.2003;303:59-78
12. Gulson BL, Mizon KJ, Korsch MJ. Mobilization of leadfrom human bone tissue during pregnancy and lactation-A summary of long-term research Sci Total Environ.2003;303:79-104
13. Yoshida T, Yamauchi H, Fan Sun G. Chronic healtheffects in people exposed to arsenic via the drinking water:dose-response relationships in review. Toxicol ApplPharmacol 2004; 198: 243-52
14. Kapaj S, Peterson H, Liber K, Bhattacharya P. Humanhealth effects from chronic arsenic poisoning-a review.J Environ Sci Health Tox Hazard Subst Environ Eng2006;41(10):2399-428
15. Health effects of lead exposure. Lead and its human eff-ects. Public Health - Seattle & King County King CountyDirt Alert at 206-263-1399 and visit www.dirtalert.info.www.kingcounty.gov. Accessed on 27-04-2016
16. Australian Government, National Health and MedicalResearch Council (NHMRC), Health Topics, Lead BloodLevels NHMRC at [email protected] Updated:Accessed on 27-04-2016
17. Schnaas L, Rothenberg SJ, Flores M-F. Reduced intele-ctual development in children with prenatal lead exposure.Environ Health Perspect 2004; 114:791-7
18. Willis MS, Monaghan SA, Miller ML, McKenna RW,Perkins WD, Levinson BS et al. Zinc-induced copperdeficiency: a report of three cases initially recognizedon bone marrow examination. Am J Clin Pathol 2005;
123:125-3119. Hu H. Human health and heavy metals exposure. In Life
Support: The Environment and Human Health; MITPress: Cumberland, RI, 2002; 4:65-82
20. Lustberg M, Silbergeld E. Blood lead levels and mortality.Arch. Intern. Med.2002; 162: 2443-9
21. Nawrot TS, Thijs L, DenHond EM. An epidemiologicalre-appraisal of the association between blood pressureand blood lead: A meta analysis. J Hum Hypertens 2002;16:123-31
22. Alfven T, Jarup L, Elinder CG. Cadmium and lead inblood in relation to low bone mineral density and tubularproteinuria. Environ Health Perspect 2002 ; 110:699-702
23. Lee MY, Jung BI, Chung SM. Arsenic-induced dysfun-ction in relaxation of blood vessels. Environ HealthPerspect 2003 ; 111:513-7
JBUMDC 2016; 6(2): 69-75 Page-74
Syed Sanowar Ali1, Nasim Karim2
24. Gonick HC, Behari JR. Is lead exposure the principalcause of essential hypertension? Med Hypotheses2000;59:239-46
25. Vaziri ND, Sica DA. Lead-induced hypertension: role ofoxidative stress. Curr Hypertens Rep 2004;6:314-20
26. Chen A, Dietrich KN, Ware JH, Radcliffe J, Rogan WJ.IQ and blood lead from 2 to 7 years of age: are the effe-cts in older children the residual of high blood lead con-centrations in 2-year-olds. Environ Health Perspect.2005;113(5):597-601
27. World Health Organization (WHO) Environmental Hea-lth Criteria Document 224.Arsenic and Arsenic compou-nds. International Programme on Chemical Safety (IPCS).2001
28. Zheng W. Toxicology of choroid plexus: Special referenceto metal-induced neurotoxicities. Microsc Res Tech2001;52:89-103
29. Popko J, Olszewski S, Hukalowicz K, Markiewicz R,Borawska MH, Szeparowicz P. Lead, Cadmium, Copperand Zinc concentrations in Blood and Hair of mothersof children with Locomotor system malformations. Poli-sh Journal of Environmental Studies 2003;12( 3):375-9
30. Singh R, Gautam N, Mishra A, Gupta R. Heavy metalsand living systems: An overview. Indian J Pharmacol.201 ; 43(3): 246-53. doi: 10.4103/0253-7613.81505
31. Sun G. Arsenic contamination and arsenicosis in China.Toxicology and Applied Pharmacology. 2004;198 (3):268-71
32. Dietert RR, Lee JE, Hussain I. Developmental immuno-toxicology of lead. Toxicol Appl Pharmacol 2004;198:86-94
33. Luebke RW, Chen DH, Dietert R. The comparative imm-unotoxicity of five selected compounds following devel-opmental or adult exposure. J Toxicol Environ HealthB Crit Rev 2006;9:1-26
34. Karmaus W, Brooks KR, Nebe T. Immune functionbiomarkers in children exposed to lead and órgano-chlorine compounds: A cross-sectional study. EnvironHealth 2005; 4:1-10
35. Carmouche JJ, Puzas JE, Zhang X. Lead exposure inhi-bits fracture healing and is associated with increasedchondrogenesis, delay in cartilage mineralization, anda decrease in osteoprogenitor frequency. Environ HealthPerspect . 2005;113:749-55
36. Campbell JR, Rosier RN, Novotny L. The associationbetween environmental lead exposure and bone densityin children. Environ Health Perspect 2004;112:1200-3
37. Silbergeld EK. Facilitative mechanisms of lead as acarcinogen. Mutat Res 2003;533:121-33
38. Silbergeld EK, Waalkes M, Rice JM. Lead as a carcino-gen: Experimental evidence and mechanisms of action.Am J Ind Med 2000;38:316-23
39. Qu W, Diwan BA, Liu J. The metallothionein-null phen-otype is associated with heightened sensitivity to leadtoxicity and an inability to form inclusión bodies. Am.J Patho 2002; l 160:1047-56
40. Wei M, Wanibuchi H, Morimura K. Carcinogenicity ofdimethyl arsenic acid in male F344 rats and geneticalterations in induced urinary bladder tumors. Carcin-ogenesis 2002;23:1387-97
41. Faller P, Hureau C, Berthoumieu O. Role of metal ionsin the self-assembly of the Alzheimer’s amyloid-betapeptide.Inorg. Chem. 2013; 52, 12193-206
42. IARC (2004) IARC Monographs on the evaluation ofcarcinogenic risks to humans. Arsenic in Drinking Water:
Some Drinking Water Disinfectants and Contaminants,including Arsenic. 2004; 84:269-477 Lyon, France:IARC
43. Jackson KM. Electro-thermal atomic absorption spectr-ometry and related techniques. Analytical Chemistry.2000;72 (12) :159R-67R
44. Levin AD, Pribytkov VA, Rukin EM., Seregina IF. Ato-mic-absorption spectrometry in elemental analysis ofbiological materials, Measurement techniques.2001;44(6) : 660-2
45. Bader N R. Sample Preparation for Flame Atomic Abso-rption Spectroscopy: An Overview Rasayan J. Chem.2011; 4(1) :49-55
46. Sneddon, J, Hardaway C, Bobbadi K.K, Reddy, A.K.Sample Preparation of Solid Samples for Metal Deter-mination by Atomic Spectroscopy-An Overview andSelected Recent Applications. Applied SpectroscopyReviews 2006; 41(1): 1-14
47. Perez Cid B, Silva C, Boia C. Determination of Lead inbiological samples by use of slurry sampling electrother-mal atomic absorption spectrometry. Analytical andBiological Chemistry. 2002; 374 (3) :477-83
48. Szymczycha-Madeja, A, Mulak, W. Comparison of var-ious digestión procedures in chemical analysis of spen-thydrodesulfurization catalyst. Journal of HazardousMaterials, 2009);164(.2-3): 776-80
49. Pengping S, Kungwankunakorn S. Determination ofSome Heavy Metals in Human Hair by Ultrasonic AcidDigestion and Atomic Absorption Spectrophotometry,Chiang Mai J. Sci. 2014; 41(1) :148-25
50. Barbosa Jr, F, Santos JET, Gerlach RF, Parsons PJ. Acritical review of biomarkers used for monitoring humanexposure to lead: advantages, limitations, and futureneeds. Environ Health Perspect. 2005; 113(12): 1669-74
51. Patrick L. Lead toxicity a review of the literature. Part1: Exposure, evaluation, and treatment. Altern Med Rev2006; 11:2-22
52. Qaisara P, Salman AM, Nazia S, Munir HS. Investigationof trace metals in the blood plasma and scalp hair ofgastrointestinal cáncer patients in comparison withcontrols, Clin. Chim.Acta 2010; 411: 531-9
53. Afridi H.I , Kazi TG, Kazi NG, Jamali MK, Arain MB,Baig S et al. Evaluation of cadmium, lead, nickel andzinc status in biological samples of smokers and nonsm-okers hypertensive patients. J. Hum. Hypertens 2010;24: 34-43
54. Tasneem GK, Hassan IA, Gul H.K, Mohammad KJ,Mohammad BA, Nusrat J. Evaluation of essential andtoxic metals by ultrasound-assisted acid leaching fromscalp hair samples of children with macular degenerationpatients, Clin. Chim. Acta 2006; 369:52-60
55. Jamshid LM, Ahad BT. Cloud point pre-concentrationand flame atomic absorption spectrometric determinationof Cd and Pb in human hair, Anal. Chim. Acta 2002;470: 215-21
56. Mehra R, Junejo M. Adverse health effects in workerexposed to trace / toxic metals at workplace. 2003;40:131-5
57. Mehra R, Junejo M. Biological monitoring of Lead andCadmium in human hair and nails and their correlationswith biopsy materials, age and exposure. Indian Journalof Biochemistry & Biophysics 2004; 41: 53-6
58. Ullah M R, Haque M E. Spectrophotometric determina-tion of toxic elements (Cadmium) in aqueous media,Journal of Chemical Engineering, IEB 2010;25( 1): 44-52

JBUMDC 2016; 6(2): 69-75 Page-75
Lead and its Health Hazards
59. Tsay T S, Huang Y L, Tseng W C. Toxicological Profilefor Copper (Update). Agency for Toxic Substances andDisease Registry (ATSDR). Atlanta, GA. September,2004http://www.merckmanuals.com/vet/toxicology/copper
poisoning / overview _of_copper_poisoning.html60. Horngm C J, Tsai J L, HuaHorng P, Lin S C, RenLin S,
Tzeng C C. Determination of urinary lead, cadmiumand nickel in steel production workers.Talanta 2002;56:1109 -15

INTRODUCTION:Disabled individuals comprise a considerable section ofthe community, and it is estimated that worldwide thereare about 500 million people having disabilities.1
Prevalence may vary from country to country,howevervariation in prevalence may be recognized on ascertain-ment basis and by standardization methods employedfrom study to study. According to World Health Organi-zation estimates, individuals with disabilities comprise10% of the population in developed countries and 12%in developing countries.2
Children with disabilities, having serious psychological,physical and intellectual problems, should obtain specialpreventive care in dental clinics.3Consequently, inadeq-uate dental care or poor dental public health measure-ments may have harmful influence on the oral healthstatus and because of inadequate or sometimes completedysfunction of their stomatognathic apparatus, oftendue to anatomical malformations of the orofacial cavityand children’s uncooperative behavior, accomplishmentof good oral hygiene measures usually require theassistance of parents or caretakers.4 The most importantrisk factor for dental caries in disabled children is poororal hygiene and inadequate tooth brushing practices.5,6
Preventive measurements should thereby includesufficient education and inspiration both for patientsand their caretakers, finally aiming at obtaining andmaintaining satisfactory oral hygiene throughoutlifetime.7
According to the Rehabilitation Council of Indian Act,it defines mental retardation as acondition of arrestedor incomplete development of the mind of an individual,which is specially characterized by sub-normality ofintelligence. Inspite of the high level of dental disease,individuals with disabilities or illnesses receive less oralcare than normal people.8 Characteristically, it has beenreported that dental treatment is the greatest unattendedhealth need of the disabled.9 Some of the most importantreasons may be inadequate recall systems, practicaldifficulties during sessions of the treatment, socioecon-omic status and underestimation of treatment needs or
ORIGINAL ARTICLE
JBUMDC 2016; 6(2): 76-80 Page-76
ABSTRACTObjective: To assess caries and oral health status of disabled individuals of special school in Gadap Town of Karachi, Pakistan.Materials and Methods: This descriptive cross sectional study was carried out in 94 participants. The study was conductedon special persons, aged between 4-33 years, who were examined for caries and oral health status and were then included inthe study upon fulfilling the inclusion criteria. A self-structured questionnaire related to the DMFT and plaque index wasdeveloped and data of each disabled individual was collected by trained house officers. Data was analyzed using SPSS software20 version.Results: In this study males were 72.6 % and females were 26.3%.Study participants with mental retardation were 41.1%, beinghighest in frequency, followed by cerebral palsy 9.5%,autistic disorder 3.2% and Down`s syndrome 3.2% respectively. Studyresults clearly indicated that oral hygiene was inadequate in all conditions of special persons who were studied. The group withlack of motor skills did not have significantly better oral hygiene than the group who had good motor skills. Overall both groupshad poor oral hygiene.Conclusion: Oral health status in disabled individuals is found to be poor.Adequate follow-up of daily oral hygiene, even inself-sufficient special persons is needed. There is a strong need for enhanced education on mechanical as well as chemicalplaque control to the parents/ guardians/ care givers of the disabled individuals.Keywords: Down syndrome, Mental retardation, Cerebral palsy, Autistic disorder, Oral hygiene
Caries Experience and Oral Health Status amongDisabled Individuals of Special School of Gadap Town
KarachiAsghar Ali1, Muhammad Ali Leghari2, Samreen Mazhar3, Mahwish Bano4
Dr. Asghar AliAssociate Professor & HODDepartment of Community DentistryBaqai Dental CollegeBaqai Medical UniversityKarachiPakistanEmail: [email protected]
Dr. Muhammad Ali LeghariAssistant ProfessorDepartment of Community DentistryBaqai Dental CollegeBaqai Medical UniversityKarachiPakistan
Dr. Samreen MazharAssistant ProfessorDepartment of Community DentistryBaqai Dental CollegeBaqai Medical UniversityKarachiPakistan
Dr. Mahwish BanoDemonstratorDepartment of Community DentistryBaqai Dental College,Baqai Medical UniversityKarachiPakistanReceived: 08-10-15Revised: 23-10-15Accepted: 03-11-15

pain, communication problems and poor cooperation.10,11
Oral health of the disabled may be ignored because ofa disability condition, and limited access to oral healthcare which is the purpose of our study. Additionally,because of their level of function and their limited abilityto undergo an oral examination, the maintenance of oralhygiene in disabled individuals is a difficult task, whentheir oral health is assessed.12 However, with appropriateplanning, clear communication and carefully drawnrestrictions to the service provided, the dramatic resultsof dental health can be successfully alleviated.13
A number of studies have shown that challenges to oralhealth are more complex for disabled children, whoareregularly unable to adequately apply the techniquesnecessary to control mechanical and chemical plaque.In several instances, a disabled child’s oral healthcarebecomes the responsibility of another human being,generally a parent or guardian, many of whom areemotionally or intellectually incapable of dealing withthe health problems of their less fortunate affiliates.Some of the most important reasons as mentioned earliermay be unsatisfactory recall systems, practical difficultiesduring treatment sessions, socioeconomic status andunderestimation of treatment needs or pain, communi-cation problems and bad cooperation of disabled children,which often requires sedation or general anesthesia indifferent hospital setup.With this background, our presentstudy was designed to assess caries and oral health statusin disabled individuals of a special school in GadapTown of Karachi, Pakistan.
MATERIALS &METHODS:The target population included all the special personsattending the special needs in the school of GadapTown,Karachi. The 94 special children and adults between theages of 4 to 33 years were examined. The subjects wereclassified according to their medical diagnosis. Thediseases present were Down’s syndrome,intellectualproblems, deafness and dumbness,blindness, learningproblems, cerebral palsy, autistic disorder, behavioraldisorder and mental retardation. Before the dentalexamination, demographic information was registeredfor each subject: age, gender along with informationregarding education and father’s occupation. Clinicalexamination was done by a single examiner forassessment of oral hygiene status with dental mouthmirror. Dental fluorosis, plaque index and any otherextra as well as intra-oral lesions were observed.Ethicalapproval for conducting the study was availed from thedental school. Informed consent was taken from principalas well as from the parents before subjects were includedin the study.Statistical analysis: Data was entered and analyzedusing the statistical package for social sciences (SPSSversion 20) was used to describe the patterns of oralhygiene status and caries experience which werecalculated for all groups.
RESULTS:Table 1a illustrates the general profile of the study pop-
ulation. Out of 100 special persons 95 were examined.The remaining individuals were either absent fromschool for a long period or highly uncooperative andvery difficult to examine and there was one questionnairewhich was incompletely filled and considered as amissing value.There was difference in the distributionof subjects according to age group as well as there wasunequal gender distribution with males comprising of72.6 % and females 26.3% of the total sample.The studyparticipant age range was from 4 years to 33 years. Thestudents belonged to the classes from nursery tomanageable senior (manageable class was special classfor special children)as shown in Table 1b.The frequencyof fathers occupation was: Private Job55.8%, Govern-ment Employee16.8%, Businessman 17.9%, Retiredofficer 2.1%, not alive 4.2% and Jobless 2.1%. Table 2illustrates the distribution of children according to theircondition:mentally retarded were 41.1%, which is highestin frequency and the other conditions were cerebralpalsy 9.5%, autistic disorder 3.2%, Down’s syndrome3.2%, blind 18.9%, deaf & dumb 15.8%, learningproblems 1.1%, intellectual problems were 1.1% andothers were 5.3%.
JBUMDC 2016; 6(2): 76-80 Page-77
Asghar Ali1, Muhammad Ali Leghari2, Samreen Mazhar3, Mahwish Bano4
Table: 1aSocio-demographic profile
Age in years
45679101112131415161718192021222533TotalMissing SystemTotal
GenderMaleFemaleTotalMissing SystemTotal
Frequency
2255248899953863122194195
Frequency692594195
Percent
2.12.15.35.32.14.28.48.49.59.59.55.33.28.46.33.21.12.12.11.198.91.1
100.0
Percent72.626.398.91.1
100.0

We examined the permanent and deciduous decayedmissing and filled teeth in disabled children. In permanentdentition the decayed teeth were 87, missing teeth were7 and filled teeth were 3.While in deciduous dentition60 teeth were decayed, 1 tooth was missing and no filledteeth was found.However the frequencies of permanentdecayed first molar were as high as 10.5% and centralincisor as low as 1.1%, the permanent central incisormissing teeth frequency was 4.2% whereas the missingcanine frequency were 1.1% and the frequencies ofpermanent filled teeth was 1.1%. The highest frequenciesof decayed first molar deciduous teeth were 6.3% andlower frequency of decayed deciduous teeth was 1.1%,the frequency of missing deciduous canine was 2.1%and there were no filled teeth present in the deciduousdentition (Table 3). The plaque index score were visibleplaque 50.5% and abundant amount of visible plaque20.0%. Dental fluorosis was 8.4% (Table 4).
JBUMDC 2016; 6(2): 76-80 Page-78
Caries Experience and Oral Health Status among Disabled Individuals of Special School of Gadap Town Karachi
Table: 1bEducational level
School Class
NurseryKG IKG IIClass 1Class 2Class 3Class 4Class 5Class 6Class 7Class 8Class 9Class 10Minimal GroupTrainable juniorTrainable seniorManageable groupTotalMissingsystemTotal
Frequency
12104719227342512211194195
Percent
12.610.54.27.420.02.12.17.43.24.22.15.31.12.12.111.61.198.91.1
100.0
Table: 2Conditions of special children
Conditions of Child
Mental RetardationCerebral PalsyAutistic DisorderDown’s SyndromeBlindDeaf & DumbLearning ProblemsIntellectual ProblemsOthersTotalMissing SystemTotal
Frequency
39933181511594195
Percent
41.19.53.23.218.915.81.11.15.398.91.1
100.0
Table: 3aTotal DMFT score and frequencies
Permanent Dentition
Decayed87
Missing7
Filled3
Average Dmft Score 09
Deciduous DentitionDecayed
60Missing
1Filled
0
Table: 3b
Permanent Decayed01234561115TotalMissing SystemTotal
Permanent Missing013TotalMissing SystemTotal
Permanent Decayed012TotalSystem
Deciduous decay01234712TotalSystemTotal
Deciduous Missing01TotalMissing SystemTotal
Deciduous filled0SystemTotal
Frequency6710614221194195
Frequency894194195
Frequency9211941
Frequency7564161194195
Frequency92294195
Frequency94195
Percent70.510.56.31.14.22.12.11.11.198.91.1
100.0
Percent93.74.21.198.91.1
100.0
Percent96.81.11.198.91.1
Percent78.96.34.21.16.31.11.198.91.1
100.0
Percent96.82.198.91.1
100.0
Percent98.91.1
100.0

DISCUSSION:Oral health disparities are found among people withmental and physical disabilities and there is limitedliterature available on the oral health status of the disabledpopulation. Little research has been conducted to assessthe impact of various socio-demographic and clinicalvariables on the oral hygiene status, periodontal statusand dental fluorosis in disabled population.14
The oral hygiene status in the study participants wasnot satisfactory. The study participants were specialchildren who had the highest percentage of childrenwith poor oral hygiene. The removal of plaque anddebris from teeth is a skill that can be mastered onlywhen an individual has the dexterity to manipulate thetoothbrush and understand the objectives of theseactions.15 The success of good oral hygiene reflects theskill and motivation of an individual. 16Several studiesof disabled children have reported that such patientstend to have poor oral hygiene than their non-disabledcounterparts. Most of these findings highlight thedifficulties encountered by disabled individuals inmaintaining an adequate level of oral hygiene. Thereasons for poor oral hygiene in disabled children havebeen attributed to low powers of concentration and lackof motor skills.17The lack of manual coordination indisabled children was afactor in the difficulty of theiroral hygiene maintenance and other studies mentionedthat the most obvious challenge is the physical inabilityto adequately clean the oral cavity 18,19,20, as same resultsseen in this study.In general, there is a wide range oftooth brushing ability, which is related to coordinatedmuscular movements, innate skills, ability to understandinstructions and age of the individual.21 According todifferent investigators, powered brushes are predomi-nantly well suited for people with reduced motor skills.On the other hand, various different types of speciallydesigned manual tooth brushes have been developed tosolve this problem.Income status of parents was also significantly associatedwith oral hygiene and periodontal status as confirmedby a previous study which observed that oral hygienestatus deteriorated as the income decreased.22Different
studies of oral disease prevalence in disabled groupsfound significantly poor levels of dental hygiene, 23,24
which is confirmed in this study. It is hoped that theresults of this study would help in planning dentalpreventive and restorative services in these children.Furthermore, caries in first permanent molars, as wellas bad habits and poor oral hygiene due to plaque andcalculus deposition, were more common in childrenwith disabilities than in healthy children. Several systemicconditions increase the risk of bad oral hygiene, whichin turn is a risk factor for a number of systemic conditions.Some authors have confirmed that effective oral healthprograms commencing well before the usual first contactwith dental services at the age of 5 are needed for youngchildren who are at high risk of dental caries. Our presentstudy has observed that poor oral health is a major healthproblem for disabled persons and their oral health seemedto indicate a cumulative ignorance, which may be a partof overall parental neglect of these special persons inrelation to other basic health measures and may reflectthe manner that oral health lacks importance in theoverall scheme of health management. The oral hygieneand periodontal status of the present population waspoor and was influenced by medical diagnosis, IQ level,disabled sibling, parent’slevel of education and socioec-onomic status. The promotion of oral health should beaimed specifically at special needs schools and parentsof disabled children. The oral health promotion shouldinclude facilitating access and regular use of oral healthservices. Taking into consideration the multi-factorialinfluence on oral hygiene and periodontal status of thepresent disabled population, oral health promotion andintervention programs should be planned and concentr-ated towards these risk groups.25
According to their previous studies, different authorshave concluded that the main barriers to equal accessto dental treatment for individuals with disabilities seemsto be inadequate facilities and insufficient time, lack ofsufficient knowledge and general stress related to treatingthis group; these are the same barriers as for non-disabledindividuals that is fear and negative attitudes towardsdentistry.22,23,24,25
JBUMDC 2016; 6(2): 76-80 Page-79
Asghar Ali1, Muhammad Ali Leghari2, Samreen Mazhar3, Mahwish Bano4
Table: 4Plaque index and dental fluorosis
Dental FluorosisYesNoTotalMissing SystemTotal
Frequency88694195
Percent8.490.598.91.1
100.0
Plaque IndexNo visible plaqueVisible plaqueAbundant amount of visible plaqueTotalMissing System
Total
Frequency27481994195
Percent28.450.520.098.91.1
100.0

In our opinion, oral health care should be approachedtogether with general health care in order to achieve amore holistic view of the individual’s physiological andpsychological well-being.To improve the oral hygienestatus of individuals with disabilities is an over whelmingtask, but it can be achieved if the parents or guardiansare given appropriate health education.
CONCLUSION:Oral hygiene is found to be inadequate in all conditionsof special persons who were studied.The groups withlack of motor skills did not have significantly better oralhygiene and even groups having good motor skills hada poor oral hygiene. Adequate follow-up of daily oralhygiene, even in self-sufficient special persons is neededand there is a strong need for enhanced education onmechanical as well as chemical plaque control.There isa strong need for in-service training programs on oralhygiene. Finally, the clinical assessment by care giversalso remains complicated. In this respect, regularrepetition of programs should be necessary. This shouldbe the primary and continuous goal of any task forcefor improving the oral health care of handicappedindividuals and for any dentist providing oral healthcareto disabled people. A higher awareness on the part ofcare givers would contribute to the quality of life of thistarget population.
Acknowledgement:It is my pleasure to entitle my achievement to the effortsof those who guided, helped and encouraged me a lotduring the conduct of study.Special thanks to all theteam members of my department.
REFERENCES:1. Watson N. Barriers. Discrimination and prejudice. In:
Nunn J, editor. Disability and Oral Care. London: WorldDental Press Ltd 2000. p.15-28
2. Baykan Z. Causes and prevention of disabilities, handi-caps, and defects. J Cont Med Educ. 2003;9:336-8
3. Mcdonald RE, Avery D.Odontoiatria per bambino el’ad-olescente. Piccin, Padova, 1988
4. Storhaug K. The mentally retarded and the dental healthservices. Treatment needs and preventive strategies. NorTannlaegeforen Tid 1991; 101(8):262-5
5. Bortolotti L, Cetrullo L, Frezza R. Iltrattamentoambulato-rialedeglihandicapati. Il dentistamoderno 1986; 10: 6570
6. Palin-Palokas T, Hausen H, Heinonen I. Relative import-ance of caries risk factors in Finnish mentally retardedchildren. Community Dent Oral Epidemiol 1987;15(1):19-23
7. Hennequin M, Faulks O, Roux O. Accuracy of estimationof dental treatment needs in special care patients. J Dent
2000;28:131-68. Boj JR, Davila JM. Differences between normal and
developmentally disabled children in a first dental visit.J Dent Child 1995;62:52-6
9. Brandes DA, Wilson S, Preisch JW, Casamassimo PS.A comparison of opinions from parents of disabled andnondisabled children on behavioral management techn-iques used in dentistry. Spec Care Dent 1995;15:119-23
10. Dicks JL. Outpatient dental services for individualswith mental illness: A program description. Spec CareDent 1995;15:239-42
11. Glassman R, Miller CE, Lechowick A. A dental school’srole in developing a rural, community based, dental caredelivery system for individuals with developmentaldisabilities. Spec Car Dent 1996;16:188-93
12. Tesini DA. An annotated review of the literature of den-tal caries and periodontal disease in mentally retardedindividuals. Spec Care Dent 1981;1:75-87
13. Haavio ML. Oral health care of the mentally retardedand other persons with disabilities in the Nordic countries:Present situation. Spec Care Dent 1995;15:65-9
14. Newacheck PW, Mc Manus M, Fox HB, Hung YY, Hal-fon N. Access to health care for children with specialhealth care needs.Pediatric 2000;105:760-6
15. Pinkham JR. Oral hygiene in children: relationship toage and brushing time. J Prev Dent 1975;2:28-31
16. Francis JR, Hunter B, Addy M. A comparison of threedelivery methods of chlorhexidine in handicappedchildren, effects on plaque, gingivitis, and tooth staining.J Periodontol 1987;58:451-5
17. Full CA, Kerber PE, Boender P, Schneberger N. Oralhealth maintenance of the institutionalized handicappedchild. J Am Dent Assoc 1977;94:111-3
18. Holcomb FH, Taylor PP, Saunders WA. Comparison oftwo oral hygiene devices for the physically handicapped.J Dent Child 1970;37:325-9
19. Unkel JH, Fenton SJ, Hobbs G Jr, Frere CL. Toothbrushing ability is related to age in children. J DentChild 1995;62:346-8
20. Johnson R, Albertson D. Plaque control for handicappedchildren. J Am Dent Assoc 1972;84:824-8
21. Sogi GM, Bhaskar DJ. Dental caries and Oral HygieneStatus of school children in Davangere related to theirSocio-Economic levels: An Epidemiological study.J Indian Soc Pedo Prev Dent 2002;20:152-7
22. Murray JJ, McLeod JP. The dental condition of severelysubnormal children in three London boroughs. Br DentJ 1973;134:380-5
23. Brown JP, Schodel DR. A review of controlled surveysof dental disease in handicapped persons. ASDC J DentChild 1976;43:313-20
24. Morton ME. Dental disease in a group of adult mentallyhandicapped patients. Public Health 1977;91:23-32
25. Miller JB, Taylor PP. A survey of the oral health of agroup of orthopedically handicapped children. J DentChild 1970;37:331-2
JBUMDC 2016; 6(2): 76-80 Page-80
Caries Experience and Oral Health Status among Disabled Individuals of Special School of Gadap Town Karachi

ORIGINAL ARTICLE
JBUMDC 2016; 6(2): 81-83 Page-81
ABSTRACT:Objective: To assess the frequency of midline swellings in the neck.Materials and Methods: A prospective survey was conducted on 150 patients (males and females) who came in for a dentalcheck-up at Altamash Institute of Dental Medicine from 1st June to 1stSeptember 2015. Permission was obtained from ethicalcommittee and verbal informed consent was taken from patients/their attendants. Selection of the subjects for the study wasdone after evaluation of the case history of each subject and clinical examination. Patients with 20 to 70 years of age wereincluded in the study. Their name, age, gender, general and local description of the midline swelling which included site, sizeshape, color, tenderness, temperature and consistency were recorded in the performa. Data analysis was done by SPSS version13.0.Results: Multi-nodular goitre was the most common form of neck swelling found in 34 patients. Women of middle aged group(31-49) followed by women of younger age group (20-30) were affected more. In all age groups only T3 was increased whilethe level of TSH and T4 was normal indicating swellings to be of thyroid in origin.2 patients had enlarged cervical lymph nodes.Conclusion: The frequency of multinodular goiter was found to be 94.4% and females of middle age group were the mostaffected ones.Keywords: Neck swellings, Midline, Thyroid, Goiter, Multinodular
INTRODUCTION:There are numerous regions within the neck where aswelling can occur. The presence of lymph nodes(a)submental(b)submandibular (c)pre-auricular (d)post-auricular (e)cervical chain and the subsequent swellingof these lymph nodes (lymphadenopathy) mainly dueto infective causes (bacterial,viral,fungal) and noninfective causes (malignancy and drug related) is acommon cause of neck swelling. When making aprovisional diagnosis for neck swellings several pointsare to be considered such as site (lateral or midline),size,shape, color,temperature,tenderness and consistencyetc. About 50% of the neck swellings are thyroid swell-ings or goiter.1 These thyroid swellings could be causedby adverse drug reactions, has hashimotos thyroiditis,pituitary disease, grave`s disease, thyroid cancer andbenign thyroid neoplasms.Other swellings are of
congenital, developmental, infective, salivary glanddiseases, neurogenic and parapharyngeal space tumours.They are classified into midline neck swellings andlateral neck swellings. The midline neck swellingsinclude thyroglossal duct cyst/ thyroglossal duct sinus,sublingual dermoid cyst/ dermoid cyst, plunging ranula,thyroid swelling at isthmus, subhyoid bursa, prelaryngeallymph nodes etc. Whereas the lateral neck swellingsinclude lymph node enlargement due to non-specificcauses, bacterial or viral infections , neoplastic, metastatic,lymphangiomas / cystic hygroma, branchial cyst/branchial sinus, salivary gland swelling- parotid swelling,submandibular gland swelling, lipoma, sebaceous cystlaryngocele / pharyngeal pouches, Carotid body tumour/schwannoma.2,3
It has been documented that incidence of thyroid lesionsis highest in 104 cases (52%) than other lesions in headand neck regions.4 Overall, incidence of thyroid lesionsis said to be proportionately more in females (84.61%).5Hyperthyroidism and hypothyroidism may be treatedwith drugs and or surgery. The type of treatment beingdetermined by the form of thyroid disease, the age ofthe patient, the size of the goiter and the presence ofcoexisting conditions.6,7 Most patients with a Thyroglossalduct cyst present with asymptomatic masses in themidline of the neck. The literature reports that most ofthese lesions occur in patients younger than 30 years ofage.7,8,9
The purpose of this study was to collect data in a sampleof a Pakistani population so as to evaluate the frequencyof midline neck swellings in patients coming in for ageneral check-up at a private dental hospital and alsoto evaluate the site, size, shape, temperature, tenderness,consistency and color of the swelling. The review ofclinical characteristics of neck swellings and theirtreatment will help in decision making in daily medicaland surgical practice.
MATERIALS AND METHODS:In this prospective study patients were selected fromthe dental outpatient department at Altamash Instituteof Dental Medicine. Selection of the subjects for the
Frequency of Neck Swellings in Patients Coming forDental Check-up
Yousuf Lakdawala1, Dawar Nadeem2, Zeerak Jarrar3, Syeda Maria Fakhar4
Dr. Yousuf LakdawalaAssociate ProfessorDepartment of SurgeryAltamash Institute of Dental MedicineKarachiE-mail: [email protected]
Dr. Dawar NadeemHouse OfficerAltamash Institute of Dental MedicineKarachi
Dr. Zeerak JarrarClinical Demonstrator Oral DiagnosisAltamash Institute of Dental MedicineKarachi
Dr. Syeda Maria FakharSenior Medical OfficerDepartment of SurgeryAltamash institute of Dental MedicineKarachiReceived: 14-11-15Revised: 02-12-15Accepted: 07-01-16

study was done after evaluation of the case history ofeach subject and clinical examination. All patients above20 years of age and below 70 years of age were included.Patient characteristics like name, age, gender in generaland local description of the midline swelling whichincluded site, size shape, color, tenderness, temperatureand consistency were recorded in a performa. The studywas approved by ethics committee of Altamash Instituteof Dental Medicine.We analyzed the incidence of midlineneck swellings and the existing factors associated withthe swelling.
RESULTS:Out of 150 patients, 36 patients came in with a mid-lineneck swelling. Most of them were women. Multi-nodulargoitre was mostly observed in middle age group that isin women with age range of 31-49 years as comparedto women with age range 20-30 years and 50-60 years(Table 1). However on the basis of percentage multinodular goitre was found to be more common in oldage group and less common in middle age group. Multi-nodular goitre was more common in our women (94.4%)as compared to simple goiter. In all age groups only T3
was increased while the level of TSH and T4 was normal.In age group 20-30 years there was no other comorbiditey.While in other age groups hypertension was present inall patients with 50-60 years , 5 years, while patients in31-49 years and 3 patients in >60 years. While 4 patientsin 31-49 years age group and 1 in > 60 years had type2 diabetes.On local examination, the characteristics ofswellings were evaluated (Table 2). 2 patients had enlar-ged cervical lymph nodes.
DISCUSSION:When examining a patient with a neck mass, thephysician’s first consideration is the patient`s age group.The incidence of congenital, inflammatory and neoplasticdisease are the three categories in any adult age group.10Areview of associated medical conditions and previoustreatments is useful in narrowing the differential diagnosisand formulating an appropriate treatment plan.11.Initialinvestigation includes taking the complete patient historyalong with the size of the mass, sex, socioeconomicstatus and lifestyle changes which includes smoking,tobacco use, alcohol consumption and dietary habits toaccurately diagnose the patient on a clinical level. Otherclinical investigations would be to look out for fever,sore throat, upper respiratory tract infections and changesin voice quality and hoarseness. History and physicalexamination can then further conclude whether the neckswelling is congenital, infective or neoplasmic.12,13 Inour patients there was no hoarseness and only 3 patientsrelated the onset of swelling with fever and respiratorytract infection.Emphasis on location, mobility and consistency of theneck mass can often place the mass within a generaletiologic grouping, such as vascular,salivary, nodal/inflammatory, congenital or neoplastic.14 A singledominant or solitary nodule is more likely to representcarcinoma than a single nodule with a multinodulargland.15,16,17 Lumps of less than three weeks' durationare most likely due to a self-limiting infection and donot require further investigation.18Confirmation can onlybe done through investigations which includebiochemical tests, Fine Needle Aspiration Cytology(FNAC), CT scan, endos-copy and biopsy for sampletesting.By combining the relevant clinical expertise withappropriate investigations, definitive diagnosis of thelump on an out-patient basis could be diagnosed in 96%of patients.19
Midline neck swellings consist of swelling related tothyroid, parathyroid, larynx etc and or neurofibromaand haemangioma.20 Thyroid nodules are most commonin women and individuals who receive head and neckirradiation at a young age .The prevalence of thyroidnodules in the general population varies depending onthe diagnostic modalities used with estimates rangingfrom 3-5% by palpation, 30-40% by ultrasound and 40-50% by autopsy. Approximately 4% of thyroid nodulesare cancerous.21Our patients were exposed to palpationand biochemical examination. Out of 36 patients 34patients had multi nodular goitre and in all age groupsonly T3 was increased while the level of TSH and T4
JBUMDC 2016; 6(2): 81-83 Page-82
Yousuf Lakdawala1, Dawar Nadeem2, Zeerak Jarrar3, Syeda Maria Fakhar4
Table 1Distribution according to age and gender
Age Group(Years)
20-3031-4950-60>60
No. ofpatientsaffected
81954
Percentage Involved (%)
25%52%16%1.2%
Gender
FemalesFemalesMalesMales
Table: 2Characteristics of Swelling
Characteristics
Size3 cm4 cmMore than 5cm
Skin color with red hueRounded shapeTendernessPresentAbsentTemperatureRaisedNot raised
ConsistencySoftHardMobilityPresentAbsentNodulesSingleMultiple
No. of patientsN=36
6822
3636
531
1521
342
288
234
Percentage(%)
16.6%22.22 %61%
100%100%
13.88%86.1%
41.66%58.33%
94.44%5.55%
77.77%22.22%
5.55%94.44%

was normal.22
It is common in developing countries where thepopulation is iodine-deficient. This iodine deficiencycan cause goitre with nodules.23 Risk factors areincreasing age and female gender.24, 25
CONCLUSION:The frequency of multinodular goiter was found to be94.4% and females of middle age group were the mostaffected ones.
REFERENCES:1. Scully C, Felix DH. Oral Medicine-Update for the dental
practitioner lumps and swellings. British Dental Journal2005; 199: 763-70
2. Gleeson M, Herbert A, Richards A. Management oflateral neck masses in adults.BMJ 2000;320:1521-4
3. www.ourhealth.com/conditions/neck-conditions/classifi-cation-and-investigations-of-neck-swelling
4. Naeimi M, Sharifi A, Erfanian Y, Velayati A, ShahlaI-zadian, Golparvar S. Differential diagnosis of cervicalmalignant lymphadenopathy among Iranian patients;Saudi Med J 2009; 4:377-81
5. Rathod GB, Parmar P. Fine needle aspiration cytologyof swellings of head and neck region. Indian J Med Sci2012; 66:49-54
6. Woeber KA. Update on the management of hyperthyro-idism and hypothyroidism. Arch Intern Med 2000;160:1067-71
7. Smith JC .Neck, Cysts, Medscape Aug 2009. Accessedon 3rd January 2016
8. Kanwar VS .Lymphadenopathy, Medscape, May 2012.Accessed on 3rd January 2016
9. Goffart Y, Hamoir M, Deron PH, Claes J, Remacle M.Management of neck masses in adults;B-ENT, 2005;(1)Suppl. 1,:133-42
10. Mcguirt WF. Differential Diagnosis of Neck Masses;
Pediatric Otolaryngology case studies 1980:1-1211. Schwetschenau E, Kelley DJ. The Adult Neck Mass;
American Family Physician 2002: 66:831-812. Underbrink M. Evaluation and Management of a patient
with Neck Mass; UTMB 2001: 1-913. Ruhl C. Evaluation of a Neck Mass.Med Health R I.
2004;87(10):307-1014. Weber AL, Montandon C, Robson CD. Neurogenic
Tumors of the Neck. Radiologic Clinics of NorthAmerica. 2000; Vol 38(5): 1077-90
15. Bomeli SR, LeBeau SO, Ferris RL. Evaluation of aThyroid Nodule.OtolaryngolClin North Am; 2010:229-38
16. Kim N, Lavertu P. Evaluation of a Thyroid Nodule;Otolaryngol. Clin North Am 2003:17-33
17. Miller MC. The Patient with a Thyroid Nodule; Otolary-ngolClin North Am 2010: 1003-15
18. http://patient.info/doctor/neck-lumps-and-bumps19. Smith OD, Ellis PD, BearcroftPW.Management of neck
lumps--a triage model. Ann R CollSurg Engl. 2000; 82(4):223-6
20. Bero C J, Simons R J. Case studies in Thyroid Diseases.Internal Medicine Board Room Manual 2002: 2-115
21. Snow G B. Consensus diagnosis suspicious lymph nodein the neck; NederlandsTijdschriftvoorGeneeskunde .1988; 132( 3):114-9
22. Afzal H, Aftab A, Ashfaq S.Association of Multi-NodularGoitre with Different Age Groups of Women PJMHS2014
23. www.nhs.uk/Conditions/Goitre/Pages/Treatment.aspx24. Lefebvre J L, Coche-Dequeant B, Van JT, Buisset E,
Adenis A. Cervical lymph nodes from an unknownprimary tumor in 190 patients. American Journal ofSurgery 1990;160( 4): 443-6
25. Rosenberg TL, Brown JJ, Jefferson GD. Evaluating theadult patient with a neck mass. Med Clin North Am.2010; 94(5):1017-29
JBUMDC 2016; 6(2): 81-83 Page-83
Frequency of Neck Swellings in Patients coming for Dental Check-up

ORIGINAL ARTICLE
JBUMDC 2016; 6(2): 84-87 Page-84
ABSTRACT:Objective:To assess the efficacy of local steroid injection in trigger finger.Materials and Methods:This prospective study was conducted at department of Orthopaedics,Civil Hospital, Dow Universityof Health Sciences, Karachi, from March 2012 to 2013. Males and females with complain of trigger finger were included inthis study during the specified period. All patients were injected depomedrol with plain xylocaine at the nodule site and functionaloutcome was assessed with respect to pain relief and finger movement.Results: Study included 43 patients with trigger finger.29 were males and 14 were females. Right hand fingers were involvedin 24 patients, remaining had left hand fingers involvement. 10 involved the index finger,7 middle finger, 4 ring finger,10 littlefinger and 12 thumb. 9 patients had associated rheumatoid arthritis and 15 were known cases of diabetes. Remaining patientswere primary with no known co-morbid. All patients had pain relief initially and regained movement of finger. 10 patientsrequired repeated injection after 3 months. Maximum pain relief and regaining of movement after steroid injection was 4 months.Conclusion:Local steroid injection provides excellent symptomatic pain relief and regained movements without any complicationin patients with trigger finger.Key words: Steroid, Local anesthesia, Trigger finger, Pain relief, Movements
INTRODUCTION:Trigger finger also known as flexor stenosing tenosy-novitis is one of the most common conditions seen inthe clinical practice of hand surgery.1The lifetime riskof developing trigger finger is between 2% and 3%.2
The condition has a reported incidence of 28 cases per100,000 population per year.3 Trigger fingers are morecommon with certain medical conditions such as goutand diabetes. Repeated and strong gripping may lead tothe condition. In most cases, the cause of the triggerfinger is not known.Trigger finger may start with afeeling of discomfort at the base of the finger or thumb,where the finger joins the palm. This area is oftensensitive to pressure. A lump might be also felt. Othersymptoms may include pain, popping, catching feeling,limited finger movement etc. Patients present with apainful triggering or clicking during active flexion of
an affected digit and the finger get locked in the flexion(Figure 1a & 1b). It needs some force to straighten thefinger. This is due to the loss of normal smooth glidingof the tendon beneath the pulley system, most commonlyat the level of the A1 pulley. This may be a result of anodule in the tendon or a diffuse swelling within thesheath as a result of a tenosynovitis.4 The A1 pulley isaffected more, owing to the high local forces and a steeppressure gradient; it is also the site of maximal tendonexcursion. Alternative sites of tendon triggering havebeen described, including the A2 and A3 pulleys andthe palmar aponeurosis.5 Little finger and thumb are themost common digits affected.6 Exact etiology of triggerfinger is unknown but it is commonly associated withdiabetes mellitus, rheumatoid arthritis, hypothyroidism,carpal tunnel syndrome and De Quervain’s disease.7,8
Trigger finger can be treated with analgesic and splintage,
Efficacy of Steroid Injection in the Treatment of TriggerFinger
Adeel Ahmed Siddiqui1, Farooq Mamji2, Badaruddin Sahito3, Syed Mohammad Tariq4,Dileep Kumar5, Syed Itaat Hussain Zaidi6
Dr. Adeel Ahmed SiddiquiAssistant ProfessorDepartment of Orthopaedic SurgeryCivil Hospital & Dow Medical CollegeDow University of Health SciencesKarachiEmail:[email protected]
Dr. Farooq MamjiAssociate ProfessorDepartment of Orthopaedic SurgeryCivil Hospital & Dow Medical CollegeDow University of Health SciencesKarachi
Dr. Badaruddin SahitoAssistant ProfessorDepartment of Orthopaedic SurgeryCivil Hospital & Dow Medical CollegeDow University of Health SciencesKarachi
Dr. Syed Mohammad TariqAssistant ProfessorDepartment of Orthopaedic SurgeryCivil Hospital & Dow Medical CollegeDow University of Health SciencesKarachi
Dr. Dileep KumarAssistant ProfessorDepartment of Orthopaedic SurgeryCivil Hospital& Dow Medical CollegeDow University of Health SciencesKarachi
Dr. Syed Itaaat Hussain ZaidiAssistant ProfessorDepartment of Orthopaedic SurgeryDow International Medical CollegeDow University of Health SciencesKarachiReceived: 03-01-2016Revised: 17-02-2016Accepted: 22-02-2016
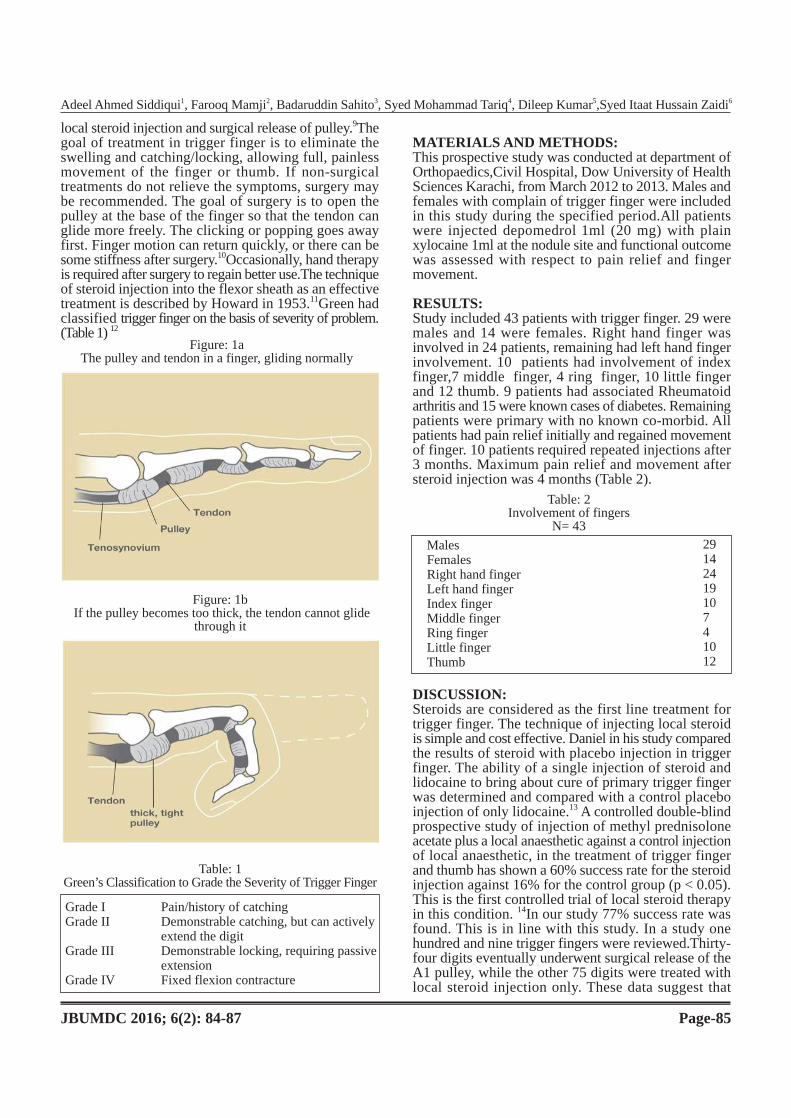
local steroid injection and surgical release of pulley.9Thegoal of treatment in trigger finger is to eliminate theswelling and catching/locking, allowing full, painlessmovement of the finger or thumb. If non-surgicaltreatments do not relieve the symptoms, surgery maybe recommended. The goal of surgery is to open thepulley at the base of the finger so that the tendon canglide more freely. The clicking or popping goes awayfirst. Finger motion can return quickly, or there can besome stiffness after surgery.10Occasionally, hand therapyis required after surgery to regain better use.The techniqueof steroid injection into the flexor sheath as an effectivetreatment is described by Howard in 1953.11Green hadclassified trigger finger on the basis of severity of problem.(Table 1) 12
MATERIALS AND METHODS:This prospective study was conducted at department ofOrthopaedics,Civil Hospital, Dow University of HealthSciences Karachi, from March 2012 to 2013. Males andfemales with complain of trigger finger were includedin this study during the specified period.All patientswere injected depomedrol 1ml (20 mg) with plainxylocaine 1ml at the nodule site and functional outcomewas assessed with respect to pain relief and fingermovement.
RESULTS:Study included 43 patients with trigger finger. 29 weremales and 14 were females. Right hand finger wasinvolved in 24 patients, remaining had left hand fingerinvolvement. 10 patients had involvement of indexfinger,7 middle finger, 4 ring finger, 10 little fingerand 12 thumb. 9 patients had associated Rheumatoidarthritis and 15 were known cases of diabetes. Remainingpatients were primary with no known co-morbid. Allpatients had pain relief initially and regained movementof finger. 10 patients required repeated injections after3 months. Maximum pain relief and movement aftersteroid injection was 4 months (Table 2).
DISCUSSION:Steroids are considered as the first line treatment fortrigger finger. The technique of injecting local steroidis simple and cost effective. Daniel in his study comparedthe results of steroid with placebo injection in triggerfinger. The ability of a single injection of steroid andlidocaine to bring about cure of primary trigger fingerwas determined and compared with a control placeboinjection of only lidocaine.13 A controlled double-blindprospective study of injection of methyl prednisoloneacetate plus a local anaesthetic against a control injectionof local anaesthetic, in the treatment of trigger fingerand thumb has shown a 60% success rate for the steroidinjection against 16% for the control group (p < 0.05).This is the first controlled trial of local steroid therapyin this condition. 14In our study 77% success rate wasfound. This is in line with this study. In a study onehundred and nine trigger fingers were reviewed.Thirty-four digits eventually underwent surgical release of theA1 pulley, while the other 75 digits were treated withlocal steroid injection only. These data suggest that
Figure: 1b If the pulley becomes too thick, the tendon cannot glide
through it
JBUMDC 2016; 6(2): 84-87 Page-85
Adeel Ahmed Siddiqui1, Farooq Mamji2, Badaruddin Sahito3, Syed Mohammad Tariq4, Dileep Kumar5,Syed Itaat Hussain Zaidi6
Figure: 1aThe pulley and tendon in a finger, gliding normally
Table: 1Green’s Classification to Grade the Severity of Trigger Finger
Grade I Pain/history of catchingGrade II Demonstrable catching, but can actively
extend the digitGrade III Demonstrable locking, requiring passive
extensionGrade IV Fixed flexion contracture
Table: 2Involvement of fingers
N= 43
MalesFemalesRight hand fingerLeft hand fingerIndex fingerMiddle fingerRing fingerLittle fingerThumb
2914241910741012

surgical management may be the next best option inpatients with trigger finger who continue to be sympto-matic after a single injection. Subjective data from thepatient questionnaire responses also supports surgeryas a reasonable choice after one injection failure.15
Patel in his comparative study of splintage and steroidinjection has showed successful results in 33 (66%) ofthe splinted digits and 42 (84%) of injected digits. Fiftypercent of the 10 splinted thumbs and 70% of the 40splinted fingers had a successful outcome. Of the 17unsuccessfully treated digits in the splinted group, 15were later cured with injections and 2 required surgery.All of the 7 unsuccessfully treated digits in the injectedgroup were cured with surgery. Splinting offers analternative for patients who have a strong objection tocortisone injection.16 Sean in his retrospective study of54 diabetic patients with 121 trigger digits treated overa 3-year period by one to three injections of corticosteroidmixed with local anesthetic found that 50% diabeticpatients responded to steroid injection. Insulin-dependentdiabetic patients have a higher incidence of multipledigit involvement (59% of patients) and of requiringsurgical release for relief of symptoms (56% of digits)when compared to non-insulin-dependent diabeticpatients (28% of patients with multiple digit involvement;28% of digits requiring surgery.17
A case has reported of delayed rupture of the flexordigitorum superficialis and profundus tendons after theuse of local corticosteroid injections for trigger finger.18
In our study we didn`t had this complication. In aprospective study published at Osaka, one hundred andtwenty-nine trigger fingers were investigated in 100adult patients.76 were women and 24 were men. Painand snapping were relieved in 98% and 74% of cases,respectively. Recurrence occurred in about half ofpatients, but the same clinical benefit was obtained afterre-injection. Surgery was performed for seven fingers.No complications of steroid injections were observed.19
We also have found no complications in our study.Onehundred and eight trigger fingers and thumbs weretreated by Micheal in 74 consecutive patients withsteroid. Minimum follow-up was 1 year. Eighty fourpercent of trigger fingers and 92% of trigger thumbswere cured with a single injection and a repeat injectionfor treatment of recurrent symptoms raised these figuresto 91% and 97%, respectively. There were no complicat-ions. He concluded that intra-synovial injection of asteroid compound is the appropriate initial treatmentfor trigger finger and thumb.20
2 groups were studied prospectively to evaluate steroidinjection placement and efficacy by John. In 1 group,intra-sheath injection and in the other subcutaneouslyinjection was given.The confirmed all-sheath injectiongroup exhibited a 47% good response, the mixed sheathand subcutaneous group had a 50% good response, andthe all-subcutaneous group had a 70% good response.The results of this study suggest that true intra-sheathinjection offers no apparent advantage over subcutaneousinjection in the treatment of trigger digits.21
Trigger finger is an underdiagnosed hand disorder
causing disability in longstanding diabetic patients. Sixtydiabetic patients,39 insulin-dependent diabetes mellitus(IDDM) and 21 non-insulin-dependent diabetes mellitus(NIDDM)] and 60 non-diabetic patients were examined.All were initially treated by steroid injections; failureto alleviate symptoms was the indication for surgery.Significantly, a higher recovery rate upon steroid injectionwas achieved in control patients as compared withdiabetic ones (p < 0.001). IDDM patients required moresurgery compared with NIDDMs and in 13.3% ofdiabetic patients, the surgical outcome was not successful.Steroid injection as the first mode of therapy is highlyrecommended although not always successful. 22In ourstudy 15 patients were diabetic and all of them hadsuccessful results after steroid injection.Forty-three patients were reviewed between 17 and 113months (mean of 47 months) following surgery foracquired stenosing tenosynovitis of the fingers or thumbs.32 (60.4%) of the 53 operations were completely success-ful. Of the remaining 21 operations, 26% either failedto relieve all symptoms, or symptoms had recurred atreview.15 operations led to complications that botheredthe patient to some extent. The three major complicationsall followed operations performed by junior surgeons.The importance of an adequate trial of conservativetherapy to avoid unnecessary surgery is emphasized.23
Studies have documented that steroid injection therapyshould be the first-line treatment of trigger fingers innon-diabetic patients. In diabetics, the success rate ofsteroid injection is significantly lower. Injection therapyfor type 1 diabetics was ineffective in this study. Surgicalrelease of the first annular (A1) pulley is most effectiveoverall in diabetics and non-diabetics alike, with nohigher rates of surgical complications in diabetics.24,25
In our study all diabetics were treated successfully bythe steroid injection.
CONCLUSION:Steroid injection along with a local anesthetic agentprovides excellent symptomatic pain relief and regainedmovement without any complication in patients havingtrigger finger.
REFERENCES:1. Newport ML, Lubbock MD, Lane LB, Manhasset NY,
Stuchin SA. Treatment of trigger finger by steroid inje-ction. J HAND SURC 1990;15A:748-50
2. Benan M, Dala-Ali, Nakhdjevani A, Lloyd MA, FrederikB, Schreude FBR.The Efficacy of Steroid Injection inthe Treatment of Trigger Finger.Clinics in Orthopedic,Surgery 2012;4:263-8
3. Verdon ME. Overuse syndromes of the hand and wrist.Prim Care 1996;23:305-19
4. Strom L. Trigger finger in diabetes. J Med Soc N J. 1977;74(11):951-4
5. Akhtar S , Bradley MJ, Quinton DN, Burke FD. Manage-ment and referral for trigger finger/thumb.2005; 331 (7507): 30-3
6. Gorsche R, Wiley JP, Renger R, Brant R, Gemer TY,Sasyniuk .Prevalence and incidence of stenosing flexortenosynovitis (trigger finger) in a meat-packing plant.
JBUMDC 2016; 6(2): 84-87 Page-86
Efficacy of Steroid Injection in the Treatment of Trigger Finger

J Occup Environ Med 1998;40 (6): 556-607. Kolind S V. Treatment of trigger fingers. Acta Grthop
Stand 1970;41:428-328. Rhoades CE, Gelberman RH, Manjanis JF. Stenosingten-
osynovitis of the fingers and thumb. Clin Grthop 1984;190:236-8
9. Freiberg A, Mulholland RS, Levine R. Non-operativetreatment of trigger fingers and thumbs. J Hand SurgAm. 1989;14(3):553-8
10. American Society for Surgery of Hand (ASSH) . Acces-sed on 2-1-2016
11. Howard LD Jr, Pratt DR, Bunnell S. The use of compou-nd F(hydrocortone) in operative and non-operative con-ditions of the hand. J Bone Joint Surg Am. 1953;35 (4):994-1002
12. Green D, Hotchkiss R, Pederson W, Wolfe S. Green’soperative hand surgery. 5th ed. London: Churchill Livi-ngstone; 2005
13. Daniel M, Joseph MF, Mark P. Koniuch. Steroid versusplacebo injection for trigger finger.J Hand Surg Am. 1995;20(4):628-31
14. Lambert MA, Morton RJ, Sloan JP. Controlled Studyof the Use of Local Steroid Injection in the Treatmentof Trigger Finger and Thumb. J Hand Surg Br. 1992;17(1):69-70
15. Bensona LS, Amy JP.Injection versus surgery in thetreatment of trigger finger .The Journal of Hand Surgery1997;22 (1):138-40
16. Patel MR, Lynn B M. Trigger fingers and thumb: Whento splint, inject, or operate.The Journal of Hand Surgery1992;17(1):110-3
17. Sean MG, Arnold P,Lewis B, Christopher S, EdwardA, KaviS.Treatment of trigger finger in patients withdiabetes mellitus.The Journal of Hand Surgery 1995;
20(5): 787-918. Brian TF, Eric PH, Ryan A F, Michael AT.Delayed
Flexor Digitorum Superficialis and Profundus Rupturesin a Trigger Finger After a Steroid Injection: A CaseReport Journal of Hand Surgery 2005;30(3):479-82
19. Kazuki,Egi T, Okada M, Takaoka K. Clinical outcomeof extrasynovial steroid for trigger finger Injection. HandSurg 2006; 11(1-2):1-4
20. Michael RM, Stephen FG. Efficacy of cortisone injectionin treatment of trigger fingers and Thumb. The Journalof Hand Surgery 1989;14(4):722-7
21. John ST, James SR, Wayne TP, Fara M, Dean GS. Corti-costeroid injections for trigger digits: Is intrasheathinjection necessary? The Journal of Hand Surgery 1998;23(4):717-22
22. Shalom S, Yoram K, Eddy K. Outcome of trigger fingertreatment in diabetes. Journal of Diabetes and its Compli-cations1997;11 (5):287-90
23. Nimigan AS, Ross DC, Gan BS: Steroid injections inthe management of trigger fingers. Am J PhysMedRehabil 2006;85:36-43
24. Mukund R, Vijay JM. Percutaneous release of triggerdigit with and without cortisone injection The Journalof Hand Surgery 1997; 22(1):150-5
25. Schubert C, Helen G, Hui-Chou, Alfred PS, Deune EG.Corticosteroid injection therapy for trigger finger orthumb: a retrospective review of 577 digits. Hand (NY). 2013 Dec; 8(4): 43944 PMCID: PMC3840755. Pub-lished online 2013 Jul 12. doi: 10.1007/s11552-013-9541-6
26. Wiwanitkit S, Wiwanitkit V. Trigger Digits and DiabetesMellitus. N Am J Med Sci. 2012; 4(3): 117-9. PMCID:
JBUMDC 2016; 6(2): 84-87 Page-87
Adeel Ahmed Siddiqui1, Farooq Mamji2, Badaruddin Sahito3, Syed Mohammad Tariq4, Dileep Kumar5,Syed Itaat Hussain Zaidi6

ORIGINAL ARTICLE
JBUMDC 2016; 6(2): 88-91 Page-88
ABSTRACT:Objective:To compare and find out the possible application of OPG for gonial angle and compare it with cephalogram inOrthodontic patients of a Public Sector Dental Institute.Materials and Methods:In this descriptive retrospective study lateral cephalograms and OPG of 103 patients, 27 males and76 females were analyzed. The gonial angle was determined in panoramic radiographs by two tangents drawn from the condyle’sposterior borders and right and left ramus and inferior border of the mandible. Landmarks in the cephalogram were identifiedand spotted. Cephalometric protractor and calipers were used to mark and measure the angles. Angles and other parameterswere rechecked to counter any missed measurement.Results: In lateral cephalograms the mean value of gonial angle was 121.77° and in panoramic radiographs 122.18°. In females,the difference among the mean gonial angle in both radiographs was 1.20 and in males 1.224 while difference among the twogenders was 0.02°. As P > 0.05 for all the variables stated above, these differences were not significant.Conclusion: OPG may be considered to evaluate the gonial angle as correctly as a lateral cephalogram because in the valuesof gonial angles measured in both radiographs there was non- significant difference. The plus point in OPG is that it is moreaccurate in evaluating patient’s gonial angles without any overlaid images.Keywords: Gonial angle, Cephalograms, Orthopantomogram, Orthodontic treatment, Dental institute
INTRODUCTION:In orthodontics to get the information regarding axialinclinations, maturation periods, and surrounding tissuesof the teeth panoramic radiograph has been widely used.For cephalometric measurements, another radiographis considered that is Lateral cephalogram. In orthodonticstreatment, planning the Gonial Angle is extensivelyconsidered. The gonial angle is the angle between animaginary tangential line along the inferior border ofthe mandible and along the posterior border of themandibular ramus.1
History, clinical examination and diagnostic recordscounting radiographs, photographs and dental casts’evaluation are the key sources, from where orthodonticdiagnostic records are taken. All the patients undergoingorthodontic treatments have cephalograms and orthop-antomogram (OPG). Vertical and Horizontal relationshipof five main functional components of face include thecranium and cranial base, skeletal mandible and maxilla,alveolar process and the mandibular dentition.
To get significant data about dentition, their growthphases, neighboring tissues and axial inclinationspanoramic radiography is considered in orthodontics.For complete evaluation of dental occlusion, hard tissuecorrelation and soft tissue proportion radiographs arerequired.For cephalometry presently, lateral and antero-posterior projections are in practice. Determiningindividual gonial angles is challenging, in this method,because other images are superimposed in lateralcephalograms. However, in Panoramic imaging thisproblem does not occur and for jaw investigations andevaluation it is in use on a very high scale. Both thevertical and horizontal relationship of these structuresis equally important because the planning of treatmentand the result of treatment is affected by pattern ofgrowth of the patient and the vertical relationships.2 Forthe craniofacial complex and craniofacial disorders,diagnosis of the external gonial angle is the significantangle. Gonial angle is one of the vital factors giving asign about the vertical parameters and symmetry of thefacial skeleton.3
In 1961 a Professor from University of Helsinki namedYrjö Paatero introduced panoramic radiography. To getsignificant data about dentition, their axial inclinations,development stages and adjacent tissues panoramicradiography is regularly recommended in orthodontics.By quality of its ability to take a solitary picture of theentire oral cavity, jaws, sinuses-panoramic, temporoman-dibular joints, radiography forms an essential orthodonticscreening tool. Studies inspecting panoramic radiographsas a source of exploring skeletal patterns are deficientin the orthodontic studies. In OPG the problem ofsuperimposed images are negligible as compared tocephalograms and it can be used for better measurementand evaluation.4The aim of the current research is tocompare and find out the possible application of OPG
Comparison of Gonial Angle Determination fromCephalograms and Orthopantomogram of
Patients under OrthodonticTreatment
Mansoor Majeed1,Imtiaz Ahmed2
Dr. Mansoor MajeedPost graduate traineeDepartment of Oral BiologyDow University of Health SciencesKarachiE-mail: [email protected]
Dr. Imtiaz AhmedProfessor and HeadDepartment of OrthodonticsDow University of Health SciencesKarachiReceived: 11-01-2016Revised: 26-02-2016Accepted: 05-03-2016

for gonial angle and compare it with cephalogram oforthodontic patients in a public sector dental instituteof Karachi.
MATERIALS AND METHODS:Records of Lateral cephalograms and OPG of 103patients from August 2014 to January 2015 were takenfrom the Department of Orthodontics,. Dow Universityof Health Sciences. There were 27 males and 76females.The mean age was 16.24 years with an agerange from 11 to 30 years.The standard for assortmentof patient`s radiographs were as follows: the OPG andLateral cephalogram should be of superior quality andclear with same X-ray machine used to take allradiographs and in natural head position (NHP). Goodquality radiographs were selected and cellulose acetatesheets were used for tracing with a pencil number 2Hby a single operator. Landmarks in cephalogram wereidentified and spotted. Cephalometric protractor andcalipers were used to mark and measure the angles.Angles and other parameters were rechecked to counterany missed measurement.The gonial angle was foundout in panoramic radiographs from two tangents drawnfrom the condyle’s posterior borders,right and left ramusand inferior border of the mandible.SPSS regressionanalysis and Student’s t test were applied to evaluatestatistically significant differences between the
variable.SPSS version 16 was used for statistical analysisand probability level of P < 0.05 was considered to bestatistically significant.
RESULTS:In lateral cephalograms the mean value of gonial anglewas 121.77° and 4.75 was the STD deviation and inpanoramic radiographs 122.18° was the mean value and4.61 STD deviation of the gonial angle (Table 1).Between the two genders there was no statisticallysignificant difference as in females gonial angle was122° and gonial angle in males was 124°. In OPG,122.14° was the mean value of the right gonial anglewith 4.77 standard deviation and 122.74° was the meanvalue of left gonial angle with a 3.55 standard deviation.The difference between the values of gonial anglesdetermined by lateral cephalogram and panoramicradiography was non- significant. Also the differencein right and left gonial angle was non-significant.According to outcomes of the current study, in femalesthe difference among the mean gonial angle in bothradiographs was 1.22 and 1.24 in males and the differenceamong the two genders was 0.02° (Table 2).As P > 0.05 for all the variables stated above, thesedifferences were non significant. In linear regressionsignificant association is observed among the means ofgonial angle in lateral cephalometry & OPG.
JBUMDC 2016; 6(2): 88-91 Page-89
Mansoor Majeed1,Imtiaz Ahmed2
Table: 1Range, standard deviation and mean of gonial angle in lateral cephalogram
and panoramic radiographs (OPG) in degrees
Variables
Gonial angle in cephalogramGonial angle in OPGRight gonial angle in OPGLeft gonial angle in OPG
Range
112-130110-136110-136110-137
STD deviation
4.754.614.773.55
Mean
121.77122.18122.14122.74
Table: 2Comparison of gonial angle in later cephalogram and OPG
Variable
Gonial angle in cephalogram and OPGRight and left gonial angle in OPGGonial angle in cephalogram and OPG (males)Gonial angle in cephalogram and OPG (females)Right gonial angle in cephalogram and OPGLeft gonial angle in cephalogram and OPG
Mean differences (degree)
-0.410.061.241.220.020.02
DISCUSSION:In our study , the difference of average measurementsof external gonial angle were not significant betweenlateral cephalogram and panoramic radiographs. A studydone by Mattila have stated that there is no suchdifference between the gonial angle in both radiographs,though the mean gonial angles were 127.8° and 128.6°in panoramic and lateral cephalogram respectively.5
Shahabi have equated the external gonial angle takenfrom panoramic radiographs and lateral cephalogramsin Class I malocclusion patients. Established on the
results, they proved that panoramic radiography is asaccurate as lateral cephalogramin determining the gonialangle.6
Application of OPGs for measurement of vertical andhorizontal angular measurement is proved by Jena.7Formandible’s linear measurement that is menton- gonion,gonion-condylion and menton-condylion, OPG is astrustworthy as a lateral cephalogram and it is anestablished radiological evaluation of changesingonialangle.8 Fisher-Brandies in his study has observeda difference of 2.2-3.6 degree in the gonial angle between

JBUMDC 2016; 6(2): 88-91 Page-90
panoramic and lateral cephalogram and the differencewas significant.9 This result is totally opposite to theresult of our study.Angle assessment on the left & right panoramicradiographs makes it feasible to precisely assess thevariations at the end of orthodontic treatment.Inevaluating inclination of mandible and gonial angle, ithas been reported that panoramic radiography has apotential. For finding out the gonial angle that isconsidered to be a decent indicator of mandibularsteepness & growth direction, panoramic radiographyhas been used widely.10Fatahi and Babouei have estimatedthe accuracy of cephalometric measurements whendetermined from an OPG.11
A comparison of actual measurements from dry skullsand panoramic radiographic measurements showed goodassociation between panoramic and cephalometricradiographs in gonial angle, whereas the minimumcorrelation was observed in the length of the mandibularbody. In different growth patterns, it was seen that gonialangle and ramus height showed highest correlationbetween the two radiographs. They reported that thecapability to determine growth direction from the OPGshould be beneficial because most of the dentists demandan OPG for patients during oral examination.12As OPGis normally suggested by a dental surgeon during oralcheckup. It appears to be a beneficial feature of thismodality for determination of direction, so the verticalgrowth tissues can be easily detected by the dentist.Astudy done by Larheim also have specified that OPGand lateral cephalograms were precise in defining gonialangle and the difference was not significant among theleft and right sides in panoramic radiography. Severalresearches have established the effectiveness formeasuring the gonial angle by panoramic radiography,the right and left gonial angles do not overlap differingwith cephalometry.13A study conducted by Al haija havereported the possibility that panoramic radiographsmeasure mandibular inclination and steepness. Extremeassociation between the measurements extracted fromboth radiographs was found. They also reported that forthe measurement of gonial angle panoramic radiographcan be a valuable tool.14A previous study by Raustiaproved that genders have irrelevant influence ongonialangle’s size.15A variance ingonial angle of left sideamong the two genders was showed by Gungor.16
However, research done by Nohadani associatedlongitudinal vertical facial and dentoalveolar variationsusing OPGs with measurements on lateral cephalometricradiographs.17After using OPG to find out mandibularsymmetry in Class II malocclusion patients, by measuringdifferent parameters Kurt has concluded that satisfactoryoutcomes can be attained with panoramic radiographs.18Furthermore the panoramic radiographs are of lowcost and chances of radiation exposure are also fairlylow.19Multiple studies have admitted that panoramicradiography is comparatively better in measuring gonialangle and other important aspects needed to be in focus,that is, there is no overlapping in right and left gonialangles on OPG as compared to Cephalometry.1,6,14,15,
20On the contrary many researchers share the idea thatthere is a person to person discrepancy in gonial angledistortion and proves that gonial angle differs in differentclasses of malocclusions in different age groups andamong genders as well.21, 22, 23,24,25
CONCLUSION:Panoramic radiography may be considered to evaluategonial angle as correctly as a lateral cephalogram becausein values of gonial angles measured by cephalogramand OPG there in non-significant difference. The pluspoint in OPG is that it is far better and more accuratein evaluating patient’s gonial angles without any overlaidimages because of the anatomical landmarks in lateralcephalogram. OPG may be a superior choice in evaluat-ing gonial angle than lateral cephalogram. Thus currentstudy confirms the opportunity of enhancing the clinicalusefulness of panoramic radiograph.
REFERENCES:1. Ceylan G, Yanikoglu N, Yilmaz AB, Ceylan Y. Changes
in the mandibular angle in the dentulous and edentulousstates. J Prosthet Dent 1998;80(6):680-4
2. Staley RN. Cephalometric analysis. In:Textbook of ort-hodontic, Bishara SE edition 3rd, W. B.Saunders, Phil-adelphia 1972 , p. 113-7
3. Mandeep KB, Amandeep SU, Gulsheen KK, Sanjay C,Anuraj S K. Comparison of gonial angle determinationfrom cephalograms and orthopantomogram. Indian JDent 2014; 5(3): 123-6
4. White SC, Pharoah MJ. Oral radiology: principles andinterpretation. 4th edition, Mosby, St Louis 2000, 205-6
5. Mattila K, Altonen M, Haavikko K. Determination ofgonial angle from the orthopantomogram. Angle Orthod1977;47:107-10
6. Shahabi M, Ramazanzadeh BA, Mokhber N. Comparisonbetween the external gonial angle in panoramic radiogr-aphs and lateral cephalograms of adult patients withClass I malocclusion. J Oral Sci 2009;51(3):425-9
7. Jena AK, Singh SP, Utreja AK. Effects of sagittal max-illary growth hypoplasia severity on mandibular asymm-etry in unilateral cleft lip and palate subjects. Angle Or-thod 2011;81:872-7
8. Ongkosuwito EM, Dieleman MM, Kuijpers-JagtmanAM, Mulder PG, van Neck JW. Linear mandibular mea-surements: Comparison Between orthopantomogramsand lateral cephalograms. Cleft Palate Craniofac J 2009;46:147-53
9. Fischer-Brandies H, Fischer-Brandies E, Dielert E. Themandibular angle in the orthopantomogram. Radiologe.1984;24(12):547-9
10. Niwa K, Maeda T, Omichi S, Sumikawa Y. Estimationof the gonial angle from the orthopantomogram. GifuShika Gakkai Zasshi 1990;17(1):7-16
11. Fatahi HR, Babouei EA. Evaluation of the precision ofpanoramic radiography in dimensional measurementsand mandibular steepness in relation to lateral cephalo-merty. J Mashhad Dent Sch Fall 2007;31:223-30
12. Zangouei-Booshehri M, Aghili H-A, Abasi M, Ezoddini-Ardakani F. Agreement Between Panoramic and LateralCephalometric Radiographs for Measuring the GonialAngle. Iranian Journal of Radiology 2012;9(4):178-82
13. Larheim TA, Svanaes DB. Reproducibility of rotational
Comparison of Gonial Angle Determination from Cephalograms and Orthopantomogram of Patients under Orthodontic Treatment

JBUMDC 2016; 6(2): 88-91 Page-91
Mansoor Majeed1,Imtiaz Ahmed2
panoramic radiography: Mandibular linear dimensionsand angles. Am J Orthod Dentofacial Orthop 1986;90:45-51
14. Alhaija ES. Panoramic radiographs: Determination ofmandibular steepness. J Clin Pediatr Dent 2005;29:165-6
15. Raustia AM, Salonen MA. Gonial angles and condylarand ramus height of the mandible in complete denturewearers-a panoramic radiograph study. J Oral Rehabil 1997;24(7):512-6
16. Gungor K, Sagir M, Ozer I. Evaluation of the gonialangle in the Anatolian populations: from past to present.CollAntropol 2007;31(2):375-8
17. Nohadani N, Ruf S. Assessment of vertical facial anddentoalveolar changes using panoramic radiography.Eur J Orthod 2008;30(3):262-8
18. Kurt G, Uysal T, Sisman Y, Ramoglu SI. MandibularAsymmetry in Class II Subdivision Malocclusion. AngleOrthod 2008;78:32-7
19. Nikneshan S, Sharafi M, Emadi N. Evaluation of theaccuracy of linear and angular measurements on panor-
amic radiographs taken at different positions.ImagingScience in Dentistry 2013;43(3):191-6
20. Akcam MO, Altiok T, Ozdiler E. Panoramic radiographs:A tool for investigating skeletal pattern. Am J OrthodDentofacial Orthop. 2003;123:175-81
21. Slagsvold O, Pedersen K .Gonial angle distortion inlateral head films: a methodologic study. Am J Orthod1977:71, 554-64
22. Altonen M, Haavikko K, Mattila K .Developmentalposition of lower third molar in relation to gonial angleand lower second molar. Angle Orthod.1977:47:249-55
23. Ohm E, Silness J.Size of the mandibular jaw anglerelated to age, tooth retention and gender. J Oral Rehabil1999;26:883-91
24. Ranta R, Altonen M .A comparative study of gonialangle and growth of the lower third molar in cleft lipand palate. An orthopantomographical study. Scand JPlast Reconstr Surg 1978;12:273-8
25. Fish SF .Change in the gonial angle. J Oral Rehabil.1979;6:219-27

ORIGINAL ARTICLE
JBUMDC 2016; 6(2): 92-96 Page-92
ABSTRACT:Objective: To assess the functional outcome of radial head fracture Mason type III and IV treated with K-wire fixation.Materials and Methods:This prospective study was conducted at Department of Orthopaedics,Civil Hospital,Dow Universityof Health Sciences Karachi from 2013 to 2015. Patients with Radial head fracture type III and IV were included in the study.Results:A total of 42 patients were included in this study. Out of these 36 were males and 6 were females. Right side wasinjured in 18 patients and left side in 24 patients. 32 patients were with Mason type III radial head fracture and 10 were Masontype IV fractures. All fractures were fixed with open reduction and internal fixation with K-wire. Lateral approach was usedin all fractures. In Type IV elbow was reduced with close technique. Outcome was measured on the basis of Morrey elbowscoring system. 22 patients with type III radial head fracture had excellent results while10 with type III had good result. Allpatients with radial head fractureType IV had good results.Conclusion:Assessment of functional outcome of radial head fracture Mason type III treated with K-wire fixation showedexcellent outcome in majority of patients while Type IV had good outcome.Mason type III radial head fractures should bereduced and fixed with K-wire. It maintains the stability of elbow joint and elbow function.Keywords: Radial head, Fracture, Mason type III, Mason type IV, K-wire, Reduction,Fixation
INTRODUCTION:Fractures of the radial head represent a common entityaccounting for 33% of all elbow fractures .The typicalmechanism involves the application of an axial load tothe forearm by a direct fall onto the outstretched handwith the elbow in the extended and the forearm in thesupinated position or by subluxation from a posterolateralrotatory movement which lead the radial head to hitagainst the capitellum of the humerus. The resultantfractures vary from the undisplaced ones to the morecomminuted with the possibility of associated elbowinstability patterns The latter are usually caused by highenergy trauma which ruptures the distal radioulnar jointand the interosseous membrane, an injury pattern referredto as the Essex-Lopresti lesion.1
Radial head fractures are challenging injuries to treat.2
In adults they are less common.3Bromberg and Morrey
in 1986, Coleman in 1987 and Esser in 1995 describedthe non-operative treatment with early mobilization inthe management of minimally displaced radial headfractures.4,5 ,6 Mason in 1954, Lindemann-Sperfeldet in2002, Herbertsson in 2004, King in 2004 haverecommended the open reduction and internal fixationwith an intra-articular step of 2 mm or more because ofearly arthritic changes that are more likely tooccur.7Mason has classified the radial head fracture thatis universally accepted.8Treatment options are radialhead excision. “If in doubt, resect” was the old dogmaregarding the treatment of fractures of the radial headwhich were first classified by Mason in 1954.9Severalclassification schemes have been introduced with themost widely used being that described by Mason .In hisoriginal article, Mason proposed a classification systemin an attempt to provide a guide for optimal management.
Radial Head Fracture Mason Type III and IV Treatedwith K-wire Fixation
Farooq Mamji1, Badaruddin Sahito2, Adeel Ahmed Siddiqui3, Syed Mohammad Tariq4, Dileep Kumar5
Syed Itaaat Hussain Zaidi6
Dr. Syed Mohammad TariqAssistant ProfessorDepartment of Orthopaedic SurgeryCivil Hospital & Dow Medical CollegeDow University of Health SciencesKarachi
Dr. Dileep KumarAssistant ProfessorDepartment of Orthopaedic SurgeryCivil Hospital& Dow Medical CollegeDow University of Health SciencesKarachi
Dr. Syed Itaaat Hussain ZaidiAssistant ProfessorDepartment of Orthopaedic SurgeryDow International Medical CollegeDow University of Health SciencesKarachiReceived: 03-02-2016Revised: 25-03-2016Accepted: 28-03-2016
Dr. Farooq MamjiAssociate ProfessorDepartment of Orthopaedic SurgeryCivil Hospital & Dow Medical CollegeDow University of Health SciencesKarachiEmail:[email protected]
Dr. Badaruddin SahitoAssistant ProfessorDepartment of Orthopaedic SurgeryCivil Hospital & Dow Medical CollegeDow University of Health SciencesKarachi
Dr. Adeel Ahmed SiddiquiAssistant ProfessorDepartment of Orthopaedic SurgeryCivil Hospital & Dow Medical CollegeDow University of Health SciencesKarachi

After evaluating the results of conservative and operativemanagement of every radial fracture pattern in a periodof 26 months’ follow-up in terms of restoration ofradiographic alignment, pain, range of motion, abstentionfrom and return to work, he categorized the fracturesinto 3 types. Type I included all the undisplaced fractures,type II described the marginal fractures with displacementincluding impaction, depression and angulation and typeIII referred to the comminuted fractures involving theentire radial head. Johnston modified the original Masonclassification adding a fourth type describing fracturesassociated with dislocation of the elbow.10Fixation canbe done with mini low profile plate,K-wire, externalfixator, mini screw, absorbable pins and radial head rep-lacement.11,12 K wire of 1.5 mm to 2 mm is used for thefixation of fractures.Mason type III fracturesIn the past, following an initial failed attempt ofconservative management the preferred option was thatof radial head excision It was not until early 80s thatthe role of radial head as a secondary stabilizer of theelbow was appreciated .In cases of intact medial andulnar collateral ligaments and interosseous membrane,the head of the radius acts as a secondary stabilizer tovalgus stresses and approximately 60% of the load ofthe forearm can be transmitted through its surfaceHowever, the situation changes when either of theligaments or the interosseous membrane is torn, as theradial head then assumes the role of primary stabilizerand therefore is subjected to supraphysiological loads.A second role is attributed to the radial head as it providesstability to the distal radio-ulnar joint in resisting forearmaxial forces .The combined injury to the interosseousligament and the triangular fibrocartilage complexleading to axial instability of the forearm has been wellrecognized and defined as the Essex-Lopresti lesion.13,14
Radial head excision, in case of associated ligamentousinjury, can lead to chronic lateral instability of the elbowas the lack of the ulnar bony support normally providedby the radial head will result in long-term overloadingof the medial collateral ligament and its subsequentfailure as well as in an increase in the carrying angle.A subgroup of patients who presented with posterolateralinstability after radial head resection was identified byHall, further emphasizing the need for accuraterecognition of the unstable fracture patterns. Laterfindings include loss of range of motion of the elbow,radiologic evidence of osteoarthritis, pain and symptomsfrom ulnar nerve compression. Additionally, the overallrisk of subsequent dislocation of the elbow is increased.Further proximal migration of the radius, which wasfirst described by Brockman in 1931, can lead to distalradioulnar joint subluxation with degenerative changesof the wrist joint.14A researcher has concluded that openreduction and internal fixation of the Mason type-IIIfractures have superior outcomes in terms of joint motion,strength and elbow function comparing to those whounderwent resection.15Furthermore, according to theresults of a large meta-analysis with a total of 1264patients, Zwingmann reported a success rate of 92% incase of open reduction and internal fixation with screws,biodegradable pins or plates.16
Mason type IV fracturesIn the case of the more complicated type III fractures,wich are named as type IV fractures in modifiedclassification reduction should be attempted first andthen it should be managed as a type III fracture. Due tothe unstable pattern of this injury, it should be managedwith either open reduction and internal fixation orexcision and arthroplasty. Better results have beenreported with open reduction and internal fixation.17
Present study was carried out to assess the functionaloutcome of radial head fracture Mason type III and IVtreated with K-wire fixation. K wire was used becausethe technique is simple for fixation, requires less surgicaltime and is easy to remove.
MATERIALS AND METHODS:This Prospective study was conducted at Departmentof Orthopaedics,Civil Hospital, Dow University ofHealth Sciences, Karachi, from 2013 to 2015. Patientswith Radial head fracture type III and IV were includedin this study while patients with intra-articular fracture,comminuted fracture and open fracture were excluded.Allfractures were fixed with open reduction and internalfixation with K-wire. Lateral approach was used in allfractures. In Type IV elbow was reduced with closetechnique. Outcome was measured on the basis ofMorrey elbow scoring system.In the categorical rating,95-100 points indicates an excellent outcome; 80-94points, a good outcome; 60-79 points, a fair outcome;60 points, a poor outcome. (Table 1).
JBUMDC 2016; 6(2): 92-96 Page-93
Farooq Mamji1, Badaruddin Sahito2, Adeel Ahmed Siddiqui3, Syed Mohammad Tariq4, Dileep Kumar5 Syed Itaaat Hussain Zaidi6
Table: 1Romberg and Morey scoring system
Variable
Motion ( total for each plane)Flexion (0.2x arc)Pronation (0.1 x arc)Supination (0.1 x arc)
StrengthNormalMild loss ( strength 80% of contralateral side)Moderate loss (strength 50 % of contralateral side)Severe loss ( limits everday task)
StabilityNormalMild loss ( perceived by patient, no limitation)Moderate loss ( limits some activity)Severe loss ( limits everyday tasks)
PainNoneMild (with activity , no medication)Moderate (with or after activity)Severe (at rest , constant medication)
Number of point
2767
201350
5420
3528150
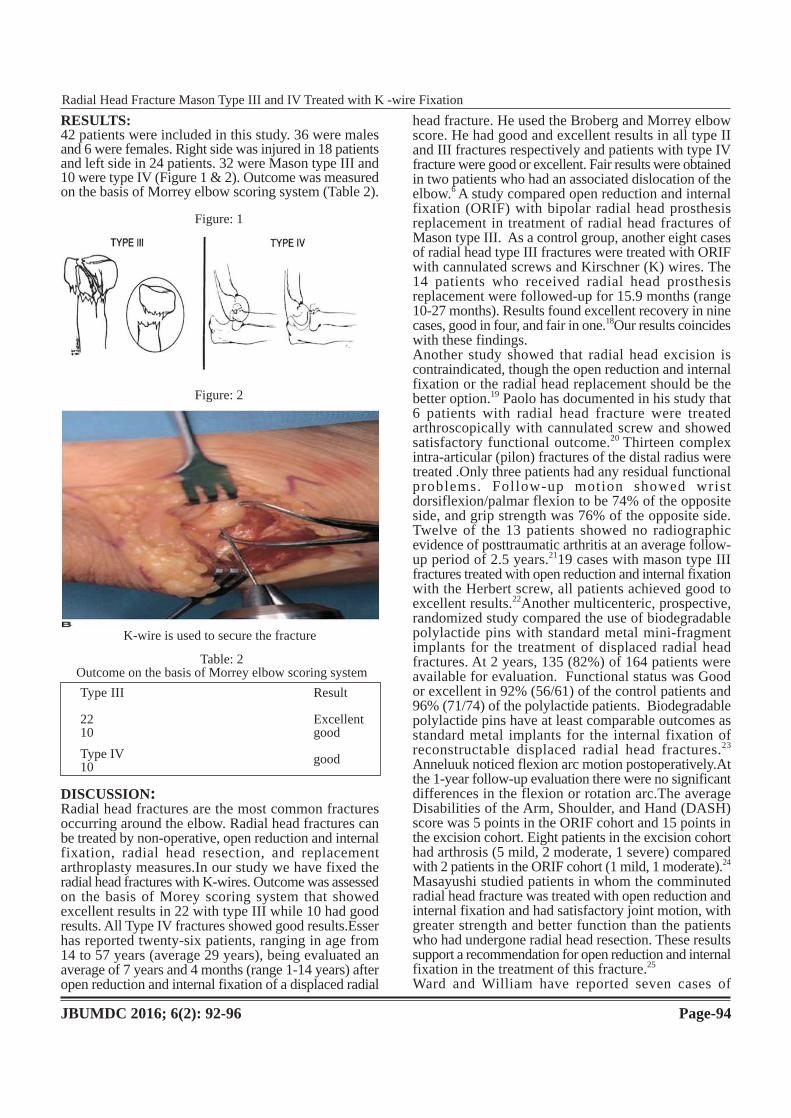
RESULTS:42 patients were included in this study. 36 were malesand 6 were females. Right side was injured in 18 patientsand left side in 24 patients. 32 were Mason type III and10 were type IV (Figure 1 & 2). Outcome was measuredon the basis of Morrey elbow scoring system (Table 2).
DISCUSSION:Radial head fractures are the most common fracturesoccurring around the elbow. Radial head fractures canbe treated by non-operative, open reduction and internalfixation, radial head resection, and replacementarthroplasty measures.In our study we have fixed theradial head fractures with K-wires. Outcome was assessedon the basis of Morey scoring system that showedexcellent results in 22 with type III while 10 had goodresults. All Type IV fractures showed good results.Esserhas reported twenty-six patients, ranging in age from14 to 57 years (average 29 years), being evaluated anaverage of 7 years and 4 months (range 1-14 years) afteropen reduction and internal fixation of a displaced radial
head fracture. He used the Broberg and Morrey elbowscore. He had good and excellent results in all type IIand III fractures respectively and patients with type IVfracture were good or excellent. Fair results were obtainedin two patients who had an associated dislocation of theelbow.6 A study compared open reduction and internalfixation (ORIF) with bipolar radial head prosthesisreplacement in treatment of radial head fractures ofMason type III. As a control group, another eight casesof radial head type III fractures were treated with ORIFwith cannulated screws and Kirschner (K) wires. The14 patients who received radial head prosthesisreplacement were followed-up for 15.9 months (range10-27 months). Results found excellent recovery in ninecases, good in four, and fair in one.18Our results coincideswith these findings.Another study showed that radial head excision iscontraindicated, though the open reduction and internalfixation or the radial head replacement should be thebetter option.19 Paolo has documented in his study that6 patients with radial head fracture were treatedarthroscopically with cannulated screw and showedsatisfactory functional outcome.20 Thirteen complexintra-articular (pilon) fractures of the distal radius weretreated .Only three patients had any residual functionalproblems. Follow-up motion showed wristdorsiflexion/palmar flexion to be 74% of the oppositeside, and grip strength was 76% of the opposite side.Twelve of the 13 patients showed no radiographicevidence of posttraumatic arthritis at an average follow-up period of 2.5 years.2119 cases with mason type IIIfractures treated with open reduction and internal fixationwith the Herbert screw, all patients achieved good toexcellent results.22Another multicenteric, prospective,randomized study compared the use of biodegradablepolylactide pins with standard metal mini-fragmentimplants for the treatment of displaced radial headfractures. At 2 years, 135 (82%) of 164 patients wereavailable for evaluation. Functional status was Goodor excellent in 92% (56/61) of the control patients and96% (71/74) of the polylactide patients. Biodegradablepolylactide pins have at least comparable outcomes asstandard metal implants for the internal fixation ofreconstructable displaced radial head fractures.23
Anneluuk noticed flexion arc motion postoperatively.Atthe 1-year follow-up evaluation there were no significantdifferences in the flexion or rotation arc.The averageDisabilities of the Arm, Shoulder, and Hand (DASH)score was 5 points in the ORIF cohort and 15 points inthe excision cohort. Eight patients in the excision cohorthad arthrosis (5 mild, 2 moderate, 1 severe) comparedwith 2 patients in the ORIF cohort (1 mild, 1 moderate).24
Masayushi studied patients in whom the comminutedradial head fracture was treated with open reduction andinternal fixation and had satisfactory joint motion, withgreater strength and better function than the patientswho had undergone radial head resection. These resultssupport a recommendation for open reduction and internalfixation in the treatment of this fracture.25
Ward and William have reported seven cases of
JBUMDC 2016; 6(2): 92-96 Page-94
Radial Head Fracture Mason Type III and IV Treated with K -wire Fixation
Figure: 1
Figure: 2
K-wire is used to secure the fracture
Table: 2Outcome on the basis of Morrey elbow scoring system
Type III
2210
Type IV10
Result
Excellentgood
good
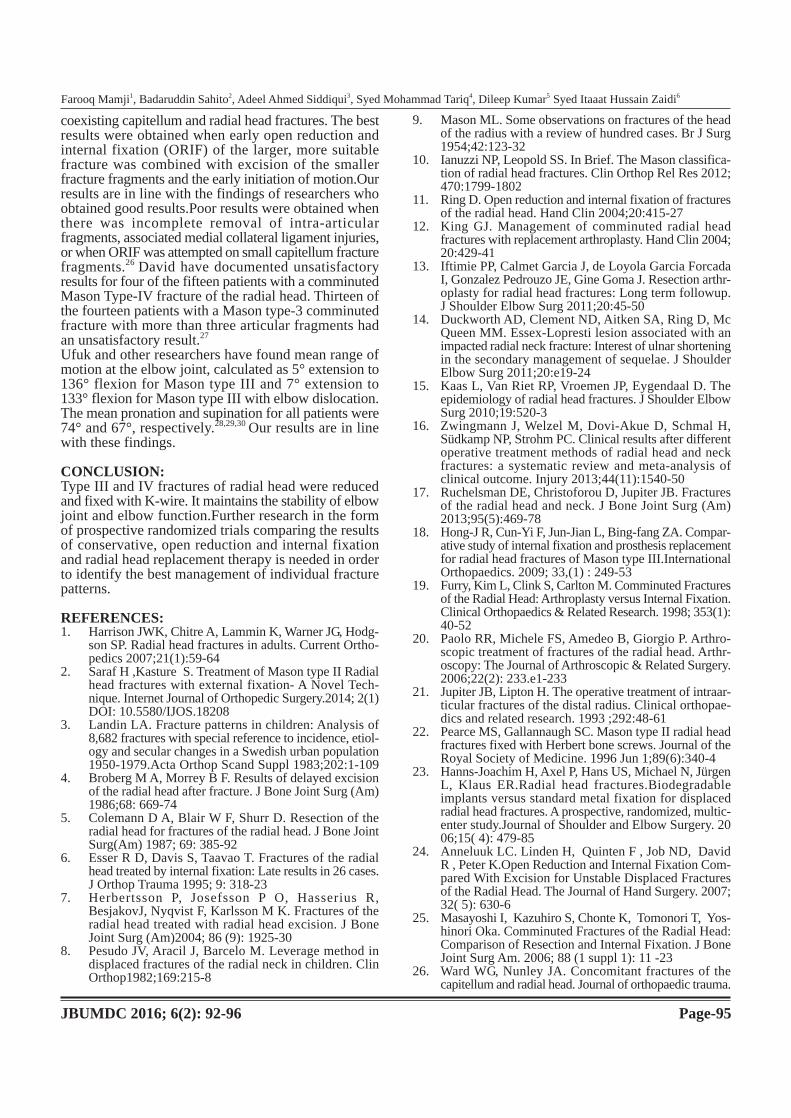
coexisting capitellum and radial head fractures. The bestresults were obtained when early open reduction andinternal fixation (ORIF) of the larger, more suitablefracture was combined with excision of the smallerfracture fragments and the early initiation of motion.Ourresults are in line with the findings of researchers whoobtained good results.Poor results were obtained whenthere was incomplete removal of intra-articularfragments, associated medial collateral ligament injuries,or when ORIF was attempted on small capitellum fracturefragments.26 David have documented unsatisfactoryresults for four of the fifteen patients with a comminutedMason Type-IV fracture of the radial head. Thirteen ofthe fourteen patients with a Mason type-3 comminutedfracture with more than three articular fragments hadan unsatisfactory result.27
Ufuk and other researchers have found mean range ofmotion at the elbow joint, calculated as 5° extension to136° flexion for Mason type III and 7° extension to133° flexion for Mason type III with elbow dislocation.The mean pronation and supination for all patients were74° and 67°, respectively.28,29,30 Our results are in linewith these findings.
CONCLUSION:Type III and IV fractures of radial head were reducedand fixed with K-wire. It maintains the stability of elbowjoint and elbow function.Further research in the formof prospective randomized trials comparing the resultsof conservative, open reduction and internal fixationand radial head replacement therapy is needed in orderto identify the best management of individual fracturepatterns.
REFERENCES:1. Harrison JWK, Chitre A, Lammin K, Warner JG, Hodg-
son SP. Radial head fractures in adults. Current Ortho-pedics 2007;21(1):59-64
2. Saraf H ,Kasture S. Treatment of Mason type II Radialhead fractures with external fixation- A Novel Tech-nique. Internet Journal of Orthopedic Surgery.2014; 2(1)DOI: 10.5580/IJOS.18208
3. Landin LA. Fracture patterns in children: Analysis of8,682 fractures with special reference to incidence, etiol-ogy and secular changes in a Swedish urban population1950-1979.Acta Orthop Scand Suppl 1983;202:1-109
4. Broberg M A, Morrey B F. Results of delayed excisionof the radial head after fracture. J Bone Joint Surg (Am)1986;68: 669-74
5. Colemann D A, Blair W F, Shurr D. Resection of theradial head for fractures of the radial head. J Bone JointSurg(Am) 1987; 69: 385-92
6. Esser R D, Davis S, Taavao T. Fractures of the radialhead treated by internal fixation: Late results in 26 cases.J Orthop Trauma 1995; 9: 318-23
7. Herbertsson P, Josefsson P O, Hasserius R,BesjakovJ, Nyqvist F, Karlsson M K. Fractures of theradial head treated with radial head excision. J BoneJoint Surg (Am)2004; 86 (9): 1925-30
8. Pesudo JV, Aracil J, Barcelo M. Leverage method indisplaced fractures of the radial neck in children. ClinOrthop1982;169:215-8
9. Mason ML. Some observations on fractures of the headof the radius with a review of hundred cases. Br J Surg1954;42:123-32
10. Ianuzzi NP, Leopold SS. In Brief. The Mason classifica-tion of radial head fractures. Clin Orthop Rel Res 2012;470:1799-1802
11. Ring D. Open reduction and internal fixation of fracturesof the radial head. Hand Clin 2004;20:415-27
12. King GJ. Management of comminuted radial headfractures with replacement arthroplasty. Hand Clin 2004;20:429-41
13. Iftimie PP, Calmet Garcia J, de Loyola Garcia ForcadaI, Gonzalez Pedrouzo JE, Gine Goma J. Resection arthr-oplasty for radial head fractures: Long term followup.J Shoulder Elbow Surg 2011;20:45-50
14. Duckworth AD, Clement ND, Aitken SA, Ring D, McQueen MM. Essex-Lopresti lesion associated with animpacted radial neck fracture: Interest of ulnar shorteningin the secondary management of sequelae. J ShoulderElbow Surg 2011;20:e19-24
15. Kaas L, Van Riet RP, Vroemen JP, Eygendaal D. Theepidemiology of radial head fractures. J Shoulder ElbowSurg 2010;19:520-3
16. Zwingmann J, Welzel M, Dovi-Akue D, Schmal H,Südkamp NP, Strohm PC. Clinical results after differentoperative treatment methods of radial head and neckfractures: a systematic review and meta-analysis ofclinical outcome. Injury 2013;44(11):1540-50
17. Ruchelsman DE, Christoforou D, Jupiter JB. Fracturesof the radial head and neck. J Bone Joint Surg (Am)2013;95(5):469-78
18. Hong-J R, Cun-Yi F, Jun-Jian L, Bing-fang ZA. Compar-ative study of internal fixation and prosthesis replacementfor radial head fractures of Mason type III.InternationalOrthopaedics. 2009; 33,(1) : 249-53
19. Furry, Kim L, Clink S, Carlton M. Comminuted Fracturesof the Radial Head: Arthroplasty versus Internal Fixation.Clinical Orthopaedics & Related Research. 1998; 353(1):40-52
20. Paolo RR, Michele FS, Amedeo B, Giorgio P. Arthro-scopic treatment of fractures of the radial head. Arthr-oscopy: The Journal of Arthroscopic & Related Surgery.2006;22(2): 233.e1-233
21. Jupiter JB, Lipton H. The operative treatment of intraar-ticular fractures of the distal radius. Clinical orthopae-dics and related research. 1993 ;292:48-61
22. Pearce MS, Gallannaugh SC. Mason type II radial headfractures fixed with Herbert bone screws. Journal of theRoyal Society of Medicine. 1996 Jun 1;89(6):340-4
23. Hanns-Joachim H, Axel P, Hans US, Michael N, JürgenL, Klaus ER.Radial head fractures.Biodegradableimplants versus standard metal fixation for displacedradial head fractures. A prospective, randomized, multic-enter study.Journal of Shoulder and Elbow Surgery. 2006;15( 4): 479-85
24. Anneluuk LC. Linden H, Quinten F , Job ND, DavidR , Peter K.Open Reduction and Internal Fixation Com-pared With Excision for Unstable Displaced Fracturesof the Radial Head. The Journal of Hand Surgery. 2007;32( 5): 630-6
25. Masayoshi I, Kazuhiro S, Chonte K, Tomonori T, Yos-hinori Oka. Comminuted Fractures of the Radial Head:Comparison of Resection and Internal Fixation. J BoneJoint Surg Am. 2006; 88 (1 suppl 1): 11 -23
26. Ward WG, Nunley JA. Concomitant fractures of thecapitellum and radial head. Journal of orthopaedic trauma.
JBUMDC 2016; 6(2): 92-96 Page-95
Farooq Mamji1, Badaruddin Sahito2, Adeel Ahmed Siddiqui3, Syed Mohammad Tariq4, Dileep Kumar5 Syed Itaaat Hussain Zaidi6

1988 Jan 1;2(2):110-6.27. David R, Jaime Q, Jesse B J.Open Reduction and Internal
Fixation of Fractures of the Radial Head. J Bone JointSurg Am, 2002; 84 (10): 1811-5
28. Ufuk N, Baris K, Arel G, Seref A, Osman G.OpenReduction and Internal Fixation of Mason Type IIIRadial Head Fractures With and Without an AssociatedElbow Dislocation. The Journal of Hand Surgery. 2007;
32(10): 1560-829. Longo UG, Franceschi F, Loppini M, Maffuli N, Den-
aroV. Rating system for the evaluation of the elbow.
British Medical Bulletin 2008;87;131-6130. Jeffrey MP, George SA, Kenneth JF, Graham JW. Radial
Head Fractures-An Update. The Journal of Hand Surgery,2009; 34(3): 557-65
JBUMDC 2016; 6(2): 92-96 Page-96
Radial Head Fracture Mason Type III and IV Treated with K -wire Fixation

ORIGINAL ARTICLE
JBUMDC 2016; 6(2): 97-100 Page-97
ABSTRACT:Objective:To assess parents’ attitude toward EPI(Expanded program on Immunization) in three Tertiary Care Hospitals ofKarachiMaterials and Methods:This cross sectional hospital based study was conducted at three tertiary care hospitals of Karachi,PNS SHIFA Hospital, Jinnah Postgraduate Medical Center (JPMC) and Liaquat National Hospital (LNH) from a period of 20th
July to 20th September, 2015. A structured questionnaire based interview was conducted on150 parents of children less than 5year of age visiting for vaccination at these three tertiary care hospitals.Data was analyzed using SPSS version 23.Results:A total of 150 parents were interviewed, out of which 93 (62.0%) parents vaccinated their child immediately after birth,148(98.7%) parents considered EPI as beneficial for their child’s health, 113 (75.3%) parents were found to be aware of thecomplete vaccination schedule, 56(37.3%)parents had appropriate knowledge regarding vaccines and diseases enlisted on theEPI card, 139 (92.7%) parents kept the record of vaccination schedule, 143(95.3 %) parents didn’t ignored vaccination due toincreased number of children and 21(14%)parents had fear regarding vaccination program.Conclusion:Parent’s attitude toward EPI was positive. However, knowledge about vaccines and diseases and vaccines enlistedon EPI card was low.Key Words:Parents, Tertiary Care Hospitals, EPI, Vaccination
INTRODUCTION:The Expanded Program on Immunization (EPI) waslaunched in Pakistan in 1976 by WHO and UNICEF toprotect children from tuberculosis, poliomyelitis,diphtheria, pertussis, tetanus and measles. In 2002, the
program of Hepatitis-B vaccination was introduced withthe help of Global Alliance for Vaccine and Immunization(now called the GAVI Alliance). In 2006, a tetravalentcombination vaccine was introduced which replacedthe vaccines of diphtheria, tetanus and pertussis (DTP)and hepatitis-B separately. In 2008, pentavalent (DTP-HepB-HIB) vaccine with the addition of the new HIBvaccine was commenced. Now a child needs only fivevisits during the first year and one visit during the secondyear of his/her life to complete the vaccination with fourantigens against eight dreadful diseases. From mid 2012,pneumococcal conjugate vaccine was added inimmunization program. This new vaccine will protectchildren from pneumonia and meningitis due topneumococcal infection. The new vaccines may jointlyavert 17% of childhood mortality in Pakistan and thushelp in achieving Millennium Development Goal 4,after reducing child mortality.However, despite thesuccess of this program, none of the targets have beenachieved yet and Pakistan is still ranked in the top 3countries worldwide where polio is endemic and amongthe 9 Asian countries where neonatal tetanus is one ofthe main causes of infant mortality.1
EPI target diseases are one of the leading causes of highchildhood morbidity and mortality, as evidenced by highInfant Mortality Rates (IMR) in developing countries.2
Immunization is considered by WHO as the most cost-effective intervention to prevent a series of majorpreventable diseases.It prevents 2 million deaths peryear worldwide. However, still 2.5 million deaths a yearcontinue to be caused by vaccine-preventable diseases,mainly in Africa and Asia among children less than 5years old.In the past few decades,immunization coveragerates have improved sufficiently in developed countries,thereby conferring herd immunity, whereas most of thedeveloping countries are still struggling with falteringrates.3,4
Assessment of Parents’ Attitude toward EPI (ExpandedProgram on Immunization) in Tertiary Care Hospitals
of KarachiAbdul Qadir1, Khola Noreen2, Tahira Zamir3, Muhammad Sajid Abbas Jaffri4, Nazish Fatima5, Rehana Khan6,
Sadia Atta7
Dr. Abdul QadirAssistant ProfessorDepartment of Community Health SciencesBahria University Medical and Dental CollegeKarachiEmail:[email protected]
Dr. Khola NoreenLecturerDepartment of Community Health SciencesBahria University Medical and Dental CollegeKarachi
Dr. Tahira ZamirAssistant ProfessorDepartment of PharmacologyBahria University Medical and Dental CollegeKarachi
Dr.Muhammad Sajid Abbas JaffriProfessorDepartment of MedicineBahria University Medical and Dental CollegeKarahi
Nazish Fatima, Rehana Khan, Sadia Atta4th Year MBBS StudentsBahria University Medical and Dental CollegeKarahiReceived:17-02-16Revised: 02-03-16Accepted:10-03-16

Rural communities constitute one of the high-risk areasfor vaccine preventable diseases.5The delivery systemsof the immunizations have many inherent problems towhich an addition may be made by the people themselves,with their prejudices, conclusions and apathy.6
In Pakistan, the reported EPI coverage is still way belowthe herd immunity threshold.7The reasons for inadequateimmunization coverage in Pakistan are several. Theissues of vaccine procurement is its storage, transportand administration, are already known to contribute toinefficiency of the immunization program.8Reasonsunderlying poor coverage have been studied byresearchers worldwide and besides other factors, parentalknowledge and beliefs have been documented toinfluence immunization uptake.9,10,11,12 The fundamentalquestion is whether or not resources should be investedin improving parents’ knowledge of and attitudes towardsvaccination. Although the evidence is unclear, it iscommonly believed, though some disagree.13thatstrengthening advocacy, communication and socialmobilization will enhance informed and willingparticipation in vaccination program and that vaccinationstrategies are likely to be more successful if they arebased on an understanding of sociocultural behavior.14,15
This study was especially designed to assess parent’sattitude toward EPI visiting Tertiary Care Hospitals ofKarachi.
MATERIALS AND METHODS:This cross sectional survey was conducted at threeTertiary Care Hospitals that is PNS SHIFA Hospital,Jinnah Postgraduate Medical Center (JPMC) and LiaquatNational Hospital (LNH) of Karachi from a period of20th July to 20th September 2015.The sample was selectedusing random sampling technique. Parents of childrenbelow 5 years of age as well as parents visiting hospitalfor vaccination of their children were included.Parentsof children above 5 years of age were excluded fromthe study. Verbal consent was taken and confidentiality
was ensured. Data was collected using structuredquestionnaire by taking oral interview from 150 parents(N=150).Data analysis was done using SPSS version23.
RESULTS:A total of 150 parents of children less than 5 years ofage visiting three Tertiary Care Hospitals of Karachi forvaccination purpose were interviewed. The demographicprofile of parents including their educational status andoccupation is shown in Table 1.A total of 148 (98.7%)parents considered EPI as beneficial for their child’shealth, 10 (6.7%) parents didnot considered EPIbeneficial for their child’s health while only one(0.7%)parent was unsure. A total of 113 (75.3%) parents werefound to be aware of the complete vaccination schedulewhereas 37(24.7%) were not aware.56 (37.3%) parentshad knowledge regarding the vaccines and diseasesenlisted on the EPI card whereas 93(62.7%) wereunaware. When maintenance of vaccination records wasasked from parents, 139 (92.7%) parents told that theykeep the record of vaccination of their children, while11(7.4%) parents reported that they donot keep thevaccination record. 143 (95.3%) parents told that theyare not ignorant of vaccination due to increased numberof children whereas 7(4.7%)were found to be ignorantof vaccination due to increased number of children,21(14%) of parents told that they had fear regardingvaccination program whereas 129(86%) did not haveany fear about vaccination. (Table 2)When the time of vaccination from parents was asked,out of 150 parents, 93 (62.0%) parents vaccinated theirchild immediately after birth, 40 (26.7%) parentsvaccinated their child after one day of their birth,10(6.7%) parents vaccinated their child 7 days afterbirth. While remaining 7(4.7%) parents vaccinated theirchild after 7 days of birth.(Table 3)
JBUMDC 2016; 6(2): 97-100 Page-98
Abdul Qadir1, Khola Noreen2, Tahira Zamir3, Muhammad Sajid Abbas Jaffri4, Nazish Fatima5, Rehana Khan6, Sadia Atta7
Parameter Frequency(Percentage%)
Educational statusMotherPrimary 30 (20%)Secondary 33 (22%)Intermediate 46(30.66%)Graduate 40 (26.66%Post graduate 01(0.66%)
FatherPrimary 5(3.33%)Secondary 15(10%)Intermediate 32(21.33%)Graduate 95(63.33%)Post graduate 3(2%)
Occupation:Unemployed noneSelf employed 22(14.66%)Government 31(20.66%)Private Service 97(64.66%)
Table: 1Demographic Profile of the respondents
(N=150)

Table: 2Responses of parents regarding Immunization
(N=150)
Table: 3Time of vaccination
Frequency Percentage %
Vaccinated child immediately after birth 93 (82.0%)Vaccinated child after one day of birth 40 (26.7%)Vaccinated child after 7 days of birth 120 ( 6 . 7 % )Vaccinated child afterwards 7 ( 4 . 7 % )
DISCUSSION:Parents, not doctors, are the primary gate keepers oftheir children’s health. Parents make choices about theamount and quality of health care their children receive,the food they eat, the amount of physical activity theyengage in, the amount of emotional support they areprovided, and the quality of their environments bothbefore and after birth. These choices are conditioned byparents’ material resources, parents’ knowledge of healthpractices and programs, their own health and healthbehavior, and the characteristics of the communities inwhich they live.16
The results of present survey have showed that overallattitude of parents visiting Tertiary Care Hospitals ofKarachi towards EPI was quite positive. However,knowledge regarding vaccines and diseases enlisted onEPI card was low, as 62.7% of parents were found tohave lack of knowledge.When compared with otherauthors, Shahab have reported that 50% of parents hadlack of awareness about EPI at Khyber Teaching Hospitalof Peshawar.17 Whereas Sheikh has reported that 18.1%parents had lack of knowledge regarding EPI visitingTertiary Care Centre.18
A KAP study conducted in an urban population ofnorthern Pakistan has reported that 88% of parents wereknowledgeable about the EPI program, 77% of mothersperceived vaccination to be beneficial, more than 90%had a positive attitude and were ready to pay for services
but only 71% had immunized their children. Reasonsfor not immunizing the children were parents' laziness(72%), uncooperative husband and perceived poor qualityof services.19In another study, mothers' knowledge aboutEPI vaccination in peri-urban area of Karachi was quitelow and not associated with their children's EPIcoverage.20Nisar also have reported in his study thatparents were not aware of the name of diseases enlistedon the EPI card.21
Another emerging issue that threatens immunizationcoverage, especially in developed countries is 'Concernsabout vaccine safety'. Parents feel more threatened bythe side effects of vaccines, which are being observedand reported more frequently than the actual diseaseitself. A study in the United States looked at parentalperceptions regarding vaccine safety and their relationwith immunization status of the child. Children of parentswho had specific concerns regarding side effects or whobelieved that their child was getting too many shots hadsignificantly lower coverage than children of parentswho had no such concern. This study concluded that inorder to sustain adequate coverage in future, additionalresearch about vaccine safety, as well as effectivestrategies to combat parental concerns are needed.22
In our study, 14 % of the parents were found to havefear regarding vaccination.The parents who did notvaccinate their children because of fear of side effectswere 33% in the Pediatric and Gynecology wards of
JBUMDC 2016; 6(2): 97-100 Page-99
Assessment of Parents’ Attitude Toward EPI (Expanded Program on Immunization) in Tertiary Care Hospitals of Karachi
Question Frequency(Percent)
Do you think EPI as beneficial for your child’s health?Yes 148(98.71%)No 10(6.7%)Are you aware of the complete vaccination schedule?Yes 113(75.3%)No 37(24.7%)Do you have knowledge regarding vaccines and diseases enlisted on the EPI card?Yes 56(37.3%)No 93(62.7%)Do you maintain the vaccination record of your child?Yes 139 (92.7%)No 11 (7.4%)Do you ignore vaccination due to increased number of children?Yes 7 (4.7%)No 21(95.3%)Do you have any fear regarding vaccination program?Yes 21(14%)No 129( 86%)
POF Hospital Wah Cantt.23 Kumar reported that 28.8%had a belief that vaccine has side effects.24Another studyhas reported that 21.4% had fear of side effects.25
One of the limitations of this study was a briefly designedquestionnaire but it has provided us a baseline to repeatthis study with a detailed questionnaire in order to reachat a definite conclusion.
CONCLUSION:Parent’s attitude towards EPI was positive. Knowledgeabout vaccines and diseases enlisted on EPI card wasquite low. Educational interventions and mass campaignshould be organized to upgrade parents’ knowledgeabout the diseases which can be prevented by vaccination.
REFERENCES:1. Tarin E, Khalil M, Mustafa T, Alvi ZM, Sy ITS, Thomson
SJ et al.Impact of community based intervention on im-munization coverage against vaccine preventable diseasesin Pakistan. Pakistan J Health 1999;36:53-6
2. Encyclopedia of the Nations. Asia and Oceania. Pakistan.Pakistan Health. (Online) 2007 (Cited 2007 December24). Available from URL:Available at: http://www.nati-onsencyclopedia.com/Asia-and-Oceania/Pakistan-HEA-LTH.html.
3. World Health Organization Media Center.Global Alliancefor Vaccines and Immunization (GAVI). (Online) 2004(Cited 2004 June 16). Available from URL:http://www. who.int/entity/mediacentre/factsheets/en
4. Bhutta ZA, Gupta I, de'Silva H, Manandhar D, AwasthiS, Hossain SM, et al. Maternal and child health: is SouthAsia ready for change? BMJ 2004; 328: 816-9
5. World Health Organization. Immunization, Vaccinesand Biologicals. (Online) 2007 (Cited 2007 December18). Available from URL:http://www.who.int/immunization/en/
6. World Health Report 1999.Making a Difference. (Online)2007 (Cited 2007 December 18). Available from URL:http://www.who.int/whr/1999/en/
7. UNICEF, State of the world Children 2004. OxfordUniversity Press. New York
8. Petrovic V, Seguljev Z, Gajin B. Maintaining the coldchain for vaccines. Med Pregl. 2005; 58: 333-41
9. Rahman M, Islam MA, Mahalanabis D. Mothers' know-ledge about vaccine preventable diseases and immuniz-ation coverage in a population with high rate of illiteracy.J Trop Pediatr 1995; 41: 376-8
10. WangYY, Wang Y, Zhang JX, Kang CY, Duan P. Statusof mother's KAP on child immunization in minorityareas, Guizhou Province [Article in Chinese]. BeijingDa XueXueBao 2007; 39: 136-9
11. Adhikari P, Dhungel S, Shrestha R. Knowledge, attitude
and practice (KAP) study regarding facts for life. NepalMed Coll J 2006; 8: 93-6
12. Anjum Q, Omair A, Inam SN. Improving vaccinationstatus of children under five through health education.JPak Med Assoc 2004; 54: 610-3
13. Wright PF. Global immunization: a medical perspective.SocSci Med 1995; 41: 609-16
14. Nichter M. Vaccination in South Asia: false expectationsand commanding metaphors. In: Coreil J, ed. Anthrop-ology and primary health care. Oxford: Westview Press;1990. p. 196-221
15. Expanded Program on Immunization. The Social Scienceand Immunization Research Project.Wkly EpidemiolRec 1998; 73:285-8
16. Case A, Paxson C. Parental Behavior and Child Health:Health coverage by itself may not influence some of thehealth-related family behavior that affects children’shealth. Health affairs 2002;21(2): 164-8
17. Shahab F,Hussain H,Gul H. Vaccination status and causesof under vaccination in pediatric patients admitted atKhyber teaching hospital Peshawar. J postgrad MedInst2013;27(4):439-4
18. Sheikh A, Iqbal B, Ehtamam A, Rahim M, Shaikh H A.Reasons for non-vaccination in pediatric patients visitingtertiary care centers in a polio-prone country. Archivesof Public Health. The official journal of the BelgianPublic Health Association 2013;71:19 DOI: 10.1186/0778-7367-71-19
19. Sultana A, Jahan S, Ahmad I. Knowledge, Attitude andPractice of immunization in an urban population. PakArmed Forces Med J 2001; 51: 177-81
20. Siddiqi N, Azfar Alam Siddiqi, Nighat Nisar, Altaf Khan.Mother’s knowledge about EPI and its relation with age-appropriate vaccination of infants in peri-urban Karachi,JPMA 2010; 15: 391-5
21. Nisar N, Mirza M, Qadri MH. Knowledge, Attitude andPractices of mothers regarding immunization of oneyear old child at Mawatch Goth, Kemari Town, Karachi.Pak J Med Sci 2010;26(1):183-6
22. Qidwai W, Ali SS, Ayub S, Ayub S. Knowledge, attitudeand practice regarding immunization among familypractice patients JDUSH 2007;1(1):15-7
23. Ramzan, Maqsood. Status of immunization of childrenand factors related to partial and non-immunizationBiomedica 2014;30(3) :1-4
24. Kumar D, Aggarwal A, Gomber S. Immunization statusof children admitted to a tertiary-care hospital of northIndia: reasons for partial immunization or non-immuniza-tion. J Health Popul Nutr 2010;28(3):300-4
25. Shoma FN, Shah NA, Sarker MN, Islam MMSU, Saad T.EPI Coverage among Under 5 Children AttendingPediatric Department of Dhaka Medical College HospitalFaridpur Med. Coll. J 2012;7(2):59-62
JBUMDC 2016; 6(2): 97-100 Page-100
Abdul Qadir1, Khola Noreen2, Tahira Zamir3, Muhammad Sajid Abbas Jaffri4, Nazish Fatima5, Rehana Khan6, Sadia Atta7
ORIGINAL ARTICLE
JBUMDC 2016; 6(2): 101-105 Page-101
ABSTRACT:Objective: To evaluate the effect of leflunomide on laboratory parameters in patients of rheumatoid arthritis.Materials and Methods: A 24-week, single-blind study was carried out on 158 consecutive patients, aged 29-70 years, diagnosedwith rheumatoid arthritis. They received tablet leflunomide 20 mg daily, orally. Laboratory tests were recorded at the initialvisit and follow-ups. Leflunomide has been known to bring about changes in various blood parameters like hemoglobin, totalwhite cell and platelet counts, erythrocyte sedimentation rate, serum creatinine and serum glutamic pyruvic transaminase levels.All patients were subjected to these laboratory tests.Results: At the end of the study at 24 weeks the hemoglobin was raised to 12.62 grams per deciliter (g/dl) from a baseline of10.81 g/dl, white cell count fell to 6,728 per cubic mm (cmm) from 8,318 / cmm, the ESR fell to 39.01 millimeters of mercury(mm of Hg) in 1st hour from 82.10 mm of Hg, the platelet count fell to 2,37,419 / cmm from 2, 96,166 / cmm, the SGPT levelswere raised to 38.01 international units per litre (IU/l) from 31.84 IU/l and the serum creatinine fell to 0.936 mg/dl from0.937 mg/dl. All values, except serum creatinine, were found to be highly significant statistically (p<0.001).Conclusion: Leflunomide showed significant effects on the laboratory parameters. These parameters may be utilizedin patients follow up to monitor the drug response and as a marker of drug safety of leflunomideKeywords: Rheumatoid arthritis, Leflunomide, Laboratory parameters, Drug response, Drug safety
INTRODUCTION:Rheumatoid arthritis (RA) is a progressive, autoimmunedisorder of long duration which involves the entire bodyand is manifested by symmetric, small joint synovitis.The inflammation so produced causes joint destructionthat in turn leads to deformities in the joints. Alteredjoint structure renders them unable to perform theirnormal function. Persistent symptoms with varyingintensity of pain and progressive joint damage thusresults in joint deformities and disabilities.1
The average annual incidence of RA is around 0.03%with a 1% worldwide prevalence rate.2 Almost one-sixth
of the world population lives in India and Pakistan withprevalence rates of 0.5% and 0.2-1% respectively.3 Aprevalence rate of 0.9 and 1.98 per thousand cases wasseen in the poor and affluent districts of Karachirespectively.4
The disease shows a rising incidence until the age of 80with hardly any cases seen below 15 years. It is a female-oriented condition, being 3-5 times more common inwomen as well as smokers. Onset in men is commonafter 45 years with the incidence approaching that ofwomen in the over 65-years age group. Smoking hasbeen seen to be associated with those who also showthe presence of RF and antibodies to cyclic, citrullinatedpeptides (CCPs). Human leukocyte antigen (HLA)marker cluster, HLA-DR4/DR1,5 Epstein-Barr virus(EBV) and Human Herpes virus 6 (HHV-6) have beenlinked with the etiology of rheumatoid arthritis.6,7,8,9
American College of Rheumatology (ACR) has classifiedRA and has framed the following criteria. A personfulfilling four of these criteria is regarded to be sufferingfrom RA (Table 1).10
Permanent joint damage is an early feature in patientswith active polyarticular disease.11 The currently availabletreatment options are disease-modifying anti-rheumaticdrugs (DMARDs), anti-inflammatory agents andanalgesics.12,13 DMARDs have been in use in patientswith RA for the last several years.14 Anti-inflammatory
Leflunomide in Rheumatoid Arthritis:Effect on Laboratory Parameters
Fuad Shaikh1, Shaikh Nadeem Ahmed2, Shamaila Khalid3, Nasim Karim4
Dr. Fuad ShaikhAssistant ProfessorDepartment of Pharmacology & TherapeuticsDow Medical CollegeDow University of Health SciencesKarachiE-mail: [email protected]
Dr. Shaikh Nadeem AhmedProfessorDepartment of Pharmacology & TherapeuticsDow Medical CollegeDow University of Health SciencesKarachi
Dr. Shamaila KhalidAssistant ProfessorDepartment of Pharmacology & TherapeuticsDow Medical CollegeDow University of Health SciencesKarachi
Dr. Nasim KarimProfessor & HeadDepartment of PharmacologyBahria University Medical & Dental CollegeKarachiReceived: 18-02-2016Revised: 25-03-2016Accepted: 29-03-2016
Table: 1The classification criteria based on ACR
S. No.12
34567
ParameterMorning stiffnessArthritis and soft-tissueswellingArthritis of hand jointsSymmetric arthritisSubcutaneous nodulesRheumatoid factorRadiological changes
Features>1 hour most mornings
of >3 of 14 joints
suggestive of joint erosion
Criteria 1-4 should have been present for at least 6 weeks.At least 4 criteria have to be met for classification as Rheumatoid arthritis

drugs and analgesics have no effect on joint damage orrate of disease progression though they may reduce theintensity of pain and joint stiffness.In September 1998 the United States Food and DrugAdministration gave approval for leflunomide to beused in the treatment of RA.15 It acts via its activemetabolite A77 1726, produced in the liver as a resultof first-pass metabolism, to block pyrimidine (uridineand cytidine) synthesis by reversibly inhibiting the rate-limiting enzyme dihydro-orotate dehydrogenase16. Rapidproliferation of activated CD4+ T cells, essential in theinitiation of RA, requires synthesis of new DNA,signalling the lymphocytes to increase their content ofpyrimidines nucleotides.17 A77 1726 intervenes here bynot allowing the T-cells to produce the pyrimidinesneeded for the production of new DNA.Diarrhea, rash, weight loss, reversible alopecia, changesin blood elements and an increase in liver enzyme levelsare associated with the use of leflunomide. Occasionallyfatal acute liver failure is seen within 6 months of startingtherapy. The dose of leflunomide should be reduced ifthe serum alanine transaminase (ALT)/serum glutamicpyruvic transaminase (SGPT) levels increase to twicethe upper limit of normal with discontinuation of drugif this increase persists. Some patients have been knownto develop acute interstitial lung disease which hasoccasionally proven fatal. Patients prescribed leflunomideshould have their platelet count, leucocyte count,hemoglobin and liver enzyme levels checked prior toinitiating therapy then regularly at the time of followup preferably at monthly interval for initial six months.18
Changes in the above parameters can be utilized tomonitor therapy response and determine level of safetyof the drug in RA. Although methotrexate is the firstline therapy for treating rheumatoid arthritis butleflunomide has been used commonly as an alternative.The present study was thus designed to evaluate theeffect of leflunomide on blood, liver and renal laboratoryparameters in patients having rheumatoid arthritis.
MATERIAL & METHODS:This was a 24-week, prospective, single-blind, interventi-onal study conducted between October 2009 to March2011, on patients of either sex suffering from rheumatoidarthritis who visited the out-patient department of a
private teaching hospital and a private consultant’s clinicin Korangi, Karachi. Approval was obtained from andgranted by the Institutional Review Board (IRB), DowUniversity of Health Sciences (DUHS). The hospitaland clinic where the study was carried out cateredpatients from different strata of society. There were dailywage earners, roadside workers, students, office workers,housewives and business executives.Of the selected 158 consecutive patients fulfilling theACR criteria 6 patients dropped out due to personalreasons despite initially agreeing and 4 patients just didnot report for follow up. The remaining 148 patientswere put on leflunomide, 20 mg orally, daily. They weregiven drugs and directed to return for follow up withcertain labs, at which time they were given drugs forfurther use. Follow ups were conducted at 6, 14 & 24weeks.Statistical analysis: Statistical analysis was done bySPSS version 18.0 with paired t-test. The results areshown as mean along with standard deviation. The cutoff P -value was taken to be less than 0.05.
RESULTS:Of the 148 patients that completed the study 118 (79.7%) were female with 109 (73.6 %) positive forRheumatoid Factor. They had a mean age of 46.35 ±9.68 years, ranging between 29 to 70 years (Table 2).The mean baseline hemoglobin was 10.81 ± 1.04 gramsper deciliter (g/dl), mean white cell count was 8,318 ±1,717 per cubic mm (/cmm), ESR was 82.10 ± 14.36mm of Hg in 1st hour, mean platelet count was 2, 96,166± 63,476 /cmm, mean SGPT value was 31.84 ± 6.38international units per litre (IU/l) and mean serumcreatinine was 0.937 + 0.19 mg/dl (Table 3).At the end of the study at 24 weeks the hemoglobin wasraised to 12.62 ± 0.89 g/dl, white cell count fell to6,727.70 ± 1171.65 /cmm, the ESR fell to 39.01 ± 12.88mm of Hg, the platelet count fell to 2, 37,418.92 ±60,968.27 /cmm, the SGPT levels was raised to 38.01± 17.32 IU/l and the serum creatinine fell to 0.936 ±0.13 mg/dl, all values, except those of serum creatinine,being statistically significant (P <0.001, Table 4a). At24 weeks there were 8 (5.4%) female patients withSGPT levels greater than twice the upper limit of normal(Table 4b).
JBUMDC 2016; 6(2): 101-105 Page-102
Fuad Shaikh1, Shaikh Nadeem Ahmed2, Shamaila Khalid3, Nasim Karim4
Table: 2Baseline characteristics
N = 148
Sex Male Female
RheumatoidFactor Present AbsentAge(years)
No ofPatients
30118
10939___
%
20.379.7
73.626.4___
Mean ±StandardDeviation_________
___
46.35 ± 9.68
No of Patients = number of patients , ______ = Nil

JBUMDC 2016; 6(2): 101-105 Page-103
Leflunomide in Rheumatoid Arthritis:Effect on Laboratory Parameters
Table: 3Laboratory parameters: baseline and follow up visits
N = 148
Table: 4aBaseline v/s 24 weeks
N = 148
*** = very highly significant statistically, Paired t-test utilized, NS = non-significant statistically
SD : Standard deviation, g/dl: grams per deciliter, mm of Hg: millimeters of mercury, IU/l: international units perlitre mg/dl: milligrams per deciliter
Parameter
Hemoglobin(g/dl)
Total leucocytecount(per cubic mm)
ErythrocyteSedimentationRate(mm of Hg in 1sthour)
Platelet count(per cubic mm)
Serum glutamicpyruvic transaminase(SGPT, IU/l)
Serum creatinine(mg/dl)
BaselineMean ± SD
10.81 ±1.04
8,318.11 ±1716.80
82.10 ±14.36
2,96,165.54± 63,475.8
31.84 ±6.38
0.937 ±0.19
6 weeksMean ± SD
13.29 ±11.41
7,548.65 ±1,407.92
65.46 ±14.19
267,094.59± 60,336.51
31.03 ±6.71
0.912 ±0 .135
14 weeksMean ± SD
12.31 ±0.96
7,120.95 ±1,295.58
52.12 ±13.51
266,817.57± 201,574.79
35.33 ±11.84
0.924 ±0.1221
24 weeksMean ± SD
12.62 ±0.89
6,727.70 ±1,171.65
39.01 ±12.88
2,37,418.92± 60,968.27
38.01 ±17 .32
0.936 ±0.13
Hemoglobin (g/dl)Hemoglobin (g/dl) at 24 weeks
White cell count (per cmm)White cell count (per cmm) at 24 weeks
Erythrocyte sedimentation rate (mm in 1st hour)Erythrocyte sedimentation rate (mm in 1st hour) at24 weeks
Platelet count (per cubic mm)
Platelet count (per cubic mm) at24 weeks
Serum glutamic pyruvic transaminase (IU/l)Serum glutamic pyruvic transaminase (IU/l) at24 weeks
Serum creatinine ( mg/dl)Serum creatinine (mg/dl) at24 weeks
Mean ±StandardDeviation
10.81 ± 1.0412.62 ± 0.89
8,318.11 ±1716.80
6,727.70 ±1,171.65
82.10 ±14.3639.01 ± 12.88
2,96,165.54 ±63,475.84
2,37,418.92 ±60,968.27
31.84 ± 6.3838.01 ± 17 .32
0.937 ± 0.190.936 ± 0.13
P value
< 0.001 ***
< 0.001 ***
< 0.001 ***
< 0.001 ***
< 0.001 ***
0.915 NS
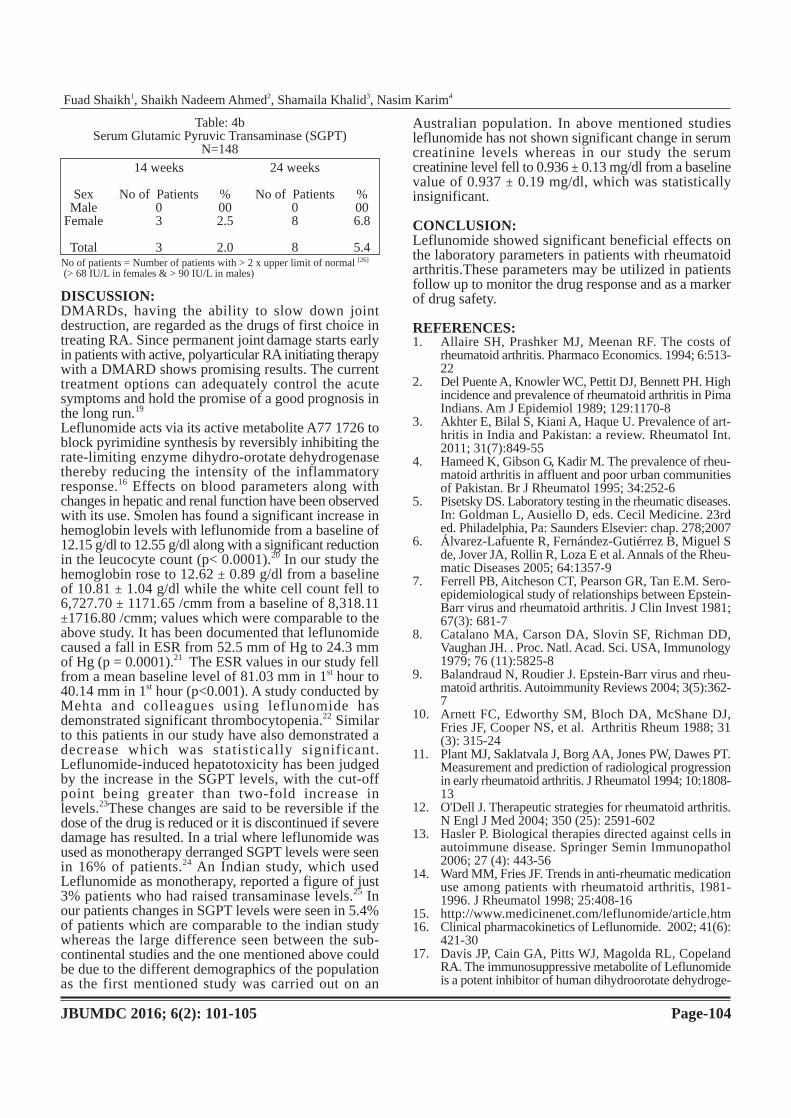
DISCUSSION:DMARDs, having the ability to slow down jointdestruction, are regarded as the drugs of first choice intreating RA. Since permanent joint damage starts earlyin patients with active, polyarticular RA initiating therapywith a DMARD shows promising results. The currenttreatment options can adequately control the acutesymptoms and hold the promise of a good prognosis inthe long run.19
Leflunomide acts via its active metabolite A77 1726 toblock pyrimidine synthesis by reversibly inhibiting therate-limiting enzyme dihydro-orotate dehydrogenasethereby reducing the intensity of the inflammatoryresponse.16 Effects on blood parameters along withchanges in hepatic and renal function have been observedwith its use. Smolen has found a significant increase inhemoglobin levels with leflunomide from a baseline of12.15 g/dl to 12.55 g/dl along with a significant reductionin the leucocyte count (p< 0.0001).20 In our study thehemoglobin rose to 12.62 ± 0.89 g/dl from a baselineof 10.81 ± 1.04 g/dl while the white cell count fell to6,727.70 ± 1171.65 /cmm from a baseline of 8,318.11±1716.80 /cmm; values which were comparable to theabove study. It has been documented that leflunomidecaused a fall in ESR from 52.5 mm of Hg to 24.3 mmof Hg (p = 0.0001).21 The ESR values in our study fellfrom a mean baseline level of 81.03 mm in 1st hour to40.14 mm in 1st hour (p<0.001). A study conducted byMehta and colleagues using leflunomide hasdemonstrated significant thrombocytopenia.22 Similarto this patients in our study have also demonstrated adecrease which was statistically significant.Leflunomide-induced hepatotoxicity has been judgedby the increase in the SGPT levels, with the cut-offpoint being greater than two-fold increase inlevels.23These changes are said to be reversible if thedose of the drug is reduced or it is discontinued if severedamage has resulted. In a trial where leflunomide wasused as monotherapy derranged SGPT levels were seenin 16% of patients.24 An Indian study, which usedLeflunomide as monotherapy, reported a figure of just3% patients who had raised transaminase levels.25 Inour patients changes in SGPT levels were seen in 5.4%of patients which are comparable to the indian studywhereas the large difference seen between the sub-continental studies and the one mentioned above couldbe due to the different demographics of the populationas the first mentioned study was carried out on an
Australian population. In above mentioned studiesleflunomide has not shown significant change in serumcreatinine levels whereas in our study the serumcreatinine level fell to 0.936 ± 0.13 mg/dl from a baselinevalue of 0.937 ± 0.19 mg/dl, which was statisticallyinsignificant.
CONCLUSION:Leflunomide showed significant beneficial effects onthe laboratory parameters in patients with rheumatoidarthritis.These parameters may be utilized in patientsfollow up to monitor the drug response and as a markerof drug safety.
REFERENCES:1. Allaire SH, Prashker MJ, Meenan RF. The costs of
rheumatoid arthritis. Pharmaco Economics. 1994; 6:513-22
2. Del Puente A, Knowler WC, Pettit DJ, Bennett PH. Highincidence and prevalence of rheumatoid arthritis in PimaIndians. Am J Epidemiol 1989; 129:1170-8
3. Akhter E, Bilal S, Kiani A, Haque U. Prevalence of art-hritis in India and Pakistan: a review. Rheumatol Int.2011; 31(7):849-55
4. Hameed K, Gibson G, Kadir M. The prevalence of rheu-matoid arthritis in affluent and poor urban communitiesof Pakistan. Br J Rheumatol 1995; 34:252-6
5. Pisetsky DS. Laboratory testing in the rheumatic diseases.In: Goldman L, Ausiello D, eds. Cecil Medicine. 23rded. Philadelphia, Pa: Saunders Elsevier: chap. 278;2007
6. Álvarez-Lafuente R, Fernández-Gutiérrez B, Miguel Sde, Jover JA, Rollin R, Loza E et al. Annals of the Rheu-matic Diseases 2005; 64:1357-9
7. Ferrell PB, Aitcheson CT, Pearson GR, Tan E.M. Sero-epidemiological study of relationships between Epstein-Barr virus and rheumatoid arthritis. J Clin Invest 1981;67(3): 681-7
8. Catalano MA, Carson DA, Slovin SF, Richman DD,Vaughan JH. . Proc. Natl. Acad. Sci. USA, Immunology1979; 76 (11):5825-8
9. Balandraud N, Roudier J. Epstein-Barr virus and rheu-matoid arthritis. Autoimmunity Reviews 2004; 3(5):362-7
10. Arnett FC, Edworthy SM, Bloch DA, McShane DJ,Fries JF, Cooper NS, et al. Arthritis Rheum 1988; 31(3): 315-24
11. Plant MJ, Saklatvala J, Borg AA, Jones PW, Dawes PT.Measurement and prediction of radiological progressionin early rheumatoid arthritis. J Rheumatol 1994; 10:1808-13
12. O'Dell J. Therapeutic strategies for rheumatoid arthritis.N Engl J Med 2004; 350 (25): 2591-602
13. Hasler P. Biological therapies directed against cells inautoimmune disease. Springer Semin Immunopathol2006; 27 (4): 443-56
14. Ward MM, Fries JF. Trends in anti-rheumatic medicationuse among patients with rheumatoid arthritis, 1981-1996. J Rheumatol 1998; 25:408-16
15. http://www.medicinenet.com/leflunomide/article.htm16. Clinical pharmacokinetics of Leflunomide. 2002; 41(6):
421-3017. Davis JP, Cain GA, Pitts WJ, Magolda RL, Copeland
RA. The immunosuppressive metabolite of Leflunomideis a potent inhibitor of human dihydroorotate dehydroge-
JBUMDC 2016; 6(2): 101-105 Page-104
Fuad Shaikh1, Shaikh Nadeem Ahmed2, Shamaila Khalid3, Nasim Karim4
Table: 4bSerum Glutamic Pyruvic Transaminase (SGPT)
N=148
SexMale
Female
Total
14 weeks
No of Patients03
3
%002.5
2.0
24 weeks
No of Patients08
8
%006.8
5.4No of patients = Number of patients with > 2 x upper limit of normal [26]
(> 68 IU/L in females & > 90 IU/L in males)

nase. Biochemistry 1996; 35:1270-318. Leflunomide monitoring guidelines 3, ebookbrowse,
200919. Nemazee D, Hogquist KA. Antigen receptor selection
by editing or down regulation of V(D) J recombination.Curr. Opin. Immunol 2003; 15: 182-9
20. Smolen JS, Kalden JR, Scott DL. European LeflunomideStudy Group. Efficacy and safety of Leflunomidecompared with placebo and sulphasalazine in activerheumatoid arthritis: a double-blind, randomized, multi-centre trial. Lancet 1999; 353: 259-66
21. Ishaq M, Muhammad JS, Hameed K, Mirza AI. Lefluno-mide or methotrexate? Comparison of clinical efficacyand safety in low socio-economic rheumatoid arthritispatients. Rheumatol 2011;21(4):375-80
22. Mehta V, Kisalay S, Balachandran C. Leflunomide. Ind-ian J Dermatol Venereol Leprol 2009; 75:422-4
23. Curtis JR, Beukelman T, Onofrei A, Cassell S, GreenbergJD, Kavanaugh A et al. Elevated liver enzyme tests am-ong patients with rheumatoid arthritis or psoriatic arthritistreated with Methotrexate and/or Leflunomide. Ann Rh-eum Dis 2010;69(1):43-7
24. Bird P, Griffiths H. Multi-Centre, Cross-Sectional, Obse-rvational Study of the Safety of Methotrexate and Leflu-nomide in Combination in the Treatment of Patientswith Rheumatoid Arthritis. The SMILE Study-Safetyof Methotrexate in Combination with Leflunomide [ab-stract #319]. ACR meeting, 2010
25. Chopra A, Saluja M, Lagu-Joshiv V, Sarmukadam S.Leflunomide is a useful DMARD in Indian (Asian)patients. A clinic based observational study of 1yeartreatment. Clin Rheumatol 2008; 27(8):1039-44
JBUMDC 2016; 6(2): 101-105 Page-105
Leflunomide in Rheumatoid Arthritis:Effect on Laboratory Parameters

INTRODUCTION:Oral health plays an important role in maintaining ahealthy human body but it has unfortunately remainedan ignored and unrealized major social problem.1 Oraldiseases ranging from dental caries (tooth decay) to oralcancer have become a major cause of pain and discom-fort. Dental caries is one of the most frequent andprevalent chronic multi-factorial, microbial, infectious
disease in developed as well as in developing countries,2 which afflict humans of all ages and all areas of theworld.3 It is characterized by demineralization ofinorganic and organic substances of the tooth in whichthe calcified tissues of teeth are being attacked by thebacteria leading to their destruction.4 Dietary sugars/carbohydrates are the most leading causes of this dentalpathology which involves fermentation by the oralbacteria with progressive decalcification of toothsubstance. In general four factors are identified regardingits etiology that are i) bacteria, ii) fermentable carbohyd-rates iii) a susceptible tooth surface and iv) time.5 Dentalcaries has become a serious problem in many populationsworld wide with marked prevalence in several countriesduring the last decade and is frequently found amongthe populations having lack of awareness towards themaintenance of oral hygiene.6
The frequency of caries increases with the increase inage.7 One of the study conducted in northeast Chinaproved that 67.5% of elderly patients when examinedwere found to have dental caries with the prevalence indifferent regions ranging from 66.03% to 87.42 %.8
Other factors that increases frequency of caries arepresence of plaque, poor oral hygiene, gender, inadequatetooth-brushing habits, frequency and timing ofconsumption of sugar-containing drinks.According toNational Oral Health Survey report 2004, cariesprevalence in India was 51.9%, 53.8% and 63.1% atages 5, 12 and 15 years respectively.According to Pakistan Oral Health survey 2006, Pakistanmay also be classified as a low caries country. However,comparing the results of 2006 survey with the findingsof similar surveys conducted in Pakistan under theauspices of the World Health Organization in 1979&1988, it was observed that the DMFT (Decay MissingFilled Teeth) score of 12 year old decreased from 2.2in 1979 to 1.2 in 1988, but the present survey reports
ORIGINAL ARTICLE
JBUMDC 2016; 6(2): 106-109 Page-106
ABSTRACT:Objectives: To determine (a) the frequency of dental caries (b) existing status including the presence of broken down roots(BDRs),missing and filled or unfilled status of permanent mandibular first molar in young adults.Materials and Methods: This study was conducted at out-patients clinics of Bahria University Medical and Dental College(BUMDC) from 1stJanuary 2014 to 30th November 2014. The total numbers of subjects were 1529. Out of which 928 weremales(60.7%) and 601 were females (39.3%). The sample was collected through convenience sampling and the performa wasdesigned which comprised of demographic data including age, gender, carious and filled/unfilled status of left and right permanentmandibular molar (36,46) and informed verbal consent was taken.Results: The study findings showed that higher caries incidence was present in left mandibular 1st molar (tooth # 36) as 232individuals (15.17%) were affected by caries, compared to right mandibular 1st molar (tooth # 46) in which the affected individualswere only 209 (13.66%).Regarding the gender distribution, caries was present more in the males then the females as 179 maleshad caries and only 125 females were affected. Examined individuals have a better knowledge and awareness about oral hygienepractice as affected individuals were only 304 (19.9%). Least contribution was of filled teeth probably because of lack ofavailability of dental services, poor socioeconomic status and high treatment cost.Conclusion:Frequency of dental caries in left and right mandibular first molars in young adults was low with least contributionof filled teeth.Keywords: Frequency,Dental caries, Missing teeth, Young adults
Frequency of Dental Caries and Status of PermanentMandibular First Molar in Young Adults
Syed Ahmed Omer1, Daud Mirza2, Isra Ahmed3, Omer Moosani4, Syed Muzzamil Ali Shah5
Dr. Syed Ahmed OmerAssistant Professor & HeadDepartment of Science of Dental MaterialsBahria University Medical and Dental CollegeKarachiE-mail: [email protected]
Dr. Daud MirzaAssistant Professor & HeadDepartment of Oral PathologyBahria University Medical and Dental CollegeKarachi
Dr. Isra AhmedLecturerDepartment of Science of Dental MaterialsBahria University Medical and Dental College
Dr. Omer MoosaniLecturerDepartment of Science of Dental MaterialsBahria University Medical and Dental CollegeKarachi
Dr. Syed Muzzamil Ali ShahAssistant Professor & HeadDepartment of Community DentistryHamdard College of Medicine and DentistryKarachiReceived: 25-02-2016Revised: 02-05-2016Accepted: 07-05-2016

an increase in this score to 1.6. Similarly for the 15 yearold the DMFT score went down to 1.8 in 1988 from 3.2in 1979 and has witnessed an increase to 2.3 in 2003.9
The aim of this study is to determine the frequency ofdental caries in left and right mandibular first molars inyoung adults attending the Dental OPD of BahriaUniversity Dental College along with the determinationof existing status including the presence of broken downroots (BDRs), missing and filled/unfilled status of thefollowing teeth (#36 and #46).
MATERIALS AND METHODS:This cross-sectional study was conducted in young adultsattending outpatient department (OPD) of BahriaUniversity Medical and Dental College (BUMDC)Karachi, from1stJanuary to 30th November` 2014. Theywere males and females between 18-35 years of age.Sample was collected through convenience sampling.Theinclusion criteria was dentate patients who came fordental treatment ,between 18-35 years of age of bothgenders, healthy individuals with no systemic diseaseand exclusion criterion was mentally retarded individualsor those who refused to give consent and patients abovethirty five years age group.Demographic data of patientsincluding age, gender of patient, carious and filled/unfilled status of left and right permanent mandibularmolar (tooth number 36 and 46 are designated accordingto FDI Brachet tooth notation system) including classI, class II and class V carious lesions, filled or unfilledstatus of the selected teeth with amalgam, compositeand Glass Ionomer restorations and presence of brokendown roots (BDRs) or missing teeth were recorded ina predesigned performa following informed verbalconsent.The data was analyzed by statistical programfor social sciences (SPSS) version 15.0. The frequencyand percentage was computed for a qualitative variablelike gender and mean ± standard deviation was computedfor quantitative variable like age. Collected data fromthese individuals was used to evaluate the frequency ofdental caries and existing status of permanent mandibularfirst molar.
RESULTS:A total of fifteen hundred and twenty nine (N=1529)individuals were examined, aged between 18-35 years(young adults). Out of which 928 (60.7%) were malesand601 (39.3%) were females (Table 1).The mean age was23.49 years with standard deviation (SD±) 4.791.Themale to female ratio was 3:2. Present study findingsshowed higher caries frequency in left mandibular1stmolar as 232(15.17%) of tooth # 36 had carious lesionsthan the right mandibular 1st molar in which 209 (13.66%)were affected by caries (Table 2) and males were affectedmore than the females with 179 males to have cariouslesions on permanent mandibular 1st molars whereasonly 125 females had it. Current study findings alsorevealed that the majority of the first molars were cariesfree or were sound teeth, which is about 1200 (78.5%),1243 (81.3%) in left and right respectively.Regarding the filled status of the teeth,5(0.3%) teeth of
#36 and 6 (0.4%) teeth of #46 were filled/ restored.Asfar as caries is concerned 157 (10.3%) had occlusalcaries (Class 1) and 74 (4.8%) occlusal involvingproximal surfaces (Class 2) and Class V caries wasfound in only in 01 (0.1%) case of 36. On the otherhand in 46, 136 (8.9%), 73(4.8%) had class I and classII caries respectively (Table 2).Chi-Square Test was used to analyze the relationshipbetween gender and caries, in lower left and rightpermanent mandibular first molars which showed asignificant relationship between lower right mandibularfirst molarand lower left mandibular first molar with P-value 0.009 and 0.004 respectively.
DISCUSSION:Oral health is a major part of general health which hasan influence on general well-being of individuals. Amongoral health problems, dental caries has been the mostcommonly investigated oral disease.Apart from othercontributing factors, frequency of sugar consumptionincluding sugary drinks and confectionery leads tooccurrence of caries.10 Sugar is considered as mostimportant dietary factor that leads to enamel dissolutionby acid fermentation of sugar in response to bacterialaction.11Sugars can become a minor determinant ofcaries provided if fluoridated tooth pastes are used andwith proper dental care, keeping this in considerationchildren are less prone to caries compared to adults.12Themain goal of our study was to determine the frequencyof dental caries in permanent mandibular 1st molars(tooth # 36 and tooth # 46) in young adults since it isthe first permanent tooth to be erupted in the dental arch
JBUMDC 2016; 6(2): 106-109 Page-107
Syed Ahmed Omer1, Daud Mirza2, Isra Ahmed3, Omer Moosani4, Syed Muzzamil Ali Shah5
Table:1Distribution of Study Subjects
N=1529
Male
Female
Total
n928
601
1529
%60.7
39.3
100.0
Table: 2Status of tooth #36 and 46
Lower Left First MolarTooth (36)
Lower Right FirstMolar Tooth (46)
Healthy(Sound)Class ICariesClass IIcariesClass VcariesBDRFilledMissing
Total
n1200
157
74
1
26566
%78.5
10.3
4.8
.1
1.70.34.3
Healthy(sound)Class ICariesClass IIcariesClass VcariesBDRFilledMissing
1529 (100.0 %)
n1243
136
73
0
20651
%81.3
8.9
4.8
.0
1.30.43.3

and is the most neglected one in terms of oral hygienemaintenance.Permanent 1st molar erupts in the mouthby the age of 6 years and is considered to be susceptibleto dental caries, therefore it requires maintenance fromearly childhood during which the oral hygienemaintenance is mostly found neglected.Studying thefrequency of caries in permanent 1st molar can be usedas an aid in planning a preventive strategy to minimizethe risk of decay. Improvement in parent’s knowledgeabout the importance of these teeth should be made akey objective especially because most parents areunaware that these teeth are the first permanent teeth toerupt.13
According to our study, the presence of caries in leftand right mandibular 1stmolarsis 232 (15.17%), 209(13.66%) respectively and overall affected individualswere only 304 (19.9%) including males and females. Itrevealed that higher caries frequency is found in leftthan right mandibular first molar and showed that thereare more chances of having occlusal caries (Class I)compared to occluso-proximal lesions (Class II). Thiscan be attributed to the preventive effects of fluoride onsmooth surface as it is consistent with the past studiesby different authors.14,15 Our research revealed lessfrequency of caries in the examined individuals as theaffected individuals were only 304 (19.9%) contrary toprevious researches which showed high frequency. Thisis attributed to a short sample size of examinedindividuals and also the sample was collected throughthe convenience sampling in which the individuals whoreported to the OPD were those who found convenientaccessibility and visited the OPD for regular consultationrather than presenting with any dental pathology of theselected tooth. A study conducted in Nigeria hasdemonstrated that the right mandibular first molar hadthe highest tooth-specific caries frequency (3.5%) inthe permanent dentition and mandibular left first molarhad highest caries frequency (4.7%) in the deciduousdentition.16In our study the frequency was higher in leftmandibular molar probably because of left-handed toothbrushing or mostly the patients included in our researchused left side for mastication that leads to higherfrequency on the left side contrary to previous researcheswhich showed bilateral occurrence in botharches.17Although the frequency and severity of dentalcaries has decreased substantially in the last two decades,this largely preventable disease is still common. Therate of decay increases significantly with age, and isstill a major public health problem.According to anotherresearch on bilateral occurrence of caries on firstpermanent molars,the caries frequency was same onboth sides in maxilla and mandible and no significantdifferences were found on the right and left side.An oral health survey of high school students conductedin Tibet, china (2013-2014) revealed that due to poororal health practice and unawareness of oral healthservices the caries frequency was 40%.18Such high cariesfrequency among Tibet population requiresimplementation of oral health promotions and healtheducation.14,19According to National Oral Health Survey
reports of 2004 caries frequency in India was 51.9%,53.8% and 63.1% at ages 5, 12 and 15 years respectivelyin different parts of India.In Pakistan the DMFT ratesreported by Oral Survey 2006, showed that the meanDMFT score for the age of 12 years was 1.38, for theage of 15 years was 1.94, for the age of 35-44 yearswas 8.02 & for the age of 65 years and above it was17.75. Other important finding of the Oral Health surveyPakistan 2006, included that more than 50% of thechildren between the ages of 12-18 years were cariesfree and on the negative side 97% of all carious lesionsin the same age group were untreated which is alsoevident in our study. For the age group of 35-44 year,half of the lesions were untreated while more than 90%of the treatment offered was extraction.Regarding the gender distribution, the present studyshowed that caries was present more in the males thenthe females as 179 males were affected and only 125females had the carious lesions on permanent mandibularright and left first molars. This is attributed to high maleto female ratio (3:2). Also females are more healthconscious and are very careful in terms of maintaininggood oral hygiene but a lot of previous studies haveshowed a greater caries ratio in females than males. Oneof the study demonstrated that caries rates are high inwomen than in men because of different factors likedifferent salivary composition and flow rate, hormonalfluctuations etc. and also some of the systemic diseasesassociated with caries have an association with femalegender.20According to another research caries assessmentbetween different age groups of males and femalesshowed no significant sex differentiation for ages between1-5 years and a same count of affected teeth was foundin adults (18-59 years). 21One of the research conductedin city of Zurich in 2008 have reported male gender asrisk factor for caries.22The study conducted among thechildren of kerala revealed that boys and girls are equallyaffected or with females slightly more affected .23Moreresearches are required to define sex disparities in dentalcaries across the population. Same is true for Pakistan.24,25
Healthy teeth formed the major component of this study,as in greater number of individuals there were no carieswhich shows that the examined individuals have a betterknowledge and awareness about oral hygiene practiceas affected individuals were only 304 (19.9%). Leastcontribution was of filled teeth probably because of lackof availability of dental services, poor socioeconomicstatus and high treatment cost.
CONCLUSION:Higher frequency of caries was found in left mandibularfirst molar compared to right mandibular molar withmales exhibiting higher rate than females. Regardingoral hygiene practice, the greater percentage of healthyteeth shows that the examined individuals have a betterknowledge and awareness about oral hygiene practiceas affected individuals were only 19.9%. Leastcontribution of filled teeth was probably because of lackof availability of dental services, poor socioeconomicstatus and high treatment cost, while those who require
JBUMDC 2016; 6(2): 106-109 Page-108
Frequency of Dental Caries and Status of Permanent Mandibular First Molar in Young Adults

treatment prefers extraction rather than restoration dueto possible drawbacks of unavailability of Dental servicesand non-affordability.
REFRENCES:1. Mitra DJ, Ashok KP, Dundappa J, Soni S, Ahmed S.
Oral hygiene-awareness and practice among patientsattending OPD at Vyas Dental College and Hospital,Jodhpur India J Indian Soc Periodontol 2012 ;16(4):524-8
2. Das D, Misra J,Mitra M, Bhattacharya B, Bagchi A.Prevalence of dental caries and treatment needs in chil-dren in coastal areas of West Bengal. ContemporaryClinical Dent 2013; 4(4): 482-7
3. Hamiss J, Ramezani GH, Ghodousi A. Prevalence ofdental caries among high school attendees in Qazvin,Iran. Journal of Indian Soc Pedod Prev Dent, 2008; 4:26-53
4. Soames JV, Southam JC. Oral pathology 1998 Jan;8:177-84
5. Narendar DN, Nisar N, Khan N, Syed S,Tanweer N.Prevalence and factors related to dental caries amongpre-school children of SaddarTown, Karachi, Pakistan:a cross sectional study. BMC Oral Health 2012;12:59-62
6. Baginska J, Rodakowska E, Milewski R, Kierklo A.Dental caries in primary and permanent molars in 7-8-year-old school children evaluated with Caries Assess-ment Spectrum and Treatment (CAST) index BMC OralHealth. 2014; 14: 74.Published online Jun 21, 2014.doi:10.1186/1472-6831-14-74
7. Riziwaguli A, Asiya Y, Liu Y, Yang R, Zou J. Cariesprevalence of the first permanent molar among 7-9 yearsold Uygur children in Urumqi, Xinjiang AutonomousRegion,2013;22(5):559-61
8. Liu L, Zhang Y, Wu W, Cheng M, Li Y, Cheng R. Preva-lence and Correlates of Dental Caries in an ElderlyPopulation in Northeast China. Tu Y-K, ed. PLoS ONE.2013;8(11):e78723
9. Ayyaz Ali Khan. Pakistan Oral Health Survey, SituationAnalysis, 2006, WHO
10. Sheiham A, Philip W, James T. A reappraisal of thequantitative relationship between sugar intake and dentalcaries: the need for new criteria for developing goalsfor sugar intake.BMC Public Health 2014; 14(1): 863.Published online 2014 September 16
11. Sadeghi M. Prevalence and bilateral occurrence of firstpermanent molar caries in 12-year-old students. Journalof dental research, dental clinics, dental prospects2007 ;1(2):86
12. Hou R, Mi Y, Xu Q, Wu F, Ma Y, Xue P et. al. Oralhealth survey and oral health questionnaire for highschool students in Tibet, China. Head Face Med 2014May 19;10:113-7
13. Ferraro M, Vieira AR. Explaining Gender Differencesin Caries: A MultifactorialApproach to a MultifactorialDisease, International Journal of Dentistry Volume 2010(2010),Article 649643, 5 pages
14. Rui Hou R, Yong Mi, Quanhog Xu, Fang Wu, YuanyuanMa, Peng X et. al. Oral Health survey & oral healthquestionnaire for high school students in Tibet, China,Published online May 12,2014
15. Jürgensen N, Petersen PE. Oral health behaviour ofurban and semi-urban school children in the Lao PDR.Community Dent Health 2011;28(4):280-5
16. Adeyemi BF, Kolude BM, Lawal AO. The knowledgeand experience of personal and professional oral careamong secondary school students in Ibadan. Odontostom-atol Trop 2012;35(137):5-11
17. Shaffer JR, Leslie EJ, Feingold E, Govil M, McNeilDW, Crout RJ, et, al.Caries experience differs betweenfemales and males across age groups in Northern Appa-lachia. International journal of dentistry 2015
18. Ueno M, Ohara S, Inoue M, Tsugane S, Kawaguchi Y.Association between education level and dentition statusin Japanese adults: Japan public health center-based oralhealth study. Community Dent Oral Epidemiol 2012;40(6):481-7. doi: 10.1111/j.1600-0528.2012.00697.x
19. Christensen LB, Petersen PE, Hede B. Oral health inchildren in Denmark under different public dental healthcare schemes. Community Dent Health 2010;27(2):94-101
20. Dengzhu C, Wang Y. Investigation and analysis on oralhygiene status and caries prevalence rate among 200Tibetan pupils in Lhasa Tibetan J Med 2008;29(2):6-7
21. Chandrashekar BR, Suma S, Kiran K, Manjunath BC.The use of school teachers to promote oral hygiene insome secondary schoolstudents at Hyderabad, AndhraPradesh, India: a short term prospective pilot study. JFamily Community Med 2012;19(3):184-9. doi: 10. 4103/2230-8229.102319
22. Menghini G, SteinerM, Thomet E, Roos M, Imfeld T,Caries prevalence in 2-year-old children in the city ofZurich. Community Dental Health 2008;25(3):154-60
23. Jose A, Joseph MR. Prevalence of dental health problemsamong school going children in rural Kerala. Journal ofthe Indian Society of Pedodontics and Preventive Dent-istry 2003; 21(4):147-51
24. Dawani N, Nisar N, Khan N, Syed S, Tanweer N.Prevalence and factors related to dental caries amongpre school children of Saddartown,Karachi,Pakistan:Across-sectional study.BMC Oral Health 2012;12(59)
25. Tariq N, Alam MA, Tahir S, Shahid U. Oral health know-ledge and practices among children 10-14 years attendingcricket summer camp.Pakistan journal of medical andhealth sciences 2012;6(4):992-4
JBUMDC 2016; 6(2): 106-109 Page-109
Syed Ahmed Omer1, Daud Mirza2, Isra Ahmed3, Omer Moosani4, Syed Muzzamil Ali Shah5

INTRODUCTION:Epilepsy is the most complex chronic and commonneuronal disorder throughout the world. InternationalLeague Against Epilepsy (ILAE) has defined Epilepsyas: "A transient occurrence of sign and or /symptomsdue to abnormal, excessive or synchronous neuronalactivity in the brain.1 Around the world about 50 millionpeople are suffering from epilepsy.2In Pakistanapproximately 1.4 million have been suffering fromEpilepsy.3 About 9.9 per 1000 of the general populationin Pakistan suffers from this disease.4 Epilepsy isgenerated when in brain groups of neurons undergoesprocess of epileptogenesis. The common causes ofepileptogenesis are genetics, neoplasm, abscesses, cysts,stroke, trauma, chronic degenerative diseases andinfections. The inhibitory and excitatory balance inneurons are adversely affected, the affects of inhibitory
neurotransmitters declines and the epileptogenic neuronsbecomes hyper excitable. Epileptic seizures are classifiedaccording to affected cortical areas of brain. Epilepticseizures are different from acute non-epileptic seizuressuch as, hypoglycemia, alcohol and narcotic withdrawal,poisonings, diabetic ketoacidosis and high grade fever.In these conditions the neurons are hyper excitable forlimited period of time and not permanent like in epilepticfoci. Genetic mutations are the common causes ofinherited epileptic syndromes.5These genetic mutationsmostly causes defective voltage gated channelopathies. 6-7 Thirty percent of the epileptic patients suffer frompharmacoresistant epilepsy.8These patients are mostdifficult to be treated as there are no specific drugregimens for their management. 9-10 Newer antiepilepticdrugs like GBP and a calcium channel blockers likeVerapamil both in randomized studies have shownantiepileptic effects to control resistant epilepsy.GBP(Gabapentin)is FDA approved AED for partial aswell as for generalized seizures. Gabapentin needed inhigher therapeutic doses for seizure control, however,the high doses are mostly tolerable and the drug ratedas tolerable and safe.11,12,13,14 While VP (Verapamil) isapproved for hypertension, angina and cardiacarrhythmias. In CNS it acts on L-type rapidly firingvoltage gated calcium channels and blocks T-type voltagegated calcium channels. Though VP is not FDA approveddrug for seizures, however, in some clinical randomizedtrials in pharmaco-resistant epilepsies it has givenantiseizure effects.15,16,17VP when used as adjunctivetherapy in patients of Pharmaco-resistance epilepsy hadsuccessfully controlled the seizures. It has beenestablished that VP has modulating effects on calcium
ORIGINAL ARTICLE
JBUMDC 2016; 6(2): 110-115 Page-110
ABSTRACT:Objective: To evaluate and compare in-vivo anticonvulsant effects of combined regimens of gabapentin and verapamil withtheir individual effects on kindled model of epilepsy in mice.Materials and Methods: This experimental study was carried out in H.E.J. Research Institute of Chemistry, InternationalCenter for Chemical and Biological Sciences, University of Karachi, from May 2009 to July 2011.Gabapentin (GBP) andVerapamil (VP) were used as tested drugs both as combined regimens as well as individual drugs, Phenytoin was used asreference drug. Kindling was produced by repeated administration of Pentylenetetrazole in a dose of 50 mg/kg by subcutaneousroute every 48 hours for 20 days. Three doses of Gabapentin from 100 mg/kg to 300 mg/kg and three doses of Verapamil from10 mg/kg to 30 mg/kg in combination regimens and individual drugs were administered by intraperitoneal route. Phenytoinwas administered by intraperitoneal route in a dose of 50 mg/kg. Gabapentin, Verapamil and Phenytoin were administered oncedaily, however, on the day of Pentylenetetrazole treatment, the tested and reference drugs were injected 40 minutes beforeinjecting Pentylenetetrazole.The anticonvulsive effects of combined regimens of tested drugs were compared to their individualeffects as well as to reference drug Phenytoin.Results:Combination regimens of GBP and VP demonstrated dose dependent anti- seizure effects up to 100%. The differentdoses of combined regimens of GBP and VP demonstrated anti-seizure effects which were superior to their individual effects.Conclusion:Combination regimens of gabapentin and verapamil showed synergistic effects which were superior to theirindividual effects on kindled model of epilepsy in mice.Keywords: Antiepileptic drugs, Phenytoin, Gabapentin, Verapamil , Pentylenetetrazole
Comparison of Anticonvulsant Effects of CombinedRegimens of Gabapentin and Verapamil
with their IndividualEffects
Itefaq Hussain Qureshi1, Shahbana Usman Simjee2
Dr. Itefaq Hussain QureshiAssistant ProfessorDepartment of PharmacologyLiaquat College of Medicine and DentistryKarachi.Email:[email protected]
Dr. Shahbana Usman SimjeeAssistant ProfessorH.E.J. Research Institute of ChemistryInternational Center for Chemical and Biological SciencesUniversity of KarachiKarachi.Received: 24-03-2016Revised: 13-04-2016Accepted: 27-04-2016

channels of CNS. 18-19Certain epilepsies are due to geneticmutations causing defective calcium channels withhyperactivities in neurons. 20-21 Pharmaco-resistantepilepsies are without any proper recommended FDAregimen. 22 VP can control such epilepsies.GBP and VPmay provide successful results as both are blockers ofcalcium channel. Hence both the drugs were employedin combination novel regimens keeping in mind theirsynergistic effects.23,24,25,26,27,28The present study wasdesigned to compare the effects of combined regimensof GBP/VP with their individual effects on kindledmodel of epilepsy in mice
MATERIALS AND METHODS:This experimental animal study was carried out inInternational Center for Chemical and BiologicalSciences, at Hussain Ebrahim Jamal (H.E.J.) ResearchInstitute of Chemistry, University of Karachi, Karachi.NMRI Albino mice with standard weight were used.The group size of 12 mice was used for standard statisticalanalyses.The use of animals in this Project was approvedby the Scientific Advisory Committee on Animal Care,Use, and Standards, International Center for Chemical& Biological Sciences, University of Karachi.GBP andVP anticonvulsive effects were studied by Internationallyrecognized chemically-Induced Kindled Model ofEpilepsy. Twenty alternate day administration of sub-convulsive dose of PTZ (50 mg/kg, s.c) was used toproduce kindling. The Kindling seizure scores wereclassified as outlined in Table 1 which is an internation-ally recognized kindling score.On 20th treatment daythe animals receiving PTZ which only showed the score4-5 were considered to be fully kindled. The effects ofthe tested drugs and reference drug on inhibiting thekindling/convulsions were recorded with reference tokindling scoring mentioned in Table 1. The tested drugsGBP and VP were given daily, however, on the day ofPTZ-treatment the drugs were administered 40 minutesbefore injecting PTZ. The animals were closely observedfor one hour on every day. Total duration of study wasforty days.Statistical Analysis:The statistical analysis wasperformed using Statistical Package for the SocialSciences (SPSS) version 10 and Graph Pad Prism.Results were reported as mean ±SEM. Data of seizureactivity was analyzed by non-parametric Student’s t-test and ANOVA statistical tests with post-hoc Dennett’smultiple comparison tests. The sequential differencesamong means were calculated at the level of p < 0.05.
RESULTS:It was observed that 100, 200 and 300 mg/kg doses ofGBP when used as a single agent therapy in PTZ-kindledanimals in a 20 day alternate day treatment elicited meanseizure scores of 3.08 ± 0.49, 2.66 ± 0.25 and 1.83 ±0.37 with seizure percentage of 62%, 53%, 37% andseizure safety or protection of 38%, 47% and 63 %respectively (Table 2).The effects were inferior toreference drug PHT. On the other hand, the treatmentof VP as a single agent therapy at the dose of 10, 20
and 30 mg/kg in 20 day alternate day treatment in kindledanimals exhibited mean seizure scores of 4.16 ± 0.37,3.91 ± 0.49, and 3.25 ± 0.43 with seizure percentageof 83%, 78%, 65% and seizure safety of 17%, 22% and35% respectively (Table 3).When GBP and VP were used as combination therapyin doses of 100: 10 mg/kg;200: 20 mg/kg; and 300:30mg/kg in kindled animals,the drugs elicited mean seizurescores of 2.91 ± 0.49, 2.25 ± 0.82 and 0.00 ± 0.00 withseizure percentage of 58%, 45%, 0.00% and seizureprotection of 41.8%, 55% and 100 % in three differentdoses regimens respectively(Table 4a).The maximumsynergistic action was seen in the groups receiving 300mg/kg GBP / 30 mg/kg VP with the mean seizure scoresof 0.00 0.0 with seizure percentage 0.00% and seizureprotection of 100% respectively. A significant differencei.e. p < 0.05 was observed i.e. the difference of 25 %,33 % and 65 % in seizure protection between these threecombined doses and VP treatment and difference ofalone was seen (Table 4b). When the same doses werecompared against GBP-treatment alone, difference of3 %, 8 % and 37 % in seizure protection was observed.The effects of maximum dose were found superior toPHT. The combination regimen at maximum dosageemployed was 10 percent more efficacious to PHT.Thus, we are inclined to hold that the combinationregimen of GBP and VP exhibited superior anti-epilepticactivity in terms of seizure protection capability comparedto their individual effects on same dosage with almostzero seizure score at the maximum dosage (100 %seizure inhibition) compared to their individual effects(Figure 1 )
JBUMDC 2016; 6(2): 110-115 Page-111
Itefaq Hussain Qureshi1, Shahbana Usman Simjee2
Table: 1Five distinct seizure patterns used for scoring of
kindling stages
Seizure Scoring inKindling by ptz012
34
5
Seizure Pattern No
ResponseEar and Facial Twitching
Convulsive Wave through thebody
Myoclonic JerksClonic-Tonic Convulsions,Turnover into Side PositionGerneralized Clonic-TonicSeizures, Loss of Postural
Control.
Figure 1
100%90%80%70%60%50%40%30%20%10%0%
Groups
Seizu
re P
rotec
tion%
VP10:PTZ50GBP100:PTZ50GBP100:VP10:PTZ50
100%
63%
35%
55%47%
22%
42%38%
1 7 %

JBUMDC 2016; 6(2): 110-115 Page-112
Table:2Effect of gabapentin treatment on the seizure score and seizure protection against PTZ-induced kindling
GroupID
GIGII
GIII
GIV
GV
GVI
Treatments
Normal ControlPTZGBPPTZGBPPTZGBPPTZPHTPTZ
Dosage(mg/kg)
Saline 0.9%501005020050300505050
Mean ± SEM ofSeizure Score
(20th treatment)(Seconds)
0.00
4.25 ± 0.59
3.08 ± 0.49
2.66 ± 0.25
1.83 ± 0.37
0.41 ± 0.19
SeizureScore (%)
0.00%
85%
61.6%
53.2%
36.6%
10%
SeizureProtection
(%)
0.00%
15%
38.4%
46.8%
63.4%
90%
Both the seizure score and seizure protection were calculated in % and the data is represented as a Mean SEM ofn = 12 animals per group
Table: 3Effect of verapamil treatment on the seizure score and seizure protection against PTZ-induced kindling
GroupID
GI
GII
GIIIGIV
GV
GVI
Treatments
NormalControl
PTZVPPTZVPPTZVPPTZVPTPTZ
Dosage(mg/kg)
0.9%Saline
5010502050305010050
Mean ± SEM ofSeizure Score
(20th treatment)0.00
4.25 ± 0.434.16 ± 0.37
3.91 ± 0.49
3.25 ± 0.43
0.5 ± 0.23
SeizureScore (%)
0.00%
85%83%
78%
65%
10%
SeizureProtection
(%)0.00%
15%17%
22%
35%
90%
Both the seizure score and seizure protection were calculated in % and the data is represented as a Mean SEM ofn = 12 animals per group.
Table: 4aSynergistic effect of gabapentin and verapamil treatment on the seizure score and seizure protection against
PTZ-induced kindling.
Both the seizure score and seizure protection were calculated in % and the data is represented as a Mean SEMof n = 12 animals per group.
GroupID
GI
GIIGIII
GIV
GV
GVI
Treatments
NormalControl
PTZGBP: VP
PTZGBP: VP
PTZGBP: VP
PTZPHTPTZ
Dosage(mg/kg)
0.9%Saline
50100: 10
50200: 20
50300: 30
505050
Mean ± SEM ofSeizure Score
(20th treatment)0.00
4.08 ± 0.64
2.91 ± 0.49
2.25 ±0.820.00
0.41 ± 0.19
SeizureScore (%)
0.00%
81.6%
58.2%
45%0%
8.2%
SeizureProtection (%)
0.00%
18.4%
41.8%
55%100%
91.8%
Comparison of Anticonvulsant Effects of combined Regimens of Gabapentin and Verapamil withtheir Individual Effects

DISCUSSION:We observed that GBP as a single therapy exhibitedmild to moderate anti-epileptic effects. The maximumanti-epileptic effects of GBP were seen at the doses of200-300 mg/kg where GBP demonstrated 47% and 63%seizure protection respectively. However, GBPdemonstrated mild anti-epileptic activities at the dosesof 100- 200 mg/kg and moderate anti-epileptic activitiesat the dose of 300 mg/kg. Likewise, VP demonstrateddose dependent anti-epileptic effects but those weremuch far inferior to GBP and were insignificant. TheVP treated group demonstrated 35% maximum seizureprotection at the maximum dose of 30 mg/kg. We are,therefore, inclined to hold that VP exhibits weakantiepileptic activity at lower doses and has no potentialto be used as a single agent for the treatment of epilepticseizures as an individual drug. Our data has shown thatnone of the doses of GBP and VP as individual treatmentregime demonstrated 100 percent seizure protection.When GBP and VP were used as combination therapyin three different doses in PTZ-kindled animals boththe drugs in combination regimens elicited seizureprotection of 41.8%, 55% and 100% respectively (Table4).The maximum synergistic action was seen in thegroups receiving 300 mg/kg GBP/30 mg/kg VP withthe mean seizure scores of 0.00 0.0 with seizurepercentage 0.00% and seizure protection of 100%respectively. A significant difference that is the differenceof 25%, 33% and 65% in seizure protection betweenthese three combined regimens and VP treatment alonewas seen. When the same combined regimens werecompared against GBP-treatment alone, a difference of3%, 8% and 37% in seizure protection was observed.Thus, we are inclined to hold that the combinationregimen of GBP and VP exhibited superior anti-epilepticactivity in terms of seizure protection capability comparedto their individual effects and reference drug PHT.Thecombination regimen exhibited almost zero seizure scoreat the maximum dosage (100% seizure inhibition)
compared to their individual effects. The P values andthe student’s t-test analysis exhibited significantdifference in combination regimens in first two dosesand with GBP alone, two initial doses but the mostsignificant effects were seen at the maximumcombination doses of GBP and VP where, 100 percentresults were achieved. (Table 5 and Figure 1) Wetherefore have found that the combination therapyexhibited synergistic effects up to 100 percent seizureprotection which cannot be achieved by individual higherdoses.The efficacy of new AED are still disappointing thoughit has provided more options for clinicians formanagement of epilepsy.29 Our study demonstrated thatanti-seizure actions of GBP can be augmented ormodified if given in combination with calcium channelblocker verapamil.30 GBP is a relatively safer drug inter-ms of its pharmacokinetics and dynamics profiles.31,32
GBP is a multipurpose drug and it has exhibited itsantiseizure effects in refractory epilepsy.33GBP has beenapproved recently by FDA as amonotherapy for partialand complex partial seizures with or without generalizedtonic-clonic seizures.34 GBP in various studies hasdemonstrated its efficacy as monotherapy equivalent tothat of carbamazepine (CMZ) for partial and generalizedseizures.35GBP has also established its efficacy inrefractory epilepsy, therefore the combination regimenwould have wider spectrum to treat various types ofepilepsies.GBP commonly is employed as an add-ontherapy for different types of Epilepsies.Our results has been supported by another animal studywhereby it was revealed that combinations of GBP withother AEDs generally results in synergistic interactions,though as an individual drug its anticonvulsive effectswere not significant. It was further observed in thesame study that GBP appeared to act synergisticallywith Carbamazepine, Valproate and Phenytoin. Thus,GBP has potential of synergistic action if used withother AED, keeping this idea in our mind, we conducted
JBUMDC 2016; 6(2): 110-115 Page-113
Itefaq Hussain Qureshi1, Shahbana Usman Simjee2
Table: 4bGBP and VP and their effects on kindled model of epilepsy when compared to
PTZ
TreatmentGroup
GBP:PTZGBP:PTZGBP:PTZVP:PTZVP:PTZVP:PTZGBP:VP:PTZGBP:VP:PTZGBP:VP:PTZ
Dose(mg/kg)
100 : 50200 : 50300 : 50
10:5020:5030:50
100:10:50200:20:50300:30:50
P value
0.00050.00010.00010.6330.1060.00010.00010.00010.00
Are MeansSignificantdifferent?p < 0.05
YESYESYESNONOYESYESYESYES
Differencebetween
the means
1.1671.4172.417
0.083 0.1720.333 0.1971.00 0.1841.33 0.2631.33 0.263
0
GBP, VP and GBP:VP vs. PTZ Control Group
Statistical analysis of data represented by P-values, means significant difference(p<0.05) and difference between the means of test drugs

the present study and used VP which is a calcium channelblocker. The purpose of using PHT reference drug wastwo fold firstly, PHT is not only approved for long termmanagement of different epilepsies but it is also reco-mmended for the long term management of status epil-epticus. Secondly, in another animal study it was observedthat GBP was more efficacious than PHT both inrefractory partial epilepsy and in PHT non responders.After the results of the present study we are inclined tohold that the regimens of GBP and VP would providebetter option for the use of these combina-tions regimenshaving synergistic effect for the treatment of typical andatypical epilepsies.
CONCLUSION:Combination regimens of GBP and VP providedsynergistic and effective therapeutic choice for thetreatment of epilepsies.The combination regimens ofGBP and VP has significant potential for different typesof epilepsies including resistant epilepsies because ofsynergistic and channel modulating effects.The mostsignificant point for future studies and trials is that whatwould be cut off dose of GBP and VP whereby both thedrugs would exhibit 100 percent seizure protection foruse in long term and short term management of epilepsiesand such query requires elaborate further animal as wellas clinical studies.
REFERENCES:1. W.H.O, IBE, ILAE. Global Campaign Against Epilepsy,
Atlas, 20052. Khatria A, Iannacconea ST, Ilyas MS, Abdullah BM,
Saleem S. Epidemiology of epilepsy in Pakistan: Reviewof literature. J Pak Med Assoc 2003; 53(12): 594-7
3. Sheerani M. Development of a comprehensive epilepsysurgery program in Pakistan. J. Pak. Med Assoc 2005;55(1):32-7
4. Annegers JF, Rocca WA, Hauser WA. Causes of epilepsy:contributions of the Rochester epidemiology project.Mayo ClinProc1996;71(6):570-5
5. Khosravani H, Zamponi GW. Voltage-gated calciumchannels and idiopathic generalized epilepsies. PhysiolRev, 2006;86(3): 941-66
6. Khosravani H, Altier C, Simms B, Hamming KS, SnutchTP, Mezeyova J et al. Gating effects of mutations in theCav3.2 T-type calcium channelassociated with childhoodabsence epilepsy. J Biol Chem 2004;279(11): 9681-4
7. Banerjee PN,Pilippi D, Allen Hauser WThe descriptiveepidemiology of epilepsy-a review. Epilepsy Res 2009;85:31-45
8. McTague A, Appleton R. Treatment of difficult epilepsy.Arch Dis Child 2011;96(2):200-4
9. Summers MA, Moore JL, McAuley JW. Use of verapamilas a potential P-glycoprotein inhibitor in a patient withrefractory epilepsy. Ann Pharmacother 2004;38(10):1631-4
10. Wahab A, Albus K, Gabriel S, Heinemann U. In searchof models of pharmaco-resistant epilepsy. Epilepsia2010;51(3): 154-9
11. Dichter MA. Innovative clinical trial designs for futureantiepileptic drugs.Epilepsia2007;48 (1): 26-30
12. Goa KL, Sorkin EM Gabapentin: A review of its pharm-acological properties and clinical potential in epilepsy.
Drugs1993;46(3):409-2713. Beydoun A, Fakhoury T, Nasreddine W, Abou-Khalil
B. Conversion to high dose gabapentin monotherapy inpatients with medically refractory partial epilepsy. Epile-psia 1998; 39(2):188-93
14. Gee NS, Brown JP, Dissanayake VU, Offord J, ThurlowR, Woodruff GN. The novel anticonvulsant drug, Gabap-entin (Neurontin), binds to the alpha2delta subunit of acalcium channel. J Biol Chem 1996; 271(10): 5768-76
15. Iannetti P, Parisi P, Spalice A, Ruggieri M, Zara F. Addi-tion of Verapamil in the treatment of severe myoclonicepilepsy in infancy. Epilepsy Res 2009; 85(1): 89-95
16. Iannetti P, Spalice A, Parisi P. Calcium-channel blockerVerapamil administration in prolonged and refractorystatus epilepticus. Epilepsia 2005;46(6): 967-9
17. Wurpel JN, Iyer SN. Calcium channel blockers verapamiland nimodipine inhibit kindling in adult and immaturerats. Epilepsia 1994;35: 443-9
18. Suman Yadav, Madhu G. Tapadia.NeurodegenerationCaused by Polyglutamine Expansion Is Regulated byP-Glycoprotein in Drosophila melanogaster Genetics,2013 195: 857-70
19. Giordanetto F, Knerr L, Wållberg A. T-type calciumchannels inhibitors: a patent review. Expert Opin TherPat 2011;21(1):85-101
20. Fletcher CF, Lutz CM, O'Sullivan TN, Shaughnessy JDJr, Hawkes R, Frankel WN et al.Absence epilepsy intottering mutant mice is associated with calcium channeldefects. Cell 1996;87(4): 607-7
21. Lerche H, Jurkat-Rott K, Lehmann-Horn F. Ion channelsand epilepsy. Am J Med Genet 2001;106: 146–59.
22. Nicholas AS, Dlugos DJ. Treatment of refractory statusepilepticus: literature review and a proposed protocol.Pediatric neurology 2008;38(6): 377-90
23. Stefani A, Spadoni F, Bernardi G. Gabapentin inhibitscalcium currents in isolated rat brain neurons. Neurophar-macol1998;37(1): 83-9
24. Kwan P, Sills GJ, Brodie MJ. The mechanisms of actionof commonly used antiepileptic drugs. PharmacolTher2001; 90(1): 21-34
25. Macdonald RL, Kelly KM. Mechanisms of action ofcurrently prescribed and newly developed antiepilepticdrugs. Epilepsia 1994;35 (4):S41-S50
26. Macdonald RL, Kelly KM. Antiepileptic drug mechani-sms of action. Epilepsia 1995;36 (2):S2-S12
27. Mulley JC, Scheffer IE, Petrou S, Berkovic SF. Channe-lopathies as a genetic cause of epilepsy. Curr Opin Neu-rol 2003;16(2): 171-6.
28. Stephen, Linda J, Martin J. Brodie. Pharmacotherapyof epilepsy. CNS drugs 2011;25(2): 89-107
29. Glauser T, Ben-Menachem E, Bourgeois B, Cnaan A,Chadwick D, Guerreiro C, et al.ILAE treatment guide-lines: evidence-based analysis of antiepileptic drug effi-cacy and effectiveness as initial monotherapy for epilepticseizures and syndromes. Epilepsia 2006;47(7): 1094-1120
30. Graeme SJ. The mechanisms of action of gabapentinand pregabalin. Current opinion in pharmacology 2006;6(1): 108-13
31. Steve WH. Comparative anticonvulsant and mechanisticprofile of the established and newer antiepileptic drugs.Epilepsia 1999;40(5): S2-S10
32. Beydoun A, Fakhoury T, Nasreddine W, Abou-KhalilB. Conversion to high dose gabapentin monotherapy inpatients with medically refractory partial epilepsy. Epilep-sia 1998;39(2):188-93
JBUMDC 2016; 6(2): 110-115 Page-114
Comparison of Anticonvulsant Effects of combined Regimens of Gabapentin and Verapamil withtheir Individual Effects

33. Gracia-Fleta F, Medrano-Martínez V, Castaño-PérezMD, Hernández-Lorido R, Mañes R. Gabapentin in 50patients with epilepsy .Revista de neurologia 2000;32(1):45-9
34. Eugene R R. Advances in the pharmacotherapy of epi-
lepsy. Epilepsia1993;34(5): S9-S1635. Chadwick, DW. A double-blind trial of gabapentin mon-
otherapy for newly diagnosed partial seizures. Neurology1998;51(5): 1282-8
JBUMDC 2016; 6(2): 110-115 Page-115
Itefaq Hussain Qureshi1, Shahbana Usman Simjee2

INTRODUCTION:Pakistan is the sixth most populous country in the worldwith an estimated population of 184.5 million. In 1951,Pakistan ranked as the 14th most populous country witha population of about 32.5 million, since then thepopulation has increased approximately 5.5 fold. Thecurrent population growth rate is 1.7 percent. It isestimated that with this rate of population growth,
Pakistan will become fifth most populous country in2050.1 This scenario presents a picture that could bedevastating for the country where 61% of its populationis living below US$2 a day.2 Such a high growth rate isa matter of serious concern for country’s economystability, health, environment and food security.According to WHO, family planning is defined as “away of thinking and living that is adopted voluntarily,upon the basis of knowledge, attitude and responsibledecisions by individuals and couples, in order to promotethe health and welfare of family group and thus contributeeffectively to the social development of a country.”3InPakistan, Family planning program was launched in theprivate sector in 1953 and in the public sector in 1960with the aim to stabilize the rapidly expanding population.Despite of all these efforts of Government of Pakistan,population control is still a debatable issue.4Familyplanning is considered as one of the four pillars of safemotherhood program for reducing high maternalmortality in developing countries.5Neglect of this sectorhas contributed to Pakistan’s failure in achieving itsMillennium Developmental Goal (MDGs) 3, 4 and 5.6Ithas been estimated that approximately 28,000 womendie annually in Pakistan due to preventable pregnancy-related complications.1
Contraception, which has been documented to be themost effective process that can improve maternal healthby reducing fertility and ensuring healthy timing andspacing of birth in a country.7Healthy timing and spacingof pregnancy (HTSP)8is a family planning interventionthat delays pregnancy by lengthening the inter-pregnancyinterval.It deals with healthy spacing between thesuccessive pregnancies for healthier outcomes forneonate, infant and child.9Contraceptive prevalence rate(CPR) is defined as the percentage of married women,aged 15-49 years, using modern and traditional methods
ORIGINAL ARTICLE
JBUMDC 2016; 6(2): 116-120 Page-116
ABSTRACT:Objective:To explore knowledge, attitudes and practices regarding contraceptive use in females and to determine the sociocultural barriers that influence contraceptive uptake and contribute to significant unmet needs of family planning.Materials and Methods:This hospital based cross sectional survey was carried out from March 2015 to September 2015 atthe Gynaecology and Obstetrics outpatient clinics (OPD) of two hospitals of Karachi, Liaquat National Hospital and PNS SHIFAHospital. 383 females of age 18-49 years were enrolled after taking informed written consent. Knowledge, attitude and practiceson contraception were evaluated with the help of predesigned questionnaire.Results: Mean age of participants was 30.12+ 3.05, youngest being 18 years old, while the eldest was 49 years old. Majority(64%) of the participants were housewives.Knowledge about contraceptive methods was found in 97.1%. Media was foundto be main source of information. Regarding contraceptive practices, 48% women were currently using some method ofcontraception. Among these the most widely used method was condoms (46%). 52% women were not currently using anymethod of contraception. Husband and mother in law opposition were found to be the strongest reason for not using anycontraception.Conclusion:Inspite of having good knowledge, utilization of contraceptives were less because of preference for a large familynorm, religious myths, cultural barriers and family oppositionKeywords:Socio- cultural determinants, Contraceptive use, Married females, Urban areas, Karachi
Socio Cultural Determinants of Low Contraceptive Useand High Unmet Needs in Married Females of Urban
KarachiKhaula Noreen1, Nadia Khalid2, Imran Shaikh3,Tahira Zamir4,Marium Shoaib5
Azka Shahab6, Aisha Siddiqua7, Osama Rehman8
Dr. Khaula NoreenLecturerDepartment of Community Health Sciences,Bahria University Medical and Dental CollegeKarachiEmail:[email protected]
Dr. Nadia KhalidLecturerDepartment of Community Health SciencesBahria University Medical and Dental CollegeKarachi
Dr. Imran ShaikhProfessor and HeadDepartment of Community Health SciencesBahria University Medical and Dental CollegeKarachi
Dr. Tahira ZamirAssistant ProfessorDepartment of PharmacologyBahria University Medical and Dental CollegeKarachi
Marium Shoaib, Azka Shahab,Aisha Siddiqua, Osama Rehman
4th year MBBS studentsBahria University Medical and Dental CollegeKarachiReceived: 28-03-2016Revised: 14-04-2016Accepted: 21-04-2016

of contraception.1In Pakistan, contraceptive prevalencewas 24% in the 1996-97.10Pakistan’s statistics given byUnited Nation’s Population Fund(UNFPA) in 2002showed total contraceptive prevalence rate of 28% andof modern methods as 20%.11
According to Pakistan Demographic and HealthSurvey(PDHS), 2012-13, contraceptive prevalence rateswere 35 percent. 26 percent women were using modernmethods, and traditional methods were used by 9 percentof married women while if we compare it with CPR ofneighboring countries,they have achieved almost doubleCPR with 56% in India, 58% in Bangladesh.12This studyaims to explore knowledge, attitudes and practicesconcerning family planning and birth spacing; healthseeking behavior; community need assessment; andvarious socio-cultural barriers that influence contraceptiveuptake and thus contributing to significant unmet needsof family planning.
MATERIALS AND METHODS:This hospital based cross sectional survey was carriedout from March 2015 to September 2015 at theGynaecology and Obstetrics outpatient clinics (OPD)of two hospitals of Karachi that is Liaquat NationalHospital and PNS SHIFA Hospital. Study participantswere enrolled by non-probability, convenient samplingmethod.Sample size was calculated by taking theprevalence of contraceptive usage as 35%1, margin oferror 5%. Estimated sample size was 349. By adding10% for non response, sample size came out to be383.Inclusion criteria included married women of age18-49 years, attending the OPD either as patients ortheir attendants. Exclusion criteria included unmarried,postmenopausal, diseased, infertile women or thoseunwilling to take part in the research study.Interviews were conducted after obtaining an informedconsent. A structured questionnaire designed in the locallanguages was used to obtain information on socio-demographic features, reproductive profile, contraceptivepractices, availability and accessibility of family planningservices. Reasons for non-utilization of contraceptiveservices were also asked from the respondents. The datawas entered and analyzed on SPSS version 21. Chi-square test was applied where necessary for significancetesting.
RESULTS:Mean age of participants was 30.12+ 3.05, youngestbeing 18 years old, while the oldest was 49 years old.Majority (63%) of the participants were housewiveswhile 36% were working women (Table 1). Knowledgeabout contraceptive methods was found in 97.1%. Oninquiring about the sources of knowledge regardingdifferent contraceptive methods, media was found to bemain source of information (Figure 1). Knowledge,attitude and practices regarding contraceptive use arementioned in Table 2a, 2b & 2c. 52% women were notcurrently using any method of contraception. The mostcommon reason was found to be family opposition fromboth husband and mother in law (Table 2b).Regarding
contraceptive practices, 48% women said that they arecurrently using some method of contraception. Amongthese, the most widely used method was condoms (46%)(Table 2c). On finding association of socio demographicfactors with contraceptive practices, female and husbandeducation was found to be strongly associated withcontraceptive practices in couples (Table 3).
JBUMDC 2016; 6(2): 116-120 Page-117
Khaula Noreen1, Nadia Khalid2, Imran Shaikh3,Tahira Zamir4,Marium Shoaib5 Azka Shahab6, Aisha Siddiqua7, Osama Rehman8
Table: 1Socio demographic profile of study participants
VariableAge of respondent(years)<2021-3031-4041-50
OccupationHousewifeEmployed
Education status of(female)respondentIlliterateBelow MatricMatricIntermediateGraduationMastersPost graduation
Family StructureNuclearJoint
Monthly income<20,00020,000 -50,000>50,000
Education status of(spouse)husbandIlliterateBelow MatricMatricIntermediateGraduationMastersPost graduation
n= 357
861079866
225132
68714649455523
225133
10198159
18515649757830
Percentage (%)
2429.927.418.4
6336.9
1919.812.813.712.615.46.4
6337.2
28.227.444.5
514.215.613.721
21.884
Figure: 1Source of knowledge about contraception
806040200
Med
ia
Family
Faiend
s
Health
...
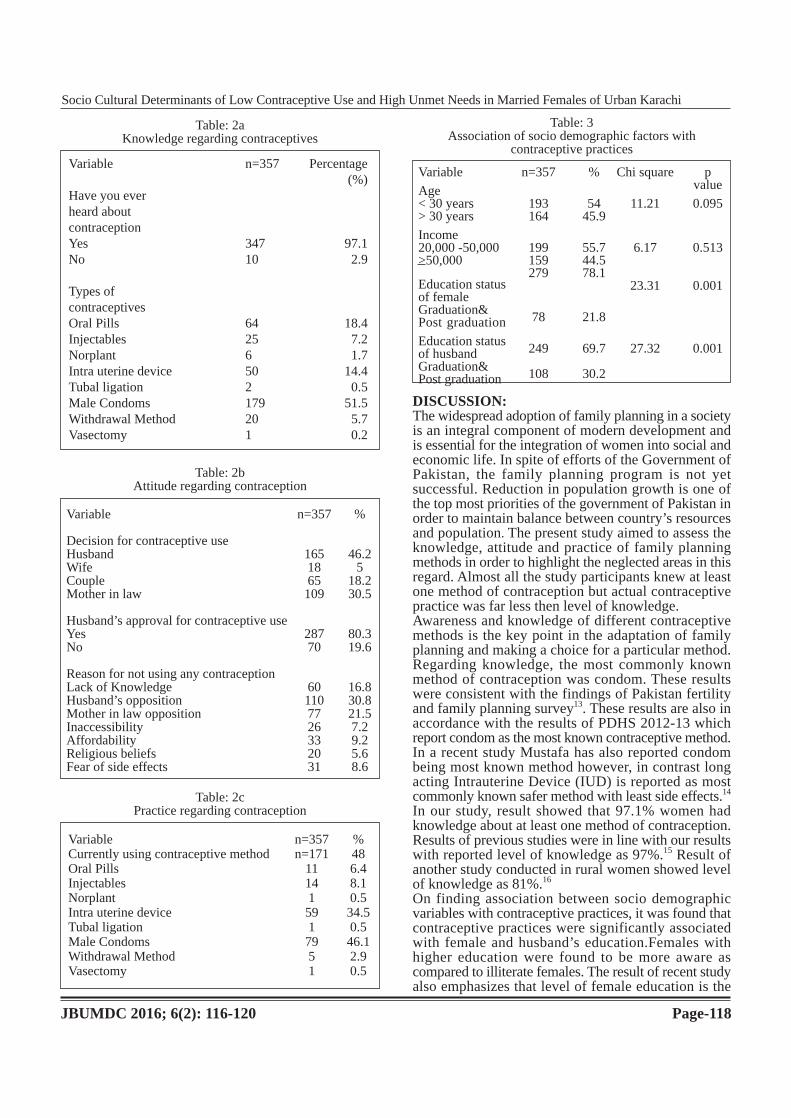
DISCUSSION:The widespread adoption of family planning in a societyis an integral component of modern development andis essential for the integration of women into social andeconomic life. In spite of efforts of the Government ofPakistan, the family planning program is not yetsuccessful. Reduction in population growth is one ofthe top most priorities of the government of Pakistan inorder to maintain balance between country’s resourcesand population. The present study aimed to assess theknowledge, attitude and practice of family planningmethods in order to highlight the neglected areas in thisregard. Almost all the study participants knew at leastone method of contraception but actual contraceptivepractice was far less then level of knowledge.Awareness and knowledge of different contraceptivemethods is the key point in the adaptation of familyplanning and making a choice for a particular method.Regarding knowledge, the most commonly knownmethod of contraception was condom. These resultswere consistent with the findings of Pakistan fertilityand family planning survey13. These results are also inaccordance with the results of PDHS 2012-13 whichreport condom as the most known contraceptive method.In a recent study Mustafa has also reported condombeing most known method however, in contrast longacting Intrauterine Device (IUD) is reported as mostcommonly known safer method with least side effects.14
In our study, result showed that 97.1% women hadknowledge about at least one method of contraception.Results of previous studies were in line with our resultswith reported level of knowledge as 97%.15 Result ofanother study conducted in rural women showed levelof knowledge as 81%.16
On finding association between socio demographicvariables with contraceptive practices, it was found thatcontraceptive practices were significantly associatedwith female and husband’s education.Females withhigher education were found to be more aware ascompared to illiterate females. The result of recent studyalso emphasizes that level of female education is the
JBUMDC 2016; 6(2): 116-120 Page-118
Socio Cultural Determinants of Low Contraceptive Use and High Unmet Needs in Married Females of Urban Karachi
Table: 2aKnowledge regarding contraceptives
Variable
Have you everheard aboutcontraceptionYesNo
Types ofcontraceptivesOral PillsInjectablesNorplantIntra uterine deviceTubal ligationMale CondomsWithdrawal MethodVasectomy
n=357 Percentage(%)
347 97.110 2.9
64 18.425 7.26 1.750 14.42 0.5179 51.520 5.71 0.2
Table: 2bAttitude regarding contraception
Variable
Decision for contraceptive useHusbandWifeCoupleMother in law
Husband’s approval for contraceptive useYesNo
Reason for not using any contraceptionLack of KnowledgeHusband’s oppositionMother in law oppositionInaccessibilityAffordabilityReligious beliefsFear of side effects
n=357
1651865109
28770
601107726332031
%
46.25
18.230.5
80.319.6
16.830.821.57.29.25.68.6
Table: 2cPractice regarding contraception
VariableCurrently using contraceptive methodOral PillsInjectablesNorplantIntra uterine deviceTubal ligationMale CondomsWithdrawal MethodVasectomy
n=357n=171
111415917951
%486.48.10.534.50.546.12.90.5
Table: 3Association of socio demographic factors with
contraceptive practices
Variable
Age< 30 years> 30 years
Income20,000 -50,000>50,000
Education statusof femaleGraduation&Post graduation
Education statusof husbandGraduation&Post graduation
n=357
193164
199159279
78
249
108
%
5445.9
55.744.578.1
21.8
69.7
30.2
Chi square
11.21
6.17
23.31
27.32
pvalue
0.095
0.513
0.001
0.001

key element that affects the knowledge regardingcontraception.17Moreover, improving the female educa-tion status can be an effective strategy that can be helpfulin combating the problem of overpopulation by increasingthe contraceptive usage in our country. The ContraceptivePrevalence Rate (CPR)1is the most widely employedand valuable measure of the success of family planningprograms. The Contraceptive Prevalence Rate (CPR) isinversely associated with Total Fertility Rate (TFR).The decline in TFR could be more substantial if thereis a greater use of contraceptives in the country. Femaleliteracy cannot only improve the level of knowledgebut also enhance the decision making power regardingthe contraceptive usage.This evidence is also proved byprevious studies.18, 19
This trend is also evident from Pakistan National Demo-graphic and Health survey 2012-13, TFR decreasesconsis-tently from 4.4 among women with no educationto 2.5 among women with a higher education.Factorsassociated with better education are higher status ofwomen, better access to health and family planninginformation and services and later marriage.1
Different sources can impart the knowledge of familyplanning methods. Factor responsible for enhancingknowledge includes exposure of messages throughmedia, discussion with family, friends and health careprovider. In present study media contributed to 72%,followed by family 41% then 39% attributed to discussionwith friends and 15% of knowledge is provided byhealth care provider. This shows that electronic mediacan play an effective role in creating awareness regardingcontrace-ptivese specially in developing countries likeours where illiteracy is high. Moreover, there is easyaccessibility of this source to a wide range of population.These results were also in line with previous studies,where main source of knowledge was media whichcontributed (64.1%) but in another study, on contraryto our results health personnel provide (20.9%) andfriends and family circle impart (14.8%) knowledge forcontraception.16 Fikree has stated that women were morereceptive when messages of family planning weredelivered through media.20
Our study showed that 80% of husbands had authorityregarding decision of contraceptive usage. The resultof our study are similar to a previous survey conductedon reproductive goals and family planning17 whichshowed that male has an authority in decision regardingfamily size and fertility outcome. Most probable reasonfor large family size is that a male wants to be economi-cally strong by having large family size. These findingsare consistent with PDHS 2012-131, which also demon-strated that males are more in favour of large familysize as compared to females and percentage of jointdecision making was very low while spouse (husband)decision is considered as influential in deciding thechoice of contraceptive method as well as size of family.Several studies have highlighted the impact of varioussocio cultural factors on contraceptive knowledge andpractices in Pakistan.21, 22
In addition, dynamics of decision making between
couples is also greatly influenced by interference ofmother in law. Mother in law opposition in our studywas found to be 21%. Previous studies have alsohighlighted that in our culture, mother in law isconsidered to be in a position that strongly affectsdecision-making spheres. This inhibits a couple to makechoices about their family size as well as familyplanning.23This is due to a high level of illiteracy andunderprivileged status of females in our society. Severalresearches have supported that females do not practicefamily planning without their husbands and mothers-in-law approval. This is the most pivotal restriction tocope within Pakistan which is at times linked withsociocultural and health issues.24, 25
Study findings also draw attention to other factorscontributing significantly to unmet needs of familyplanning. These factors include affordability, accessibility,fear of side effects, economic constraint and mostimportantly religious beliefs and taboos. Religiousconstraints and restriction to practice family planningis an important impediment to contraceptive use in manyother Islamic countries also.26, 27Such findings are alsodocumented in national representative survey ofPakistan.1These factors contribute to significant unmetneeds for family planning. According to Pakistandemographic and health survey 2012-13, 20% of curre-ntly married women have an unmet need for familyplanning, 9% have an unmet need for spacing, and 11%have an unmet need for limiting births.1These are mainissues behind the failure of family planning program inPakistan. If all these factors contributing to significantunmet needs are effectively addressed and all currentlymarried women who want to space or limit their childrenwill become able to use family planning methods, theCPR can be increase to 56 percent.27Our study fairlyhighlighted the reasons behind the unmet need and lowcontraceptive prevalence rate in Pakistanbut resultscannot be generalized as it may not represent the truepicture of the general population of Pakistan. In orderto enhance generalizibility, further representative studiesare needed with large sample size especially involvingwomen from underprivileged and underserved areas ofcountry.
CONCLUSION:Inspite of having good knowledge, utilization ofcontraceptives were found to be less because of largefamily norm, religious myth, cultural barriers and familyopposition. Number of females actually using contra-ceptives was almost half of those having knowledgeabout contraceptives.Suggestions:As family planning is a component of four pillars ofSafe Motherhood Initiative, promotion of contraceptiveusage should be a major tenet in improving maternaland child health as a public health agenda. Females withunmet needs for family planning services should bedealt on priority basis. Sociocultural issues includinghusband opposition, cultural taboos, in laws opposition,low esteem of female in our society, myths and health
JBUMDC 2016; 6(2): 116-120 Page-119
Khaula Noreen1, Nadia Khalid2, Imran Shaikh3,Tahira Zamir4,Marium Shoaib5 Azka Shahab6, Aisha Siddiqua7, Osama Rehman8

issues which are a barrier in the way of contraceptiveusage should be addressed on priority. Intensified mediacampaigns in regional languages, continuous supply ofcommodities to enhance the affordability and accessibilityissues can prove to be an effective strategy in reducingthe significant unmet needsof family planning.There isa dire need of integration of all concerned stake holdersincluding both public and private health care sectorsand health education to integrate and make effectivestrategies to halt this problem. Training of communityhealth workers is essential with an aim to achieve max-imum benefit with cost effectiveness.
REFERENCES:1. National Institute of Population Studies (NIPS) and ICF
International, Pakistan Demographic and Health Survey2012-13, National Institute of Population Studies (NIPS),Islamabad, Pakistan; ICF International, Calverton, Md,USA, 2013
2. Population Reference Bureau, “World Population DataSheet,” 2013.http://www.prb.org/Publications/Datasheets/2012/world-population-data-sheet.aspx
3. K. Park. Chapter 9. In: K. Park, eds. Text Book of Preve-ntive & Social Medicine. 21st ed. Jabalpur: BanarsidasBhanot; 2011:445
4. Khan AA, Khan A, Javed W, Hamza HB, Orakzai M,Ansari A et al. Family planning in Pakistan: applyingwhat we have learned. Journal of the Pakistan MedicalAssociation 2013;63:3-10
5. Ahmed S, Li Q, Liu L, Tsui AO. Maternal deaths avertedby contraceptive use: an analysis of 172 countries. TheLancet 2012;380(9837):111-25
6. Cleland J, Bernstein S, Ezeh A, Faundes A, Glasier A,Innis J. Family planning: the unfinished agenda. TheLancet. 2006;368(9549):1810-27
7. Stover J, Ross J. How increased contraceptive use hasreduced maternal mortality. Maternal and Child HealthJournal 2010;14(5): 687-95
8. Marston C, Report of WHO Technical Consultation onBirth Spacing, World Health Organization, Geneva, Swi-tzerland, 2005
9. Cleland J, Conde-Agudelo A, Peterson H, Ross J, TsuiA. Contraception and health. The Lancet 2012;380 (9837):149-56
10. National Institute of Population Studies. Pakistan fertilityand family planning survey 1996-1997. Islamabad: TheInstitute 1998
11. UNFPA worldwide. Population, health and socio econom-ic indicators/policy developments. Overview Pakistan:keystatistics 2002. Available from: http://www.unfpa.org/profile/pakistan.cfm
12. USAID worldwide. Population, health and socioeconomi-cindicators/policy developments. Overview Pakistan:keystatistics 2012. Available from:
http://www.uSAID.org/profile/pakistan.cfm13. Hakim A, Cleland J, Bhatti M. Main Report, Pakistan
fertility and family planning survey 1996 - 1997, Dec1998
14. MustafaG,KhurramAS, Hameed W, Ali S, Ishaque M,Hussain W et al. Family Planning Knowledge, Attitudes,and Practices among Married Men and Women in RuralAreas of Pakistan: Findings from a Qualitative NeedAssessment Study. International Journal of ReproductiveMedicine2015
15. Ayub A, Kibria Z, Khan F. Assessment of Knowledge,Attitude and Contraceptive use in Married Women ofPeshawar. Journal of Dow University of Health Sciences2015;9(1):1-2
16. Mustafa R, Afreen U, Hashmi HA. Contraceptive know-ledge, attitude and practice among rural women. J CollPhysicians Surg Pak 2008;18(9):542-5
17. Mahmood N. Reproductive goals and family planningattitudes in Pakistan: A couple-level analysis. The PakDevelop Review 1998; 37: 19-34
18. Saleem S, Bobak M. Women's autonomy, education andcontraception use in Pakistan: a national study. Reprodu-ctive health. 2005;2(8):1-8
19. Pazol K, Zapata LB, Tregear SJ, Mautone-Smith N, Ga-vin LE. Impact of contraceptive education on contrace-ptive knowledge and decision making: a systematic rev-iew. American journal of preventive medicine. 2015;49(2):46-56
20. Fikree FF, Khan A, Kadir MM, Sajan F, Rahbar MH.Whatinfluences contraceptive use among young womenin urbansquatter settlements of Karachi, Pakistan? IntFam Plann Perspect 2001; 27:130-6
21. Ali M, Ushijima H. Perceptions of men on role of relig-ious leaders in reproductive health issues in rural Pakistan.J Biosoc Sci. 2005;37(1): 115-22
22. Pasha O, Fikree FF, Vermund S. Determinants of unmetneed for family planning in squatter settlements in Kar-achi, Pakistan. Asia-Pacific Population Journal 2001;16(2):93-108
23. Kadir MM, Fikree F, KhanA,Sajan F. Do mothers-in-law matter? Family dynamics and fertility decision-making in urban squatter settlements of Karachi, Pakistan.Journal of Biosocial Science, 2003;35(4):545-58
24. Salem RM, Bemstein J, Sullivan T M,Lamde R. Commu-nication for Better Health. Population Reports, JohnsHopkins Bloomberg School of Public Health, Baltimore,Md, USA, 2008
25. Mir AM., Shaikh, GR. Islam and family planning: chan-ging perceptions of health care providers and medicalfaculty in Pakistan. Global Health, Science and Practice2013;1(2): 228-36
26. Nuruzzaman H. Unmet need for contraceptive: the caseof married adolescent women in Bangladesh. Internatio-nal Journal of Current Research 2010; 9:29-35
27. Raza H, Sheraz A, Zafar R, Khan N, Ali H. Effect ofIslamic perception on family planning practices. OIDAIntJ Sust Dev 2012;5(3): 85-96
JBUMDC 2016; 6(2): 116-120 Page-120
Socio Cultural Determinants of Low Contraceptive Use and High Unmet Needs in Married Females of Urban Karachi

COMMENTARY
JBUMDC 2016; 6(2): 121-123 Page-121
ABSTRACT:Spinal cord infarction is one such disease which is quite uncommon and often goes undetected because of variation in its onset,severity, duration and presentation. Spinal cord is supplied by anterior and posterior spinal arteries.Around three quarters ofblood supply to spinal cord is derived from anterior spinal artery. Mostly Spinal Cord Syndrome is due to vascular compromisepathologically or due to any iatrogenic insult. Spinal cord stroke, either ischemic or hemorrhagic presents abruptly over fewminutes to several hours with severe back pain along with bilateral weakness or paralysis depending upon the site and severityof lesion. Aspirin is standard treatment along with low-dose heparin administered subcutaneously, and physiotherapy to improvemotor function. Various factors like patient health, age and condition of the disease might influence clinical evolution andfunctional outcome. Weakness or paralysis may improve as time passes especially in those where complete infarction did notoccur.Keywords: Spinal cord infarction, Limb weakness, Vascular compromise, Variable presentation, Aspirin, Physiotherapy
INTRODUCTION:Spinal cord infarction is one such disease which is quiteuncommon and often goes undetected because ofvariation in its onset, severity, duration and presentation.It has been pointed out that its incidence is 1.2% ofhospital admissions related to vascular pathology of thenervous system.1
Background of the Disease:To explain the disease ‘Spinal Cord Syndrome’ weshould keep arterial supply of the spinal cord in mind.Spinal cord is supplied by three major vessels; there isone anterior spinal artery(ASA) and 2 posterior spinalarteries (PSAs). Majorly (around three quarters) theblood supply to the spinal cord is derived from theanterior spinal artery. Thus the anterior portion of thecord is much more vulnerable to vascular compromise,typically presenting as an anterior cord syndrome affec-ting corticospinal, lateral spinothalamic, and autonomicpathways.2
Pathogenesis and the Vascular supply of the SpinalCord:The ASA supplies the anterior two-thirds of the spinalcord and PSAs supply the posterior one-third. The ASAis formed at the level of foramen magnum by intracranialvertebral arteries and receive branches at different levelsfrom radicular branches of aorta. The ASA and PSAsanastomose distally at the conus medullaris.3 Anypathology arising within aorta or in its branches canlead to ischemia or infarction of spinal cord with symp-toms corresponding to the level of cord.2
Chief Causes of the Spinal Cord Syndrome:Mostly Spinal Cord Syndrome is due to vascular comp-romise pathologically or due to any iatrogenic insult,commonly local space occupying lesions compressinganterior spinal artery (such as granulomas, abscesses,tuberculoma, neoplasms, sarcoidosis etc), generalizedatherosclerosis, Coronary artery diseases,hyperlipidemia,hypercoagulable states, systemic hypotension or hypovo-lemia, vascular malformations, surgery of aortic aneur-ysm, aortic dissection, any risk factor of thrombo-embol-ism such as atrial myxoma, atrial fibrillation, infectiveendocarditis, thrombocytosis etc. Any local or systemicfactor compromising the perfusion of spinal cord canbe the culprit.4,5,6
Non Vascular Causes of the Spinal Cord Syndrome:Anterior spinal artery syndrome (ASAS) is a rare neurol-ogic complication characterized by the sudden develop-ment of paraplegia, unusual complication of epiduralanalgesia used to facilitate postoperative pain relief.Itcan be transient or persistent, with variably preservedsensory perception due to limited blood flow throughthe anterior spinal artery.7,8
Also, there exists some literature that the pathogenesisof the spinal cord syndrome is associated particularlyto cervical spondolysis, cervical spondylotic myelopathy,due to compression or may be while its correctiveapproach.9,10
Spectrum of the Disease Presentation:Spinal cord stroke, either ischemic or hemorrhagic prese-nts abruptly over few minutes to several hours withsevere back pain along with bilateral weakness or paraly-sis depending upon the site and severity of lesion. Overhours to days, few or all of the following symptomsmay also present in any sequence:1. weakness or paralysis involving either all 4 limbs
or lower limbs bilaterally depending upon the siteof infarct
2. sensory loss distal to the lesion with relative sparingof light touch, proprioception and vibration if onlyanterior spinal artery is involved
3. flaccidity in acute phase followed by spasticity4. numbness or paraesthesia5. loss of deep tendon reflexes acutely, followed by
hyper-reflexia
Spinal Cord Stroke: An Uncommon Diagnosis behindCommon Symptoms!!
Anoshia Afzal1, Maria Shoaib2
Dr. Anoshia AfzalDow Medical CollegeDow University of Health SciencesKarachiE-mail: [email protected]
Dr. Maria ShoaibDow Medical CollegeDow University of Health SciencesKarachiReceived: 01-03-2016Revised: 16-03-2016Accepted: 19-03-2016
6. hypotension7. sexual dysfunction8. bowel or bladder dysfunction9. there may be chest pain or abdominal pain prior to
the onset of weakness or paralysis if the initiatingevent was myocardial ischemia or gut ischemia11,12,13
Making Diagnosis of the Spinal Cord Syndrome:Once the presentation seems enough to be diagnosed asspinal cord stroke, an immediate spinal MRI should bedone which will reveal the site and nature of lesionalong with any mass lesion if present.Following is thelist of workup to be done in patients having spinal cordstroke to identify the etiology behind it:14
1. CT myelography to rule out mass lesion2. Spinal arteriography to detect vascular lesions or
malformations3. Spinal fluid analysis to rule out infections, neoplasm
or other inflammatory disorders4. CT guided biopsy or culture may be helpful in
some cases5. Temporal artery biopsy if giant cell arteritis is to
be ruled out6. Blood complete picture along with inflammatory
markers to rule out systemic vasculitis or chronicinflammatory conditions
7. Lipid profile8. Auto immune profile9. Electromyography (EMG)and nerve conduction
velocity (NCV) to differentiate it from other disor-ders with same presentation such as transverse my-elitis, Guillain-Barre Syndrome (GBS) and spaceoccupying lesions in the cord
Treatment and Management of the Disease:There is no definite therapy for spinal cord infarction,once it occurred, all we can do is to prevent further isc-hemia, minimize the complications and reduce disabilitythrough rehabilitation. Aspirin is the standard treatmentalong with low-dose heparin administered subcutane-ously, and physiotherapy to improve motor function.Only symptomatic treatment is all that can be offeredat this time like spasticity can be treated with oralbaclofen, tizanidine, and occasionally diazepam. Usuallylong term stay in a rehabilitation hospital is requiredsince the neurologic disabilities are either permanent orslowly resolving. Other comorbidities such as diabetesmellitus, hyperlipidemia, hypertension or heart diseasesshould be strictly controlled and treated. Weakness orparalysis may improve as time passes especially in thosewhere complete infarction did not occur.2,14
Prognosis and the Counseling Points:Spinal Cord Syndrome’s prognosis has not been compl-etely determined since, given its low frequency, thepublished series are of few cases. Various factors suchas a patient health, age and condition of the diseasemight influence their clinical evolution and functionaloutcome.Acute spinal cord ischemia is a serious diseasewhose functional outcome are disabling in a high perce-ntage of patients. Best predictor of the prognosis is anadvanced age. In Spinal Cord Infarct clinical (mostsensitive are the ASIA motor scores) and electrophysi-
ological (tibial SSEP) examinations are of prognosticvalue to predict the functional recovery and thus allowearly planning of rehabilitation aims and procedures.13
Patient should be counseled and educated properlyregarding the prognosis and outcome of the situationdue to its high morbidity and disability. Patient shouldbe advised to control risk factors and remain compliantto the medications in order to get improvement insymptoms. Sphincter disturbance is an important sequelin the whole neurological syndrome, issues of bladderand bowel control should be specially addressed. Patientsshould be offered rehabilitation care and their familiesshould also be counseled for playing a supportive role.1
CONCLUSION:Many patients present with bilateral lower limb weaknessprogressing slowly over many days but none of themare suspected to be suffering from spinal cord ischemia.While many patients remain undiagnosed or left againstmedical advice (LAMA) owing to any reason, it ishighly possible that any of them suffered from spinalcord ischemia which is a catastrophic event with anabrupt onset and variable symptoms depending on thesite involved. Hence we emphasize on physicianknowledge to pick this unusual diagnosis presentingwith common neurological symptoms.In future we hopethat like many other neurological disorders where definiteinterventions are yet to be known, Spinal Cord Syndromeis also one of the challenging frontiers that needexploration in future years.
REFERENCES:1. De la Barrera SS, Barca-Buyo A, Montoto-Marques A,
Ferreiro-Velasco ME, Cidoncha-Dans M, Rodriguez-Sotillo A. Spinal cord infarction: prognosis and recoveryin a series of 36 patients. Spinal cord 2001;39(10):520-5
2. Lynch K, Oster J,Apetauerova D ,Hreib K. Spinal CordStroke: Acute Imaging and Intervention.Case Reportsin Neurological Medicine, Volume 2012 (2012), ArticleID 706780, 3 pages, doi:10.1155/2012/706780
3. Hurst RW. Spinal vascular disorders. In: ResonanceImaging of the Brain and Spine, 2nd, Atlas SW (Ed),Lippincott, Philadelphia 2006. p.1387
4. Hughes JT, Brownell B. Spinal cord ischemia due toarteriosclerosis. Archives of neurology. 1966;15(2):189-202
5. Singh U, Silver JR, Welply NC. Hypotensive infarctionof the spinal cord. Spinal Cord. 1994 ;32(5):314-22
6. Thomas NJ, Harvey AT. Paraplegia after coronary bypassoperations: relationship to severe hypertension andvascular disease. The Journal of thoracic and cardiovasc-ular surgery 1999;117(4):834-6
7. Martirosyan NL, Feuerstein JS, Theodore N, CavalcantiDD, Spetzler RF, Preul MC. Blood supply and vascularreactivity of the spinal cord under normal and pathologicalconditions: A review. Journal of Neurosurgery: Spine.2011;15(3):238-51
8. Richman JM, Wu CL. Epidural analgesia for postopera-tive pain. Anesthesiology Clinics of North America2005;23(1):125-40
9. Nurjck S. The pathogenesis of the spinal cord disorder
JBUMDC 2016; 6(2): 121-123 Page-122
Anoshia Afzal1, Maria Shoaib2

associated with cervical spondylosis. Brain1972;95(1):87-100
10. Ebersold MJ, Pare MC, Quast LM. Surgical treatmentfor cervical spondylitic myelopathy. Journal of neurosurg-ery 1995;82(5):745-51
11. Foo D, Rossier AB. Anterior spinal artery syndrome andits natural history. Paraplegia 1983; 21:1.
12. Cheshire WP, Santos CC, Massey EW, Howard JF Jr.Spinal cord infarction: etiology and outcome. Neurology1996; 47:321
13. Mohr JP, Benavente O, Barnett HJ. Spinal Cord Ischemia.
In: Stroke Pathophysiology, Diagnosis, and Management,Barnett HJ, Mohr JP, Stein BM, Yatsu FM (Eds),Churchill Livingstone, Philadelphia 1998. p.423.http://emedicine.medscape.com/article/1164217-clinical#showall
14. Iseli E, Cavigelli A, Dietz V, Curt A. Prognosis andrecovery in ischaemic and traumatic spinal cord injury:clinical and electrophysiological evaluation. Journal ofNeurology, Neurosurgery & Psychiatry. 1999 ;67(5):567-71
JBUMDC 2016; 6(2): 121-123 Page-123
Spinal Cord Stroke: An Uncommon Diagnosis behind Common Symptoms!!

JBUMDC 2016; 6(2): 124-126 Page-124
Cultural day was organized in Bahria University Medical& Dental College (BUMDC) on 8th February, 2016.Students guided by the faculty, participated in organizingthe cultural day celebration to highlight the importanceof traditions related to different ethnicities of Pakistanwith emphasis on unity.Cultural day events started inthe afternoon around 2 pm in the grand campusauditorium. Honorable Director General BUMDC ViceAdmiral (Retd) Tahseen ullah Khan HI (M) and Principaldental Section Prof. Zubair Ahmed Abbasi were thechief guests.The auditorium too was decorated accordingto the theme and presented an atruistic view. All thestudents and faculty were dressed in colorful culturalattires and were a joy to look at. Quite appropriately theevent started with an instrumental note of Nationalanthem by a group of students which was electrifyingand received a standing ovation from the audience.The anthem was followed by a marvelous medley songsung by five students dressed in cultural apparelrepresenting the national theme of four provinces ofPakistan. The cultural songs were heartwarming andaudiences cheered with all their heart. The epitome ofthis performance was when the performers sang thepatriotic song “SOHNI DHARTI ALLAH RAKHAY”together. It was definitely a fitting end to the medley asit embodied the unity of our nation proud of theirindividual culture but together for each other in thename of this Sohni Dharti Pakistan.The medley was followed by the Declamation contestwhich was delivered both in Urdu and in English. Theparticipants put forward their opinion on whether“BASANT”; the spring festival celebrated primarily byKite flying; should be condemned considering the death
toll during kite flying annually or celebrated as a nationaltradition as it has been going on since ages. Argumentsfrom both sides were flawlessly delivered, eachsupporting their school of thought with out of the boxreasoning. Although everyone did a splendid job butonly 2 students could be awarded, one being WardahZainab (English) and the other was Zeenat Junaid (Urdu).In contrast to the heavy thoughts of declamation contesta singing performance was followed which includedamazing vocals of Sana Safdar, Aqib Javed, AbdulMalik and Nimra. All the singers delivered spell boundingperformances on folk songs from different cultureincluding Jugni, Qarara Rasha, Danay pay Dana, Sufipoetry by Shah Latif. Thought provoking poetry, soultouching melodies and powerful vocals were enhancedby great string work on guitar by Abdul Hadi. All theperformances received applause and cheers from theaudiences.As soon as the singers left the stage students dressed inrural get up start rolling in with “charpai ” and all otherkind of props. So the stage was all set for a short palywhich were produced and performed by students ofDrama and Art society. The whole play revolved aroundthe stereotypical behavior of parents from differentcultural backgrounds considering education, marriageby self-choice or mingling with the people of othercultures as taboo. The crescendo for the play was whena person belonging to Kashmiri background, asked allthe other culture people that why are you fighting fordominance? This is not what we are struggling for inKashmir. Kashmiris are fighting for the Pakistan whichwas the vision of Quaid- e -Azam, a united and proudPakistan in which every ethnicity and religion maintainedits identity freely but was united and harmonious witheach other.The somber message from the play was shaken by thegreatest aspiring vocals of Guest Music Band lead singerWaqar and spell bounding performance of his colleagueon sitar. Sitar being the symbol of south Asian culturewas never played this beautifully at least in BUMDCpremises. Sitar segment was indeed the most melodiousmoment of the event.The highlight of the afternoon came from the mostsurprising dimension. It was a Gilgit Baltistan folk danceperformance by the duo Fahmeed and Hassan and itwas mind blowing. As the song of Gilgit Baltistan,which was played prior to the performance said, “Mohtajkahan-pehchan k hain, ham Gilgit Baltistan k hain”.This folk dance performance and the performancejust swept all of the audience from their feet.Lastly a singing competition which was candidly namedas Bahria Idol was held which had 6 competitors. And
STUDENTS CORNER
Cultural Day Celebrations atBahria University Medical & Dental College
ReportSara Abbassi1,Tahira Zamir2, Hasan Ali3
Sara Abbassi4th year MBBS studentBahria University Medical and Dental CollegeKarachiE-mail: [email protected]
Dr. Tahira ZamirAssistant ProfessorDepartment of PharmacologyBahria University Medical and Dental CollegeKarachi
Dr. Hasan AliProfessor and HeadDepartment of BiochemistryBahria University Medical and Dental CollegeKarachiReceived: 23-03-2016Revised: 05-04-2016Accepted: 07-04-2016

JBUMDC 2016; 6(2): 124-126 Page-125
Sara Abbassi1,Tahira Zamir2, Hasan Ali3
what a treat for ears it was. But as all competitions weredealt, winner was only one so Amina Javed bagged thetitle of Bahria Idol this time. Shields were awarded tothe winners by the Honorable Director General BUMDCVice Admiral (Retd) Tahseen ullah Khan HI (M).With indoor event coming to the end focus was movedto the outdoor events.The parking ground of BUMDC was temporarily madeinto a rural “Mela” like environm-ent. There were stallsfor food representing different cultures and games andhandicraft from all the provinces. Stall from Sindh wasdecorated with “Ralli ”and “Ajrak” and a variety ofembroided clothes. Live “makkai di roti” and “sarsonda saag” was getting served at Punjab stall. KPK boastedthe appetites from traditional “Chai and Paratha ” and“Chapli kebab”. Balochistan stall was colorfully decora-
ted with handicrafts and artifacts from the region. Andhow can the national gastronomical sensation “Biryani”,“Gol Gappa”, “Kulfi” be forgotten. More urban tastebuds were satisfied by a steady supply of pizza andshawarma.The event concluded, although with a heavy heart, ataround 11 pm. The whole day was filled with festivities,patriotism, and unity and how can we forget pure funand joy. Without a doubt the event was a smashingsuccess and it would not have been possible without thededication and hard work of the faculty and the studentswho took time out of the most hectic schedule of medicaland dental education and played there part in makingthis event a success hence paving the way for manyothers to come.
Sindh Stall Balochistan Stall
KPK Stall Punjab Stall

JBUMDC 2016; 6(2): 124-126 Page-126
Cultural Day Celebrations at Bahria University Medical & Dental College Report
Skit Presentation Folk Dance Gilgit Baltistan
Melody Performance Games Stall
Debate Competition Singing Competition

JBUMDC 2016; 6(2): 127-129 Page-127
ABSTRACT:Brenner tumors of ovary are relatively uncommon neoplasms and constitute about 1.4-2.5% of all tumors of ovary. Most ofthese tumors present as an incidental finding either on gross examination of ovary or as a microscopic finding. They are classifiedin surface epithelial tumors of ovary. We report here a case of a 50 year old woman who presented to the gynecology andobstetrics department of Jinnah Post Graduate Medical Center, Karachi, Pakistan. The presenting complaints were irregularand heavy per vaginal bleeding for a few months. Total abdominal hysterectomy and bilateral salpingo-oophorectomy wasperformed and the specimen was received at the department of Pathology, Basic Medical Sciences Institute (BMSI), JPMC,Karachi. The microscopic examination of left ovary revealed benign Brenner tumor composed of well demarcated nests ofuniform transitional cells.Keywords: Ovarian neoplasm, Brenner tumor, Transitional cell tumor, Incidental finding
INTRODUCTION:Brenner tumors are uncommon ovarian neoplasms andconstitute about 1.4-2.5% of all tumors of ovary.1 Theaverage age of presentation is 50 years with 70% ofthese are diagnosed in over 40 years of age group.2 Mostof them are incidentally found.3 They are classified inthe surface epithelial tumors of ovary.4,5 It is hypothesizedthat transitional epithelia of these tumors arise frommetaplasia of ovarian surface epithelium. Majority ofthe neoplasms are benign however they can also presentwith borderline or malignant morphology and clinicalcourse.
CASE REPORT:A 50 year old woman presented to the Gynecology andObstetrics outpatient department, Jinnah Post Graduate
Medical Center, Karachi with the presenting complaintsof irregular and heavy bleeding for a few months.Clinically adenomyosis was suspected. Hystrectomyand bilateral Salpingo-oophorectomy was performedand the specimen was sent to the department ofPathology, Basic Medical Sciences Institute (BMSI),Jinnah Post Graduate Medical Center, Karachi.On gross examination the cut surface of uterus showedan uncircumscribed gray white area in the myometriummeasuring 6x5x3cm. Left ovary was slightly larger thanthe right measuring 3.2x1.0x0.6 cm. Cut surface of bothovaries were unremarkable. No firm circumscribed graywhite or cystic areas were seen in the left ovary.Microscopically the left ovary revealed multiple welldemarcated solid nests of uniform transitional cellsexhibiting oval nuclei, prominent cell borders, eosinop-hilic cytoplasm and occasional small basophilic nucleoli.Some nuclei had longitudinal grooves exhibiting coffeebean appearance. The tumor nests were surrounded bydense fibrous stroma (Figure 1).
No papillary projections or cellular atypia was identified.Microscopically the tumor size was 1.2x1.1 cm. Theright ovary and both fallopian tubes were histologicallyunremarkable. The whitish area of myometrium showedmultiple foci of adenomyosis.Immunohistochemical stains were performed and
CASE REPORT
An Incidental Finding of Ovarian Brenner TumorNazish Jaffar1, Noshaba Rahat2, Saroona Haroon3, Syed Mehmood Hasan4
Dr. Nazish JaffarAssistant ProfessorDepartment of PathologySindh Medical CollegeJinnah Sindh Medical UniversityKarachi.Email:[email protected]
Dr. Noshaba RahatAssistant ProfessorDepartment of of PathologyBasic Medical Sciences InstituteJinnah Post Graduate Medical CenterKarachi.
Dr. Saroona HaroonConsultant HistopathologistDepartment of of HistopathologyPrince Faisal Cancer CentreKing Fahad Specialist HospitalBuraidahKingdom of Saudi Arabia (KSA).
Dr. Syed Mehmood HasanProfessorDepartment of PathologySindh Medical CollegeJinnah Sindh Medical UniversityKarachi.Received: 20-04-2016Revised: 04-05-2016Accepted: 06-05-2016
Figure: 1
H&E 40x. Nest of uniform transitional cells exhibiting oval nuclei,prominent cell borders & eosinophilic cytoplasm. Some nuclei havelongitudinal grooves exhibiting coffee bean appearance

Cytokeratin 7 and cytokeratin 20 were applied.Cytokeratin 7 revealed diffuse and strong positivity(Figure2) while cytokeratin 20 was negative.
DISCUSSION:Benner tumors of ovary were first explained in 1907 byFritz Brenner.1 Majority of Brenner tumors are inciden-tally found either during surgery or pathological examina-tion, where the ovaries are excised for other reasons.Most of the Brenner tumors are benign, however border-line and malignant forms although rare, have been repor-ted.2,3
Various theories exist regarding the origin of Brennertumor. Some suggest that it arises either from heterotopicwolffian epithelium, or from multipotential ovariancoelomic epithelial cells. Other studies propose theirorigin from urothelium or transitional metaplasia ofepithelial inclusion cyst. Theories suggesting Walthardcell nests as the precursor of Brenner tumor are alsopresent. The most widely accepted theory regarding theorigin of Brenner tumor is that they are derived fromthe multipotential coelomic epithelium of the ovarywhich undergoes transitional metaplasia. The coelomicepithelial cells can be found either on surface or onepithelial inclusion cysts.4,5
Most Brenner tumors are asymptomatic however someof them can produce symptoms of abnormal vaginalbleeding, pelvic pain and a palpable pelvic mass. In ourcase the patient presented with complaints of heavy andirregular vaginal bleeding since few months but it wasdue to concomitant adenomyosis.Macroscopically benign tumors are well circumscribedtumors with a gray white or slightly yellow cutsurface.Most of the Brenner tumors are small in sizeusually measure less than 4.5cm The largest benignBrenner tumor in literature, however has been reportedto be 39 cm. Borderline tumors are usually cystic witheither unilocular or multilocular presentation. Malignanttumors may be cystic or solid.6,7,8,9,10 In the present casethe effected left ovary was slightly larger in size thanthe left , however the cut surface was unremarkable. No
solid or cystic areas were identified. Imaging techniqueslike ultrasonography, CT and MRI are usually non-specific to diagnose Brenner tumor. Benign tumorscomposed uniformly of solid component in imagingstudies are mostly similar to fibroma, thecoma or leio-myoma.11,12 In the present case no information wasprovided regarding the imaging diagnostics of the patient.Microscopically Benign Brenner tumors are composedof sharply demarcated small nests of transitional cellswithin fibromatous stroma. The cells are uniform in sizewith promin-ent cell borders and eosinophilic cytoplasm.The nuclei are oval and some have longitudinal grooves.Calcifications are commonly seen in the stroma.Borderline Brenner tumors show complexity of architec-ture in the form of papillary projections within the dilatedcystic spaces. Cytologic atypia is moderate comprisingof atypical nuclei with dense chromatin, prominentnucleoli and conspicuous mitotic figures. Stromalinvasion is not seen. Malignant Brenner tumor displayinvasion into the stroma.In comparison to benign tumors,stroma in malignant Brenner tumors is sparse.2,8,9 In thepresent case the tumor displayed the typical morphologyof benign Brenner tumor. The left ovary revealed multiplewell demarcated solid nests of uniform transitional cellssurrounded by dense fibrous stroma. Some nuclei showedlongitudinal grooves. No papillary projections or cellularatypia was noted. The right ovary and both fallopiantubes were unremarkable.Most immunohistochemical studies show cytokeratin7positivity and cytokeratin 20 negativity in Brenner tumorbe it benign, borderline or malignant. Other studiesreveal uroplakin III positivity in benign Brenner tumorwhich also shows positive immune reaction in Walthardcell nests sugges-ting a link between the origin of Brennertumor and Walthard cell nests. 1,9
In the present case we used cytokeratin 7 and cytokeratin20 immune markers. The cytokeratin 7 showed strongand diffuse positivity in tumor cell nests while cytokeratin20 was negative.Treatment of choice for benign Brenner tumor is unilate-ral oophorectomy. Complete surgical resection is thecure in majority of the cases of benign Brenner tumorsince they are well circumscribed and easy to locate.Benign Brenner tumor presents with good prognosis.Borderline Brenner tumors also have favorable prognosisand thus they may also be treated by complete surgicalresection. However malignant tumors may affect thesurrounding tissue and they may also metastasize intonearby structures, their treatment may require furtherintervention in addition to complete surgical resection.2,4,8
In some cases hystrectomy specimens received alongwith oophorectomy specimens demonstrated othergynecologic pathologies including leiomyoma;adenomyosis, adenomatous endometrial polyp andWalthard cell rest.1 In the present case foci of adeno-myosis were present.Brenner tumors have also beenrarely reported in association with pregnancy. 4 Reviewof literature also reveals 7 reported cases of Brennertumor and Struma ovarii coexisting in the same ovarianneoplasm.6
JBUMDC 2016; 6(2): 127-129 Page-128
Nazish Jaffar1, Noshaba Rahat2, Saroona Haroon3, Syed Mehmood Hasan4
Figure: 2
40x. Immune marker cytokeratin 7 showing diffuse and strongpositivity in Brenner cell element

JBUMDC 2016; 6(2): 127-129 Page-129
CONCLUSION:In the present case benign Brenner tumor of left ovarywas an incidental finding. The tumor nests revealedstrong and diffuse positivity with immune markercytokeratin. A diligent gross and microscopic examinationis required so as not to miss the diagnosis. Surgical treat-ment has been found to be curative in benign Brennertumors.
REFERENCES:1. Kondi-Pafiti A, Kairi-Vassilatou E, Iavazzo C, Vouza
E, Mavrigiannaki P, Kleanthis C et al. Clinicopathologicalfeatures and immunoprofile of 30 cases of Brenner ova-rian tumors. Arch Gynecol & Obstet 2012; 285:1699-702
2. Borah T, Mahanta RK, Bora BD, Saikia S. Brennertumor of ovary: An incidental finding. J Midlife Health.2011; 2(1): 40-1
3. Vukmirovic F, Vukmirovic IT, Vukmirovic M. Clinico-pathological features of ovarian Brenner tumors in Mont-enegro. Cent Eur J Med. 2013; 8(2):146-8
4. Gedikbasi A, Ulker V, Aydin O, Akyol A, NumanogluC, Ceylan Y. Brenner tumor in pregnancy: Clinical app-roach and pathological findings. J Obstet Gynaecol Res2008; 35:565-8
5. Roma AA, Masand RP. Ovarian Brenner tumors andWalthard nests: a histologic and immunohistochemicalstudy. J human path.2014. doi:10.1016/j.humpath 2014.08.003
6. Terada T, Tateoka K. Ovarian cystic tumor composedof Brenner tumor and struma ovarii. Int J Clin Exp Path-ol 2012; 5(3): 274-7
7. Kurman RJ , Shih LM. The origin and pathogenesis ofepithelial ovarian cancer- a proposed unifying theory.Am J Surg Pathol 2010; 34(3):433-43. doi:10.1097/PAS.0b013e3181cf3d79
8. Ruggiero S, Ripetti V. Binachi A, Vaccara VL, AlloniR, Coppola R. A singular observation of a giant benignBrenner tumor of the ovary. Arch Gynecol Obstet 2011;284(2): 513-6: doi:10.1007/s00404-011-1930-x. Epub2011 May 19
9. Ali RH, Seidman JD, Luk M, Kalloger S, Gilks CB.Transitional cell carcinoma of the ovary is related tohigh-grade serous carcinoma and is distinct from mali-gnant brenner tumor. Int J Gynecol Pathol 2012; 31(6):499-106
10. Zaidi S, Trimeche M, Hammedi F, Hidar S, Sriha B,Mestiri S. Bilateral proliferating Brenner tumor of theovary associated with recurrent urothelial carcinoma ofthe urinary bladder. N Am J Med Sci 2010; 2(1): 39-41
11. Arnogiannaki N, Grigoriadis C, Zygouris D, TerzakisE, Sebastiadou M, Tserkezoglou A. Proliferative Brennertumor of the ovary. Clinicopathological study of twocases and review of the literature. Eur J Gynaecol Oncol2011; 32(5):576-8
12. Wang XY, Dai JR, Zhu Z, Zhao YF, Zhou CW. CT feat-ures of ovarian Brenner tumor and a report of 9 cases.Chinese Journal of Oncology. 2010; 35(2):359-62
An Incidental Finding of Ovarian Brenner Tumor

To,The editor,
The human genomic project describes a greater similarityin human gene sequences which unites us as specie butthe minor allelic variations in terms of single nucleotidepolymorphism makes every individual unique.1 Thisreveals an insight into the role of human genetic variationbehind differential susceptibility of human diseases andresponse to pharmacological agents. They also act asan environmental factor in producing varied diseasephenotypes more than other factors like patient`s age,gender or body weight. This compels to the idea ofPersonalized Medicine as an emerging therapeuticscience.2 The name Personalized Medicine suggests anexclusive treatment strategy based on individual genomicinfo. It is aimed to comprehensively identify genomicdifferences and correlate with human diseases likemalignant tumors and inherited disorders. It is alsohelpful in further research of genetic risk factors,polygenic variations and also as an important tumormarker or diagnostic tool. Application of Pharmacog-enomics, pharmacokinetics and pharmacoproteomicsare its basic principles.3
Hereditary factors interplay with genetic and environme-ntal factors for many diseases. Carcinomas and tumors,cardiovascular abnormalities like long QT syndrome,myocardial infarction, auto immune pathology, co-morbids like hypertension, diabetes and other geneticdisorders have proven multi-factorial etiology. Theadvances in Personalized Medicine will revolutionizeuse of genomics for identification of molecular tumormarkers, prognostic assessment, disease screening andmonitoring of treatment plan. Physicians may eventuallybe able to perform optimal interventions for patients’condition and genetically informed clinical trial.Moreover, the healthy population can also get aware oftheir inherited disease risk factors and can live cautiouslife ahead.4Ethical implication lies while compiling the
genomic sequences, further there would be the risk ofracial or personal discrimination. Still gettingcomprehensive knowledge of the personalized genomeis a big hurdle as information should be obtainedefficiently with routine analysis and in a cost effectiveway. For this, medical genetics and its medical andethical perspectives should be a part of education andcapital investment for research advances and applicationwhich is the need of time.1In clinical practice,personalized medication may bring real progress inhealth care and treatment modalities. Collaboratingacademic experts, medical personnel and public sectorcan make it a reality and a therapeutic miracle. ThusPersonalized Medicine is really opening up a newgenomic era where possibilities of better treatments andeven finding a cure can become even closer. Moreoverwe could be able to identify a person’s risk factorsextremely early in their life and even prevent some ofthese diseases from developing.5
REFERENCES:1. Lee C, Morton CC. Structural genomic variation and
personalized medicine. New England Journal ofMedicine. 2008;358(7):740-1
2. Agrawal S, Khan F. Human genetic variation and perso-nalized medicine. Indian J Physiol Pharmacol. 2007;51(1):7-28
3. Hamburg MA, Collins FS. The path to personalizedmedicine. New England Journal of Medicine 2010;363(4):301-4
4. Guttmacher AE, Collins FS. Welcome to the genomicera. New England Journal of Medicine 2003;349(10):996-8
5. Samadi D. Conquering Cancer: Personalized MedicineIs the Future. www.huffingtonpost.com conquering-cancer-personalized-medicine.Updated Jun 19, 2015.www.twitter.com/drdavidsamadi
JBUMDC 2016; 6(2): 130 Page-130
LETTER TO EDITOR
Personalized Medicine- A New Genomic EraMaria Shoaib
Dr. Maria ShoaibDow Medical CollegeDow University of Health ScienceEmail: [email protected]: 08-02-2016Accepted: 14-02-2016

The Journal of Bahria University Medical and Dental Collegeabbreviated as JBUMDC is a peer reviewed biannual multidis-ciplinary biomedical journal of basic and clinical healthsciences.It accepts manuscripts prepared in accordance withthe “Uniform Requirements for Submission of Manuscriptsfor Biomedical Journals, updated October 2008”, adopted byInternational Committee of Medical Journal Editors (ICMJE).& PMDC guidelines for medical & Dental journals ,TheJournal will encompass manuscripts from all fields ofbiomedical sciences in the form ofEditorial (Invited),OriginalArticle, Review Article,Short Communication (Commentary),Case report and Letter to editor.Peer Review Policy:Every paper will be read by the editor. Selected papers willbe sent to two reviewers .If statistical analysis is includedexamination by the staff statistician will be carried out.Plagiarism:JBUMDC follows the ICMJE, PMDC and HEC guidelinesfor plagiarism.Preparation of Manuscript:Type the manuscript on ISO A4 (212 × 297 mm), with marginsof at least 25 mm (1 inch). Type or print on only one side ofthe paper. Use double spacing throughout the manuscript.Start each section on new page.Number pages consecutively,beginning with the title page. Put the page number in thelower right-hand corner of each page.Contents of Manuscript for submission:Submission items include a Covering letter, Letter of undertak-ing duly signed by all authors,Title page and the Manuscript(Abstract,Key words,Introduction, Materials & Methods,Results, discussion, conclusion, acknowledgement, Authorship,Conflict of interest, References, Tables , Figures).Title pageshould have complete title of the manuscript, the names ofall authors with qualifications, their department ,affiliation,telephone number,e-mail, corresponding author ,address forcorrespondence, short running title,source of funding (grant/equipment/drugs), number of figures and tables, total wordcount, total number of pages.1. AbstractIt should have no more than 150 words for unstructuredabstracts or 250 words for structured abstracts. The abstractshould state the purpose of the study(objective), basicprocedures (materials & methods with study design,subjects/animals, place & duration of study, drug/chemical/equipment, procedure or protocol), main findings (results)and conclusion. It should emphasize new and importantaspects of the study.Below the abstract provide, 3-10 keywords that will assist indexers in cross-indexing the articleand may be published with the abstract.2. IntroductionState the purpose of the article and summarize the rationalefor the study. Give only strictly pertinent references and donot include data or conclusions from the work being reported.3. Materials &MethodsDescribe your selection of the observational or experimentalsubjects (patients or laboratory animals, including controls)clearly. Identify the age, sex, and other important characteristicsof the subjects. Identify the methods, apparatus (give themanufacturer's name and address in parentheses), andprocedures in sufficient detail to allow other workers toreproduce the results.. Identify precisely all drugs and chemicalsused, including generic name(s), dose(s), and route(s) ofadministration.For randomized clinical trials provideinformation on all major study elements, including the protocol
(study population, interventions or exposures, outcomes, andthe rationale for statistical analysis), assignment of interventions(methods of randomization, concealment of allocation totreatment groups), and the method of masking (blinding).Authors submitting review manuscripts should include asection describing the methods used for locating, selecting,extracting, and synthesizing data. These methods should alsobe summarized in the abstract.All studies must be approvedby the relevant Ethics Committee/ Institution Review Boardof the respective institutions.4. ResultsPresent your results in logical sequence in the text, tables,and illustrations. Do not repeat in the text all the data in thetables or illustrations; emphasize or summarize only importantobservations. Describe appropriate indicators of measurementerror or uncertaintysuch as confidence intervals, P values.Report complications of treatment & dropouts from a clinicaltrial. Specify any general-use computer programs employedfor analysis.5. Discussion & ConclusionEmphasize the new and important aspects of the study andthe conclusions that follow from them. Do not repeat in detaildata or other material given in the Introduction or the Resultssection. Include in the Discussion section the implications ofthe findings and their limitations, including implications forfuture research. Relate the observations to other relevantstudies.Link the conclusions with the goals of the study6. AcknowledgmentList all contributors who do not meet the criteria for authorship,such as a person who provided purely technical help, writingassistance, or a department chair who provided only generalsupport. Financial and material support should also beacknowledged.7. AuthorshipAuthorship credit is based only on 1) substantial contributionsto conception and design, or acquisition of data, or analysisand interpretation of data; 2) drafting the article or revisingit critically for important intellectual content; and 3) finalapproval of the version to be published. Conditions 1, 2, and3 must all be met.Authors should provide a description ofwhat each contributed.8. Conflict of interestAll authors have to disclose and submit any financial /personnelrelationship that might bias and inappropriately influencetheir work.9. ReferencesMajority of the references must be from last five years. Localreferences must also be included. Vancouver style should befollowed. Examples are:a) Standard journal articleList the f irst s ix authors fol lowed by et al .I)Less than 6 authors:Vega KJ, Pina I, Krevsky B. Hearttransplantation is associated with an increased risk forpancreato-biliary disease. Ann Intern Med 1996 Jun 1;124(11):980-3.II) More than six authors:Parkin DM, Clayton D, Black RJ, Masuyer E, Friedl HP,Ivanov E, et al. Childhood leukaemia in Europe afterChernobyl: 5 year follow-up. Br J Cancer 1996;73:1006- 12.b) Organization as authorThe Cardiac Society of Australia and New Zealand. Clinicalexercise stress testing. Safety and performance guidelines.Med J Aust 1996; 164: 282-4.
JBUMDC 2016; 6(1): 131-133 Page-131
JBUMDC INSTRUCTION TO AUTHORS

c) No author givenCancer in South Africa [editorial]. S Afr Med J 1994;84:15.d) Chapter in a bookPhillips SJ, Whisnant JP. Hypertension and stroke. In: LaraghJH, Brenner BM, editors. Hypertension: pathophysiology,diagnosis, and management. 2nd ed. New York: Raven Press;1995. p. 465-78.e) NewspaperHasanMansoor. Excessive use of drugs creating resistance toantibiotics. The Dawn 2013, 24 June; sect. Metropolitan(col.1-4)10. TablesType or print out each table with double spacing on a separatesheet of paper. Number tables consecutively in the order oftheir first citation in the text and supply a brief title for each.Give each column a short or abbreviated heading. Placeexplanatory matter in footnotes. Explain in footnotes allnonstandard abbreviations that are used in each table. Identifystatistical measures of variations, such as standarddeviation and standard error of the mean.Do not use internalhorizontal and vertical rules.11. Illustrations (Figures)Figures should be professionally drawn and photographed.Photographic prints 127 × 173 mm (5 × 7 inches). Photomicro-graphs should have internal scale markers. Symbols, arrows,or letters used in photomicrographs should contrast with thebackground.If photographs of people are used, either thesubjects must not be identifiable or their pictures must beaccompanied by written permission to use the photographFigures should be numbered consecutively according to the
order in which they have been first cited in the text. If a figurehas been published, acknowledge the original source andsubmit written permission from the copyright holder toreproduce the material.Legends for IllustrationsType or print out legends for illustrations using double spacing,starting on a separate page, with Arabic numerals correspondingto the illustrations. When symbols, arrows, numbers, or lettersare used to identify parts of the illustrations, identify andexplain each one clearly in the legend. Explain the internalscale and identify the method of staining in photomicrographs.Units of MeasurementMeasurements of length, height, weight, and volume shouldbe reported in metric units. Temperatures in degrees Celsius,Blood pressure in millimeters of mercury & all hematologicand clinical chemistry measurements in the metric system interms of the International System of Units (SI).Abbreviations and SymbolsUse only standard abbreviations. Avoid abbreviations in thetitle and abstract. The full term for which an abbreviationstands should precede its first use in the text unless it is astandard unit of measurement.Sending the Manuscript to the JournalSubmit manuscript by e-mail: [email protected] by post on CD with two hard copies to: Editor, JBUMDC,Bahria University Medical & Dental College, DHA Phase-II, Adjacent PNS Shifa, Karachi. All correspondence regardingsubmitted manuscripts will be via e-mail.
JBUMDC 2016; 6(1): 131-133 Page-132

JBUMDC 2016; 6(1): 131-133 Page-133
S #Type of
Article
Abstract type & word
countKey words
Tables
(Max)
Figures
(Max)References
1
2
3
4
5
6
7
8
9
Editorial
Review Article
Original Article
MedicalEducation
Student Corner
Case Report
Letter to Editor
Short
Communication
/Commentary/
Opinions/
Perspective
Instruction toAuthor
- -
Unstructured (150)
Structured (250)
Unstructured (150)
Unstructured (150)
1. Original Structured
(250)
2. Review Unstructured
(150)
3. Reproducible work (guide lines, questionnaire)
1. Original article Structured (250)
-
3-6
3-10
3-6
10-12
15-20
Please See the Text Detail
Total word
count
1000-1500
1200-1500
3-6
3-10
-
3-10
3-6
3-5
2500-3000
1200-1500
1200-1300
400-500
3000-3500
2500-3000
2500-3000
3000-3500
40-60
25-35
25-35
40-60
25-35
8-10
10-12
5
-
2
4
4
4
4
4
1
1
-
-
1
2
3
3
2
3
1
2
-
Mention Source, Accessed on, Retrieval date
2. Views/Perspectives/ Opinions Unstructured (150) Students Activity Report (BUMDC)

BAHRIA MEDICAL MAGZINE 2015 CYAN MAGANTA YELLOW BLACK
Published by: Bahria University Medical & Dental College
Adjacent PNS Shifa DHA Phase II Karachi, Pakistan.
Ph: +92-21-35319491-9
Website: http://jbumdc.bahria.edu.pk
JBUMDC Web Mail: [email protected]
Bahria University Medical and Dental College, Karachi





























