Embed Size (px)
Citation preview

SEVOFLURANE ANESTHESIA WITHOUT MUSCLE RELAXANTS
FOR THORACOSCOPIC THYMECTOMY
IN MYASTHENIA GRAVIS
Vo Van HienNguyen Huu Tu
Mai Van Vien
Introduction Myasthenia gravis (MG) is a chronic autoimmune disorder
related to the thymus gland.
Thymectomy is one of the effective methods to treat MG.
Patients with myasthenia gravis did sentitivity to the drugs
were used in anesthesia → Choice drugs and anesthesia
technique plays an important role in the success of
operation.
Respiratory complications depend on anesthetic technique:
Mulder et al (1972): 50% of pts need ventilatory support.
Suwanchi (1995): Comparision general anesthesia vs
epidural anesthesia and iv. propofol: early extubation in
operating room 29%- 78%.
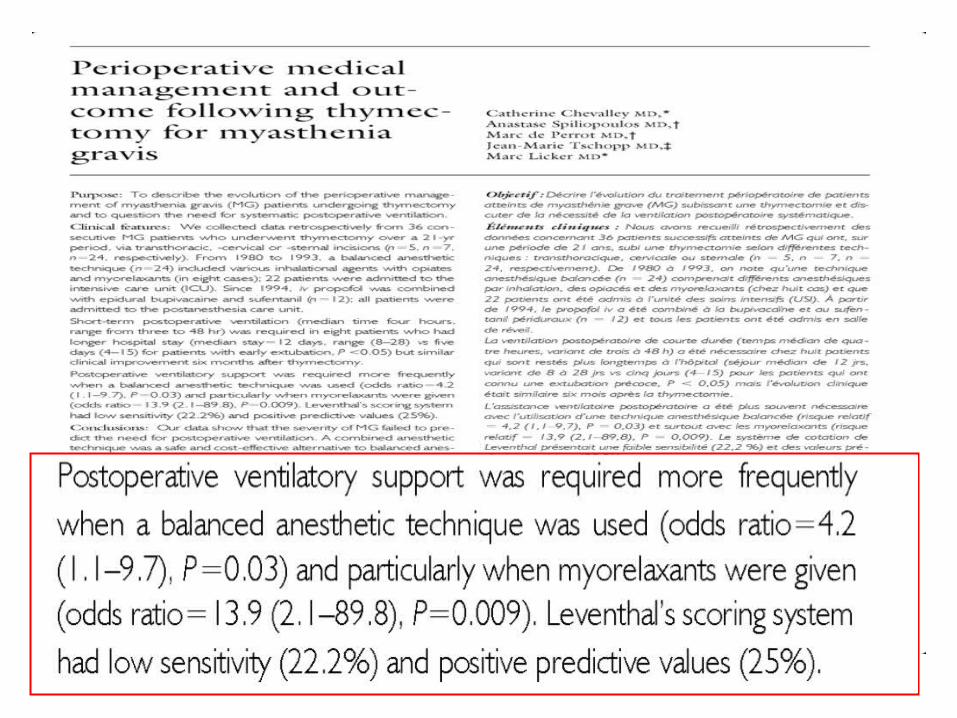
Catherine Chevalley et al (2001)(*):
+ Time need ventilation support : 2-48h
+ Propofol was used (1994): No need to ventilate
postoperative.
introduction
In Vietnam, Đo Tat Cuong (1996) reported postoperative
ventilation depend on method of anesthesia :
Anesthesia: 15.65%
Acupunture: 3.5%
Nguyen Van Thanh (1998) studied on 47 pts:
Required ventilation support: 15/47pts
Mortality: 3 patients due to respiratory infections.
introduction
Side effects of long-term ventilatory support on MG pts:
• Infections: respiratory, pneumonia, sepsis → death.
• Prolonged hospitalization days
• Increased treatment costs
Anesthesiologists’ recommendations:
introduction
“Avoid muscle relaxants in MG patients”

Choice drug ?Choice drug ?
Dose?Dose?
Intubation ?Intubation ?
Airways injuries?Airways injuries?
Hemodynamic change?Hemodynamic change?
Easy for surgeon?Easy for surgeon?
Early extubation?Early extubation?
Respiratory complication?Respiratory complication?
NO MUSCLE NO MUSCLE RELAXANTS RELAXANTS
!!!!!!
introduction

objectives
To evaluate the use of sevoflurane and
without muscle relaxants
for thoracoscopic thymectomy in MG patients
and post-operative respiratory status
methods
Subjects: Intervention study on 28 MG patients scheduled to
undergo thoracoscopic thymectomy
Monitor: Datex Omeda: ECG (DII), SpO2, EtCO2, invasive
aterial blood pressure (ABP), module Entropy (RE, SE), TOF.
Induction:
- Atropin: 0.5mg; Sufentanil: 0.5mcg/kg;
- Propofol 2.5-3 mg/kg
- Local anesthesia with 10 cc of lidocaine hydrochloride 2%
was sprayed on the vocal cords and into the trachea
Intubation Univent tube
- Loss eyelid reflex
- RE, SE<50
- Check tube and blocker’s position by endoscopy equipment
(Olympus)
Ventilate A/C mode : Vt = 10ml/kg; f=14l/ph; FiO2= 60%→
PetCO2= 28-32 mmHg.
OLV: Vt=5ml/kg, f=16-20; FiO2= 100% → Ppeak < 30 cm
H2O, PetCO2=30-35mmHg.
Sufentanil: 0.2mcg/kg/h
methods
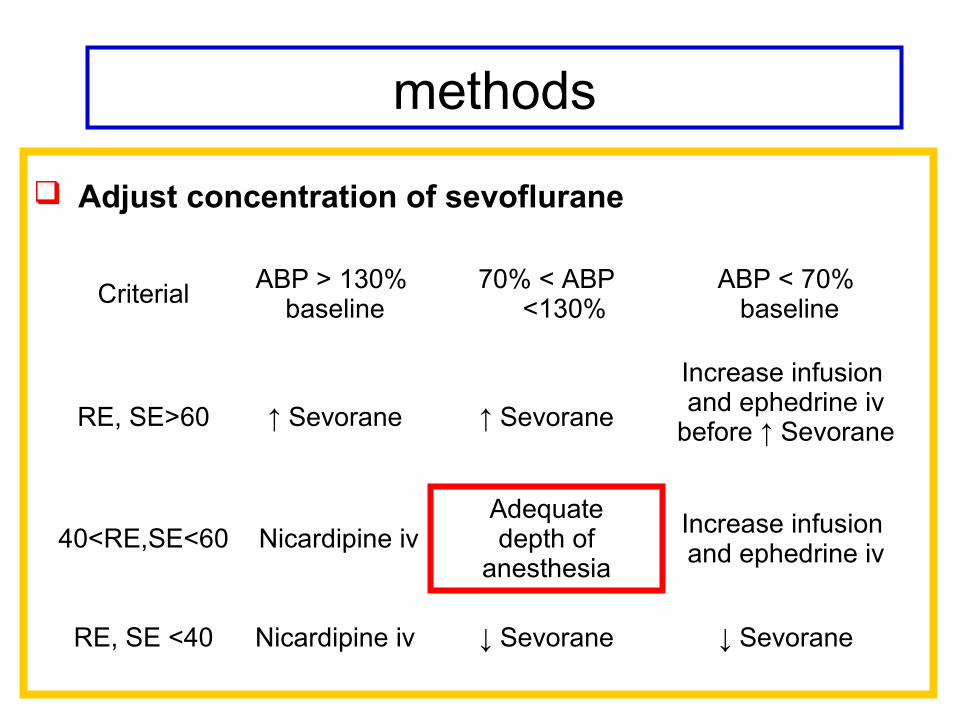
Adjust concentration of sevoflurane
Criterial ABP > 130% baseline
70% < ABP <130%
ABP < 70% baseline
RE, SE>60 ↑ Sevorane ↑ Sevorane
Increase infusion and ephedrine iv
before ↑ Sevorane
40<RE,SE<60 Nicardipine ivAdequatedepth of
anesthesia
Increase infusion and ephedrine iv
RE, SE <40 Nicardipine iv ↓ Sevorane ↓ Sevorane
methods
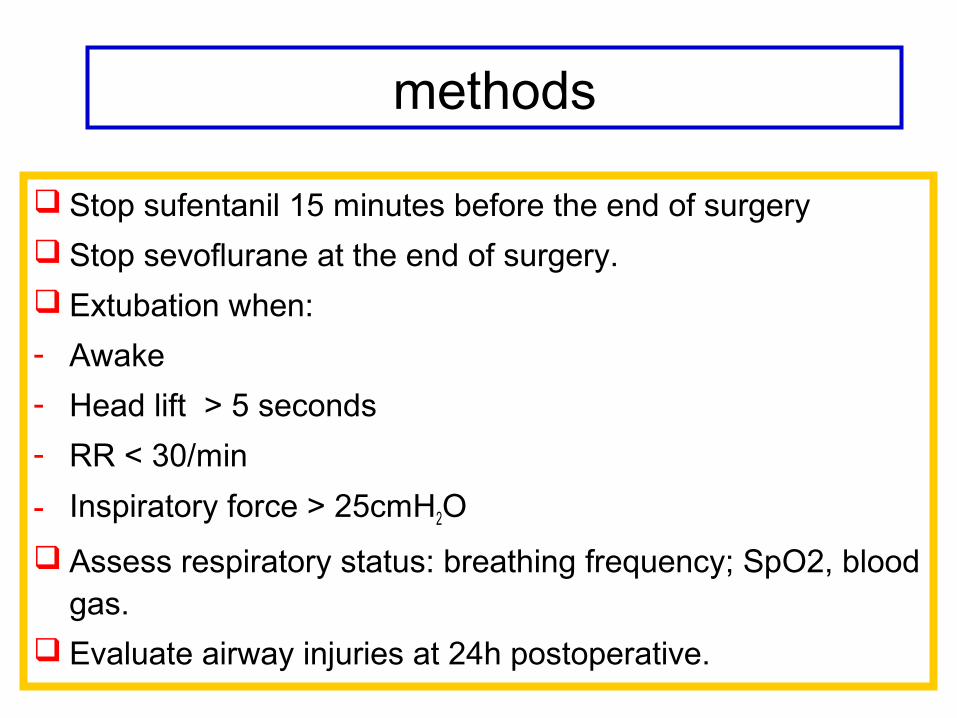
Stop sufentanil 15 minutes before the end of surgery
Stop sevoflurane at the end of surgery.
Extubation when:
- Awake
- Head lift > 5 seconds
- RR < 30/min
- Inspiratory force > 25cmH2O
Assess respiratory status: breathing frequency; SpO2, blood gas.
Evaluate airway injuries at 24h postoperative.
methods
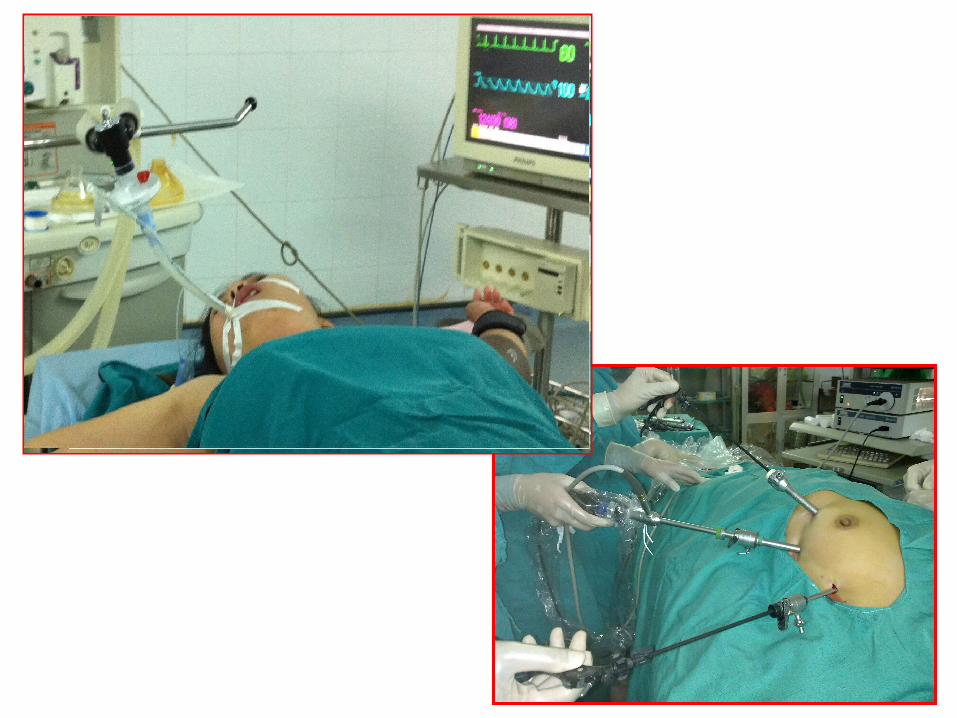
Medical equiments used in studyUnivent tube’s Univent tube’s
position position
in trachea in trachea
I- STAT portable I- STAT portable
clinical analyserclinical analyser
-pH-pH
-PaO2PaO2
-PaCO2PaCO2
-HCO3HCO3--
-BEBE
-BBBB

recorded Data General characteristics
Intubation conditions (Viby Mogensen Score), number of attemps to intubate.
Hemodynamic changes at induction, before and after intubation and intraoperative.
Neuromuscular effect of sevoflurane on MG: TOF
Surgeons’ satisfaction: VAS score
Time to extubation and respiratory status: f, SpO2 , PaO2,
PaCO2, pH,…
Clinical symtom due to airway injuries: sorethroat,
hoarseness and observe by laryngostroboscopy.
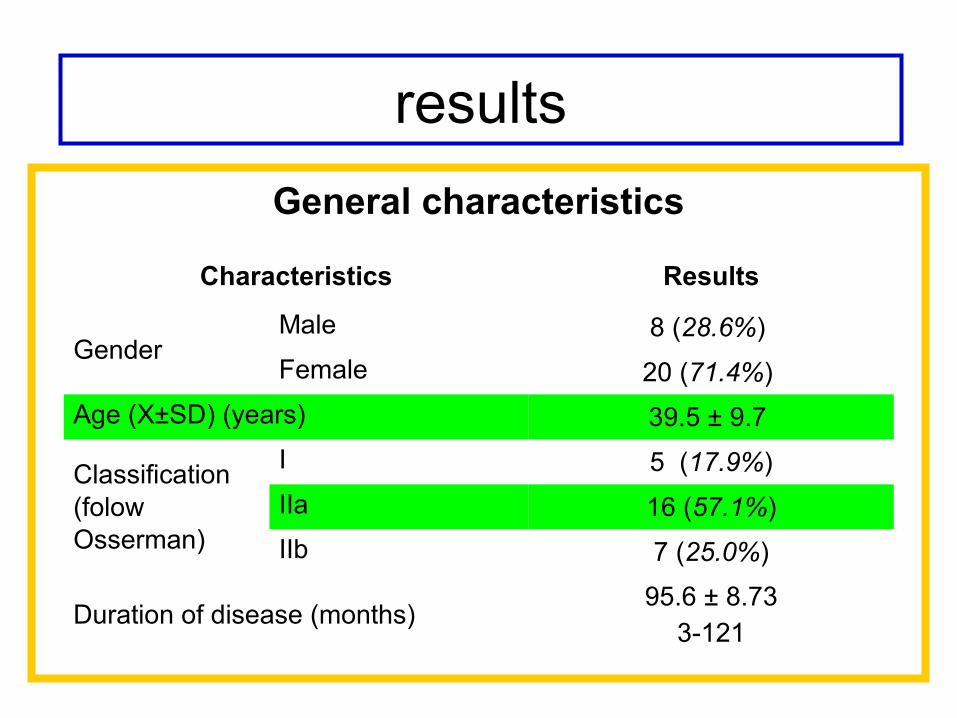
resultsGeneral characteristics
Characteristics Results
GenderMale 8 (28.6%)
Female 20 (71.4%)
Age (X±SD) (years) 39.5 ± 9.7
Classification (folow Osserman)
I 5 (17.9%)
IIa 16 (57.1%)
IIb 7 (25.0%)
Duration of disease (months)95.6 ± 8.73
3-121
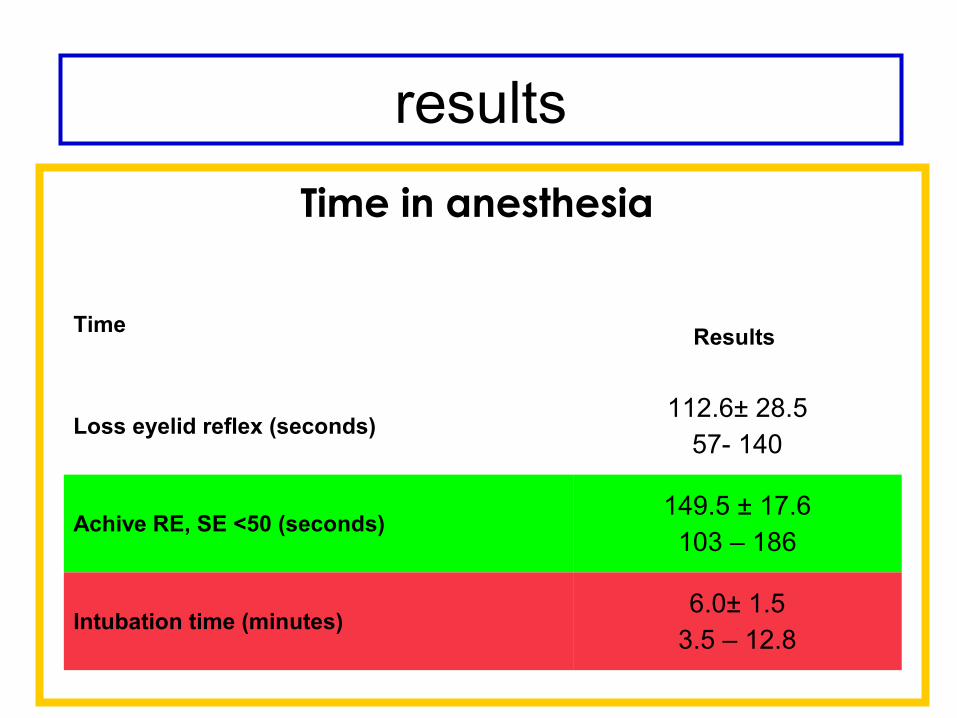
Time in anesthesia
Time
Results
Loss eyelid reflex (seconds)112.6± 28.5
57- 140
Achive RE, SE <50 (seconds)149.5 ± 17.6
103 – 186
Intubation time (minutes)6.0± 1.5
3.5 – 12.8
results
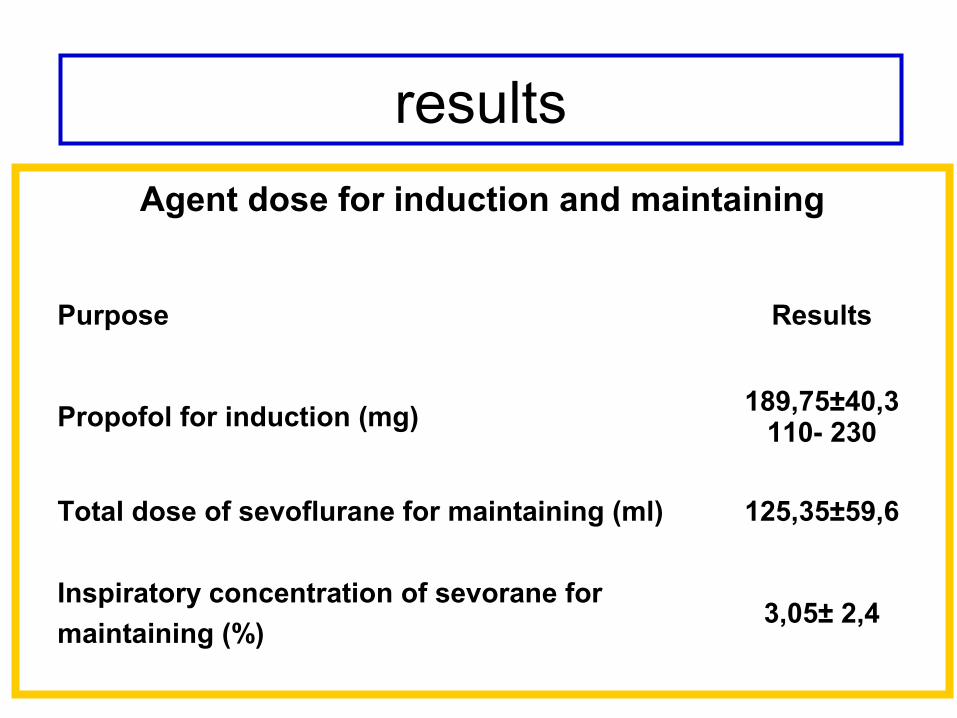
Agent dose for induction and maintaining
Purpose Results
Propofol for induction (mg) 189,75±40,3110- 230
Total dose of sevoflurane for maintaining (ml) 125,35±59,6
Inspiratory concentration of sevorane for
maintaining (%)3,05± 2,4
results
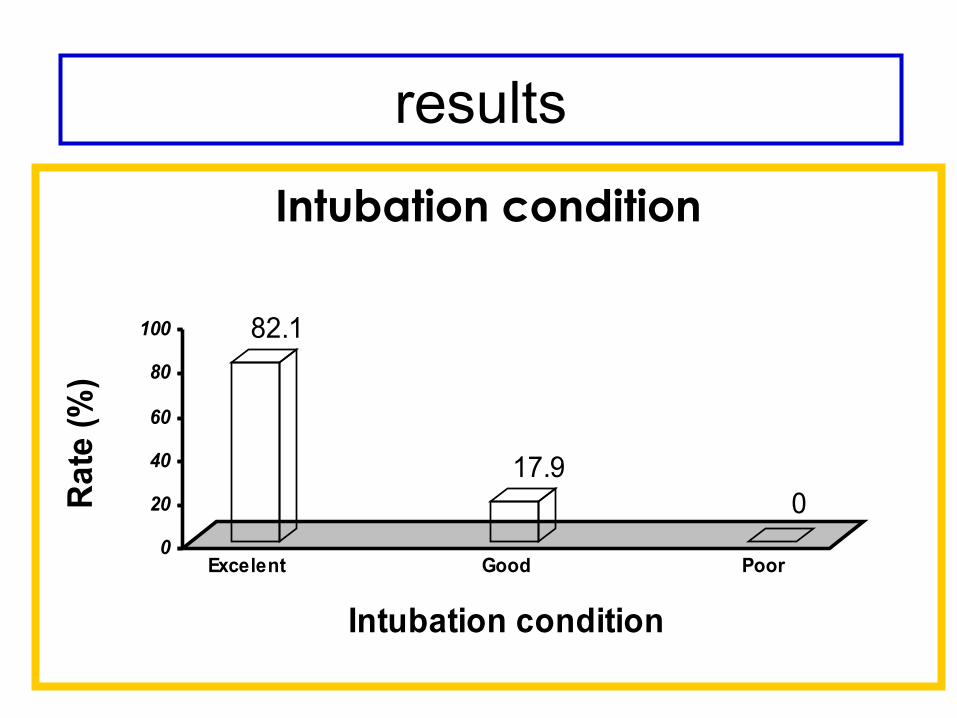
Intubation condition
82.1
17.90
0
20
40
60
80
100
Rat
e (%
)
Excelent Good Poor
Intubation condition
results
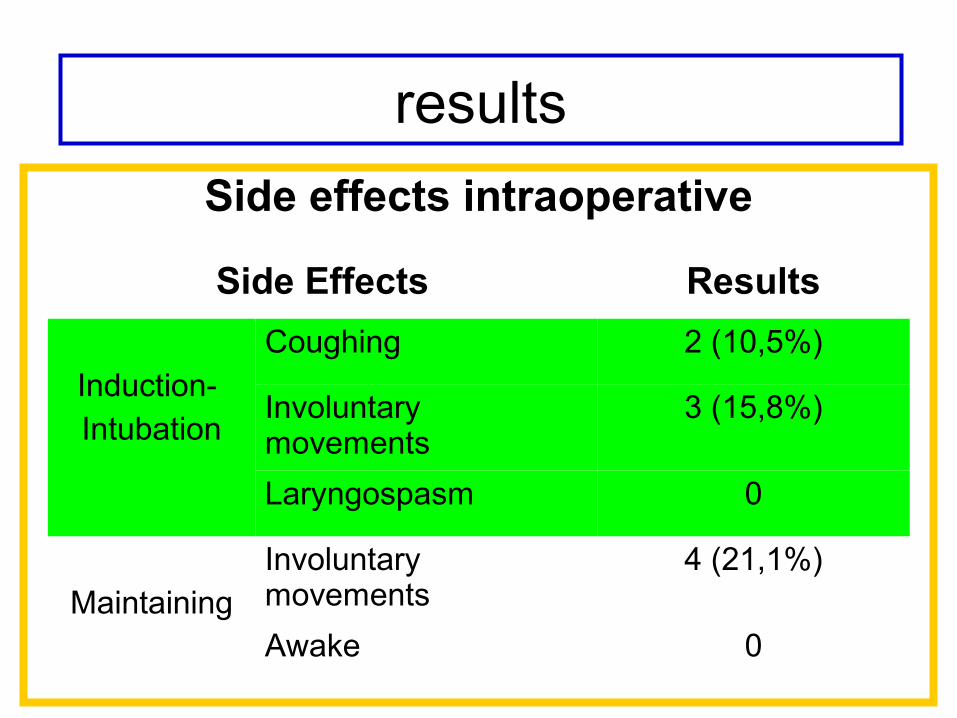
Side effects intraoperative
Side Effects Results
Induction- Intubation
Coughing 2 (10,5%)
Involuntary movements
3 (15,8%)
Laryngospasm 0
MaintainingInvoluntary movements
4 (21,1%)
Awake 0
results

50
70
90
110
130
150
T0 T1 T2 T3 T4 T5 T6 T7 T8 T9 T10 T11 T12 T13 T14
Mea
n I
AB
P (
mm
Hg
)
InductionIntubation Surgery The
end
Mean IABP changes
results
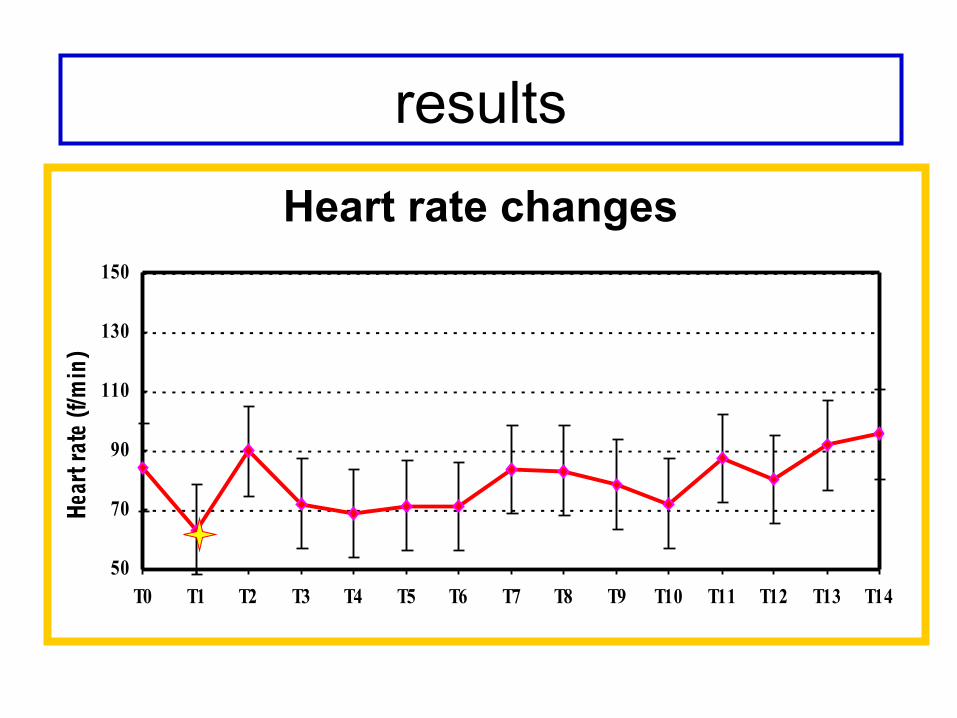
Heart rate changes
results
50
70
90
110
130
150
T0 T1 T2 T3 T4 T5 T6 T7 T8 T9 T10 T11 T12 T13 T14
Hear
t rat
e (f/
min
)
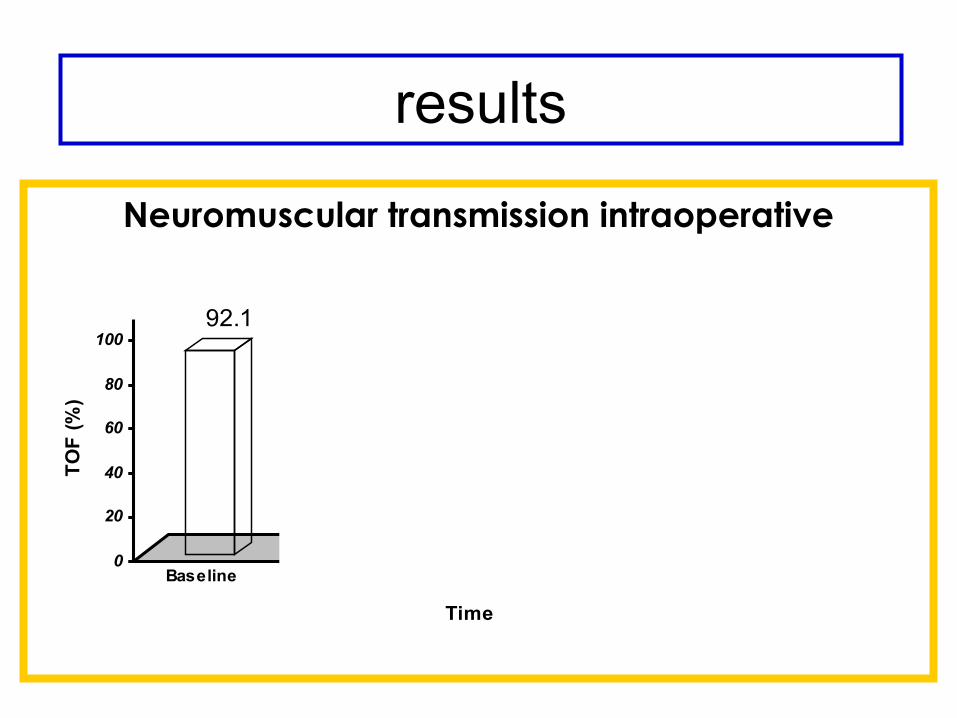
Neuromuscular transmission intraoperative
92.179.3* 75.3* 76.5*
91.7
0
20
40
60
80
100
TO
F (
%)
Baseline 30 min 60 min 90 min The end
Time
results

Dù kiÕn kÕt luËn
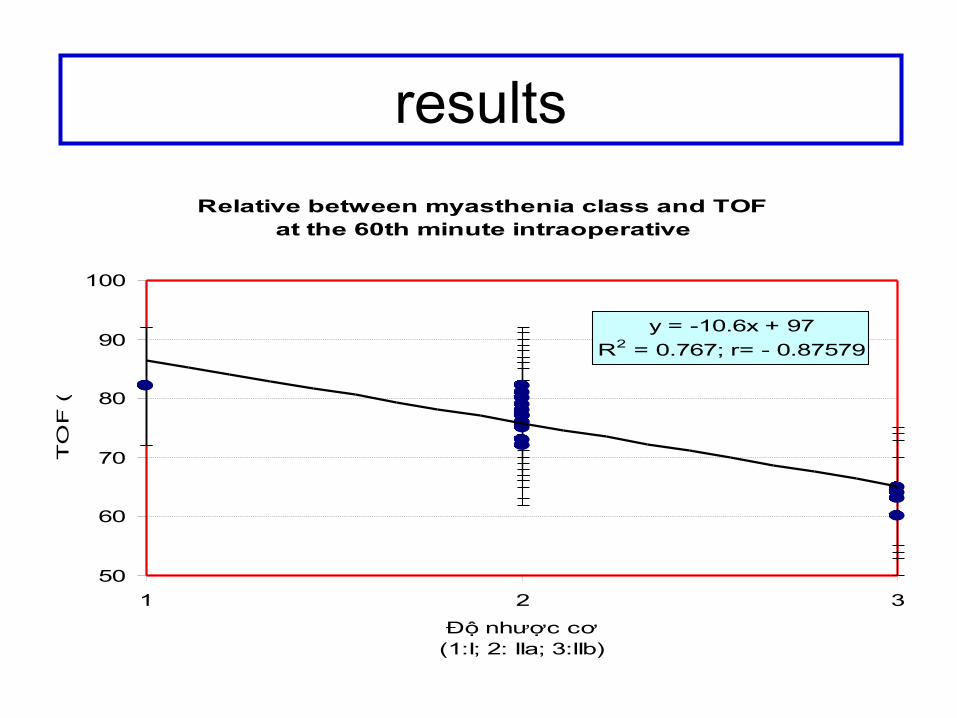
Relative between myasthenia class and TOF at the 60th minute intraoperative
y = -10.6x + 97
R2 = 0.767; r= - 0.87579
50
60
70
80
90
100
1 2 3
Độ nhược cơ (1:I; 2: IIa; 3:IIb)
TO
F (
%)
results
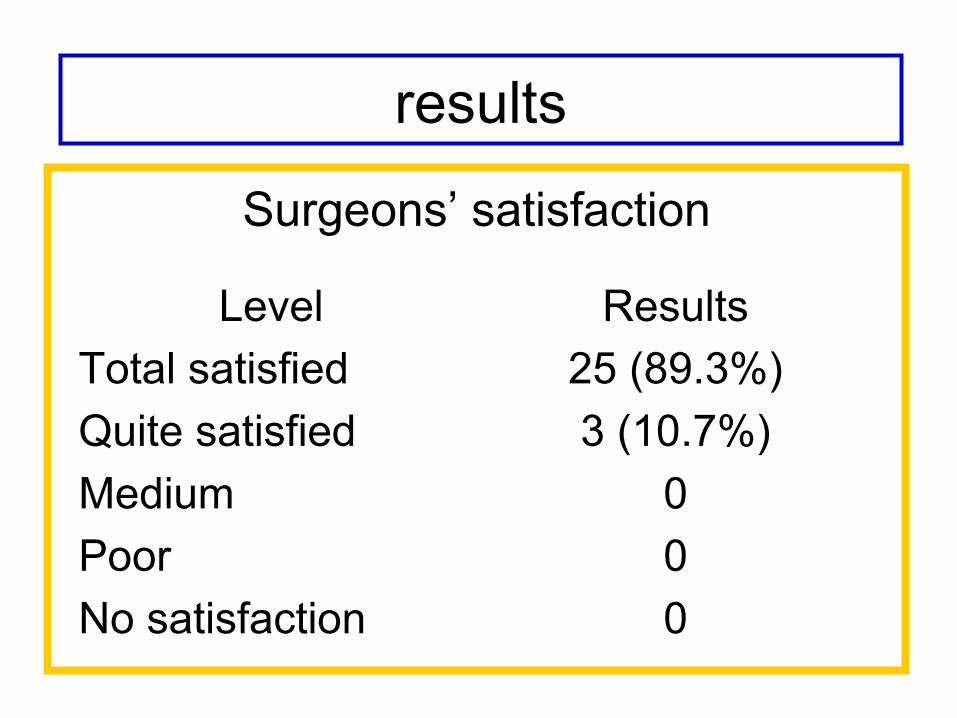
Surgeons’ satisfaction
Level Results
Total satisfied 25 (89.3%)
Quite satisfied 3 (10.7%)
Medium 0
Poor 0
No satisfaction 0
results
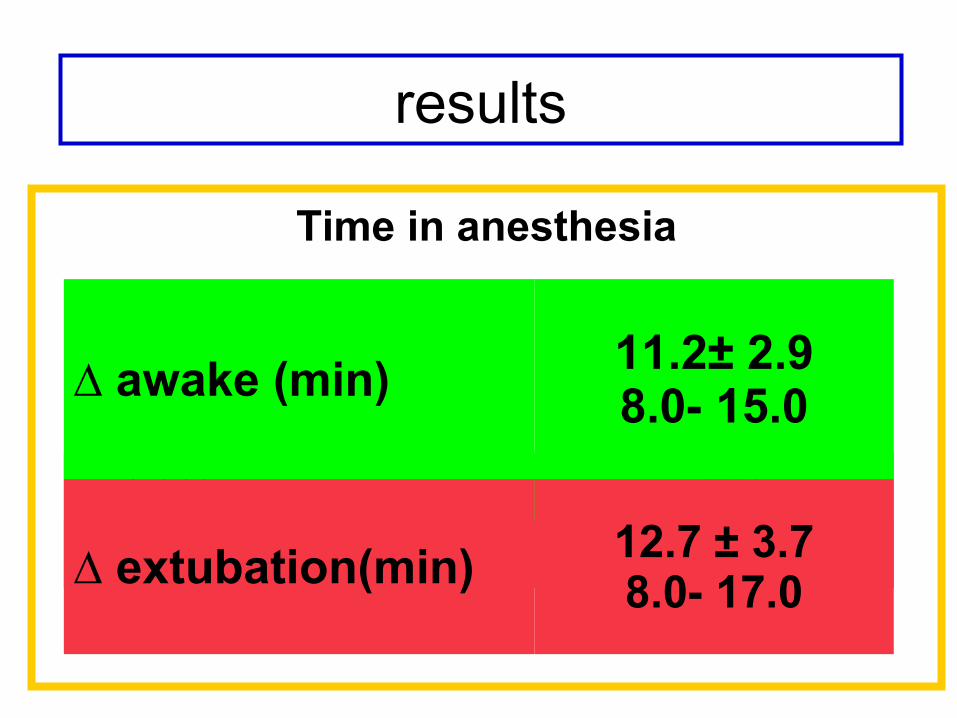
Time in anesthesia
Duration Results
Duration of surgery (min)125.6 ± 20.3
85 - 145
Duration of anessthesia (min)143.7 ± 18.9
90 -180
∆ awake (min)11.2± 2.98.0 – 15.0
∆ extubation (min)12.7 ± 3.78.0 -17.0
Self-awareness (min)13.9 ± 1.9
8 -18
results
∆ awake (min)11.2± 2.98.0- 15.0
∆ extubation(min) 12.7 ± 3.78.0- 17.0
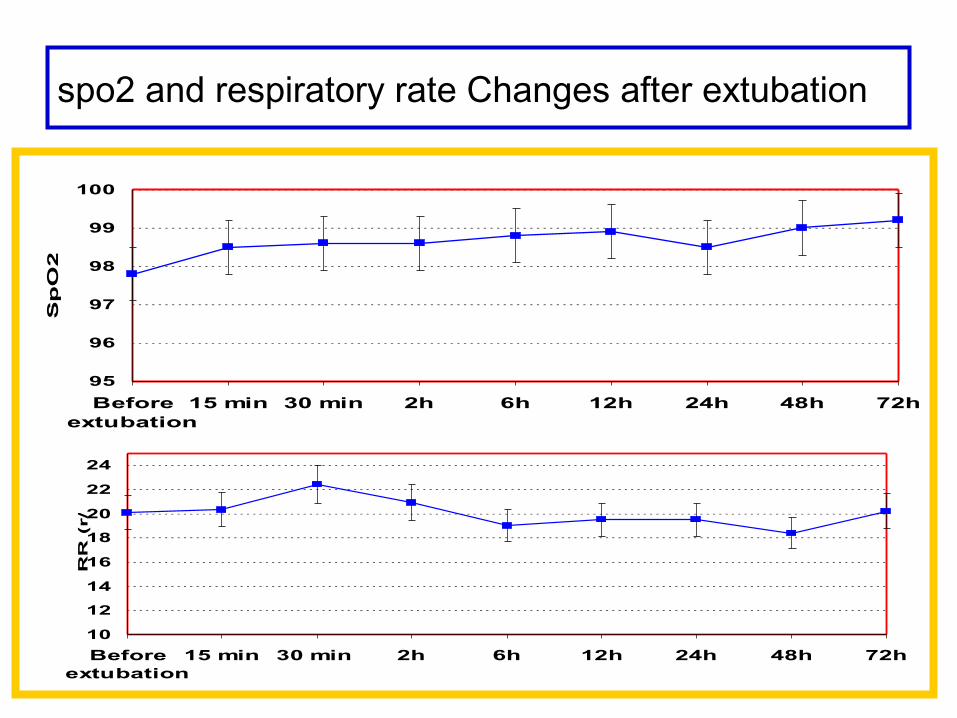
10
12
14
16
18
20
22
24
Beforeextubation
15 min 30 min 2h 6h 12h 24h 48h 72h
RR
(r/p
h)
95
96
97
98
99
100
Beforeextubation
15 min 30 min 2h 6h 12h 24h 48h 72h
Sp
O2
(%
)
spo2 and respiratory rate Changes after extubation

PaO2 changes
50
100
150
200
250
300
350
Pre-ope DLV OLV 2h afterextubation
1st daypost ope
2nd daypost-ope
3 rd daypost -ope
Arterial blood gas changes

PaCO2 changes
35
37
39
41
43
45
Pre-ope DLV OLV 2h afterextubation
1st daypost ope
2nd daypost ope
3rd postope
Arterial blood gas changes
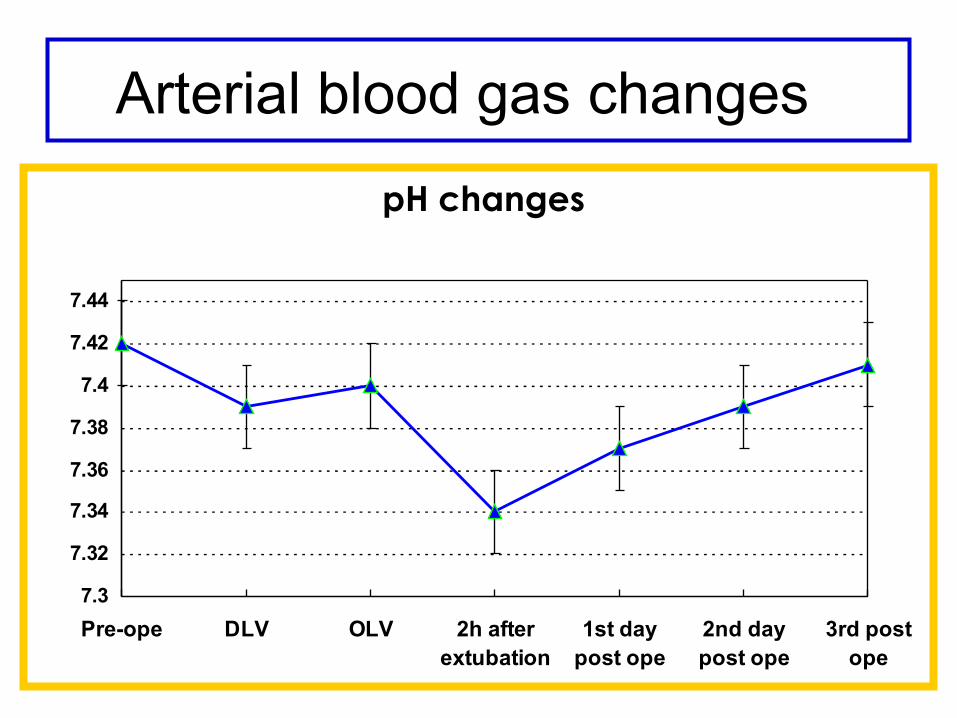
pH changes
7.3
7.32
7.34
7.36
7.38
7.4
7.42
7.44
Pre-ope DLV OLV 2h afterextubation
1st daypost ope
2nd daypost ope
3rd postope
Arterial blood gas changes
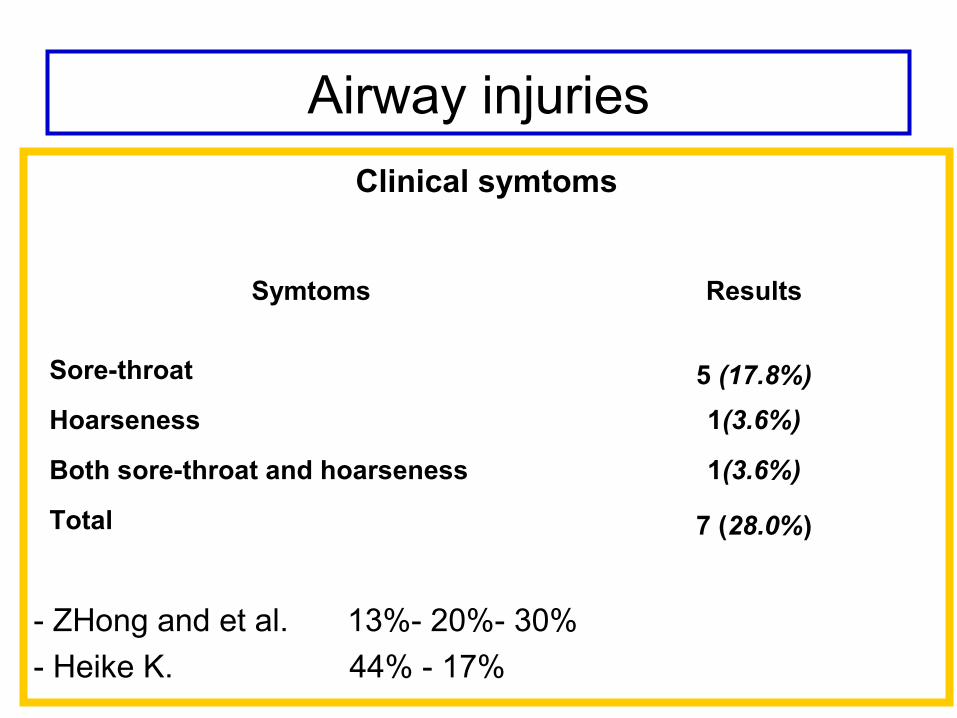
Airway injuriesClinical symtoms
- ZHong and et al. 13%- 20%- 30%
- Heike K. 44% - 17%
Symtoms Results
Sore-throat 5 (17.8%)
Hoarseness 1(3.6%)
Both sore-throat and hoarseness 1(3.6%)
Total 7 (28.0%)
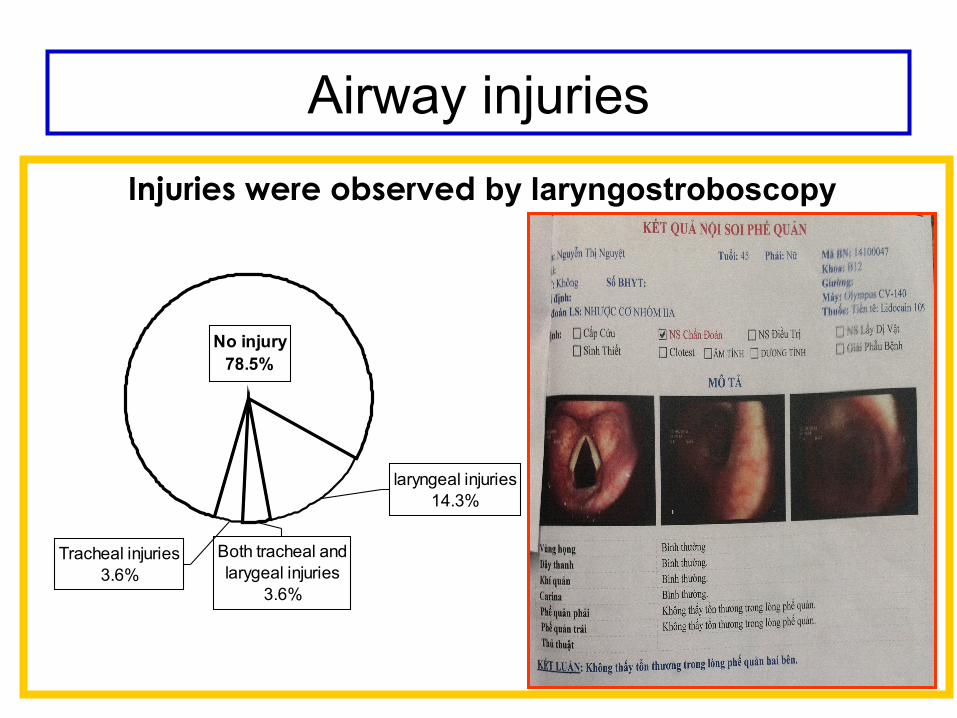
Injuries were observed by laryngostroboscopy
No injury 78.5%
laryngeal injuries14.3%
Both tracheal and larygeal injuries
3.6%
Tracheal injuries3.6%
Airway injuries

Sevoflurane anesthesia without muscular relaxants for thoracoscopic thymectomy in MG
Good intubating conditions
Stable hemodynamic
Faster recovery
100% of the patients successfully to extubate at operating room.
No patients required reintubation due to respiratory failure.
Airway injuries due to intubation: 28%
conclusions

Thank for your attention!























![14 phung hien tu van [compatibility mode]](https://img.dokumen.tips/doc/110x75/5587e32fd8b42a6f068b4683/14-phung-hien-tu-van-compatibility-mode.jpg)



![van mieu quoc tu giam [vo kim cuong]](https://img.dokumen.tips/doc/110x75/558fd71c1a28ab59778b4784/van-mieu-quoc-tu-giam-vo-kim-cuong.jpg)
