Embed Size (px)
Citation preview

21/12/12 CME Slides Forum - J. Bacchetta
1/16ndt-educational.org/bacchettaslide2012.htm
VITAMIN D, FGF23 AND INNATE IMMUNITY IN CKD
Justine Bacchetta, Bron, France
Chair: Marc De Broe, Antwerp, Belgium
Marc Vervloet, Amsterdam, Netherlands
Dr Justine BacchettaC entre de Référence des Maladies Rénales Rares
Hôpital Femme Mère Enfant
Hospices C ivils de Lyon
Bron, France
Slide 1
Good morning ladies and gentlemen, it’s my pleasure to present to you this morning some data about the interplaybetween vitamin D and FGF23 in innate immunity.
Slide 2
CME Slides Forum - J. Bacchetta
2/16ndt-educational.org/bacchettaslide2012.htm
Before that I will go very quickly through this background.
Slide 3
You know now that when GFR decreases, probably the first biomarker to increase is circulating FGF23 levels. Fromhealthy controls we have some data between 15-30 UI/ml and then with CKD you have a progressive increase and indialysis patients you can go up to more than 10.000 UI/ml.
Slide 4
21/12/12 CME Slides Forum - J. Bacchetta
3/16ndt-educational.org/bacchettaslide2012.htm
However, we don’t really know which is the trigger of the increasing FGF23 in osteocytes and we know after that thatyou have an increase in PTH and phosphate
Slide 5
and a decrease in 1, 25 vitamin D leading to the main complications of CKD:
Slide 6
21/12/12 CME Slides Forum - J. Bacchetta
4/16ndt-educational.org/bacchettaslide2012.htm
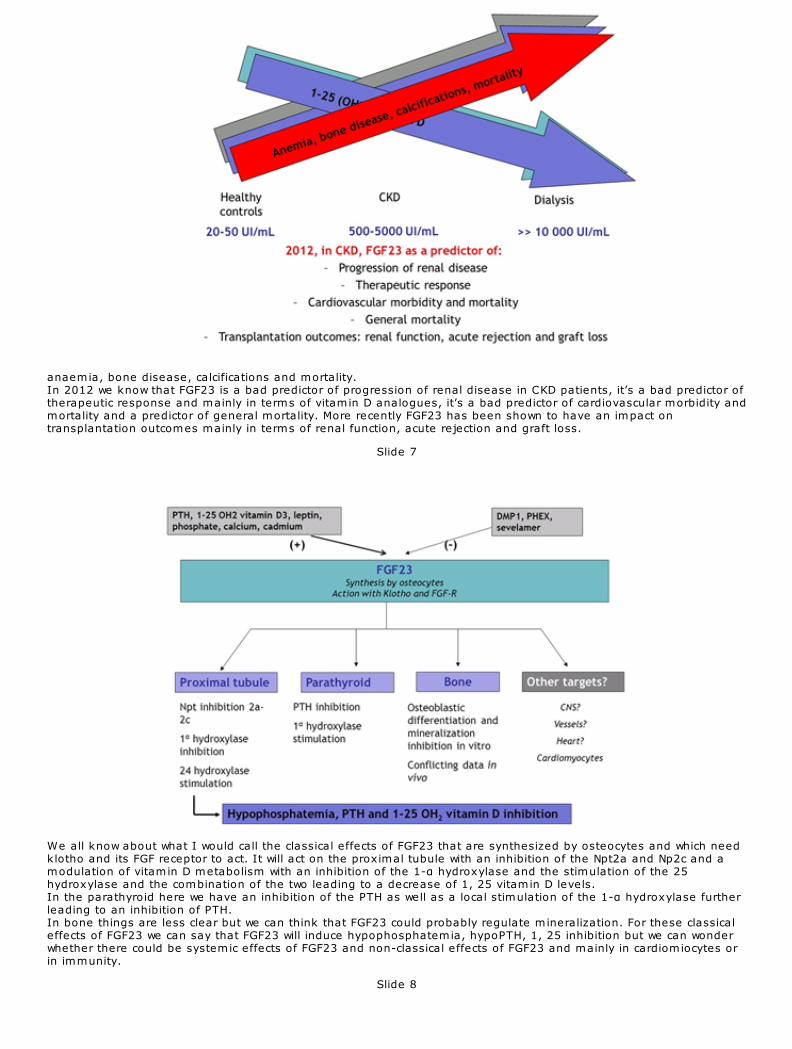
anaemia, bone disease, calcifications and mortality. In 2012 we know that FGF23 is a bad predictor of progression of renal disease in CKD patients, it’s a bad predictor oftherapeutic response and mainly in terms of vitamin D analogues, it’s a bad predictor of cardiovascular morbidity andmortality and a predictor of general mortality. More recently FGF23 has been shown to have an impact ontransplantation outcomes mainly in terms of renal function, acute rejection and graft loss.
Slide 7
We all know about what I would call the classical effects of FGF23 that are synthesized by osteocytes and which needklotho and its FGF receptor to act. It will act on the proximal tubule with an inhibition of the Npt2a and Np2c and amodulation of vitamin D metabolism with an inhibition of the 1-α hydroxylase and the stimulation of the 25hydroxylase and the combination of the two leading to a decrease of 1, 25 vitamin D levels. In the parathyroid here we have an inhibition of the PTH as well as a local stimulation of the 1-α hydroxylase furtherleading to an inhibition of PTH. In bone things are less clear but we can think that FGF23 could probably regulate mineralization. For these classicaleffects of FGF23 we can say that FGF23 will induce hypophosphatemia, hypoPTH, 1, 25 inhibition but we can wonderwhether there could be systemic effects of FGF23 and non-classical effects of FGF23 and mainly in cardiomiocytes orin immunity.
Slide 8

21/12/12 CME Slides Forum - J. Bacchetta
5/16ndt-educational.org/bacchettaslide2012.htm
Before going to the immunity question I would just like to remind you the data published by Faul and Myles Wolffrom Miami in JSI recently and they did some epidemiological studies from the CRIC cohort showing that increasedFGF23 levels were associated with left ventricular hypertrophy and more interestingly when they took FGF23 levels atbaseline in the cohort and they just looked at the risk for onset of LVH, the increased FGF23 levels at baseline are arisk factor for developing LVH. When they take rat cardiomiocytes and they put them with FGF23, you can see that they induce very importanthypertrophy of cardiomiocytes with increased markers for LVH.
Slide 9
This is a really important study because this is the first study showing a klotho-independent effect of FGF23. You cansee from these blots that klotho is not expressed in cardiomiocytes but you have an expression of at least twoFGF23 receptors: FGFR-1 and FGFR-4 in these miocytes. When they studied the signalling in the classical pathways of FGF23, the usual pathways that have been described tobe stimulated by FGF23 are the MAP-kinase pathway with ERK1 and ERK2 and the Akt pathways and in thesecardiomiocytes there is a weak activation of ERK and there is no activation of Akt but there is an activation of thePLCγ and the NFAT signalling that can be reversed by cyclosporine. The next step of this paper was to take some wild type mice and put them with IV injection of FGF23. You can see inthe figure that after 7 and 14 days of FGF23 infusions you can induce LVH in these wild type mice. Very interestingly, when they took some klotho deficient mice and we know that klotho deficient mice will expresshigh FGF23 levels without klotho by definition, they also show LVH. So it’s another rationale to say that it’s a klotho-independent effect of FGF23 on these cardiomiocytes.
Slide 10
21/12/12 CME Slides Forum - J. Bacchetta
6/16ndt-educational.org/bacchettaslide2012.htm
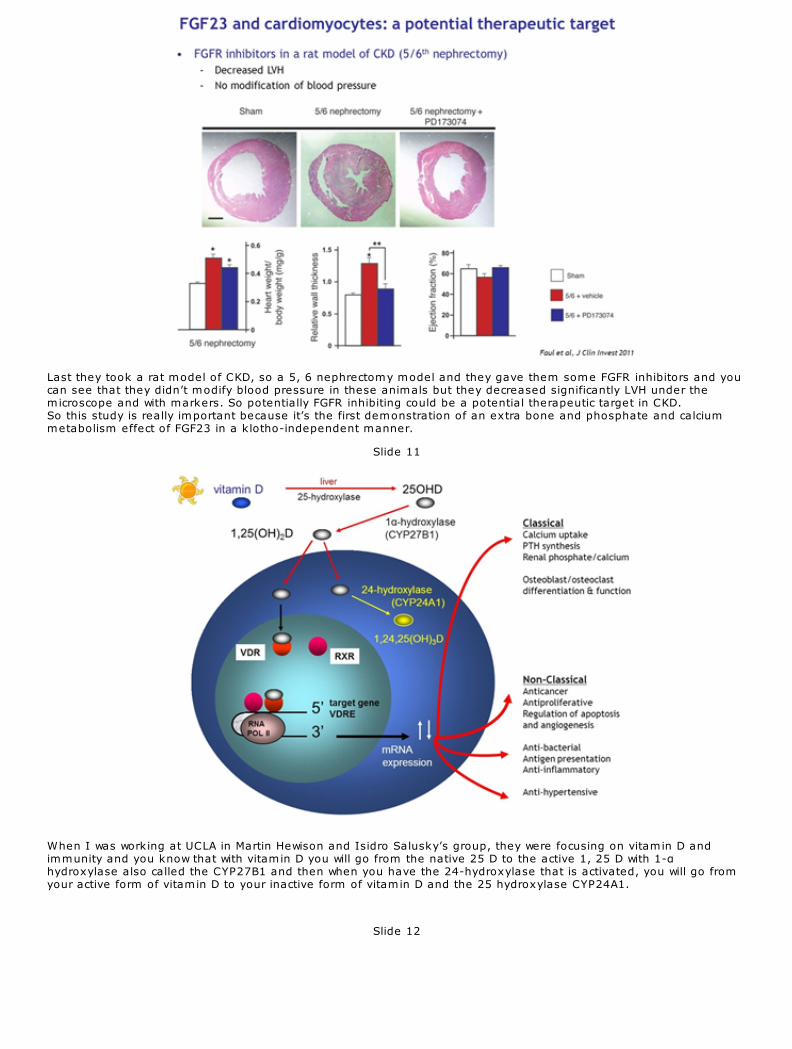
Last they took a rat model of CKD, so a 5, 6 nephrectomy model and they gave them some FGFR inhibitors and youcan see that they didn’t modify blood pressure in these animals but they decreased significantly LVH under themicroscope and with markers. So potentially FGFR inhibiting could be a potential therapeutic target in CKD. So this study is really important because it’s the first demonstration of an extra bone and phosphate and calciummetabolism effect of FGF23 in a klotho-independent manner.
Slide 11
When I was working at UCLA in Martin Hewison and Isidro Salusky’s group, they were focusing on vitamin D andimmunity and you know that with vitamin D you will go from the native 25 D to the active 1, 25 D with 1-αhydroxylase also called the CYP27B1 and then when you have the 24-hydroxylase that is activated, you will go fromyour active form of vitamin D to your inactive form of vitamin D and the 25 hydroxylase CYP24A1.
Slide 12
21/12/12 CME Slides Forum - J. Bacchetta
ndt-educational.org/bacchettaslide2012.htm
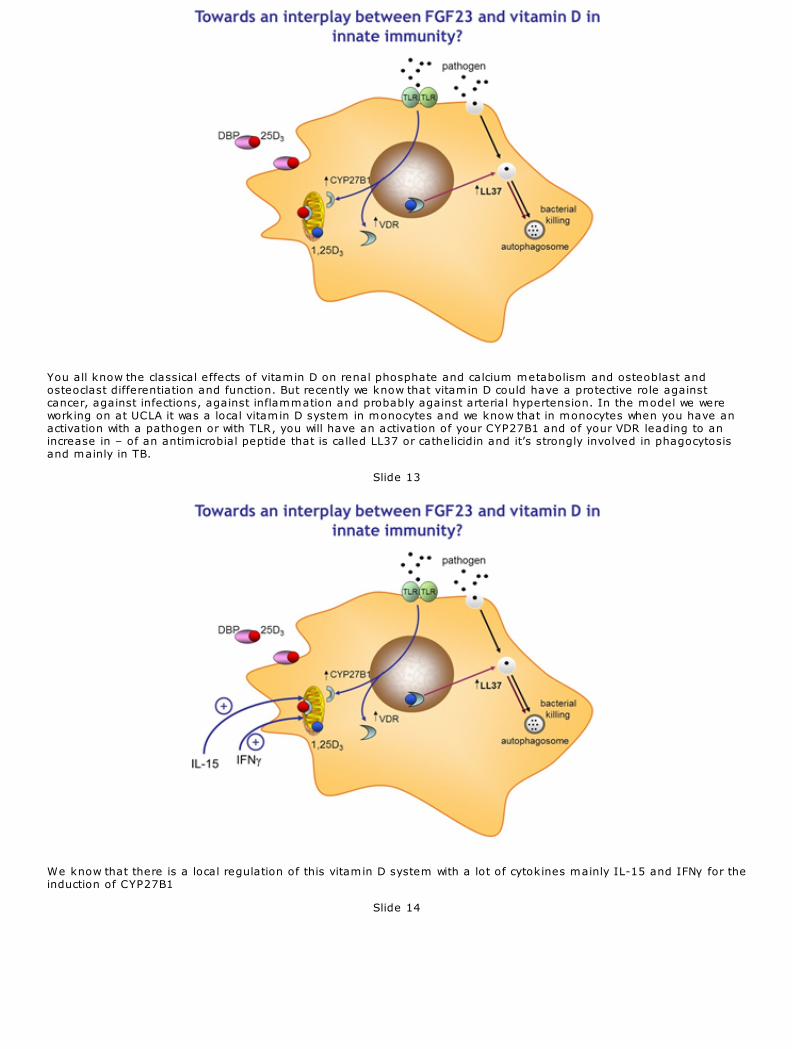
You all know the classical effects of vitamin D on renal phosphate and calcium metabolism and osteoblast andosteoclast differentiation and function. But recently we know that vitamin D could have a protective role againstcancer, against infections, against inflammation and probably against arterial hypertension. In the model we wereworking on at UCLA it was a local vitamin D system in monocytes and we know that in monocytes when you have anactivation with a pathogen or with TLR, you will have an activation of your CYP27B1 and of your VDR leading to anincrease in – of an antimicrobial peptide that is called LL37 or cathelicidin and it’s strongly involved in phagocytosisand mainly in TB.
Slide 13
We know that there is a local regulation of this vitamin D system with a lot of cytokines mainly IL-15 and IFNγ for theinduction of CYP27B1
Slide 14
CME Slides Forum - J. Bacchetta
8/16ndt-educational.org/bacchettaslide2012.htm
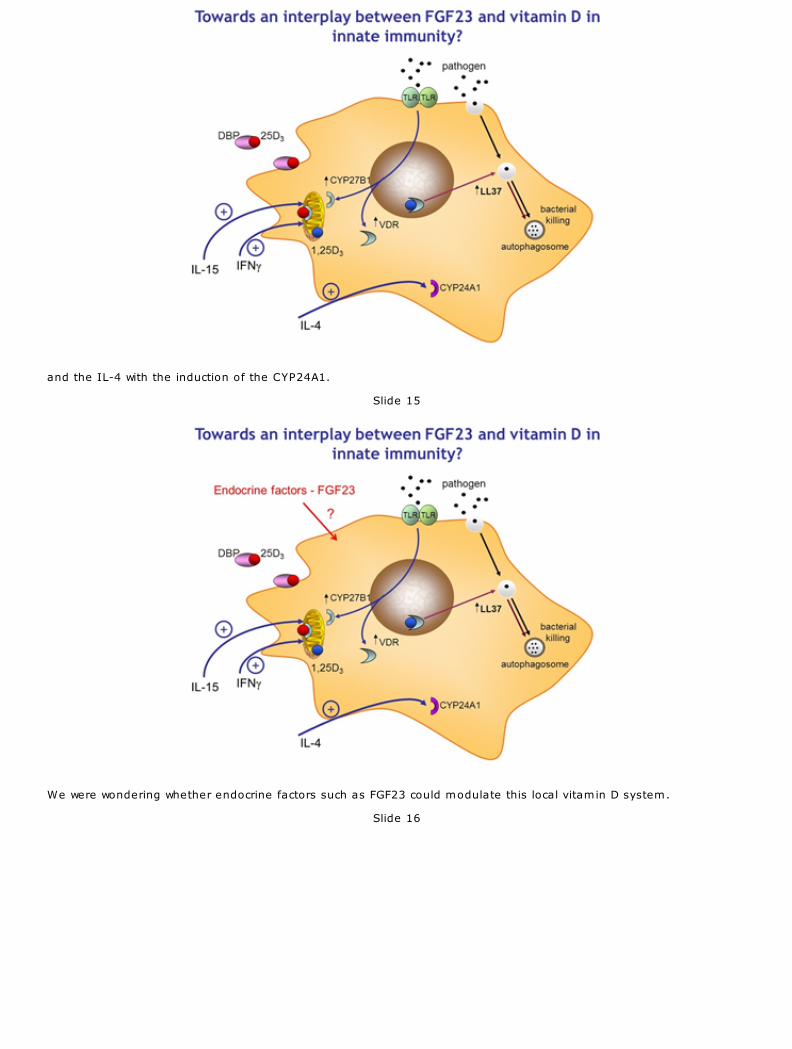
and the IL-4 with the induction of the CYP24A1.
Slide 15
We were wondering whether endocrine factors such as FGF23 could modulate this local vitamin D system.
Slide 16
21/12/12 CME Slides Forum - J. Bacchetta
9/16ndt-educational.org/bacchettaslide2012.htm
So our hypothesis was we knew that FGF23 could down regulate 1, 25 D in the proximal tubule cells and we also knewthat vitamin D could increase the expression of the antimicrobial LL37 in monocytes. The last thing we knew was thatLL37 was probably clinically relevant in CKD because Gombart et al. showed in 2009 that decreased circulating levelsof LL37 were associated with an increased risk of infections in CKD patients. So globally we thought that FGF23 couldsuppress vitamin D induced anti-bacterial responses by inhibiting CYP27B1 in monocytes. To assess this hypothesis we studied two different types of monocytes. The first one was PBMCs from healthy donorsand the second ones were peritoneal monocytes derived from patients undergoing peritoneal dialysis, so it would bea CKD model of monocytes.
Slide 17
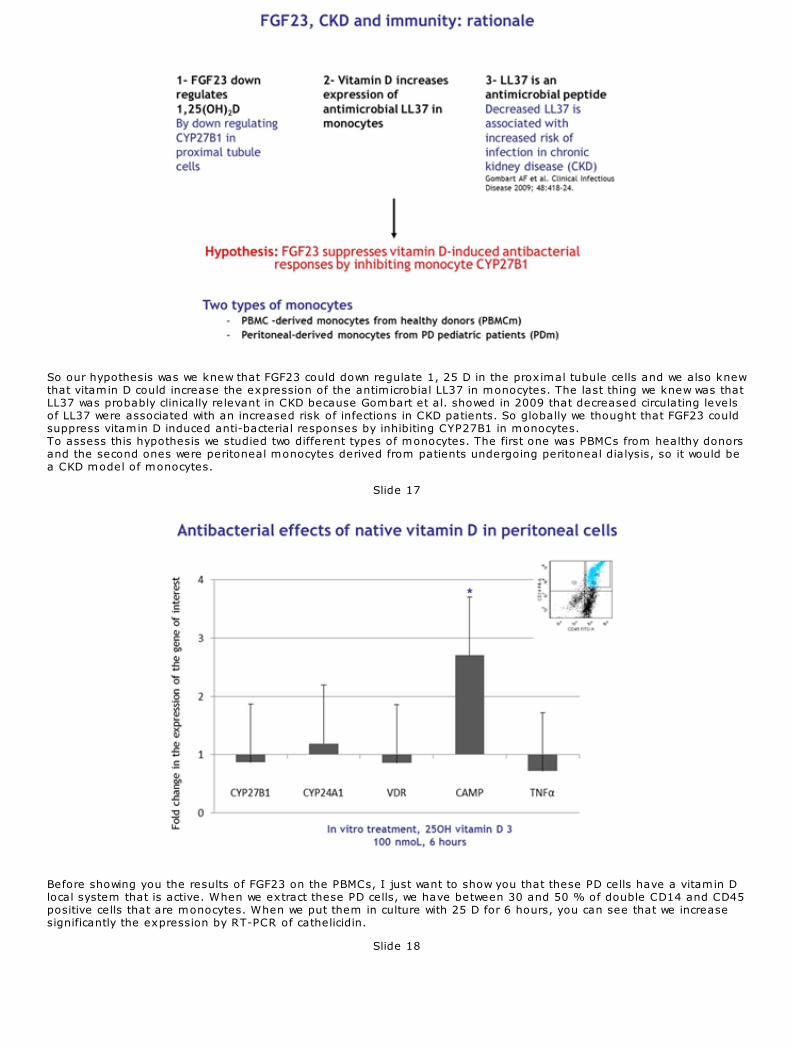
Before showing you the results of FGF23 on the PBMCs, I just want to show you that these PD cells have a vitamin Dlocal system that is active. When we extract these PD cells, we have between 30 and 50 % of double CD14 and CD45positive cells that are monocytes. When we put them in culture with 25 D for 6 hours, you can see that we increasesignificantly the expression by RT-PCR of cathelicidin.
Slide 18
21/12/12 CME Slides Forum - J. Bacchetta
10/16
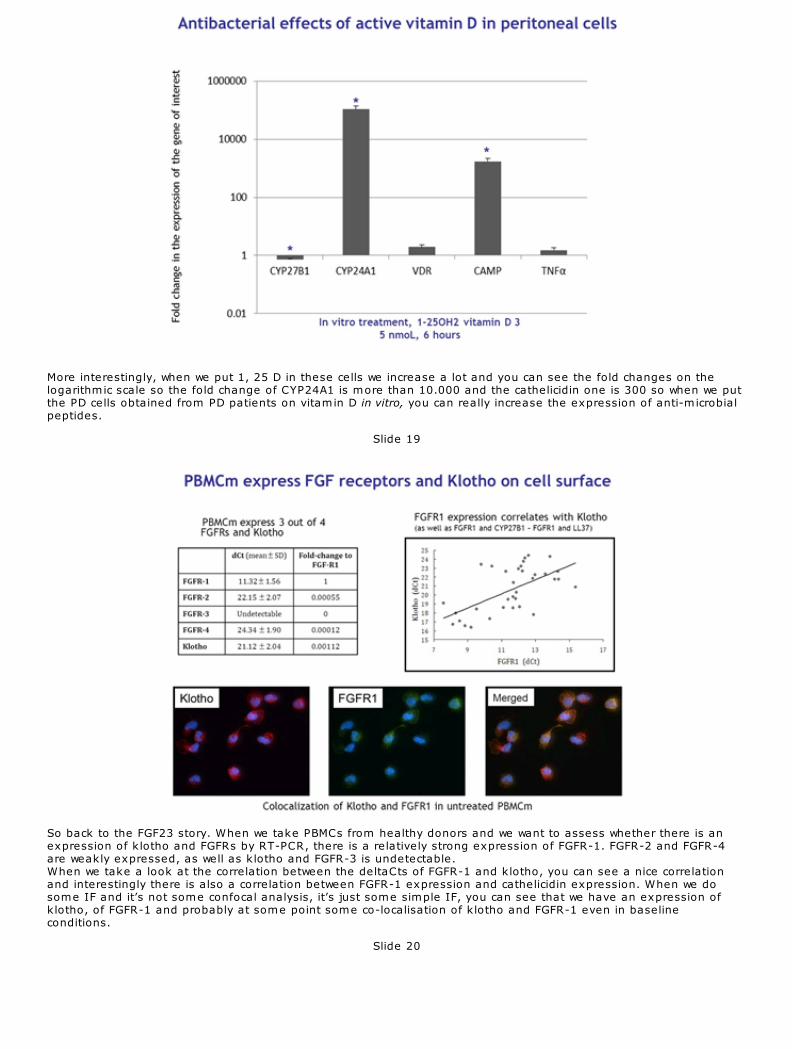
More interestingly, when we put 1, 25 D in these cells we increase a lot and you can see the fold changes on thelogarithmic scale so the fold change of CYP24A1 is more than 10.000 and the cathelicidin one is 300 so when we putthe PD cells obtained from PD patients on vitamin D in vitro, you can really increase the expression of anti-microbialpeptides.
Slide 19
So back to the FGF23 story. When we take PBMCs from healthy donors and we want to assess whether there is anexpression of klotho and FGFRs by RT-PCR, there is a relatively strong expression of FGFR-1. FGFR-2 and FGFR-4are weakly expressed, as well as klotho and FGFR-3 is undetectable. When we take a look at the correlation between the deltaCts of FGFR-1 and klotho, you can see a nice correlationand interestingly there is also a correlation between FGFR-1 expression and cathelicidin expression. When we dosome IF and it’s not some confocal analysis, it’s just some simple IF, you can see that we have an expression ofklotho, of FGFR-1 and probably at some point some co-localisation of klotho and FGFR-1 even in baselineconditions.
Slide 20
21/12/12 CME Slides Forum - J. Bacchetta
11/16ndt-educational.org/bacchettaslide2012.htm
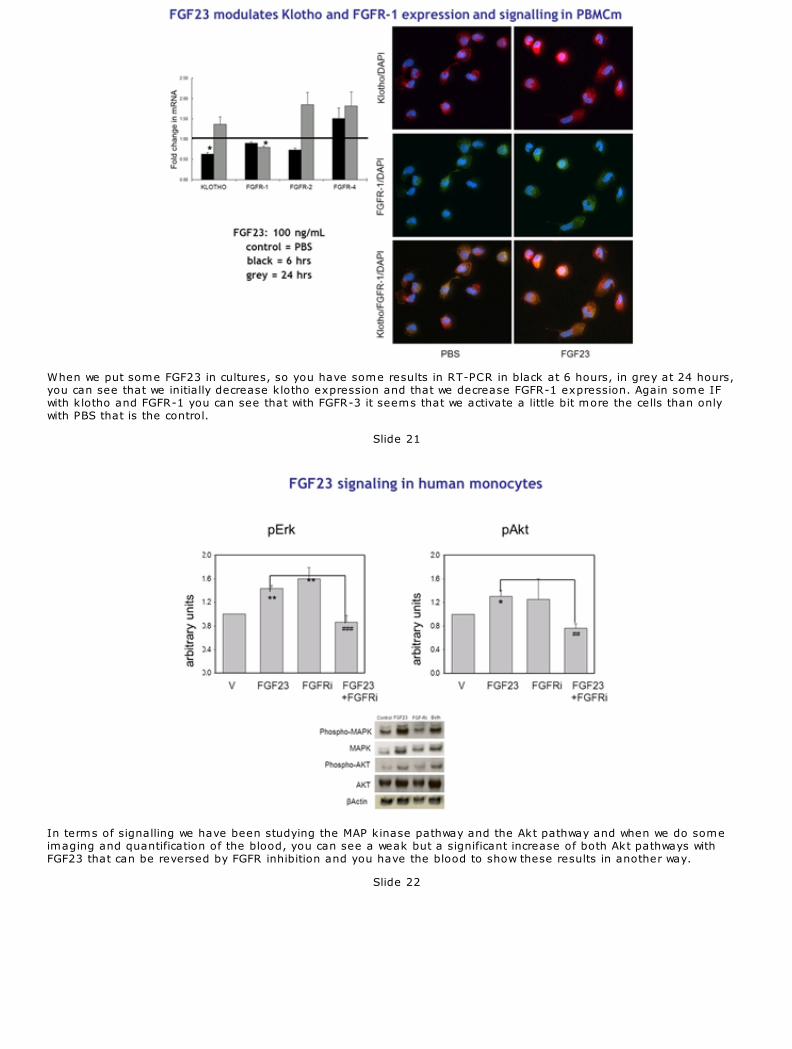
When we put some FGF23 in cultures, so you have some results in RT-PCR in black at 6 hours, in grey at 24 hours,you can see that we initially decrease klotho expression and that we decrease FGFR-1 expression. Again some IFwith klotho and FGFR-1 you can see that with FGFR-3 it seems that we activate a little bit more the cells than onlywith PBS that is the control.
Slide 21
In terms of signalling we have been studying the MAP kinase pathway and the Akt pathway and when we do someimaging and quantification of the blood, you can see a weak but a significant increase of both Akt pathways withFGF23 that can be reversed by FGFR inhibition and you have the blood to show these results in another way.
Slide 22
21/12/12 CME Slides Forum - J. Bacchetta
12/16ndt-educational.org/bacchettaslide2012.htm
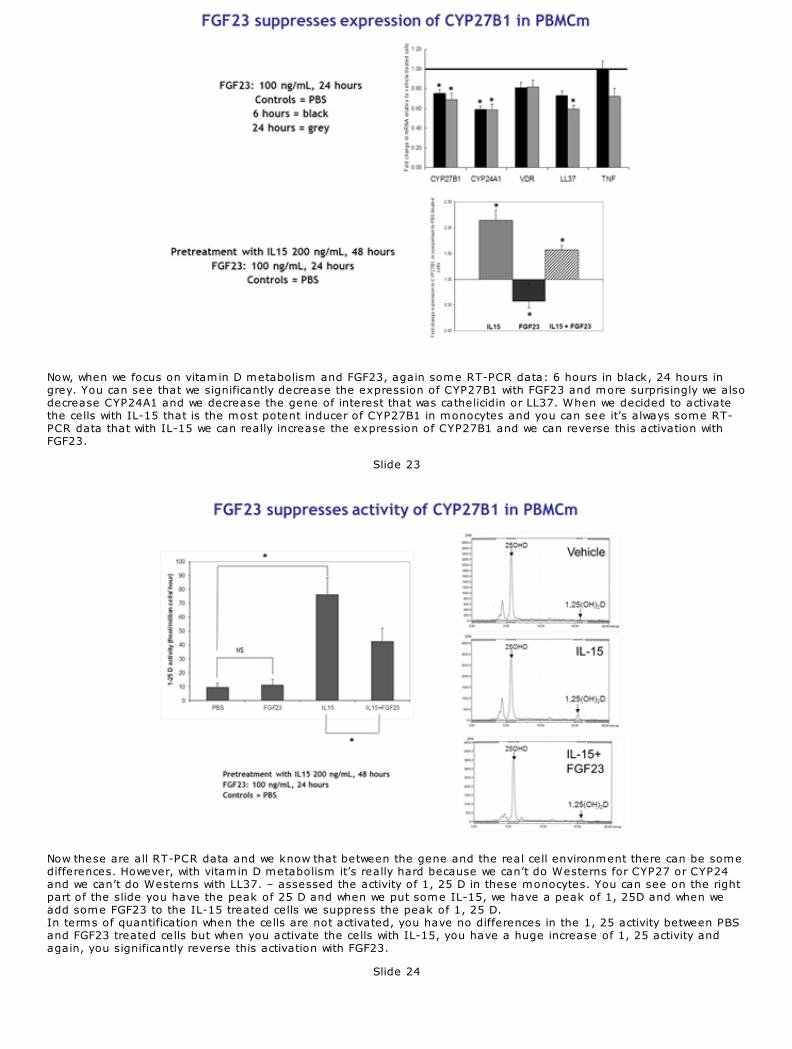
Now, when we focus on vitamin D metabolism and FGF23, again some RT-PCR data: 6 hours in black, 24 hours ingrey. You can see that we significantly decrease the expression of CYP27B1 with FGF23 and more surprisingly we alsodecrease CYP24A1 and we decrease the gene of interest that was cathelicidin or LL37. When we decided to activatethe cells with IL-15 that is the most potent inducer of CYP27B1 in monocytes and you can see it’s always some RT-PCR data that with IL-15 we can really increase the expression of CYP27B1 and we can reverse this activation withFGF23.
Slide 23
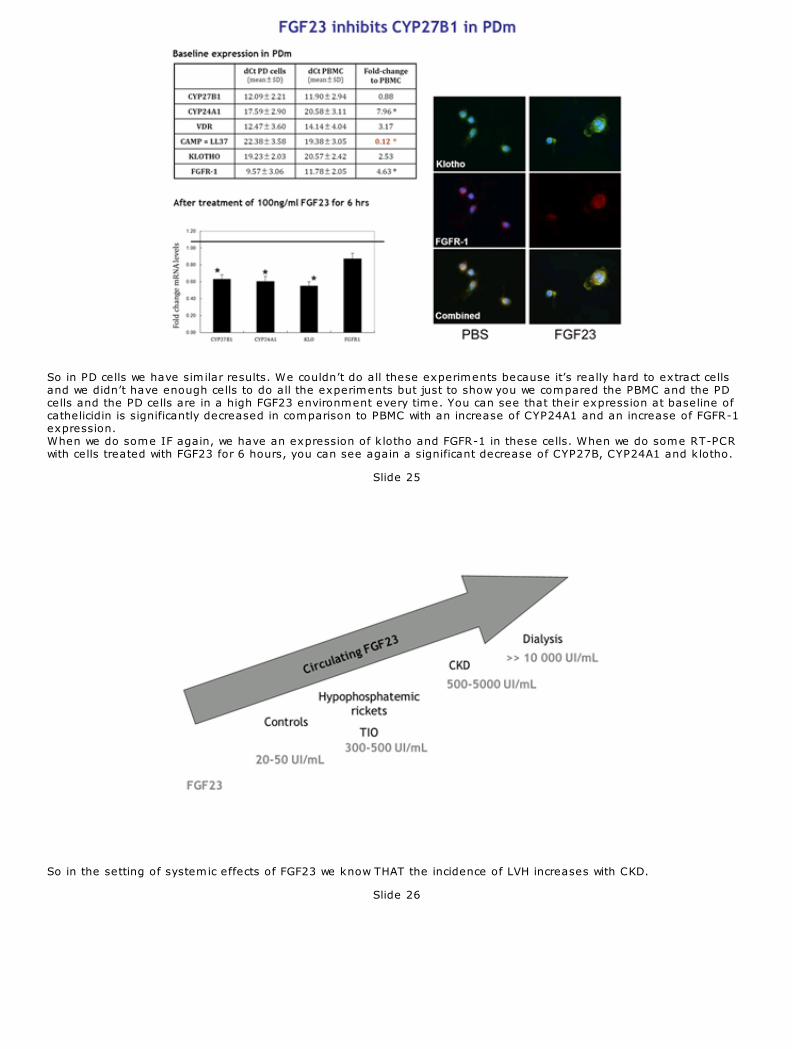
Now these are all RT-PCR data and we know that between the gene and the real cell environment there can be somedifferences. However, with vitamin D metabolism it’s really hard because we can’t do Westerns for CYP27 or CYP24and we can’t do Westerns with LL37. – assessed the activity of 1, 25 D in these monocytes. You can see on the rightpart of the slide you have the peak of 25 D and when we put some IL-15, we have a peak of 1, 25D and when weadd some FGF23 to the IL-15 treated cells we suppress the peak of 1, 25 D. In terms of quantification when the cells are not activated, you have no differences in the 1, 25 activity between PBSand FGF23 treated cells but when you activate the cells with IL-15, you have a huge increase of 1, 25 activity andagain, you significantly reverse this activation with FGF23.
Slide 24
21/12/12 CME Slides Forum - J. Bacchetta
13/16ndt-educational.org/bacchettaslide2012.htm
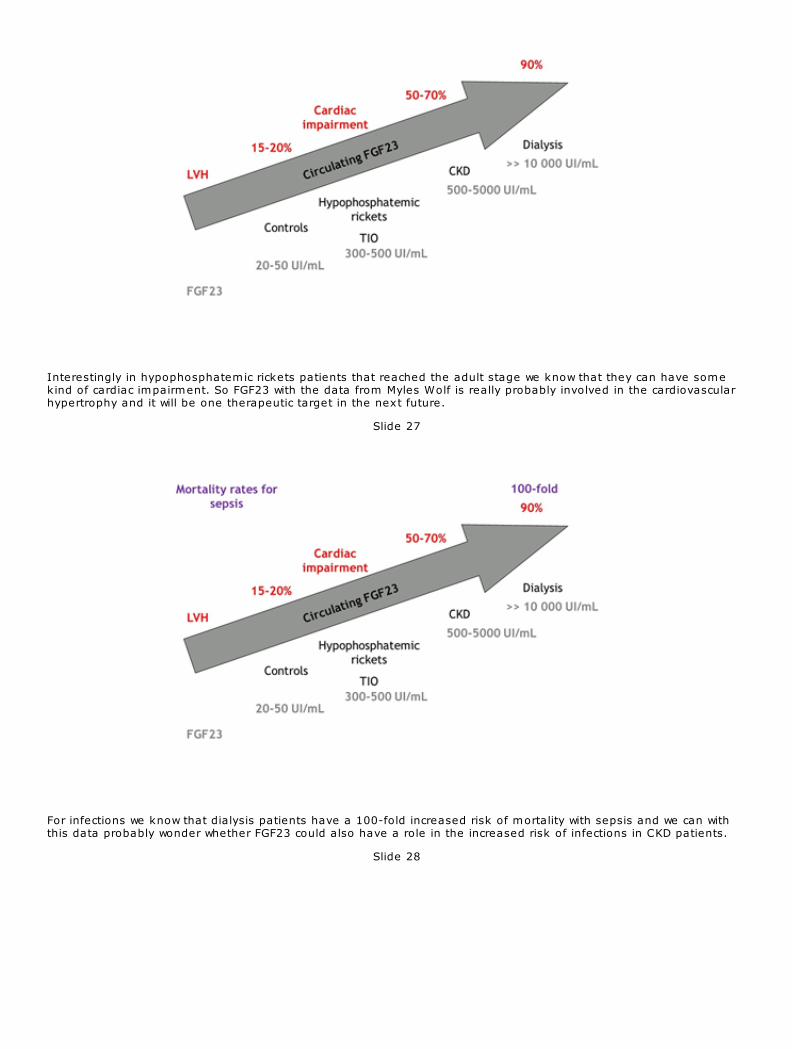
So in PD cells we have similar results. We couldn’t do all these experiments because it’s really hard to extract cellsand we didn’t have enough cells to do all the experiments but just to show you we compared the PBMC and the PDcells and the PD cells are in a high FGF23 environment every time. You can see that their expression at baseline ofcathelicidin is significantly decreased in comparison to PBMC with an increase of CYP24A1 and an increase of FGFR-1expression. When we do some IF again, we have an expression of klotho and FGFR-1 in these cells. When we do some RT-PCRwith cells treated with FGF23 for 6 hours, you can see again a significant decrease of CYP27B, CYP24A1 and klotho.
Slide 25
So in the setting of systemic effects of FGF23 we know THAT the incidence of LVH increases with CKD.
Slide 26
21/12/12 CME Slides Forum - J. Bacchetta
14/16ndt-educational.org/bacchettaslide2012.htm
Interestingly in hypophosphatemic rickets patients that reached the adult stage we know that they can have somekind of cardiac impairment. So FGF23 with the data from Myles Wolf is really probably involved in the cardiovascularhypertrophy and it will be one therapeutic target in the next future.
Slide 27
For infections we know that dialysis patients have a 100-fold increased risk of mortality with sepsis and we can withthis data probably wonder whether FGF23 could also have a role in the increased risk of infections in CKD patients.
Slide 28
21/12/12 CME Slides Forum - J. Bacchetta
15/16ndt-educational.org/bacchettaslide2012.htm
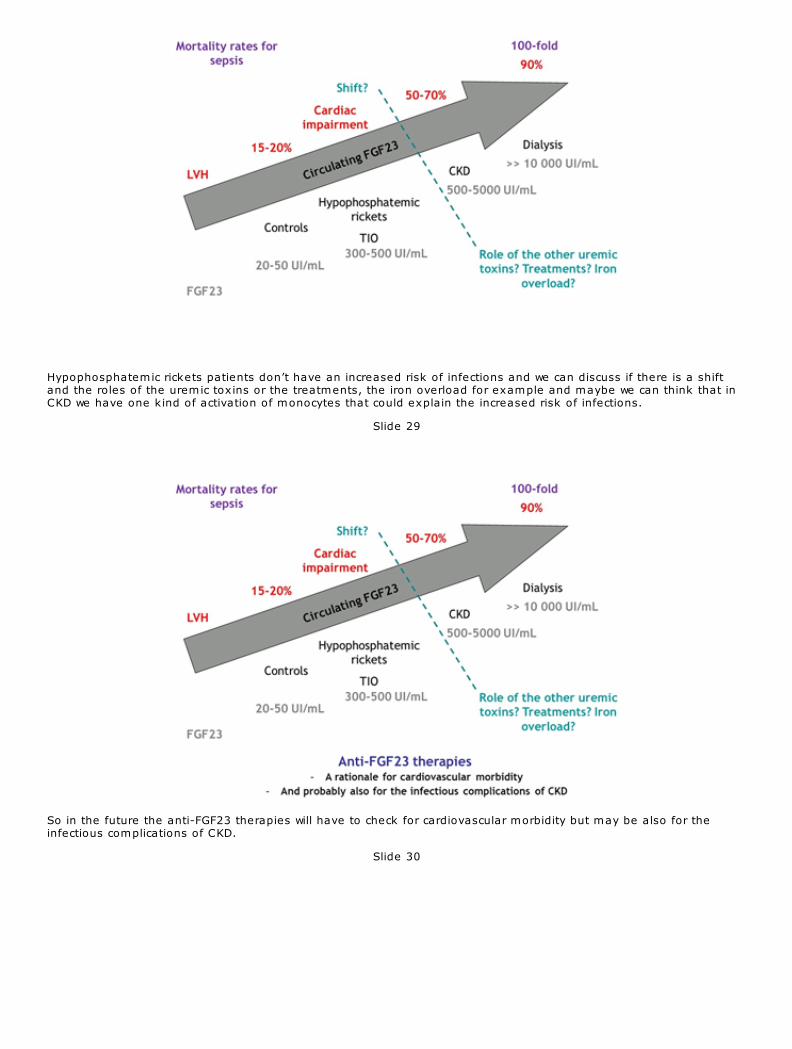
Hypophosphatemic rickets patients don’t have an increased risk of infections and we can discuss if there is a shiftand the roles of the uremic toxins or the treatments, the iron overload for example and maybe we can think that inCKD we have one kind of activation of monocytes that could explain the increased risk of infections.
Slide 29
So in the future the anti-FGF23 therapies will have to check for cardiovascular morbidity but may be also for theinfectious complications of CKD.
Slide 30
21/12/12
16/16ndt-educational.org/bacchettaslide2012.htm
I would like to thank the organisers for the invitation, all my mentors and mainly Martin Hewison and Isidro Saluskyat UCLA and Pierre Cochat in Lyon and all of you for your attention.





























