Embed Size (px)
Citation preview

2/22/2016
1
DO YOU SEE WHAT I SEE?VISUAL DISTURBANCES FOLLOWING STROKE
ACUTE STROKE BEST PRACTICES WORKSHOP
“ADVANCING BEST PRACTICES IN ACUTE STROKE CARE”FEBRUARY 23, 2016
Laura Swancar O.T. Reg (Ont.)
Stroke Occupational Therapist
VISUAL DEFICITS FOLLOWING STROKE:OUTLINE
Why is vision important?
Common visual disturbances following stroke
Homonymous Hemianopsia
Assessment
Strategies/treatment
Unilateral Spatial Neglect
Safe Mobility in Patients with visualdisturbances and/or neglect following stroke
The “How to”: Basic visual field confrontationtesting in acute stroke
VISION IS IMPORTANT BECAUSE….
A. It is our most farreaching sense.
B. Related closely tobalance, safety andfall prevention.
C. Important formotor and posturalcontrol.
D. A key part of allour daily lifeactivities.
E. All of the above.
WHY IS VISION IMPORTANT?
Vision is our most far reaching sense
Provides speed and instant identification ofobjects and situations
Vision and mobility, balance, safety
Important part of motor and postural control(closed eyes item on Berg balance test)
Vision and the older patient

2/22/2016
2
VISUAL PERCEPTUAL HIERARCHYADAPTATION THROUGH VISION
Adaptation throughVisual Cognition
Visual Memory
Pattern RecognitionScanning
Attention = Alert and Attending
Visual Acuity, Visual field, OcculomotorControl
Warren, 1993
VISUAL DEFICITS AND DAILY LIFE
How does the disability affect a person’s DAILYACTIVITIES, WORK, LIFE ROLES?
Self care – washing, dressing, toileting, grooming
Home and community management – driving,reading, cooking, finances
Return to work
Mobility – safety
THREE COMPONENT MODEL OF VISION
MITCHELL SCHEIMAN, OD, FCOVD
Visual IntegrityVisual acuity
Refraction
Eye Health
Visual Fields
VisualInformationProcessing
Visual spatial skills
Visual Analysis skills
Visual motor integrationskills
Visual EfficiencyAccomodation
Binocular vision
Eye Movements

2/22/2016
3
VISUAL PROCESSING
HOMONYMOUS HEMIANOPSIA IS…..
A. A special type oforganic milk.
B. A condition affectinghalf the population.
C. Blindness in half thevision in both eyes.
D. A visual field deficit.
E. C and D.
F. A and C.
HOMONYMOUS HEMIANOPSIA
Also called Visual Field deficit
Blindness in ½ visual field of each eye
Quadrantanopsia – ¼ visual field of each eye

2/22/2016
4
BEHAVIOURAL CHANGES IN
HOMONYMOUS HEMIANOPSIA
Adopt a narrow search pattern confined tomidline and sound side
Person scans very slowly towards deficit side
Missing and /or “misidentifying” visual detail onthe “blind” side
Reduced visual monitoring of the hand
May feel unsafe due to loss of peripheral vision
Decreased engagement, withdraws socially
VISUAL FIELD DEFICIT:DAILY LIVING CHALLENGES
Driving
Shopping and community events
Yard Work
Meal preparation
Financial management
Functional communication
Housekeeping
Self care - grooming
HOMONYMOUS HEMIANOPSIA
BEST STRATEGY - EDUCATION
Compensation requires conscious cognitivestrategy – increase visual search strategies.
Must believe vision cannot be trusted on deficitside.
Awareness allows client to develop “intellectualover-ride”.
Develop awareness through practice.
Provide an anchor on the affected side
Ensure important items are in their intact visual
field
Encourage pacing to scan slowly
Use low vision devices like magnifying lenses
Ensure adequate lighting
Watch for glare
Increase visual contrasts
MORE STRATEGIES
2/22/2016
5
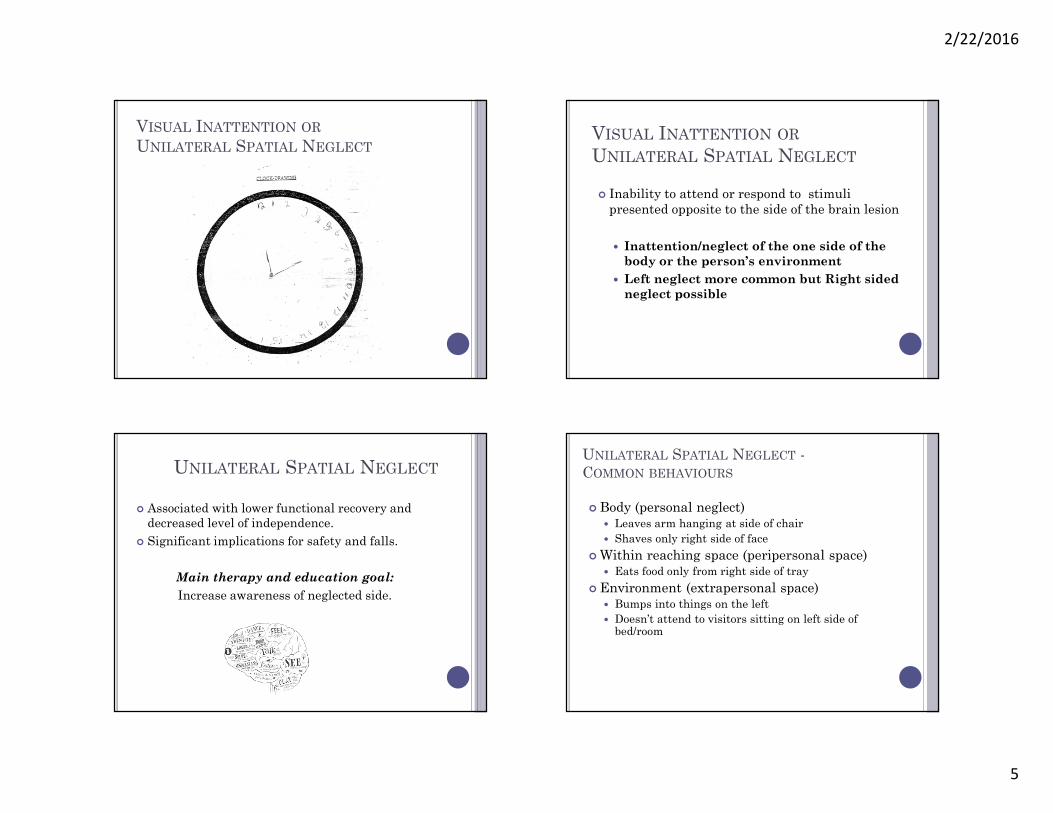
VISUAL INATTENTION OR
UNILATERAL SPATIAL NEGLECTVISUAL INATTENTION OR
UNILATERAL SPATIAL NEGLECT
Inability to attend or respond to stimulipresented opposite to the side of the brain lesion
Inattention/neglect of the one side of thebody or the person’s environment
Left neglect more common but Right sidedneglect possible
UNILATERAL SPATIAL NEGLECT
Associated with lower functional recovery anddecreased level of independence.
Significant implications for safety and falls.
Main therapy and education goal:
Increase awareness of neglected side.
UNILATERAL SPATIAL NEGLECT -COMMON BEHAVIOURS
Body (personal neglect) Leaves arm hanging at side of chair
Shaves only right side of face
Within reaching space (peripersonal space) Eats food only from right side of tray
Environment (extrapersonal space) Bumps into things on the left
Doesn’t attend to visitors sitting on left side ofbed/room

2/22/2016
6
STRATEGIES FOR VISUAL OR BODY NEGLECT
Ensure essential items, such as call bell,urinal, telephone are on good/intact side sothat they are accessible if needed
Approach the person on their best side (iefrom Right if left inattention)
Speak to person midline with eye contact –move to left side if possible
NEGLECT/INATTENTION
STRATEGIES CONTINUED
Position neglected arm in midline positionwithin visual field
Use a reference point or anchor
on left side
Help family to learn strategies byrespectful modeling and positivereinforcement
Encourage client to wash neglected side
Functional Category Observed Behaviour Strategies
Mobility
Walking
Wheelchair
transfers
Bumps into things/walls/people on the
left
FALLS, numerous close calls
Misses target in pivot transfers
-Supervision, frequent checks for needs
-Transfer belt, transfer to unaffected side
-Instructions to good side, eye contact
-Bed alarm
-grab bars for toilet/arm rests for chairs
ADL’s
washing
eating
toileting
grooming
dressing
Shave ½ face, eat ½ tray, wash ½ body
Clumsy/knocks over items
Misses important steps in tasks
Forgets to dress left side
-Position necessary items on good side
-Cues, reminder to wash left side
-Use anchor on left ie tea cup, red band, cell
phone
-Set up an organized and predictable
environment
-Dress affected side first, undress good side
first
Social Interactions Ignores visitors/family
Tires easily
Orients body and attention to right
side
-Help family to understand, teach strategies
-Encourage breaks/rest for client
Cognition/Thinking skills May have difficulty learning new skills
Poor insight and safety judgement
Difficulty reading
Inefficient visual scanning pattern
during activities ie ambulation
Rushes to complete tasks, no rechecks
-Important info to good side
-Respectful Repetition
-Supervision!
-Pay attention to level of cognitive FATIGUE
-Shorter sessions with frequent rests/breaks
UNILATERAL SPATIAL NEGLECT:STRATEGIES SUMMARY
VISUAL INATTENTION OR NEGLECT VERSUS
VISUAL FIELD DEFICIT: CONTINUUM
Visual neglect with noawareness
.….continuum……
Visual FieldDeficit with
full awareness

2/22/2016
7
Balance problems +visual deficits = high risk
for FALLS
SAFE MOBILITY IN PATIENTS
WITH HOMONYMOUS
HEMIANOSPIA
Fiona Maclean, Physiotherapist,
Regional Stroke Unit (RSU)
ALL STROKE PATIENTS SHOULD BE
CONSIDERED AT RISK OF FALLING
Presence of Unilateral Spatial Neglect has beenstrongly associated with increased risk of injury andwith poor functional outcomes
Patient’s have reduced ability to learn to compensatedue to the stroke, therefore repeated cuing andsupervision is required
PATIENTS WITH VISUAL FIELD DEFICIT
MAY:
Collide into their surroundings on one side(usually left) with walker or with their body
Fall if they run into objects or people, or trip overitems.
Most patients also have weakness and reducedbalance which makes it harder to regain balanceif they do bump into objects.

2/22/2016
8
HOW YOU CAN HELP WHEN WALKING WITH
PATIENT
Ensure both hands are on walker, may need toassist hand to stay on walker
Stand on the patients’ affected side
Provide cueing – verbal, tactile to assist patientto attend to affected side
Use walking aids, transfer belt, non slip shoes
Stay close to the patient
Tell patients to slow down
Encourage pt. to find a target to walk towards(chair, doorway, family member)
Have 2 assists when necessary
FALL PREVENTION
Stress importance of safety and calling for help toget out of bed (have call bell within visual field)
Bed alarms on, bed in lowest position
Attach call bell to pts. gown if you think they arelikely to get up on their own
Toileting regime (pts often fall trying to get towashroom on time)
Transfer to the unaffected side
Don’t rush
Don’t attempt to transfer or walk with a patientif you don’t feel it is safe
A WORD ABOUT MOBILITY AND ATAXIA
Patients who present with co-ordinationproblems can be difficult to manage whenwalking
They often present with good strength but can bevery unsteady walking due to lack of control intheir legs
Often walkers do not provide the support theyneed
May require 2 assists to transfer and walk
TAKE HOME MESSAGE
Vision is a complex and important function
for everyday functioning.
Many older clients already have
decreased vision.
Make visual screening a regular part
of your assessment.
Know how to screen for common visual
issues.
SAFETY! Monitor clients with suspected visualinattention or field deficits closely to preventfalls.

2/22/2016
9
BASIC VISUAL SCREENING
Remember EYEGLASSES and room lighting
Visual fields – confrontation testing
Right, Left , both together
Upper, Middle, Lower quadrants
Visual Acuity – object identification and reading.
Occulomotor control – horizontal and verticalvisual tracking
Visual inattention/neglect – clinical observations
YOUR TURN:VISUAL FIELD CONFRONTATION TESTING
FOR ACUTE STROKE PATIENTS
Sitting face to face, eyes at same level, test one eye ata time, then with both eyes open to look forinattention.
Testing procedure:1. Patient covers left eye. Test four quadrants of Right eye.
2. Patient covers right eye. Test four quadrants of Left eye. Can use ‘number of fingers’ and ‘wiggling fingers’.
3. Both eyes open: Test both Right and Left together toscreen for visual inattention.
**?Where to position your fingers? If you can see it, then thepatient can see it.**
REFERENCES
Harvey, R., Macko, R., Stein, J., Winstein., C. & Zorowity. R. (2009).Stroke Recovery and Rehabilitation. Demo Medical Publishing, LLC.
Lotery, A.J., Wiggam, M.I., Jackson, J., Silvestri, G., Refson, K.Fullerton,K.J., et all. (2000). Correctable visual impairment in stroke rehabilitationpatients. Age and Ageing, 29, 221-222.
Pedretti, L. (2001). Occupation Therapy : Pracitce Skills for PhysicalDysfunction. Elsevier Science Health Science Division: Evaluation andTreatment of Visual Deficits Following Brain Injury (p. 532 – 572).
Scheiman, M. (2014). Understanding and Managing Visual Deficits afterStroke: A Guide for Therapists.
Warren, M. (1996). Pre-reading and Writing Exercises for Persons withMacular Scotomas. visABILITIES Rehab Services Inc.
Zoltan, B. (2007). Vision, Perception and Cognition. A Manual for theEvaluation and Treatment of the Adult with acquired Brain Injury, 4th
Ed. SLACK incorporated.







![SCISCITATOR 2015 · [1]. Riverine communities experience two main types of disturbances: natural disturbances and anthropogenic disturbances. Natural disturbances in riverine ecosystems](https://img.dokumen.tips/doc/110x75/5f27dd3959f0c41da22eeec5/sciscitator-1-riverine-communities-experience-two-main-types-of-disturbances.jpg)






















