Embed Size (px)
Citation preview
Available online at www.sciencedirect.com
Computers in
Computers in Human Behavior 24 (2008) 1032–1040
Human Behavior
www.elsevier.com/locate/comphumbeh
Viability of virtual reality exposure therapyas a treatment alternative
Jimmy Bush *
Iowa State University, Human Computer Interaction, 388 Marblerock Way, Lexington,
KY 40503, United States
Available online 10 May 2007
Abstract
Virtual reality (VR) has garnered the interest of many scientific communities over the last decade.One promising track of research lies in VR exposure therapy (VRET), where gradual exposure to anegative stimulus is used to reduce anxiety. Virtual exposure is desirable in many situations, as it canbe less intimidating and less expensive than traditional in vivo treatment with much the same success.Examining the benefits and drawbacks of VRET is an important first step toward an accurate assess-ment of its viability as a treatment alternative. This paper will review current literature on the topicof VRET and answer several questions regarding the viability of the treatment. It will also providesome additional research direction for improving the case for mainstreaming VRET.� 2007 Elsevier Ltd. All rights reserved.
Keywords: Virtual reality; Psychotherapy; Treatment effectiveness evaluation; Anxiety disorders; Exposuretherapy
1. Introduction
Anxiety disorders run rampant in society today. Currently, 18% of American adultssuffer the effects of some form of anxiety disorder (Kessler, Chiu, Demler, and Walters,as cited in National Institute of Mental Health [NIMH], 2006). Kessler et al. found thatspecific phobias afflict some 19 million of these adults and social anxiety disorder about15 million, with several million more plagued by generalized anxiety disorder, post
0747-5632/$ - see front matter � 2007 Elsevier Ltd. All rights reserved.
doi:10.1016/j.chb.2007.03.006
* Tel.: +1 859 232 2792; fax: +1 859 232 5649.E-mail address: [email protected]
J. Bush / Computers in Human Behavior 24 (2008) 1032–1040 1033
traumatic stress disorder, or panic disorder. Given time, these disorders can trap the indi-vidual in patterns of worry and avoidance. Hyman and Rudorfer (as cited in NIMH) alsopoint out that these disorders have proven responsive to medicinal or psychotherapeutictreatment, or a combination thereof. Medicinal treatment is outside the scope of this paper.
However, many such disorders go untreated. Garcia-Palacios, Hoffman, Carlin, Fur-ness, and Botella (2002) point to several studies indicating that 60–85% of specific phobiasufferers may never seek treatment. Unless the disorder causes an unacceptable hardship,many choose avoidance over treatment (NIMH, 2006), since even considering facing theirfears induces strong anxiety. Fear of public breakdown and embarrassment can also keepan afflicted person from treatment (Juan et al., 2005).
The most widely accepted form of psychotherapy for dealing with anxiety disorder iscognitive behavior therapy (CBT). CBT trains patients to change their patterns of thinkingand action to prepare them to face their fears (NIMH, 2006). Once the patient is ready, thetherapist will expose the patient to the feared stimulus using one of two methods. Imaginal
exposure uses the imagination to recreate a feared situation, while in vivo exposure uses aphysical recreation of the feared situation.
It is generally agreed that for exposure therapy to work, the patient must feel the sameanxiety as they feel in the actual situation. Imaginal exposure therapy is attractive due tothe safety of an office setting and the confidentiality that setting provides (Riva, Molinari,& Vincelli, 2002). Imaginal exposure therapy’s success hinges largely on the patient’s abil-ity to elicit the same level of anxiety, making its results unpredictable. In vivo exposuretherapy is more effective at eliciting anxiety, as the feared stimulus is often faced directly.However, this prospect is daunting for the patient, and the procedure can be costly, espe-cially for treatment of fear of flying, as it is expensive to schedule real-life flying experi-ences. Also, the environment is unpredictable, giving the therapist little control over thepatient’s experience and increasing the risk of public embarrassment. Still, in vivo expo-sure is generally preferred, as it has a higher success rate (Krijn, Emmelkamp, Olafsson,& Biemond, 2004).
2. Defining virtual reality exposure therapy (VRET)
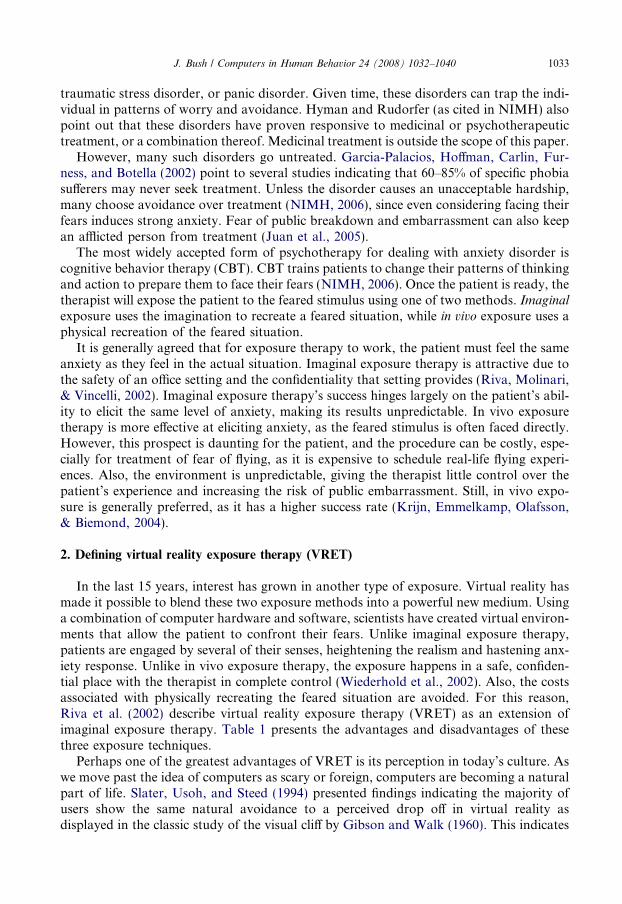
In the last 15 years, interest has grown in another type of exposure. Virtual reality hasmade it possible to blend these two exposure methods into a powerful new medium. Usinga combination of computer hardware and software, scientists have created virtual environ-ments that allow the patient to confront their fears. Unlike imaginal exposure therapy,patients are engaged by several of their senses, heightening the realism and hastening anx-iety response. Unlike in vivo exposure therapy, the exposure happens in a safe, confiden-tial place with the therapist in complete control (Wiederhold et al., 2002). Also, the costsassociated with physically recreating the feared situation are avoided. For this reason,Riva et al. (2002) describe virtual reality exposure therapy (VRET) as an extension ofimaginal exposure therapy. Table 1 presents the advantages and disadvantages of thesethree exposure techniques.
Perhaps one of the greatest advantages of VRET is its perception in today’s culture. Aswe move past the idea of computers as scary or foreign, computers are becoming a naturalpart of life. Slater, Usoh, and Steed (1994) presented findings indicating the majority ofusers show the same natural avoidance to a perceived drop off in virtual reality asdisplayed in the classic study of the visual cliff by Gibson and Walk (1960). This indicates
Table 1Comparison of exposure therapy techniques
Imaginal In vivo Virtual reality
Advantages Disadvantages Advantages Disadvantages Advantages Disadvantages
Low setup cost Difficult anxietalresponse
Easy anxietal response Not confidential Complete therapistcontrol
High setup cost
Private and confidential Limited therapistcontrol
Proven high successrate
High risk ofembarrassment
Private and confidential Unfamiliar totherapists
Low risk ofembarrassment
Low success rate Familiar to therapists Limited therapist control Low risk ofembarrassment
Low treatment cost High treatment cost Low treatment costFamiliar to therapists Unappealing to patients Emerging high success
rateEasy anxietal responseAppealing to patients
1034J
.B
ush
/C
om
pu
tersin
Hu
ma
nB
eha
vior
24
(2
00
8)
10
32
–1
04
0

J. Bush / Computers in Human Behavior 24 (2008) 1032–1040 1035
that users are likely to accept the virtual world as a mirror of reality, governed by the samephysics and similarly approachable. Garcia-Palacios, Hoffman, See, Tsai, and Botella(2001) conducted a survey of a large sample of college students to determine their prefer-ence between in vivo therapy and VRET in treatment of a fear of spiders. Their resultsoverwhelmingly leaned toward VRET. Even if this sample set is not indicative of the pop-ulation as a whole, it bodes well for success in the future. It stands to reason that patientswill be more hesitant about the real stimulus than a virtual reproduction.
3. Virtual reality exposure therapy in practice
Understanding the usefulness of VRET begins with understanding how it manifestsitself in a treatment scenario. This can change depending on the type of anxiety disorderunder treatment. Acrophobia, or fear of heights, lends itself to a spacious though relativelystatic virtual scene with the patient having the ability to move within the scene. Panic dis-order and agoraphobia, the fear of going outdoors, warrants virtual scenes that are smalland enclosed with static humans crowding the space. Fear of flying concentrates on a par-ticular feared environment of the airport and airplane.
3.1. Acrophobia
One very helpful resource when evaluating the procedure of VRET is the acrophobiastudy done by Emmelkamp et al. (2002). Their study is constructed to test the relativeeffectiveness of treating fear of heights with VRET and in vivo exposure as faithfully aspossible. To this end, the virtual scenes are reproductions of the actual environments usedin the in vivo treatment. Treatment time was short, consisting of 4 weekly sessions ofabout 1 h. In the in vivo exposure, patients were placed in the areas designed to invokefear response and were guided and encouraged by the therapists. They were repeatedlychallenged to look down, and they were polled for their perceived fear level throughoutthe experience.
The virtual exposure therapy was conducted in much the same way. The patient wasexposed to an environment that invoked fear, and as the patient gained confidence inthe environment, the therapist evaluated the self-assessed fear level to best determinethe time to switch environments. The therapist was able to see the view shown to thepatient by way of a computer monitor. There was also a short break in the middle ofthe virtual reality sessions to minimize fatigue and motion sickness. Sense of reality wasenhanced by a handrail that could be seen and held.
Thirty-three patients participated (16 VR, 17 in vivo) and were evaluated before andafter the regiment of treatment, and 6 months after treatment concluded there was a fol-low-up. The results showed very similar results after treatment and at the follow-up. Bothtreatments were effective in treating the phobia and had lasting results.
3.2. Panic disorder and agoraphobia
Agoraphobia stems from anxiety over having panic attacks in public places. Obviouslythis phobia would be particularly hard to treat using in vivo exposure, due to the high riskof embarrassment for the patient. Virtual reality exposure therapy must therefore recreatethese public places and allow the patient to gradually adapt to the situation. Botella et al.
1036 J. Bush / Computers in Human Behavior 24 (2008) 1032–1040
(2004) present an excellent implementation of a virtual scenario for treatment of agora-phobia. Their implementation is a series of virtual scenes woven into a task scenario.The patient begins in virtual living area and checks a message left by a friend on theanswering machine. The friend asks the patient to do something, such as buying milk.From there, the patient progresses from the room to the elevator to public transportationto the mall where the task can be completed. Each of these stages can induce anxiety, andthe therapist can vary the crowdedness of the scenes to increase anxietal response. Noresults are presented in this paper.
3.3. Fear of flying
Fear of flying can take many forms, as many different parts of the flight experience caninduce anxiety. Hodges, Rothbaum, Watson, Kessler, and Opdyke (1996) present a virtualairplane that would take off, fly, and land in normal or stormy conditions. The virtualscene was comprised of a painstakingly constructed replica of the interior of an aircraft,with storminess and motion depicted through the windows of the airplane and enhancedby appropriate sound effects. Work by Banos et al. (2002) takes a more encompassingview, including in the study the anxiety in trip preparation and arrival at the airport. Bothwere successful in treating the patients.
4. The big questions of the wary therapist
At the heart of every therapeutic act is the hope for healing. Therefore, careful consid-eration must be lent to new treatment options to maximize the therapist’s ability to treateffectively. Chasing fanciful dreams can waste as much time as ignoring superior practices.While we have discussed the existence of VRET and its advantages over traditional treat-ment techniques, many questions remain before recommendations can be made regardingits viability as a treatment alternative.
4.1. What are the risks of VRET?
One of the first questions a responsible therapist is likely to ask concerns the safety ofthe procedure. Motion sickness is a primary concern of many therapists and researchers.Golding (2006) states that it is difficult to predict motion sickness susceptibility on an indi-vidual basis, but there are some basic factors that can minimize the effect of a given virtualenvironment. Image lag, or the responsiveness of displayed image to head motion, cangreatly impact motion sickness. Draper (as cited in Golding) finds that image updatelag of as little as 48 ms can induce motion sickness. For this reason, it is desirable to havea sufficiently faster frame rate. Another indicator of motion sickness is length of exposure.Several studies, including Krijn et al. (2004), have included breaks during the treatmentsession to reduce such effects.
Another well-studied risk of VRET is dropout due to lack of anxietal response. Pres-ence is the feeling of being within a virtual environment, looking past the reality of tech-nological presentation (Krijn, Emmelkamp, Biemond et al., 2004). This study showed alack of presence to be a factor in completion of the experiment. Several factors can influ-ence presence, and some recommended practices to maximize presence are discussed later.However, presence unfortunately is highly individualistic, and therefore is outside of a
J. Bush / Computers in Human Behavior 24 (2008) 1032–1040 1037
therapist’s complete control. Presence is often seen as an essential ingredient to successfultreatment, as the virtual environment must produce the same anxiety that the real one doesto elicit change (Vincelli & Riva, 2002).
A patient’s readiness for change can also influence the results (Vincelli & Riva, 2002).Several of the case studies in various VRET treatments mention a driving factor thatcaused the participant to seek treatment. Wald and Taylor (2000) show a woman moti-vated by employment to alleviate her fear of driving. Botella et al. (1998) report a studyof claustrophobia treatment arising from a patient’s personal health motivation and desireto undergo a CTS scan to diagnose back pain. With motivation comes receptivity, andwith receptivity comes presence.
4.2. Will VRET produce positive results?
Once it is decided that the risks of harm to the patient are minimal, the next questionto be answered is whether the treatment is effective in producing the desired results.Over 50 therapeutic experiments have been performed to date, with more than 95%reporting success. These controlled studies and case studies have focused on the effec-tiveness of treating phobias with VRET. Krijn, Emmelkamp, Olafsson et al. (2004) pro-vide a good review of the results of about 30 of these individual experiments. Insummary, VRET has been shown as effective in treating acrophobia (fear of heights),fear of flying, and fear of spiders. Other anxiety disorders, such as fear of driving, claus-trophobia (fear of enclosed spaces), agoraphobia (fear of the outdoors)/panic disorder,social phobia, and post-traumatic stress disorder, have shown some promise in limitedresearch.
Perhaps the most useful research compares virtual reality exposure therapy (VRET) toexisting treatment techniques. Wiederhold et al. (2002) studied fear of flying and the effec-tiveness of VRET versus imaginal exposure therapy (IET). Several indicators showedVRET to be superior to IET in this study. One indicator was the self-reported anxiety dur-ing the experiment, which as previously mentioned is key to effective exposure therapy.Another indicator was the ability to fly without anxiety or medication at a three monthfollowup. Emmelkamp et al. (2002) compared VRET to in vivo exposure therapy in thetreatment of fear of heights. VRET is shown to be equally effective as in vivo exposurein the reduction in anxiety.
4.3. Is VRET cost-effective?
As it has been shown that VRET seems to be as effective as in vivo treatment, the realcost basis for investing in VRET lies in the existing expense of in vivo treatment, which canbe high for a number of reasons. Fear of flying seems especially expensive to treat, as thecost per flight is likely to be hundreds of US dollars. Also, there may be other costs, liketravel time to the nearest airport. This could also result in longer therapy sessions, whichcould preclude healthcare insurance reimbursement (Rothbaum, Hodges, Smith, Lee, &Price, 2000).
Another consideration is the return on the investment. As previously stated, VRET ismore appealing than other therapy options, which could mean increased business andnotoriety. Also, groups with a vested interest may be willing to help. Banos et al. (2002)cites a report that the airline industry lost $16 million in 1982 due to fear of flying. While
1038 J. Bush / Computers in Human Behavior 24 (2008) 1032–1040
this would tend to abate with acceptance, recent terrorist activity may make treatmentresearch as important as ever.
As for the actual cost of the systems, they vary greatly depending on the technology.The most expensive option is the computer automated virtual environment (CAVE).These range in size and price but are likely to cost over $1 million (Messner, Yerrapathr-uni, Baratta, & Whisker, 2003). Head mounted displays (HMDs) are considerably lessexpensive. Virtually Better, Inc., a company specializing in VR therapy solutions, recom-mends a $549 HMD for use with their applications (http://www.virtuallybetter.co/hard-ware.htm). Little research has been done to assess the relative effectiveness of these twotechnologies, but Krijn, Emmelkamp, Biemond et al. (2004) showed no statistical differ-ence in the success of the two methods in treating fear of heights. In the future, other dis-play technologies may be proven effective, but for now these two technologies are the mostwidely accepted.
Apart from the display technology, there may also be some other costs. Software islikely to be costly, though there are some freeware or open source solutions available.Another cost may lie in the additional hardware setup. Some display techniques or soft-ware programs may require significant computing power. The therapist’s monitoring sta-tion may require a little additional hardware for video or sound transmission. Also,hardware allowing the patient to interact with the virtual environment may be necessary,including hardware granting the ability to move within a virtual scene or to handle virtualobjects.
4.4. What is my role in treatment?
Another question many face is the therapist’s role in the VR treatment session itself.One of the primary functions of the therapist surrounds incremental exposure to fearedstimuli. The therapist monitors the patient, at times encouraging or guiding the patient,and decides when to administer the next step of the exposure. For example, Juan et al.(2005) used an augmented reality system for the treatment of fear of spiders. Here, thetherapist controls the number and size of the spiders present.
Another responsibility of the therapist is to measure the anxietal response of thepatient. One test that is common in much of the research is the subjective units of distressscale (SUDS), a self-evaluation of anxiety level, often with a range of zero (low anxiety) to10 or 100 (high anxiety). Other tests may include assessment tests to quantify the pretreat-ment state and the effectiveness of treatment, as well as physiological monitoring of bloodpressure, heart rate, or skin conductance. Several studies used instruction on the copingtechniques such as controlled breathing prior to VRET (Rothbaum et al., 2000; Wieder-hold et al., 2002).
5. Best practices for maximizing success
When the system finally comes together and is ready for use, there are some consider-ations that can increase the effectiveness of the procedure. One of the most freeing find-ings, noted by Strickland, Hodges, North, and Weghorst (1997), is that precise realismis not as important as continuity. This suggests that rough modeling can be done withoutrisking success, that presence is more important than perfection. Jang et al. (2002) con-ducted a study on acrophobia treatment and paid special attention to the therapeutic envi-

J. Bush / Computers in Human Behavior 24 (2008) 1032–1040 1039
ronment. They observed that their head-mounted display (HMD) allowed the patients tosee their feet, minimizing presence through distraction. To remedy this situation, the lightswere lowered in the treatment room. Also, the location of the therapist in the treatmentroom diminished presence, as the subjects would focus on therapist’s location rather thanthe virtual scene, especially in high anxiety situations. This was corrected by moving thetherapist into a separate observation room with microphone communication.
Another study that deals greatly with maximizing user presence comes from a far dif-ferent source. Pausch, Snoddy, Taylor, Watson, and Haseltine (1996) released a studybased on their experience developing an amusement park VR experience. While notdirectly related to VRET, the large sample size (45000) is intriguing, and some of the sameprinciples hold. For instance, an uncomfortably warm room could negatively affect pres-ence. Also, inconsistencies in the environment cause instantaneous loss of presence thatcan destroy the effectiveness of the rest of the session. Head-mounted display comfortwas a concern raised by both studies.
6. Future research
Despite the growing popularity of VRET, many more areas of research still promisefruit. Studies comparing virtual reality exposure to in vivo exposure for other types of anx-iety disorders continue to be important for increasing acceptance of this new treatmenttechnique. Another area of focus is lowering the cost of operating a VR system by findingcheaper transmission techniques. Cliburn (2004) describes one $1500 system where theimage is displayed on two projectors, polarized to allow the eye to see in three dimensions.Tichon and Banks (2006) investigate using a desktop PC to execute and display the virtualenvironment. A third possible focus area would be VRET treatment protocols for variousanxiety disorders.
7. Conclusion
As virtual reality exposure therapy gains acceptance and support, it moves naturallyfrom a research topic to a desirable patient application. While many areas of anxiety dis-orders have not been fully explored, the limited testing has shown promise. As the hard-ware becomes less and less expensive, budget concerns give way to ability for greaterimpact. As the software base expands and becomes more usable, technological trepidationcan be replaced by confident care. Ultimately, the goal of adopting new practices is alwaysto try to better help people, and with the strong appeal of VRET, a whole new populationmay finally break free.
References
Banos, R. M., Botella, C., Perpina, C., Alcaniz, M., Lozano, J. A., Osma, J., et al. (2002). Virtual reality
treatment of flying phobia [Electronic version]. IEEE Transactions on Information Technology in Biomedicine,
6, 206–212.Botella, C., Banos, R. M., Perpina, C., Villa, H., Alcaniz, M., & Rey, A. (1998). Virtual reality treatment of
claustrophobia: a case report [Electronic version]. Behaviour Research and Therapy, 36, 239–246.Botella, C., Villa, H., Garcia-Palacios, A., Banos, R. M., Perpina, C., & Alcaniz, M. (2004). Clinically significant
virtual environments for the treatment of panic disorder and agoraphobia [Electronic Version]. CyberPsy-
chology and Behavior, 7(5), 527–535.
1040 J. Bush / Computers in Human Behavior 24 (2008) 1032–1040
Cliburn, D. (2004). Virtual Reality for small colleges [Electronic version]. Journal of Computing Sciences in
Colleges, 19(4), 28–38.Emmelkamp, P. M. G., Krijn, M., Hulsbosch, A. M., de Vries, S., Schuemie, M. J., & van der Mast, C. A. P. G.
(2002). Virtual reality treatment versus exposure in vivo: a comparative evaluation in acrophobia [Electronic
version]. Behaviour Research and Therapy, 40, 509–511, 516.Garcia-Palacios, A., Hoffman, H., Carlin, A., Furness, T. A., III, & Botella, C. (2002). Virtual reality in the
treatment of spider phobia: a controlled study [Electronic version]. Behaviour Research and Therapy, 40,983–993.
Garcia-Palacios, A., Hoffman, H. G., See, S. K., Tsai, A., & Botella, C. (2001). Redefining therapeutic success
with virtual reality exposure therapy. CyberPsychology and Behavior, 4, 341–348, Retrieved October 15, 2006,fromhttp://www.liebertonline.com/toc/cpb/4/3.
Gibson, E. J., & Walk, R. D. (1960). The visual cliff [Electronic version]. Scientific American, 202, 64–71.Golding, J. F. (2006). Motion sickness susceptibility [Electronic version]. Autonomic Neuroscience, 129, 67–76.Hodges, L. F., Rothbaum, B. O., Watson, B., Kessler, G. D., & Opdyke, D. (1996). A Virtual airplane for fear of
flying therapy [Electronic version]. In: Proceedings of the IEEE virtual reality annual international symposium,1996, (pp. 86–93).
Jang, D. P., Ku, J. H., Choi, Y. H., Wiederhold, B. K., Nam, S. W., Kim, I. Y., et al. (2002). The development of
virtual reality therapy (VRT) system for the treatment of acrophobia and therapeutic case [Electronic version].IEEE Transactions on Information Technology in Biomedicine, 6, 213–217.
Juan, M. C., Alcaniz, M., Monserrat, C., Botella, C., Banos, R., & Guerrero, B. (2005). Using augmented reality
to treat phobias [Electronic version]. IEEE Computer Graphics and Applications, 25(6), 31–37.Krijn, M., Emmelkamp, P. M. G., Biemond, R., de Wilde de Ligny, C., Schuemie, M. J., & van der Mast, C. A. P.
G. (2004). Treatment of acrophobia in virtual reality: The role of immersion and presence [Electronic version].Behaviour Research and Therapy, 42, 229–239.
Krijn, M., Emmelkamp, P. M. G., Olafsson, R. P., & Biemond, R. (2004). Virtual reality exposure therapy of
anxiety disorders: A review [Electronic version]. Clinical Psychology Review, 24, 259–281.Messner, J.I., Yerrapathruni, S.C.M., Baratta, A.J., & Whisker, V.E. (2003). Using virtual reality to improve
construction engineering education. In: Proceedings of the 2003 American society for engineering education
annual conference and exposition. Retrieved October 27, 2006, from http://www.asee.org/acPapers/2003-2034_Final.pdf.
National Institute of Mental Health. (2006). Anxiety disorders [Brochure]. NIH Publication No. 06-3879.Retrieved October 15, 2006, from http://www.nimh.nih.gov/publicat/NIMHanxiety.pdf.
Pausch, R., Snoddy, J., Taylor, R., Watson, S., & Haseltine, E. (1996). Disney’s Aladdin: First steps towardstorytelling in virtual reality [Electronic version]. In: Proceedings of the 23rd annual conference on computer
graphics and interactive techniques, (pp. 193–203).Riva, G., Molinari, G., & Vincelli, F. (2002). Interaction and presence in the clinical relationship: Virtual reality
(VR) as communicative medium between patient and therapist [Electronic version]. IEEE Transactions on
Information Technology in Biomedicine, 6, 198–205.Rothbaum, B. O., Hodges, L., Smith, S., Lee, J. H., & Price, L. (2000). A controlled study of virtual reality
exposure therapy for the fear of flying [Electronic version]. Journal of Consulting and Clinical Psychology, 68,1020–1026.
Slater, M., Usoh, M., & Steed, A. (1994). Steps and ladders in virtual reality [Electronic version]. RetrievedMarch 6, 2007 from http://www.cs.umu.se/kurser/TDBD12/HT01/papers/slater94step.pdf.
Strickland, D., Hodges, L., North, M., & Weghorst, S. (1997). Overcoming phobias by virtual exposure
[Electronic version]. Communications of the ACM, 40(8), 34–39.Tichon, J., & Banks, J. (2006). Virtual reality exposure therapy: 150-Degree screen to desktop PC.
CyberPsychology and Behavior, 9, 480–488, Retrieved October 15, 2006, fromhttp://www.liebertonline.com/toc/cpb/9/4.
Vincelli, F., & Riva, G. (2002). Virtual reality: A new tool for panic disorder therapy [Electronic version]. Expert
Review of Neurotherapeutics, 2, 89–95.Wiederhold, B. K., Jang, D. P., Gevirtz, R. G., Kim, S. I., Kim, I. Y., & Wiederhold, M. D. (2002). The treatment
of fear of flying: A controlled study of imaginal and virtual reality graded exposure therapy [Electronic
version]. IEEE Transactions on Information Technology in Biomedicine, 6, 218–223.Wald, J., & Taylor, S. (2000). Efficacy of virtual reality exposure therapy to treat driving phobia: A case report
[Electronic version]. Journal of Behaviour Therapy and Experimental Psychiatry, 31, 249–257.