-
8/9/2019 Vene Puncture
1/25
Venepuncture 2013 1
CLINICAL GUIDELINES/NURSING
Guideline for Venepuncture Using the Vacutainer System
Reference 1438
Date approved
Approving Body Matron’s Forum
Supporting Policy/ Working inNew Ways (WINW) Package
Venepuncture using vacutainer system
Implementation date January 2013
Supersedes Version 1
Consultation undertaken Nursing Practice Guidelines Group,
WardSisters/Charge Nurses, PracticeDevelopment Matrons (PDMs),
ClinicalLeads, Matrons
Target audience All Clinical Nursing Staff
Document derivation /evidence base:
See main references
Review Date January 2016
Lead Executive Director of Nursing
Author/Lead Manager Di Ryan, Colorectal Chemotherapy
CNS,Oncology
Further Guidance/Information
Distribution: Ward Sisters/Charge Nurses, PDMs, ClinicalLeads,
Matrons, Nursing Practice GuidelinesGroup (includes University of
Nottinghamrepresentative)
This guideline has been registered with the Trust. However,
clinicalguidelines are guidelines only. The interpretation and
application ofclinical guidelines will remain the responsibilit y
of the individualclinician. If in doubt contact a senior colleague
or expert. Caution isadvised when using the guidelines after the
review date.
-
8/9/2019 Vene Puncture
2/25
-
8/9/2019 Vene Puncture
3/25
Venepuncture 2013 3
DEFINITION OF VENEPUNCTURE
Venepuncture is the procedure of inserting a needle into a vein,
usually to
obtain blood.
In order to do this safely, the Intravenous Nursing Society
(1998) Lavery I.Ingram P, (2005), and the RCN (2010) suggests the
practitioner must have abasic knowledge of the following broad
aspects:
The relevant anatomy and physiology
The criteria for selection of an appropriate vein and
device
The potential problems that may be encountered, how to
prevent orminimise them and how to manage them if they occur
The associated health and safety/risks involved in
undertaking theprocedure and the correct disposal of equipment.
INDICATIONS FOR VENEPUNCTURE
Venepuncture is carried out for the following reasons:
To obtain a sample of venous blood for diagnostic
purposes To establish and subsequently monitor levels of
blood components To establish and subsequently monitor levels
of drugs To monitor response to medical treatments (e.g.
fluids, drugs) To provide a sample of blood to cross match
for a blood transfusion To screen for infection.
-
8/9/2019 Vene Puncture
4/25
Venepuncture 2013 4
ANATOMY AND PHYSIOLOGY
Texas Heart Institute (2008)
VEIN CONSTRUCTION -Veins consist of three layers: the
tunica adventitia,the tunica media and the tunica intima
The tunica adventitia is the outer layer of the vein and
consists ofconnective tissue, which surrounds and supports the
vessel. Its role isprotective and in some patients/clients this can
make penetration of the veindifficult.
The tunica media is the middle layer of the vein and is
composed ofmuscular tissue and nerve fibres that can stimulate the
veins to contract orrelax in response to stimuli from the vasomotor
centre of the medulla. The
muscle is not as well developed as that of an artery and
therefore the veinscan distend or collapse as blood pressure rises
or falls (Weinstein, 2007).
-
8/9/2019 Vene Puncture
5/25
Venepuncture 2013 5
Stimulation of this layer by changes in temperature, mechanical
stimulation(e.g. introducing the needle into the vein) or chemical
stimulation (e.g. drugs)can produce spasm which can make
venepuncture more difficult. Additionally, if the patient is
anxious or clinically unwell (dehydrated,
hypotensive) the blood vessel will constrict also causing the
procedure to bemore difficult to perform.
The tunica intima is the inner lining of the vein and is
constructed of smoothendothelial cells which facilitates the
passage of blood cells etc. Damage tothe tunica intima results in
the internal lumen of the vein becoming roughenedand increases the
risk of thrombus formation. In addition, the endotheliallayer
develops folds, which are known as semilunar valves. The purpose
ofthe valves is to ensure that the blood moves towards the heart by
preventing
backflow. They are present in larger blood vessels and at points
ofbranching. These can sometimes be seen visually by noticeable
bulges inthe veins; the practitioner needs to learn to palpate the
vein to check for thepresence of valves and ensure that
venepuncture occurs above the valve inorder to facilitate
collection of the blood sample (Weinstein, 2001).
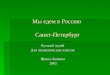
SELECTING A SITE FOR VENEPUNCTURE -The veins normally used
forvenepuncture are those found in the antecubital fossa because
they are
usually of a good size and are capable of providing copious and
repeatedblood specimens (Weinstein, 2007; Phillips, Collins and
Doherty 2011) );They are also easily accessible thus ensuring that
the procedure can beperformed safely and with the minimum of
discomfort for the patient/client(Marieb, 1998). The main veins of
choice are:
The median cubital vein The cephalic vein The
basilic vein
The median cubital vein may not always be visible, but its
size and locationmake it easy to palpate. It is also well supported
by subcutaneous tissue,which prevents it from rolling under the
needle.
On the lateral aspect of the wrist, thecephalic vein rises
from the dorsalveins and flows upwards along the radial border of
the forearm, crossing theantecubital fossa as the median cephalic
vein. Care must be taken to avoidaccidental arterial puncture, as
this vein crosses the brachial artery. It is also
in close proximity to the radial nerve (Perucca, 1995).
-
8/9/2019 Vene Puncture
6/25
Venepuncture 2013 6
The basilic vein, originating in the ulnar border of the hand
and forearm(Wilson & Waugh, 2001), is often overlooked as a
site for venepuncture: thisis for good reason. Although the basilic
vein may be prominent (particularly inmen), it is awkward to access
and it is not well supported by subcutaneous
tissue and tends to roll easily. These features make
venepuncture of thebasilic vein difficult. Care must also be taken
to avoid accidental puncture ofthe median nerve.
The metacarpal veins are easily visualised and palpated.
However, the useof these veins is contraindicated in the elderly
where the skin turgor andsubcutaneous tissue are diminished
(Weinstein, 2007; Lister and andDougherty 2011,)
Occasionally the veins of a lower limb may be used for
venepuncture,although the practitioner must understand the relevant
anatomy and specificproblems associated with these sites.
Venepuncture of veins in the lowerlimbs is associated with a higher
risk of complications due to the increasedpresence of valves and
the fact that, comparatively, the blood flow in thelower limb is
diminished (Weinstein, 2007).
CHOOSING A VEIN
The choice of vein must be that which is best for the individual
patient/client.The best veins are those where the vein is
accessible, unused, easilydetected and appear healthy and patent.
However, the most prominent veinis not necessarily the most
suitable vein for venepuncture (Weinstein, 2007 ).There are two
stages involved in locating a vein:
1. Visual inspection2. Palpation
Visual inspection involves scrutinising the veins in both
arms and isessential prior to choosing a vein. The following areas
should be avoided:
Veins adjacent to foci of infection, bruising and
phlebitis due to the riskof causing more local tissue damage or
systemic infection.
An oedematous limb as there is danger of stasis of
lymph thatpredisposes to such complications as phlebitis and
cellulites (Hoeltke2006, Smith, 1998).
Areas of previous venepunctures, where possible, as
repeated trauma
to the vein can result in pain (Ahrens et al, 1991).
-
8/9/2019 Vene Puncture
7/25
Venepuncture 2013 7
Palpation is an important assessment technique, as it
determines thelocation and condition of the vein. It assists in
distinguishing a vein fromarteries and tendons, identifies the
presence of valves and can detect deeperveins (Scales (2008). The
practitioner should use the same fingers for each
palpation to increase the sensitivity and ability of the
practitioner in detectingthe appropriate site to use (
Phillips,Collins and Dougherty, 2011 ). Thethumb should not be used
as it is not as sensitive and has a pulse, which maylead to
confusion in distinguishing veins from arteries in the
patient/client(Weinstein, 2007 ). Healthy veins feel soft and
bouncy and will refill whendepressed (Weinstein, 2007 ).
VEINS TO AVOID
Thrombosed veins – these feel hard and cord-like
Tortuous, sclerosed, fibrosed, inflamed, fragile veins – these
may
not be able to accommodate the device being used
Veins that cross over joints, bony prominences and those
with littlesubcutaneous cover (e.g. the inner aspect of the wrist)
– these cansubject the patient/client to more discomfort
For renal patients with an arterio-venous fistula/graft,
the non-fistula/graft arm should not be used as this increases risk
of stenosisand thus decreases the success of future venous access
for
haemodialysis.
OTHER FACTORS INFLUENCING VEIN SELECTION
Injury, disease or t reatment may prevent the use of
a limb forvenepuncture by reducing the venous access (e.g.
amputation,fracture, cerebrovascular accident). Use of a limb may
becontraindicated because of an operation on one side of the body,
forexample, mastectomy and axillary node dissection, as this can
leadto impairment of lymphatic drainage, which can influence
venousflow regardless of whether there is obvious lymphoedema
(Smith,1998; Rowland, 1991).
Position of the patient/client, for example, having to
lie on aparticular side, may also dictate the site of the
venepuncture(Millam, 1992; Rowland, 1991).
The age of the patient/client – the elderly may have
prominent veins
but they are often fragile. The largest vein should be selected
along
-
8/9/2019 Vene Puncture
8/25
Venepuncture 2013 8
with the smallest gauge device to reduce the amount of trauma
tothe vessel.
The weight of the patient/client – malnourished
patients/clients will
often present with friable veins. Obese patients/clients may
causepractitioners to have difficulty in locating the vein due to
extrasubcutaneous tissue being present.
Patients/clients who are dehydrated or in shock –
there will bepoor superficial peripheral access. It may be
necessary to takeblood after the patient is rehydrated as this will
promote venousfilling and blood will be obtained more easily
(Mallett & Dougherty,2000).
Medications or conditions that cause bleeding or s low
healing (e.g. anticoagulants, steroids, thrombocytopenia) –
these situationspredispose the patient/client to having more risk
of bruising bothduring venepuncture and on removal of the needle;
this then limitsthe availability of veins that are not damaged.
IMPROVING VENOUS ACCESS
The success of venepuncture is influenced by a number of factors
related tothe patient/client and the practitioner. The more
experienced the practitioneris the easier venepuncture becomes.
However, no matter how experiencedthe practitioner is, factors that
cause the blood vessels to vasoconstrict willmake the procedure of
venepuncture more difficult. A number of approachesto improve
venous access and thereby facilitate the procedure beingsuccessful
are identified below.
1. Fear about the procedure of venepuncture may itself result
in
vasoconstriction. The practitioner’s manner and approach will
have adirect bearing on the patient’s experience (Weinstein, 2007
). Approaching the patient/client with a confident manner,
giving anadequate explanation of the procedure together with
careful preparationand an unhurried approach may help to reduce
anxiety which will in turnincrease vasodilation.
2. Ensuring the correct ambient temperature of the environment
isimportant – if it is cold the blood vessels of the patient/client
may
vasoconstrict to compensate.
-
8/9/2019 Vene Puncture
9/25
Venepuncture 2013 9
3. Application of a tourniquet – this promotes venous
distension. Thetourniquet should be tight enough to impede venous
return but notrestrict arterial flow.
4. Opening and closing the fist ensures the muscles will force
the blood intothe veins and encourage distension.
5. Lowering the arm below heart level may also increase blood
supply tothe veins.
6. The use of heat in the form of a warm pack or by immersing
the arm in abowl of warm water for 10 minutes helps to encourage
vasodilation andvenous filling.
7. Ointments or patches containing small amounts of glyceryl
trinitrate havebeen used to cause local vasodilatation to aid
venepuncture. Aprescription is required to enable this
technique.
8. Stroking the vein (rather than patting it) can also assist
with venousdilation.
HAZARDS ASSOCIATED WITH VENEPUNCTURE
1. Infection – the circulation is a closed sterile system and a
venepuncture,however quickly performed, is a breach of this system
providing a meansof entry for bacteria. Adherence to an Aseptic
None Touch Technique(ANTT) will minimise the risk of cross
infection from practitioner topatient/client (e.g. thorough hand
cleansing using soap and waterfollowed by alcohol hand rub).
Non-sterile gloves may be required toprotect the practitioner from
cross infection from the patient/client but allother equipment
should be sterile and single use only.
2. Accidental damage – the nerve, tendon or artery might be
inadvertentlypunctured if these have not been identified during
visualinspection/palpation. This can result in pain, damage and
haemorrhagefor the patient/client as well as loss of confidence for
the practitioner.
3. Haematoma – this is the commonest complication arising
fromvenepuncture (Weinstein, 2007 ). There are a number of factors
thatinfluence the development of a haematoma – poor technique on
the part
of the practitioner, failure to release the tourniquet before
removingneedle and inadequate pressure on the venepuncture site
once the
-
8/9/2019 Vene Puncture
10/25
Venepuncture 2013 10
needle has been removed. A haematoma may also occur if
thepatient/client is asked to flex the arm on completion of the
procedure(Weinstein, 2007 ).
4. Prolonged bleeding time – this may be due to a medical
condition or drugtherapy (e.g. anticoagulation medication). It
increases the risk ofbruising/haematoma formation and worsens the
consequences ofinadvertent arterial puncture. Practitioners should
ensure they are awareof the patient/client’s relevant drug and
medical history prior toperforming venepuncture to reduce this
risk.
5. Incorrect or lack of details on the request card and/or
sample – thisincreases the likelihood of errors occurring and
therefore any
discrepancies will cause the sample to be rejected by the
laboratory,necessitating repetition of the procedure.WARNING: the
wrong patient details on the card can result in apatient receiving
unnecessary or dangerous treatment. All samplesmust be
correctly labelled and the details must correspond with those onthe
request card. The patient’s details, both on the request form and
thespecimen bottle should be ascertained using the Trust policy for
thepositive identification of Patients.
6. All cross match samples – the bottle and form should be
checked for
correct labelling by 2 Registered nurses. The patient should
already havean identity band on. If not, attach one to the patient
that states thepatient’s last name, first name, gender, date of
birth and NHS number.(NUH 2012)Check these details are correct with
the patient and thepatient’s hospital notes. Patient labels should
not be applied to crossmatch bottles- both the cross match form and
the blood bottles shouldhave hand written details on them.
7. Insufficient sample/wrong specimen bottle – the laboratory
will not be
able to process the sample necessitating repetition of the
procedureHowever, if the patient/client was difficult to bleed,
check with thelaboratory staff whether they might be able to
process the smallersample without it compromising the results.
8. Needlestick (sharps) Injury – use of vacutainer systems helps
to reducethe incidence of this occurring ( Centre for Disease
Control, 1997).However, the use of a needle and syringe may be
preferential to obtainblood from “poor veins” as it applies less
pressure on the vein and thus
has a higher success rate. Needles, if used, must not be
resheathed,and practitioners must adhere to the Trust sharps
policy. In the event of
-
8/9/2019 Vene Puncture
11/25
Venepuncture 2013 11
a needlestick injury the practitioner must follow the NUH Safe
handling,disposal and reporting of sharps and blood borne exposure
injuriespolicy (2008).
9. Infected samples – whether known or suspected, these pose a
healthrisk to any staff that have to handle them – this includes
porters andlaboratory staff. Appropriate identification through
labelling andtransportation of infected samples is covered in other
documents whichshould be read by the practitioner (refer to Trust
Policy and guidance asappropriate, e.g. Infection Control
Guidelines).
10. Blood spillage – use of the vacutainer system reduces the
risk of bloodspillage since the blood is drawn directly into the
evacuated sample tube.
However, there is a risk of blood spurting from the vein
whenvenepuncture commences. For those blood samples that cannot
betaken using the vacutainer system there is a risk of blood
spillage whendecanting blood from the syringe to the sample tube.
Blood spillage kitsare available in all clinical areas (refer to
Trust Policy). Staff should beusing goggles if there is any risk of
the practitioner being splashed byblood
11. Needle or Blood Phobia – if the patient/client has a needle
or bloodphobia it might make their behaviour difficult to manage.
They might
also faint at some point during the procedure. It is
important to establishwhether the patient/client has had previous
problems with venepunctureand to take appropriate action.
-
8/9/2019 Vene Puncture
12/25
Venepuncture 2013 12
EQUIPMENT LIST
Alcohol hand gel Plastic apron
Non-sterile gloves Goggles if required Clean tray or
receiver DisposableTourniquet Low linting swab (e.g.
gauze)
Tape Vacutainer device Sharps container
Patient identification labels (if
available/appropriate) Specimen request form
Specimen bottles
See General Principles for all Procedures.
PRIOR TO COMMENCING VENEPUNCTURE
PRINCIPLE / ACTION RATIONALE
1 Assemble the equipmentnecessary for venepuncture.
You should contact thepathology department if you areunsure what
bottles arerequired for the blood samplesrequested
To ensure that time is not wastedand that the procedure
goessmoothly without unnecessary
interruptions.
2 Check all packaging and expirydates before use.
To ensure the sterility of the productsprior to use.
3 Select appropriate size devicebased on vein size and numberof
samples required (21g is themost frequently used size).
To reduce damage or trauma to thevein.
4 Discuss any previousexperiences ofvenepuncture;
This might reduce anxiety which canreduce vasoconstriction. If
thepatient/client has a history of fainting,the practitioner can
put measures inplace to reduce/prepare for this.
-
8/9/2019 Vene Puncture
13/25
Venepuncture 2013 13
5 Make the patient/clientcomfortable (with back wellsupported)
in an environmentthat is suitable in terms of
lighting, ventilation, privacy,positioning and safety.
These factors will assist thepractitioner to be successful with
theprocedure.
PRINCIPLE RATIONALE
Discuss the procedure with thepatient/client to include:
Information about the
procedure and obtainconsent;
To ensure that the patient/client
understands the procedure and givesinformed consent.
What test(s) is (are) beingdone and why;
In addition to the patient/clientunderstanding the procedure,
thepractitioner needs to ensure that therequirements of the test
are met (e.g.if fasting blood sugar is being takenthe patient needs
to have fasted).
6
Relevant medical history(and allergies);
This might influence choice of limbfor venepuncture (e.g. if
thepatient/client has had surgery or eversuffered from lymphoedema)
orchoice of occlusive dressing.The practitioner may need to
takeadditional precautions if the patient isknown to have a blood
borne
infection (see relevant policy). Relevant drug history
(e.g.
anticoagulant therapy);The patient/client will be at higherrisk
of bleeding and therefore needto apply pressure on thevenepuncture
site for longer postprocedure.
-
8/9/2019 Vene Puncture
14/25
Venepuncture 2013 14
PRINCIPLE RATIONALE
7 Check that the patient/clientidentity matches the details
onthe venepuncture request formand label the sample tubes
withpatient details at the bedside.
To ensure that the correct sample istaken from the correct
patient/clientand comply with SHOT (SeriousHazards of Transfusion)
guidelines.
8. If patient expressesanxietyrelating to a phobiaabout needles
or concernsabout pain offer localanaesthetic and apply prior
toprocedure,
Emla cream, 45 minutes before Ametrop 15 minutes before
To ensure the comfort of thepatient/client and increase
venousaccess.
COMMENCING VENEPUNCTURE USING THE VACUTAINER SYSTEM
PRINCIPLE ACTION
1 Wash and dry hands thoroughlyusing antiseptic soap and
dry.Check hands for any brokenareas, and cover with anocclusive
dressing.
To reduce the risk of cross infection.
NUH Hand Hygiene Policy (2011)
Pratt et al (2007)
DoH (2007)
2 Break seal on vacutainerneedle, remove clear plasticcover and
screw disposablesyringe barrel onto thevacutainer needle (leave
thecoloured shield on the needleas this will be inserted into
the
patient/client’s vein).
In preparation for venepuncture ofthe patient/client’s vein.
-
8/9/2019 Vene Puncture
15/25
Venepuncture 2013 15
PRINCIPLE ACTION
4 Extend the upper limb (fullelbow extension) and support iton a
pillow.
To ensure the comfort of thepatient/client and increase
venousaccess.
5 Gel hands with alcohol hand ruband put on gloves (see
BestPractice Box Glove Use) andapron.
To reduce the risk of cross infectionand potential contamination
of thepractitioner
NUH Hand Hygiene Policy (2011)
Pratt et al (2007)
DH (2007)
6 Apply tourniquet to chosen limbin appropriate location.It may
be necessary to utiliseother methods to facilitatevenous distension
(SeeIMPROVING VENOUS ACCESS – page 6).
Dilates the veins by obstructingvenous return.Increase the
prominence of the veinsand/or promote blood flow
Best Practice USE OF TOURNIQUETS
‘Single-use’ tourniquets should be used for all patients.
The use of reusable tourniquets as well as other reusable
equipment(sphygmomanometer cuffs etc.) is starting to be
questioned, as they are apotential source of infection. Single use
tourniquets have financialimplications but this could be offset
against the increasing problem ofiatrogenic infections occurring in
hospitals. If using reusable tourniquets thenit must be cleaned
between each patient.
The tourniquet should be applied with enough pressure to impede
venousflow – if the radial pulse cannot be felt the tourniquet is
too tight. (Weinstein,2007 ).
-
8/9/2019 Vene Puncture
16/25
Venepuncture 2013 16
PRINCIPLE RATIONALE7 Select an appropriate vein – in
relation to size, location andcondition. Refer to the
followingsections:
Anatomy and physiology
Selecting a site,
Choosing a vein –appendix 1
Veins to avoid
– page 6
To complete procedure successfully
Best PracticeGLOVE USE
Non sterile gloves are to be used when undertaking venepuncture
andhandling blood and body fluids (NUH, 2011). This may help
preventcontamination from blood spills and cross infection but does
not preventneedlestick injuries and prevent cross infection. Please
refer to NUH Gloveselection guidelines (2011)
Best Practice SKIN CLEANSING chaThe use of skin cleansing
remains controversial. A study by Sutton et al(1999) concluded that
there was no difference with respect to complicationsat the site of
venepuncture that received skin cleaning when compared tothose that
had not. A cursory wipe is known to do more harm by disturbingthe
patient skin flora, thus increasing the risk of infection (Wilson,
2006). In
addition alcohol that is left on the skin that has not
completely dried cancause haemolysis of the sample (Perry and
Potter, 2002.) See NUHInfection Prevention and Control intranet
site for information on the use of‘Sanicloth and Chloraprep’
decontamination products.
-
8/9/2019 Vene Puncture
17/25
Venepuncture 2013 17
PRINCIPLE RATIONALE
7 Remove the coloured needleshield and hold the syringebarrel
with the needle beveluppermost.
This provides the cutting edge toincise through skin and tunica
layersof the vein.
8 Anchor the vein by applyingmanual traction on the skin ofthe
upper limb a few centimetresbelow the proposed insertionsite
To immobilise the vein and prevent itfrom rolling. Traction also
providesa counter-tension to the vein, whichwill facilitate a
smoother needleentry.
9 Insert the needle smoothly at anangle of approximately 15 –
30°depending on the vein location(degree of superficiality)
andadvance slowly into the vein –with experience it is possible
todistinguish when the vein wallhas been punctured.
To promote a successful, pain-freevenepuncture.
Advancing the needle stabilises thedevice within the vein
preventing itfrom becoming dislodged duringwithdrawal of blood.
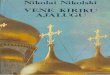
Introduce the blood bottle tubeinto the vacutainer
holder.Placing forefinger and middlefinger on the flange of the
holderand the thumb on the bottom ofthe tube, push the tube to
theend of the holder puncturing thestopper on the blood bottle.
It is important to retain the positionof the needle in the vein
whilstpushing the tube “home” in thevacutainer holder.
11 If venepuncture has beensuccessful, the bottle will
automatically fill to its requiredvolume. If nothing
happens,draw the needle back slightly –as long as the needle
remainsunder the skin the tube willretain its vacuum and when
thevein is found, blood willimmediately flow into the tube.
-
8/9/2019 Vene Puncture
18/25
-
8/9/2019 Vene Puncture
19/25
Venepuncture 2013 19
ON COMPLETION OF VENEPUNCTURE
PRINCIPLE / ACTION RATIONALE1 Once all the samples have
been
obtained, remove the last tubeand release the tourniquetbefore
withdrawing the needlefrom the vein.
To reduce the risk of: blood spillage discomfort for
the patient/client damage to the vein/development
of haematoma.
2 Place a low lint swab over thepuncture site applying
pressureto site AFTER the needle has
been removed.
To prevent pain on removal anddamage to the intima of the
vein.
3 Discard needle and vacutainerbarrel in sharps container.
To prevent needlestick injury.
4 Check that the tubes andrequest documentation arecorrect.
Check cross matchsamples with second nurse.
To reduce the risk of incorrect orunnecessary treatment
beinginitiated.
5 Check puncture site has sealedbefore applying an
occlusivedressing to the puncture site.(NB check that the
patient/clientis not allergic to the occlusivedressing to be
applied).Instruct the patient/client toremove the occlusive
dressingafter 24 hours.
To prevent the risk of blood spillageby ensuring the
patient/client doesnot bleed after leaving the clinicalarea.
6 Discard waste into appropriatereceptacles (in accordance
withTrust policies and procedures).
To reduce the risk of contamination.
7 Record type of blood sampletaken and any complicationsthat
occurred with the procedurein the appropriatedocumentation.
Medico-legal reasons.
-
8/9/2019 Vene Puncture
20/25
Venepuncture 2013 20
PRINCIPLE RATIONALE
8 Ensure samples are sent via theair tube system. At
present,
glass bottles (e.g. bloodcultures) or high-risk specimensshould
not be sent via the airtube system but taken to thelabs as soon as
possible.Community samples arecollected by van and taken tothe
appropriate laboratory.Urgent requests require a P1priority number
which can beobtained from the P1 line(55084) and written on
therequest form
The air tube system provides thequickest route to the
laboratories
and rapid processing of thesamples.
9 Advise the patient/client whenthe blood results will
beavailable and what action isrequired (if any) to obtain
theresult.
Effective communication
Best Practice PATHOLOGY REQUESTS
A role expansion package now exists in Nottingham
University HospitalTrust to allow nurses and/or other health
professionals to request pathologytests directly under certain
circumstances. This package meets therequirements set out in the
“Working in New Ways Policy and Guidelines(NUH 2011).
-
8/9/2019 Vene Puncture
21/25
Venepuncture 2013 21
REFERENCES
Ahrens T, Wiestma R & Weiltz PB (1991) Differences in
pain perception
associated with intravenous catheter insertion. Journal of
IntravenousNursing. 14,( 2), pp 85 – 89
Becan-McBride K (1999) Laboratory Sampling: Does the Process
Affect theOutcome? Journal of Intravenous Nursing. 22,( 3), pp 137
- 142
Centre for Disease Control (1997) Evaluation of safety devices
for preventingpercutaneous injuries among health care workers
during phlebotomyprocedures. Journal of the American Medical
Association. 277( 6) pp 449 –
450
Department of Health (2007) Saving Lives: reducing infection,
deliveringclean safe care (revised edition), London, Crown
Copyright.
Department of Scientific Publications, Texas Heart Institute
(2008)Vasculature of the Arm
http://www.texasheart.org/AboutUs/Depart/scipub.cfm accessed
on 11.03.09
Dimond B (2011) Legal Aspects of Nursing. 6th Edition
Prentiss Hall
Dougherty L (1996) Intravenous Cannulation. Nursing Standard.11
(2) pp 47 – 51
Dougherty L (2008) Obtaining vascular access. IN Dougherty
L & Lamb J(eds) IV Therapy in Practice. 2nd Edition
Chapter 9 Edinburgh: ChurchillLivingstone
Gabriel J. British Joural of Nursing( 2012) ( I.v.
supplement)21(2)
Heath Protection Unit (2002) Infection Control – Guidance on
Cleaning andDecontamination Nottingham: NPU
Intravenous Nursing Society (1998) Revised intravenous nursing
standardsof practice. Journal of Intravenous Nursing. 21,
Supplement 1S
Hoeltke LB (2006) the complete Textbook of Phlebotomy.
3rd edition cited in
Vennepuncture and Cannulation. Phillips, Collins and Dougherty
L. chapter 5
-
8/9/2019 Vene Puncture
22/25
Venepuncture 2013 22
Inwood S (1996) Designing a nurse training programme for
venepuncture.Nursing Standard. 10 ( 21) pp 40 – 42
Lavery I Ingram P(2005) Venepuncture: Best practice. Nursing
Standard 19(49) 55-65
Lister S & Dougherty L (2008) Royal Marsden Hospital: Manual
of ClinicalNursing Procedures. 8th edition Chapter 15, Oxford:
Blackwell Science
Marieb E N (1998) Essentials of Human Anatomy and Physiology.
5th editionCalifornia: Benjamin/Cummings
McConnell A A & McKay G M (1996) Venepuncture: the
medico-legalhazards. Postgraduate Medicine Journal. Vol. 72, pp 23
– 24
McGowan D (2010) British Journal of Nursing. 19,(14) p.878
Millam D A (1992) Starting IVs – how to develop venepuncture
skills.Nursing. 92, pp33 – 46
Nottingham University Trust (2008) Working in New Ways: Policy
andGuidelines Nottingham: NAT
NUH, Dept. of Microbiology (2008) BACTEC Blood Culture
CollectionInstructions NUH
Nottingham University Hospitals NHS Trust Trust (2011) Hand
Hygiene Policy
Nottingham University Hospitals NHS Trust (2008) Glove
SelectionGuidelines
Nottingham University Hospitals NHS Trust (2008) Safe handling,
disposaland reporting of sharps and blood borne exposure injuries
policy (2008).
Perry AG & Potter PA (2002) Clinical Nursing Skills and
Techniques 5th Edition London: Mosby
Perucca R (1995) Obtaining vascular access. IN Terry J,
Baranowksi L,Lonsway R A, & Hedrick C (eds) Intravenous
Therapy: Clinical Principles
and Practices. Chapter 21 Philadelphia: WB Saunders
-
8/9/2019 Vene Puncture
23/25
Venepuncture 2013 23
Pratt, R, Pellowe, C Wilson, J, Loveday, H, Harper, P, Jones,
S, McDougall, ,C,Wilcox, M (2007) epic2: National
Evidence-Based Guidelines forPreventing Healthcare-Associated
Infections inNHS Hospitals in England, Journal of Hospital
Infection, Vol 65, Suppliment,
S1-64.
Price J & Moss J (1998) The pitfalls of practice nursing.
Nursing Times. 94,(30) pp 64 – 66
Rowland R (1991) Making sense of venepuncture. Nursing Times.
87( 32)
pp 41 – 43
Royal College of Nursing (1995) Universal Precautions. London:
RCN
Royal College of Nursing (2010) Standards for Intravenous
Therapy.London: RCN
Scales K ( 2008) A practical guide to Venepuncture and blood
sampling.Nursing Standard vol. 22,no.29,pp29-36
Scales K ( 2009) Intravenous therapy ; the legal and
professional aspects ofpractice. Nursing Standard. 23, pp51-57
Smith J (1998) The practice of venepuncture in lymphoedema.
EuropeanJournal of Cancer Care. Vol. 7, pp 97 – 98
Sutton CD, White SA, Edwards R, Lewis MH (1999) A prospective
controlledtrial of the efficacy of isopropyl alcohol wipes before
venesection in surgicalpatients Annals of the Royal College of
Surgeons of England. (3) May
pp.183-6
Weinstein S (2007) Plumer’s Principles and Practice of
IntravenousTherapy. 8th edition. Philadelphia: JB
Lippincott
Wilson J (2006) Infection Control in Clinical Practice.
3rd edition. London:Bailliere Tindall
Wilson K J W & Waugh A (2001) Anatomy and Physiology.
9th edition.
Churchill Livingstone, Edinburgh
-
8/9/2019 Vene Puncture
24/25
Venepuncture 2013 24
Author: Diane Ryan,Colorectal Chemotherapy Nurse
Specialist ,CASDirectorate
NPGRG Link: Vivian Blackburn
January 2013
Review: March 2015
SUGGESTED AUDIT POINTS
1. Has a suitable vein been chosen, using the criteria outlined
in theguidelines?
2. Are all relevant details, including correct identification
information, on
the request card/sample bottles?
3. Has an appropriate size device been chosen?
4. Did the practitioner discuss the procedure with the
patient?
5. Has the patient’s identity been confirmed?
6. Have gloves been used appropriately?
7. Has the skin been cleansed according to guidelines?
-
8/9/2019 Vene Puncture
25/25
8. Has no more than two unsuccessful attempts at
venepuncture been
attempted?
9. Has the puncture site been sealed correctly?