Embed Size (px)
Citation preview

R
V
Sa
b
c
a
KIVVIRCO
C
DNT
0h
Vaccine 31S (2013) B43– B53
Contents lists available at SciVerse ScienceDirect
Vaccine
jou rn al h om epa ge: www.elsev ier .com/ locate /vacc ine
eview
accine development and deployment: Opportunities and challenges in India
anjukta Sen Guptaa, G. Balakrish Naira, Narendra Kumar Arorab, Nirmal Kumar Gangulyc,∗
Translational Health Science and Technology Institute, Plot No. 496, Phase-III, Udyog Vihar, Gurgaon 122 016, Haryana, IndiaThe INCLEN Trust International & CHNRI, I F-1/5, 2nd Floor, Okhla Industrial Area, Phase I, New Delhi 110 020, IndiaNational Institute of Immunology, Aruna Asaf Ali Marg, New Delhi 110 067, India
r t i c l e i n f o
eywords:ndiaaccine developmentaccine coverage
ntroduction of new vaccinesecent developmentshallengespportunities
a b s t r a c t
The Indian economy is among the fastest growing economies in the world. The country forayed into man-ufacturing vaccines starting with a few public-sector manufacturers in the late 1960s but has emerged asthe major supplier of basic Expanded Programme on Immunization vaccines to the United Nations Chil-dren’s Fund (UNICEF) because of substantial private-sector investment in the area. The Indian vaccineindustry is now able to produce new and more complex vaccines such as the meningitis, Haemophilusinfluenzae type b, and pneumococcal conjugate vaccines, rotavirus vaccine and influenza A (H1N1) vac-cines. This has been possible because of an attractive investment environment, effective and innovativegovernmental support, international partnerships and the growing in-country technical work force. Alarge number of vaccines, including those mentioned, is available and administered in the private sector
within the country, but India has been slow in introducing new vaccines in its publically funded pro-grams. Growth in the economy and technological accomplishments are not reflected in a reduction inhealth inequalities, and India continues to contribute significantly to global child mortality figures. Thispaper reviews the development of the Indian vaccine industry, policy support for it and its current status. It also highlights opportunities and challenges for the introduction of new and underutilized vaccines athome.© 2012 Elsevier Ltd. All rights reserved.
ontents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B442. Vaccine development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B44
2.1. Vaccine research and development in India . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B442.1.1. New institutional mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B442.1.2. New funding mechanisms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B44
2.2. Vaccine manufacturing in India . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B452.2.1. History and overview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B452.2.2. Policy changes affecting manufacturing capacity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B462.2.3. Private sector-driven initiatives to enhance manufacturing capacity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B462.2.4. Innovative international partnerships for indigenous manufacture of vaccines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B46
2.3. Regulations pertaining to vaccine development and manufacture. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B472.4. Vaccine development: suggestions for the way forward . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B47
2.4.1. Vaccine research and development . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B472.4.2. Manufacturing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B472.4.3. Regulatory issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B47
3. Vaccine deployment within India . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3.1. Current coverage for basic EPI vaccines and polio-free status . . . . .
3.2. Recent vaccine introductions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Abbreviations: AIIMS, All India Institute of Medical Sciences; BBIL, Bharat Biotech Inrugs Controller General of India; GDP, Gross domestic product; ICMR, Indian CouncilRHM, National Rural Health Mission; NTAGI, National Technical Advisory Group for Imranslational Health Science Technology Institute.∗ Corresponding author. Tel.: +91 11 26741501; fax: +91 11 26741501.
E-mail address: [email protected] (N.K. Ganguly).
264-410X/$ – see front matter © 2012 Elsevier Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.vaccine.2012.11.079
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B48. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B48
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B48
ternational Limited; CDSCO, Central Drugs Standard Control Organization; DCGI, of Medical Research; NICED, National Institute of Cholera and Enteric Diseases;munization; R&D, research and development; SII, Serum Institute of India; THSTI,

B44 S.S. Gupta et al. / Vaccine 31S (2013) B43– B53
3.3. Institutional mechanisms for decision-making . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B493.4. Challenges in decisions-making process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B50
3.4.1. Lack of locally generated evidence . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B503.4.2. Financing. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B503.4.3. Health system issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B50
3.5. Advocacy and communication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B503.6. Vaccine deployment: the way forward . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B50
3.6.1. VPD surveillance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B503.6.2. Public- vs. private-sector delivery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B503.6.3. Advocacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B51
4. Recent initiatives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B514.1. National vaccine policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B514.2. Comprehensive multi-year plan (2012–2017) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B514.3. Revised AEFI guidelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B514.4. Year of intensification of routine immunization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B514.5. Alternate vaccine delivery vehicles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B51
5. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B51Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B51Conflict of interest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B52
. . . . . .
1
wi2cmvgforowpoknwIwc
mibbu1s[
vCtJsc(p
nI
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. Introduction
India is among the fastest growing economies in the world,ith a gross domestic product (GDP) growth rate of nearly 7%
n 2011 and an average of approximately 3% rise annually since002 [1]. The pharmaceutical industry is among the importantontributors to the national GDP, with a value of around US$900illion, and is poised to grow 20% annually by 2020 [2,3]. Indian
accine manufacturers have emerged as significant players in thelobal market. When the multinational manufacturers moved awayrom producing basic vaccines for use by the Expanded Programmen Immunization (EPI) toward more complex and economicallyewarding vaccines in the 1960s, Indian vaccine manufacturersccupied this niche. Initially, a few public-sector manufacturersere encouraged to enter this area, but privately owned com-anies soon followed them. They contributed an estimated 53%f the GAVI Alliance’s supply of vaccines from emerging mar-ets in 2008. This fraction dropped to 29% in 2010 because ofew vaccines such as rotavirus and pneumococcal conjugates,hich are supplied by multinational companies [2,4]. Today,
ndian private-sector vaccine manufacturers also are competingith multinationals in developing and marketing complex vac-
ines.It is paradoxical, then, that the country has emerged as a
ajor global supplier of basic EPI vaccines and yet approx-mately 40% of Indian children do not receive the completeenefit of these vaccines. Access to basic vaccines varies greatlyetween and within states, between urban and rural pop-lations and among wealth quintiles [5]. Moreover, merely% of India’s total budget is spent on health and only amall fraction of this is spent on immunization activities6].
Until a few years ago, India had only six antigens in theaccines supplied in the national immunization program—bacillealmette-Guerin for tuberculosis (TB); diphtheria, tetanus, per-ussis; oral polio vaccine and measles. Hepatitis B virus (HBV),apanese encephalitis (JE), Haemophilus influenzae type b (Hib) andecond dose of measles vaccines were added only recently. Vac-ines for diseases causing most childhood mortality and morbidityi.e., pneumonia and diarrhea) are yet to be included in the national
rogram.This article is a critical review of the achievements, opportu-ities and challenges for vaccine development and deployment in
ndia during the last several decades.
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B52
2. Vaccine development
2.1. Vaccine research and development in India
In recent years, vaccine research and development (R&D) inIndia has surged because of several new initiatives both in the pub-lic and private sectors, which affected industry and academia. Someof these initiatives are described below.
2.1.1. New institutional mechanismsIn the last five years, several new institutions, clusters and con-
sortia were established to carry out basic and multidisciplinaryapplied research to support vaccine development. The Transla-tional Health Science Technology Institute (THSTI) houses theVaccine and Infectious Disease Research Center that carries outtranslation-related activities for rotavirus, TB and JE vaccines andis now expanding to research on human immunodeficiency virus(HIV) vaccines, in collaboration with the International AIDS Vac-cine Initiative (IAVI). The Clinical Development Services Agency,an extramural center of THSTI, has been created to provide cost-effective, high-quality preclinical and clinical product developmentsupport services. This agency also works to enhance clinical trialcapacity by conducting training programs, monitoring trials for GCPcompliance and working with public sector institutions and smalland medium enterprises in India through its Centers of Excellence,supporting similar work by the Indian Council of Medical Research(ICMR). CDSA has partnered with Bill and Melinda Gates Foundationand the NIH, USA to ensure availability of experienced internationalfaculty for their courses [7]. In addition, several repositories and abiosafety level 4 facility have been created to support vaccine R&D[8]. A partnership between Merck Sharp & Dohme and the globalcharity Wellcome Trust created Hilleman Laboratories, which aimsto take vaccines important for developing countries from benchto Phase II, develop adjuvants and conduct research to improvethermostability of vaccines [9]. New international initiatives suchas the Vaccine Grand Challenge Program, ICGEB-EMORY VaccineCenter and the Malaria Vaccine Development Program have beencreated to accelerate vaccine R&D [10–12]. Whether or not thesenew models benefit the vaccine enterprise in India likely will beapparent only over the next decade.
2.1.2. New funding mechanisms2.1.2.1. National mechanisms. To ensure a supply of good qual-ity and innovative products at an affordable price to the Indian

S.S. Gupta et al. / Vaccine 31S (2013) B43– B53 B45
Table 1Vaccines under development in India in academic institutions.a
Human vaccines underdevelopment
Institutions involved Status
Cholera vaccine IMTECH, Chandigarh;NICED, Kolkata
Live oral cholera vaccine candidate vaccine strain VA1.4 Phase II studies completed, Phase III willbegin soon.
Dengue vaccine ICGEB, N. Delhi Efforts on developing safe, efficacious and inexpensive tetravalent dengue vaccine candidate areunderway.
Hepatitis A NIV, Pune An agreement for transfer has been signed with BBIL for further development.HIV vaccine THSTI, Gurgaon; IAVI Efforts are underway to design of candidate vaccines to elicit neutralizing antibodies against HIV.Japanese encephalitis
vaccineNII, N. Delhi (1) Vero cell-derived inactivated JEV vaccine developed was transferred to Panacea Biotech.
NIV and University ofPune, Pune
(2) JE chimeric peptide based vaccine has been transferred BBIL, Hyderabad.
Leishmania vaccine IOP and IMM, N. Delhi Use of live-attenuated Leishmania donovani parasites as vaccine candidates against visceralleishmaniasis is being tested at laboratory scale.
Malaria vaccine ICGEB, N. Delhi PvDBPII for P. vivax and JAIVAC-1 vaccine for P. falciparum has been transferred to BBIL, Hyderabad.Phase I clinical trials completed.
Rotavirus vaccine AIIMS, New Delhi; CDCand NIH, USA
Phase III clinical trial of rotavirus vaccine 116E underway at three sites: SAS, N. Delhi; CMC, Vellore;KEM Hospital Pune.
Tuberculosis vaccine THSTI and UDSC, N.Delhi
Recombinant BCG 85c (rBCG85c), one of several candidates that showed promising results in animals,is being developed as a TB vaccine.
Typhoid vaccine AIIMS, N. Delhi A Vi-conjugate typhoid vaccine technology has been transferred to USV Ltd. Mumbai.
AIIMS, All India Institute of Medical Sciences; BBIL, Bharat Biotech International Ltd.; CDC, US Centers for Disease Control and Protection; HIV, Human immunodeficiencyvirus; IAVI, International AIDS Vaccine Initiative; ICGEB, International Center for Genetic Engineering and Biotechnology; IMM, Institute of Molecular Medicine; IMTECH,Institute of Microbial Technology; IOP, Institute of Pathology; JEV, Japanese encephalitis virus; NICED, National Institute of Cholera and Infectious Diseases NII, NationalI te of Vo
ncil of
pDtBgLabismmvLLBiadtvdatseison(cit
2ocU
by the Serum Institute of India Ltd. in 1966—both family-ownedenterprises. Panacea Biotech emerged during the critical need forfilling and packaging of imported bulk oral polio vaccines in quick
Table 2Vaccines under development in the Biotechnology Industry Partnership Program(BIPP).
Industry Project title
Virchow Biotech Private Ltd.,Hyderabad
Mucosal vaccine for HPV
Gennova BiopharmaceuticalsLtd., Pune
Recombinant HPV vaccine
Tergene Biotech Pvt. Ltd.,Secunderabad
Affordable, Asia-specific 15-valentpneumococcal polysaccharide—CRM197
protein conjugate vaccineSerum Institute of India Ltd.,
PuneHPV vaccine
Panacea Biotec Ltd., New Delhi 13-valent pneumococcal conjugate
nstitute of Immunology; NIH, US National Institutes of Health; NIV, National Instituf Delhi, South Campus.a Compiled from Annual reports of Department of Biotechnology and Indian Cou
opulation, the Ministry of Science and Technology, through itsepartment of Biotechnology and Council for Scientific and Indus-
rial Research, has initiated new funding mechanisms. The Smallusiness Innovation Research Initiative supports innovative ideasenerated by start-ups, and the New Millennium Indian Technologyeadership Initiative supports novel projects from both industrynd academia very early in development. These initiatives haveeen used by domestic vaccine manufacturers to cushion risks
n the initial development of vaccines, especially complex onesuch as rotavirus, pneumococcal conjugate and human papillo-avirus vaccines. The Government of India provided funds to fouranufacturers to develop and manufacture influenza A (H1N1)
accines following the pandemic in 2009 (Serum Institute of Indiatd. (SII), Cadila Pharmaceuticals Ltd., Bharat Biotech Internationaltd. (BBIL), and Panacea Biotec Ltd.). The Technology Developmentoard of the Department of Science and Technology provides fund-
ng to industry for setting up manufacturing and other facilities;n example of such support is that provided to Biological E Ltd. forevelopment of their HBV and Hib pentavalent vaccines. Recently,he Biotechnology Ignition Grant was launched to support inno-ation in affordable health care products in the initial phase ofevelopment [13]. These grants are available to students, facultynd small and medium enterprises that have incubator space orheir own infrastructure to carry out the proposed work. Severalcience ministries and the Department of Health Research are gen-rously funding academic and other research institutions to workn the area of vaccinology for product development and supportingcience (Table 1). The Biotechnology Industry Partnership Program,n the other hand, funds product development with industry part-ers and has supported some major projects in the area of vaccinese.g., H1N1, human papillomavirus, hepatitis C virus and pneumo-occal conjugate vaccines) (Table 2). However, it should be keptn mind that these recently instituted funding mechanisms mightake some time to show measurable impact.
.1.2.2. International mechanisms. The Department of Biotechnol-gy also has initiated bilateral programs with countries that haveontributed immensely to the science of vaccinology [e.g., thenited States (US), Norway, France, Australia and Finland]. The
irology; THSTI, Translational Health Science Technology Institute; UDSC, University
Medical Research.
Indo-US Vaccine Action Program provided support to key vaccinedevelopment projects in India including those for rotavirus, malariaand dengue [14], in partnership with the Department of Biotech-nology and ICMR.
2.2. Vaccine manufacturing in India
2.2.1. History and overviewIndia has a long history of vaccine manufacture, dating to the
early 19th century. Of several institutes established in the pre-independence era, only Haffkine Institute Mumbai remains onthe list of manufacturers that produce World Health Organiza-tion (WHO) prequalified vaccines (Table 3). Of the major publicallyfunded establishments, the BCG Vaccine Laboratory, HLL LifecareLtd. and Indian Immunologicals Ltd. still manufacture vaccines forhuman use.
The entry of private enterprise into vaccine manufacturingstarted with Biological E Ltd. of Hyderabad in 1953, followed
vaccine against Streptococcuspneumoniae infections
CRM197, a nontoxic recombinant variant of diphtheria toxin HPV, human papillo-mavirus.

B46 S.S. Gupta et al. / Vaccine 3
Table 3Indian manufacturers producing World Health Organization prequalified vaccines.a
Manufacturer WHO prequalified products
Serum Institute of India Ltd.,Pune
BCG; DT; DTwP; DTwP-Hib;DTwP-HepB-Hib*; Hib; HepB**;measles#; MR; MMR; Rubella;MenAfriVacTM
Biological E Ltd., Hyderabad TT; DTwP-HepB-HibChiron Behring Vaccines
Private Ltd., MumbaiRabies
Shantha, a Sanofi company,Hyderabad
Whole cell cholera; HepB
Zydus Cadila, Ahmadabad RabiesHaffkine Bio Pharmaceutical
Corporation Ltd., MumbaiPolio OPV Bivalent Types 1 and 3
Polio OPV monovalent Type 1
BCG, bacille Calmette-Guerin; DT, diptheria and tetanus toxoids; DTwP, diphthe-ria toxoid, tetanus toxoid and whole cell pertussis; DTwP-Hib, diphtheria toxoid,tetanus toxoid and whole cell pertussis with Haemophilus influenzae type b; DTwP-HepB-Hib, diphtheria toxoid, tetanus toxoid and whole cell pertussis with hepatitisB and Haemophilus influenzae type b; HepB, hepatitis B; Hib, Haemophilus influen-zae type b; MR, measles and rubella; MMR, measles, mumps, and rubella; OPV, oralpolio vaccine; TT, tetanus toxoid; WHO, World Health Organization.
i
rtiBBceCDn
2
tcfpTawIoabJa
w2fR“feiWtffbt[
a Based on data from the WHO website: available from: http://www.who.int/mmunization standards/vaccine quality/pq suppliers/en/.
esponse to a national need. The last two decades have witnessedhe entry of scientist and engineer entrepreneurs into the vaccinendustry, with establishment of biotechnology companies. Shanthaiotech, Bharat Biotech International Ltd., Tergene Biotech (P) Ltd.,iovel Life Sciences (P) Ltd. and Biomed (P) Ltd. are examples of thishange. In addition, several Indian pharmaceutical companies withstablished business in biopharmaceuticals, such as Zydus Cadila,adila Pharmaceuticals Ltd., Ranbaxy Laboratories Ltd., Wockhardt,r. Reddy’s Laboratories Ltd. and Intas Pharmaceuticals Ltd., areow finding it attractive to expand into the vaccine business.
.2.2. Policy changes affecting manufacturing capacityIndian vaccine manufacturers did not engage in vaccine R&D
hemselves, nor did they take up indigenously developed con-epts but rather relied heavily on mature technologies licensedrom outside the country, until very recently [4], when the newatent situation increased the need for home-grown innovations.o remain competitive in the global market and yet supply afford-ble vaccines, they had to invest in in-house R&D and collaborateith scientific institutions within the country. In the last decade,
ndian companies have produced more complex vaccines. Whilene such vaccine, the meningiococcal vaccine developed by SII haslready been commercialized, several others like Rotavirus vacciney BBIL, SII and Shantha; HINI by SII, Panacea Biotec. Ltd. and BBIL;apanese encephalitis by BBIL, Biological E and Panacea Biotec Ltd.re in late stages of development.
Industrial growth in the country has, for a long time, trackedith the growth rate of the GDP, averaging 6.7% between 1991 and
012, compared with a GDP rate of 6.9% [15]. Recent changes inoreign direct investment policies have brought basic and applied&D in biotechnology and the life sciences under the category ofindustrial parks” [15] as industrial activities, and has allowed 100%oreign direct investment through a government approval route forxisting industries. This has created motivation for global giants tonvest in Indian vaccine enterprises, a field previously neglected.
ith favorable industrial policies and six Indian vaccine manufac-urers in the private sector that have received WHO prequalificationor their products, the situation is changing. Each of these six manu-
acturers has a world-class manufacturing facility that is complex touild and expensive to maintain. The assured income from domes-ic sales and the capacity to fulfill orders for large global markets16] make them lucrative targets for global pharmaceutical players,1S (2013) B43– B53
which are losing revenue because of expiring patents on severaldrugs.
2.2.3. Private sector-driven initiatives to enhance manufacturingcapacity
A new ecosystem that encourages partnerships and new mar-ket forces have strengthened vaccine manufacturing in the country.Because manufacturing plants for vaccines must conform to currentgood manufacturing practice standards to obtain WHO prequal-ification for their products, they are expensive to maintain. Inaddition, an appropriately trained labor force with experience inthe vaccine industry is difficult to find and retain in India. Inorder to overcome these barriers and maintain their position inthe vaccine industry, companies have opted to either form jointventures or enter into innovative partnerships with nonprofit orga-nizations each partner contributing to an important componentof development of the final product [17,18]. The former type ofarrangement led to the manufacture of H1N1 influenza vaccinein a timely manner during the recent pandemic within a shortperiod [19]. The new venture now is in advanced stage of devel-opment of a rabies virus-like particle subunit vaccine, which is onein a series of products based on this platform (personal commu-nication to the authors). In another effort, by partnering with twononprofit organizations—one providing the construct and the otherthe adjuvant—and creating a facility exclusively for leishmaniasisvaccines, a company will produce the number of doses needed fortrial of a candidate leishmaniasis vaccine in India. The vaccine islikely to undergo simultaneous trials in India and the United States,thereby reducing the lag period in the uptake of new vaccines indeveloping countries, which usually exceeds more than a decade[20].
Company acquisitions are another way of providing the requiredstrengths to run a vaccine industry in the country. While acquisi-tion of Indian companies such as Shantha by Sanofi is at one end ofthe spectrum, the recent acquisition of Bilthoven Biologicals, whichis owned by the Government of the Netherlands, by the SerumInstitute of India Ltd., marks the other end of it [21]. Acquisition ofsmaller vaccine manufacturers, such as Biovel Life Sciences (P) Ltd.by Ranbaxy Laboratories Ltd. [22], is the beginning of a trend thatunderscores the growing importance of vaccines in the pharma-ceutical business in the next decades. Such acquisitions potentiallycan provide access to technology, unique capability and expertisethat are currently present in very few other vaccine manufacturingplants globally, as in case of Bilthoven Biologicals.
2.2.4. Innovative international partnerships for indigenousmanufacture of vaccines
India has benefited tremendously from innovative internationalpartnerships due to its strong scientific base and manufacturingcapabilities. A good example of this is the conjugate vaccine againstthe group A meningitis strain, manufactured at the Serum Instituteof India at extremely low price and high quality, for the sub-SaharanAfrican meningitis belt. The transfer of the conjugation technologydeveloped at the Center for Biologics Evaluation and Research ofthe US Food and Drug Administration has strengthened capacitywithin the company to venture into similar complex and challeng-ing vaccines, such as pneumococcal conjugate vaccines. In additionto support for generating country-specific evidence for introducingthe vaccine in Africa, an important contribution of the US Agency forInternational Development has been addressing regulatory issuesand strengthening capacity at the Drugs Controller General of India(DCGI) through this partnership [23].
Rotavirus and the cholera bacterium cause most of the diar-rheal disease burden in India [24–27] and have evoked interestfrom funding agencies, academia and industry in investing in devel-opment of vaccines against these two pathogens [28–30]. The

cine 3
iwbYfIIttSipttioTNb
oManawmsri
tiogasepa
2m
ovitAaptoGmpaoprwsni
S.S. Gupta et al. / Vac
ndigenous development of these enteric vaccines was initiatedith public funding, ensuring that the cost of the vaccine would
e much lower than that of the licensed imported vaccines [31,32].et another example of a successful transnational technology trans-
er is that of an inactivated oral cholera vaccine modified by thenternational Vaccine Institute (IVI), field-tested by the Nationalnstitute of Cholera and Enteric Diseases (NICED) and manufac-ured by Shantha (now a Sanofi company) [33,34]. IVI modifiedhe Swedish version of the vaccine [35,36], and the new vaccine,hancol®, was licensed in February 2009. However, even when pol-cymakers were apprised of the advantages of using the vaccine forublic health through various meetings conducted in the country,he WHO prequalified the vaccine only in September 2011—afterhe death-toll from the Haiti outbreak that began after the devastat-ng earthquake in 2010 and vociferous support by champions. It wasnly then that the company was able to market it globally [37–39].his partnership enabled strengthening of clinical trial capacities atICED and also highlighted the manufacturing capacity of Shantha,ringing it to the forefront globally.
In regard to the rotavirus vaccine, success was possible becausef the involvement of credible institutions [All India Institute ofedical Sciences (AIIMS), US National Institutes of Health (NIH),
nd US Centers for Disease Control (CDC)], a champion, a promi-ent national need and a local manufacturer capable of providingffordable and high-quality vaccines. A rotavirus vaccine strain thatas isolated and characterized at AIIMS was transferred to a localanufacturer, Bharat Biotech International Ltd., after it was exten-
ively tested in collaboration with the NIH and CDC [40–42]. Thisemains one of the most successful ventures in development of anndigenous vaccine in India thus far.
Partnerships among multiple stakeholders also have facilitatedhe two AIDS trials conducted by ICMR. Multiple partners, includ-ng IAVI, the National AIDS Control Organization, United Nationsrganizations, human rights activists, ethicists, lawyers, health andender experts, media representatives and members of nationalnd international nongovernmental organizations were involvedimultaneously to take on the challenges as needed [43–46]. Thisxperience demonstrated the benefits of having a very strongipeline of candidates when attempting to produce a vaccine for
difficult pathogen such as HIV [47,48].
.3. Regulations pertaining to vaccine development andanufacture
Until recently, India enjoyed a near monopoly in the supplyf vaccines to United Nations Children’s Fund (UNICEF). However,accine manufacturers in China will soon be eligible for prequal-fication of their products, following the WHO decision in 2011hat China’s national regulatory authority, State Food and Drugdministration and affiliated institutions meet WHO indicators for
functional vaccine regulatory system—indicating increased com-etition in this market [49]. All vaccines that use recombinantechnologies in India must undergo assessments per guidelinesf the Review Committee on Genetic Manipulation (RCGM) andenetic Engineering Approval Committee (GEAC), each taking ainimum of six to eight months. The DGCI also reviews data for
reclinical toxicity prior to permitting Phase I clinical trials andfter each subsequent Phase of clinical trial. The recent de-listingf few Indian vaccine manufacturers from the possibility of WHOrequalification for their products is a matter of concern. In thisegard, the Central Drugs Standard Control Organization (CDSCO),
hich houses the national regulatory authority of India, has beentrengthened in terms of manpower and processes [50]. Begin-ing in 2009, mandatory registration of clinical trial organizations,
nspection and better monitoring of clinical trials was implemented
1S (2013) B43– B53 B47
[51]. Registration of ethicsal committees is also under consider-ation.
2.4. Vaccine development: suggestions for the way forward
2.4.1. Vaccine research and developmentVaccine research and development is a time- and resource-
intensive process, with risks increasing as one moves up thepathway of development. Academicians, industry and policy-makers in India tend to work in vertical “silos,” with minimalhorizontal connections. Building connections between them willhelp ensure the necessary synergy among these stakeholders.
There are in-country examples of highly promising vaccine can-didates that were developed—for example, for HIV, hepatitis E andmalaria—that are having difficulty proceeding to the commerciallevel due to lack of participation by partners at all stages of devel-opment. Individually generated initiatives to solve public healthproblems are important, but for a large and diverse country such asIndia, top-down, focused programs for vaccine development thathave the flexibility to engage with diverse stakeholders could bemore productive. For successful indigenous research in India, thereis a need to create a concerted multidisciplinary, multi-stakeholderapproach with frequent opportunities for dialog among the stake-holders to support a common platform to discuss and overcomebarriers of intellectual property rights, infrastructure and a skilledwork force.
Another important factor for success in R&D is the availabilityof funding to support the types of collaborations mentioned above.Further, existing institutions with mechanisms for health policyanalysis could take on the additional tasks of synthesizing evidenceand catalyzing communication among stakeholders to accelerateindigenous vaccine development and commercialization. A mentornetwork with people experienced in vaccine R&D from industry andacademia would provide additional impetus.
2.4.2. ManufacturingA prerequisite for strong manufacturing infrastructure in the
country is the presence of an appropriate mechanism for the gov-ernment to cushion risks taken by the industry. Alignment withtechnical and scientific institutions could strengthen this manufac-turing base. Innovative procurement policies, including long termprojections for vaccine requirements and purchase commitment,also could help build an attractive ecosystem for the industry. Thestartups in vaccine manufacture could benefit from GMP-compliantincubator facilities for scaling up proof-of-concept studies. Appro-priate funding from both national and international agencies, aswell as venture capitalists, in the form of soft loans and grants,could improve this sector. As previously mentioned, four Indianvaccine manufacturers were supported by the government to pro-duce the H1N1 influenza vaccine during the pandemic (Table 4).This is a good example where lack of appropriate policies and delayin regulatory clearances hampered proper utilization of these vac-cines. Platforms for interactions between government, industry andregulators, could benefit the vaccine manufacturing in the country.
2.4.3. Regulatory issuesThe safety and efficacy of vaccines are the highest priorities of
any regulatory body. The strengths in manufacturing of the Indianvaccine industry should be complemented by a robust regula-tory system that is in sync with international regulatory norms.There is a need to develop the capacity to establish and eval-uate new platforms and innovative technologies that translate
scientific advancements. Establishment of a fast-track mechanismfor regulatory clearance of vaccines using new platforms, albeitbased on sound evidence, would be immensely helpful, espe-cially for vaccines required quickly in emergencies. The WHO
B48 S.S. Gupta et al. / Vaccine 3
Table 4Vaccine manufacturers funded by Department of Biotechnology, Government ofIndia for developing H1N1 vaccines.
Manufacturer Vaccine Datemanufacturinglicensereceived
Serum Institute ofIndia Ltd., Pune
Influenza vaccine (live attenuated,freeze-dried) for intranasal [61]
18 June 2010a
Serum Institute ofIndia Ltd., Pune
Swine A/H1N1 Influenza Vaccineinactivated, adjuvanted.
23 July 2010a
Cadila HealthcareLtd., Ahmedabad
Inactivated Influenza vaccine(whole-virion) Pandemic Influenza(H1N1) 2009, Monovalent vaccine
11 May 2010a
Bharat BiotechInternationalLtd., Hyderabad
Adjuvanted-H1NIvaccine(Inactivated)-HN-VAC PurifiedHemagglutinin (HA) Antigen ofA/California/7/2009 NYNCX
30 September2010
Panacea Biotec Ltd.,India
Inactivated H1N1 split virionVaccine (both adjuvanted andnon-adjuvanted
8 November2010
o
ppmaawiicatbtto
3
tPeduvtIIvTatrtgatavdtai
public distribution system to private practitioners for vaccination
a Received manufacturing license much before the WHO declared the pandemicver.
requalification processes should be carried out in a manner thatrevents unnecessary delays, enabling manufacturers to supplyarkets outside India and encouraging them to take higher risks
nd invest capital into development of more indigenously producednd epidemiologically suitable vaccines. A streamlined single-indow assessment system would prevent avoidable delays. There
s also an urgent need for recognition of national regulatory author-ties from other developing countries with vaccine manufacturingapacity; this will speed up assessment and availability of vaccineslready tested in these countries. Having an accredited labora-ory to support national regulatory authority function would beeneficial in the long run. In addition, vaccine quality and regula-ory systems should be understood by all stakeholders involved inhe development and utilization of vaccines, including civil societyrganizations.
. Vaccine deployment within India
The EPI was launched in India in 1978. In 1985, the name ofhe program in India was changed to the Universal Immunizationrogram (UIP), with activities scaled up in a phased manner to thentire country by 1990. This program was included in the repro-uctive and child health program in 1997 and was finally broughtnder the National Rural Health Mission (NRHM) in 2005. Withaccines against six vaccine-preventable diseases (VPDs) adminis-ered under UIP targeting a birth cohort of 27 million each year,ndia has one of the largest immunization systems in the world.mmunization is carried out through the public system and by pri-ate practitioners, the latter serving about 25% of the population.he Federal structure for health delivery system is both strengthnd a weakness in the Indian context. The central governmentakes most of the decisions related to vaccine introduction and isesponsible for procuring all the vaccines used in the country. Onhe other hand, state governments execute the immunization pro-ram, with some help from external development partners as wells the central government. Communication between the state andhe central government therefore, has to be very prompt to avoidny stock-outs. The States have some freedom to choose additionalaccines depending of the available finances, sometimes promptingecisions to introduce the vaccine at a national level. In addition
o the major challenges for vaccine deployment posed by hugend diverse population, spread over various geographical terrainsn the country; drought, floods, a large migrating population and1S (2013) B43– B53
problems with the cold chain system effect vaccine deployment ata more local level with in states.
3.1. Current coverage for basic EPI vaccines and polio-free status
The current full coverage for six basic vaccines is 61%; most ofthe remaining 40% of children belong to the most vulnerable sec-tion of the population. The national average for coverage of routineimmunization has been increasing at a very slow pace [52]. Thereare wide variations between and within states; some of the betterperforming states have vaccine coverage above 90%, but 11 stateshave over 50% of children who have no access to even the basicvaccines. Approximately 12% of children do not receive a singledose of any vaccine, and nearly 30% of children receive only partialimmunization [52].
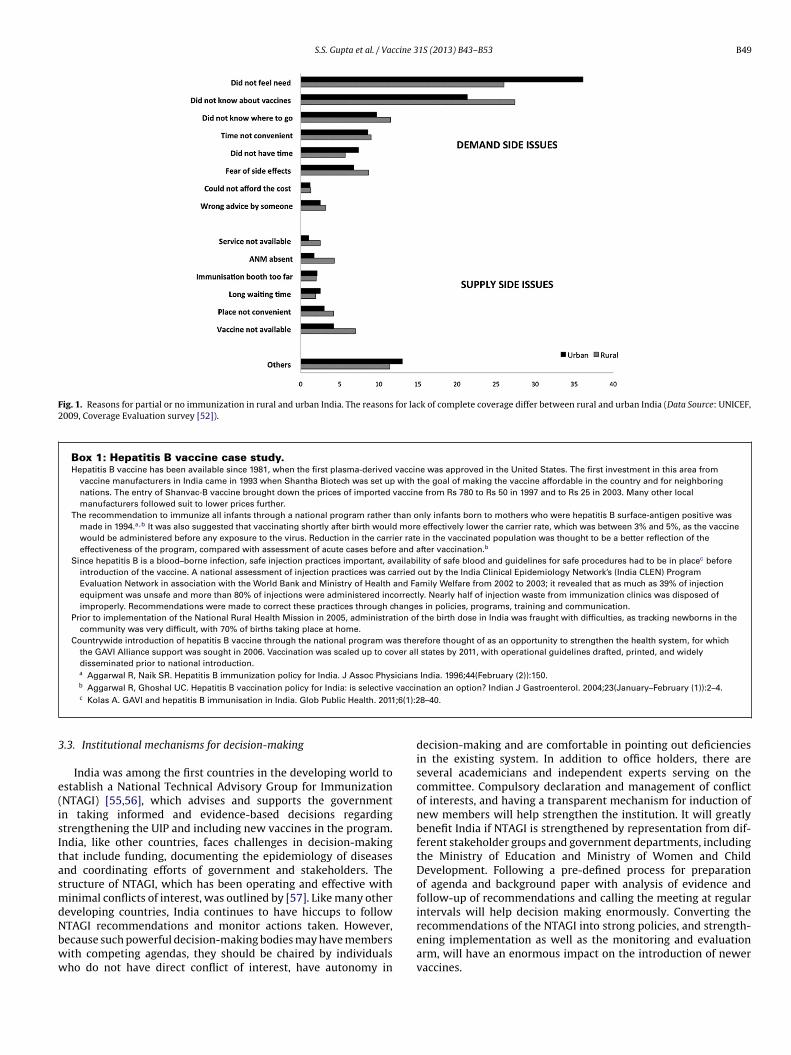
Both lack of utilization of vaccines and lack of access to themhave been key reasons for poor coverage (Fig. 1). The Coverage Eval-uation Survey 2009 undertaken by UNICEF shows that 36% of urbanand 26% of parents living in rural areas did not feel there was a needto vaccinate their children while approximately 25% of parents didnot know that their children could be protected with vaccines.These fractions would translate to substantially large numbers ofchildren not being immunized. Different reasons for partial or noimmunization in rural and urban India also highlights that our com-munication strategy for has to be different according to the targetpopulation.
Notwithstanding the poor performance of the immunizationprogram in general, India was able to interrupt the transmissionof the wild poliovirus and has been polio-free since January 2011.This was an extremely challenging task and indicates that thecountry is capable of ensuring access to and uptake of the vac-cine across all population segments and geographic regions of thecountry. The country was able to achieve this feat not only becauseof technological innovation (introduction of mono- and bivalentoral polio vaccine) but also because of specific targeting of migrantpopulations, identifying high risk areas, modifying communica-tion strategies to address issues of resistance to the vaccine andreinforcing programs such as the total sanitation campaign in highrisk areas [53]. All these interventions were possible in the contextof a high level of political commitment and international advocacy.
3.2. Recent vaccine introductions
India has been slow to introduce new vaccines in its UIP. Immu-nization with the HBV vaccine, initially introduced in 10 states,was extended to the entire country beginning in 2011. This is aclassic example of delayed introduction of a vaccine even whenindigenous vaccines were available (see Box 1). JE vaccine has beengradually introduced since 2005, and by 2011, 111 districts in 15JE-endemic states were reached. Introduction of the second dose ofmeasles vaccine in India through routine immunization and sup-plemental immunization activities was a big challenge that Indiasuccessfully met [54]. However, supplemental immunization activ-ities put a strain on the insufficient work force and resources ofroutine immunization in most areas, affecting the vaccine coverage.
The pentavalent vaccine containing the Hib antigen is anothereffort toward improving coverage. This vaccine was successfullyintroduced in the states of Kerala and Tamil Nadu in 2011, whichwere chosen because of their efficient health systems; it will beintroduced in other states over next two or three years. With goodlocal production capacity to produce this combination vaccine, thecost is likely to spiral down as demand increases, as was the casewith HBV vaccine. For the pentavalent vaccine, parents preferred
(experience shared by state immunization officer in a meeting)indicating their increasing confidence in the public immunizationprogram.
S.S. Gupta et al. / Vaccine 31S (2013) B43– B53 B49
Fig. 1. Reasons for partial or no immunization in rural and urban India. The reasons for lack of complete coverage differ between rural and urban India (Data Source: UNICEF,2009, Coverage Evaluation survey [52]).
Box 1: Hepatitis B vaccine case study.Hepatitis B vaccine has been available since 1981, when the first plasma-derived vaccine was approved in the United States. The first investment in this area from
vaccine manufacturers in India came in 1993 when Shantha Biotech was set up with the goal of making the vaccine affordable in the country and for neighboringnations. The entry of Shanvac-B vaccine brought down the prices of imported vaccine from Rs 780 to Rs 50 in 1997 and to Rs 25 in 2003. Many other localmanufacturers followed suit to lower prices further.
The recommendation to immunize all infants through a national program rather than only infants born to mothers who were hepatitis B surface-antigen positive wasmade in 1994.a,b It was also suggested that vaccinating shortly after birth would more effectively lower the carrier rate, which was between 3% and 5%, as the vaccinewould be administered before any exposure to the virus. Reduction in the carrier rate in the vaccinated population was thought to be a better reflection of theeffectiveness of the program, compared with assessment of acute cases before and after vaccination.b
Since hepatitis B is a blood–borne infection, safe injection practices important, availability of safe blood and guidelines for safe procedures had to be in placec beforeintroduction of the vaccine. A national assessment of injection practices was carried out by the India Clinical Epidemiology Network’s (India CLEN) ProgramEvaluation Network in association with the World Bank and Ministry of Health and Family Welfare from 2002 to 2003; it revealed that as much as 39% of injectionequipment was unsafe and more than 80% of injections were administered incorrectly. Nearly half of injection waste from immunization clinics was disposed ofimproperly. Recommendations were made to correct these practices through changes in policies, programs, training and communication.
Prior to implementation of the National Rural Health Mission in 2005, administration of the birth dose in India was fraught with difficulties, as tracking newborns in thecommunity was very difficult, with 70% of births taking place at home.
Countrywide introduction of hepatitis B vaccine through the national program was therefore thought of as an opportunity to strengthen the health system, for whichthe GAVI Alliance support was sought in 2006. Vaccination was scaled up to cover all states by 2011, with operational guidelines drafted, printed, and widelydisseminated prior to national introduction.a Aggarwal R, Naik SR. Hepatitis B immunization policy for India. J Assoc Physicians India. 1996;44(February (2)):150.b
vaccin;6(1):2
3
e(isItasmdNbww
Aggarwal R, Ghoshal UC. Hepatitis B vaccination policy for India: is selectivec Kolas A. GAVI and hepatitis B immunisation in India. Glob Public Health. 2011
.3. Institutional mechanisms for decision-making
India was among the first countries in the developing world tostablish a National Technical Advisory Group for ImmunizationNTAGI) [55,56], which advises and supports the governmentn taking informed and evidence-based decisions regardingtrengthening the UIP and including new vaccines in the program.ndia, like other countries, faces challenges in decision-makinghat include funding, documenting the epidemiology of diseasesnd coordinating efforts of government and stakeholders. Thetructure of NTAGI, which has been operating and effective withinimal conflicts of interest, was outlined by [57]. Like many other
eveloping countries, India continues to have hiccups to followTAGI recommendations and monitor actions taken. However,
ecause such powerful decision-making bodies may have membersith competing agendas, they should be chaired by individualsho do not have direct conflict of interest, have autonomy ination an option? Indian J Gastroenterol. 2004;23(January–February (1)):2–4.8–40.
decision-making and are comfortable in pointing out deficienciesin the existing system. In addition to office holders, there areseveral academicians and independent experts serving on thecommittee. Compulsory declaration and management of conflictof interests, and having a transparent mechanism for induction ofnew members will help strengthen the institution. It will greatlybenefit India if NTAGI is strengthened by representation from dif-ferent stakeholder groups and government departments, includingthe Ministry of Education and Ministry of Women and ChildDevelopment. Following a pre-defined process for preparationof agenda and background paper with analysis of evidence andfollow-up of recommendations and calling the meeting at regularintervals will help decision making enormously. Converting therecommendations of the NTAGI into strong policies, and strength-
ening implementation as well as the monitoring and evaluationarm, will have an enormous impact on the introduction of newervaccines.
B cine 3
3
3
oPtdsvtod
tfwiTwec
3
icetafoiibwwapsa
33becpmsfpgo2icilarep
3c
50 S.S. Gupta et al. / Vac
.4. Challenges in decisions-making process
.4.1. Lack of locally generated evidenceTraditionally, the Central Bureau of Health Intelligence carries
ut VPD surveillance in India. The Integrated Disease Surveillanceroject (IDSP), a World Bank-funded project, was initiated in 2004o institutionalize surveillance of key infectious and non-infectiousiseases throughout the country [58]. However, both systems havehortfalls and provide fragmented data. In addition, for some newaccines, such as Hib and the pneumococcal conjugate vaccine,here is a need for continuous surveillance over a long period inrder to identify changes in occurrence of the diseases and serotypeistribution.
The National Polio Surveillance Project (NPSP), supported byhe WHO, has a network of approximately 40,000 reporting unitsor syndrome-based detection of acute flaccid paralysis associatedith poliomyelitis. These units are assisted by a good laboratory
nfrastructure with capability for molecular analysis of isolates [53].he NPSP is now supporting the national immunization programith VPD surveillance, particularly for measles. There also are sev-
ral initiatives from professional bodies and vaccine industries toarry out VPD surveillance [59,60].
.4.2. FinancingAs a result of the growing GDP, more resources are available
n India for health care than ever before, yet the amount allo-ated remains much below expected level. Almost 25% of the globalxpenditure on polio eradication initiatives is in India and the coun-ry has been utilizing approximately 130 million for this programt the national level, which is roughly twice the central budgetor all routine immunizations. There has been an increase in theverall budget of the NRHM to Indian Rupees (Rs) 208,220 millionn 2012–2013, a 27% rise from 2010 to 2011. Even if governmentnvestment in health care reaches the predicted 3% of GDP marky 2020, a separate allocation for immunization is desirable, failinghich, priorities of providing universal coverage for curative healthill continue to compete endlessly with that of expanding cover-
ge and introducing new vaccines. Having a sustainable financinglan for the introduction of new vaccines and allowing the privateector to play a significant role along with the public sector, willlso improve coverage of existing current EPI vaccines.
.4.3. Health system issues
.4.3.1. Human resources. Shortages in the trained work force,oth technical (researchers and analysts, public heath specialists,pidemiologists) and operational (health care providers, staff forold chain maintenance, etc.), exist at all levels and more so inoorly performing states. Although the numbers of auxiliary nurseidwives, who provide last-mile delivery to the community, at
ub-centers and primary health centers increased by about 56%rom 2005 to 2011 [61], there are a significant number of vacantositions [62]. There is nearly a 40% shortage of qualified medicalraduates for health facilities at the grassroots level. Introductionf schemes such as Janani Suraksha Yojna (JSY) under NRHM in005 brought about an increase in the number of births occurring in
nstitutions [5], and this type of access to maternal and child healthare in the community was expected to bring about an increasen immunization coverage. But the rise in caseloads following theaunch of JSY actually reduced the time auxiliary nurse midwivesnd other providers could spend on immunization and resulted ineduced coverage, at least in certain states. The immunization cov-rage improved where it was adequately supported by additional
roviders through the Yashoda Scheme [63]..4.3.2. Supply chain. Lack of oversight and coordination of the pro-esses for producing and deploying vaccines have led to problems
1S (2013) B43– B53
regarding the supply chain and regular availability of vaccines atoutreach clinics. A number of public and private sector manufac-turers in India supply vaccines for use in the UIP. As has beenmentioned, accurate and timely forecasting of the demand for vac-cines is a major bottleneck in the timely manufacture and deliveryof required doses of vaccines in the country.
3.4.3.3. Cold chain. There are several new vaccines waiting forentry into the UIP program. With this anticipated increased pres-sure on the cold chain, a nationwide assessment of cold chainequipment was carried out in 2008 by UNICEF [64], with a 300%increase in capacity in the cold chain predicted to be needed. Unlessgood use is made of storage facilities (e.g., multi-dose packaging ofvaccines and innovative power back-up systems), the capacity ofthe cold chain will be a major challenge, especially in remote areaswith limited power supply.
3.5. Advocacy and communication
Advocacy and effective communication for immunization pro-grams maintain the confidence of stakeholders and should betailored for specific audiences, whether policymakers, parlia-mentarians, industry or the community. In communicating withcommunity members and policymakers alike, there is a need toconvey the broader spectrum of health benefits brought about byvaccination. For example, studies that could illustrate improve-ments in other health indicators when immunization servicesare provided need to be carried out and the results widely dis-seminated. There should also be efforts to establish educationalprograms for civil society organizations that work in health-relatedprograms, so that they can be informed of the risks and benefits ofvaccines and can then appropriately educate the community. Thisengagement with civil society should include medical and scien-tific experts and industry professionals so that concerns that ariseare adequately addressed. Addressing disinformation is anotherimportant activity communication experts need to carry out proac-tively to prevent erosion of public confidence in immunization.
3.6. Vaccine deployment: the way forward
3.6.1. VPD surveillanceNew initiatives for establishing nationwide disease surveillance
mechanisms are in place and studies have been funded to estimatethe burden of VPDs. Supporting science for development of appro-priate diagnostics and validation for VPDs should be in place inorder to make surveillance cost-effective. These efforts can includebiomarker discovery, instrumentation and in-country sources ofdiagnostic intermediates. Moving from regular surveys to system-atically planned community-based surveillance will enhance andquicken the decision-making process regarding new vaccines inthe country. Until this initiative yields results, in order to supportdecision-making, datasets available from neighboring countriescan be analyzed and modeled in support of the introduction ofnewer vaccines in the immunization program.
The public institutions lack the capability to carry out Phase IVpost-marketing surveillance studies for the newer vaccines. Whilethis capacity is being built, the wealth of data that is available fromvaccine manufacturers that can be used for documenting the safetyof many of these vaccines.
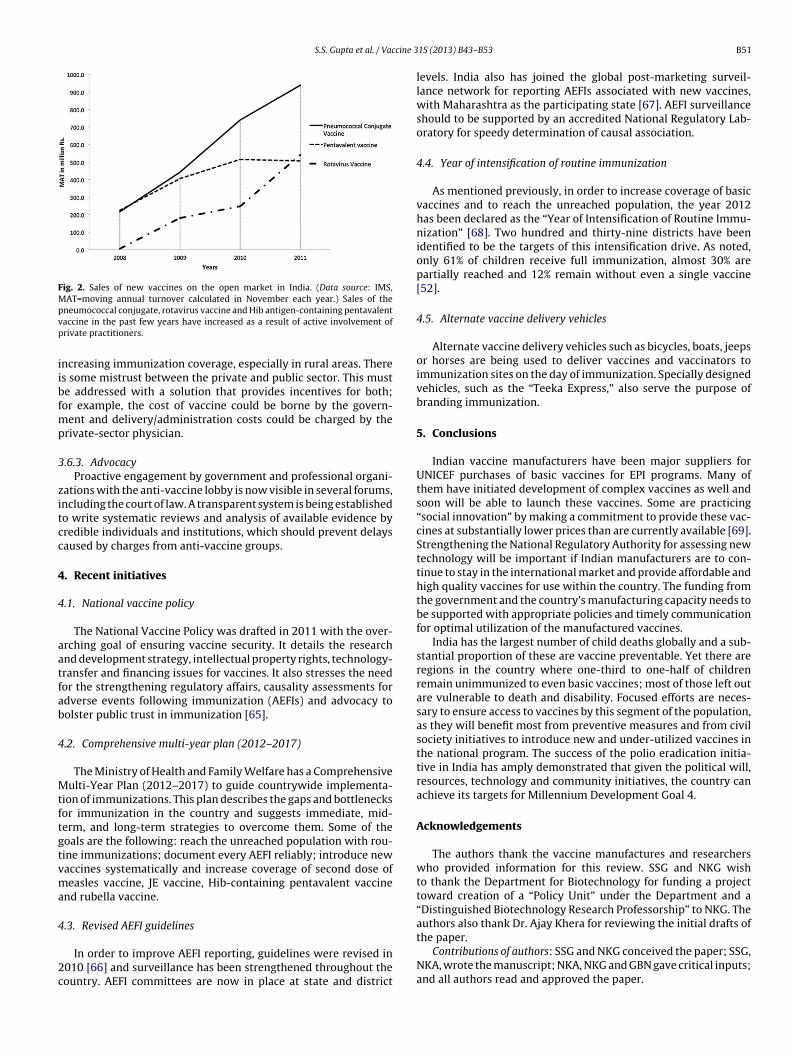
3.6.2. Public- vs. private-sector deliveryThe sales of new vaccines in the open market through the private
sector in the country can provide critical data for decision makingfor their nation wide introduction (Fig. 2). Nearly 75% of curativecare in the country is delivered by the private sector in both urbanand rural areas, and this sector could contribute immensely to
S.S. Gupta et al. / Vaccine 3
Fig. 2. Sales of new vaccines on the open market in India. (Data source: IMS,MAT=moving annual turnover calculated in November each year.) Sales of thepvp
iibfmp
3
zitcc
4
4
aatfab
4
Mtftgtvma
4
2c
neumococcal conjugate, rotavirus vaccine and Hib antigen-containing pentavalentaccine in the past few years have increased as a result of active involvement ofrivate practitioners.
ncreasing immunization coverage, especially in rural areas. Theres some mistrust between the private and public sector. This muste addressed with a solution that provides incentives for both;or example, the cost of vaccine could be borne by the govern-
ent and delivery/administration costs could be charged by therivate-sector physician.
.6.3. AdvocacyProactive engagement by government and professional organi-
ations with the anti-vaccine lobby is now visible in several forums,ncluding the court of law. A transparent system is being establishedo write systematic reviews and analysis of available evidence byredible individuals and institutions, which should prevent delaysaused by charges from anti-vaccine groups.
. Recent initiatives
.1. National vaccine policy
The National Vaccine Policy was drafted in 2011 with the over-rching goal of ensuring vaccine security. It details the researchnd development strategy, intellectual property rights, technology-ransfer and financing issues for vaccines. It also stresses the needor the strengthening regulatory affairs, causality assessments fordverse events following immunization (AEFIs) and advocacy toolster public trust in immunization [65].
.2. Comprehensive multi-year plan (2012–2017)
The Ministry of Health and Family Welfare has a Comprehensiveulti-Year Plan (2012–2017) to guide countrywide implementa-
ion of immunizations. This plan describes the gaps and bottlenecksor immunization in the country and suggests immediate, mid-erm, and long-term strategies to overcome them. Some of theoals are the following: reach the unreached population with rou-ine immunizations; document every AEFI reliably; introduce newaccines systematically and increase coverage of second dose ofeasles vaccine, JE vaccine, Hib-containing pentavalent vaccine
nd rubella vaccine.
.3. Revised AEFI guidelines
In order to improve AEFI reporting, guidelines were revised in010 [66] and surveillance has been strengthened throughout theountry. AEFI committees are now in place at state and district
1S (2013) B43– B53 B51
levels. India also has joined the global post-marketing surveil-lance network for reporting AEFIs associated with new vaccines,with Maharashtra as the participating state [67]. AEFI surveillanceshould to be supported by an accredited National Regulatory Lab-oratory for speedy determination of causal association.
4.4. Year of intensification of routine immunization
As mentioned previously, in order to increase coverage of basicvaccines and to reach the unreached population, the year 2012has been declared as the “Year of Intensification of Routine Immu-nization” [68]. Two hundred and thirty-nine districts have beenidentified to be the targets of this intensification drive. As noted,only 61% of children receive full immunization, almost 30% arepartially reached and 12% remain without even a single vaccine[52].
4.5. Alternate vaccine delivery vehicles
Alternate vaccine delivery vehicles such as bicycles, boats, jeepsor horses are being used to deliver vaccines and vaccinators toimmunization sites on the day of immunization. Specially designedvehicles, such as the “Teeka Express,” also serve the purpose ofbranding immunization.
5. Conclusions
Indian vaccine manufacturers have been major suppliers forUNICEF purchases of basic vaccines for EPI programs. Many ofthem have initiated development of complex vaccines as well andsoon will be able to launch these vaccines. Some are practicing“social innovation” by making a commitment to provide these vac-cines at substantially lower prices than are currently available [69].Strengthening the National Regulatory Authority for assessing newtechnology will be important if Indian manufacturers are to con-tinue to stay in the international market and provide affordable andhigh quality vaccines for use within the country. The funding fromthe government and the country’s manufacturing capacity needs tobe supported with appropriate policies and timely communicationfor optimal utilization of the manufactured vaccines.
India has the largest number of child deaths globally and a sub-stantial proportion of these are vaccine preventable. Yet there areregions in the country where one-third to one-half of childrenremain unimmunized to even basic vaccines; most of those left outare vulnerable to death and disability. Focused efforts are neces-sary to ensure access to vaccines by this segment of the population,as they will benefit most from preventive measures and from civilsociety initiatives to introduce new and under-utilized vaccines inthe national program. The success of the polio eradication initia-tive in India has amply demonstrated that given the political will,resources, technology and community initiatives, the country canachieve its targets for Millennium Development Goal 4.
Acknowledgements
The authors thank the vaccine manufactures and researcherswho provided information for this review. SSG and NKG wishto thank the Department for Biotechnology for funding a projecttoward creation of a “Policy Unit” under the Department and a“Distinguished Biotechnology Research Professorship” to NKG. Theauthors also thank Dr. Ajay Khera for reviewing the initial drafts of
the paper.Contributions of authors: SSG and NKG conceived the paper; SSG,NKA, wrote the manuscript; NKA, NKG and GBN gave critical inputs;and all authors read and approved the paper.

B cine 3
C
R
[
[
[
[
[
[
[
[[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
52 S.S. Gupta et al. / Vac
onflict of interest
The authors declare they have no conflict of interest.
eferences
[1] World Development Indicators & Global Development Finance database [Inter-net]. Washington: The World Bank; 1960–2011. India data. Available from:http://data.worldbank.org/country/india?display=graph [cited 30.07.12].
[2] Bhadoria V, Mitra P. India Pharma 2020: propelling access and acceptance, real-ising true potential [white paper]. New Delhi: McKinsey & Company, Inc.; 2010.Available from: http://www.mckinsey.com/client service/pharmaceuticalsand medical products/latest thinking [cited 30.07.12].
[3] Press Information Bureau, Government of India. Indian vaccine marketreaches $900 million [press release]. New Delhi: Press Information Bureau;2011 November. Available from: http://www.pib.nic.in/newsite/erelease.aspx?relid=77172 [cited 22.08.12].
[4] Wilson P, Rao A. India’s role in global R&D. Washington, DC: Results for Devel-opment Institute; 2012.
[5] International Institute for Populations Sciences (IIPS). District Level Householdand Facility Survey (DLHS-3), 2007–08 [Internet]. Mumbai: IIPS; 2010 April.Available from: http://www.rchiips.org/pdf/INDIA REPORT DLHS-3.pdf [cited28.07.12].
[6] Laxminarayan R, Ganguly NK. India’s vaccine deficit: why more than half ofIndian children are not fully immunized, and what can—and should—be done.Health Aff 2011;30(June (6)):1096–103.
[7] Translational Health Science and Technology Institute (THSTI) [Internet]. Gur-gaon: THSTI; 2012. Clinical Development Services Agency. Available from:http://www.thsti.res.in/cdsa/about cdsa.php [cited 06.08.12].
[8] Indian Council of Medical Research (ICMR) [Internet]. New Delhi: ICMR;2010. Highlights of ICMR Activities & Achievements. Available from:http://www.icmr.nic.in/About Us/ICMR Achievements.html [cited 08.08.12].
[9] MSD. Wellcome Trust Hilleman Laboratories Pvt. Ltd. [Internet]. New Delhi:MSD Wellcome Trust; 2012. Available from: http://www.hillemanlabs.org[cited 30.07.12].
10] Vaccine Grand Challenge Programme at Department of Biotechnology,Ministry of Science and Technology, Government of India [Internet].New Delhi; 2010. Available from: http://www.google.co.in/url?sa=t&rct=j&q=&esrc=s&source=web&cd=2&ved=0CE0QFjAB&url=http%3A%2F%2Fdbtindia.nic.in%2Fdocs%2FVGCP DBT.doc&ei=l14gUMPmC5HrrQeokoD4Cg&usg=AFQjCNHT wm9aGBHZKzMeWP51pAcInpIkA [cited 06.08.12].
11] Malaria Vaccine Development Programme (MVDP) [Internet]. New Delhi:MVDP; 2012. Available from: http://www.mvdp.org.in/index.php [cited05.08.12].
12] ICGEB-EMORY Vaccine Center [Internet]. Atlanta: Emory University;2007. Available from: http://www.globalhealth.emory.edu/programs/facultyPrograms/globalVaccines.php [cited 05.08.12].
13] Biotech Ignition Grants [Internet]. New Delhi: BIRAC; 2012. Available from:http://www.birac.nic.in/programmes.php?prg=big [cited 29.07.12].
14] Division of Microbiology and Infectious Diseases, National Institute ofAllergy and Infectious Diseases (NIAID) [Internet]. Indo-US Vaccine ActionProgram. Bethesda, MD: NIAID. Available from: http://www.niaid.nih.gov/about/organization/dmid/indo/Pages/funding.aspx [updated 16.10.12; cited28.07.12].
15] Economic survey 2011–12. New Delhi: Ministry of Finance, Government ofIndia [chapter 9], 2012.
16] Singh S. A shot of India: the vaccine market. Forbes India Magazine[Internet]; 2011 May. Available from: http://www.forbesindia.com/article/boardroom/a-shot-of-india-the-vaccine-market/24822/1?id=24822&pg=1.Epub 2011 May 9 [cited 15.08.12].
17] Jayaraman K. India opens malaria vaccine center. Nat Med 2012;18(3):332–3.18] PATH Malaria Vaccine Initiative partners with Tulane University and India’s
Gennova Biopharmaceuticals to push development of transmission-blockingvaccine. Washington: PATH Malaria Vaccine Initiative; 1995–2012. Avail-able from: http://www.malariavaccine.org/MVI-Tulane-Gennova-2011.php[15.02.11; cited 30.07.12].
19] Lopez-Macias C, Ferat-Osorio E, Tenorio-Calvo A, Isibasi A, Talavera J, Arteaga-Ruiz O, et al. Safety and immunogenicity of a virus-like particle pandemicinfluenza A (H1N1) 2009 vaccine in a blinded, randomized, placebo-controlledtrial of adults in Mexico. Vaccine 2011;29(October (44)):7826–34.
20] First vaccine against fatal visceral leishmaniasis enters clinical trial [pressrelease]. Seattle: Infectious Disease Research Institute; 2012 February. Avail-able from: http://www.idri.org/press-2-22-12.html [cited 03.08.12].
21] Serum Institute of India Ltd. acquires Bilthoven Biologicals of Netherlands[press release]. Pune: Serum Institute of India Ltd.; 2012 July. Available from:http://www.seruminstitute.com/content/news 9.htm [cited 08.08.12].
22] Rabaxy enters vaccines arena with the acquisition of product rights and man-ufacturing facility from Biovel [press release]. Gurgaon: Ranbaxy Laboratories
Ltd.; 2010 January. Available from: http://www.ranbaxy.com/news/newsdisp.aspx?cp=950&flag=LN [cited].23] The Meningitis Vaccine Project [fact sheet]. Seattle: PATH; 2011 September.Available from: http://www.path.org/publications/files/ER mvp fs.pdf [cited15.07.12].
[
1S (2013) B43– B53
24] Deen JL, von Seidlein L, Sur D, Agtini M, Lucas ME, Lopez AL, et al. The highburden of cholera in children: comparison of incidence from endemic areas inAsia and Africa. PLoS Negl Trop Dis 2008;2(February (2)):e173.
25] Sur D, Deen JL, Manna B, Niyogi SK, Deb AK, Kanungo S, et al. The burden ofcholera in the slums of Kolkata, India: data from a prospective, communitybased study. Arch Dis Child 2005;90(November (11)):1175–81.
26] Miles MG, Lewis KD, Kang G, Parashar UD, Steele AD. A systematic reviewof rotavirus strain diversity in India, Bangladesh, and Pakistan. Vaccine2012;30(April (Suppl. 1)):A131–9.
27] Jain V, Parashar UD, Glass RI, Bhan MK. Epidemiology of rotavirus in India.Indian J Pediatr 2001 Sep;68(9):855–62.
28] Lopez-Gigosos RM, Plaza E, Diez-Diaz RM, Calvo MJ. Vaccination strate-gies to combat an infectious globe: oral cholera vaccines. J Glob Infect Dis2011;3(January (1)):56–62.
29] Verma R, Khanna P, Chawla S. Cholera vaccine: new preventive tool for endemiccountries. Hum Vaccin Immun 2012;8(May (5)):682–4.
30] Neogi SB, Hasan H, Sheikh K, Zodpey S. Scope for rotavirus vaccination inIndia: revisiting the scientific evidence. Indian J Pediatr 2011;78(October(10)):1251–5.
31] Esposito DH, Tate JE, Kang G, Parashar UD. Projected impact and cost-effectiveness of a rotavirus vaccination program in India, 2008. Clin Infect Dis2011;52(January (2)):171–7.
32] Bhandari N, Sharma P, Glass RI, Ray P, Greenberg H, Taneja S, et al. Safety andimmunogenicity of two live attenuated human rotavirus vaccine candidates,116E and I321, in infants: results of a randomised controlled trial. Vaccine2006;24(July (31–32)):5817–23.
33] Mahalanabis D, Lopez AL, Sur D, Deen J, Manna B, Kanungo S, et al. A ran-domized, placebo-controlled trial of the bivalent killed, whole-cell, oral choleravaccine in adults and children in a cholera endemic area in Kolkata, India. PLoSOne 2008;3(June (6)):e2323.
34] Sur D, Lopez AL, Kanungo S, Paisley A, Manna B, Ali M, et al. Efficacy andsafety of a modified killed-whole-cell oral cholera vaccine in India: an interimanalysis of a cluster-randomised, double-blind, placebo-controlled trial. Lancet2009;374(November (9702)):1694–702.
35] Holmgren J, Clemens J, Sack DA, Svennerholm AM. New cholera vaccines. Vac-cine 1989;7(April (2)):94–6.
36] Anh DD, Canh do G, Lopez AL, Thiem VD, Long PT, Son NH, et al. Safety andimmunogenicity of a reformulated Vietnamese bivalent killed, whole-cell, oralcholera vaccine in adults. Vaccine 2007;25(January (6)):1149–55.
37] Date KA, Vicari A, Hyde TB, Mintz E, Danovaro-Holliday MC, Henry A,et al. Considerations for oral cholera vaccine use during outbreak afterearthquake in Haiti, 2010–2011. Emerg Infect Dis 2011;17(November (11)):2105–12.
38] von Seidlein L, Deen JL. Considerations for Oral Cholera vaccine use duringoutbreak after earthquake in Haiti, 2010–2011. Emerg Infect Dis 2012;18(July(7)):1211–4.
39] Ivers LC, Farmer PE, Pape WJ. Oral cholera vaccine and integrated cholera con-trol in Haiti. Lancet 2012;379(June (9831)):2026–8.
40] Bhan MK, Lew JF, Sazawal S, Das BK, Gentsch JR, Glass RI. Protection conferredby neonatal rotavirus infection against subsequent rotavirus diarrhea. J InfectDis 1993;168(August (2)):282–7.
41] Cunliffe NA, Das BK, Ramachandran M, Bhan MK, Glass RI, Gentsch JR.Sequence analysis demonstrates that VP6, NSP1 and NSP4 genes of Indianneonatal rotavirus strain 116E are of human origin. Virus Genes 1997;15(1):39–44.
42] Glass RI, Bhan MK, Ray P, Bahl R, Parashar UD, Greenberg H, et al. Developmentof candidate rotavirus vaccines derived from neonatal strains in India. J InfectDis 2005;192(September (Suppl. 1)):S30–5.
43] Excler JL, Kochhar S, Kapoor S, Das S, Bahri J, Ghosh MD, et al. Preparedness forAIDS vaccine trials in India. Indian J Med Res 2008;127(June (6)):531–8.
44] Berkley S. HIV vaccine trials in India [author reply 6]. Nat Biotechnol2008;26(May (5)):495.
45] Sahay S, Mehendale S. Addressing ethical concerns in the Indian HIV vaccinetrials. Indian J Med Ethics 2004;1(October–December (4)):109–12.
46] Suhadev M, Nyamathi AM, Swaminathan S, Suresh A, Venkatesan P. Factorsassociated with willingness to participate in HIV vaccine trials among high-risk populations in South India. AIDS Res Hum Retroviruses 2009;25(February(2)):217–24.
47] Mehendale S, van Lunzen J, Clumeck N, Rockstroh J, Vets E, Johnson PR, et al. Aphase 1 study to evaluate the safety and immunogenicity of a recombinant HIVtype 1 subtype C adeno-associated virus vaccine. AIDS Res Human Retroviruses2008;24(June (6)):873–80.
48] Mehendale S, Sahay S, Thakar M, Sahasrabuddhe S, Kakade M, SheteA, et al. Safety & immunogenicity of tgAAC09, a recombinant adeno-associated virus type 2 HIV-1 subtype C vaccine in India. Indian J Med Res2010;132(August):168–75.
49] Hendriks J, Liang Y, Zeng B. China’s emerging vaccine industry. Hum Vaccin2010;6(July (7)):602–7.
50] Central Drugs Standard Control Oragnisation (CDSCO) [Internet]. New Delhi:CDSCO; 2012. Available from: http://www.cdsco.nic.in [cited 20.07.12].
51] Clinical Trials Registry—India. New Delhi Indian Council of Medical Research;
2012. Available from: http://www.ctri.in [cited 20.07.12].52] United Nations Children’s Fund (UNICEF). 2009 coverage evaluation sur-vey: all India report [Internet]. New Delhi: UNICEF; 2010. Availablefrom: http://www.unicef.org/india/1 - CES 2009 All India Report.pdf [cited03.08.12].

cine 3
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
who.int/LinkFiles/RC64 R3.pdf [cited 20.08.12].[69] GAVI welcomes lower prices for life-saving vaccines [press release].
S.S. Gupta et al. / Vac
53] National Polio Surveillance Project (NPSP) [Internet]. New Delhi: NPSP; 2012.Lab Network. Available from: http://www.npspindia.org/Lab Network.asp[cited 04.08.12].
54] Gupta SK, Sosler S, Haldar P, Hombergh H, Bose AS. Introduction strategy of asecond dose measles containing vaccine in India. Indian Pediatr 2011;48(May(5)):379–82.
55] John TJ. National Technical Advisory Group on Immunization: a major stepforward for child health. Indian Pediatr 2002;39(April (4)):327–30.
56] John TJ. India’s National Technical Advisory Group on immunisation. Vaccine2010;28(April (Suppl. 1)):A88–90.
57] Duclos P. National Immunization Technical Advisory Groups (NITAGs): guid-ance for their establishment and strengthening. Vaccine 2010;28(Suppl.1):A18–25.
58] Integrated Disease Surveillance Project (IDSP) [Internet]. Delhi: IDSP; 2012.Available from: http://idsp.nic.in [cited 20.10.12].
59] Indian Academy of Pediatrics Committee on Immunization. Consensus recom-mendations on immunisations and IAP immunization timetable 2012. IndianPediatr 2012;49(July (7)):549–64.
60] IDsurv.org [Internet]. Gandhidham Indian Academy of Pediatrics; 2011. Avail-able from: http://www.idsurv.org [cited 20.10.12].
61] Rural Health Statistics in India, 2011 [Internet]. New Delhi: Min-
istry of Health and Family Welfare; 2012. Highlights Available from:http://nrhm-mis.nic.in/UI/RHS/RHS 2011/Key Highlights from Rural HealthStatistics in India 2011.pdf [updated 2011 March; cited 05.08.12].62] Garg S, Singh R, Grover M. India’s health workforce: current status and the wayforward. Natl Med J India 2012;25(March–April (2)):111–3.
1S (2013) B43– B53 B53
63] Yashoda: an initiative to improve the quality of care for mother andnewborn in the maternity ward [brochure]. New Delhi: Norway India Partner-ship Initiative; 2012. Available from: http://www.nipi.org.in/Items/ResourcesOtherPublications BrochureYashoda.pdf [cited 08.08.12].
64] National cold chain assessment, India. New Delhi: UNICEF; 2008 July. Avail-able from: http://www.unicef.org/india/National Cold Chain AssessmentIndia July 2008.pdf [cited 08.08.12].
65] National vaccine policy. New Delhi: Ministry of Health and Family Welfare,Government of India; 2011.
66] Adverse events following immunization (AEFI): operational guidelines onsurveillance and response. New Delhi: Ministry of Health and Family Welfare,Government of India; 2010.
67] WHO Country Office, National Polio Surveillance Project, India. StrengtheningAEFI surveillance and investigation, Maharashtra state, India. Global Immu-nization News; 2012 May. Available from: http://www.who.int/immunization/GIN May 2012.pdf [cited 08.08.12]: 14.
68] World Health Organization Regional Office for Southeast Asia (WHO/SEARO).Resolution of WHO Regional Committee for South-East Asia. Jaipur, India.New Delhi: WHO/SEARO; 2011 September. Available from: http://www.searo.
Geneva: GAVI Alliance; 2011. Available from: http://www.gavialliance.org/library/news/press-releases/2011/gavi-welcomes-lower-prices-for-life-saving-vaccines [70] Bh [cited Insert date].