Embed Size (px)
Citation preview

Utilization of the extended rectus abdominis myofasciocutaneous free flap in upper extremity reconstruction
Degfoving injuries of the upper extremity may require extensivemoft tissue coverage. Free tissue transfer is often useful in the management of these injuries. We describe the use of an extended rectus abdomhrii myofasciocutaneous vascularized free flap in the management of a massive longitudinal upper extremity traumatic soft tissue defect. (J HAND SIJRG 1991;16A:590-3.)
Guy D. Foulkes, MD, Waldo E. Floyd III, MD, and Christopher L. McLendon, MD, Macon, Ga.
A variety of reconstructive alternatives are currently available to provide soft-tissue coverage
of extensive extremity wounds. Although transfer of muscle or fasciocutaneous free flaps offers distinct ad-
vantages, donor choices may be limited by flap dimen-
sion, donor site morbidity, or donor site accessibility. We report the utilization of a rectus abdominis free muscle flap with additional length provided by a fas- ciocutaneous banner in the management of an extensive upper extremity wound.
Case report
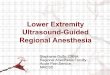
A 27-year-old man sustained a degloving injury to his dominant right upper extremity while attempting to repair a cotton cording machine (Fig. 1). The lateral arm was denuded
of skin, and a loose muscle flap based at the deltoid insertion covered the underlying humerus. The entire extensor com- partment of the forearm was avulsed except for a remnant of
brachioradialis. The radial nerve was avulsed in the spiral groove, and the radial artery was avulsed just distal to its origin. The radiocapitellar joint was open and the elbow joint hinged on the ulnar collateral ligament. The median nerve, although exposed, was intact. Bone was exposed from the
From the Department of Surgery, Mercer University School of Med-
icine, Emory University School of Medicine, 870 High St., Macon,
Ga.
Received for publication March 13, 1990; accepted in revised form
July 3, 1990.
No benefits in any form have been received or will be received from
a commercial party related directly or indirectly to the subject of
this article.
Reprint requests: Waldo E. Floyd III, MD, Clinical Associate F’ro-
fessor of Surgery, Mercer University School of Medicine, Emory University School of Medicine, 870 High St., Macon, GA 31201.
3/l/24062
proximal radius to the distal aspect of the first metacarpal.
The entire length of exposed bone measured 30 cm. Several therapeutic options were considered. including a
pedicled abdominal flap, latissimus dorsi flap,‘.’ and an ex- tended rectus abdominis myofasciocutaneous (ERAM) free flap.3,4 Because of the extensive area requiring coverage, it was believed that an extended ERAM free flap would be efficacious.
Five days after the injury, definitive wound coverage was planned. A template of the proposed flap was fashioned and transferred to the abdominal site, and an extended fasciocu- taneous banner flap originating over the superior aspect of the rectus muscle and terminating towards the tip of the right scapula was incised down to the external oblique aponeurosis (Fig. 2). The rectus abdominis muscle was then dissected from its sheath, and the periumbilical perforating vessels serv-
ing the fasciocutaneous portion of the flap were protected. After elevation of the muscle to the level of the arcuate line, the inferior epigastric vessels were identified and the vascular pedicle was followed to its origin from the external iliac artery and vein. The rectus abdominis muscle was then transected at its origin from the pubis.
After transfer of the flap to the upper extremity wound, microvascular end-to-end anastomosis of the deep inferior epigastric vein to the recipient basilic vein was done, and the deep inferior epigastric artery was anastomosed to the radial artery stump. The flap was oriented with the rectus muscle overlying the radius and the fasciocutaneous flap overlying the first metacarpal (Figs. 3 and 4). The exposed muscle and wound were then covered with split-thickness skin grafts.
The ERAM flap accomplished excellent coverage of this challenging wound (Fig. 5). Tendon transfers to provide ex- tensor function in the wrist and hand were subsequently done and the patient continues to progress in rehabilitation.
Discussion
Adequate coverage may be difficult to obtain in major degloving injuries. Traditional approaches involve a va-
590 THE JOURNAL OF HAND SURGERY

Vol. 16A, No. 4
July 1991 Extended rectus abdominis free muscle Jlap 591
Fig. 1. Massive degloving injury at time of initial debridement. Note exposed portion of radius
Fig. 2. Schematic view of extended rectus abdominis myofasciocutaneous free flap.

592 Foulkes et al. The Journal of
HAND SURGERY
Fig. 3. Orientation of the free flap overlying the right radius and first metacarpal.
Fig. 4. Flap in place after vascular anastomoses.
riety of pedicle truncal flaps and upper extremity flaps, including pectoralis major, latissimus dorsi, and rectus
abdominis , I* 4-6 or free flaps from the medial and lateral arm, groin, chest wall, and foot.‘.2.7 Limitations of the former group include difficult wound access, joint im-
mobilization, and the need for second-stage procedures. Free tissue transfer may obviate many of these short-
comings, but few of the previously described free flaps allow coverage of exceptionally large defects such as the case described. The transverse rectus abdominis myo- cutaneous (TRAM) flap, although capable of providing large surface area, lacks the longitudinal axially based pedicle that proved to be of great value in this case.
The rectus abdominis myocutaneous free flap, first described by Pennington and Pelly,3 seems to offer the ideal solution to this dilemma. Based on the vascular
studies of Boyd and colleagues,’ this flap offers length exceeding 30 cm, as well as large caliber vessels, a long vascular pedicle (up to 15 cm), and the option of fasciocutaneous extension.3 The banner modification employed in this case offered additional length, addi- tional skin coverage, and, by use of the ipsilateral rec- tus, a natural angle between the myo- and fasciocuta- neous portions to mold easily across the wrist (Fig. 2). This reconstructive alternative combines principles of vascularized muscle and vascularized fasciocutaneous free transfer of tissue. The arterial perforators sustaining the fasciocutaneous portion of this flap arise from the vascularized muscular segment. The entire operation can be performed on the supine patient. Unlike the TRAM flap, the ERAM flap offers less bulk, an end- based axial pedicle, and an oblique rather than perpen-

Vol. 16A, No. 4
July 1991 Extended rectus abdominis free muscle Jlap 593
Fig. 5. Two months postoperatively wound is well healed, with extended rectus abdominis flap and split-thickness skin grafts.
dicular fasciocutaneous extension. These three advan-
tages were of key importance in management of this
longitudinal defect.
The rectus abdominis myofasciocutaneous free flap has not been previously described for the upper extrem- ity, although its use was anticipated by Manktelow.’ We believe that this versatile flap may serve as a valu- able adjunct in the management of extensive traumatic longitudinal soft tissue deficiency in the upper limb.
We gratefully acknowledge the assistance of Sheryl Bed- good for manuscript preparation, and Paula Huffmaster and Marjorie Lawrence for graphic aids.
REFERENCES
1, Manktelow RT. Free muscle transfers. In: Green DP, ed. Operative hand surgery, New York: Churchill Livingstone, 1988:1215-44.
2.
3.
4.
5.
6.
7.
8.
Lister G, Scheker L. Emergency free flaps to the upper extremity. J HAND SURG 1988;13A:22-8.
Pennington DG, Pelly AD. The rectus abdominis myo- cutaneous free flap. Br J Plast Surg 1980;33:277-82. Dowden RV, McGraw JB. Muscle flap reconstruction of shoulder defects. J HAND SURG 1980;5:382-90. Montoreano IE, Pujato D. Latissimus dorsi and rectus abdominis breast reconstruction postmastectomy: mus- culocutaneous breast reconstruction. Sem Surg Oncology 1987;3:247-57.
Sbitany V, Wray RC. Use of the rectus abdominis muscle flap to reconstruct an elbow defect. Plast Reconstr Surg 1985;77:988-99. Becker DW. Total arm flap. Ann Plast Surg 1987; 19:5,466-8.
Boyd JB, Taylor GI, Corlett R. The vascular territories of the superior epigastric systems. Plast Reconstr Surg 1984;73: l-14.