Embed Size (px)
Citation preview
ASSOCIATION FOR ACADEMIC SURGERY AND SOCIETY OF UNIVERSITY SURGEONS—ABSTRACTS 205
camera navigation (CN30), 30 degree with grasping (CN30G), tissueretracting (RET), tissue retracting and dissection (RETDIS), tube tra-verse (TUBE), and arrowmanipulation (ARROW). The table presentsiTCTs by task with means with standard deviations, medians withrange, and skewness. All eight tasks demonstrated wide ranges(over 10X) and positive skewness (long low performance tails).Conclusions: Novice learners display a very wide range of initialperformance levels on laparoscopic VR simulators despite the absenceof pre-practice effects. Our findings confirm the absence of a well-defined starting level of laparoscopic skill upon which to base a train-ing curriculum. Further studies examining the correlation of thesefindings to the amount and type of training required to reach profi-ciency are required.
Mean Median
Task
# Learners TotalTrialsiTCT (SD)Seconds
iTCT (Range)Seconds
SkewnessCN0
147 3346 192 (146) 138 (40-824) 1.46 CN0G 143 3749 229 (201) 115 (33-1106) 2.25 CN30 128 2578 198 (205) 170 (34-1096) 2.14 CN30G 114 2376 202 (170) 147 (43-958) 2.24 RET 111 1872 137 (75) 120 (35-437) 1.53 RETDIS 105 1573 201 (129) 173.5 (76-1100) 3.79 TUBE 95 1053 249 (142) 214 (59-865) 2.19 ARROW 86 1252 137 (124) 103 (44-1073) 5.4718.9. Use Of Decision-Based Simulations To Assess TeamSkills. C. M. Pugh; Northwestern University, Chicago, IL
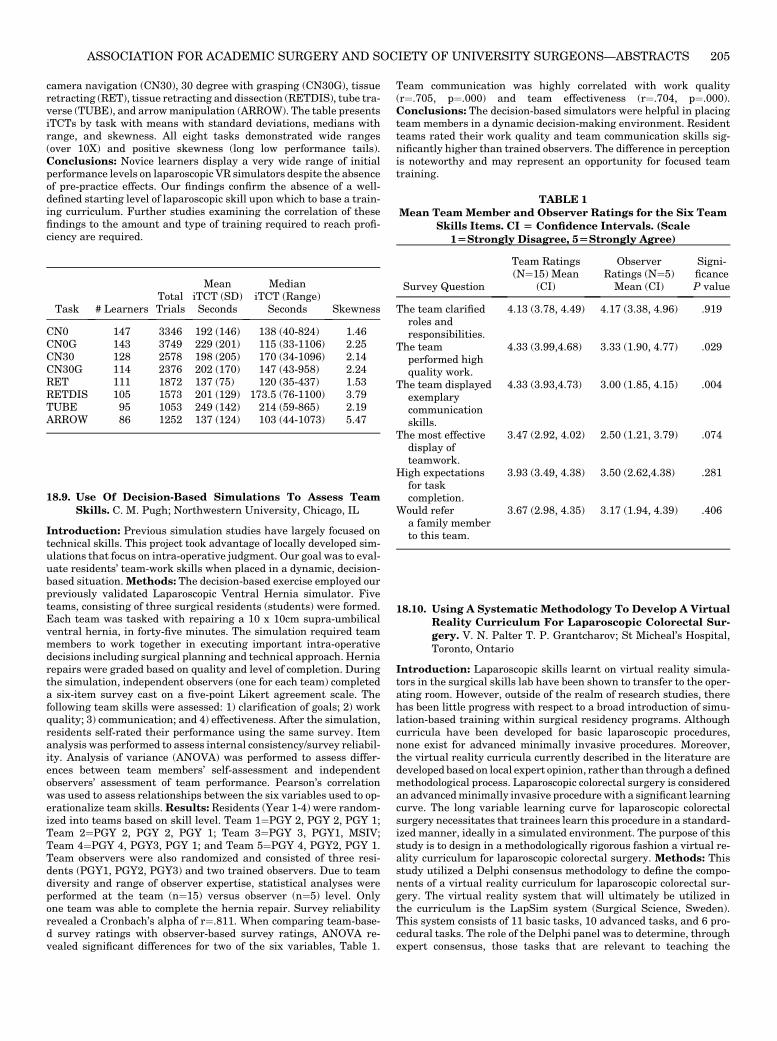
Introduction: Previous simulation studies have largely focused ontechnical skills. This project took advantage of locally developed sim-ulations that focus on intra-operative judgment. Our goal was to eval-uate residents’ team-work skills when placed in a dynamic, decision-based situation.Methods: The decision-based exercise employed ourpreviously validated Laparoscopic Ventral Hernia simulator. Fiveteams, consisting of three surgical residents (students) were formed.Each team was tasked with repairing a 10 x 10cm supra-umbilicalventral hernia, in forty-five minutes. The simulation required teammembers to work together in executing important intra-operativedecisions including surgical planning and technical approach. Herniarepairs were graded based on quality and level of completion. Duringthe simulation, independent observers (one for each team) completeda six-item survey cast on a five-point Likert agreement scale. Thefollowing team skills were assessed: 1) clarification of goals; 2) workquality; 3) communication; and 4) effectiveness. After the simulation,residents self-rated their performance using the same survey. Itemanalysis was performed to assess internal consistency/survey reliabil-ity. Analysis of variance (ANOVA) was performed to assess differ-ences between team members’ self-assessment and independentobservers’ assessment of team performance. Pearson’s correlationwas used to assess relationships between the six variables used to op-erationalize team skills.Results: Residents (Year 1-4) were random-ized into teams based on skill level. Team 1¼PGY 2, PGY 2, PGY 1;Team 2¼PGY 2, PGY 2, PGY 1; Team 3¼PGY 3, PGY1, MSIV;Team 4¼PGY 4, PGY3, PGY 1; and Team 5¼PGY 4, PGY2, PGY 1.Team observers were also randomized and consisted of three resi-dents (PGY1, PGY2, PGY3) and two trained observers. Due to teamdiversity and range of observer expertise, statistical analyses wereperformed at the team (n¼15) versus observer (n¼5) level. Onlyone team was able to complete the hernia repair. Survey reliabilityrevealed a Cronbach’s alpha of r¼.811. When comparing team-base-d survey ratings with observer-based survey ratings, ANOVA re-vealed significant differences for two of the six variables, Table 1.
Team communication was highly correlated with work quality(r¼.705, p¼.000) and team effectiveness (r¼.704, p¼.000).Conclusions: The decision-based simulators were helpful in placingteam members in a dynamic decision-making environment. Residentteams rated their work quality and team communication skills sig-nificantly higher than trained observers. The difference in perceptionis noteworthy and may represent an opportunity for focused teamtraining.
TABLE 1Mean Team Member and Observer Ratings for the Six Team
Skills Items. CI [ Confidence Intervals. (Scale1[Strongly Disagree, 5[Strongly Agree)
Team Ratings Observer Signi-
Survey Question
(N¼15) Mean(CI)
Ratings (N¼5)Mean (CI)ficanceP value
The team clarifiedroles andresponsibilities.
4.13 (3.78, 4.49)
4.17 (3.38, 4.96) .919The teamperformed highquality work.
4.33 (3.99,4.68)
3.33 (1.90, 4.77) .029The team displayedexemplarycommunicationskills.
4.33 (3.93,4.73)
3.00 (1.85, 4.15) .004The most effectivedisplay ofteamwork.
3.47 (2.92, 4.02)
2.50 (1.21, 3.79) .074High expectationsfor taskcompletion.
3.93 (3.49, 4.38)
3.50 (2.62,4.38) .281Would refera family memberto this team.
3.67 (2.98, 4.35)
3.17 (1.94, 4.39) .40618.10. Using A Systematic Methodology To Develop A VirtualReality Curriculum For Laparoscopic Colorectal Sur-gery. V. N. Palter T. P. Grantcharov; St Micheal’s Hospital,Toronto, Ontario
Introduction: Laparoscopic skills learnt on virtual reality simula-tors in the surgical skills lab have been shown to transfer to the oper-ating room. However, outside of the realm of research studies, therehas been little progress with respect to a broad introduction of simu-lation-based training within surgical residency programs. Althoughcurricula have been developed for basic laparoscopic procedures,none exist for advanced minimally invasive procedures. Moreover,the virtual reality curricula currently described in the literature aredeveloped based on local expert opinion, rather than througha definedmethodological process. Laparoscopic colorectal surgery is consideredan advancedminimally invasive procedurewith a significant learningcurve. The long variable learning curve for laparoscopic colorectalsurgery necessitates that trainees learn this procedure in a standard-ized manner, ideally in a simulated environment. The purpose of thisstudy is to design in a methodologically rigorous fashion a virtual re-ality curriculum for laparoscopic colorectal surgery. Methods: Thisstudy utilized a Delphi consensus methodology to define the compo-nents of a virtual reality curriculum for laparoscopic colorectal sur-gery. The virtual reality system that will ultimately be utilized inthe curriculum is the LapSim system (Surgical Science, Sweden).This system consists of 11 basic tasks, 10 advanced tasks, and 6 pro-cedural tasks. The role of the Delphi panel was to determine, throughexpert consensus, those tasks that are relevant to teaching the

ASSOCIATION FOR ACADEMIC SURGERY AND SOCIETY OF UNIVERSITY SURGEONS—ABSTRACTS206
technical skills required to perform laparoscopic colorectal surgery.These tasks were compiled into an on-line survey. 20 internationalexperts in surgical simulation and colorectal surgery were recruitedto participate in the survey. The participants rated each identi-fied LapSim task on a Likert scale from 1 to 5 detailing the degreeto which they agreed or disagreed that a particular component shouldbe included in a final technical skills curriculum. Results of the surveywere sent back to participants with group averages and standarddeviations until expert consensus was reached. Expert consensuswas pre-defined as Cronbach’s Alpha>0.8. After consensus wasreached, specific curricular tasks that over 80% of the experts ratedas either ‘‘agree’’ or ‘‘strongly agree’’ on the final scale were includedin the final curriculum. Results: In the first round of the survey,Cronbach’s a was 0.715 and after the second round, consensus wasreached at 0.865. Consensus was reached for 7 of the basic tasksand for 1 advanced suturing task. Conclusions: The Delphi methodallowed for expert consensus to be reached on the essential compo-nents of a virtual reality curriculum for laparoscopic colorectalsurgery. The systematic way in which this curriculum was develo-ped represents a departure from traditional methods of curriculumdesign.
EMERGING TECHNOLOGY 1: EMERGINGTECHNOLOGIES
19.1. IntravenousMultipotent Adult Progenitor Cell TherapyFor Traumatic Brain Injury: Modulation Of The Resi-dent Neuronal Macrophage Population. P. A. Walker,1 F.Jimenez,1 S. K. Shah,1 H. Xue,1 J. A. Hamilton,2 R. W. Mays,2
R. Deans,2 S. Pati,1 C. S. Cox1; 1University of Texas-HoustonDepartment of Pediatric Surgery, Houston, TX; 2AthersysInc., Cleveland, OH
Introduction: Multipotent adult progenitor cells (MAPC) are bonemarrow derived progenitor cells that offer neuroprotection after TBIin a rodent model. Previous work from our laboratory has demon-strated that the observed neuroprotection is dependent on MAPC in-teraction with resident splenocytes. Furthermore, the response of theresident microglia/macrophage to CNS injury is of interest as it ap-pears to play a role in acute and chronic phases following injury. Wehypothesize that MAPCs interact with resident splenocytes toincrease the differentiation of naive T cells into T regulatory cellsleading to systemic increases in anti inflammatory cytokine produc-tion and that the modulation of the systemic inflammatory responseaffects the resident microglial and macrophage populations leadingto functional benefit. Methods: C57 Black 6 mice underwentcontrolled cortical impact (CCI) injury or sham injury (1 group).One group of injured animals had 10 * 106 MAPC / kg injected viathe tail vein at 2 and 24 hours after CCI injury. Blood brain barrierpermeability was measured via Evan’s blue extravasation 72 hoursafter CCI injury (n¼6/group). The CD4+/CD25+/FOXP3+ T regula-tory cells populations were quantified in the spleen and blood at 24,48, and 72 hours after injury (n ¼4/group). Additionally, the CD86+M1 and CD206+ M2 macrophage populations were quantified usingflow cytometry at 24, 48, 72, and 120 hours after CCI injury (n¼6/group). Results: Mice showed an increase in BBB permeability afterCCI injury that was reversed by the intravenous injection of MAPCs(p¼0.009). A significant increase in T regulatory cells within the sple-nocyte populations of MAPC treated mice at 24 hours (p¼0.003) withno difference seen at 48 or 72 hours. Additionally, a significant in-crease in blood T regulatory cells from MAPC treated mice was seenat 48 hours after CCI injury (p¼0.006). Additionally, a significantincrease in the M2/M1 macrophage ratio in MAPC treated animalsat both 48 (p¼0.006) and 120 hours (p¼0.002) after CCI injury.Conclusions: The intravenous injection of MAPC preserves the in-tegrity of the blood brain barrier after TBI. Furthermore,MAPC ther-apy increases the differentiation of T regulatory cells which are
known to produce anti inflammatory cytokines. The modulation ofthe systemic inflammatory response could shift the microglia M2/M1 ratio accounting for the observed benefit of progenitor cell therapyfor TBI.
19.2. Delivery Of Mesenchymal Stem Cells In A BiomimeticHydrogel Enhances Wound Healing. K. C. Rustad, V. W.Wong, M. Sorkin, M. R. Major, J. P. Glotzbach, J. Rajadas,M. T. Longaker, G. C. Gurtner; Stanford University,Stanford, CA
Introduction: Mesenchymal stem cells (MSCs) have demonstratedtherapeutic potential in repairing wounds in models of pathologicalhealing. Previous studies have delivered MSCs into wounds via sub-cutaneous injection, but cell engraftment has been suboptimal. Wehypothesized that post-implantation cell survival and wound healingwould be enhanced through the delivery of MSCs within a structureddermal-like microenvironment. Thus we utilized a synthetic hydrogelscaffold previously developed by our laboratory that mimics thedermal patterning of fetal skin and can be used as a biodegradablebandage and cell delivery vehicle to sites of cutaneous injury.Methods: Collagen-pullulan hydrogels were fabricated using a salt-induced phase inversion technique via crosslinking of a collagen-pullulan mixture with STMP and subsequent induction of porosityby in-gel crystallization with KCl. Bone marrow-derived MSCs wereharvested from luciferase+/GFP+ mice and seeded onto hydrogels.MSC viability was assessed in vitro via a live/dead assay. EitherMSC-seeded or non-seeded hydrogel scaffolds were placed withinwild-type murine excisional wounds, and wound closure was com-pared to wounds treated with subcutaneously injected MSCs. Biolu-minescence imaging was performed to compare viability of MSCsseeded within hydrogels versus MSCs injected subcutaneously.Woundhistology and immunofluorescent localization ofMSCswas ex-amined. Statistical significance was determined by student’s un-paired t test. Results: MSCs demonstrated>90% viability withinthe hydrogel for up to two weeks in vitro. Wound healing at earlytime points was enhanced with non-seeded hydrogel treatment alonecompared to untreated wounds. Bioluminescence imaging indicatedprolonged viability of MSCs delivered within hydrogels compared toinjection. Wounds treated with MSC-seeded hydrogels demonstratedaccelerated healing compared to non-treated wounds at day 5 (49.3 vs30.8% wound closure, p<0.001), day 7 (78.5 vs 64.0%, p<0.01), day 9(93.6 vs 82.0%, p<0.01) and day 11 (100.0 vs 93.0%, p<0.05). MSCsthat were seeded in dermal-like hydrogels versus subcutaneously in-jected into thewound demonstrated enhanced engraftment in the der-mis of healed wounds at days 7,14 and 28. Conclusions: Biomimeticcollagen-pullulan hydrogels viably sustain MSCs in vitro and aug-ment early wound healing. Hydrogel delivery of MSCs improves cellsurvival and engraftment following implantation compared to localinjection. MSC-seeded hydrogels accelerate normal wound healingand are a promising cell-scaffold construct for skin regeneration.
19.3. Enhancement Of Bone Regeneration Using An EnrichedSkeletal Progenitor Cell Population From Human Adi-pose Derived Stromal Cells. B. Levi,1 J. P. Glotzbach,1
E. R. Nelson,1 A. W. James,1 M. Januszyk,1 S. Li,1 G. C.Gurtner,1 M. Lee,2 N. Quarto,1 M. T. Longaker1; 1StanfordUniversity, Stanford, CA; 2Universtiy of California LosAngeles, Los Angeles, CA
Introduction: Human adipose-derived stromal cells (hASCs) repre-sent a multipotent stromal cell type with proven capacity to differen-tiate along an osteogenic lineage.Multiple studies have demonstratedthat hASCs are able to undergo osteogenic differentiation in vitro andin vivo, however, little is known about the heterogeneity that existswithin the hASC population. We sought to enrich for a subpopulationof hASCs with superior osteogenic potential, based on a cell surfacemarker noted to decrease heterogeneity with a novel microfluidictechnique. We demonstrate that CD105low hASCs possessed










![LAPAROSCOPIC SURGERY FOR COLONIC CANCERincluding surgery for colorectal malignancies, has been demonstrated [1-7]. Currently, indications for laparoscopic surgery are continuing to](https://img.dokumen.tips/doc/110x75/5f088a2f7e708231d4228374/laparoscopic-surgery-for-colonic-cancer-including-surgery-for-colorectal-malignancies.jpg)


















