Embed Size (px)
Citation preview

aDivisiMedical CWashingtoWashingtoand dDivisEpidemioloCalifornia.received an
See pa*CorreE-mail
0002-9149http://dx.do
Usefulness of an Echocardiographic Composite CardiacCalcium Score to Predict Death in Patients With Stable
Coronary Artery Disease (from the Heart and Soul Study)
Sandeep A. Saha, MDa,*, Alexis L. Beatty, MDb, Rakesh K. Mishra, MDc,d, Mary A. Whooley, MDc,d,e,and Nelson B. Schiller, MDc,d
Mitral annular calcium and aortic valve sclerosis on transthoracic echocardiography (TTE)
on of Center, Cn and Vn; cVeteion of Cgy andManusd accege 57 fospondinaddres
/15/$ -i.org/1
are independently associated with cardiovascular (CV) events in patients with coronaryartery disease (CAD). However, the prognostic value of calcific deposits at multiple sites isunknown. We performed TTEs in a prospective cohort of 595 outpatients with stable CADand graded the severity of calcific deposition at 6 sites: mitral annulus, aortic valve, aorticring, sinotubular junction, papillary muscle tip, and left main coronary artery. For each sitewith moderate calcific deposition or greater, 1 point was given to generate a compositecardiac calcium score (maximum of 6). The primary end point was the occurrence of CVevents—a composite of death, myocardial infarction, stroke, transient ischemic attack, andheart failure. The association of the composite calcium score with CV events was evaluatedusing multivariate Cox proportional hazards models. Over a median follow-up of 4.2 years,205 CV events occurred. Participants with a composite calcium score ‡2 had a higher risk ofCV events (11.1 events/100 person-years) than those with a score of 0 (5.5 events/100 person-years, unadjusted hazard ratio [HR] 2.01, p <0.001), but this association was not significantafter multivariate adjustment. The risk of death was higher in participants with a compositecalcium score of ‡2 (8.9 events/100 person-years) versus those with a score of 0 (3.6 events/100 person-years, unadjusted HR 2.51, p <0.001). After adjustment for age, diabetes mellitus,previous coronary revascularization, diastolic blood pressure, estimated glomerular filtrationrate, and serum phosphorus level, the risk of death remained higher in participants with acomposite calcium score of ‡2 compared with those with a score of 0 (adjusted HR 1.76, 95%confidence interval 1.10 to 2.81, p [ 0.02). In conclusion, a simple TTE-derived compositecardiac calcium score was independently predictive of death in patients with pre-existingCAD. � 2015 Elsevier Inc. All rights reserved. (Am J Cardiol 2015;116:50e58)
The presence of calcium deposits in the cardiovascular(CV) system has been associated with the presence ofatherosclerotic disease in autopsy studies1 and population-based cohort studies.2e4 Two-dimensional (2D) trans-thoracic echocardiography (TTE) is able to detect calcificdeposits at several discrete sites within the heart, epicardialcoronary arteries, and great vessels. Other imaging tech-niques such as transesophageal echocardiography (TEE) andcardiac computed tomography (CT) to study cardiac calci-fication are limited because of the invasive nature andanesthetic and procedural risks in the case of TEEs andexposure to ionizing radiation and high cost in the case ofCT.5,6 Mitral annular calcification (MAC) is associated with
ardiology, Department of Medicine, Rush Universityhicago, Illinois; bDivision of Cardiology, University ofeterans Affairs Puget Sound Health Care System, Seattle,rans’ Affairs Medical Center, San Francisco, California;ardiology, Department of Medicine and eDepartment ofBiostatistics, University of California, San Francisco,cript received February 24, 2015; revised manuscriptpted March 19, 2015.r disclosure information.g author: Tel: (312) 942-8771; fax: (312) 942-5829.s: [email protected] (S.A. Saha).
see front matter � 2015 Elsevier Inc. All rights reserved.0.1016/j.amjcard.2015.03.041
CV events, cardiac mortality, and all-cause mortalityindependent of traditional CV risk factors.7e12 Similarly,aortic valve sclerosis is associated with the presence ofcoronary artery disease (CAD) and elevated risk of CVmorbidity and mortality.3,4,13e15 TTE studies enable detec-tion of calcific deposits at other sites, including the aorticroot, sinotubular junction, tips of the papillary muscles, andthe proximal coronary arteries.16 In the present study, wedeveloped a composite cardiac calcium score that grades thepresence and severity of calcific deposition at 6 discrete sitesas seen on conventional 2D TTE. The 6 sites chosen todevelop this composite cardiac calcium score are mitralvalve annulus, aortic valve annulus, aortic ring/root (definedas the portion between the aortic valve annulus and thesinuses of Valsalva), sinotubular junction, papillary muscletip, and left main coronary artery. We then estimated theprognostic value of this composite cardiac calcium score forthe prediction of CV events in patients with establishedCAD enrolled in the Heart and Soul Study.
Methods
The Heart and Soul Study is a prospective cohort studyof outpatients with stable CAD.
The enrollment process for the Heart and Soul Studyhas been previously described.17 We used administrative
www.ajconline.org

Table
1Descriptio
nof
thecompo
site
cardiaccalcium
score
Site
(Views)
Severity
ofcalcificdepositio
n
Mild
Moderate
Severe
Mitral
annulus(PSAX)
Calcificdepositslim
itedto
postero-medial
term
inus
ofposteriormitral
annulus
Non
-contig
uous
calcificdepositson
thepostero-medialand
antero-lateral
term
iniof
theposteriormitral
annulus
Con
tiguous
calcificdepositsextendingfrom
the
lateralto
medialterm
iniof
theposteriormitral
annulus
Aortic
valve(PLAX,PSAX)
Focal
calcificdepositson
oneor
more
leafletswith
outleaflet
restriction
Non
-contig
uous
calcificdepo
sitson
oneor
more
leafletswith
norestrictionor
mild
restriction
Con
tiguous
calcificdepositson
oneor
more
leafletswith
anydegree
ofleaflet
restriction
Aortic
Root(PSAX)
Calcificdepositslim
itedto
anterior
orpo
steriorbo
rder
oftheaortic
ring
Non
-con
tiguous
calcificdepo
sitson
both
anterior
andposteriorbordersof
theaortic
ring
Con
tiguous
calcificdepositsof
theentire
aortic
ring
(circumferentialinvolvem
ent)
Sino-tubu
larjunctio
n(PLAX)
Focal
calcificdepo
sitson
oneor
both
sino
-tub
ular
junctio
nsCalcificdepositson
both
sino
-tub
ular
junctio
nswith
nointrusioninto
theaortic
lumen
Calcificdepo
sitson
both
sino
-tub
ular
junctio
nswith
nointrusioninto
theaortic
lumen
Papillarymuscletip
(PSAX,A2C
,A4C
)Calcificdepo
sitson
one(usually
postero-medial)papillary
muscletip
Calcificdepositson
both
papillary
muscletip
sbutnotextendinginto
thechordalapparatus
Calcificdepositson
both
papillary
muscle
tipswith
extensioninto
thechordalapparatus
Leftmaincoronary
artery
(PSAX,PLAX)
Focal
calcificdepo
sitson
oneor
both
wallsof
theleftmaincoronary
artery
Linear,no
n-contiguo
usinvo
lvem
ent
of<1cm
ofon
eor
both
walls
Linear,contiguo
usinvo
lvem
ent
of>1cm
ofbo
thwalls
PLAX
¼parasternallong
-axisview
;PSAX
¼parasternalshortaxisview
;A2C
¼apical
2-cham
berview
;A4C
¼apical
4-cham
berview
.
Coronary Artery Disease/Composite Cardiac Calcium Score by Echocardiography in CAD 51
databases to identify outpatients with documented CAD at 2departments of the Veterans Affairs (San Francisco and PaloAlto, California), the University of California, San Fran-cisco, and 9 public health clinics from the CommunityHealth Network of San Francisco.
Participants were eligible to participate if they met 1 ofthe following1: history of myocardial infarction,2 angio-graphic evidence of �50% stenosis by area in �1 coronaryvessel,3 evidence of exercise-induced ischemia by treadmillelectrocardiogram or stress nuclear perfusion imaging,4
history of coronary revascularization,5 or a previous diag-nosis of CAD by an internist or a cardiologist. Subjects wereexcluded if they had a myocardial infarction within theprevious 6 months, deemed themselves unable to walk 1block, or were planning to move out of the local area within3 years. From September 2000 to December 2002, 1,024study participants provided informed consent and completedbaseline echocardiographic and laboratory testing. Thisincluded 549 subjects (54%) with a history of myocardialinfarction, 237 (23%) with a history of revascularization butnot myocardial infarction, and 238 (23%) with a diagnosisof CAD that was documented by their physician (based on apositive angiogram or treadmill test in 98% of cases). Theinstitutional review board at each enrolling center approvedthe study protocol, and all participants provided writteninformed consent.
Of the 1,024 participants who completed the baselineexamination, a total of 595 participants underwent a repeatechocardiographic examination 5 years after enrollment,comprising the analytical cohort for this study. At the 5-yearfollow-up visit, the 595 participants completed an exami-nation that included an interview, fasting blood draw,questionnaire, and TTE. A complete 2D TTE at rest wasobtained in all patients using an Acuson Sequoia UltrasoundSystem and a 3.5-MHz transducer (Siemens Medical Solu-tions, Mountain View, California). All standard views wereobtained during quiet respiration. Two highly experiencedsonographers made all sonographic measurements, and asingle, blinded cardiologist reader (NBS) evaluated,confirmed, and, when needed, corrected each measurement.In addition, the presence and severity of calcific depositionwas measured at a total of 6 sites in the heart, using apredefined scoring system described in Table 1 and illus-trated in Figure 1. For each site with moderate or severecalcific deposition as defined earlier, the participant received1 point, allowing for a composite calcium score rangingfrom 0 to 6. The composite calcium score was computed bya single cardiologist reader (NBS), who was blinded to theparticipants’ baseline clinical and laboratory informationand did not participate in the adjudication of clinical out-comes. Age, gender, race, and medical history were deter-mined by self-report. Study personnel measured height,weight, and blood pressure. Fasting blood samples wereobtained to measure serum calcium, phosphorus, creatinine,cystatin C, C-reactive protein, total cholesterol, HDLcholesterol, LDL cholesterol, and triglyceride levels. Esti-mated glomerular filtration rate was calculated using theChronic Kidney Disease Epidemiology Collaboration(CKD-EPI) creatinine-cystatin C equation.18
Annual telephone interviews were conducted with studyparticipants (or their proxy) to inquire about interval
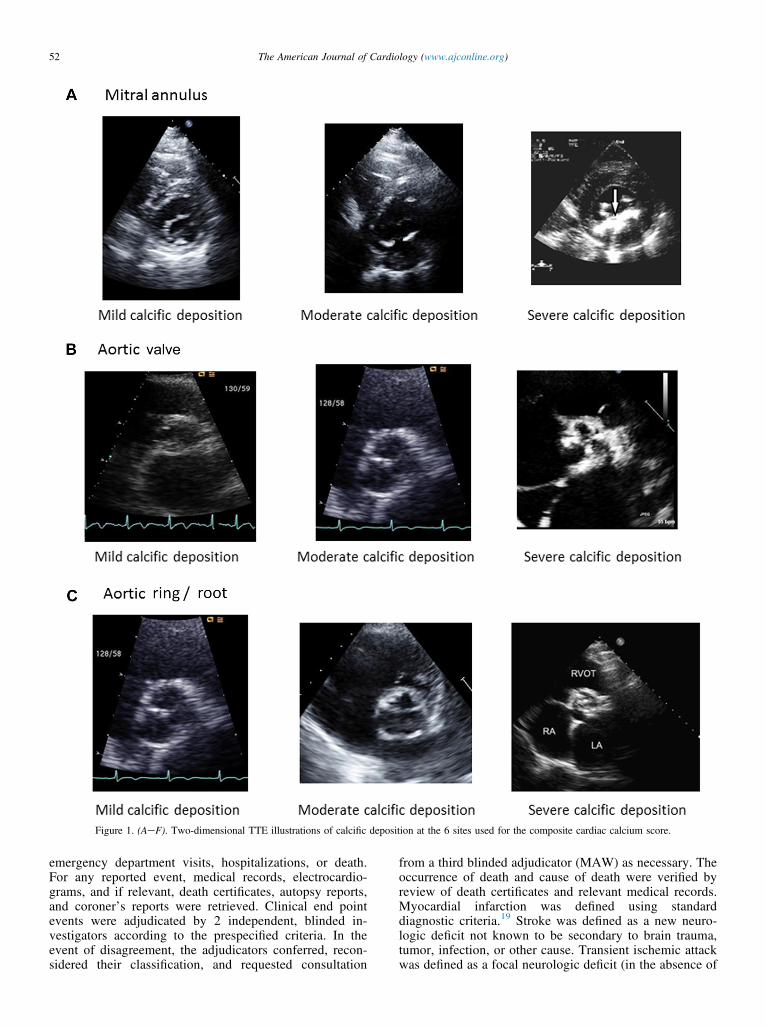
Figure 1. (AeF). Two-dimensional TTE illustrations of calcific deposition at the 6 sites used for the composite cardiac calcium score.
52 The American Journal of Cardiology (www.ajconline.org)
emergency department visits, hospitalizations, or death.For any reported event, medical records, electrocardio-grams, and if relevant, death certificates, autopsy reports,and coroner’s reports were retrieved. Clinical end pointevents were adjudicated by 2 independent, blinded in-vestigators according to the prespecified criteria. In theevent of disagreement, the adjudicators conferred, recon-sidered their classification, and requested consultation
from a third blinded adjudicator (MAW) as necessary. Theoccurrence of death and cause of death were verified byreview of death certificates and relevant medical records.Myocardial infarction was defined using standarddiagnostic criteria.19 Stroke was defined as a new neuro-logic deficit not known to be secondary to brain trauma,tumor, infection, or other cause. Transient ischemic attackwas defined as a focal neurologic deficit (in the absence of
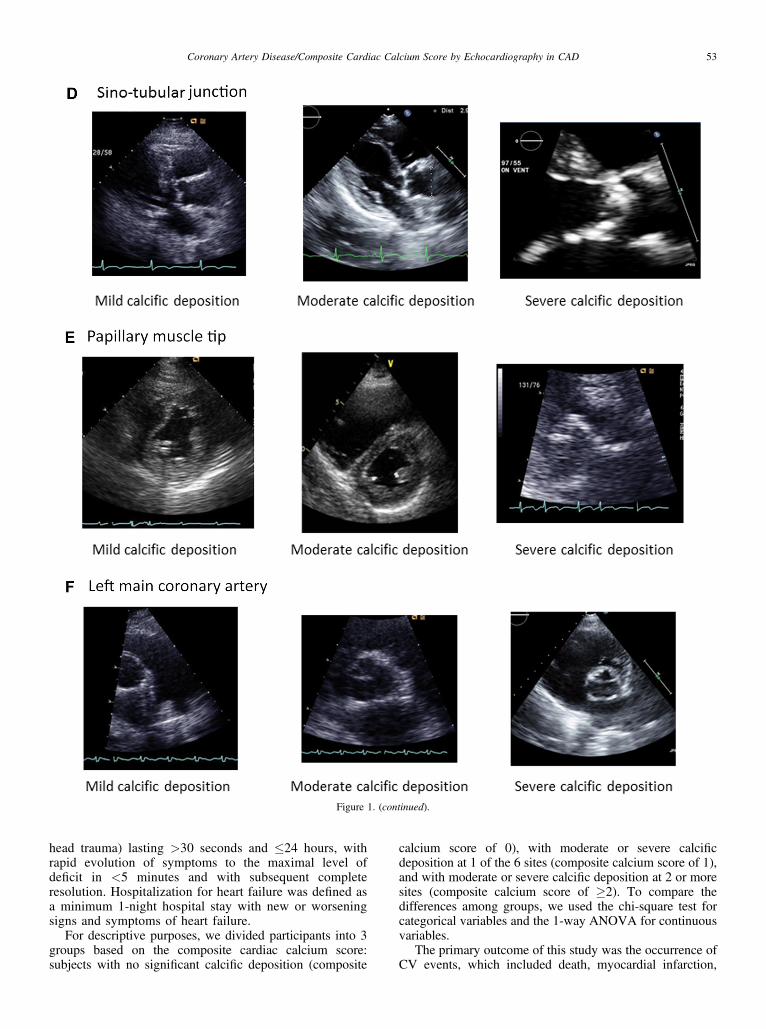
Figure 1. (continued).
Coronary Artery Disease/Composite Cardiac Calcium Score by Echocardiography in CAD 53
head trauma) lasting >30 seconds and �24 hours, withrapid evolution of symptoms to the maximal level ofdeficit in <5 minutes and with subsequent completeresolution. Hospitalization for heart failure was defined asa minimum 1-night hospital stay with new or worseningsigns and symptoms of heart failure.
For descriptive purposes, we divided participants into 3groups based on the composite cardiac calcium score:subjects with no significant calcific deposition (composite
calcium score of 0), with moderate or severe calcificdeposition at 1 of the 6 sites (composite calcium score of 1),and with moderate or severe calcific deposition at 2 or moresites (composite calcium score of �2). To compare thedifferences among groups, we used the chi-square test forcategorical variables and the 1-way ANOVA for continuousvariables.
The primary outcome of this study was the occurrence ofCV events, which included death, myocardial infarction,
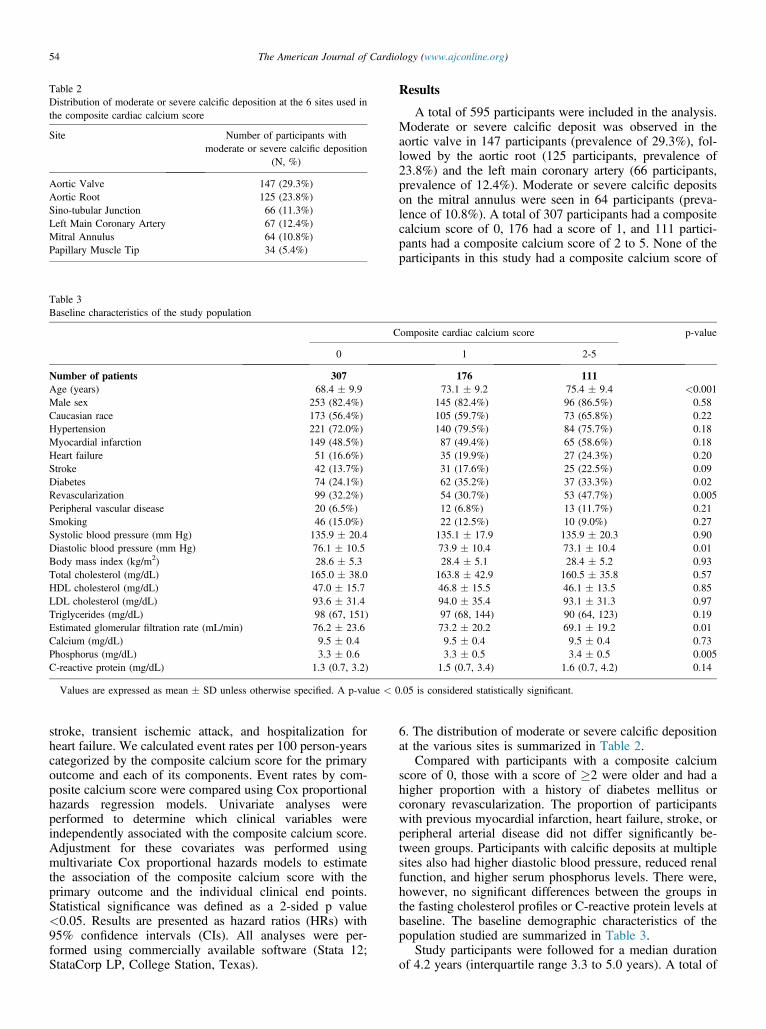
Table 2Distribution of moderate or severe calcific deposition at the 6 sites used inthe composite cardiac calcium score
Site Number of participants withmoderate or severe calcific deposition
(N, %)
Aortic Valve 147 (29.3%)Aortic Root 125 (23.8%)Sino-tubular Junction 66 (11.3%)Left Main Coronary Artery 67 (12.4%)Mitral Annulus 64 (10.8%)Papillary Muscle Tip 34 (5.4%)
Table 3Baseline characteristics of the study population
Composite cardiac calcium score p-value
0 1 2-5
Number of patients 307 176 111Age (years) 68.4 � 9.9 73.1 � 9.2 75.4 � 9.4 <0.001Male sex 253 (82.4%) 145 (82.4%) 96 (86.5%) 0.58Caucasian race 173 (56.4%) 105 (59.7%) 73 (65.8%) 0.22Hypertension 221 (72.0%) 140 (79.5%) 84 (75.7%) 0.18Myocardial infarction 149 (48.5%) 87 (49.4%) 65 (58.6%) 0.18Heart failure 51 (16.6%) 35 (19.9%) 27 (24.3%) 0.20Stroke 42 (13.7%) 31 (17.6%) 25 (22.5%) 0.09Diabetes 74 (24.1%) 62 (35.2%) 37 (33.3%) 0.02Revascularization 99 (32.2%) 54 (30.7%) 53 (47.7%) 0.005Peripheral vascular disease 20 (6.5%) 12 (6.8%) 13 (11.7%) 0.21Smoking 46 (15.0%) 22 (12.5%) 10 (9.0%) 0.27Systolic blood pressure (mm Hg) 135.9 � 20.4 135.1 � 17.9 135.9 � 20.3 0.90Diastolic blood pressure (mm Hg) 76.1 � 10.5 73.9 � 10.4 73.1 � 10.4 0.01Body mass index (kg/m2) 28.6 � 5.3 28.4 � 5.1 28.4 � 5.2 0.93Total cholesterol (mg/dL) 165.0 � 38.0 163.8 � 42.9 160.5 � 35.8 0.57HDL cholesterol (mg/dL) 47.0 � 15.7 46.8 � 15.5 46.1 � 13.5 0.85LDL cholesterol (mg/dL) 93.6 � 31.4 94.0 � 35.4 93.1 � 31.3 0.97Triglycerides (mg/dL) 98 (67, 151) 97 (68, 144) 90 (64, 123) 0.19Estimated glomerular filtration rate (mL/min) 76.2 � 23.6 73.2 � 20.2 69.1 � 19.2 0.01Calcium (mg/dL) 9.5 � 0.4 9.5 � 0.4 9.5 � 0.4 0.73Phosphorus (mg/dL) 3.3 � 0.6 3.3 � 0.5 3.4 � 0.5 0.005C-reactive protein (mg/dL) 1.3 (0.7, 3.2) 1.5 (0.7, 3.4) 1.6 (0.7, 4.2) 0.14
Values are expressed as mean � SD unless otherwise specified. A p-value < 0.05 is considered statistically significant.
54 The American Journal of Cardiology (www.ajconline.org)
stroke, transient ischemic attack, and hospitalization forheart failure. We calculated event rates per 100 person-yearscategorized by the composite calcium score for the primaryoutcome and each of its components. Event rates by com-posite calcium score were compared using Cox proportionalhazards regression models. Univariate analyses wereperformed to determine which clinical variables wereindependently associated with the composite calcium score.Adjustment for these covariates was performed usingmultivariate Cox proportional hazards models to estimatethe association of the composite calcium score with theprimary outcome and the individual clinical end points.Statistical significance was defined as a 2-sided p value<0.05. Results are presented as hazard ratios (HRs) with95% confidence intervals (CIs). All analyses were per-formed using commercially available software (Stata 12;StataCorp LP, College Station, Texas).
Results
A total of 595 participants were included in the analysis.Moderate or severe calcific deposit was observed in theaortic valve in 147 participants (prevalence of 29.3%), fol-lowed by the aortic root (125 participants, prevalence of23.8%) and the left main coronary artery (66 participants,prevalence of 12.4%). Moderate or severe calcific depositson the mitral annulus were seen in 64 participants (preva-lence of 10.8%). A total of 307 participants had a compositecalcium score of 0, 176 had a score of 1, and 111 partici-pants had a composite calcium score of 2 to 5. None of theparticipants in this study had a composite calcium score of
6. The distribution of moderate or severe calcific depositionat the various sites is summarized in Table 2.
Compared with participants with a composite calciumscore of 0, those with a score of �2 were older and had ahigher proportion with a history of diabetes mellitus orcoronary revascularization. The proportion of participantswith previous myocardial infarction, heart failure, stroke, orperipheral arterial disease did not differ significantly be-tween groups. Participants with calcific deposits at multiplesites also had higher diastolic blood pressure, reduced renalfunction, and higher serum phosphorus levels. There were,however, no significant differences between the groups inthe fasting cholesterol profiles or C-reactive protein levels atbaseline. The baseline demographic characteristics of thepopulation studied are summarized in Table 3.
Study participants were followed for a median durationof 4.2 years (interquartile range 3.3 to 5.0 years). A total of

Figure 2. Unadjusted annual event rates of the primary outcome stratified bycomposite cardiac calcium score. Results are expressed as events per100 person-years (error bars represent 95% confidence limits) (*p <0.05;**p <0.001).
Figure 3. Unadjusted annual event rates of individual CV end pointsstratified by the composite cardiac calcium score. Results are expressed asevents per 100 person-years (error bars represent 95% confidence limits)(*p <0.05; **p <0.001).
Coronary Artery Disease/Composite Cardiac Calcium Score by Echocardiography in CAD 55
205 CV events were recorded, which included 152 deaths,28 myocardial infarctions, 22 strokes or transient ischemicattacks, and 40 hospitalizations for heart failure. Participantswith a composite calcium score of 0 had a significantlylower incidence of CV events than participants with acomposite calcium score of �2 (5.5 vs 11.1 events per 100person-years, p <0.001, Figure 2). Participants with acomposite score of 0 also had significantly lower rates ofdeath (3.6 vs 8.9 deaths per 100 person-years, p <0.001)and myocardial infarction (0.6 vs 2.1 events per 100 person-years, p ¼ 0.01) compared with participants with a com-posite score of �2. The incidence of stroke or transientischemic attack and hospitalization for heart failure did notdiffer significantly between the groups (Figure 3).
Univariate analyses indicated that the following variableswere significantly associated with the composite cardiaccalcium score: age, history of diabetes mellitus, previous
coronary revascularization, diastolic blood pressure, esti-mated glomerular filtration rate, and serum phosphoruslevel. In unadjusted analyses, the risk of CV events wastwofold higher in participants with a composite calciumscore of �2 compared with those with a composite score of0 (HR 2.01, 95% CI 1.38 to 2.92, p <0.001). Adjustment forage attenuated but did not completely abrogate this associ-ation, but after additional adjustment for diabetes mellitus,previous coronary revascularization, diastolic blood pres-sure, estimated GFR, and serum phosphorus level, the riskof CV events in participants with a composite score of �2did not significantly differ from those with a compositescore of 0 (HR 1.38, 95% CI 0.92 to 2.08, p ¼ 0.12)(Table 4, Figure 4). Participants with a composite calciumscore of �2 had a 2.5-fold increased risk of death comparedwith those with a composite calcium score of 0 (HR 2.51,95% CI 1.63 to 3.85, p <0.001) in unadjusted analyses. Inmodels adjusted for age, diabetes mellitus, previous coro-nary revascularization, diastolic blood pressure, estimatedGFR, and serum phosphorus level, the risk of death was45% higher in participants with a composite calcium scoreof 1 (HR 1.45, 95% CI 0.94 to 2.23, p ¼ 0.09), and 76%higher in participants with a composite calcium score of �2(HR 1.76, 95% CI 1.10 to 2.81, p ¼ 0.02) (Figure 4). Theresults of the multivariate analyses for the primary com-posite outcome and death are listed in Table 4.
Discussion
To our knowledge, this is the first report that describes acomprehensive, semiquantitative, composite cardiac cal-cium score that includes multiple relevant sites of calciumdeposition as seen on a conventional 2D TTE study andshows that moderate-to-severe calcific deposition at �2discrete sites (corresponding to a composite cardiac calciumscore of �2) is independently associated with mortality inpatients with CAD. Indeed, it is well known that cardiaccalcification occurs in a nonuniform manner with normalaging, and some studies suggest that mild valvular calcifi-cation routinely seen on 2D TTE studies in elderly patientsmay not be independently predictive of adverse CVevents.10 Our scoring system recognizes this phenomenonand, therefore, focuses on the presence of moderate or se-vere calcific deposition (rather than the presence or absenceof calcification) at each of the 6 sites and assigns a binaryvalue (0 or 1) for each site to make the composite calciumscoring system easy to use during routine interpretation ofTTE studies. The use of standard 2D echocardiographicviews, combined with the ease of use of the scoring system,should enable echocardiographers to compute the compositecardiac calcium score as part of their routine TTE inter-pretation and should, therefore, be associated with little orno additional cost to the patient.
Our results agree with previous studies that have exam-ined the association of MAC, aortic valve sclerosis, aorticannular calcification, and various combinations thereof, withall-cause and CV mortality. An analysis of the Cardiovas-cular Health Study reported that the combined presence ofMAC, aortic valve sclerosis, and aortic annular calcificationwas independently predictive of both all-cause mortality andCV mortality in an observational cohort of 3,782 elderly
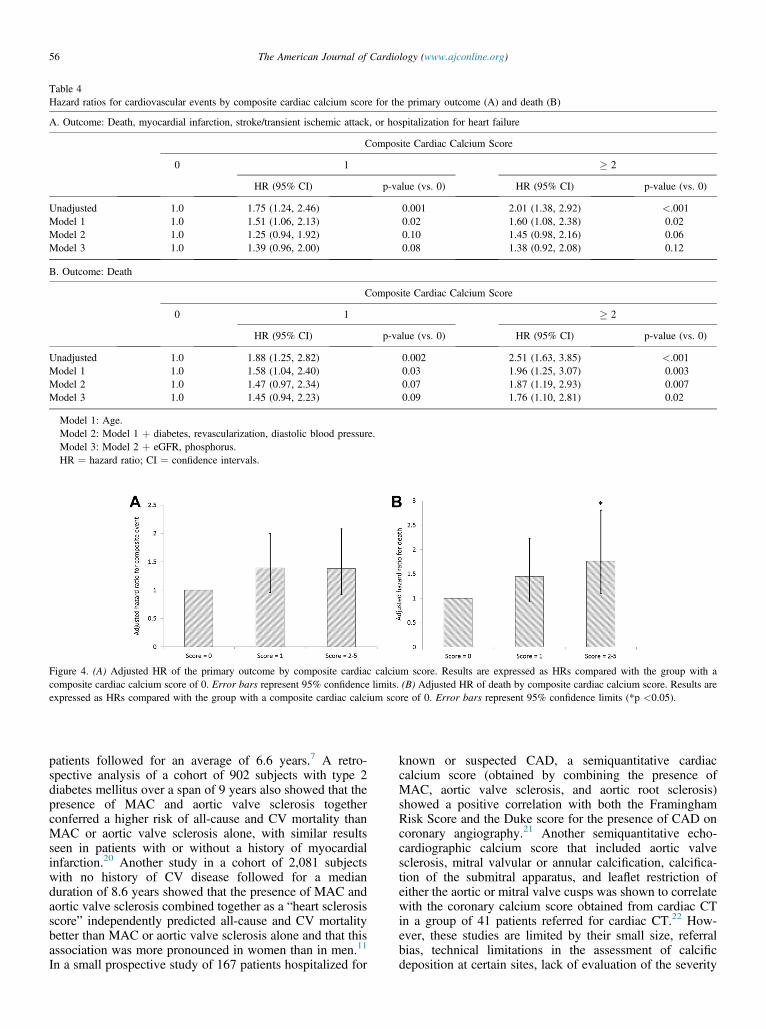
Table 4Hazard ratios for cardiovascular events by composite cardiac calcium score for the primary outcome (A) and death (B)
A. Outcome: Death, myocardial infarction, stroke/transient ischemic attack, or hospitalization for heart failure
Composite Cardiac Calcium Score
0 1 � 2
HR (95% CI) p-value (vs. 0) HR (95% CI) p-value (vs. 0)
Unadjusted 1.0 1.75 (1.24, 2.46) 0.001 2.01 (1.38, 2.92) <.001Model 1 1.0 1.51 (1.06, 2.13) 0.02 1.60 (1.08, 2.38) 0.02Model 2 1.0 1.25 (0.94, 1.92) 0.10 1.45 (0.98, 2.16) 0.06Model 3 1.0 1.39 (0.96, 2.00) 0.08 1.38 (0.92, 2.08) 0.12
B. Outcome: Death
Composite Cardiac Calcium Score
0 1 � 2
HR (95% CI) p-value (vs. 0) HR (95% CI) p-value (vs. 0)
Unadjusted 1.0 1.88 (1.25, 2.82) 0.002 2.51 (1.63, 3.85) <.001Model 1 1.0 1.58 (1.04, 2.40) 0.03 1.96 (1.25, 3.07) 0.003Model 2 1.0 1.47 (0.97, 2.34) 0.07 1.87 (1.19, 2.93) 0.007Model 3 1.0 1.45 (0.94, 2.23) 0.09 1.76 (1.10, 2.81) 0.02
Model 1: Age.Model 2: Model 1 þ diabetes, revascularization, diastolic blood pressure.Model 3: Model 2 þ eGFR, phosphorus.HR ¼ hazard ratio; CI ¼ confidence intervals.
Figure 4. (A) Adjusted HR of the primary outcome by composite cardiac calcium score. Results are expressed as HRs compared with the group with acomposite cardiac calcium score of 0. Error bars represent 95% confidence limits. (B) Adjusted HR of death by composite cardiac calcium score. Results areexpressed as HRs compared with the group with a composite cardiac calcium score of 0. Error bars represent 95% confidence limits (*p <0.05).
56 The American Journal of Cardiology (www.ajconline.org)
patients followed for an average of 6.6 years.7 A retro-spective analysis of a cohort of 902 subjects with type 2diabetes mellitus over a span of 9 years also showed that thepresence of MAC and aortic valve sclerosis togetherconferred a higher risk of all-cause and CV mortality thanMAC or aortic valve sclerosis alone, with similar resultsseen in patients with or without a history of myocardialinfarction.20 Another study in a cohort of 2,081 subjectswith no history of CV disease followed for a medianduration of 8.6 years showed that the presence of MAC andaortic valve sclerosis combined together as a “heart sclerosisscore” independently predicted all-cause and CV mortalitybetter than MAC or aortic valve sclerosis alone and that thisassociation was more pronounced in women than in men.11
In a small prospective study of 167 patients hospitalized for
known or suspected CAD, a semiquantitative cardiaccalcium score (obtained by combining the presence ofMAC, aortic valve sclerosis, and aortic root sclerosis)showed a positive correlation with both the FraminghamRisk Score and the Duke score for the presence of CAD oncoronary angiography.21 Another semiquantitative echo-cardiographic calcium score that included aortic valvesclerosis, mitral valvular or annular calcification, calcifica-tion of the submitral apparatus, and leaflet restriction ofeither the aortic or mitral valve cusps was shown to correlatewith the coronary calcium score obtained from cardiac CTin a group of 41 patients referred for cardiac CT.22 How-ever, these studies are limited by their small size, referralbias, technical limitations in the assessment of calcificdeposition at certain sites, lack of evaluation of the severity

Coronary Artery Disease/Composite Cardiac Calcium Score by Echocardiography in CAD 57
of calcific deposition, lack of inclusion of other importantsites of calcific deposition, and perhaps most importantly,lack of data about the association of the composite scorewith clinical events.
Our study adds to the published literature in 3 distinctways. First, this is the first study in the literature that showsthat moderate-to-severe calcific deposition at sites other thanthe mitral annulus, aortic valve, and aortic root, such as thesinotubular junction, papillary muscle tip, and left maincoronary artery, is also associated with higher risk ofadverse CV events in elderly patients with CAD. Theprevalence of moderate or severe calcific deposits in the leftmain coronary artery (12.4%) and sinotubular junction(11.3%) was higher than that of MAC (10.8%) in this study,whereas the site with the highest prevalence of moderate orsevere calcific deposition was the aortic valve (147 partici-pants, 29.3%). Second, the composite cardiac calcium scoreis able to identify patients with pre-existing CAD at asignificantly higher risk of death, even when the traditionalmarkers of clinical risk, such as fasting lipid profiles, sys-tolic blood pressure, and C-reactive protein levels, are notsignificantly different. Finally, we have defined standardizedcriteria for determining the severity of calcific deposition at6 distinct anatomic sites within the heart and have developeda simple, easy-to-use scoring system that can be used toreport the extent of global cardiac calcific deposition as seenon conventional 2D TEE. Most patients with CAD undergoTTE studies as part of the longitudinal follow-up of their CVdisease. Whether the addition of this composite cardiaccalcium score in TTE reports of patients with CAD leads todifferences in the clinical management of these high-riskpatients remains to be studied.
Our study has important limitations that must beconsidered. First, the study population consisted predomi-nantly of older men from Northern California, and nearlyhalf of these patients were enrolled from the Veterans’ Af-fairs medical centers, and therefore, the results may not begeneralizable to women or younger patients with CAD.Second, this study was performed in subjects who attended a5-year follow-up examination as part of a prospective cohortstudy of patients with CAD. Thus, the study populationcomprised patients with CAD who survived for at least5 years with CAD with close follow-up within the Heart andSoul Study, which may not be representative of the generalpopulation of patients with newly diagnosed CAD or thosewith established CAD. Third, the number of myocardialinfarctions, strokes, and transient ischemic attacks in thisstudy was small, and the relatively low CV event rate mayhave reduced the statistical power of the study. Fourth, thecomposite cardiac calcium score for all study participantswas computed by 1 experienced echocardiographer (NBS),and although the scoring system was defined a priori indetail (Table 1, Figure 1), the reproducibility of these resultswas not specifically evaluated. Finally, the lack of a vali-dation cohort analysis of the composite cardiac calciumscore remains a limitation of the present study, but wedecided not to split the Heart and Soul population intoderivation and validation cohorts to allow for such ananalysis because of the small number of clinical events inthis population. We hope, however, that investigators willbe attracted to the simple and intuitive nature of this scoring
system to determine the global cardiac calcific burden intheir patients and will choose to apply this scoring system toother patient populations to determine the prognostic valueof the composite cardiac calcium score in their studypopulations.
Disclosures
The Heart and Soul Study supported by grants from theDepartment of Veterans Affairs, Washington, DC (Epide-miology Merit Review Program), grant R01HL079235 fromthe National Heart, Lung, and Blood Institute, Bethesda,MD,the Robert Wood Johnson Foundation, Princeton, NJ(Generalist Physician Faculty Scholars Program), theAmerican Federation for Aging Research, New York, NY(Paul Beeson Faculty Scholars in Aging Research Program),the Ischemia Research and Education Foundation, South SanFrancisco, CA, and the Nancy Kirwan Heart Research Fund,San Francisco, CA. Dr. Beatty received support from awardnumber F32 HL110518 from the National Heart, Lung, andBlood Institute and KL2TR000143 from the National Centerfor Advancing Translational Sciences, Bethesda, MD. Theauthors have no conflicts of interest to disclose.
1. Roberts WC. Morphologic features of the normal and abnormal mitralvalve. Am J Cardiol 1983;51:1005e1028.
2. Rossi A, Faggiano P, Amado AE, Cicoira M, Bonapace S, FranceschiniL, Dini FL, Ghio S, Agricola E, Temporelli PL, Vassanelli C. Mitraland aortic valve sclerosis/calcification and carotid atherosclerosis:results from 1065 patients. Heart Vessels 2014;29:776e783.
3. Agno FS, Chinali M, Bella JN, Liu JE, Arnett DK, Kitzman DW,Oberman A, Hopkins PN, Rao DC, Devereux RB. Aortic valvesclerosis is associated with preclinical cardiovascular disease inhypertensive adults: the Hypertension Genetic Epidemiology Networkstudy. J Hypertens 2005;23:867e873.
4. Agmon Y, Khandheria BK,Meissner I, Sicks JR, O’FallonWM,WiebersDO, Whisnant JP, Seward JB, Tajik AJ. Aortic valve sclerosis and aorticatherosclerosis: different manifestations of the same disease? Insightsfrom a population-based study. J Am Coll Cardiol 2001;38:827e834.
5. Tolstrup K, Roldan CA, Qualls CR, Crawford MH. Aortic valvesclerosis, mitral annular calcium, and aortic root sclerosis as markers ofatherosclerosis in men. Am J Cardiol 2002;89:1030e1034.
6. Owens DS, Budoff MJ, Katz R, Takasu J, Shavelle DM, Carr JJ,Heckbert SR, Otto CM, Probstfield JL, Kronmal RA, O’Brien KD.Aortic valve calcium independently predicts coronary and cardiovas-cular events in a primary prevention population. JACC CardiovascImaging 2012;5:619e625.
7. Barasch E, Gottdiener JS, Marino Larsen EK, Chaves PH, NewmanAB. Cardiovascular morbidity and mortality in community-dwellingelderly individuals with calcification of the fibrous skeleton of thebase of the heart and aortosclerosis (The Cardiovascular Health Study).Am J Cardiol 2006;97:1281e1286.
8. Boon A, Cheriex E, Lodder J, Kessels F. Cardiac valve calcification:characteristics of patients with calcification of the mitral annulus oraortic valve. Heart 1997;78:472e474.
9. Fox CS, Vasan RS, Parise H, Levy D, O’Donnell CJ, D’Agostino RB,Benjamin EJ; Framingham Heart Study. Mitral annular calcificationpredicts cardiovascular morbidity and mortality: the Framingham HeartStudy. Circulation 2003;107:1492e1496.
10. Kohsaka S, Jin Z, Rundek T, Boden-Albala B, Homma S, Sacco RL,Di Tullio MR. Impact of mitral annular calcification on cardiovascularevents in a multiethnic community: the Northern Manhattan Study.JACC Cardiovasc Imaging 2008;1:617e623.
11. Völzke H, Haring R, Lorbeer R, Wallaschofski H, Reffelmann T,Empen K, Rettig R, John U, Felix SB, Dörr M. Heart valve sclerosispredicts all-cause and cardiovascular mortality. Atherosclerosis2010;209:606e610.
12. Holtz JE, Upadhyaya DS, Cohen BE, Na B, Schiller NB, WhooleyMA. Mitral annular calcium, inducible myocardial ischemia, and
58 The American Journal of Cardiology (www.ajconline.org)
cardiovascular events in outpatients with coronary heart disease (fromthe Heart and Soul Study). Am J Cardiol 2012;109:1092e1096.
13. Otto CM, Lind BK, Kitzman DW, Gersh BJ, Siscovick DS.Association of aortic-valve sclerosis with cardiovascular mortality andmorbidity in the elderly. N Engl J Med 1999;341:142e147.
14. Olsen MH, Wachtell K, Bella JN, Gerdts E, Palmieri V, Nieminen MS,Smith G, Ibsen H, Devereux RB; LIFE substudy. Aortic valve sclerosisrelates to cardiovascular events in patients with hypertension (a LIFEsubstudy). Am J Cardiol 2005;95:132e136.
15. Shah SJ, Ristow B, Ali S, Na BY, Schiller NB, Whooley MA. Acutemyocardial infarction in patients with versus without aortic valvesclerosis and effect of statin therapy (from the Heart and Soul Study).Am J Cardiol 2007;99:1128e1133.
16. Roberts WC. The senile cardiac calcification syndrome. Am J Cardiol1986;58:572e574.
17. Whooley MA, de Jonge P, Vittinghoff E, Otte C, Moos R, Carney RM,Ali S, Dowray S, Na B, Feldman MD, Schiller NB, Browner WS.Depressive symptoms, health behaviors, and risk of cardiovascularevents in patients with coronary heart disease. JAMA 2008;300:2379e2388.
18. Inker LA, Schmid CH, Tighiouart H, Eckfeldt JH, Feldman HI, GreeneT, Kusek JW, Manzi J, Van Lente F, Zhang YL, Coresh J, Levey AS;CKD-EPI Investigators. Estimating glomerular filtration rate fromserum creatinine and cystatin C. N Engl J Med 2012;367:20e29.
19. Luepker RV, Apple FS, Christenson RH, Crow RS, Fortmann SP, GoffD, Goldberg RJ, Hand MM, Jaffe AS, Julian DG, Levy D, Manolio T,
Mendis S, Mensah G, Pajak A, Prineas RJ, Reddy KS, Roger VL,Rosamond WD, Shahar E, Sharrett AR, Sorlie P, Tunstall- Pedoe H;AHA Council on Epidemiology and Prevention; AHA StatisticsCommittee; World Heart Federation Council on Epidemiology andPrevention; European Society of Cardiology Working Group onEpidemiology and Prevention; Centers for Disease Control andPrevention; National Heart, Lung, and Blood Institute. Case definitionsfor acute coronary heart disease in epidemiology and clinical researchstudies: a statement from the AHA Council on Epidemiology andPrevention; AHA Statistics Committee; World Heart FederationCouncil on Epidemiology and Prevention; the European Society ofCardiology Working Group on Epidemiology and Prevention; Centersfor Disease Control and Prevention; and the National Heart, Lung, andBlood Institute. Circulation 2003;108:2543e2549.
20. Rossi A, Targher G, Zoppini G, Cicoira M, Bonapace S, Negri C,Stoico V, Faggiano P, Vassanelli C, Bonora E. Aortic and mitralannular calcifications are predictive of all-cause and cardiovascularmortality in patients with type 2 diabetes. Diabetes Care 2012;35:1781e1786.
21. Corciu AI, Siciliano V, Poggianti E, Petersen C, Venneri L, Picano E.Cardiac calcification by transthoracic echocardiography in patients withknown or suspected coronary artery disease. Int J Cardiol 2010;142:288e295.
22. Pressman GS, Crudu V, Parameswaran-Chandrika A, Romero-CorralA, Purushottam B, Figueredo VM. Can total cardiac calcium predictthe coronary calcium score? Int J Cardiol 2011;146:202e206.





























