Embed Size (px)
Citation preview

Use of Intravascular Ultrasound Imaging in Percutaneous Coronary Intervention on Left Main Coronary Artery Disease
Adrian Banning MD, MBBS; Giovanni Luigi De Maria MDJohn Radcliffe Hospital, Oxford University Hospitals, Oxford, UK
Professor Adrian BanningJohn Radcliffe Hospital, Oxford University Hospitals, Oxford, UK
Adrian Banning
Professor Banning is a Consultant Interventional Cardiologist in Oxford. He
has an interest in the development of drug-eluting stents and participated in
many landmark interventional studies (e.g. Taxus, Syntax, Noble and Excel). He
has a particular interest in interventions for left main coronary artery diesase
and revascularisation injury. He has >300 PubMed citations and is the current
President of the British Cardiovascular Intervention Society (BCIS).
Dr Giovanni Luigi De MariaJohn Radcliffe Hospital, Oxford University Hospitals, Oxford, UK
Giovanni Luigi De Maria
Dr Giovanni Luigi De Maria completed medical school at the Catholic University
of the Sacred Heart in Rome, Italy and his cardiology training at the Policlinico
Agostino Gemelli in Rome. He moved to the UK in 2013 and he is currently
working as Fellow in Interventional Cardiology at the Heart Centre of Oxford
University Hospitals.
His main research interests are predicting outcome in patients with STEMI,
coronary physiology and intravascular imaging. He is involved in a number
of randomised clinical trials including (SYNTAX II, NOBLE, EBC- Main, FAME 3,
ERIC PPCI).
IntroductionDetecting obstructive disease of the left main coronary artery (LMCA) disease is a relatively unusual
occurrence in the catheterisation laboratory, as it accounts for approximately 4 % of all coronary
angiograms, with isolated LMCA disease observed in only 5–10 % of these cases.1 Historically, coronary
artery bypass grafting (CABG) represented the treatment of choice with a well-documented prognostic
benefit, mainly related to the high rate of long-term patency of the left internal mammary artery graft.2,3
Data from four large studies have highlighted the potential equivalence of stenting and CABG in the
LMCA setting.4–7 In particular, the Synergy between Percutaneous Coronary Intervention (PCI) with
TAXUS and Cardiac Surgery (SYNTAX) study showed that when coronary anatomy complexity was
low or relatively low (defined by a SYNTAX score <32) then CABG and PCI performed well with similar
outcomes at 1 and 5 years’ follow-up, with PCI affected by a higher rate of repeated revascularisation
and CABG by a higher rate of stroke.5 These conclusions led to a change in European guidelines
on myocardial revascularisation, with PCI having a IA indication for LMCA disease when SYNTAX
score is <22 and IIaB when SYNTAX score is >22 and <32.8 They also prompted the initiation and
recruitment of the randomised Evaluation of the Xience Everolimus-Eluting Stent Versus CABG
Surgery for Effectiveness of Left Main Revascularization (EXCEL) and CABG Vs Drug Eluting Stent
Percutaneous Coronary Angioplasty in the Treatment of Unprotected Left Main Stenosis (NOBLE)
studies comparing CABG versus PCI for LMCA disease.9
In our opinion, LMCA intervention is worthy of special consideration compared with treatment of
coronary stenosis elsewhere in the coronary tree. First, potential complications occurring during
LMCA intervention may have a rapid progression towards haemodynamic instability, since LMCA
provides blood supply to 80 % of left ventricle in patients with right coronary dominance.10 Second,
LMCA disease is difficult to assess angiographically because of the possible lack of a proximal
reference.11 Third, atherosclerosis at the LMCA site is diffuse in most cases, with frequent involvement
of the bifurcation, and often featured by a higher rate of fibrotic and calcific component, making
LMCA lesion tougher with the consequent need for appropriate and careful lesion preparation.12,13
As a result of this technical complexity and the proven efficacy of CABG in LMCA disease, it is
essential that when PCI is performed on LMCA, every effort is made to ensure that the final outcome
of revascularisation is as good as that potentially achievable with CABG. This requires careful
patient selection, rigorous procedural planning and application of the best available technology
(in terms of stent and imaging techniques). Consequently, we consider use of intravascular imaging
and usually intravascular ultrasound (IVUS) to be mandatory during most LMCA interventions; this is
supported by a IIaB indication in the European myocardial revascularisation guidelines.8
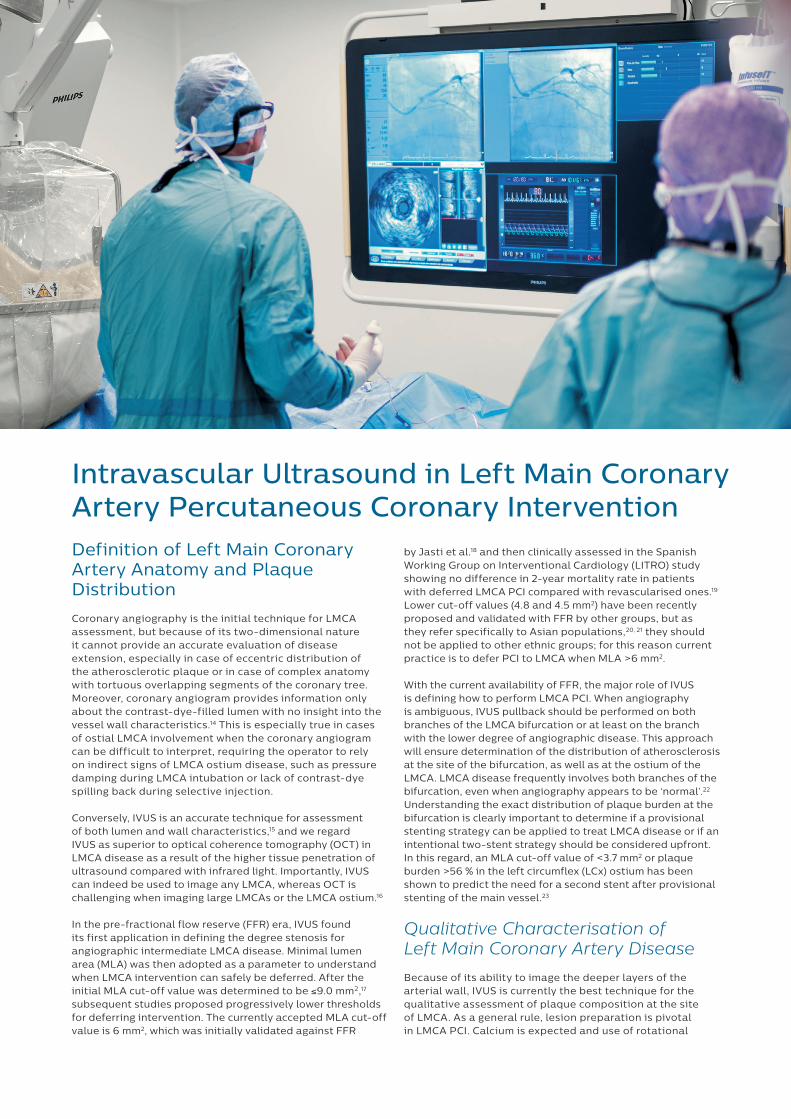
Intravascular Ultrasound in Left Main Coronary Artery Percutaneous Coronary InterventionDefinition of Left Main Coronary Artery Anatomy and Plaque Distribution
Coronary angiography is the initial technique for LMCA assessment, but because of its two-dimensional nature it cannot provide an accurate evaluation of disease extension, especially in case of eccentric distribution of the atherosclerotic plaque or in case of complex anatomy with tortuous overlapping segments of the coronary tree. Moreover, coronary angiogram provides information only about the contrast-dye-filled lumen with no insight into the vessel wall characteristics.14 This is especially true in cases of ostial LMCA involvement when the coronary angiogram can be difficult to interpret, requiring the operator to rely on indirect signs of LMCA ostium disease, such as pressure damping during LMCA intubation or lack of contrast-dye spilling back during selective injection.
Conversely, IVUS is an accurate technique for assessment of both lumen and wall characteristics,15 and we regard IVUS as superior to optical coherence tomography (OCT) in LMCA disease as a result of the higher tissue penetration of ultrasound compared with infrared light. Importantly, IVUS can indeed be used to image any LMCA, whereas OCT is challenging when imaging large LMCAs or the LMCA ostium.16
In the pre-fractional flow reserve (FFR) era, IVUS found its first application in defining the degree stenosis for angiographic intermediate LMCA disease. Minimal lumen area (MLA) was then adopted as a parameter to understand when LMCA intervention can safely be deferred. After the initial MLA cut-off value was determined to be ≤9.0 mm2,17 subsequent studies proposed progressively lower thresholds for deferring intervention. The currently accepted MLA cut-off value is 6 mm2, which was initially validated against FFR
by Jasti et al.18 and then clinically assessed in the Spanish Working Group on Interventional Cardiology (LITRO) study showing no difference in 2-year mortality rate in patients with deferred LMCA PCI compared with revascularised ones.19 Lower cut-off values (4.8 and 4.5 mm2) have been recently proposed and validated with FFR by other groups, but as they refer specifically to Asian populations,20, 21 they should not be applied to other ethnic groups; for this reason current practice is to defer PCI to LMCA when MLA >6 mm2.
With the current availability of FFR, the major role of IVUS is defining how to perform LMCA PCI. When angiography is ambiguous, IVUS pullback should be performed on both branches of the LMCA bifurcation or at least on the branch with the lower degree of angiographic disease. This approach will ensure determination of the distribution of atherosclerosis at the site of the bifurcation, as well as at the ostium of the LMCA. LMCA disease frequently involves both branches of the bifurcation, even when angiography appears to be ‘normal’.22 Understanding the exact distribution of plaque burden at the bifurcation is clearly important to determine if a provisional stenting strategy can be applied to treat LMCA disease or if an intentional two-stent strategy should be considered upfront. In this regard, an MLA cut-off value of <3.7 mm2 or plaque burden >56 % in the left circumflex (LCx) ostium has been shown to predict the need for a second stent after provisional stenting of the main vessel.23
Qualitative Characterisation of Left Main Coronary Artery Disease
Because of its ability to image the deeper layers of the arterial wall, IVUS is currently the best technique for the qualitative assessment of plaque composition at the site of LMCA. As a general rule, lesion preparation is pivotal in LMCA PCI. Calcium is expected and use of rotational

atherectomy24 should be considered as a default strategy. In this context IVUS defines the extension of calcium25 by the high backscattering signal with posterior shadowing.26
The extension of the calcific arch is a parameter easily available with IVUS, with a calcific arch greater than 180° representing a strong indication for rotational atherectomy. Pre-stenting IVUS can help to identify those cases in whom rotational atherectomy is mandatory from those in whom predilation with non-compliant balloons at high pressure could be a possible alternative, especially in those catheterisation laboratories with no operators trained in rotational atherectomy. Beside identifying its circular and longitudinal extension, IVUS can also help to identify the depth of the calcific component.27 This is relevant as deep and thick calcium might be associated with a higher risk of coronary perforation during balloon inflation and thus mandate rotational atherectomy.28
Stent Sizing
After having clarified plaque burden, plaque distribution and plaque composition, IVUS can in the end provide information about true vessel dimensions in order to facilitate stent sizing. Because of its large calibre and the mismatch in diameter between LMCA and the LMCA-bifurcation branches, stent sizing in LMCA PCI can be tricky using angiography only, with the operator called to make a decision according to the less-accurate information achievable with a two-dimensional technique. Conversely, IVUS-defined lumen area can provide a more detailed definition of the lumen, with stent sizing performed taking into account not just one single diameter (as in angiography), but at least three diameters, namely maximum, minimum and mean diameter.
By providing a more accurate detection of atherosclerosis, IVUS can assure a better definition of proximal and distal references for stent diameter sizing, and better identification of proximal and distal landing zones free from disease, thus ultimately providing information for stent length sizing, minimising the risk of longitudinal miss during stent deployment.
Consequently, we believe IVUS should be applied before stenting to aid proper planning of LMCA PCI as it can:
1) define LMCA anatomy and plaque burden distribution; 2) characterise the disease, especially the extent of calcification; 3) determine initial stent sizing.
Use of IVUS post-stenting is mainly meant to assure stent result optimisation and plaque coverage.
Stent Optimisation
Stent optimisation is the main indication for IVUS in LMCA PCI, and in our opinion a post-stenting IVUS should always be performed when it is safe to do so. Although there are no large randomised clinical trials to assess ad hoc whether intravascular imaging-guided LMCA PCI is associated with better long-term clinical outcomes, convincing data from large registries suggest a long-term mortality benefit in patients undergoing IVUS-guided compared with angio-guided LMCA PCI.29, 30
Stent malapposition, stent underexpansion, geographical miss and large uncovered stent-edge dissection are all possible stent-related complications detectable by IVUS.31 Importantly, stent underexpansion is the main predictor of stent failure. For this reason Kang et al. have proposed a minimum value of stent area that should be achieved in each segment of the LMCA bifurcation after stenting (>5 mm2 at LCx ostium; >6 mm2 at left anterior descending [LAD] ostium; >7 mm2 at polygon of confluence [POC]; >8 mm2 at LMCA).32 The decision to intervene in case of stent malapposition or edge dissection is more complex as proven thresholds have not been proposed or prospectively validated.
When treating LMCA bifurcation, IVUS can be used to identify the mechanism of side-branch compromise after main-branch stenting. It is important to recognise whether intervention on the side branch can be avoided if safe and efficacious, and IVUS can have a role in the decision process in order to define how the operator should eventually intervene. If carina shift is identified as the underlying mechanism, then kissing balloon inflation could be enough to reshape the carina and restore normal flow down both limbs of the bifurcation. Conversely, if plaque shift is detected then the operator may bail out from the provisional single-stent strategy into a two-stent procedure.
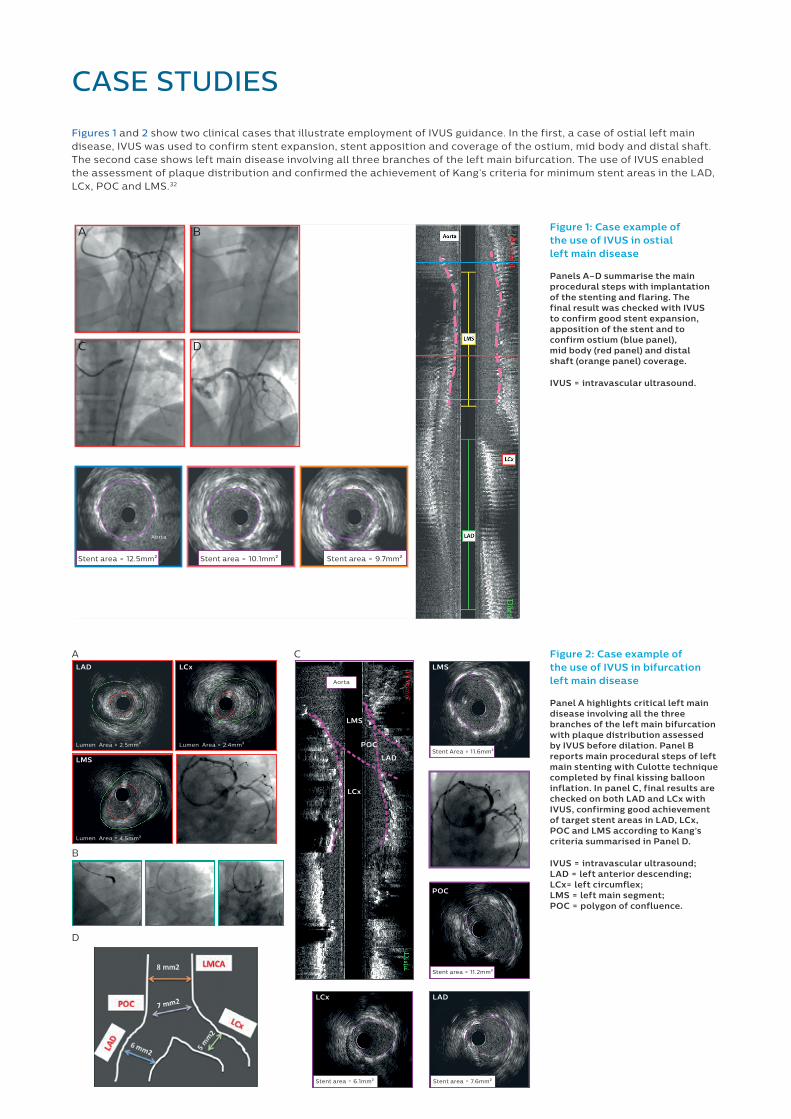
Figures 1 and 2 show two clinical cases that illustrate employment of IVUS guidance. In the first, a case of ostial left main disease, IVUS was used to confirm stent expansion, stent apposition and coverage of the ostium, mid body and distal shaft. The second case shows left main disease involving all three branches of the left main bifurcation. The use of IVUS enabled the assessment of plaque distribution and confirmed the achievement of Kang’s criteria for minimum stent areas in the LAD, LCx, POC and LMS.32
CASE STUDIES
Figure 1: Case example of the use of IVUS in ostial left main disease
Panels A–D summarise the main procedural steps with implantation of the stenting and flaring. The final result was checked with IVUS to confirm good stent expansion, apposition of the stent and to confirm ostium (blue panel), mid body (red panel) and distal shaft (orange panel) coverage.
IVUS = intravascular ultrasound.
Figure 2: Case example of the use of IVUS in bifurcation left main disease
Panel A highlights critical left main disease involving all the three branches of the left main bifurcation with plaque distribution assessed by IVUS before dilation. Panel B reports main procedural steps of left main stenting with Culotte technique completed by final kissing balloon inflation. In panel C, final results are checked on both LAD and LCx with IVUS, confirming good achievement of target stent areas in LAD, LCx, POC and LMS according to Kang’s criteria summarised in Panel D.
IVUS = intravascular ultrasound; LAD = left anterior descending; LCx= left circumflex; LMS = left main segment; POC = polygon of confluence.
Stent area = 12.5mm2
A B
C D
Aorta
Stent area = 10.1mm2 Stent area = 9.7mm2
Stent area = 11.2mm2
Lumen Area = 2.5mm2
Lumen Area = 4.5mm2
LMS
LMS
LMS
POC
POC
LAD
LAD
LCx
LADLCx
LCx
Lumen Area = 2.4mm2
Stent area = 7.6mm2
Stent Area = 11.6mm2
Stent area = 6.1mm2
Aorta
A C
D
B
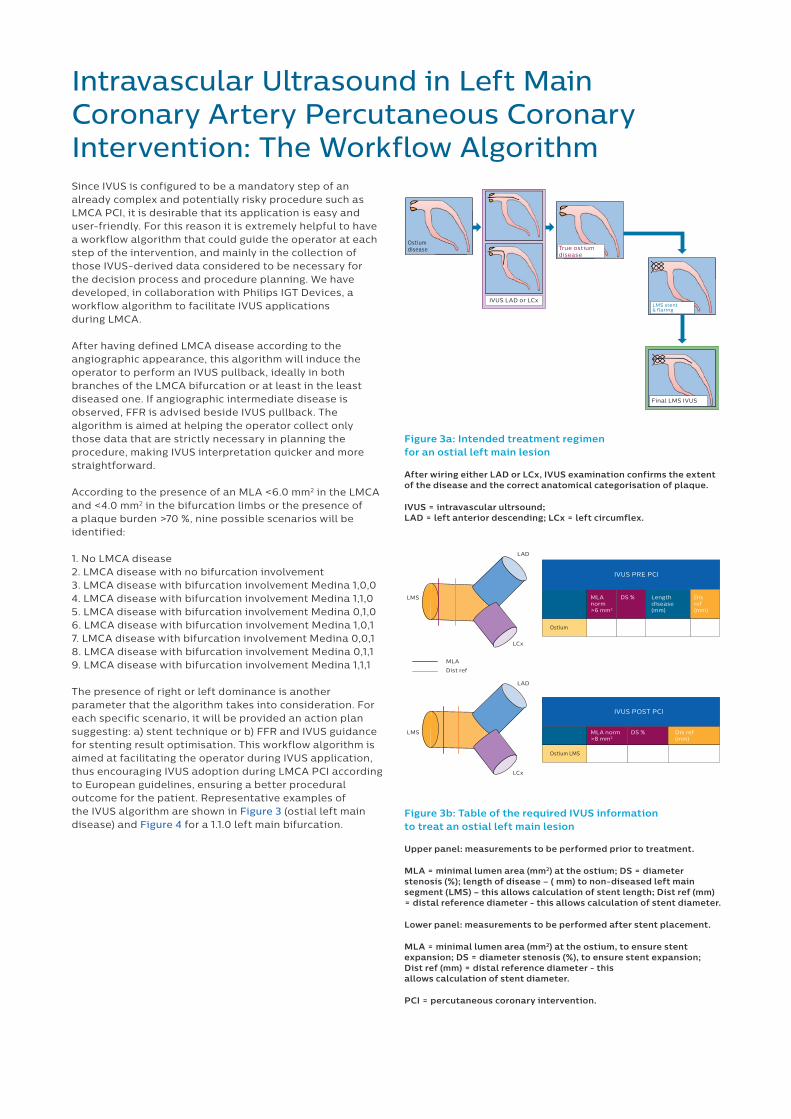
Intravascular Ultrasound in Left Main Coronary Artery Percutaneous Coronary Intervention: The Workflow AlgorithmSince IVUS is configured to be a mandatory step of an already complex and potentially risky procedure such as LMCA PCI, it is desirable that its application is easy and user-friendly. For this reason it is extremely helpful to have a workflow algorithm that could guide the operator at each step of the intervention, and mainly in the collection of those IVUS-derived data considered to be necessary for the decision process and procedure planning. We have developed, in collaboration with Philips IGT Devices, a workflow algorithm to facilitate IVUS applications during LMCA.
After having defined LMCA disease according to the angiographic appearance, this algorithm will induce the operator to perform an IVUS pullback, ideally in both branches of the LMCA bifurcation or at least in the least diseased one. If angiographic intermediate disease is observed, FFR is advised beside IVUS pullback. The algorithm is aimed at helping the operator collect only those data that are strictly necessary in planning the procedure, making IVUS interpretation quicker and more straightforward.
According to the presence of an MLA <6.0 mm2 in the LMCA and <4.0 mm2 in the bifurcation limbs or the presence of a plaque burden >70 %, nine possible scenarios will be identified:
1. No LMCA disease2. LMCA disease with no bifurcation involvement3. LMCA disease with bifurcation involvement Medina 1,0,04. LMCA disease with bifurcation involvement Medina 1,1,05. LMCA disease with bifurcation involvement Medina 0,1,06. LMCA disease with bifurcation involvement Medina 1,0,17. LMCA disease with bifurcation involvement Medina 0,0,18. LMCA disease with bifurcation involvement Medina 0,1,19. LMCA disease with bifurcation involvement Medina 1,1,1
The presence of right or left dominance is another parameter that the algorithm takes into consideration. For each specific scenario, it will be provided an action plan suggesting: a) stent technique or b) FFR and IVUS guidance for stenting result optimisation. This workflow algorithm is aimed at facilitating the operator during IVUS application, thus encouraging IVUS adoption during LMCA PCI according to European guidelines, ensuring a better procedural outcome for the patient. Representative examples of the IVUS algorithm are shown in Figure 3 (ostial left main disease) and Figure 4 for a 1.1.0 left main bifurcation.
Ostiumdisease
Ostium
True ostium disease
LMS stent& �aring
IVUS LAD or LCx
Final LMS IVUS
IVUS PRE PCI
MLAnorm >6 mm2
DS % Lengthdisease(mm)
Disref(mm)
Ostium LMS
IVUS POST PCI
MLA norm >8 mm2
DS % Dis ref(mm)
LAD
LCx
LCx
LAD
LMS
LMS
MLA
Dist ref
Ostiumdisease
Ostium
True ostium disease
LMS stent& �aring
IVUS LAD or LCx
Final LMS IVUS
IVUS PRE PCI
MLAnorm >6 mm2
DS % Lengthdisease(mm)
Disref(mm)
Ostium LMS
IVUS POST PCI
MLA norm >8 mm2
DS % Dis ref(mm)
LAD
LCx
LCx
LAD
LMS
LMS
MLA
Dist ref
Figure 3a: Intended treatment regimen for an ostial left main lesion
After wiring either LAD or LCx, IVUS examination confirms the extent of the disease and the correct anatomical categorisation of plaque.
IVUS = intravascular ultrsound; LAD = left anterior descending; LCx = left circumflex.
Figure 3b: Table of the required IVUS information to treat an ostial left main lesion
Upper panel: measurements to be performed prior to treatment.
MLA = minimal lumen area (mm2) at the ostium; DS = diameter stenosis (%); length of disease – ( mm) to non-diseased left main segment (LMS) – this allows calculation of stent length; Dist ref (mm) = distal reference diameter - this allows calculation of stent diameter.
Lower panel: measurements to be performed after stent placement.
MLA = minimal lumen area (mm2) at the ostium, to ensure stent expansion; DS = diameter stenosis (%), to ensure stent expansion; Dist ref (mm) = distal reference diameter - this allows calculation of stent diameter.
PCI = percutaneous coronary intervention.
In conclusion, IVUS has become a standard part of the PCI procedure for treatment of the left main. Improving consistency of its application and the subsequent technical approach(es) is likely to improve technique and, consequently, patient outcomes.
Good angiographicresult on LCx?
1,1,0True 1,1,0
Target: Kang’s criteriaTarget MLA as in 1,1,1
Double stent+ FKI
ProvisionalMB & POT
FKI
NoNo
No
Yes
FFR >0.80 on LCx
IVUS LAD & LCx
Final IVUS
FFR <0.80on LCx
FFR on LCx >0.80
Yes
Final IVUS
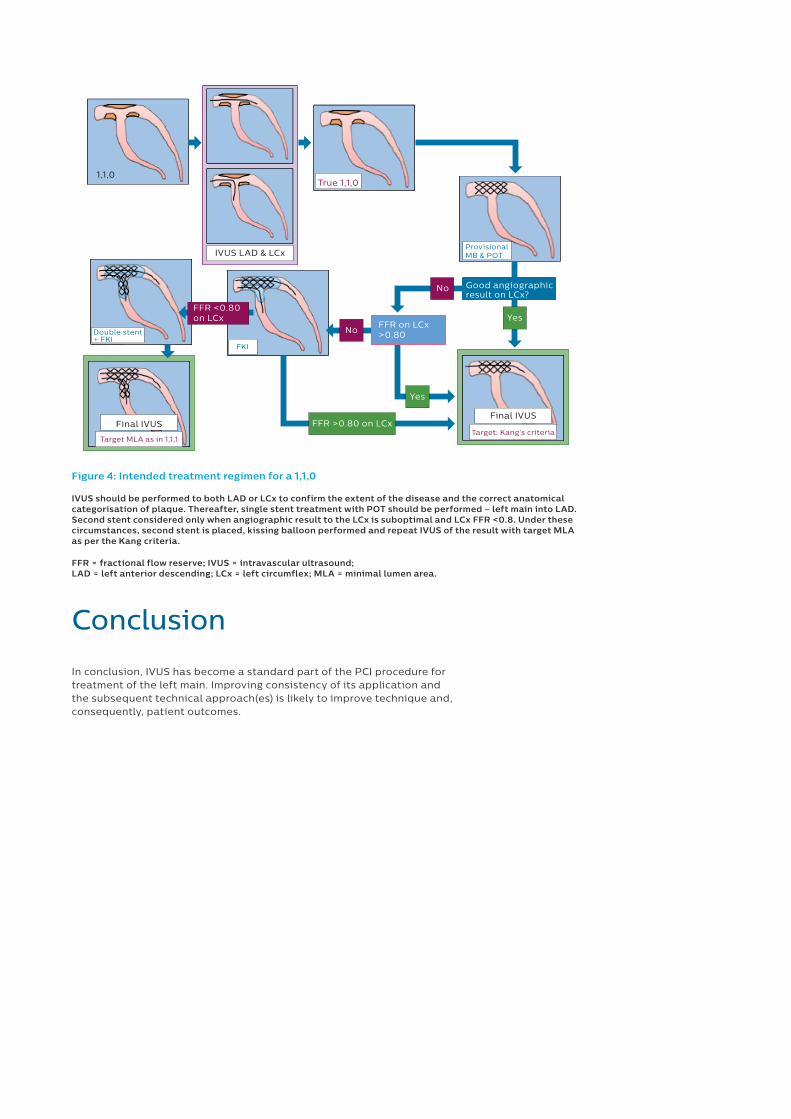
Figure 4: Intended treatment regimen for a 1,1,0
IVUS should be performed to both LAD or LCx to confirm the extent of the disease and the correct anatomical categorisation of plaque. Thereafter, single stent treatment with POT should be performed – left main into LAD. Second stent considered only when angiographic result to the LCx is suboptimal and LCx FFR <0.8. Under these circumstances, second stent is placed, kissing balloon performed and repeat IVUS of the result with target MLA as per the Kang criteria.
FFR = fractional flow reserve; IVUS = intravascular ultrasound; LAD = left anterior descending; LCx = left circumflex; MLA = minimal lumen area.
Conclusion
References1. Giannoglou GD, Antoniadis AP, Chatzizisis
YS, et al. Prevalence of narrowing >or=50% of the left main coronary artery among 17,300 patients having coronary angiography. Am J Cardiol 2006;98:1202–5. DOI: 10.1016/j.amjcard.2006.05.052; PMID: 17056328.
2. Shah PJ, Durairaj M, Gordon I, et al. Factors affecting patency of internal thoracic artery graft: clinical and angiographic study in 1434 symptomatic patients operated between 1982 and 2002. Eur J Cardiothorac Surg 2004;26:118–24. DOI: 10.1016/j.ejcts.2004.02.037; PMID: 15200989.
3. Chaitman BR, Fisher LD, Bourassa MG, et al. Effect of coronary bypass surgery on survival patterns in subsets of patients with left main coronary artery disease. Report of the Collaborative Study in Coronary Artery Surgery (CASS). Am J Cardiol 1981;48:765–77. PMID: 7025604.
4. Buszman PE, Buszman PP, Kiesz RS, et al. Early and long-term results of unprotected left main coronary artery stenting: the LE MANS (Left Main Coronary Artery Stenting) registry. J Am Coll Cardiol 2009;54:1500–11. DOI: 10.1016/j.jacc.2009.07.007; PMID: 19699048.
5. Morice MC, Serruys PW, Kappetein AP, et al. Outcomes in patients with de novo left main disease treated with either percutaneous coronary intervention using paclitaxel-eluting stents or coronary artery bypass graft treatment in the Synergy Between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery (SYNTAX) trial. Circulation 2010;121:2645–53. DOI: 10.1161/CIRCULATIONAHA.109.899211; PMID: 20530001.
6. Boudriot E, Thiele H, Walther T, et al. Randomized comparison of percutaneous coronary intervention with sirolimus-eluting stents versus coronary artery bypass grafting in unprotected left main stem stenosis. J Am Coll Cardiol 2011;57:538–45. DOI: 10.1016/j.jacc.2010.09.038; PMID: 21272743.
7. Park SJ, Kim YH, Park DW, et al. Randomized trial of stents versus bypass surgery for left main coronary artery disease. N Engl J Med 2011;364:1718–27. DOI: 10.1056/NEJMoa1100452; PMID: 21463149.
8. Windecker S, Kolh P, Alfonso F, et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J 2014;35:2541–619. DOI: 10.1093/eurheartj/ehu278; PMID: 25173339.
9. Campos CM, Christiansen EH, Stone GW, Serruys PW. The EXCEL and NOBLE trials: similarities, contrasts and future perspectives for left main revascularisation. EuroIntervention 2015;11 Suppl V:115–9. DOI: 10.4244/EIJV11SVA26; PMID: 25983143.
10. Patel N, De Maria GL, Kassimis G, et al. Outcomes after emergency percutaneous coronary intervention in patients with unprotected left main stem occlusion: the BCIS national audit of percutaneous coronary intervention 6-year experience. JACC Cardiovasc Interv 2014;7:969–80. DOI: 10.1016/j.jcin.2014.04.011; PMID: 25234669.
11. Lefèvre T, Girasis C, Lassen JF. Differences between the left main and other bifurcations. EuroIntervention 2015;11 Suppl V:106–10. DOI: 10.4244/EIJV11SVA24; PMID: 25983141.
12. Wykrzykowska JJ, Mintz GS, Garcia-Garcia HM, et al. Longitudinal distribution of plaque burden and necrotic core-rich plaques in nonculprit lesions of patients presenting with acute coronary syndromes. JACC Cardiovasc Imaging 2012;5(3 Suppl):10–8. DOI: 10.1016/j.jcmg.2012.01.006; PMID: 22421223.
13. Mercado N, Moe TG, Pieper M, et al. Tissue characterisation of atherosclerotic plaque in the left main: an in vivo intravascular ultrasound radiofrequency data analysis. EuroIntervention 2011;7:347–52. DOI: 10.4244/EIJV7I3A59; PMID: 21729837.
14. Topol EJ, Nissen SE. Our preoccupation with coronary luminology. The dissociation between clinical and angiographic findings in ischemic heart disease. Circulation 1995;92:2333–42. PMID: 7554219.
15. St Goar FG, Pinto FJ, Alderman EL, et al. Intravascular ultrasound imaging of angiographically normal coronary arteries: an in vivo comparison with quantitative angiography. J Am Coll Cardiol 1991;18:952–8. PMID: 1894869.
16. Burzotta F, Dato I, Trani C, et al. Frequency domain optical coherence tomography to assess non-ostial left main coronary artery. EuroIntervention 2015;10:e1–8. DOI: 10.4244/EIJV10I9A179; PMID: 25599698.
17. Nissen SE, Yock P. Intravascular ultrasound: novel pathophysiological insights and current clinical applications. Circulation 2001;103:604–16. PMID: 11157729.
18. Jasti V, Ivan E, Yalamanchili V, et al. Correlations between fractional flow reserve and intravascular ultrasound in patients with an ambiguous left main coronary artery stenosis. Circulation 2004;110:2831–6. DOI: 10.1161/01.CIR.0000146338.62813.E7; PMID: 15492302.
19. de la Torre Hernandez JM, Hernández Hernandez F, Alfonso F, et al. Prospective application of pre-defined intravascular ultrasound criteria for assessment of intermediate left main coronary artery lesions results from the multicenter LITRO study. J Am Coll Cardiol 2011;58:351–8. DOI: 10.1016/j.jacc.2011.02.064; PMID: 21757111.
20. Kang SJ, Lee JY, Ahn JM, et al. Intravascular ultrasound-derived predictors for fractional flow reserve in intermediate left main disease. JACC Cardiovasc Interv 2011;4:1168–74. DOI: 10.1016/j.jcin.2011.08.009; PMID: 22115656.
21. Park SJ, Ahn JM, Kang SJ, et al. Intravascular ultrasound-derived minimal lumen area criteria for functionally significant left main coronary artery stenosis. JACC Cardiovasc Interv 2014;7:868–74. DOI: 10.1016/j.jcin.2014.02.015; PMID: 25147031.
22. Oviedo C, Maehara A, Mintz GS, et al. Intravascular ultrasound classification of plaque distribution in left main coronary artery bifurcations: where is the plaque really located? Circ Cardiovasc Interv 2010;3:105–12. DOI: 10.1161/CIRCINTERVENTIONS.109.906016; PMID: 20197513.
23. Kang SJ, Ahn JM, Kim WJ, et al. Functional and morphological assessment of side branch after left main coronary artery bifurcation stenting with cross-over technique. Catheter Cardiovasc Interv 2014;83:545–52. DOI: 10.1002/ccd.25057; PMID: 23765939.
24. Barbato E, Carrié D, Dardas P, et al. European expert consensus on rotational atherectomy. EuroIntervention 2015;11:30–6. DOI: 10.4244/EIJV11I1A6; PMID: 25982648.
25. Tuzcu EM, Berkalp B, De Franco AC, et al. The dilemma of diagnosing coronary calcification: angiography versus intravascular ultrasound. J Am Coll Cardiol 1996;27:832–8. PMID: 8613611.
26. Lotfi A, Jeremias A, Fearon WF, et al. Expert consensus statement on the use of fractional flow reserve, intravascular ultrasound, and optical coherence tomography: a consensus statement of the Society of Cardiovascular Angiography and Interventions. Catheter Cardiovasc Interv 2014;83:509–18. DOI: 10.1002/ccd.25222; PMID: 24227282.
27. Mintz GS, Popma JJ, Pichard AD, et al. Patterns of calcification in coronary artery disease. A statistical analysis of intravascular ultrasound and coronary angiography in 1155 lesions. Circulation 1995;91:1959–65. PMID: 7895353.
28. Hendry C, Fraser D, Eichhofer J, et al. Coronary perforation in the drug-eluting stent era: incidence, risk factors, management and outcome: the UK experience. EuroIntervention 2012;8:79–86. DOI: 10.4244/EIJV8I1A13; PMID: 22580251.
29. Park SJ, Kim YH, Park DW, et al. Impact of intravascular ultrasound guidance on long-term mortality in stenting for unprotected left main coronary artery stenosis. Circ Cardiovasc Interv 2009;2:167–77. DOI: 10.1161/CIRCINTERVENTIONS.108.799494; PMID: 20031713.
30. de la Torre Hernandez JM, Baz Alonso JA, Gómez Hospital JA, et al. Clinical impact of intravascular ultrasound guidance in drug-eluting stent implantation for unprotected left main coronary disease: pooled analysis at the patient-level of 4 registries. JACC Cardiovasc Interv 2014;7:244–54. DOI: 10.1016/j.jcin.2013.09.014; PMID: 24650399.
31. Bing R, Yong AS, Lowe HC. Percutaneous transcatheter assessment of the left main coronary artery: current status and future directions. JACC Cardiovasc Interv 2015;8:1529–39. DOI: 10.1016/j.jcin.2015.07.017; PMID: 26493245.
32. Kang SJ, Ahn JM, Song H, et al. Comprehensive intravascular ultrasound assessment of stent area and its impact on restenosis and adverse cardiac events in 403 patients with unprotected left main disease. Circ Cardiovasc Interv 2011;4:562–9. DOI: 10.1161/CIRCINTERVENTIONS.111.964643; PMID: 22045969.

© 2017 Koninklijke Philips N.V. All rights reserved. Specifications are subject to change without notice. Trademarks are the property of Koninklijke Philips N.V. (Royal Philips) or their respective owners.
www.philips.com/IGTdevicespart nr.: D000125288