Embed Size (px)
Citation preview

resecting large head and neck tumours which requiresacrifice of the facial nerve. This technique providesadequate tissue to fill the facial defect and the vascularisedfascia lata can be fashioned to form a sling to provideexcellent static support to the lower face.
References
1. Harrison DH. Surgical correction of unilateral and bilateral facialpalsy. Postgrad Med J 2005;81:562e7.
2. Chana J, Wei FC. ‘A review of the advantages of theanterolateral thigh flap in head and neck reconstruction’.Br J Plast Surg 2004 Oct;57:603e9.
3. Koshima I, Yamamoto H, Hosoda M, et al. Free combinedcomposite flaps using the lateral circumflex femoral system forrepair of massive defects of the head and neck regions: anintroduction to the chimeric flap principle. Plast Reconstr Surg1993 Sep;92:411e20.
4. Lin YT, Lin CH, Wei FC. More degrees of freedom by usingchimeric concept in the applications of anterolateral thigh flap.J Plast Reconstr Aesthet Surg 2006;59:622e7.
5. Deiler S, Pfadenhauer A, Widmann J, et al. Tensor fasciae lataeperforator flap for reconstruction of composite achilles tendondefects with skin and vascularized fascia. Plast Reconstr Surg2000 Aug;106:342e9.
Daniel J. MarshJagdeep S. Chana
Department of Plastic Surgery, Royal Free Hospital,London, Uk
E-mail address: [email protected]
ª 2008 British Association of Plastic, Reconstructive and AestheticSurgeons. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.bjps.2008.02.027
Correspondence and communications 1119
Upper extremity reconstruction with pedicledanterolateral thigh perforator flap: a simplemodification for a difficult situation*
Management of soft tissue defects of the hand requiresboth aesthetic and functional consideration. Local andpedicled flaps offer favourable coverage for small ormedium-sized defects.1 However, larger defects requirelarger amounts of soft tissue which can be obtained fromdistant or free flaps.2 Recently, distant flaps such as groinflaps have been rarely used because of patient discomfortand the requirement for more than one procedure. One ofthe popular members of the perforator flap family, the freeanteolateral thigh (ALT) flap, which is elevated on skinperforators originating from descending branch of thelateral circumflex femoral artery, is an excellent option forcovering the hand dorsum.3 Among numerous advantages, it
* This paper was presented at 10th National Hand and UpperExtremity Meeting and 28th Annual Meeting of the Turkish Societyof Plastic Reconstructive and Aesthetic Surgery.
allows a two-team approach and reduces the operationtime.
We present the case of an ALT flap, prepared for freetransfer to a hand dorsum defect during a two teamapproach but used as a distant flap on its pedicle because ofinsufficient recipient veins.
A 35-year-old man presented with a soft tissue defecton the dorsum of his left hand, after an injury with a woodshaving machine. A 10� 10 cm soft tissue defect on thedorsum of his left hand was apparent on physical exami-nation. Reconstruction with a free ALT perforator flap wasplanned and a two-team approach was started undergeneral anaesthesia. The first team elevated the flap ona single, long perforator uneventfully. The pedicle of theflap was not divided to maintain perfusion until therecipient vessels were prepared (Figure 1). The other teaminitially performed debridement and tendon grafting, fol-lowed by dissection of recipient vessels for free tissuetransfer. Vessels at the radial side were dissected and itwas seen that the artery was appropriate for anastomosis.However, the radial concomitant veins and other vesselsincluding ulnar concomitant, basilic and cephalic veinswere extremely small and inappropriate for anastomosis.So we decided to use the perforator flap as a pedicleddistant flap. The patient’s hand was approximated to his
Figure 1 Soft tissue defect on the dorsum of the left hand.ALT flap elevated on a long perforator vessel.
1120 Correspondence and communications
ipsilateral thigh and the flap was attached to the softtissue defect. The pedicle was secured under an ulnarly-based small skin flap at the first web space in order toavoid pedicle exposure (Figure 2). Three weeks later, thepedicle was divided under local anaesthesia and thereconstruction was completed (Figure 3). Reconstructionwith this modified technique provided an excellentanatomic and aesthetic result but the functional outcomewas moderate due to prolonged immobilisation.
The anterolateral thigh flap, which was first introducedby Song et al. in 1984, offers an excellent option for softtissue reconstruction.4 This versatile flap provides a thinand large skin paddle with a long vascular pedicle. It hasa reliable blood supply and leaves minimal donor sitemorbidity. Upper extremity defects, especially in the dorsalregion of the hand, can be perfectly covered with freea ALT flap.3 On the other hand, colour mismatch, hair-bearing characteristics, variations in perforator anatomyand steep learning curve are the most common problemsattributed to this flap.5,6
Reconstruction with an ALT perforator flap allowsa two-team approach in the supine position. However, insome instances, this can turn out to be a disadvantage. Itis not rare to have a problem during flap dissection or findinappropriate perforators that necessitate changing theoperative plan or raising another flap. On the other hand,it is more complicated if the flap is raised uneventfullybut the other team could not find any suitable recipientvessels. The described modification, using the flap asa distant pedicled flap on its perforator bundle, can bea solution for such problem. The flap can be transferredwith this technique only if an ipsilateral flap is preferred.
Figure 2 Pedicle of the ALT flap was not divided and the flapwas used as a distant pedicled flap. The pedicle of the flap wassecured under a skin flap based on the index finger at the firstweb space.
The pedicle should be prepared as long as possible so asto prevent pedicle tension and allow easy flap insetting.Also, a small flap prepared on the first web spaceprotects the pedicle from drying and thrombosis. Anuncomfortable period until the flap is divided and somejoint stiffness due to prolonged immobilisation are themain disadvantages.
References
1. Soutar DS, Tanner NSB. The radial forearm flap in the manage-ment of soft tissue injuries of the hand. Br J Plast Surg 1984;37:18e25.
2. Chen HC, Tang YB, Mardini S, et al. Reconstruction of the handand upper limb with free flaps based on musculocutaneousperforators. Microsurgery 2004;24:270e80.
3. Adani R, Tarallo L, Marcoccio I, et al. Hand reconstruction usingthe thin anterolateral thigh flap. Plast Reconstr Surg 2005;116:467e73.
4. Song YG, Chen GZ, Song YL. The free thigh flap: a new free flapconcept based on the septocutaneous artery. Br J Plast Surg1984;37:149e59.
5. Koshima I, Fukuda H, Utunomiya R, et al. The anterolateralthigh flap: variations in its vascular pedicle. Br J Plast Surg 1989;42:260e2.
6. Kimata Y, Uchiyama K, Ebihara S. Anatomic variationsand technical problems of the anterolateral thigh flap: a reportof 74 cases. Plast Reconstr Surg 1998;102:1517e23.
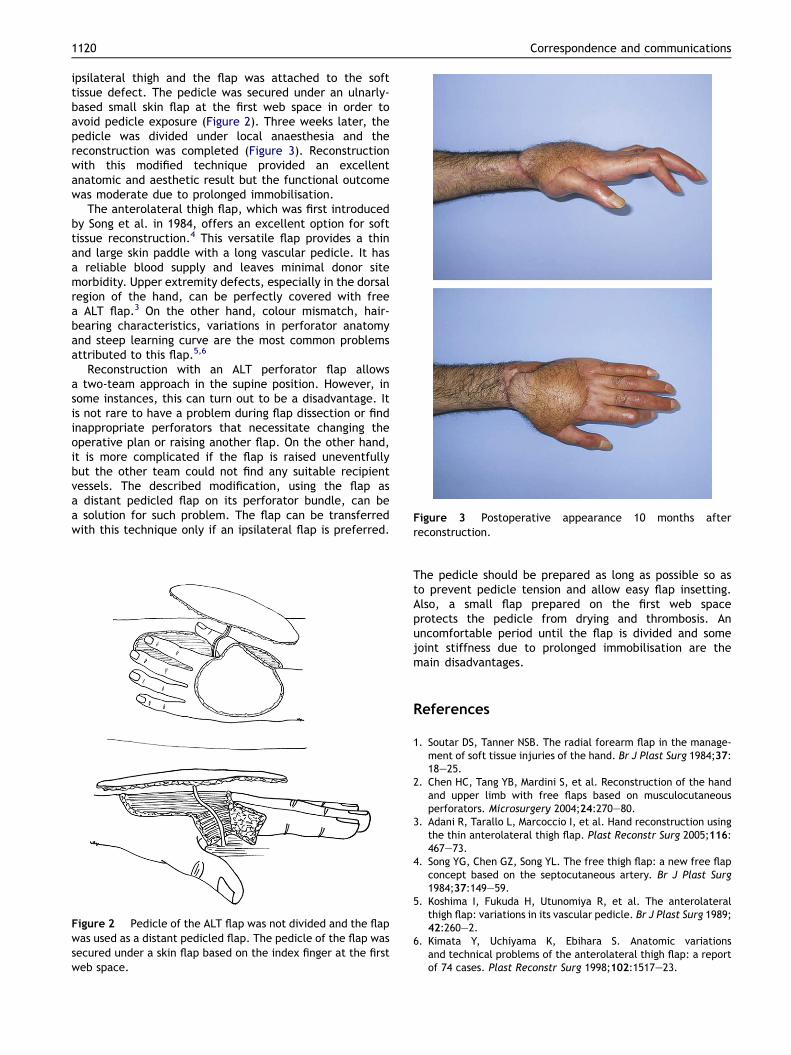
Figure 3 Postoperative appearance 10 months afterreconstruction.

Correspondence and communications 1121
Serhan TuncerKemal Findikcioglu
Suhan AyhanGazi University, Faculty of Medicine,
Department of Plastic, Reconstructive and AestheticSurgery, Ankara, Turkey
E-mail address: [email protected]
ª 2008 British Association of Plastic, Reconstructive and AestheticSurgeons. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.bjps.2007.11.071
The submersion technique for vascular injection ofperforator flaps
Anatomical injection studies have always been a driving forcein experimental plastic surgery research. It has lead plasticsurgeons to gain more knowledge about the vascularisation ofmuscle, bone, and soft tissue including skin. Althoughinjecting into defined tissue areas is a very old technique,initially used by Jean Roilan in the 1500’s1 it continues to berefined and is a vital part of the study of perforator flaps.
Techniques used range from simple dye injections usingIndia ink, Prussian blue, coloured latex injections, leadoxide, radio-opaque materials and corrosion casting.2
We are carrying out injection studies on a regular basis inour research and have found several complicating factors inachieving adequate samples. One persisting problem issignificant leaking of material from the injected tissue. It isnever possible to ligate all bleeding vessels, especially whenlarge tissue flaps, muscle or fascio-cutanous flaps, are raised.
We recently tried a new technique, which has provenvery beneficial in limiting the problem with leaking. We arenow using this technique for various materials and it hasproven to be reproducible and simple to use.
Technique
We fix the tissue that is being injected on a board with thehelp of pins, cannulate the vessel securely as describedpreviously3 and secure it for injection. We then submerge thefixed tissue into a bath of water, only at this point do we startinjection. This allows us to recognise any significant leaksimmediately and these areas can be ligated if necessary. Thewater surrounding the specimen will prevent contaminationof the surrounding tissue, as the material is not in prolongedcontact with the tissue. During the injection, the materialwill contaminate the water fairly quickly and may disrupt thevisibility. In order to ensure a well-controlled injectionwe use a gentle flow of running water to keep the tissuevisible as well as a large sink for submersion (Figure 1).
Thebigadvantageof using this technique is that it doesnotstain the surface of the tissue we are testing. Other tech-niques often leave the injected specimens unusable as thecolour from the injected material seep into the surroundingtissues and obliterate the anatomy. Our technique gives us aninjection specimen of good quality where the arterialnetwork is injected and where no marked staining of the
surrounding tissue occurs. This might seem a complicatedmodel for someone commencing anatomical research orinjection studies but it is an easy model to use. Fresh cadav-eric tissue is expensive and difficult to obtain, and in order toachieve reliable and high quality results we now use thistechnique routinely when performing injections studies.
References
1. Paweletz N. Birth of the life sciences in The Netherlands andBelgium. Nat. Rev. Mol. Cell. Biol. 2001;2:857.
2. Bergeron L, Tang M, Morris SF. A review of vascular injectiontechniques for the study of perforator flaps. Plast Reconstr Surg2006;117:2050e7.
3. Dabernig J, Zetlitz E, Cotrufo S, et al. A new method for securecannulation of blood vessels in experimental free flap surgery.Ann Plast Surg 2007;59:352e3.
Jorg DabernigStefano Cotrufo
Canniesburn Plastic Surgery Unit, Glasgow Royal Infirmary,Glasgow, UK
Department of Anatomy,Glasgow University, Glasgow, UK
Tom WalkerAnthony P. Payne
Department of Anatomy, Glasgow University,Glasgow, UK
Elisabeth ZetlitzCanniesburn Plastic Surgery Unit,
Glasgow Royal Infirmary, Glasgow, UKE-mail address: [email protected]
Crown Copyright ª 2008 Published by Elsevier Ltd on behalf ofBritish Association of Plastic, Reconstructive and AestheticSurgeons. All rights reserved.
doi:10.1016/j.bjps.2008.05.007
Figure 1 Tissue to be injected is completely submersed in thebath, and a constant flow of running water is used to ensurecompletevisualizationof theperforatorand the injectedvessels.





























