Embed Size (px)
Citation preview

Upper Extremity
Proprioceptive TrainingJennifer A. Stone, MS, ATC
Nina B. Partin, MS, ATCJoseph S. Lueken, MS, ATC
Kent E. Timm, PhD, ATC, PT, FASCMEdward J. Ryan, III, MS, ATC
Abstract: Proprioception followinglower extremity injuries is commonlyrecommended, but there is little in-formation on proprioception trainingfollowing upper extremity injuries.No studies have evaluated whetherproprioception programs for athletesin open kinetic chain activities(throwing, shot putting) should bedifferent than programs for athletesin closed kinetic chain activities(gymnastics, swimming, kayaking,or rowing). In this paper, we providea rationale for proprioception train-ing for upper extremity injuries inathletes and the importance of ana-lyzing the athlete's sport and activityfor specificity ofproprioception exer-cises. We then discuss one popularproprioception exercise, rhythmicstabilization, and propose severaladditional upper extremity proprio-ception e-xercises, along with instruc-tions for the athletic trainer on howto direct the athlete through these ex-ercises.
Jennifer A. Stone is Manager of InternalPrograms in the Sports Medicine Divisionof the US Olympic Committee at Colo-rado Springs, CO 80909.Nina B. Partin is an athletic trainer in Na-cogdoches, Tex and Joseph S. Lueken isan athletic trainer at Indiana University inBloomington, IN.Edward J. Ryan is Manager of ExternalPrograms in the Sports Medicine Divisionof the US Olympic Committee at Colo-rado Springs.Kent E. Timm is Director of Sports Med-icine at St. Luke's Sports Medicine inSaginaw, MI.
P roprioception training is an es-sential part of any rehabilita-tion program to return an ath-
lete to preinjury performance levels.Special proprioception exercises area relatively new addition to sport re-habilitation but have been an integralpart of programs for patients withbrain and spinal cord injuries.5There are two essential parts of
proprioception: the "body's abilityto vary contractile forces of musclesin immediate response to outsideforces"2 and the "sense that tells thebrain which position the limb is in atany moment in time." 15 Exercisesfor range of motion, muscularstrength and endurance, and cardio-vascular endurance aid redevelop-ment of proprioception by contract-ing muscles and moving joints, butathletes require specific propriocep-tion exercises to regain full muscu-loskeletal and athletic function.'
Recurrent joint instability is eithermechanical or functional, existing sep-arately or together. With capsular orligamentous laxity, the joint is mechan-ically unstable due to nonfunctionalsupporting structures. Muscular weak-ness can also cause mechanical insta-bility since the musculature crossingthe joint cannot hold the joint in posi-tion. The third cause of instability islack of proprioceptive feedback, a func-tional instability, causing an uncoordi-nated muscular response to motionand/or stress. A functional instabilitydoes not necessarily connote a mechan-ical instability, and muscular weaknessdoes not necessarily cause a functionalinstability.8 11 18
AnatomyProprioceptive feedback reaches the
central nervous system from receptorslocated in muscles and joints 2,3,9,14,16,17vestibular apparatus in the inner ear,17and the eyes. 16 Muscle and joint recep-tors are stimulated by movements ofthe musculoskeletal system. 2'3'914'16'17The vestibular apparatus provides in-formation on whole body position andis stimulated when upright body pos-ture changes.17 The eyes help orient thehead and body with respect to the en-vironment. Since athletes must attendto sport-related stimuli when perform-ing, they rely on information from mus-cle and joint receptors and the vestibu-lar apparatus to balance and maintainbody position. When visual stimuli areremoved or are distracting, damagedmuscle and joint receptors are re-educated to provide accurate positionalinformation to the central nervous sys-tem.10,14,15 Proprioception exercises at-tempt to simulate sport situations in therehabilitation setting.
Muscle receptors are comprised ofmuscle spindles and Golgi tendon or-gans.?6"7 Muscle spindles are specialmuscle fibers in parallel with regularskeletal muscle fibers.2"6"7 They oc-cur in larger numbers in "skill" mus-cles in the hands than in "strength"muscles in the legs and back.2 Musclespindles provide information via thegamma feedback loop to the centralnervous system. This loop monitorschange in muscle length and velocityof contraction,2"16 providing indirectjoint position information.'7 Whenskeletal muscle is stimulated, musclespindles are co-activated, maintainingtension. Decreased muscle spindletension reduces or stops its firing. Thegamma feedback loop permits rapiderror correction of muscular tension in30 to 80 ms, while correction throughvisual stimuli may take as long as 200ms.16
Golgi tendon organs are located intendons near the musculotendinousjunction and in series with the musclefibers. They monitor muscle tensionwith firing rate escalating with in-creased muscle tension. Excessive fir-ing rates from Golgi tendon organscause a reflex decrease in muscle ten-
2,16,17sion.'
Journal of Athletic Training 15

Joint receptors are located in jointcapsules, ligaments, fat pads, and pe-
riosteum of the various joints of thebody. 29"14"16"17 As these structuresare deformed by motion, joint recep-
tors are stimulated, signaling jointposition and movement over the en-
tire range of motion.17 Joint recep-
tors complement information frommuscle spindles and Golgi tendon or-
gans by directly registering joint mo-tion.16No single receptor provides all the
information needed by the centralnervous system to evaluate postureand body position. Input from mus-
cle and joint receptors, vestibular ap-
paratus, and the eyes is synthesizedfor total body position information.17
RationaleProprioception retraining following
lower extremity injuries is commonlyrecommended 1-3,6,10,12-14 but there islittle information on proprioceptiontraining following upper extremity in-juries, especially in athletes.4 7'18 Nostudies have evaluated whether prop-
rioception programs for athletes inopen kinetic chain activities, eg,
throwing or shot putting, should bedifferent than programs for athletes inclosed kinetic chain activities, eg,
gymnastics, swimming, kayaking, or
rowing.Injuries requiring surgery and/or
periods of immobilization tend tohave larger proprioceptive deficitsdue to time loss and decreased use.2
Current injury management, there-fore, encourages early, protectedmotion whenever possible.12 Asmentioned earlier, musculoskeletalmotion stimulates muscle and jointreceptors in the injured area, main-taining a limited neurological re-
sponse of these receptors.Rehabilitation programs begin with
restoration of range of motion, mus-
cular endurance, and muscularstrength. These exercises, in a non-
specific fashion, stimulate joint andmuscle proprioceptors in the injuredextremity.2 Proprioceptive neuromus-
cular facilitation exercises (PNF), bytheir design, contribute to propriocep-tion while developing range of motion,
muscular endurance, and/or muscularstegh2,4,7,19strength.2''"
Analyze ActivityThe specific activity and sport the
athlete is returning to must be ana-
lyzed for specificity of propriocep-tion exercises. If athletes normallyuse the upper extremity in an open
kinetic chain fashion, such as throw-ers in various sports, volleyball play-ers, basketball players, and weightlifters, the proprioception program
should emphasize open chain exer-
cises, such as rhythmic stabilizationat multiple positions in the range ofmotion and the first two exerciseslisted below. If the athlete uses theupper extremity in a closed kineticchain fashion, as in gymnasticswhere he/she is weight bearing, or inswimming, canoeing, rowing, or kay-
aking where the body is moved over
the stationary hand (swimming) or
extension of the hand (canoeing,rowing, or kayaking), proprioceptionexercises should be performed in thatmanner. Such exercises involve bal-ancing or moving on a trampoline,wobble board, or slide board witheyes closed, analogous to lower ex-
2,3,10,12,15tremity exercises. In con
trast to lower extremity propriocep-tion training, closed kinetic chainupper extremity proprioception exer-
cises appear later in the rehabilitationprogram due to the amount ofstrength required to support bodyweight on the injured extremity.
ExercisesOpen kinetic chain proprioception
exercises begin when range of mo-
tion and pain permit. One popularproprioception exercise for the upper
extremity is rhythmic stabilization.No other open kinetic chain exer-
cises are reported in the literature.We are proposing several additionalupper extremity proprioception exer-
cises. The exercises move from open
to closed kinetic chain. If an athletedoes not use his/her upper extremityin a closed kinetic chain fashion, theprogression finishes with open ki-netic chain exercises.
Exercise 1-Rhythmic StabilizationThe athlete positions his/her upper
extremity anywhere in its availablerange of motion and holds an isomet-ric contraction. The athletic trainerprovides enough resistance to cause
the athlete to react, but not enough tobreak the isometric contraction.19 Asthe athlete progresses, length of timeof rhythmic stabilization increases,athletic trainer resistance increases,and amount of contact area betweenathletic trainer's hands and athlete'supper extremity decreases.
Exercise 2-Mirroring UpperExtremityMove the uninjured upper extrem-
ity passively to various positions inthe available range of motion. Askthe athlete to duplicate this positionwith his/her injured upper extremity,first with eyes open, then closed. Ifhe/she misses the position, he/sheopens his/her eyes and actively dupli-cates the desired position. Concen-trate movement on the injured area,
ie, focus on shoulder positions forathletes with shoulder pathology, el-bow positions for elbow pathology,and so on. Perform 10 to 20 repeti-tions of varying positions 5 to 10times daily. Use isokinetic testingequipment with an electrogoniometerfor exact joint position measure-
ments, if desired.18
Exercise 3-Duplicating Position,Injured Upper ExtremityMove the injured upper extremity
passively to a position within itsavailable range of motion, then re-
turn it to its resting position. Again,emphasize positions in the injuredarea. Then, ask the athlete to ac-
tively duplicate the movement, firstwith his/her eyes open, then closed.If he/she misses the position, he/sheopens his/her eyes and activelymoves to the desired position. Per-form 10 to 20 repetitions of varyingpositions 5 to 10 times daily.
Exercise 4-Double and Single ArmBalancingHave the athlete balance with both
hands on the floor, a wobble board(Fig 1), and finally a trampoline (Fig
16 Volume 29 * Number 1 * 1994

Fig 1.-Eyes open, double arm bal- Fig 2.-Eyes open, single arm balanceance in kneeling push-up position on in push-up position on trampoline.wobble board.
2). Progress through the followingbody positions, first with eyes open,then closed. Start in the quadrupedposition and progress to kneelingpush-up, full push-up, and finallyfeet-elevated (feet level or higherthan shoulders) positions. Also,move from balancing on both handsto balancing only on the injuredhand. Initially, perform each balancefor 15 seconds and gradually extend
to 60 seconds. Perform 5 to 10 repe-titions three to five times daily.
Exercise 5-Fitter®Have the athlete "stand" on the Fit-
ter (Stack Enterprises, Calgary, Al-berta, Canada) on his/her hands. Movethrough the following body positionsfirst with eyes open, then with eyesclosed. Stabilize the Fitter with four re-sistance cords and position the athleteperpendicular to it. Rock the Fitter
from right to left in the frontal plane(Fig 3), then move the athlete parallel tothe Fitter and rock it back and forth inthe sagittal plane (Fig 4). Next, movethe athlete so that he/she is at a 450 an-gle to the Fitter and rock it on that di-agonal. Repeat on the other diagonal.Progress through the four body posi-tions as in Exercise 3. As the athleteprogresses, decrease the number of re-sistance cords on the Fitter, making theplatform more unstable. Start with onerepetition of 15 seconds and extend tothree to five repetitions of 60 secondseach.
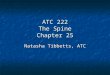
Exercise 6-Ball BalancingHave the athlete balance on his/her
hands on a 48-inch Gymnastikball®(Ledragomma, Italy), first with eyesopen, then closed (Fig 5). Progressfrom both hands on one large ball toeach hand on separate balls and then tothe injured arm on one ball. Also, prog-ress through the four body positions asin Exercise 3. Use a spotter, especiallywhen doing this exercise for the firsttime or changing body positions, sincethe athlete may fall off the Gymnastik-ball®. Start with one repetition of 10seconds and progress to three to fiverepetitions of 60 seconds each.These exercises help redevelop
proprioception in athletes with inju-ries to the upper extremity. The last
Fig 4.-Fitter® balance in push-upposition with platform rocking in thesaggital plane.
Journal of Athletic Training 17
Fig 3.-Eyes open, Fitter® balance in push-up position with platform rocking inthe frontal plane.

"w-f44r
A-01 k,AW .4
Fig 5.-Eyes open, Gymnastikball® balance in feet-elevated position.
three exercises are especially usefulfor athletes who use the upper ex-
tremity in a closed kinetic chain fash-ion and become more challengingthrough the progression from eyes
open to eyes closed and through thevarious body positions.
This paper was funded throughgrants provided by the National Ath-letic Trainers' Association and Bax-ter Healthcare.
References1. Brunt D, Andersen JC, Huntsman B, Reinhert
LB, Thorell AL, Sterling JC. Postural re-
sponses to lateral perturbation in healthy sub-jects and ankle sprain patients. Med Sci SportExerc. 1992;24:171-176.
2. Day RW, Wildermuth BP. Proprioceptivetraining in rehabilitation of lower extremity in-juries. In: Grana WA, Lombardo JA, SharkeyBJ, Stone JA, eds. Advances in Sport Medi-cine and Fitness. Chicago, IL: Year Book;1988:241-257.
3. Derscheid GL, Brown WC. Rehabilitation ofthe ankle. Clin Sports Med. 1985;4:527-544.
4. Dilorenzo CE, Parkes JC, Chmelar RD. Im-portance of shoulder and cervical dysfunctionin etiology and treatment of athletic elbow in-juries. J Orthop Sport Phys Ther. 1990;11:402-409.
5. Griffin JW. Use of proprioceptive stimuli intherapeutic exercise. Phys Ther. 1974;54:1072-1079.
6. Hunter SL. Rehabilitation of ankle injuries.In: Prentice WE, ed. Rehabilitation Tech-
niques in Sports Medicine. St. Louis, MO:Times Mirror/Mosby College Publishing;1990:331-341.
7. Janda DH, Loubert P. A preventive programfocusing on the glenohumeral joint. ClinSports Med. 1991;10:955-971.
8. Karlsson J, Andreasson GO. The effect of ex-
ternal ankle support in chronic lateral anklejoint instability. Am J Sports Med. 1992;20:257-261.
9. Kennedy JC, Alexander IJ, Hayes KC. Nervesupply of the human knee and its functionalimportance. Am J Sports Med. 1982;10:329-335.
10. Kulund DN. The Injured Athlete. Philadel-phia, PA: JB Lippencott; 1982:527-528.
11. Lentell GL, Katzman LL, Walters MR. Therelationship between muscle function and an-kle stability. J Orthop Sport Phys Ther. 1990;11:605-611.
12. Maddalo A, Walter JF. Rehabilitation of footand ankle linkage system. In: Nicholas JA,Hershman EB, eds. The Lower Extremity andSpine in Sports Medicine. St. Louis, MO: TheCV Mosby Company; 1986:560-583.
13. Markey KL. Functional rehabilitation of theanterior cruciate ligament deficient knee.Sports Med. 1991;12:407-417.
14. Markey KL. Rehabilitation of the anterior cru-ciate ligament deficient knee. Clin SportsMed. 1985;4:513-526.
15. Riehl R. Rehabilitation of lower leg injuries.In: Prentice WE, ed. Rehabilitation Tech-niques in Sports Medicine. St Louis, MO:Times Mirror/Mosby College Publishing;1990:316-330.
16. Sage GH. Motor Leaning and Control:A Neu-ropsychologicalApproach. Dubuque, IA: Wm CBrown Publishers; 1984:178-179, 214-217.
17. Schmidt RA. Motor Learning Performance.Champaign, IL: Human Kinetics Books; 1991:47-48.
18. Smith RL, Brunolli J. Shoulder kinesthesia af-ter anterior glenohumeral joint dislocation. JOrthop Sport Phys Ther. 1990;11:507-513.
19. Voss DE, Ionta MK, Myers BJ. Propriocep-tive Neuromuscular Facilitation: Patterns andTechniques. Philadelphia: Harper & Row,Publishers; 1985;302-303.
18 Volume 29 * Number 1 * 1994
--I