Embed Size (px)
Citation preview

Update on pharmacological treatment of heart failure
Aldo Pietro Maggioni, MD, FESC
ANMCO Research Center
Firenze, Italy

Presenter Disclosures
Dr. Maggioni :
• Serving in Committees of studies sponsored by: Amgen, Bayer, Abbott Vascular, Johnson & Johnson, Novartis Pharma AG

Agenda
• Systolic heart failure (NYHA class II-IV)
• treatment options

HF-REF: Drug treatment 2008

HF-REF: Drug treatment 2012 (1)
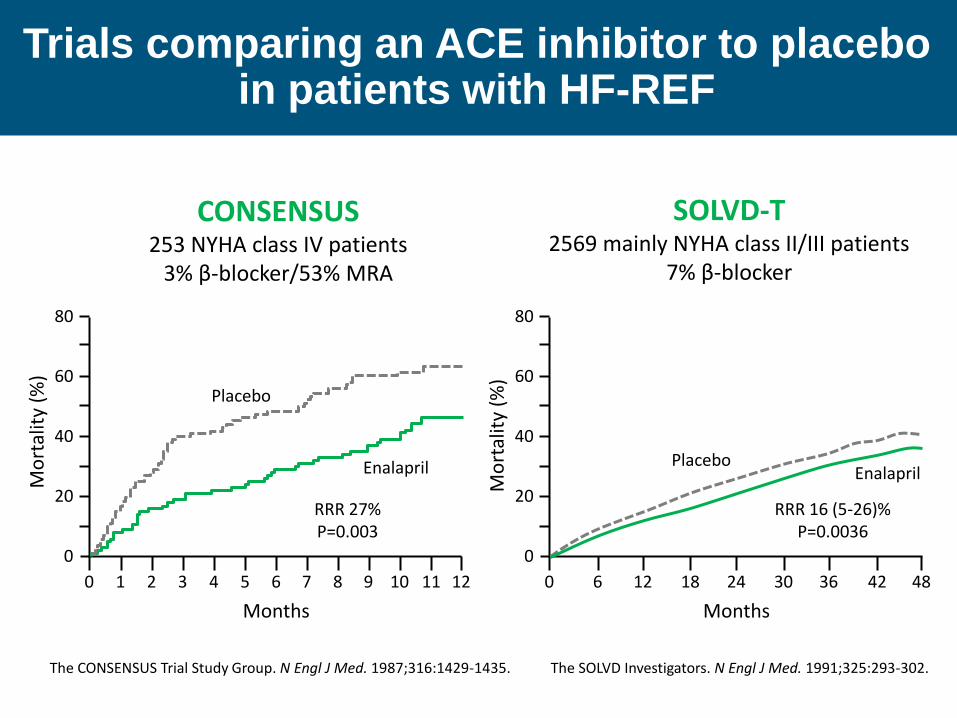
CONSENSUS 253 NYHA class IV patients
3% β-blocker/53% MRA
SOLVD-T 2569 mainly NYHA class II/III patients
7% β-blocker
Placebo
Enalapril
RRR 27% P=0.003
Mo
rtal
ity
(%)
Months
0 1 2 3 4 5 6 7 8 9 10 11 12
20
40
60
80
0
Placebo Enalapril
RRR 16 (5-26)% P=0.0036
Mo
rtal
ity
(%)
Months
0 6 12 18 24 30 36 42 48
20
40
60
80
0
The CONSENSUS Trial Study Group. N Engl J Med. 1987;316:1429-1435. The SOLVD Investigators. N Engl J Med. 1991;325:293-302.
Trials comparing an ACE inhibitor to placebo in patients with HF-REF

Total Sudden
p=0.001 p=0.04
US Carvedilol
(n=1014)
Total Sudden
CIBIS-II
(n=2647)
p=0.0001 p=0.001
Total Sudden
MERIT-HF
(n=3991)
p=0.0001 p=0.0002
3.2% 1.7%
7.8%
3.8%
7.2%
10.8%
3.9%
6.6%
11.8%
17.3%
3.6%
6.3%
Effects on total mortality and sudden
death in patients with HF-REF
Carvedilol Placebo Bisoprolol Metoprolol
US Carv Program. N Engl J Med 1996;334:1349–1355
CIBIS-II. Lancet, 1999; 353:9–13
MERIT-HF. Lancet 1999; 353:2001–2007

RALES 1663 NYHA class III/IV patients
95% ACE-I/10% β-blocker
EMPHASIS-HF 2737 NYHA class II patients
93% ACE-I or ARB/87% β-blocker
RRR (95% CI) 22 (5-36)% P = 0.0139
Eplerenone
Placebo
Placebo
Spironolactone
RRR (95% CI) 30 (18-40)% P < 0.001
Pro
bab
ility
of
surv
ival
Years from randomization 0 1 2 3
0.50
0.70
0.80
0.90
0.00
1.00
0.60 P
rob
abili
ty o
f su
rviv
al
Years from randomization 0 1 2 3
0.50
0.70
0.80
0.90
0.00
1.00
0.60
Pitt B, et al. N Engl J Med. 1999;341:709-717. Zannad F, et al. N Engl J Med. 2010;364:11-21.
Trials comparing an aldosterone/MR antagonist to
placebo (added to an ACE-I and a BB) in HF-REF

Pharmacological treatments indicated in potentially all patients with symptomatic (NYHA class II–IV) HF-REF
AP Maggioni, Belgrade May 19, 2012

Agenda
• Systolic heart failure (NYHA class II-IV)
• treatment options
• other treatments with less-certain benefits

HF-REF Other treatments with less-certain benefits

CHARM-Added and Val-HeFT
0
10
20
30
40
50
CHARM Val-HeFT
Placebo ARB
42.3%
37.9% 29.5%
25.9%
HR 0.85
95% CI 0.75-0.96
P=0.011
HR 0.86
95% CI 0.77-0.95
P=0.004
%
CV death or HF hospitalisation

HF-REF Other treatments with less-certain benefits


HF-REF: Drug treatment 2012 (2)

HF-REF Other treatments with less-certain benefits

HF-REF Other treatments with less-certain benefits
AP Maggioni, Belgrade May 19, 2012

NNT = 56
ARR = 1·8%
adjusted HR (95·5% CI)* p value
0·91 (0·833 – 0·998) 0·041
unadjusted HR (95·5% CI) p value
0·93 (0·852 – 1·021) 0·124
0.4
0.3
0.2
0.1
0.0
0 6 12 18 24 30 36 42 48 54
Pro
ba
bili
ty o
f d
ea
th
Months since randomization
*Cox proportional hazards model adjusted for HF hospitalization in the previous year, prior pacemaker, and aortic stenosis
Pts at risk
n-3
Plac.
3,494
3,481 3,336
3,344 3,215
3,209 3,080
3,083
2,947
2,941
2,844
2,805
2,680
2,631
2,164
2,122
1,588
1,558
844
816
Placebo
1014/3481 (29·1%)
GISSI-HF n-3 PUFA: All-cause Death
n-3 PUFA
955/3494 (27·3%)

Agenda
• Systolic heart failure (NYHA class II-IV)
• treatment options
• other treatments with less-certain benefits
• treatments not recommended
• Statins (neutral results of CORONA and GISSI-HF)
• Renin inhibitors (studies still ongoing)
• Oral anticoagulants other than in patients with AF
• Treatments that may cause harm
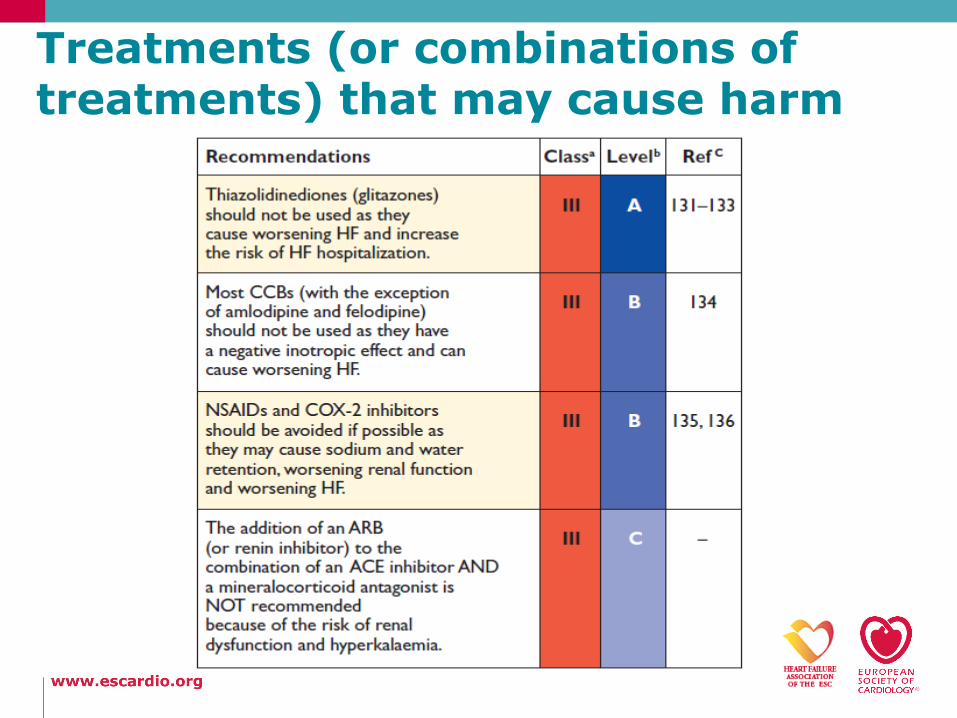
Treatments (or combinations of treatments) that may cause harm
Agenda
• Systolic heart failure (HF-REF)
• treatment options
• other treatments with less-certain benefits
• treatments not recommended
• Preserved ejection fraction (HF-PEF)

Pharmacological treatment of patients with HF-PEF (1)
• No treatment has yet been shown, convincingly, to reduce morbidity and mortality in these patients
• Diuretics are used to control sodium and water retention and relieve breathlessness and oedema
• Adequate treatment of hypertension and myocardial ischaemia is also considered to be important, as is control of the ventricular rate in patients with AF
• The drugs that should be avoided in HF-REF should also be avoided in HF-PEF, with the exception of CCBs

Pharmacological treatment of patients with HF-PEF (2)
• The key mortality–morbidity trials to date are:
Trial n. of
pts Drug Result
CHARM Preserved
3023 Candesartan Neutral
PEP-CHF 850 Perindopril Neutral
I-Preserve 4128 Irbesartan Neutral

Agenda
• Systolic heart failure (HF-REF)
• treatment options
• other treatments with less-certain benefits
• treatments not recommended
• Preserved ejection fraction (HF-PEF)
• Update on pharmacological treatment of co-morbidities

Some new anticoagulants such as the oral direct
thrombin inhibitors and oral factor Xa inhibitors are now
available but they are contraindicated in severe renal
impairment (creatinine clearance <30 mL/min)

Anaemia and iron deficiency
• Anaemia is associated with worse functional status, greater risk of HF hospitalization, and reduced survival
• Correctable causes should be treated in the usual way
• The value of erythropoietin-stimulating agents is unknown but is currently being tested in a large mortality–morbidity RCT (RED-HF)
• Iron deficiency may independently contribute to muscle dysfunction in HF and causes anaemia
• FAIR HF evaluated 459 HF-REF patients (NYHA class II-III), a haemoglobin level 9.5 to 13.5 g/dL, and iron deficiency
• IV iron therapy improved self-reported patient global assessment
• IV iron may be considered as a treatment for these patients
Agenda
• Systolic heart failure (HF-REF)
• treatment options
• other treatments with less-certain benefits
• treatments not recommended
• Preserved ejection fraction (HF-PEF)
• Update on pharmacological treatment of co-morbidities
• Acute HF

Algorithm for management of acute pulmonary
oedema/congestion
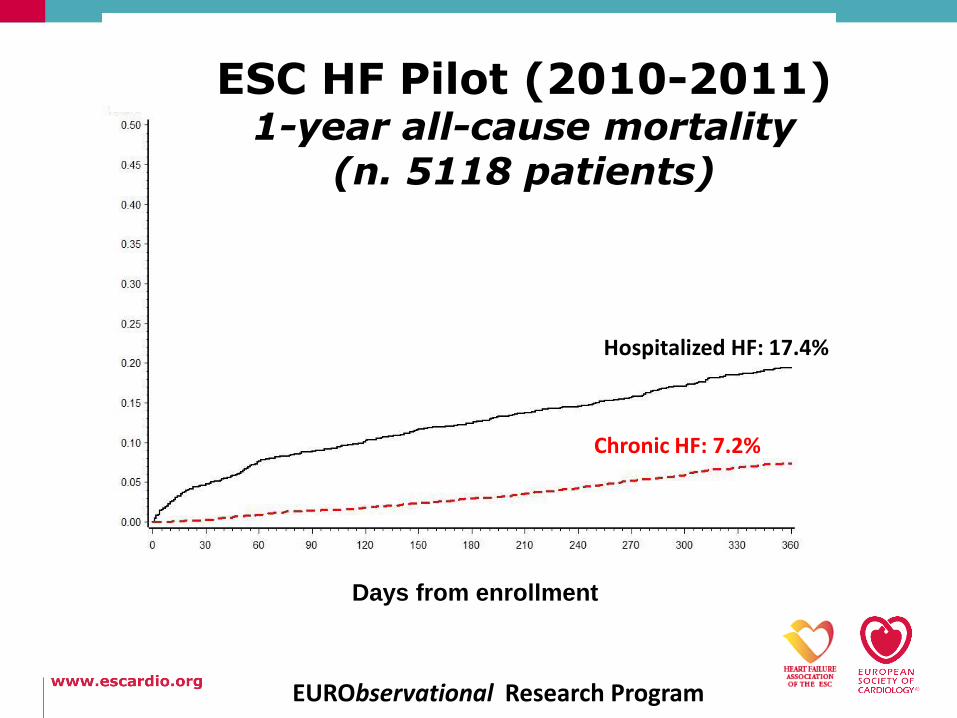
ESC HF Pilot (2010-2011) 1-year all-cause mortality
(n. 5118 patients)
Days from enrollment
Chronic HF: 7.2%
Hospitalized HF: 17.4%
EURObservational Research Program


Initial assessment of patient with suspected acute heart failure





























