Embed Size (px)
Citation preview

University of Groningen
Clinical studies with biological response modifiers in the treatment of solid tumorsButer, Jan
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:1994
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Buter, J. (1994). Clinical studies with biological response modifiers in the treatment of solid tumors.Groningen: s.n.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 10-07-2020

Clinical studies with biological response modifiersin the treatment of solid tumors

RIJKSUNIVERSITEIT GRONINGEN
Clinical studies with biological response modifiersin the treatment of solid tumors
Proefschrift
Ter verkrijging van het doctoraat in de Geneeskunde
aan de Rijksuniversiteit Groningen
op gezag van de Rector Magnificus Dr. F. van der Woudein het openbaar te verdedigen op
woensdag 26 oktober 1994des namiddags te 4.00 uur
door
Jan Buter
geboren op 23 februari 1963
te Schoonebeek

Promotores: Prof. Dr. N.H. MulderProf. Dr. L. F. M. H. de Leij
Co-promotor: Dr. D. Th. Sleijfer

Promotiecommissie: Prof. Dr. T. H. TheProf. Dr. W.D. Reitsma
Prof. Dr. H. J. A. Mensink
ISBN 90-9007563-1
The printing costs were supported by kind contributions of the Stichting Wergroep Interne
Oncologie, Roche Nederland BV and Chiron Benelux BV.
Lay-out : Jan Buter
Druk : Krips Repro, Meppel

Voorwoord
Het in dit proefschrift beschreven onderzoek werd verricht binnen de Werkgroep InterneOncologie van de sectie Algemene Interne Geneeskunde in samenwerking met sectie
Klinische Immunologie (Prof. Dr. T. H. The), Vakgroep Inwendige Geneeskunde, Faculteit
der Geneeskunde van de Rijksuniversiteit Groningen.Mijn promotor Prof. Dr. Nanno Mulder wil ik bedanken voor het initieren en leiding geven
aan het onderzoek. Zijn originele ideeën waren verademend op de momenten dat ze het hardstnodig waren. Dr. Dirk Sleijfer dank ik voor zijn begeleiding en het nauwgezet beoordelen van
de door mij geschreven epistels. Van zijn zeer directe en consequente aanpak van zowel
kliniek als onderzoek heb ik veel geleerd. Prof. Dr. Loe de Leij wil ik bedanken voor desamenwerking en de gastvrijheid die ik binnen zijn onderzoeksgroep de afgelopen jaren heb
mogen genieten. De overige leden van de interne oncologie-staf, Dr. Pax Willemse, Dr.Liesbeth de Vries en Dr. Winette van der Graaf dank ik voor de prettige samenwerking bij
de behandeling van de patienten. De leden van de promotiecommissie, Prof. Dr. T. H. The,
Prof. Dr. W.D. Reitsma en Prof. Dr. H. J. A. Mensink ben ik zeer erkentelijk voor hetbeoordelen van het proefschrift. Dr. Richard Janssen en Drs. Bart-Jan Kroesen hielden tijdens
de verschillende studies de immunologische parameters in het oog en zorgden voor debereiding van de ’bispecifieken’. Dr. W.J. Sluiter van de sectie Endocrinologie was bij
herhaling in staat om ondanks de rook in zijn kamer een helder zicht te geven op de statistiek
van onze gegevens. Willy Bruins-van der Weij en Christien Wijma zorgden ervoor dat demanuscripten niet alleen correct de deur uit gingen maar ook op tijd aankwamen bij de juiste
personen. Jacob Pleiter en Jan Brouwer zorgden voor de figuren en afbeeldingen. Deoncologie verpleegkundigen Bregtje Oosterhuis en Jos Dijkstra en de verpleegkundigen van
gebouw 28 en afdeling B3 dank ik voor de begeleiding van onze patienten. Mijn collega’s Dr.
Bonne Biesma, Dr. Jourik Gietema, Drs. Annemiek Cats, Drs. Mieke van Gameren, Dr. HarmSinnige, Drs. Gerrit-Jan Veldhuis, Drs. Judith Nieken zorgden voor een prettige sfeer zowel
in het ziekenhuis als rond de snookertafel.Mijn kamergenoten Drs. Els Weersink en Drs. Ron Ganzevoort stonden garant voor de vele
zinvolle en minder zinvolle discussies die nog lang de herinnering aan groningen levend
zullen houden.

Contents
Introduction 11
Chapter 1. Clinical use of Interleukin-2 and interferon in
the treatment of solid tumors. A review.
13
Chapter 2. Phase II study of subcutaneous interleukin-2 inunselected patients with advanced renal cell
cancer on an outpatient basis.
J Clin Oncol 1992; 10:1119-1123.
51
Chapter 3. A progress report on the outpatient treatment ofpatients with advanced renal cell carcinoma
using subcutaneous interleukin-2.
Sem of Oncol 1993; 6 (suppl 9): 16-21.
61
Chapter 4. Phase I/II study of low dose intravenous OKT3
and subcutaneous IL-2 in metastatic cancer.
Eur J Cancer 1993; 29A: 2108-2113.
73
Chapter 5. Phase I study of intravenously applied bispecificantibody in renal cell cancer patients receiving
subcutaneous IL-2.
Br J Cancer 1994, in press.
85
Chapter 6. Recombinant interleukin-2 for metastatic renalcell carcinoma in hemodialysis patients.
Eur J Cancer, 28A: 1770-1771, 1992.
109
Chapter 7a. Infection after subcutaneous interleukin-2
Lancet 339: 552, 1992 (letter).
117
Chapter 7b. Neuropsychiatric symptoms during treatment
with interleukin-2
Lancet 341: 628, 1993 (letter).
121
Chapter 8. Fluorouracil/Leucovorin/Interferonα-2a inpatients with advanced colorectal cancer. Effects
of maintenance therapy on remission duration.Submitted
125
9

Chapter 9. Dose escalation of dacarbazine combined with
interferon-alfa, G-CSF and ondansetron inpatients with metastatic melanoma.
Anticancer Res 1994; 14:1325-1328
137
Chapter 10. Summary, conclusions.
Samenvatting en conclusies
147
151
10

Introduction
Recombinant cytokines have been studied for their clinical applicability for two decades now.However, their role in the struggle against solid cancer is only just beginning to emerge.
These proteins are studied for their properties as hematopoietic growth factors, as activators
of the host defence mechanisms, and as modulators of cell behavior to increase tumor cellsusceptibility to chemotherapy. The cytokines used in the last two mentioned modes are also
referred to as biological response modifiers.This thesis attempts to further define some clinical aspects of a hematological growth
factor granulocyte colony stimulating factor (G-CSF) and two biological response modifiers,
interferon-α (IFN) and interleukin-2 (IL-2). These biological agents were studied either aloneor in combination with monoclonal antibodies or chemotherapy to determine their optimal
dose, their activity and side effects in the treatment of patients with disseminated renal cellcancer, melanoma or colorectal cancer.
Chapter 1 gives an overview of the literature on the clinical use of IL-2 and IFN in
the treatment of solid tumors. Chapters 2 and 3 report the results of studies with subcutaneous(sc) IL-2 in patients with renal cell cancer. Chapters 4 and 5 study the addition of monoclonal
antibodies to the IL-2 treatment in attempt to increase and redirect T-cell activation. Chapter6 describes the treatment of two hemodialysis patients with renal cell cancer using sc IL-2.
Two side effects of single-agent sc IL-2, infection and neurotoxicity, are reported in chapter
7. In chapters 8 and 9 the results of two studies are presented using interferon-α incombination with chemotherapy in the treatment of patients with colorectal cancer and
melanoma. Chapter 10 summarizes the results of our studies and briefly reflects on the roleof recombinant cytokines in medical oncology.
11

Chapter 1
Biological response modifiers in medical oncology
A review on the clinical use of Interleukin-2 and Interferon-alfa in the
treatment of solid tumors.
J. Buter, D. Th. Sleijfer, N. H. Mulder
Department of Internal Medicine, Division of Medical Oncology, University Hospital
Groningen
Contents
1 Introduction 15
2 Interleukin-2 15
2.1 Biology 162.1.1 IL-2 receptor 16
2.1.2 Soluble IL-2 receptor 162.1.3 Biological effect on cells 17
2.2 Preclinical studies 172.3 Pharmacokinetics 18
2.4 Clinical spectrum of IL-2 192.5 Markers of clinical response 24
2.6 Tolerabillity 252.6.1 Cardiovascular effects 25
2.6.2 Pulmonary effects 262.6.3 Renal effects 26
2.6.4 Gastrointestinal and hepatic toxicity 262.6.5 Endocrine effects 26
2.6.6 Neurological effects 272.6.7 Dermatological effects 27
2.6.8 Hematological effects 28
13

2.6.9 Infectious complications 282.7 Combination treatment 28
2.8 Conclusions and perspectives 30
3 Interferon 303.1 Biology 31
3.2 Preclinical studies 313.3 Clinical spectrum 31
3.3.1 Renal cell carcinoma 323.3.2 Malignant melanoma 32
3.3.3 Aids related Kaposi’s sarcoma 333.3.4 Colorectal cancer 33
3.3.5 Carcinoid 343.3.6 Ovarian cancer 34
3.3.7 Bladder cancer 353.3.8 Benign Tumors 35
3.4 Tolerabillity 35
3.5 Conclusions and perspectives 36
14

1 Introduction
Biological therapy is referred to as the fourth modality in cancer treatment because it differs
conceptually from surgery, radiation and chemotherapy as it acts not only directly by
attacking the tumor cells but also by stimulating the immune system to mediate the regressionof cancer (1,2). Translating the expanding knowledge of the immune system into biological
therapies has been difficult because of the complexity of the immune system includingcytokines, growth factors, antibodies, oncogenes and their products, and the vast array of
effector and suppressor cells and their receptors. Furthermore, in patients with cancer
cytokines and cytokine receptors are often deregulated and cytokines produced by the tumormay contribute to the pathophysiology of cancer. Early biological treatments were performed
using crude preparations of immunostimulants mostly derived from bacterial products ortumor extracts with usually disappointing results (3). However, the development of recom-
binant DNA and hybridoma techniques has enabled the synthesis of purified proteins capable
of more selective interventions in the immune cascade (4). Since then, intensive research hasbeen devoted to define the therapeutic use of these proteins in the treatment of cancer. In this
review the current state of clinical application of the biological response modifiers Interleukin-2 (IL-2) and Interferon-α (IFN) in the treatment of solid tumors will be discussed.
2 Interleukin-2
The first observations of mitogenic factors in the supernatant of stimulated leucocytes datefrom 1963 (5) but it was not until more than 10 years later that a growth factor for bone
marrow derived T-cells was described by Morgan and coworkers (6). This T-cell growth
factor (TCGF) was renamed Interleukin-2 (IL-2) in 1979 after discovery of its pleiotropiceffects (7). IL-2 is a 15Kd glycoprotein produced by T-helper cells that plays a central role
in the immune response. The human IL-2 gene has been mapped to chromosome 4q (bands
26 to 28). It has been isolated, cloned and expressed inE. Coli (8). The IL-2 gene consistsof four exons separated by introns with strong similarity to the genes of interleukin-4 and the
growth factor granulocyte-macrophage-colony stimulating factor (9). Subsequent to itsproduction IL-2 undergoes a variety of different post-translational steps including cleavage
of a 20 amino acid signal peptide, the addition of a carbohydrate at position 3 (threonine) and
creation of a disulfide bond between cysteines located at positions 58 and 105. This bondguarantees the stability of the tertiary structure which is essential for its biological activity
(10). Although IL-2 is naturally sialylated and glycosylated, the carbohydrate component ap-pears to play no part in the activity of the peptide since non-glycosylated recombinant IL-2
is equally effective at stimulating T-cell proliferation as glycosylated IL-2 (11).
15

2.1 BiologyThe biological effects of IL-2 have been described in detail by Smith (12,13). IL-2 is
produced by T-helper cells upon activation by Interleukin-1 and an antigen. The regulationof IL-2 production is only partly understood. In many cells at least two signals are required
for induction that are mimicked by phorbol ester and calcium ionophore stimulation (14).Presumably this usually involves ligation of the T-cell receptor and co-signaling through a
second cytokine or a receptor pair (CD28-B7) (15,16). Biologic activities of IL-2 are mediated
through both direct interaction with specific receptors on T cells, B cells, natural killer (NK)cells, monocytes, macrophages, and oligodendrocytes and through secondary effects resulting
from the induction of a variety of cytokines.
2.1.1 IL-2 receptorThe IL-2 receptor consists of at least three transmembrane associated units, each with anexternal domain of approximately 215 amino acid residues: a 55kDα chain (IL-2Rα, Tac,
p55), a 70 to 75kDβ chain (IL-2Rß, p70), and a 64kDγ chain (IL-2Rγ, p64) that combinenoncovalently (17-20). Only NK-cells and possiblyγδ T cells constitutively express theβ-
chain (Kd of 10-9 mol/L) in the absence of antigenic stimulation, and these cells are therefore
the immediately IL-2 responsive cell population (21). The biological activity on unstimulatedNK cells is presumably due to interaction of the slow binding intermediate affinityβ/γ dimer
that rapidly leads to upregulation of the fast bindingα chain ( Kd of 10-8 mol/L) to create ahigh-affinity α/β/γ heterotrimer with a Kd of 10-12 mol/L. Interaction of IL-2 with the high-
affinity receptor results in internalization through receptor-mediated endocytosis. The 75 kD
β chain, with the largest cytoplasmic domain of 286 amino residues, and theγ chain areprobably responsible for triggering intracellular biochemical pathways (22). Signal transduc-
tion after receptor binding remains obscure. The IL-2 receptor itself has no known enzymaticactivity. Upon IL-2 interaction with its receptors a variety of intracellular events occur.
Hydrolysis of inositol phosphates and increases in intracellular calcium are coupled with
activation of calcineurin, a calcium/calmodulin-responsive protein phosphatase, activation oftyrosine kinase and ultimately induction of transcriptional regulatory molecules. NK-506 and
cyclosporine appear to block these early events (23).
2.1.2 Soluble IL-2 receptorSoluble forms of the IL-2Rα chain have been identified in the serum of patients withmalignant, autoimmune and allergic disorders, systemic parasitic infections and in patients
undergoing graft versus host disease. Theα chain is thought to be released from the cell-membrane of activated T cells by proteolytic cleavage. The presence of the soluble IL-2Rαis therefore thought to reflect the state of T cell activation in these patients (24). Soluble IL-
2Rα has been found to be increased during IL-2 therapy (25). Some investigators suggest an
16

inhibitory effect of sIL-2Rα, the soluble form competing with the signal transducingmembrane bound receptor for the IL-2 molecules (26). This is however debatable regarding
the different affinities of the receptors for the IL-2 molecule.
2.1.3 Biological effect on cellsThe phenotype of a variety of lymphoid cells proliferating in response to IL-2in vitro appear
to depend on the concentration of IL-2 and the duration of culture. At relative lowconcentrations IL-2 is able to induce cytolytic activity in MHC-restricted, antigen specific T
lymphocytes (CTL) after 6-7 days. These CTL express CD3, CD8, CD10 and CD16 surfaceantigens. Natural killer (NK) cells exhibit a broad range of MHC-nonrestricted cytotoxic
responses when exposed to IL-2 after 2 to 3 days. NK cells comprise 2-5% of the peripheral
blood mononuclear cells and these cells may express CD2, CD3, CD7, CD8, CD11, CD16,CD35 and CD56 surface antigens. When incubated with higher concentrations of IL-2, resting
peripheral blood large granular lymphocytes, T lymphocytes and possible even B lymphocytesbecome capable of non-specific lysis of fresh cancer cells but not normal cells after 5 to 10
days in short-term assays. This was named the Lymphokine Activated Killer (LAK) cell
phenomenon (27). Lymphocytes expressing LAK activity may express CD2, CD3, CD5, CD6,CD7, CD8, CD11, CD16, CD45 and CD57 surface antigens (28,29). Lymphocytes infiltrating
a tumor are frequently found in surgically removed tumors. These cells can be selectivelyexpanded to large numbers from tumor cell suspensions using IL-2. These tumor infiltrated
lymphocytes (TIL) are generally of the CD3 CD8 positive phenotype and have been reported
to show specific MHC-restricted killing (30). Upon stimulation by IL-2 several secondarycytokines are induced. NK-cells produce IFN-γ, GM-CSF and TNF-α and -β (31). Monocytes
release large amounts of IL-1, IL-6, and TNF-α when stimulated by cytokines in conjunctionwith bacterial agonists (32,33). In vivo IL-2 treatment induces the production of several
growth factors including IL-5, GM-CSF, M-CSF and IL-6 (34).
2.2 Preclinical studiesIn murine models, repeated systemic administration of high doses IL-2 induced LAK-cytotoxicity in vivo and resulted in significant antitumor responses in disseminated murine
leukemia, as well as in fibrosarcoma and melanoma metastases (35-37). The intravenous ad-
ministration of in vitro activated LAK-cells in combination with IL-2 induced also a sig-nificant reduction in the number and size of murine pulmonary and hepatic metastases
(38-40). These effects were dependent on the dose and schedule of IL-2 administered (41-45),the number of LAK-cells infused (36,38,40) and on the extend of the tumor burden (36,46).
Tumor inhibition has also been observed with low doses of IL-2 (43,47). Established 10-day
metastases but not 3-day metastases were sensitive to low dose IL-2 (43). Athymic nude micefailed the low dose IL-2 treatment while they were responsive to high dose IL-2, suggesting
that the antitumor activity of low dose IL-2 was T cell mediated (47). Local intratumoral
17

injections with low doses of IL-2 could cure mice bearing a large burden of metastatic tumor(48,49). How an effective antitumor response in vivo is orchestrated using these different
mechanisms is poorly understood. Despite the direct cytotoxicity of LAK cells against tumor
cells in vitro, in vivo studies have shown that LAK cells do not selectively localize to tumorsites. In a rat model, systemically infused labeled-LAK cells migrated first to the lung and
subsequently to the liver and spleen in a 2 to 6 hours period. No difference in the distributionpattern was observed between normal and tumor bearing animals (50). Adoptively
administered TIL cells have been shown to travel to metastatic sites in clinical imaging
studies (30,51,52). Lymphocytes infiltrating renal cell carcinoma or lung carcinoma, however,have been shown to be functionally impaired, possibly due to tumor-derived
immunosuppressive factors (53,54). Interestingly, lymphocytes of tumor bearing mice havebeen found to have structurally altered CD3-TCR complexes, including the loss of the signal-
transducing CD3-ζ chain (55). If these findings also apply to human lymphocytes, this may
have important consequences for future immunotherapy studies.
2.3 PharmacokineticsUnder physiological conditions IL-2 is thought to act in an autocrine and paracrine way in
localized areas of inflammation with no detectable levels in the circulation. Pharmacokinetics
of exogenous administered IL-2 have been studied in rodents and in humans. The differentmutated recombinant proteins of IL-2 do not differ significantly in their pharmacological
properties and they will not be discussed separately. After intravenous administration, IL-2is rapidly distributed to the extravascular, extracellular space. Approximately 30% of the
administered dose initially distributes over the plasma volume. After high peak levels, serum
concentrations decrease with an alfa and beta half-life of 13 minutes and 2 hours, respectively(56). With a clearance rate of approximately 120 ml/min, the kidneys appear to be the main
site of clearance where IL-2 is probably metabolized by the proximal renal tubules, asminimal levels of active IL-2 are found in the urine (56,57). During 24-hour infusion serum
IL-2 concentrations appear to reach a steady state after 2 to 6 hours (56,58). The hydrophobic
nature of IL-2 necessitates formulation with albumin or a detergent to maintain solubility (59).At slow infusion rates and low concentrations the bioavailabillity of some IL-2 muteins may
be reduced due to adherence to the infusion material (60). After subcutaneous bolus injectionIL-2 serum concentrations rise slowly, reaching a maximum concentration after 3 to 4 hours.
The serum levels decline slowly with prolonged mean half-lives of 4 to 5 hours (58).
Intraperitoneal infusion of IL-2 results in long half-life times with medians of 22 and 6.3hours in peritoneal fluid and serum respectively. The serum concentrations seem to reflect the
efflux from the peritoneal cavity (56). Other routes of administration of IL-2 includeinhalation (61) and regional injection of IL-2 (62). No pharmacological data on these routes
are available. Modifications of IL-2 with monomethoxy-polyethylene-glycol (PEG-IL-
2)(63,64) or a collagen matrix (65) alters its pharmacokinetics properties resulting in a
18

prolonged serum half life time.
2.4 Clinical spectrum of IL-2In contrast to the broad spectrum of activity in pre-clinical models, IL-2 has in clinicaloncology emerged as a treatment for renal cell cancer almost exclusively. The overall
response in this tumor is around 20% and this is not different from the remission rate inpatients with melanoma. Probably the acceptance of IL-2 as a treatment of renal cell cancer
is dictated also by the lack of active alternatives in that tumor (although as is discussed later,
activity of interferon is at least quantitatively not very different). In melanoma dacarbazine(DTIC) has the same response rate as IL-2 but since the introduction of 5-HT3-receptor
antagonistic anti-emetics this treatment is less toxic. Alternatives for IL-2, in the sense ofequally (in)effectivity exist in all tumors other than renal cell cancer. However occasional
responses have been described for IL-2 in a broad spectrum of tumors. Colorectal
adenocarcinoma for instance is relatively insensitive to IL-2 based immunotherapy. In theNational Cancer Institute trials 5 out of 30 patients responded to IL-2/LAK treatment while
no responses were observed in 12 patients treated with IL-2 alone (66). In a review of 15trials with IL-2 containing trials, the National Biotherapy Group reported only one partial
response among 76 patients treated (67). In patients with ovarian cancer with disease confined
to the abdomen, intraperitoneal administration of IL-2 or LAK cells have been used withreported response rates of 20%. Intraperitoneal fibrosis and abdominal pain were dose limiting
factors in this approach (68,69). In patients with bladder cancer, intravesical instillation ofhigh dose IL-2 produced almost no toxicity. One complete response lasting more than 6
months was observed in a small group of 5 patients (70). In patients with lung cancer, a
response rate of 16% was reported by the National Biotherapy Study Group, but most of theseresponses could be attributed to the concomitant treatment with etoposide or cisplatin (67).
Clamon et al. reported a response rate of 21% in a phase II trial with continuous infusion IL-2in patients with extensive small cell lung cancer who failed first line combination
chemotherapy with cisplatinum, doxorubicin, cyclophosphamide and etoposide. Complete
responses were observed in 17% of patients, but toxicity, especially pulmonary toxicity, wasconsiderable, requiring discontinuation of treatment in 46% of patients (71). In patients with
non-Hodgkin lymphoma, early trials showed promising results mainly with IL2/LAKtreatment with reported response rates up to 40% but this has not been confirmed by other
trials. Small patient numbers and conflicting results preclude any conclusions about the role
of IL-2 in the treatment of non-Hodgkin lymphoma (66).In conclusion, the actual activity spectrum of IL-2 in human tumors may not differ that
much from the earlier experience with this drug in model systems. Its clinical use isinfluenced primarily by the alternatives in therapy and especially by the IL-2 related toxicity
(and possibly economic considerations). The concept that there is a relation between
"immunogeneity" of tumors and IL-2 activity is challenging but needs substantiating. Despite
19

considerable clinical experience with the use of IL-2 in the treatment of patients with cancer,several important issues still remain unresolved. This review will address some of these key
questions; 1) Is there a relation between tumor response and route of administration? 2) Is
there a dose response relation for IL-2? 3) Does the addition of adoptively administered LAKor TIL cell increase response rate? 4) Does IL-2 based immunotherapy have an effect on
survival?
Effect of route of administration on responseMost patients are treated systemically by the intravenous or subcutaneous route. Intravenous
therapy, given either as bolus injections or as a continuous infusion is associated withconsiderable dose dependent toxicity which necessitates special care for patients treated.
Subcutaneous administration produces local toxicity at the injection sites that can be
inconvenient, but the systemic toxicity with the vascular leak syndrome is rarely observed.No randomized experiences concerning efficacy are available between subcutaneous and
intravenous IL-2 treatment. However, in view of the range of activity of IL-2 given eitherway, a difference in response rate, if present, will be limited to 5%. Also the incidence of
complete remissions after both administrations is limited to a narrow range. So differences
in effects of the two routes of administration if present will be found in the duration ofresponse and the quality of life of non-responders. If eventually comparative studies are going
to be done, these questions will have to be addressed.IL-2 has also been administered regionally by several other routes including
intraperitoneal (69,72,73), intravesical (70), intrapleural (74), intraspinal (75), intralymphatic
(76), extracorporal perfusion (77), arterial perfusion of the liver or spleen (78,79), local slowdelivery pellets into the tumor (65), and by inhalation (61). Toxicity of these regional
applications were mostly less than with intravenous administration, but patient numbers areto small to draw conclusions about the clinical efficacy of these routes of administration.
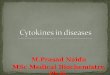
Legend to figure 1. Response rates with 95% confidence intervals of IL2 monotherapy studies inpatients with metastatic renal cell carcinoma. The dashed line expresses the mean, the box the 95%confidence interval of the cumulative response of all patients included.
Legend to figure 2. Response rates with 95% confidence intervals of IL2 monotherapy studies inpatients with metastatic melanoma.The dashed line expresses the mean, the box the 95% confidenceinterval of the cumulative response of all patients included.
20


Effect of dose and treatment regimen on antitumor efficacyIn a randomized phase II trial comparing intravenous high-dose IL-2 bolus injections with
24-hour continuous infusion at equivalent toxic doses in the treatment of patients with renalcell carcinoma, no difference was shown in antitumor activity (80). No comparative studies
on the dose-response relationship of IL-2 among humans have been reported but numerousphase II studies have been performed using different doses and treatment regimens. Taking
into account the limitations of comparing results between different phase II trials, acomparison of the impact of dose on clinical results in patients with renal cell cancer and
melanoma is presented here (Fig. 1 to 4) To prevent the bias of small studies, a selection hasbeen made, including only those trials with more than 20 patients. In figures 1 and 2 the
response of several trials with the 95% confidence intervals is shown for patients with RCCand melanoma, respectively. In an attempt to compare different treatment schedules, the IL-2
dose is expressed as dose intensity (DI), defined as the dose of IL-2 administered in the firstseven days of treatment. Figures 3 and 4 show the response rates in patients with renal cell
cancer (66,80-104) or melanoma (66,88,89,101a,105-111). We conclude that no dose responserelation is observed in either renal cell cancer or melanoma patients. IL-2 induces an objectiveresponse rate of 18% (14%-19%, 95% confidence interval) of the patients with renal cell
cancer; in approximately 6% these responses are complete. In melanoma response rates of15% (11%-19%, 95% confidence interval) are observed with complete responses in less than
5%. In both groups response duration in patients with a complete response can be durablewith some of the patients remaining free of disease for more than 2 years.
Adoptive immunotherapyWe conclude (Figs. 3 and 4) that the considerable logistic burden of LAK acquisition is nottranslated into improved results. In a overview on 15 different phase II protocols with
inpatient IL-2 treatment, the National Biotherapy Study Group reported a higher response ratein the protocols involving adoptive immunotherapy than in those without in vitro activated
cells (15% versus 7%, respectively, p=0.003), but without any effect on survival (67). Inanother analysis of 327 patients treated in 5 different protocols Palmer, using multivariant
analysis, could not observe any difference in objective response nor in survival when hecompared treatment with IL-2 alone or in conjunction with LAK-cells (97). In three
prospective randomized controlled trials, the addition of LAK-cell treatment to continuousinfusion or high-dose bolus injection IL-2 in melanoma and renal cell cancer patients had no
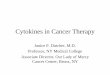
Legend to figure 3. Dose intensity/response relation of IL-2 with or without adoptive immunotherapyin patients with metastatic renal cell carcinoma. Open points ( ), IL2 monotherapy ; solid points ( ) IL2+ adoptive immunotherapy.Legend to figure 4. Dose intensity/response relation of IL-2 with or without adoptive immunotherapyin patients with metastatic melanoma. Open points ( ), IL2 monotherapy ; solid points ( ) IL2 +adoptive immunotherapy.
22


effect on response rate or on survival (80,101,112). One study among melanoma patientsreported a correlation between the number of TIL-cells infused and the clinical response, with
responding patients receiving significantly more TIL’s than non-responders (113).Rosenberg reported initially a response rate of 50% in patients with melanoma (114) but these
results could not be confirmed in other studies. Dillman could raise TIL’s in only 21 out of82 patients with melanoma, and he reported responses in 5 out 21 patients (24%, 10% - 49%,
95% confidence interval) (115). Bukowski was able to raise TIL’s in 18 of 25 eligible patientswith renal cell carcinoma, but no responses were observed (116). Baars et al also observed
no responses in 4 patients with melanoma (117). The treatment with TIL’s is possible in onlya minority of patients, it is technically difficult, costly, and the clinical results are not superior
to those with other IL-2 based regimens.
Effect on survivalThe effect of IL-2 treatment on survival remains unclear. Randomized trials comparing
patients treated with IL-2 with control patients that could answer this issue are not availableand ethical considerations limit the institution of these trials. Retrospective studies are limited
by the influence of patient selection and changes in diagnostic procedures over time
(118,119). In historical control groups the median survival of patients with metastatic renalcell carcinoma was 8 months (120). In an analysis of a cumulated single center experience
in 181 patients with RCC who were candidate for IL-2 therapy, median survival afteroccurrence of metastases was 16 months in all patients irrespective of treatment with IL-2
(intention to treat). Comparison of this survival with a historical control group from the same
institution was however impaired due to the lack of information on two important prognosticfactors being weight loss and performance status in the control group. The relative high
median survival of this group may reflect the difference in diagnostic procedures over timewith the availability of a new treatment modality (121). Given the small numbers of
responders in all series the effect of IL-2 therapy on survival is influenced by especially
patients with stable disease and possibly also by non-responders.
2.5 Markers of clinical responseOnly a minority of patients respond to IL-2 based immunotherapy, while toxicity occurs in
all. Therefore, several investigators have looked for markers that could predict or monitor
clinical response. Despite intensive research, no consistent relationship betweenimmunological changes and clinical response has been found (97,101). Several factors have
been partially related to treatment efficacy. These include the number of pretreatmentlymphocytes, the number of eosinocphils, the expression of CD56 on NK-cells, sustained
serum levels of TNF, high levels of soluble CD8 and low pretreatment C-reactive protein
(CRP) serum levels (122-128). Elevated levels of IL-6 before IL-2 treatment were associatedwith disease progression after therapy and shorter survival (129). Previous chemotherapeutic
24

treatments had a negative effect on clinical response in patients with renal cell carcinoma(130) but not in melanoma patients (113). Among melanoma patients HLA Class I phenotypes
were correlated with response to IL-2 based immunotherapy. Responding patients had a
significantly higher frequency of the alleles A11 and A19 than the overall melanoma patientpopulation (113). High numbers of CD8bright and CD56-cells that express the HLA-DR
activation marker were found to be prognostic for a good therapeutic response tosubcutaneous IL-2 treatment (123). As to the localization of responses, most responses are
observed in the lung or soft tissues, while few responses are observed in the primary tumor
or bone lesions.
2.6 TolerabillityBecause of a dose relationship observed in animal studies the initial clinical studies were
performed with high dose bolus injections of IL-2 (37,38,40,131,132). High dose treatmentis associated with severe toxicity for which intensive care support is necessary in an number
of patients. IL-2 therapy is accompanied by considerable side effects, including fever, chills,nausea, vomiting, skin toxicity, hepatic and renal dysfunction, mental status changes, and
respiratory failure. The most frequent dose limiting side effect of high dose intravenous IL-2
is hypotension. Frequency and severity of IL-2 toxicity is dose-related and schedule-dependent. High dose intravenous regimens require intensive treatment care monitoring and
patient selection. Most adverse reactions are self limiting and are usually reversible within 2to 3 days after discontinuation of therapy. The mechanisms of IL-2 induced toxicity are partly
understood. The release of secondary cytokines such as IFN-γ and TNF-α are thought to be
important mediators of toxicity (133,134). Passive immunization against TNF-α could indeedpartially abrogate IL-2 toxicity (135). More recently, the role of cytokine induced nitric oxide
has been proposed as a central factor in IL-2 induced hypotension (134). The L-alanine analogNG-methyl-L-arginine has been used in patients with renal cell cancer in order to reduce nitric
oxide production to suppress IL-2 toxicity (136). Since the effector mechanism of IL-2
therapy in vivo is not defined care has to be taken with these approaches not to suppress theantitumor effects of IL-2 as well.
2.6.1 Cardiovascular effectsSeveral cardiac side effects have been observed during IL-2 therapy including arrhythmias,
ischemia, myocarditis, hypocontractility and pericardial effusions (66,137-140).Supraventricular arrhythmias, particularly supraventricular tachycardia and atrial fibrillation,
occur in 10% or more of the patients treated with intensive regimes and generally resolveafter discontinuation of IL-2 (138). In patients over 65 years of age who were treated with
intravenous IL-2, cardiac side effects, especially arrhythmias were the most important dose
limiting toxicities (96). Angina and myocardial infarction have been observed by several
25

investigators in patients treated with IL-2. In large series ischemia occurred in 3% to 9% ofpatients and myocardial infarction in 1 to 4% (3,139,141). The frequency of these toxicities
depend on patient selection and treatment regimen. ECG changes, CPK-MB band elevations,
with or without chest pain have been described that may not represent infarction or ischemiabut rather an IL-2 induced, nonischaemic myocardial injury or myocarditis (142).
Hemodynamic changes after IL-2 administration resemble those observed in early septicshock. Shortly after IL-2 administration, a fall in mean arterial pressure resulting from the
decreased systemic vascular resistance induced by IL-2 is observed, which is countered by
an increase in heart rate and cardiac output (140,143). Subsequently, the development of a’vascular leak syndrome’ (VLS) leads to extravasation of fluid and albumin from the
intravascular space, resulting in edema and extravascular fluid accumulation which may leadto or exacerbate pleural effusions and ascites. These effects may be due to a variety of
lymphokines induced by IL-2 such as interferon-γ and tumor necrosis factor-α. Nitric oxide
produced by macrophages and endothelial cells might play a role in the induction ofhypotension during treatment with IL-2 (134,144).
2.6.2 Pulmonary effectsPulmonary congestion, interstitial oedema, dyspnoea and pleural effusions are common results
of the VLS (66,82,137,138). In high dose regimens, approximately 20% of the patientsdevelop respiratory distress and 5- 10% require intubation and mechanical ventilation
(66,137,138). Reversible bronchospasm has been observed in patients undergoing IL-2therapy.
2.6.3 Renal effectsRenal dysfunction is one of the major complications of IL-2 therapy. Azotemia, oliguria,
elevated plasma aldosterone and renin activity with low fractional sodium excretion andincreased serum creatinine levels are found in more than 60% of patients. Prerenal
mechanisms with impaired renal perfusion due to the reduced cardiac function, peripheral
vascular dilatation and intravascular volume depletion are thought to be the cause of theseabnormalities in renal function (145). An additional intrarenal defect has been postulated
(146). Most nephrotoxicities are transient and tend to resolve after cessation of treatment,although in some patients recovery may be prolonged or incomplete (147,148). Administration
of non-steroidal anti-inflammatory drugs can contribute to the impairment of renal function
(81).
2.6.4 Gastrointestinal and hepatic toxicityNausea and vomiting, stomatitis, peptic ulceration, anorexia and diarrhea are frequently
observed during IL-2 therapy. Rarely, bowel hemorrhage, perforation, infarction and
exacerbation of Crohn’s disease have been reported (149-151). Elevated values of liver
26

enzymes are frequently observed. Intravenous IL-2 treatment related reversible intrahepaticcholestase with elevated billirubin levels has been described in a number of patients (152).
2.6.5 Endocrine effectsThyroid dysfunction is reported by several investigators, with a frequency ranging from 20-90
percent of patients treated with IL-2. Initially LAK cells appeared to be essential for thedevelopment of hypothyroidism (153), but in later studies thyroid dysfunction has also been
reported after treatment with single agent IL-2 (154), IFN (155), or combinations of IL-2 and
IFN (156-159). Primary hypothyroidism, hyperthyroidism as well as biphasic dysfunction withhyperthyroidism followed by hypothyroidism have been reported. Thyroid dysfunction has
been found to correlate with treatment duration (160), cumulative dose of IL-2 (161) and afavorable tumor response to treatment (161,162). However, in another study no relation
between response and thyroid dysfunction was observed (160). The pathogenesis of
hypothyroidism is probably multifactorial. Because of elevated anti-thyroglobulin antibodyand anti-microsomal antibody titers, autoimmunity has been implicated as a mechanism for
thyroid dysfunction. However, in most studies the presence of auto-antibodies did notcorrelate with hypothyroidism.
Increased hormone levels of beta-endorphin, adrenocorticotropic hormone (ACTH),
and cortisol have been reported after intravenous IL-2 administration given as a bolus orconstant infusion. The effect of IL-2 was not altered by the concomitant administration of
LAK cells. Increased hormonal stimulation occurred upon re-exposure to IL-2 (163).Melatonin levels were found to be significantly decreased during IL-2 infusion. The IL-2-
induced effects on cortisol, beta-endorphin and melatonin levels resulted in a complete
abolition of their physiological circadian rhythm (164). Endocrine effects of subcutaneousIL-2 therapy were found to be similar to those observed with intravenous administration
(165).
2.6.6 Neurological effectsNeuropsychiatric changes are frequently observed during IL-2 therapy. On intensive treatmentregimens, patients become frequently agitated, combative, and disoriented, or somnolent and
occasionally comatose (66,82,137). These symptoms may progress even in the first days aftercessation of IL-2 therapy (166). Increased brain water content of both grey and white matter
in patients receiving intravenous IL-2 therapy have been observed using magnetic resonance
imaging (167). Perivascular demyelinization was observed on autopsy in a patient with amalignant melanoma who developed neurological symptoms (ataxia, visual disturbances) and
subsequently died after receiving IL-2 therapy (168). Hyperesthesia and paresthesia have beenobserved in patients on IL-2 therapy. Transient ischemic attacks and cerebrovascular accidents
have occurred during IL-2 administration (137).
27

2.6.7 Dermatological effectsCutaneous toxicities include macular erythema, pruritus, and general erythrodermia with dry
desquamation, especially of palms and soles, affecting almost all patients treated with the high
dose regimens and approximately half of the patients at the intermediate dose regimens. Theerythema resolves within 48 hours but the desquamation can last for several weeks. Sporadic
erythema nodosum, angioneurotic edema, lobular panniculitis, urticaria, fatal pemphigus andlife threatening bullous skin lesions have been observed (169-173). Subcutaneous
administration of IL-2 caused transient inflammation at the injection sites, and nodular lesions
resembling subcutaneous lipomas, that gradually disappeared within 6 months. Concomitantuse of anticoagulant therapy can cause sometimes local hemorrhage at the injection sites
(174). Exacerbations of pre-existing psoriasis and polymyositis/dermatomyositis have beenreported after intravenous IL-2 therapy (137,175).
2.6.8 Hematological effectsEosinophilia, probably due to an increase in IL-5 levels (176); early transient lymphopenia
and rebound lymphocytosis are observed in all patients. Thrombocytopenia is frequentlyreported as a clinical important toxic side effect of intravenous IL-2 therapy.
Thrombocytopenia was found to be directly related to IL-2 dose and indirectly to renal
function. A peripheral clearing mechanism triggered by the IL-2 dependent release of aleucocyte-produced eicosanoid that initiates platelet degranulation and clearing by the
reticuloendothelial system is hypothesized (177). Using a cDNA-polymerase chain reaction(PCR) with specific primer sets for the various colony stimulating factors, Schaafsma et al
showed that IL-2 treatment induced the expression of mRNA for M-CSF, GM-CSF, IL-3, and
IL-5, but not for G-CSF, in peripheral blood monocuclear cells. Furthermore no IFN-γ orTNF was detected in plasma (34).
2.6.9 Infectious complicationsIL-2 therapy is complicated by development of bacterial infections in approximately 23% of
the patients.Staphylococcus Aureusis the most commonly isolated organism (178-180).Bacterial sepsis is one of the major causes of death related to IL-2 therapy, and is frequently
catheter related. Prophylactic use of antibiotics before the placement of central venous
catheters markedly reduces the incidence of infection to approximately 7% (181).Subcutaneous administration may also limit the incidence of infection, although inflammation
at the injection site is frequently observed (174,182). Reversible impaired neutrophilchemotaxis during IL-2 therapy has been reported that may contribute to the development of
infection (183) These effects may be due to secondary release of TNF since concomitant use
of dexamethasone both decreases IL-2 induced release of TNF and almost completelyabrogates the chemotactic defect (184).
28

2.7 Combination treatmentIL-2 based immunotherapy has been investigated in combination with a number of other
molecules including interferons (156,185-187), TNF (188-190), cytokines (26,191) and
cytotoxic agents (192-196) to increase response rates or to reduce toxicity.
IL-2 and interferonSynergistic activity of IL-2 and IFN-α has been suggested in preclinical studies (197,198),
because interferon induces upregulation of MHC-molecules on tumor cells (199,200). In
several phase I/II studies the activity of this combination was shown (156,185-187). Howeverin 3 randomized controlled trials comparing IL-2 alone or combined with IFN-α no
differences in immune parameters, nor antitumor activity were observed (100,111,201). Inrenal cell cancer the IFN/IL- 2 combination induced response rates of 4 to 42%, with an
average response rate of all patients of 18% and complete responses occurring in 5%
(67,100,112,130,185,202-213) In melanoma response rates of 4 to 59% are reported with anaverage response rate of all included patients of 29% and CR occurring in 7%
(111,196,214-216).
IL-2 and other cytokinesCombination of IL-2 and TNF resulted in synergistic activity in generating LAK-cells (217),enhanced activation of peritoneal macrophages (218), and antitumor activity in murine models
against sarcoma cells (189). Clinical results were reported by Rosenberg and Dillman withresponses only in patients with melanoma and renal cell carcinoma. The response rates in
these trials were not different from that expected from the use of IL-2 alone (66,67). In a
phase I trial with low dose IL-2 and TNF in patients with non small cell lung cancer, TNFshowed a four fold lower MTD compared to the single-agent use of TNF with
thrombocytopenia as dose limiting factor. One partial response was observed in 12 evaluablepatients (188).
IL-3 and the pineal hormone melatonin (MLT) inhibited neopterin release and
significantly decreased IL-2 induced sIL-2R secretion when given in combination with IL-2(191). The increase in soluble IL-2 receptor (sIL-2R) and neopterin levels were related to the
generation of macrophage-mediated immunosuppression and these were associated with areduced clinical efficacy during IL-2 therapy. In a phase II study with combined s.c. IL-2 and
i.v. IL-3 treatment the increase in serum neopterin, serum sIL-2R and serum cortisol were
neutralized by IL-3. Toxicity was decreased in the IL-3/IL-2 combination compared withtreatment with IL-2 alone. One out of six patients treated with the IL-2/IL-3 combination had
a partial response of a lung adenocarcinoma with a response duration of 7+ months (26).
IL-2 and chemotherapyThe combination of IL-2 based immunotherapy with chemotherapy has been studied in several
29

trials. In early studies low doses of cyclophosphamide have been used in an attempt to reduceimmunosuppressive cell populations during IL-2 therapy without improving response rates
(192,193). Sequential combination of IL-2/LAK immunotherapy with DTIC in melanoma
patients resulted in a response rate of 26% (194). In two recent studies in melanoma patientspromising results have been reported with sequential combined chemoimmunotherapy
consisting of IL-2/IFN with CDDP(195) or CDDP, BCNU and DTIC resulting in responserates of 54 and 57%, respectively (196).
2.8 Conclusions and perspectivesClearly the early promise of IL-2 as a major breakthrough in cancer treatment has not beenfulfilled. Nevertheless IL-2 has permitted the conclusion that tumors in patients can regress
as a result of the immune response from that patient. This confirmation of the applicability
of the immune response in the setting of advanced cancer should form the basis for furtherstudies. What directions should these studies take? In our opinion not much is to be gained
by further analysis of modifications in dose or schedule. Also the impact of reducing toxicitywill be marginal. The addition of other drugs to IL-2 does not seem to be promising although
occasional observations such as the results of the combination IL-2, IFN and platinum in
patients with melanoma are provocative (195). If such observations are reproducible theymight lead to the direction of changes brought about by cytotoxic drugs, presumably
membrane changes, that makes these cells more easily recognizable for activated lymphocytes.A systematic approach into the problem of non-responders to IL-2 should start with analyzing
the mechanism for resistance. This could stem from a general lack of stimulation of the
immune system, however, this seems not likely as with present day techniques no differencescan be found between cell populations in responders and non-responders. If the relevant cells
are present in the circulation, the problem may be for them to reach the tumor. This is notunlikely as homing experiments fail to demonstrate selective penetration of LAK cells into
the tumor. The fact that TIL cells do home, suggests that these cells have some memory of
their past migration pattern. Analysis of this pattern might solve some of the problems.However in clinical practice, at least during subcutaneous treatment a pattern of mixed
response is often seen; some lesions grow, others remain stable or diminish. This suggestsclonal differences in the metastases with regard to recognition by LAK cells. Retargetting of
LAK cells to a more common antigen may deal with this problem. Another way would be to
trigger tumor cells to express recognizable antigens, this will probably require the applicationof gene transfer techniques into clinical oncology.
3 Interferon
The use of the interferons in solid tumors has been reviewed by several investigators
30

(4,219-222). Originally they were described as antiviral factors (223), but after discovery oftheir antiproliferative and immune modulatory activities, partly purified human leucocyte
derived interferon (IFN) was investigated as a potential anticancer agent. Numerous clinical
trials started after highly purified interferons produced by recombinant DNA-technologybecame available. Today, interferon is used in the treatment of several hematologic
malignancies as well as in patients with solid tumors. In this review the role of IFN-α in thetreatment of solid tumors will be discussed.
3.1 BiologyInterferons are a family of more than 20 proteins which are produced by different cell types
under specific activating conditions. Type I IFNs are synthesized in response to viralinfections or following exposure to B-cell mitogens, foreign cells or tumor cells. Lymphocytes
produce primarily IFN-α, whereas IFN-β is produced by fibroblasts. The originally termed
IFN-β2, now renamed interleukin-6, will not be discussed here. Type II IFN, IFN-γ isproduced by antigen- or mitogen-activated T lymphocytes. A new interferon family, IFN-ω,
has been distinguished from other interferons (224). The genes for IFN-α, IFN-β and IFN-ωhave been found on chromosome 9 and the one for IFN-γ on chromosome 12. There are 23
IFN-α genes (8 pseudogenes) encoding acid-stable peptides of 18-20 kD. Only one single
gene for IFN-β has been identified encoding 166 amino acids. IFN-β is an acid stableglycoprotein of 23 kD. For IFN-γ a single gene encoding for a protein of 144 amino acids
has been identified. There are two active forms of IFN-γ: glycosilated proteins of 20 kD and25 kD. The genes for theα, β andγ interferones have been cloned and expressed in bacterial
systems. Interferons bind specifically to receptors on the target cell membrane. IFN-α and
IFN-β share the same receptor, found on the surface of most cells. The gene for the receptorfor IFN-α and -β has been found on chromosome 21 while chromosome 6 encodes for the
IFN-γ receptor (225,226). The IFN-γ receptor is found on T-cells, B-cells, monocytes,neutrophils, fibroblasts and colony forming cells. Antineoplastic activity of IFN probably
results form a direct inhibitory effect on cell growth and proliferation, and from indirect
effects on the immune system, including increased NK-cell activity, enhanced expression ofMHC class I and II cell surface antigens (200, 227) and stimulatory or inhibitory effects on
certain B- and T-cell functions.
3.2 Preclinical studiesPharmacokineticsThe pharmacokinetics of IFN-α have been studied in healthy volunteers. After an intravenous
injection plasma levels of IFN-α decrease with an alfa and beta half life times of 5-10minutes and 4-5 hours, respectively. Intramuscular or subcutaneous injections results in peak
levels occurring after 4 to 7 hours. The area under the plasma concentration-time curve
(AUC) after subcutaneous or intramuscular injection is approximately 80 to 100% of that after
31

intravenous administration. The distribution volume at a steady state condition was 31.4 L.The clearance of IFN-α occurs mainly by catabolism in the renal tubulus, no active protein
is found in the urine (228,229).
3.3 Clinical spectrumThe clinical use for oncological purpose of IFN-β and IFN-γ has been investigated lessintensively than IFN-α. IFN-β has been studied mainly in patients with RCC (230,231). IFN-
γ has been studied alone (232-234), or in combination with IFN-α (235), or IL-2 (236-238)
or TNF (239). This review will focus on the clinical use of IFN-α in solid tumors. Mostquestions as to potential influence of dose and route of administration seem to have been
solved and the answers have been dictated by acceptability of toxicity. A narrow field ofindications seem to be emerging, although recently its limits may have been changed by
descriptions of influence of IFN-α on chemotherapeutic effects especially on 5FU. IFN-α is
approved for the treatment of patients with hairy cell leukemia, where response rates of 80%could be achieved. In chronic myeloid leukemia treatment with IFN-α has resulted in
therapeutic responses in up to 70% of the patients and occasional in the reversion to a normalchromosomal state (240). Responses to IFN-α are also reported in patients with Kaposi’s
sarcoma (30%), myeloma (10-20%), and carcinoid tumors (40%). Reproducible activity also
was found against tumors such as melanoma and renal cell carcinoma, which are unresponsiveto conventional chemotherapy.
3.3.1 Renal cell carcinomaThe use of the interferons in renal cell carcinoma has been reviewed by Muss (241).
Interferon induces responses in 13% of patients with renal cell carcinoma, with mostly partialresponses. Median response duration was 6 months. Routes of administration do not appear
to influence response rates or toxicity although intramuscular or subcutaneous administrationmay be preferable. Maximal response rates are obtained with both low and intermediate doses.
Randomized studies addressing the dose-response issue suggested in two trials that a high
dose regimen was superior, while a third study did not show any difference between the lowand high dose treatment. Toxicity was substantially enhanced using the high dose IFN in all
trials (242-244). A dose of 5-10 MU, given subcutaneous or intramuscular, at least three timesa week appears to result in the best therapeutic index. In one study, antibody formation,
occurring in up to 38% of the patients was associated with a loss of toxicity and a decrease
in median survival and remission duration (243).
3.3.2 Malignant melanomaThe use of IFN in the treatment of patients with malignant melanoma has recently been
reviewed by Kirkwood (245). In several clinical trials response rates of 12% - 22% were
reported with occasional complete responses. No dose response relationship has been found
32

in melanoma patients in the range of 10 to 100 MU IFN with daily or alternate-day dosing.Responses may be observed late during therapy after 3 - 6 month, with most of them being
partial, with a median response duration of 4 months. However, a small minority of patients
may achieve long term disease free remissions of several years following IFN-α therapy(246). IFN-α has been used in combination with cimetidine (247), zidovudine (248) and
cytotoxic agents with either no or small improvement in response rates. The combination ofDTIC with recombinant interferonα-2a has been shown to produce objective response rates
of 26%, with low toxicity and maintenance of quality of life. In some, but not all randomized
trials with DTIC as a single agent, the combination treatment showed improved response rates(249-252). The combination treatment of patients with melanoma using IFN, IL-2 and
cytotoxic agents is discussed in section 2.7.
3.3.3 Aids related Kaposi’s sarcomaKaposi’s sarcoma is a rare malignant disease that is associated with the acquiredimmunodeficiency syndrome (AIDS). Numerous controlled trials have demonstrated
reproducible response rates in the range of 20-40% with IFN-α therapy; a substantialproportion have been complete responses. Higher doses IFN (>=20 MIU/m2/day) have been
associated with better responses than lower doses. The total lymphocyte count, CD4
lymphocyte count, and CD4/CD8 ratio, as well as the beta-2- microglobulin level have beenassociated with better responses (253). Combination of IFN-α with chemotherapeutic agents
have not produced significant enhanced response rates compared with IFN alone. Howeverthe hematological and other organ related toxicity were enhanced and dose reductions of both
IFN and the cytotoxic drug were often necessary. Combination of IFN with zidovudine
produces good results, with reproducible response rates of approximately 40%, whilesuppressing HIV-infection (248,254). The clinical use of this combination is however
frequently complicated by the overlapping myelotoxicity, particularly neutropenia, of theseagents. Hematopoietic growth factors such as granulocyte (G-CSF) or granulocyte-macrophage
colony-stimulating factor (GM-CSF) can be useful in restoring neutrophil counts and
preventing of otherwise required dose modifications, but it did not have an effect on theresponse rate, the CD4-cell count, or the improvement in any other hematologic parameter.
The use of growth factors was not associated with an increased toxicity or a change in serumHIV p24 antigen (255).
3.3.4 Colorectal cancerIFN-α as a single agent has only little activity in the treatment of patients with colorectal
cancer, with response rates of approximately 10% (256,257). In vitro IFN-α synergisticallyaugments the cytotoxic effects of the antimetabolite fluorouracil (5-FU) against human colon
cancer cell lines (258). IFN-α can also improve 5-FU/Leucovorin mediated growth inhibition
in fluoropyrimidine sensitive colon cancer cells (259,260). In animal studies interferon
33

potentiates the effect of 5-FU in inhibiting liver metastases in nude mice (261). Themechanisms of the synergy between IFN and 5-FU are not clarified. IFN-α treatment of
HT-29 colon carcinoma cells induced a greater than two-fold increase in the intracellular
levels of the active metabolite of 5-FU, FdUMP. Using cell extracts from HT-29 cells and 5-FU as substrate, IFN-α produced a 1.9- and 8.7-fold increase, respectively, in the activities
of uridine phosphorylase and pyrimidine nucleoside phosphorylase (PyNP). The effect wasselective for the conversion of 5-FU to FdUMP, as IFN-α did not increase the cellular levels
of FUTP, nor did it change the extent of incorporation of 5-FU into RNA (or DNA). IFN-αalso had no effect on thymidine kinase activity, the second step in the activation of 5-FU.Hence the effect of IFN-α on PyNP-activity is likely a critical biochemical event that
modulates the cytotoxicity of 5-FU (258). IFN also alters the pharmacokinetics of 5-FU,inducing higher serum levels of 5-FU and increased drug exposure (262,263). In a clinical
trial, treatment of patients with advanced colorectal carcinoma with the combination of 5-FU
750 mg/m2/d for 5 days as a continuous infusion followed by weekly outpatient bolus therapyand IFN 9 MU subcutaneously starting day 1 and administered three times per week resulted
in objective tumor regression in 62% of patients (264). In a multi-institutional setting phaseII clinical trial by the Eastern Cooperative Oncology Group (ECOG) the addition of IFN to
5-FU enhanced the objective response rates achieved in patients with advanced colorectal
carcinoma with acceptable toxicities. IFN also enhances fluorouracil-induced toxicities,especially mucositis (265). The triple combination of 5-FU, IFN and Leucovorin was highly
active in patients with advanced colorectal cancer, at the cost of increased toxicity, mainlymucositis and diarrhea (262,266).
3.3.5 CarcinoidThe malignant carcinoid is a slowly growing tumor arising from cells of the neural crest that
are capable of amine precursor uptake and decarboxylation. Multiple small tumors in the gutor metastases in the liver may produce a variety of biological active peptides that can cause
the carcinoid syndrome, which includes severe diarrhea, cutaneous flushes, hypotension, and
cardiac valvular lesions. The primary form of treatment in this disease is surgery. When thetumor is unresectable or metastatic, chemotherapeutic approaches have been investigated, with
combination treatment of streptozocin and fluorouracil being the most effective regimenreported (267,268). Besides the symptomatic treatment with somatostatin analogues (269,270),
interferons have been investigated in the treatment of the malignant carcinoid. IFN-α, at doses
of 2.5 to 42 MU/week induced responses in 30% to 60% of the patients with reduction ofserum tumor marker levels and symptomatic improvement, rather than a reduction in tumor
size (271-278). Side effects, consisting of anorexia and fatigue, were observed inapproximately one third of the patients treated. These side effects were dose related and they
required dose reductions of IFN or discontinuation of treatment in a number of patients. Dose
escalation of IFN did not improve response rate (277). Low doses of 3 to 9 MU/d i.m. at least
34

3 times a week have been reported to have the best therapeutic index with prolongedsymptomatic improvement and tolerable toxicity.
3.3.6 Ovarian cancerDespite the improved results of platinum-based combination chemotherapy, local tumor
recurrence remains a major problem in the treatment of patients with ovarian cancer.Interferon has been used intraperitonally in patients with ascites from a local relapse. In three
studies, using high doses (50 MU) of IFN-α administered in 2 L dialysate, response rates up
to 52% were observed (279-281). When alternated with intraperitoneal cisplatin, a responserate of 50% was described in one study (282).
3.3.7 Bladder cancerTreatment of superficial bladder cancer with IFN administered intravesically has been
effective with complete responses against both carcinoma in situ and recurrent noninvasivelow-grade transitional cell carcinomas. In a phase II study intravesical instillations of
recombinant IFN-α, at a daily dose of 54 MU for 5 days for 2 consecutive weeks resulted ina response rate of 79% of patients. The median relapse time was 40 weeks, while clinical and
local tolerance were optimal (283).
3.3.8 Benign TumorsInterferon-α appears to induce the early regression of life-threatening corticosteroid-resistanthemangiomas including pulmonary hemangiomatosis of infancy (284,285).
3.4 TolerabillityThe clinical toxicity of interferon has been reviewed by Quesada (219) and Dorr (221). The
most common acute toxicity is a flu like syndrome with fever up to 38 to 40 C, startingwithin 6 hours after a parenteral dose and lasting for 4 to 8 hours, if untreated. Chills,
myalgias, arthralgias and headache may accompany the febrile reaction. These side effects can
be partially inhibited with acetaminophen. With repeated daily treatment the febrile reactionand accompanying symptoms usually decrease in intensity in seven to ten days. With
intermittent cyclic administration no such tachyphylaxis is observed, with symptomsfrequently reoccurring after re-exposure to IFN. Fatigue and anorexia are the most prominent
dose limiting toxicities of chronic interferon treatment. Alternate-day administration may be
better tolerated than daily administration in this setting. At high doses IFN can be neurotoxic,with symptoms of vertigo, confusion and decreased mental status. Severe IFN toxicities are
rare, but isolated reports of coma, cerebrovascular accidents have been reported.Hematological toxicity consists of mild leucopenia, and sometimes anemia and
thrombocytopenia. Few gastrointestinal symptoms are observed with low dose IFN (3-5
MU/day). With higher doses toxicity consisting of nausea, vomiting, and diarrhoea become
35

more prominent. Cardiovascular effects of IFN are uncommon and rarely serious. Elevationof serum transaminases may reflect hepatic toxicity. Renal toxicity is usually low, but severe
renal toxicities with reversible renal failure and nephrotic syndrome have been reported.
Interferon toxicity is dose related. In general, tolerance and compliance are excellent withdoses of 1-9 MU. At doses above 18 MU there is a significant increase in the incidence of
severe adverse effects particularly gastro-intestinal and neurological effects. Doses over 36MU are rarely tolerated for more than 8 weeks.
3.5 Conclusions and perspectivesThe clinical spectrum of IFN seems, as far as oncology is concerned to have almost
crystallized. It is an active agent in some hematological tumors, but usually alternatives areavailable. This is important considering its side effects and high costs. However in view of
the reversibility of these side effects, in contrast to those of many cytotoxic agents, doubtless
IFN-α will remain part of the armamentarium in the fight against cancer. In solid tumors itsplace is still uncertain, until now the only synergy that has reproducibly been found is that
with the cytostatic 5-FU. However, the possibilities to translate this into clinical practicedeserve further study.
References
1. Oldham R. Biotherapy: The 4th Modality of Cancer Treatment. J. Cell. Physiol. 1986; (Suppl),4: 91-99.2. Rosenberg SA. Karnofsky Memorial Lecture. The immunotherapy and gene therapy of cancer. J. Clin.
Oncol. 1992; 10: 180-199.3. Currie GA. Eighty years of immunotherapy: a review of immunological methods used for the treatment
of human cancer. Br. J. Cancer 1972; 26: 141-153.4. Wadler S. The role of interferons in the treatment of solid tumors. Cancer 1992; 70: 949-958.5. Hirschhorn K, Kolodny RL, Hashem N and Bach FH. Mitogen action of phytohaemagglutinin. Lancet
1963; i: 305-306.6. Morgan DA, Ruscetti FW and Gallo RC. Selective in vitro growth of T lymphocytes from normal
human bone marrows. Science 1976; 193: 1007-1008.7. Aarden LA, Brunner TK, Cerottini JC et al. Revised Nomenclature for Antigen-Nonspecific T Cell
Proliferation and Helper Factors. J. Immunol. 1979; 123: 2928-2929.8. Chanda PK, Chen GF, Baine Y, Leonard WJ, Greene WC, Chang TW and Chang NT. Expression of
human interleukin-2 receptor cDNA in E. coli. Biochem. Biophys. Res. Commun. 1986; 141: 804-811.9. Fujita T, Takaoka C, Matsui H and Taniguchi T. Structure of the human interleukin 2 gene. Proc. Natl.
Acad. Sci. U. S. A. 1983; 80: 7437-7441.10. Brandhuber BJ, Boone T, Kenney WC and McKay DB. Three-dimensional structure of interleukin-2.
Science 1987; 238: 1701-1709.11. Robb RJ, Kutny RM, Panico M, Morris HR and Chowdhry V. Amino acid sequence and
post-translational modification of human interleukin 2. Proc. Natl. Acad. Sci. U. S. A. 1984; 81:6486-6490.
12. Smith KA. Interleukin-2: inception, impact, and implications. Science 1988; 240: 1169-1176.13. Smith KA. Lowest dose interleukin-2 immunotherapy. Blood 1993; 81: 1414-1423.14. Vyth-Dreese FA, Van der Reijden HJ and De Vries JE. Phorbol-ester-mediated induction and
augmentation of mitogenesis and interleukin-2 production in human T-cell lymphoproliferative disease.
36

Blood 1982; 60: 1437-1446.15. Schwartz RH. Costimulation of T lymphocytes: The role of CD28, CTLA-4, and B7/BB1 in
interleukin-2 production and immunotherapy. Cell 1992; 71: 1065-1068.16. Townsend SE and Allison JP. Tumor rejection after direct costimulation of CD8+ T cells by B7-
transfected melanoma cells. Science 1993; 259: 368-370.17. Leonard WJ, Depper JM, Crabtree GR, Rudikoff S, Pumphrey J, Robb RJ, Kronke M, Svetlik PB,
Peffer NJ, Waldmann TA et al. Molecular cloning and expression of cDNAs for the human interleukin-2receptor. Nature 1984; 311: 626-631.
18. Nikaido T, Shimizu A, Ishida N, Sabe H, Teshigawara K, Maeda M, Uchiyama T, Yodoi J and HonjoT. Molecular cloning of cDNA encoding human interleukin-2 receptor. Nature 1984; 311: 631-635.
19. Hatakeyama M, Tsudo M, Minamoto S, Kono T, Doi T, Miyata T, Miyasaka M and Taniguchi T.Interleukin-2 receptorβ chain gene: Generation of three receptor forms by cloned humanα and βchain cDNA’s. Science 1992; 257: 379.
20. Takeshita T, Asao H, Ohtani K, Ishii N, Kumaki S, Tanaka N, Munakata H, Nakamura M andSugamura K. Cloning of theτ chain of the human IL-2 receptor. Science 1992; 257: 379.
21. Ritz J, Schmidt RE, Michon J, Hercend T and Schlossman SF. Characterization of functional surfacestructures on human natural killer cells. Adv. Immunol. 1988; 42: 181-211.
22. Wang HM and Smith KA. The interleukin-2 receptor: Functional consequenses of its bimolecularstructure. J. Exp. Med. 1981; 154: 1455-1474.
23. Hatfield SM. Cyclosporine and FK506 inhibition of murine mast cell cytokine production. J. Pharmacol.Exp. Ther. 1992; 260: 680-688.
24. Rubin LA and Nelson DL. The soluble interleukin-2 receptor: biology, function, and clinical application.Ann. Intern. Med. 1990; 113: 619-627.
25. Lissoni P, Tisi E, Brivio F, Barni S, Rovelli F, Perego M and Tancini G. Increase in solubleinterleukin-2 receptor and neopterin serum levels during immunotherapy of cancer with interleukin-2.Eur. J. Cancer 1991; 27: 1014-1016.
26. Lissoni P, Barni S, Tisi E, Rovelli F, Pittalis S, Rescaldani R, Vigore L, Biondi A, Ardizzoia A andTancini G. In vivo biological results of the association between interleukin-2 and interleukin-3 in theimmunotherapy of cancer. Eur. J. Cancer 1993; 29A: 1127-1132.
27. Grimm EA, Mazumder A, Zhang HZ and Rosenberg SA. Lymphokine-activated killer cell phenomenon.Lysis of natural killer-resistant fresh solid tumor cells by interleukin 2- activated autologous humanperipheral blood lymphocytes. J. Exp. Med. 1982; 155: 1823-1841.
28. Pfizenmaier K, Scheurich P, Daubener W, Kronke M, Rollinghoff M and Wagner H. Quantitativerepresentation of all T cells committed to develop into cytotoxic effector cells and/or interleukin 2activity- producing helper cells within murine T lymphocyte subsets. Eur. J. Immunol. 1984; 14: 33-39.
29. Lotze MT, Grimm EA, Mazumder A, Strausser JL and Rosenberg SA. Lysis of fresh and culturedautologous tumor by lymphocytes cultured in T-cell growth factor. Cancer Res. 1981; 41: 4420-4425.
30. Rosenberg SA, Spiess PJ and Lafreniere R. A new approach to the adoptive immunotherapy of cancerwith tumor infiltrating lymphocytes. Science 1986; 233: 1318-1321.
31. Ortaldo JR, Mason AT, Gerard JP, Henderson LE, Farrar W, Hopkins RF, Herberman RB and RabinH. Effects of natural and recombinant IL 2 on regulation of IFN gamma production and natural killeractivity: lack of involvement of the Tac antigen for these immunoregulatory effects. J. Immunol. 1984;133: 779-783.
32. Saraya KA and Balkwill FR. Temporal sequence and cellular origin of interleukin-2 stimulated cytokinegene expression. Br. J. Cancer 1993; 67: 514-521.
33. Kovacs EJ, Becker SK, Longo DL, Versio L and Young HA. Cytokine gene expression during thegenration of lymphokine activated killer cells: early induction of IL-1β by IL-2. Cancer Res. 1989; 49:940-944.
34. Schaafsma MR, Falkenburg JH, Landegent JE, Duinkerken N, Osanto S, Ralph P, Kaushansky K,Wagemaker G, Van Damme J, Willemze R and Fibbe WE. In vivo production of interleukin-5,granulocyte-macrophage colony-stimulating factor, macrophages colony-stimulating factor, andinterleukin-6 during intravenous administration of high-dose interleukin-2 in cancer patients seecomments. Blood 1991; 78: 1981-1987.
35. Donohue JH, Rosenstein M, Chang AE, Lotze MT, Robb RJ and Rosenberg SA. The systemicadministration of purified interleukin 2 enhances the ability of sensitized murine lymphocytes to cure
37

a disseminated syngeneic lymphoma. J. Immunol. 1984; 132: 2123-2128.36. Thompson JA, Peace DJ, Klarnet JP, Kern DE, Greenberg PD and Cheever MA. Eradication of
disseminated murine leukemia by treatment with high-dose interleukin 2. J. Immunol. 1986; 137:3675-3680.
37. Rosenberg SA, Mule JJ, Spiess PJ, Reichert CM and Schwarz SL. Regression of established pulmonarymetastases and subcutaneous tumour mediated by the systemic administration of high-dose recombinantinterleukin 2. J. Exp. Med. 1985; 161: 1169-1188.
38. Mule JJ, Shu S, Schwarz SL and Rosenberg SA. Adoptive immunotherapy of established pulmonarymetastases with LAK cells and recombinant interleukin-2. Science 1984; 225: 1487-1489.
39. Mazumder A and Rosenberg SA. Successful immunotherapy of natural killer-resistant establishedpulmonary melanoma metastases by the intravenous adoptive transfer of syngeneic lymphocytesactivated in vitro by interleukin 2. J. Exp. Med. 1984; 159: 495-507.
40. Lafreniere R and Rosenberg SA. Succesful immunotherapy of murine experimental hepatic metastaseswith lymphokine-activated killer cells and recombinant interleukin-2. Cancer Res. 1985; 45: 3735-3741.
41. Donohue JH, Lotze MT, Robb RJ, Rosenstein M, Braziel RM, Jaffe ES and Rosenberg SA. In vivoadministration of purified Jurkat-derived interleukin 2 in mice. Cancer Res. 1984; 44: 1380-1386.
42. Chang AE, Hyatt CL and Rosenberg SA. Systemic administration of recombinant human interleukin2 in mice. J. Biol. Resp. Mod. 1984; 3: 561-572.
43. Cheever MA, Thompson JA, Kern DE and Greenberg PD. Interleukin-2 (IL-2) administered in vivo:influence of IL-2 route and timing on T cell growth. J. Immunol. 1985; 134: 3895-3899.
44. Mule JJ, Shu S and Rosenberg SA. The anti-tumor efficacy of lymphokine-activated killer cells andrecombinant interleukin 2 in vivo. J. Immunol. 1985; 135: 646-652.
45. Ettinghausen SE and Rosenberg SA. Immunotherapy of murine sarcomas using lymphokine activatedkiller cells: optimization of the schedue and route of administration of recombinant interleukin 2. CancerRes. 1986; 46: 2784-2792.
46. Mule JJ, Yang JC, Lafreniere R, Shu S and Rosenberg SA. Identification of cellular mechanismsoperational in vivo during the regression of esthablished pulmonary metastases by the systemicadministration of high dose recombinant interleukin 2. J. Immunol. 1987; 139: 285-294.
47. Talmadge JE, Phillips H, Schindler J, Tribble H and Pennington R. Systemic Preclinical Study of theTherapeutic Properties of Recombinant Human Interleukin 2 for the Treatment of Metastatic Disease.Cancer Res. 1987; 47: 5725-5732.
48. Maas RA, Dullens HF, De Jong WH and Den Otter W. Immunotherapy of mice with a large burdenof disseminated lymphoma with low-dose interleukin 2. Cancer Res. 1989; 49: 7037-7040.
49. Forni G, Giovarelli M, Santoni A, Modesti A and Forni M. Tumour inhibition by interleukin-2 at thetumour/host interface. Biochim. Biophys. Acta 1986; 865: 307-327.
50. Felgar RE and Hiserodt JC. In vivo migration and tissue localization of highly purifiedlymphokine-activated killer cells (A-LAK cells) in tumor-bearing rats. Cell. Immunol. 1990; 129:288-298.
51. Griffith KD, Read EJ, Carrasquillo JA, Carter CS, Yang JC, Fisher B, Aebersold P, Packard BS, YuMY and Rosenberg SA. In vivo distribution of adoptively transferred indium-111- labeled tumorinfiltrating lymphocytes and peripheral blood lymphocytes in patients with metastatic melanoma. J. Natl.Cancer Inst. 1989; 81: 1709-1717.
52. Fisher B, Packard BS, Carrasquillo JA, Carter CS, Topalian SL, Yang JC, Yolles P, Larson SM andRosenberg SA. Tumor localization of adoptively transferred indium-111 labeled tumor infiltratinglymphocytes in patients with metastatic melanoma. J. Clin. Oncol. 1989; 7: 250-261.
53. Yoshino I, Yano T, Murata M, Ishida T, Sugimachi K, Kimura G and Nomoto K. Tumor-reactiveT-cells accumulate in lung cancer tissues but fail to respond due to tumor cell-derived factor. CancerRes. 1992; 52: 775-781.
54. Alexander JP, Kudoh S, Melsop KA, Hamilton TA, Edinger MG, Tubbs RR, Sica D, Tuason L, KleinE, Bukowski RM and Finke JH. T cells infiltrating renal cell carcinoma display a poor proliferativeresponse even though they can produce interleukin 2 and express interleukin 2 receptors. Cancer Res.1993; 53: 1380-1387.
55. Miescher S, Whiteside TL, Carrel S and Von Fliedner V. Functional properties of tumor-infiltrating andblood lymphocytes in patients with solid tumors: effects of tumor cells and their supernatants onproliferative responses of lymphocytes. J. Immunol. 1986; 136: 1899-1907.
38

56. Konrad MW, Hemstreet G, Hersh EM, Mansell PWA, Mertelsmann R, Kolitz JE and Bradley EC.Pharmacokinetics of recombinant interleukin 2 in humans. Cancer Res. 1990; 50: 2009-2017.
57. Donohue JH and Rosenberg SA. The fate of interleukin 2 after in vivo administration. J. Immunol.1983; 130: 2203-2208.
58. Gustavson LE, Nadeau RW and Oldfield NF. Pharmacokinetics of Teceleukin (recombinantinterleukin-2) after intravenous or subcutaneous administration to patients with cancer. J. Biol. Resp.Mod. 1989; 8: 440-449.
59. Lamers CHJ, Stoter G, Goey SH, Oosterom R and Bolhuis RLH. Bioavailabillity of interleukin-2 afterreconstitution with albumin. Correspondence. Lancet 1992; 340: 241.
60. Vlasveld LT, Beijnen JH, Sein JJ, Rankin EM, Melief CJM and Hekman A. Reconstitution ofrecombinant interleukin-2 (rIL-2): a comparative study of various rIL-2 Muteins. Eur. J. Cancer 1993;29A: 1977-1979.
61. Huland E, Huland H and Heinzer H. Interleukin-2 by inhalation: Local therapy for metastatic renal cellcarcinoma. J. Urol. 1992; 147: 344-348.
62. Pizza G, Severini G, Menniti D, De Vinci C and Corrado F. Tumour regression after intralesionalinjection of interleukin 2 (IL-2) in bladder cancer. Preliminary report. Int. J. Cancer 1984; 34: 359-367.
63. Zimmerman RJ. Schedule dependency of the antitumor activity and toxicity of polyethyleneglycol-modified interleukin 2 in murine tumor models. Cancer Res. 1989; 49: 6521-6528.
64. Feruglio C, Zambello R, Trentin L, Bulian P, Franceschi T, Cetto GL and Semenzato G. Cytotoxic invitro function in patients with metastatic renal cell carcinoma before and after alpha-2b-interferontherapy. Effects of activation with recombinant interleukin-2. Cancer 1992; 69: 2525-2531.
65. Matsuoka J, Sakagami K, Higaki K, Idani H, Fujiwara T, Kaneshige T and Orita K. Site directedimmunotherapy by intratumoral administrations of slow delivery system of interleukin 2: A pilot studyin 14 breast cancer patients. Proc. Am. Assoc. Cancer Res. 1993; 12: 934. (Abstract)
66. Rosenberg SA, Lotze MT, Yang JC, Aebersold PM, Linehan WM, Seipp CA and White DE. Experiencewith the use of high-dose interleukin-2 in the treatment of 652 cancer patients. Ann. Surg. 1989; 210:474-485.
67. Dillman RO, Church C, Oldham RK, West WH, Schwartzberg L and Birch R. Inpatientcontinuous-infusion interleukin-2 in 788 patients with cancer. The National Biotherapy Study Groupexperience. Cancer 1993; 71: 2358-2370.
68. Stewart JA, Belinson JL, Moore AL, Dorighi JA, Grant BW, Haugh LD, Roberts JD, Albertini RJ andBranda RF. Phase I trial of intraperitoneal recombinant interleukin- 2/lymphokine-activated killer cellsin patients with ovarian cancer. Cancer Res. 1990; 50: 6302-6310.
69. Steis RG, Urba WJ, VanderMolen LA, Bookman MA, Smith JW, Clark JW, Miller RL, Crum ED,Beckner SK, McKnight JE, Ozols RF, Stevenson HC, Young RC and Longo DL. Intraperitoneallymphokine-activated killer-cell and interleukin- 2 therapy for malignancies limited to the peritonealcavity. J. Clin. Oncol. 1990; 8: 1618-1629.
70. Huland E and Huland H. Local continuous high dose interleukin 2: a new therapeutic model for thetreatment of advanced bladder carcinoma. Cancer Res. 1989; 49: 5469-5474.
71. Clamon G, Herndon J, Perry MC, Ozer H, Kreisman H, Maher T, Ellerton J and Green MR.Interleukin-2 activity in patients with extensive small-cell lung cancer: A phase II trial of caner andleukemia group B. J. Natl. Cancer Inst. 1993; 85: 316-320.
72. Lotze MT, Custer MC and Rosenberg SA. Intraperitoneal administration of interleukin-2 in patients withcancer. Arch. Surg. 1986; 121: 1373-1379.
73. Berek JS. Intraperitoneal adoptive immunotherapy for peritoneal cancer. editorial. J. Clin. Oncol. 1990;8: 1610-1612.
74. Viallat JR, Boutin C, Rey F, Astoul Ph, Farisse P and Brandely M. Intrapleural immunotherapy withescalating doses of interleukin-2 in metastatic pleural effusions. Cancer 1993; 71: 4067-4071.
75. List J, Moser RP, Steuer M, Loudon WG, Blacklock JB and Grimm EA. Cytokine responses tointraventricular injection of interleukin 2 into patients with leptomeningeal carcinomatosis: rapidinduction of tumor necrosis factor alpha, interleukin 1 beta, interleukin 6, gamma-interferon, and solubleinterleukin 2 receptor (Mr 55,000 protein). Cancer Res. 1992; 52: 1123-1128.
76. Galvani DW, Walton S, Davies JM, Owen RR, Carr R et al. Endolymphatic delivery of IL2 in patientswith melanoma and lymphoma. Biotherapy 1992; 4: 251-255.
77. Belli F, Arienti F, Rivoltini L, Santinamini M, Mascheroni L et al. Treatment of recurrent in transit
39

metastases from cutaneous melanoma by isolation perfusion in extracorporal circulation withinterleukin-2 and lymphokine activated killer cells. A pilot study. Melanoma. Res 1992; 2: 263-271.
78. Keilholz U, Schlag P, Tilgen W, Brado B, Galm F, Görich J, Kauffmann GW, Möller P, Schneider Sand Hunstein W. Regional administration of lymphokine-activated killer cells can be superior tointravenous application. Cancer 1992; 69: 2172-2175.
79. Klasa RJ, Silver HKB and Kong S. In vivo induction of lymphokine activated killer cells byinterleukin-2 splenic artery perfusion in advanced malignancy. Cancer Res. 1990; 50: 4906-4910.
80. Weiss GR, Margolin KA, Aronson FR, Sznol M, Atkins MB, Dutcher JP, Gaynor ER, Boldt DH,Doroshow JH, Bar MH, Hawkins MJ, Demchak PA, Gucalp R and Fisher RI. A randomized phase IItrial of continuous infusion interleukin-2 or bolus injection interleukin-2 plus lymphokine-activated killercells for advanced renal cell carcinoma. J. Clin. Oncol. 1992; 10: 275-281.
81. Sosman JA, Kohler PC, Hank JA, Moore KH, Bechhofer R, Storer B and Sondel PM. Repetitive weeklycycles of interleukin-2. II. clinical and immunologic effects of dose, schedule, and addition ofindomethacin. J. Natl. Cancer Inst. 1988; 80: 1451-1461.
82. Fisher RI, Coltman CA, Doroshow JH, Rayner AA, Hawkins MJ, Mier JW, Wiernik P, McMannis JD,Weiss GR, Margolin KA, Gemlo BT, Hoth DF, Parkinson DR and Paietta E. Metastatic renal cancertreated with interleukin-2 and lymphokine activated killer cells. Ann. Intern. Med. 1988; 108: 518-523.
83. Negrier S, Philip T, Stoter G, Fossa SD, Janssen S, Iacone A, Cleton FS, Eremin O, Israel L, JasminC, Rugarli C, Masse HVD, Thatcher N, Symann M, Bartsch HH, et al. Interleukin-2 with or withoutLAK cells in metastatic renal cell carcinoma: A report of a European multicenter study. Eur. J. Cancerand Clin. Oncol. 1989; 25(suppl. 3): S21-S28.
84. West WH. Continuous infusion recombinant interleukin-2 (rIL-2) and adoptive cellular therapy of renalcell carcinoma and other molignancies. Cancer Treat. Rev. 1989; 16(supp. A): 83-89.
85. Dillman RO, Barth NM, Oldham RK et al. Continuous interleukin-2 and lymphokine activated killercells in advanced cancer. Proc. Am. Soc. Clin. Oncol. 1989; 8: 188. (Abstract)
86. Bajorin DF, Sell K, Richards JM et al. A randomized trial of interleukin-2 plus lymphokine activatedkiller cells versus interleukin-2 alone in renal cell carcinoma. Proc. Am. Assoc. Cancer Res. 1990; 31:186. (Abstract)
87. Bukowski RM, Goodman P, Crawford ED, Sergi JS, Redman BG and Whitehead RP. Phase II trial ofhigh-dose intermittent interleukin-2 in metastatic renal cell carcinoma: A Southwest Oncology GroupStudy. J. Natl. Cancer Inst. 1990; 82: 143-146.
88. Parkinson DR, Fisher RI, Rayner AA, Paietta E, Margolin KA, Weiss GR, Mier JW, Sznol M, GaynorER, Bar MH, Gucalp R, Boldt DH, Mills B and Hawkins MJ. Therapy of renal cell carcinoma withinterleukin-2 and lymphokine-activated killer cells: Phase II experience with a hybrid bolus andcontinuous infusion interleukin-2 regimen. J. Clin. Oncol. 1990; 8: 1630-1636.
89. Gaynor ER, Weiss GR, Margolin KA et al. Phase I study of high-dose recombinant interleukin-2 andautologous lymphokine activated killer cells in patients with metastatic or unresectable malignantmelanoma and renal cell carcinoma. J. Natl. Cancer Inst. 1990; 82: 1397-1402.
90. Von der Maase H, Geertsen PF, Thatcher N, Jasmin C, Marcatello A, Fosså SD, Symann M, Stoter G,Nagel G, Israel L, Oskam R, Palmer P and Franks CR. Recombinant interleukin-2 in metastatic renalcell carcinoma. A European multicenter phase II study. Eur. J. Cancer 1991; 27: 1583-1589.
91. Douillard JY, Chevreau C, Perrocheau G, Mignot L, Tueni E, Lanson Y, Namer M, Mangin P, SuretJY, Burki F and Brandely M. Phase II trial of interleukin II (rIL2) for metastatic renal cell carcinoma.Eur. J. Cancer 1991; 27 (suppl. 2): S99. (Abstract)
92. Sorio R, Galligioni E, Sacco C, Errante D, Freschi A, Quaia M, Spada A, Santarosa M, Franchini M,Morassut S, Monfardini S and Aviano CRO. Recombinant interleukin-2 (rIL-2) by continuous infusion(CI) in 20 patients with advanced renal cell cancer (RCC). Eur. J. Cancer 1991; 27 (suppl. 2): S98.(Abstract)
93. Koretz MJ, Lawson DH, York RM, Graham SD, Murray DR, Gillespie TM, Levitt D and Sell KM.Randomized study of interleukin 2 (IL-2) alone vs IL-2 plus lymphokine-activated killer cells fortreatment of melanoma and renal cell cancer. Arch. Surg. 1991; 126: 898-903.
94. Escudier B, Rossi JF, Ravaud A, Douillard JY, Negrier S, Baume D, Dorval T, Chevreau C, MignotL, Pein F, Fargeot P, Lesimple T and Brandely M. French expirience of high dose IL2 on a two-daysa week schedule in metastatic renal cell carcinoma: a multicenter study. Proc. Am. Soc. Clin. Oncol.1992; 11: 651. (Abstract)
40

95. Sleijfer DTh, Janssen RAJ, Willemse PHB, Martens A, Leij de L, De Vries EGE and Mulder NH.Low-dose regimen of interleukin-2 for metastatic renal carcinoma. Lancet 1990; 335: 1522-1523.
96. Negrier S, Mercatello A, Bret M, Thiesse P, Blay JY, Coronel B, Merrouche Y, Oskam R, Franks CR,Clavel M, Moskovtchenko JF and Philip T. Intravenous interleukin-2 in patients over 65 with metastaticrenal carcinoma. Br. J. Cancer 1992; 65: 723-726.
97. Palmer PA, Vinke J, Evers P, Pourreau C, Oskam R and Roest G. Continuous infusion of recombinantinterleukin-2 with or without autologous lymphokine activated killer cells for the treatment of advancedrenal cell carcinoma. Eur. J. Cancer 1992; 67: 1038-1044.
98. Geertsen PF, Hermann GG, Von der Maase H and Steven K. Treatment of metastatic renal cellcarcinoma by continuous intravenous infusion of recombinant interleukin-2: a single- center phase IIstudy. J. Clin. Oncol. 1992; 10: 753-759.
99. Thompson JA, Shulman KL, Benyunes MC, Lindgren CG, Collins C, Lange PH, Bush WH,Jr., BenzLA and Fefer A. Prolonged continuous intravenous infusion interleukin-2 and lymphokine-activatedkiller-cell therapy for metastatic renal cell carcinoma. J. Clin. Oncol. 1992; 10: 960-968.
100. Atkins MB, Sparano JA, Fisher RI, Weiss GR, Margolin KA, Fink KI, Rubinstein L, Louie A, MierJW, Gucalp R, Sosman JA, Boldt DH, Doroshow JH, Aronson FR and Sznol M. Randomized phaseII trial of high-dose interleukin-2 either alone or in combination with interferon alfa-2b in advancedrenal cell carcinoma. J. Clin. Oncol. 1993; 11: 661-670.
101. Rosenberg SA, Lotze MT, Yang JC, Topalian SL, Chang AE, Schwartzentruber DJ, Aebersold P,Leitman S, Linehan WM, Seipp CA, White DE and Steinberg SM. Prospective randomized trial ofhigh-dose interleukin-2 alone or in conjunction with lymphokine-activated killer cells for the treatmentof patients with advanced cancer. J. Natl. Cancer Inst. 1993; 85: 622-632.
101a. Rosenberg SA, Yang JC, Topalian SL, Schwartzentruber DJ, Weber JS, Parkinson DR, Seipp CA,Einhorn JH and White DE. Treatment of 283 consecutive patients with metastatic melanoma or renalcell cancer using high-dose-bolus interleukin-2. JAMA 1994; 271: 907-913.
102. Kuebler JP, Whitehead RP, Ward DL, Hemstreet GPIII and Bradley EC. Treatment of metastatic renalcell carcinoma with recombinant interleukin-2 in combination with vinblastine or lyphokine-activatedkiller cells. J. Urol. 1993; 150: 814-820.
103. Lopez M, Carpano S, Cancrini A, Marcellini M, Del Medico P, Rinaldi M and Vici P. Interleukin-2(IL-2) by cintinuous intravenous infusion (CIV) in advanced renal cell carcinoma (RCC). Proc. Am.Soc. Clin. Oncol. 1993; 12: 251. (Abstract)
104. Whitehead RP, Wilf MK, Solanki DL, Benedetto P, Flanigan RC and Craword ED. A phase II trial ofcontinuous infusion recombinant interleukin-2 (rIL-2) in patients with advanced renal cell carcinoma:A Southwest oncology group study. Proc. Am. Soc. Clin. Oncol. 1993; 12: 253. (Abstract)
105. Thatcher N, Dazzi H, Gosh A and Johnson RJ. Recombinant IL-2 given intra-splenically andintravenously in advanced malignant melanoma: a phase I/II study. Cancer Treat. Rev. 1989; 16 (Suppl.A): 49-52.
106. Dutcher JP, Creekmore SP, Weiss GR, Margolin K, Markowitz AB, Roper M, Parkinson D, CiobanuN, Fisher RI, Boldt DH, Doroshow JH, Rayner AA, Hawkins MJ and Atkins M. A phase II study ofinterleukin-2 and lymphokine-activated killer cells in patients with metastatic malignant melanoma. J.Clin. Oncol. 1989; 7: 477-485.
107. Bar MH, Sznol M, Atkins MB, Ciobanu N, Micetich KC et al. Metastatic malignant melanoma treatedwith combined bolus and continuous infusion interleukin-2 and lymphokine-activated killer cells. J. Clin.Oncol. 1990; 8: 1138-1147.
108. Whitehead RP, Kopecky KJ, Samson MK, Constanzi JJ, Natale RB, Feun LG, Hersh EM and RinehartJJ. Phase II study of intravenous bolus recombinant interleukin-2 in advanced malignant melanoma:Southwest Oncology Group study. J. Natl. Cancer Inst. 1991; 83: 1250-1251.
109. Dutcher JP, Gaynor ER, Boldt DH, Doroshow JH, Bar MH, Sznol M, Mier J, Sparano J, Fisher RI,Weiss G et al. A phase II study of high-dose continuous infusion interleukin-2 withlymphokine-activated killer cells in patients with metastatic melanoma. J. Clin. Oncol. 1991; 9: 641-648.
110. Dorval T, Fridman WH, Mathiot C and Pouillart P. Interleukin-2 therapy for metastatic uvealmelanoma. Eur. J. Cancer 1992; 28A: 2087.
111. Sparano JA, Micetich KC, Sunderland M, Margolin K, Aronson F, Sznol M and Rubinstein LV. Arandomized Phase III trial of treatment with high-dose interleukin-2 (IL-2) either alone or in
41

combination with interferonα-2a (IFN) in patients with advanced melanoma. Proc. Am. Soc. Clin.Oncol. 1993; 12: 1332. (Abstract)
112. Sznol M, Clark JW, Smith JW, Steis RG, Urba WJ, Rubinstein LV, VanderMolen LA, Janik J,Sharfman WH, Fenton RG, Creekmore SP, Kremers P, Conlon K, Hursey J, Beveridge J, et al. Pilotstudy of interleukin-2 and lymphokine-activated killer cells combined with immunomodulatory dosesof chemotherapy and sequenced with interferon alfa-2a in patients with metastatic melanoma and renalcell carcinoma. J. Natl. Cancer Inst. 1992; 84: 929-937.
113. Marincola FM, Venzon D, White D, Rubin JT, Lotze MT, Simonis TB, Balkissoon J, Rosenberg SAand Parkinson DR. HLA association with response and toxicity in melanoma patients treated withInterleukin-2 based immunotherapy. Cancer Res. 1992; 52: 6561-6566.
114. Rosenberg SA, Packard BS, Aebersold PM, Solomon D, Topalian SL, Toy ST, Simon P, Lotze MT,Yang JC, Seipp CA, Simpson C, Carter C, Bock S, Schwartzentruber D, Wei JP, et al. Use oftumor-infiltrating lymphocytes and interleukin-2 in the immunotherapy of patients with metastaticmelanoma: A preliminary report. N. Engl. J. Med. 1988; 319: 1676-1680.
115. Dillman RO, Oldham RK, Barth NM, Cohen RJ, Minor DR, Birch R, Yanelli JR, Maleckar JR,Sferruzza A, Arnold J and West WH. Continuous interleukin-2 and tumor-infiltrating lymphocytes astreatment of advanced melanoma. Cancer 1991; 68: 1-8.
116. Bukowski RM, Sharfman W, Murthy S, Rayman P, Tubbs R, Alexander J, Budd GT, Sergi JS, BauerL, Gibson V, Stanley J, Boyett J, Pontes E and Finke J. Clinical results and characterization oftumor-infiltrating lymphocytes with or without recombinant interleukin 2 in human metastatic renal cellcarcinoma. Cancer Res. 1991; 51: 4199-4205.
117. Baars JW, Fonk JC, Scheper RJ, Von Blomberg-Van der Flier ME, Bril H, Van der Valk P, Pinedo HMand Wagstaff J. Treatment with tumour infiltrating lymphocytes and interleukin-2 in patient withmetastatic melanoma: A pilot study. Biotherapy 1992; 4: 289-297.
118. Peto R, Pike MC, Armitage J, Breslow NE, Cox DR, Howard SV, Mantel N, McPherson K, Peto J andSmith PG. Design and analysis of randomized clinical trials requiring prolongued observation of eachpatient. I. Introduction and design. Br. J. Cancer 1976; 34: 585-612.
119. Peto R, Pike MC, Armitage J, Breslow NE, Cox DR, Howard SV, Mantel N, McPherson K, Peto J andSmith PG. Design and analysis of randomized clinical trials requiring prolongued observation of eachpatient. II. Analysis and examples. Br. J. Cancer 1977; 35: 1-39.
120. deKernion JB, Ramming KP and Smith RB. The natural history of metastatic renal cell carcinoma: acomputer analysis. J. Urol. 1978; 120: 148-152.
121. Philip T, Negrier S, Lasset C, Coronel B, Bret M, Blay JY, Merrouche Y, Carrie C, Kaemmerlen P,Chauvin F, Favrot M, Oskam R, Tabah I, Clavel M, Moskovtchenko JF, et al. Patients with metastaticrenal carcinoma candidate for immunotherapy with cytokines. Alanysis of a single institution study on181 patients. Br. J. Cancer 1993; 68: 1036-1042.
122. West WH, Tauer KW, Yanelli JR, Marshall GD, Orr DW, Thurman GD and Oldham RK. Constantinfusion recombinant interleukin-2 in adoptive immunotherapy of advanced cancer. N. Engl. J. Med.1987; 316: 898-905.
123. Janssen RAJ, Sleijfer DTh, Heijn AA, Mulder NH, The TH and Leij de L. Peripheral blood lymphocytenumber and phenotype prior to therapy correlate with response in subcutaneously applied rIL-2 therapyof renal cell carcinoma. Br. J. Cancer 1992; 66: 1177-1179.
124. Arinaga S, Karimine N, Takamuku K, Nanbara S, Inoue H, Abe R, Watanabe D, Matsuoka H, Ueo Hand Akiyoshi T. Correlation of eosinophilia with clinical response in patients with advanced carcinomatreated with low-dose recombinant interleukin-2 and mitomycin C. Cancer Immunol. Immunother. 1992;35: 246-250.
125. Hanninen EL, Korfer A, Hadam M, Schneekloth C, Dallmann I, Menzel T, Kirchner H, Poliwoda Hand Atzpodien J. Biological monitoring of low-dose interleukin 2 in humans: soluble interleukin 2receptors, cytokines, and cell surface phenotypes. Cancer Res. 1991; 51: 6312-6316.
126. Blay JY, Favrot MC, Negrier S, Combaret V, Chouaib S, Mercatello A, Kaemmerlen P, Franks CR andPhilip T. Correlation between clinical response to IL-2 therapy and sustained production of TNF. CancerRes. 1990; 50: 2371-2374.
127. Martens A, Janssen RAJ, Sleijfer DTh, Heijn AA, Mulder NH, The TH and De Leij L. Early sCD8plasma levels during subcutaneous rIL-2 therapy in patients with renal cell carcinoma correlate withresponse. Br. J. Cancer 1993; 67: 1118-1121.
42

128. Broom J, Heys SD, Whiting PH, Park KGM, Strachan A, Rothnie I, Franks CR and Eremin O.Interleukin 2 therapy in cancer: identification of responders. Br. J. Cancer 1992; 66: 1185-1187.
129. Blay JY, Negrier S, Combaret V, Attali S, Goillot E, Merrouche Y, Mercatello A, Ravault A, TouraniJM, Moskovtchenko JF and Philip T. Serum level of interleukin 6 as a prognosis factor in metastaticrenal cell carcinoma. Cancer Res. 1992; 52: 3317-3322.
130. Atzpodien J and Kirchner H. The out-patient use of recombinant human interleukin-2 and interferonalfa-2b in advanced malignancies. Eur. J. Cancer 1991; 27 Suppl 4P S88-91;:
131. Lotze MT, Chang AE, Seipp CA, Simpson C, Vetto JT and Rosenberg SA. High-dose recombinantinterleukin 2 in the treatment of patients with disseminated cancer. Responses, treatment-relatedmorbidity, and histologic findings. JAMA 1986; 256: 3117-3124.
132. Rosenberg SA, Lotze MT, Muul LM, Chang AE, Avis FP, Leitman S, Lineham WM, Robertson CN,Lee RE, Rubin JT, Seipp CA, Simpson CG and White DE. A progress report on the treatment of 157patients with advanced cancer using lymphokine-activated killer cells and interleukin-2 or high-doseinterleukin-2 alone. N. Engl. J. Med. 1987; 316: 889-897.
133. Economou JS, Hoban M, Lee JD, Essner R, Swisher S, McBride W, Hoon DB and Morton DL.Production of tumor necrosis factor alpha and interferon gamma in interleukin-2-treated melanomapatients: correlation with clinical toxicity. Cancer Immunol. Immunother. 1991; 34: 49-52.
134. Ochoa JB, Curti B, Peitzman AB, Simmons RL, Billiar TR, Hoffman R, Rault R, Longo DL, Urba WJand Ochoa AC. Increased circulating nitrogen oxides after human tumor immunotherapy: correlationwith toxic hemodynamic changes published erratum appears in J Natl Cancer Inst 1992 Aug 19;84(16):1291. J. Natl. Cancer Inst. 1992; 84: 864-867.
135. Fraker DL, Langstein HN and Norton JA. Passive immunization against tumor necrosis factor partiallyabrogates interleukin-2 toxicity. J. Exp. Med. 1989; 170: 1015-1020.
136. Kilbourn RG, Logothesis CJ, Striegel A and Griffith OW. Interleukin-2 (IL-2) mediated hypotensionin humans is reversed by NG-monomethyl-L-arginine (NMA) an inhibitor of nitric oxide (NO-)production. Proc. Am. Soc. Clin. Oncol. 1993; 12: 759. (Abstract)
137. Siegel JP and Puri RK. Interleukin-2 toxicity. J. Clin. Oncol. 1991; 9: 694-704.138. Margolin KA, Rayner AA, Hawkins MJ, Atkins MB, Dutcher JP, Fisher RI, Weiss GR, Doroshow JH,
Jaffe HS, Roper M, Parkinson DR, Wiernik PH, Creekmore SP and Boldt DH. Interleukin-2 andlymphokine-activated killer cell therapy of solid tumors: analysis of toxicity and management guidelines.J. Clin. Oncol. 1989; 7: 486-498.
139. Lee RE, Lotze MT, skibber JM, Tucker E, Bonow RO et al. Cardiorespiratory efects of immunotherapywith interleukin-2. J. Clin. Oncol. 1989; 7: 7-20.
140. Ognibene FP, Rosenberg SA, Lotze MT et al. Interleukin-2 administration causes reversiblehemodynamic changes and left ventricular dysfunction similar to those seen in septic shock. Chest 1988;94: 750-754.
141. Nora R, Abrams JS, Tait NS, Hiponia DJ and Silverman HI. Myocardial toxic effects duringrecombinant interleukin-2 therapy. J. Natl. Cancer Inst. 1989; 81: 59-63.
142. Osanto S, Cluitmans FH, Franks CR, Bosker HA and Cleton FJ. Myocardial injury after interleukin-2therappy. Lancet 1988; 11: 48-49.
143. Gaynor ER, Vitek L and Sticklin L. The haemodynamic effects of treatment with interleukin-2 andLymphokine Activated Killer cells. Ann. Intern. Med. 1988; 109: 953-958.
144. Hibbs JB,Jr., Westenfelder C, Taintor R, Vavrin Z, Kablitz C, Baranowski RL, Ward JH, Menlove RL,McMurry MP, Kushner JP and Samlowski WE. Evidence for cytokine-inducible nitric oxide synthesisfrom L- arginine in patients receiving interleukin-2 therapy. J. Clin. Invest. 1992; 89: 867-877.
145. Belldegrun A, Webb DE, Austin III HA, Steinberg SM, White DE, Linehan WM and Rosenberg SA.Effects of interleukin-2 on renal function in patients receiving immunotherapy for advanced cancer.Ann. Intern. Med. 1987; 106: 817-822.
146. Shalmi CL, Dutcher JP, Feinfeld DA, Chun KJ, Saleemi KR, Freeman LM, Lynn RI and Wiernik PH.Acute renal dysfunction during interleukin-2 treatment: suggestion of an intrinsic renal lesion. J. Clin.Oncol. 1990; 8: 1839-1846.
147. Webb DE, Austin III HA, Belldegrun A et al. Metabolic and renal effects of interleukin-2immunotherapy for metastatic cancer. Clin. Nephr. 1988; 30: 141-145.
148. Belldegrun A, Webb DE, Austin III HA, Steinberg SM, Lineham WM and Rosenberg SA. Renaltoxicity of interleukin-2 administration in patients with metastatic renal cell cancer: effect of pre-therapy
43

nephrectomy. J. Urol. 1989; 141: 499-503.149. Schwartzentruber D, Lotze MT and Rosenberg SA. Colonic perforation. An unusual complication of
therapy with high dose interleukin-2. Cancer 1988; 11: 2350-2353.150. Sparano JA, Dutcher JP, Kaleya R, Caliendo G, Fiorito J, Mitsudo S, Shechner R, Boley SJ, Gucalp
R, Ciobanu N, Grima K, Wiernik PH and Brandt LJ. Colonic ischemia complicating immunotherapywith interleukin-2 and interferon-alpha. Cancer 1991; 68: 1538-1544.
151. Sparano JA, Brandt LJ, Dutcher JP, DuBois JS and Atkins MB. Symptomatic exacerbation of Crohndisease after treatment with high-dose interleukin-2. Ann. Intern. Med. 1993; 118: 617-618.
152. Fisher B, Keenan AM, Garra BS, Steinberg SM, White DE, DiBisceglie AM, Hoofnagle JH, Yolles P,Rosenberg SA and Lotze MT. Interleukin-2 induces profound reversible cholestasis: a detailed analysisin treated cancer patients. J. Clin. Oncol. 1989; 7: 1852-1862.
153. Atkins MB, Mier JW, Parkinson DR, Gould JA, Berkman EM and Kaplan MM. Hypothyroidism aftertreatment with interleukin-2 and lymphokine-activated killer cells. N. Engl. J. Med. 1988; 318:1557-1563.
154. Mattijssen VJM, Mulder de PHM, Liessum van PA, Corstens FHM, Franks CR and Wagener DTW.Hypothyroidism and goiter in a patient during treatment with interleukin-2. Cancer 1990; 65: 2686-2688.
155. Conlon KC, Urba WJ, Smith JW, Steis RG, Longo DL and Clark JW. Exacerbation of symptoms ofautoimmune disease in patients receiving alpha-interferon therapy. Cancer 1990; 65: 2237-2242.
156. Kirchner H, Korfer A, Palmer PA, Evers P, De Riese W, Knuver-Hopf J, Hadam M, Goldman U,Franks CR, Poliwoda H et al. Subcutaneous interleukin-2 and interferon-alpha 2b in patients withmetastatic renal cell cancer: the German outpatient experience. Mol. Biother. 1990; 2: 145-154.
157. Pichert G, Jost LM, Zobeli L, Odermatt B, Pedia G and Stahel RA. Thyroiditis after treatment withinterleukin-2 and interferon alpha-2a. Br. J. Cancer 1990; 62: 100-104.
158. Scalzo S, Gengaro A, Boccoli G, Masciulli R, Giannella G, Salvo G, Marolla P, Carlini P, MassiminiG, Holdener EE et al. Primary hypothyroidism associated with interleukin-2 and interferon alpha-2therapy of melanoma and renal carcinoma. Eur. J. Cancer 1990; 26: 1152-1156.
159. Pichert G, Jost LM, Fierz W and Stahel RA. Clinical and immune modulatory effects of alternativeweekly interleukin-2 and interferon alfa-2a in patients with advanced renal cell carcinoma andmelanoma. Br. J. Cancer 1991; 63: 287-292.
160. Kruit WH, Bolhuis RL, Goey SH, Jansen RL, Eggermont AM, Batchelor D, Schmitz PI and Stoter G.Interleukin-2-induced thyroid dysfunction is correlated with treatment duration but not with tumorresponse. J. Clin. Oncol. 1993; 11: 921-924.
161. Weijl NI, Van der Horst D, Brand A, Kooy Y, Van Luxemburg S, Schroder J, Eentjes E, Van RoodJJ, Cleton FJ and Osanto S. Hypothyroidism during immunotherapy with interleukin-2 is associated withantithyroid antibodies and response to treatment. J. Clin. Oncol. 1993; 11: 1376-1383.
162. Reid I, Sharpe I, McDevitt J, Maxwell W, Emmons R, Tanner WA and Monson JR. Thyroiddysfunction can predict response to immunotherapy with interleukin-2 and interferon-2 alpha. Br. J.Cancer 1991; 64: 915-918.
163. Denicoff KD, Durkin TM, Lotze MT, Quinlan PE, Davis CL, Listwak SJ, Rosenberg SA and RubinowDR. The neuroendocrine effects of interleukin-2 treatment. J. Clin. Endocrinol. Metab. 1989; 69:402-410.
164. Lissoni P, Barni S, Archili C, Cattaneo G, Rovelli F, Conti A, Maestroni GJ and Tancini G. Endocrineeffects of a 24-hour intravenous infusion of interleukin-2 in the immunotherapy of cancer. AnticancerRes. 1990; 10: 753-757.
165. Lissoni P, Barni S, Rovelli F, Crispino S, Fumagalli G, Pescia S, Vaghi M, Camesasca G and TanciniG. Neuroendocrine effects of subcutaneous interleukin-2 injection in cancer. Tumori. 1991; 77: 212-215.
166. Denicoff KD, Rubinow DR, Papa MZ and Seipp CA. The neuropsychiatric effects of treatment withinterleukin-2 and lymphokine activated killer cells. Ann. Intern. Med. 1987; 107: 293-300.
167. Saris SC, Patronas NJ, Rosenberg SA, Alexander JT and Frank J. The effect of intravenousinterleukin-2 on brain water content. J. Neurosurg. 1989; 71: 169-174.
168. Vecht CJ, Keohane C, Menon RS, Punt CJA and Stoter G. Acute fatal leukoencephalopathy afterinterleukin-2 therapy. N. Engl. J. Med. 1990; 323: 1146-1147.
169. Gaspari G, Lotze MT, Rosenberg SA, Stern JB and Katz SI. Dermatological changes associated withinterleukin-2 administration. JAMA 1987; 258: 1624-1629.
44

170. Weinstein A, Brijak D, Mittelman A et al. Erythema nodosum in a patient with renal celll carcinomatreated with interleukin-2 and lymphokine activated killer cells. JAMA 1987; 258: 3120-3121.
171. Baars JW, Wagstaff J, Hack CE, Wolbink GJ, Eerenberg-Belmer AJM and Pinedo HM. Angioneuroticoedema and urticaria during therapy with interleukin-2. Br. J. Cancer 1992; 3: 243-244.
172. Baars JW, Coenen JL, Wagstaff J, Van der Valk P and Pinedo HM. Lobular panniculitis aftersubcutaneous administration of interleukin-2 (IL-2), and its exacerbation during intravenous therapy withIL-2. Br. J. Cancer 1992; 66: 698-699.
173. Ramseur WL, Richards F,II. and Duggan DB. A case of fatal pemphigus vulgaris in association withbeta interferon and interleukin-2 therapy. Cancer 1989; 63: 2005-2007.
174. Sleijfer DT, Janssen RA, Buter J, De Vries EGE, Willemse PHB and Mulder NH. Phase II study ofsubcutaneous interleukin-2 in unselected patients with advanced renal cell cancer on an outpatient basis.J. Clin. Oncol. 1992; 10: 1119-1123.
175. Lee RE, Gaspari AA, Lotze MT et al. Interleukin-2 and psoriasis. Arch. Dermatol. 1988; 124:1811-1815.
176. Van Haelst Pisani C, Kovach JS, Kita H, Leiferman KM, Gleich GJ, Silver JE, Dennin R and AbramsJS. Administration of interleukin-2 (IL-2) results in increased plasma concentrations of IL-5 andeosinophilia in patients with cancer. Blood 1991; 78: 1538-1544.
177. Paciucci PA, Mandeli J, Oleksowicz L, Ameglio F and Holland JF. Thrombocytopenia duringimmunotherapy with interleukin-2 by constant infusion. JAMA 1990; 89: 308-312.
178. Richards JM, Gilewski TA and Vogelzang NJ. Association of interleukin-2 therapy with staphylococcalbacteriemia. Cancer 1991; 67: 1570-1575.
179. Snydman DR, Sullivan B, Gill M, Gould JA, Parkinson DR and Atkins MB. Nosocomial sepsisassociated with interleukin-2 see comments. Ann. Intern. Med. 1990; 112: 102-107.
180. Lim SH, Giles FJ, Smith MP and Goldstone AH. Bacterial infections in lymphoma patients treated withrecombinant interleukin-2 infusion. Acta Haematol. 1991; 85: 135-138.
181. Pockaj BA, Topalian SL, Steinberg SM, White DE and Rosenberg SA. Infectious complicationsassociated with interleukin-2 administration: A retrospective review of 935 treatment courses. J. Clin.Oncol. 1993; 11: 136-147.
182. Buter J, De Vries EGE, Sleijfer DT, Willemse PHB and Mulder NH. Infection after subcutaneousinterleukin-2. Lancet 1992; 339: 552.
183. Klempner MS, Noring R, Mier JW and Atkins MB. An acquired chemotactic defect in neutrophils frompatients receiving interleukin-2 immunotherapy see comments. N. Engl. J. Med. 1990; 322: 959-965.
184. Mier JW, Vachino G, Klempner MS, Aronson FR, Noring R, Smith S, Brandon EP, Laird W andAtkins MB. Inhibition of interleukin-2-induced tumor necrosis factor release by dexamethasone:prevention of an acquired neutrophil chemotaxis defect and differential suppression of interleukin-2associated side effects. Blood 1990; 76: 1933-1940.
185. Rosenberg SA, Lotze MT, Yang JC, Linehan WM, Seipp C, Calabro S, Karp SE, Sherry RM, SteinbergS and White DE. Combination therapy with interleukin-2 and alpha-interferon for the treatment ofpatients with advanced cancer. J. Clin. Oncol. 1989; 7: 1863-1874.
186. Figlin RA, Abi-Aad AS, Belldegrun A and deKernion JB. The role of interferon and interleukin-2 inthe immunotherapeutic approach to renal cell carcinoma. Semin. Oncol. 1991; 18: 102-107.
187. Von Rohr A, Ghosh AK, Thatcher N and Stern PL. Immunomodulation during prolonged treatment withcombined interleukin-2 and interferon-alpha in patients with advanced malignancy. Br. J. Cancer 1993;67: 163-171.
188. Yang SC, Grimm EA, Parkinson DR, Carinhas J, Fry KD, Mendiguren-Rodriguez A, Licciardello J,Owen-Schaub LB, Hong WK and Roth JA. Clinical and immunomodulatory effects of combinationimmunotherapy with low-dose interleukin 2 and tumor necrosis factor alpha in patients with advancednon-small cell lung cancer: a phase I trial. Cancer Res. 1991; 51: 3669-3676.
189. McIntosh JK, Mule JJ, Merino MJ and Rosenberg SA. Synergistic anti-tumor effects of immunotherapywith recombinant interleukin-2 and recombinant tumor necrosis factor-alfa. Cancer Res. 1988; 48:4011-4017.
190. Zimmerman RJ, Gauny S, Chan A, Landre P and Winkelhake JL. Sequence dependence ofadministration of human tumor necrosis factor and interleukin-2 in murine tumor therapy. J. Natl.Cancer Inst. 1989; 81: 227-231.
191. Lissoni P, Pittalis S, Brivio F, Tisi E, Rovelli F, Ardizzoia A, Barni S, Tancini G, Giudici G, Biondi
45

A, Conti A and Maestroni G. In vitro modulatory effects of interleukin-3 on macrophage activationinduced by interleukin-2. Cancer 1993; 71: 2076-2081.
192. Mitchell MS, Kempf RA, Harel W, Shau H, Boswell WD, Lind S and Bradley EC. Effectiveness andtolerability of low dose cyclophosphamide and low-dose intravenous interleukin-2 disseminatedmelanoma. J. Clin. Oncol. 1988; 6: 409-424.
193. Mitchell MS. Chemotherapy in combination with biomodulation: a 5-year experience withcyclophosphamide and interleukin-2. Semin. Oncol. 1992; 19: 80-87.
194. Dillman RO, Oldham RK, Barth NM, Birch R, Arnold J and West WH. Recombinant interleukin-2 andadoptive immunotherapy alternated with dacarbazine therapy in melanoma: a National Biotherapy StudyGroup trial. J. Natl. Cancer Inst. 1990; 82: 1345-1349.
195. Khayat D, Borel C, Tourani JM, Benhammouda A, Antoine E, Rixe O, Vuillemin E, Bazex PA, ThillL, Franks R, Auclerc G, Soubrane C, Banzet P and Weil M. Sequential chemoimmunotherapy withcisplatin, interleukin-2, and interferon alfa-2a for metastatic melanoma. J. Clin. Oncol. 1993; 11:2173-2180.
196. Richards JM, Mehta N, Ramming K and Skosey P. Sequential chemoimmunotherapy in the treatmentof metastatic melanoma. J. Clin. Oncol. 1992; 10: 1338-1343.
197. Cameron RB, McIntosh JK and Rosenberg SA. Synergistic antitumor efects of combinationimmunotherapy with interleukin-2 and an recombinant hybrid interferon-alpha in the treatment ofestablished murine hepatic metastases. Cancer Res. 1988; 48: 5810-5817.
198. Chikkala NF, Lewis I, Ulchaker J, Stanley J, Tubbs R and Finke JH. Interactive effects ofalpha-interferon A/D and interleukin 2 on murine lymphokine-activated killer activity: analysis at theeffector and precursor level. Cancer Res. 1990; 50: 1176-1182.
199. Weber JS and Rosenberg SA. Effects of murine tumor class I major histocompatibility complexexpression on antitumor activity of tumor-infiltrating lymphocytes. J. Natl. Cancer Inst. 1990; 82:755-761.
200. Tanaka K, Yoshioka T, Bieberich C and Jay G. Role of the major histocompatibility complex class Iantigens in tumor growth and metastasis. Ann. Rev. Immunol. 1988; 6: 359-380.
201. Schiller JH, Hank J, Storer B, Borchert AA, Moore KH, Albertini M, Bechhofer R, Wesley O, BrownRR, Bastin AM and Sondel PM. A direct comparison of immunological and clinical effects ofinterleukin 2 with and without interferon-α in humans. Cancer Res. 1993; 53: 1286-1292.
202. West W, Schwartzberg L, Blumenchein G et al. Continuous infusion interleukin-2 plus subcutaneousinterferon alpha in advanced malignancy. Proc. Am. Soc. Clin. Oncol. 1990; 9: 191. (Abstract)
203. Demchak P, Atkins M, Sell K et al. Phase II study of interleukin-2 (IL-2) and interferon alpha-2a(IFN-α) outpatient therapy for metastatic renal cancer. Proc. Am. Assoc. Cancer Res. 1991; 32: 191.(Abstract)
204. Figlin RA, Belldegrun A, Moldawer N, Zeffren J and deKernion JB. Concomitant administration ofrecombinant human interleukin-2 and recombinant interferon alfa-2A: an active outpatient regimen inmetastatic renal cell carcinoma. J. Clin. Oncol. 1992; 10: 414-421.
205. Budd GT, Murthy S, Finke J, Sergi J, Gibson V, Medendorp S, Barna B, Boyett J and Bukowski RM.Phase I trial of high-dose bolus interleukin-2 and interferon alfa-2a in patients with metastaticmalignancy. J. Clin. Oncol. 1992; 10: 804-809.
206. Thomas H, Barton C, Saini A, Dalgleish A and Waxman J. Sequential interleukin-2 and alpha interferonfor renal cell carcinoma and melanoma. Eur. J. Cancer 1992; 28A: 1047-1049.
207. Ilson DH, Motzer RJ, Kradin RL, Vogelzang NJ, Bajorin DF, Scher HI, Nanus D, O’Moore P,Marathias K and Bosl GJ. A phase II trial of interleukin-2 and interferon alfa-2a in patients withadvanced renal cell carcinoma. J. Clin. Oncol. 1992; 10: 1124-1130.
208. Wang JCL, Walle A, Novogrodsky A, Suthanthiran M, Silver RT, Bander NH, Rubin AL and StenzelKH. A phase II clinical trial of adoptive immunotherapy for advanced renal cell carcinoma usingmitogen-activated autologous leucocytes and continous infusion interleukin-2. J. Clin. Oncol. 1989; 7:1885-1891.
209. Krigel RL, Radavic-Shaller KA, Rudolph AR, Konrad M, Bradley ED and Comis RL. Renal cellcarcinoma: treatment with recombinant interleukin-2 plus beta-interferon. J. Clin. Oncol. 1990; 8:460-467.
210. Negrier S, Ravaud A, Bui BN, Rebattu P, Lakdja F, Merrouche Y, Clavel M and Philip T.Subcutaneous interleukin-2 (IL-2) and interferon alpha (IFN) in metastatic renal cell cancer (MRCC):
46

a double institution study on 37 patients. Eur. J. Cancer 1991; suppl. 2: S233-A1365. (Abstract)211. Dutcher JP, Fisher RI, Weiss G, Aronson FR, Margolin K, Caliendo G, Louie A and Atkins M. An
outpatient (OPT) regimen of subcutaneous (SC) interleukin-2 (IL2) plus alpha-interferon (IFN) inmetastatic renal cell cancer (RCC). Proc. Am. Soc. Clin. Oncol. 1993; 12: 248. (Abstract)
212. Enzinger HM, Bergmann L, Fenchel K, Neugebauer T, Jahn B et al. Daily alternating schedules ofinterferon-α and interleukin-2 in advanced cancer - clinical results and biological effects. Onkologie1992; 24 (Suppl. 1): P-10. (Abstract)
213. Lipton A, Harvey H, Givant E, Hopper K, Lawler J et al. Interleukin-2 and interferon-α-2a outpatienttherapy for metastatic renal cell carcinoma. J. Immunother. 1993; 13: 122-129.
214. Keilholz U, Scheibenbogen C, Bergmann L, Tilgen W and Hunstein W. IFN-α and IL-2 in metastaticmelanoma: comparizon of two phase II trials. Onkologie 1992; 15 (Suppl. 1): 17. (Abstract)
215. Kirchner H, Lopez Haenninen E, Volkenandt M and Atzpodien J. Chemoimmunotherapy of advancedmalignant melanoma with carboplatin and DTIC followed by subcutaneous interleukin-2 andinterpheron-alpha. Proc. Am. Soc. Clin. Oncol. 1993; 12: 1356. (Abstract)
216. Kruit WH, Goey SH, Monson JR, Stahel RA, Calabresi F, Mertelsmann R, Holdener EE, EggermontAM, Bolhuis RL, De Mulder PHM et al. Clinical experience with the combined use of recombinantinterleukin-2 (IL2) and interferon alfa-2a (IFN alpha) in metastatic melanoma. Br. J. Haematol. 1991;79 Suppl 1P 84-6. XX:
217. Chouaib S, Bertoglio J, Blay J, Marchiol-Fournigault C and Fradelizi D. Generation oflymphokine-activated killer cells: synergy between tumor necrosis factor and interleukin-2. Proc. Natl.Acad. Sci. U. S. A. 1988; 85: 6875-6879.
218. Verstovsek S, Maccubbin D, Ehrke MJ and Mihich E. Tumoricidal activation of murine residentperitoneal macrophages by interleukin 2 and tumor necrosis factor alpha. Cancer Res. 1992; 52:3880-3885.
219. Quesada JR, Talpaz M, Rios A, Kurzrock R and Gutterman JU. Clinical toxicity of interferons in cancerpatients. J. Clin. Oncol. 1986; 4: 234-243.
220. Goldstein D and laszlo J. Interferon therapy in cancer: from imaginon to interferon. Cancer Res. 1986;46: 4315.
221. Dorr RT. Interferon-α in malignant and viral diseases. A review. Drugs 1993; 45(2): 177-211.222. Hansen RM and Borden EC. Current status of interferons in the treatment of cancer. Oncology
(Huntingt). 1992; 6: 19-24; discus.223. Isaacs H and Lindemann J. Virus interference: 1. The interferon. Proc. R. Soc. Lond. [Biol]. 1957; 147:
257-262.224. Adolf GR. Antigenic structure of human interferonΩ1 (interferon aplha II1): comparison with other
human interferons. J. Gen. Virol. 1987; 68: 1669-1676.225. Tan YH. Chromosome 21 and the cell growth inhibitory effect of humaninterferon prepartations. Nature
1976; 260: 141-143.226. Rashidbaigi A, Langer JA, Jung V et al. The gene for the human immune interferon receptor is located
on chromosome 6. Proc. Natl. Acad. Sci. U. S. A. 1986; 83: 384-388.227. Becker S. Interferon-τ accelerates immune proliferation via its effect on monocyte HLA-DR expression.
Cell. Immunol. 1985; 91: 301-307.228. Wills RJ, Dennis S, Spiegel HE, Gibson DM, Nadler PI et al. Interferon kinetics and adverse reactions
after intravenous, intramuscular, and subcutaneous injection. Clin. Pharm. Ther. 1984; 35: 755-757.229. Radwanski E, Perentesis G, Oden E, Jacobs S, Affrime M et al. Pharmakokinetics of IFN-α-2b in
healthy volunteers. J. Clin. Pharmacol. 1987; 27: 432-435.230. Tamura T, Sasaki Y, Shinkai T, Eguchi K, Sakurai M, Fujiwara Y, Nakagawa K, Minato K and Saijo
N. Phase I study of combination therapy with interleukin 2 andβ-interferon in patients with advancedmalignancy. Cancer Res. 1989; 49: 730-735.
231. Kinney P, Triozzi P and Young D. Phase II trial of interferon-beta-serine in metastatic renal cellcarcinoma. J. Clin. Oncol. 1990; 8: 881-885.
232. Greiner JW, Guadagni F, Hand PH, Pestka S, Noguchi P, Fisher PB and Schlom J. Augmentation oftumor antigen expression by recombinant human interferons: enhanced targeting of monoclonalantibodies to carcinomas. Cancer Treat. Res. 1990; 51P 413-32. XX:
233. Aulitzky W, Gastl G, Aulitzky WE et al. Successful treatment of metastatic renal cell carcinoma witha biological active dose of recombinant interferon-gamma. J. Clin. Oncol. 1989; 7(12): 1875-1884.
47

234. Ernstoff MS, Gooding W, Nair S, Bahnson RR, Miketic LM, Banner B, Day R, Whiteside T,Titus-Ernstoff L and Kirkwood JM. Immunological effects of treatment with sequential administrationof recombinant interferon gamma and alpha in patients with metastatic renal cell carcinoma during aphase I trial. Cancer Res. 1992; 52: 851-856.
235. Ernstoff MS, Nair S, Bahnson RR, Miketic LM, Banner B, Gooding W, Day R, Whiteside T, HakalaT and Kirkwood JM. A phase IA trial of sequential administration recombinant DNA- producedinterferons: combination recombinant interferon gamma and recombinant interferon alfa in patients withmetastatic renal cell carcinoma. J. Clin. Oncol. 1990; 8: 1637-1649.
236. Weiner LM, Padavic-Shaller K, Kitson J, Watts P, Krigel RL and Litwin S. Phase I evaluation ofcombination therapy with interleukin 2 and gamma-interferon. Cancer Res. 1991; 51: 3910-3918.
237. Escudier B, Farace F, Angevin E, Triebel F, Antoun S, Leclerc B, Brandely M, Aboudaram A,Nitenberg G and Hercend T. Combination of interleukin-2 and gamma interferon in metastatic renal cellcarcinoma. Eur. J. Cancer 1993; 29A: 724-728.
238. Baars JW, Wagstaff J, Van Groeningen CJ, Vermorken JB, Bijvank EM, Pinedo HM and Nauta JJ.Phase II study of interferon-gamma and interleukin-2: tachyphylaxis of toxicity to the liver duringincreasing immune enhancement letter. J. Natl. Cancer Inst. 1993; 85: 410-411.
239. Urba WJ, Kopp WC, Clark JW, Smith II JW, Steis RG, Huber C, Coggin D and Longo DL. The invivo immunomodulatory effects of recombinant interferon gamma plus recombinant tumor necrosisfactor-alfa. J. Clin. Oncol. 1991; 10: 1831-1839.
240. Talpaz M, Kantarjian H, Kurzrock R, Trujillo JM and Gutterman JU. Interferon-alpha producessustained cytogenetic responses in chronic myelogenous leukemia. Philadelphia chromosome-positivepatients. Ann. Intern. Med. 1991; 114: 532-538.
241. Muss HB. Interferon therapy for renal cell carcinoma. Semin. Oncol. 1987; 14 (suppl 2): 36-42.242. Kirkwood JM, Harris JE, Vera R, Sandler S, Fischer DS, Khandekar J, Ernstoffo MS, Gordon L, Lutes
R, Boninie P, Lytton B, Gobleigh M and Taylor SJ. A randomized study of low and high doses ofleucocyte-α-interferon in metastatic renal cell carcinoma: the American Cancer Society collaborativetrial. Cancer Res. 1985; 45: 863-871.
243. Quesada JR, Rios A, Swanson DA, Trown P and Gutterman JU. Antitumor activity ofrecombinant-derived interferon alpha in metastatic renal cell carcinoma. J. Clin. Oncol. 1985; 3:1522-1528.
244. Muss HB, Constanzi JJ, Leavit R, Williams RD and Kempf RA. Recombinant alfa interferon in renalcell carcinoma: A randomized trial of two routes of administration. J. Clin. Oncol. 1987; 5: 286-291.
245. Kirkwood JM. Studies of interferons in the therapy of melanoma. Semin. Oncol. 1991; 18: 83-90.246. Creagan ET, Ahmann DL, Frytak S, Long HJ and Itri M. Recombinant leucocyte A interferon
(rIFN-alpha A) in the treatment of disseminated malignant melanoma: analysis of complete and longterm responding patients. Cancer 1986; 58: 2576.
247. Creagan ET, Ahmann DL, Green SJ, Long HJ, Frytak S and Itri LM. Phase II study of recombinantleukocyte A interferon (IFN-rA) plus cimetidine in disseminated malignant melanoma. J. Clin. Oncol.1985; 3: 977.
248. De Wit R, Danner SA, Bakker PJ, Lange JM, Eeftinck Schattenkerk JK and Veenhof CH. Combinedzidovudine and interferon-alpha treatment in patients with AIDS-associated Kaposi’s sarcoma. J. Intern.Med. 1991; 229: 35-40.
249. Falkson CI, Falkson G and Falkson HC. Improved results with the addition of interferon alfa-2b todacarbazine in the treatment of patients with metastatic malignant melanoma. J. Clin. Oncol. 1991; 9:1403-1408.
250. Sertoli MR, Queirolo P, Bajetta E, Negretti E, Calabresi F, Barduagni L, Giannotti B, Brogelli L,Bernengo MG, Sofra MC, Maifredi G, Zumiani G, Comella G, Bruzzoni R, DiLeo A, et al. Dacarbazine(DTIC) with or without recombinant interferon alpha-2a at different dosages in the treatment of stageIV melanoma patients. Prilimary results of a randomized trial. Proc. Am. Soc. Clin. Oncol. 1992; 11:1185. (Abstract)
251. Kirkwood JM, Ernstoff MS, Giuliano A, Gams R, Robinson WA, Costanzi J, Pouillart P, Speyer J,Grimm M and Spiegel R. Interferon alpha-2a and dacarbazine in melanoma. J. Natl. Cancer Inst. 1990;82: 1062-1063.
252. Thomson D, Adena M, McLeod GRC, Hersey P, Gill P, Coates A, Olver I, Kefford R, Lowenthal R,Beadle G, Walpole E, Boland K and Kingston D. Interferonα-2a (IFN) does not improve response or
48

survival when added to dacarbazine(DTIC) in metastatic melanoma: results of a multi-institutionalaustralian randomised trial QMP8704. Proc. Am. Soc. Clin. Oncol. 1992; 11: 1177. (Abstract)
253. Rozenbaum W, Gharakhanian S, Navarette MS, De Sahb R, Cardon B and Rouzioux C. Long-termfollow-up of 120 patients with AIDS-related Kaposi’s sarcoma treated with interferon alpha-2a. J.Invest. Dermatol. 1990; 95: 161S-165S.
254. Krown SE, Gold JW, Niedzwiecki D, Bundow D, Flomenberg N, Gansbacher B and Brew BJ.Interferon-alpha with zidovudine: safety, tolerance, and clinical and virologic effects in patients withKaposi sarcoma associated with the acquired immunodeficiency syndrome (AIDS) published erratumappears in Ann Intern Med 1990 Aug 15;113(4):334. Ann. Intern. Med. 1990; 112: 812-821.
255. Scadden DT, Bering HA, Levine JD, Bresnahan J, Evans L, Epstein C and Groopman JE.Granulocyte-macrophage colony-stimulating factor mitigates the neutropenia of combined interferon alfaand zidovudine treatment of acquired immune deficiency syndrome-associated Kaposi’s sarcoma. J.Clin. Oncol. 1991; 9: 802-808.
256. Silgals RM, Ahlgren JD and Neefe JR. A phase II trial of high-dose intravenous interferon alpha-2 inadvanced colorectal cancer. Cancer 1984; 54: 2257-2261.
257. Neefe JR, Sullivan JE, Ayoob M, Phillips E and Smith FP. Augmented immunity in cancer patientstreated withα-interferon. Cancer Res. 1985; 45: 874-878.
258. Schwartz EL, Hoffman M, O’Connor CJ and Wadler S. Stimulation of 5-fluorouracil metabolicactivation by interferon- alpha in human colon carcinoma cells. Biochem. Biophys. Res. Commun. 1992;182: 1232-1239.
259. Houghton JA, Adkins DA, Rahman A and Houghton PJ. Interaction between 5-fluorouracil,[6RS]leucovorin, and recombinant human interferon-α2a in cultured colon adenocarcinoma cells. CancerComm. 1991; 3: 225-231.
260. Sinnige HAM, Timmer-Bosscha H, Peters GF, De Vries EGE and Mulder NH. Combined modulationof leucovorin andα-2a interferon of fluoropyrimidine mediated growth inhibition. Anticancer Res.1993; 13: 1335-1340.
261. McBee P, Petraiuolo W and Katoh A. Inhibition of liver metastases in nude mice by the combinedaction of 5-fluorouracil and interferon. Anticancer Drugs 1990; 1: 165-170.
262. Grem JL, McAtee N, Murphy RF, Balis FM, Steinberg SM, Hamilton JM, Sorensen JM, Sartor O,Kramer BS, Goldstein LJ et al. A pilot study of interferon alfa-2a in combination with fluorouracil plushigh-dose leucovorin in metastatic gastrointestinal carcinoma. J. Clin. Oncol. 1991; 9: 1811-1820.
263. Grem JL, Chu E, Boarman D, Balis FM, Murphy RF, McAtee N and Allegra CJ. Biochemicalmodulation of fluorouracil with leucovorin and interferon: preclinical and clinical investigations. Semin.Oncol. 1992; 19: 36-44.
264. Wadler S and Wiernik PH. Clinical update on the role of fluorouracil and recombinant interferon alfa-2ain the treatment of colorectal carcinoma. Semin. Oncol. 1990; 17: 16-21; discus.
265. Wadler S, Lembersky B, Atkins M, Kirkwood J and Petrelli N. Phase II trial of fluorouracil andrecombinant interferon alfa- 2a in patients with advanced colorectal carcinoma: an Eastern CooperativeOncology Group study. J. Clin. Oncol. 1991; 9: 1806-1810.
266. Sinnige HAM, Buter J, De Vries EGE, Uges DRA, Roenhorst HW, Verschueren RCJ, Sleijfer DTh,Willemse PHB and Mulder NH. Phase I-II study of the addition ofα-2a interferon to5-fluorouracil/leucovorin. Pharmacokinetic interaction ofα-2a interferon and leucovorin. Eur. J. Cancer1993; 29A(12): 1715-1720.
267. Kvols LA. Metastatic carcinoid tumors and the carcinoid syndrome. A selective review of chemotherapyand hormonal therapy. Am. J. Med. 1986; 81,(Suppl 6B): 49-55.
268. Moertel CG. An Odyssey in the land of small tumors. J. Clin. Oncol. 1987; 5: 1503-1522.269. Kvols LK, Moertel CG, O’Connel MJ, Schutt AJ, Rubin J and Hahn RG. Treatment of the malignant
carcinoid syndrome. Evaluation of a long-acting somatostatin analogue. N. Engl. J. Med. 1986; 315:663-666.
270. Vinik AJ, Thompson N, Eckhauser F and Moatarri AR. Clinical features of the carcinoid syndrome andthe use of somatostatin analogue in its management. Acta Oncol. 1989; 28: 389-402.
271. Öberg K, Funa K and Alm G. Effects of leucocyte interferon on clinical symptoms and hormone levelsin patients with mid-gut carcinoid tumors and carcinoid syndrome. N. Engl. J. Med. 1983; 309: 129-133.
272. Öberg K, Norheim I, Lind E, Alm G, Lundqvist G, Wide L, Jonsdotter B, Magnusson A and WilanderE. Treatment of malignant carcinoid tumors with human leucocyte interferon: long term results. Cancer
49

Treat. Rep. 1986; 70: 1297-1304.273. Smith DB, Scarfee JH, Wagstaff J and Johnston RJ. Phase II trial of rDNA alfa 2b interferon in patients
with malignant carcinoid tumor. Cancer Treat. Rep. 1987; 71: 1265-1266.274. Öberg K, Alm G, Magnusson A, Lundqvist G, Theodorsson E, Wide L and Wilander E. Treatment of
malignant carcinoid tumors with recombinant interferon alfa-2b: development of neutralizing antibodiesand possible loss of antitumor activity. J. Natl. Cancer Inst. 1989; 81: 531-535.
275. Hanssen LE, Schrumpf E, Kolbenstved AN, Tausjo J and Dolva LO. Treatment of malignant metastaticmidgut carcinoid tumours with recombinant humanα2b interferon with or without prior hepatic arteryembolization. Scand. J. Gastroenterol. 1989; 24: 787-795.
276. Moertel CG, Rubin J and Kvols LK. Therapy of metastatic carcinoid tumor an the malignant carcinoidsyndrome with recombinant leucocyte A interferon. J. Clin. Oncol. 1989; 7: 865-868.
277. Veenhof CHN, De Wit R, Taal BG, Dirix LY, Wagstaff J, Hensen A, Huldij AC and Bakker PJM. Adose escalation study of recombinant interferon-alpha in patients with a metastatic carcinoid tumour.Eur. J. Cancer 1992; 28: 75-78.
278. Biesma B, Willemse PHB, Mulder NH, Verschueren RCJ, Kema IP, De Bruijn HWA, Postmus PE,Sleijfer DTh and De Vries EGE. Recombinant interferon alpha-2b in patients with metastatic apudomas:effect on tumours and tumour markers. Br. J. Cancer 1992; 66: 850-855.
279. Berek JS, Hacker NF, Lichtenstein A, Jung T, Spina C, Knox RM, Brady J, Greene T, Ettinger LM,Lagasse LD, Bonnem EM, Spiegel RJ and Zighelboim J. Intraperitoneal recombinant interferon for‘salvage‘ immunotherapy in stage III epithelian ovarian cancer: a gynaecologic oncology group study.Cancer Res. 1985; 45: 4447-4453.
280. Willemse PHB, De Vries EGE, Mulder NH, Aalders JG, Bouma J and Sleijfer DTh. Intraperitonealhuman recombinant interferon alpha-2b in minimal residual ovarian cancer. Eur. J. Cancer 1990; 26:353-358.
281. Bezwoda WR, Golombick T, Dansey R and Keeping J. Treatment of malignant ascites due torecurrent/refractory ovarian cancer: the use of interferon-alpha or interferon-alpha plus chemotherapyin vivo and in vitro. Eur. J. Cancer 1991; 27: 1423-1429.
282. Nardi M, Cognetti F, Giulia MD, Sternberg C, Lombardi A et al. Intraperitoneal rα2-interferon (IFN)alternating with cisplatin (DDP) as salvage therapy for minimal residual disease ovarian cancer. Proc.Am. Soc. Clin. Oncol. 1989; 8: 157. (Abstract)
283. Bartoletti R, Massimini G, Criscuolo D and Rizzo M. Interferon alfa 2a in superficial bladder cancerprophylaxis: toleration and long-term follow-up. A phase I-II study. Anticancer Res. 1991; 11:2167-2170.
284. Ezekowitz RA, Mulliken JB and Folkman J. Interferon alfa-2a therapy for life-threatening hemangiomasof infancy see comments. N. Engl. J. Med. 1992; 326: 1456-1463.
285. White CW, Wolf SJ, Korones DN, Sondheimer HM, Tosi MF and Yu A. Treatment of childhoodangiomatous diseases with recombinant interferon alfa-2a. J. Pediatr. 1991; 118: 59-66.
50

Chapter 2
Phase II study of subcutaneous interleukin-2 in unselectedpatients with advanced renal cell cancer
on an outpatient basis
D. Th. Sleijfer, R. A. J. Janssen, J. Buter, E. G. E. De Vries, P. H. B. Willemse,
and N. H. Mulder.
Department of Medical Oncology, University Hospital, Oostersingel 59,9713 EZ Groningen, The Netherlands.
Summary
Purpose: A single-institution phase II study was undertaken to evaluate the efficacy andtoxicity of interleukin-2 (IL-2) administration by subcutaneous injection.
Patients and Methods:Twenty-seven unselected patients (15 male) with a mean age of 60
years (range, 42 to 76 years) who had advanced renal cell cancer were treated as outpatients.IL-2 was given once a day, 5 days per week for 6 weeks. During the first 5-day cycle, 18 x
106 IU was given once daily; in the following cycles, the doses in the first 2 days were
reduced to 9 x 106 IU. After a 3-week rest period, treatment was repeated in patients who hada response or stable disease (SD). To prevent pyretic reactions, patients also received
acetaminophen (250 to 500 mg given orally every 4 to 6 hours).Results: After 6 weeks, 26 patients were assessable for response. Two patients (8%) had a
complete remission (CR), four (15%) had a partial remission (PR), and 13 (50%) had SD.
A second cycle was given to 19 patients; one patient with a PR and six with SD showedprogression. Duration of CR the was 17+ and 19+ months, and length of the PR was 2, 8,
11, and 11+ months. The median survival of the patients who were nonresponders and
responders was 10 and 20+ months, respectively, and for all patients was 13 months. Onepatient died as a result of myocardial infarction and brain stem ischemia. Systemic side
effects in other patients were tolerated and accepted, and included transient inflammation andlocal induration at the injection sites, fever and chills, and nausea.
Conclusion: Subcutaneous IL-2 is clinically active, has an acceptable toxicity, and can be
given to patients with concomitant disease.
51

Introduction
Recombinant interleukin-2 (IL-2), a lymphokine produced by T-lymphocytes and natural-killer(NK) cells, is currently being explored in clinical trials as treatment for metastatic or
unresectable renal cell adenocarcinoma. The optimal dosage and scheduling of IL-2, with or
without autologous in vitro activated killer (LAK) cells has not been defined yet (1-6). IL-2toxicity is dose-related and is severe when given by intravenous (IV) bolus or infusion (7,8).
Therefore, entry criteria for phase II studies are defined strictly with regard to renal,pulmonary and cardiovascular function. Consequently, many patients are not eligible for these
trials because of concomitant disease.
In an attempt to reduce the toxicity of IL-2 administration, and to treat patients withadvanced renal cell cancer (RCC) who are not eligible for IV treatment, we initially
performed a feasibility study of a once-daily subcutaneous injection of 18 x 106 IU IL-2(unpublished observations). After 7 to 8 days, this schedule induced comparable toxicity
levels as has been described for IV IL-2 administration, which consisted of hypotension and
capillary leak. Although one 5-day cycle of 18 x 106 IU was given without toxicity, the nextcycle, which started after a 2-day rest period, induced toxicity. Therefore, the dose of IL-2
in the second and following cycles was reduced. This treatment schedule was evaluated in aphase II study in patients with RCC. Preliminary results were published previously (9).
Patients and methods
PatientsBetween December 1989 and December 1990, 27 consecutive patients with progressivehistologically proven advanced or disseminated RCC and measurable or assessable disease
were entered onto a phase II treatment study with subcutaneous IL-2 after informed consent
was obtained. Patient characteristics are listed in table I. There were no additional eligibilityor exclusion criteria. Concomitant diseases leading to a possible exclusion for intravenous IL-
2 are shown in table 2. One patient with a complete spinal cord lesion had a grade 3 WorldHealth Organization (WHO) performance, all other patients had grade 0 to 1 toxicity. In 23
of 27 patients a prior nephrectomy was performed. In four patients, disseminated disease and
concomitant medical contraindications for surgery precluded a palliative nephrectomy.After the patients were trained to administer the injections themselves, treatment
consisted of IL-2 (EuroCetus B.V., Amsterdam, the Netherlands) administered in a 5-daycycle subcutaneously every week for 6 consecutive weeks on an outpatient basis.
During the first 5-day cycle 18 x 106 IU were given once daily; in the following
cycles,
52

Table 1. Patient characteristics
No. treated 27
Sex, male/female 15/12
Age (years)
Mean 60
Range 42-76
Previous chemotherapy 1
Previous nephrectomy 23
Concomitant disease 15
Metastatic sites
Lung 20
Bone 5
Lymph nodes 5
Liver 3
Parotic gland 1
Skin 2
the dose in the first 2 days was reduced to 9 x 106 IU. After a 3-week rest period, the same
treatment was repeated in those patients with a complete response (CR), a partial response
(PR) or with stable disease (SD). Other treatment consisted of acetaminophen (250 to 500 mgorally every 4 to 6 hours) to prevent pyretic reactions. The study was approved by the
Medical Ethical Committee.
Assessment of response and toxicityBefore entry onto the study, patients were staged by full clinical examination, measurementof complete blood cell counts, serum electrolytes, creatinine clearance, liver and thyroid
function, chest radiograph, and computed tomographic (CT) scanning. Staging was repeatedafter completion of each 6-week treatment. Patients were examined twice weekly (day 1 and
6) during treatment. Toxicity was assessed according to standard WHO criteria during each
visit.A CR required the disappearance of all evidence of tumor for a minimum of 4
53

Table 2. Concomitant disease in 15 patients.
N
Previous myocardial infarction 1
Angina pectoris ≥ NYHA classII
5
Cardiac arrhythmias 3
Cardiac ischemias 3
Aortic-femoral bypass 2
Valvular heart disease 2
Complete spinal cord lesion 1
Porphyria, acute intermittent 1
Transient ischemic attacks 1
Abbreviation: N, number of diagnoses; NYHA, New York Heart Association.
weeks; a PR was registrated when a 50% or more decrease in the sum of the products of all
diameters of assessable lesions was reached; patients who had less than a PR or an increaseof less than 25% were classified as SD. Progression was defined as an increase of more than
25% or the development of new lesions. Responses were evaluated by the investigators aswell as by the independent reviewers.
The duration of the response was calculated from the moment the response was
reached. The overall survival was calculated from the start of the treatment. Survival curveswere plotted by using the Kaplan-Meier method (10), and statistical differences were
estimated by using the log-rank test (11). ReportedP values are two-sided.
Results
After 6 weeks treatment, 26 patients were assessable for response and 27 for toxicity. Twopatients had a CR, four had a PR, 13 patients had SD and seven patients progressed, which
led to a response rate of 23% (six of 26; 95% confidence limit [CI] 9% to 44%). A second
cycle of 6-week treatment was given to 19 patients. One patient who had a PR showedprogression, as did 6 of the patients who had initially SD. With regard to disease site, one PR
was in the liver; all other remissions were in the lung. Length of the CRs was 19+ andTable
54

3. Characteristics of responding patients.
PtAge
(years) Sex
Performance
status(WHO grade)
Metastatic
sites
Intervalnephrectomy
dissemination(months) Response
Durationof
response(months)
Overallsurvival(months)
1 42 F 0 Lung 3 CR 19+ 21+
2 68 M 0 Pleura,
lung
6 PR 11 20
3 66 F 0 Lung <1 CR 17+ 19+
4 71 M 0 Lung <1 PR 8 16+
5 66 M 0 Lung, bone 60 PR 2 15+
6 64 F 0 Liver 36 PR 11+ 13+
Abbreviations: Pt, patient number; F, female; M, male; CR, complete response; PR, partial response
17+ months, and the length of the PRs 2, 8, 11 and 11+ months. In all patients, no further
treatment was given after the second 6-week cycle. The characteristics of the patients whoresponded are listed in Table 3. Figure 1A shows the pretreatment chest x-ray of patient no.
2 (Table 3) who had histologically proven pleural metastases, whereas Fig 1B shows the PRafter treatment. The median survival of all patients was 13 months (Fig 2), whereas the
median survival of both nonresponders and responders was 10 and 20+ months (P=.01),
respectively (Fig 3).We could not find a difference between the characteristics of responders and
nonresponders in regard to performance status, prior nephrectomy, and sites of metastases.
This may be due to the small number of responders.Subcutaneous treatment was well tolerated, but transient inflammation and local
induration at the injection sites occurred in all patients; however this was not a dose-limitingtoxicity. After subcutaneous treatment was discontinued, the nodular lesions that resembled
subcutaneous lipomas disappeared slowly during a 3- to 6-month period. In one patient who
had an aortic-femoral bypass and anticoagulant therapy, injection sites at the upper legbecame hemorrhagic, however, this was not a reason for therapy discontinuation.
One male patient who was 76 years old and had a history of vascular disease, whichincluded transient ischemic attacks, developed a myocardial infarction during the third week
of treatment. Although hypotension did not occur, he died with signs and symptoms of brain-
stem ischemia.
55


Figure 2. Survival curve of all treated patients.
Although in some patients the pretreatment creatinine clearance level was decreased
(mean 65; range, 13 to 145 ml/min); renal toxicity was mild. Before treatment, the meanserum creatinine level was 109 µmol/L (range, 59 to 250), and after six weeks of IL-2
treatment 147 µmol/L (range, 82 to 309). Oliguria was not observed. Hepatic toxicity also wasmild, and an increase in the bilirubin level was found in only one patient (grade 1). Increases
in serum values of alkaline phosphatase and asparate aminotransferase were found frequently,
but these values decreased to normal after therapy was discontinued. Other forms of toxicity,including hematologic toxicity, were not observed, although a marked eosinophilia developed
during treatment in nearly all of the patients.
57

Figure 3. Survival curve of responders and nonresponders.
Discussion
This study suggests that IL-2 administered subcutaneously has significant antitumor activityin patients with advanced RCC. The observed response rate was similar to the 9% to 35%
response rate that was observed in IV IL-2, with or without LAK-cells (2-4). Until the last
10 years, the treatment of patients with metastatic RCC was limited largely to a symptomatictreatment. Thereafter, biological response modifiers were introduced. A recent review reported
that interferon had induced a CR rate of 2% and a PR rate of 14% (12). Since 1985, IV IL-2,with or without LAK cells, has been used in patients with advanced or metastatic RCC.
A number of prognostic factors have influenced survival, eg, a good performance
status, previous nephrectomy, interval between nephrectomy and metastatic disease, and sitesof metastases (13). In our study of subcutaneous IL-2, responses were observed in patients
who had favorable prognostic factors, although a difference among responders and
58

nonresponders in regard to these prognostic factors could not be found. On the other hand,survival of responders was increased significantly compared with nonresponders; however,
this could be an indication of a better pretreatment condition as a result of treatment.
Studies that have used subcutaneous IL-2 are scarce. Whitehead et al (14) used a dose-escalating regimen and found only one minor response in 15 patients. This response was
observed at a dose level of 2 x 106 Cetus U/m2/d (Cetus Corporation, Emeryville, CA). Steinet al (15) also used a dose-escalating regimen and found two PRs and SD in three of nine
patients, at a dose level of 100 µg IL-2 daily. Atzpodien et al (16) combined subcutaneous
IL-2 with interferon and found two CRs and three PRs of 14 assessable patients. As has beendescribed (14,15), subcutaneous IL-2 treatment can alter immunologic parameters, such as the
development of LAK-cell activity and enhanced NK-cell activity, although a relation betweenimmunological effects and clinical response could not be found.
IL-2 treatment is associated with significant toxic side effects. Although initially it
seemed that continuous IV infusion was less toxic when compared with bolus infusion, IL-2toxicity seems to be dose related (2,4). Moreover, with respect to the toxicity described, IV
IL-2 therapy is only suitable for patients considered fit. To decrease toxicity and to allowtreatment of patients with compromised renal, cardiac and pulmonary function, we have used
the subcutaneous route of administration. Treatment-related side effects were limited, and
most patients experienced fever and nausea. No capillary leak syndrome, hypotension, weightgain, or renal toxicity was observed. Only in one patient with a spinal cord lesion was dose
reduction necessary because of hypotension. However, Whitehead et al (14) found fatigue andelevated levels of serum creatinine dose-limiting at dose levels of 0.5 to 5 x 106 Cetus
U/m2/d. In one patient erythema and tenderness at the injection site also contributed to the
dose-limiting toxicities. Stein et al (15) found in 16 patients who were treated at a dose levelof 100 µg IL-2 daily one dose limiting toxicity caused by dyspnea, whereas dose reduction
was required in three patients because of fever, rash, lethargy, nausea, and vomiting.Atzpodien et al (16) described dose reduction in six patients.
Our results that concern the clinical efficacy and toxicity with subcutaneous IL-2 in
unselected patients with advanced RCC suggest that this treatment is attractive whencompared with IV schedules, especially in patients with compromised organ function.
59

References
1. Rosenberg SA, Lotze MT, Muul LM, Leitman S, Chang AE, Ettinghausen SE, Matory YL, skibber JM,Shiloni E, Vetto JT, Seipp CA, Simpson C and Reichert CM. Observations on the systemicadministration of autologous lymphokine-activated killer cells and recombinant interleukin-2 to patientswith metastatic cancer. N. Engl. J. Med. 1985; 313: 1485-1492.
2. Rosenberg SA, Lotze MT, Muul LM, Chang AE, Avis FP, Leitman S, Lineham WM, Robertson CN,Lee RE, Rubin JT, Seipp CA, Simpson CG and White DE. A progress report on the treatment of 157patients with advanced cancer using lymphokine-activated killer cells and interleukin-2 or high-doseinterleukin-2 alone. N. Engl. J. Med. 1987; 316: 889-897.
3. Fisher RI, Coltman CA, Doroshow JH, Rayner AA, Hawkins MJ, Mier JW, Wiernik P, McMannis JD,Weiss GR, Margolin KA, Gemlo BT, Hoth DF, Parkinson DR and Paietta E. Metastatic renal cancertreated with interleukin-2 and lymphokine activated killer cells. Ann. Intern. Med. 1988; 108: 518-523.
4. West WH, Tauer KW, Yanelli JR, Marshall GD, Orr DW, Thurman GD and Oldham RK. Constantinfusion recombinant interleukin-2 in adoptive immunotherapy of advanced cancer. N. Engl. J. Med.1987; 316: 898-905.
5. Sosman JA, Kohler PC, Hank JA, Moore KH, Bechhofer R, Storer B and Sondel PM. Repetitive weeklycycles of interleukin-2. II. clinical and immunologic effects of dose, schedule, and addition ofindomethacin. J. Natl. Cancer Inst. 1988; 80: 1451-1461.
6. Parkinson DR, Fisher RI, Rayner AA, Paietta E, Margolin KA, Weiss GR, Mier JW, Sznol M, GaynorER, Bar MH, Gucalp R, Boldt DH, Mills B and Hawkins MJ. Therapy of renal cell carcinoma withinterleukin-2 and lymphokine-activated killer cells: Phase II experience with a hybrid bolus andcontinuous infusion interleukin-2 regimen. J. Clin. Oncol. 1990; 8: 1630-1636.
7. Margolin KA, Rayner AA, Hawkins MJ, Atkins MB, Dutcher JP, Fisher RI, Weiss GR, Doroshow JH,Jaffe HS, Roper M, Parkinson DR, Wiernik PH, Creekmore SP and Boldt DH. Interleukin-2 andlymphokine-activated killer cell therapy of solid tumors: analysis of toxicity and management guidelines.J. Clin. Oncol. 1989; 7: 486-498.
8. Siegel JP and Puri RK. Interleukin-2 toxicity. J. Clin. Oncol. 1991; 9: 694-704.9. Sleijfer DTh, Janssen RAJ, Willemse PHB, Martens A, Leij de L, De Vries EGE and Mulder NH.
Low-dose regimen of interleukin-2 for metastatic renal carcinoma. Lancet 1990; 335: 1522-1523.10. Kaplan EL and Meier P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc.
1958; 53: 457-481.11. Peto R, Pike MC, Armitage J, Breslow NE, Cox DR, Howard SV, Mantel N, McPherson K, Peto J and
Smith PG. Design and analysis of randomized clinical trials requiring prolonged observation of eachpatient. II. Analysis and examples. Br. J. Cancer 1977; 35: 1-39.
12. Horoszewiwitcz JS and Murphey GP. An Assessment of the current use of human interferons in therapyof urological cancers. J. Urol. 1989; 142: 1173-1180.
13. Maldazys JD and deKernion JB. Prognostic factors in metastatic renal cell carcinoma. J. Urol. 1986;136: 376-379.
14. Whitehead RP, Ward D, Hemmingway L, Hemstreet GPIII, Bradly E and Konrad M. Subcutaneousrecombinant interleukin 2 in a dose escalating regimen in patients with metastatic renal celladenocarcinoma. Cancer Res. 1990; 50: 6708-6715.
15. Stein RC, Malkovska V, Morgan S, Galazka A, Aniszewski C, Roy SE, Shearer RJ, Marsden RA,Bevan D, Gordon-Smith EC and Coombes RC. The clinical effects of prolonged treatment of patientswith advanced cancer with low-dose interleukin-2. Br. J. Cancer 1991; 63: 275-278.
16. Atzpodien J, Korfer A, Franks CR, Poliwoda H and Kirchner H. Home therapy with recombinantinterleukin-2 and interferon-α2b in advanced human malignancies. Lancet 1990; 335: 1509-1512.
60

Chapter 3
A progress report on the outpatient treatment of patientswith advanced renal cell carcinoma using subcutaneous
interleukin-2
Jan Buter, Dirk Th. Sleijfer, Winette T. A. van der Graaf, Elisabeth G. E. de Vries,Pax H. B. Willemse and Nanno H. Mulder
Department of Medical Oncology, University Hospital, Oostersingel 59, 9713 EZ
Groningen, The Netherlands.
Summary
In an attempt to increase the therapeutic index of IL-2 based immunotherapy, the efficacy andtoxicity of subcutaneous IL-2 was studied in forty-seven patients, mean age 59 years (range
42-76), with advanced renal cell carcinoma (RCC). IL-2 was administered by subcutaneousinjection at 18x106 IU daily for 5 days. After the first weekly cycle the dose in the first two
days was reduced to 9x106 IU. Patients were treated for 4 or 6 consecutive weeks. Two 6-week cycles or three 4-week cycles were given maximally. Fourteen patients in this study
where 65 years or older. Twenty-one patients had concomitant disease that would probablyrender them not eligible for intravenous IL-2 treatment. Forty-six patients were evaluable for
response. One patient died of a myocardial infarction after 3 week treatment. Nine responseswere observed, two complete and seven partial. Four out of the nine responding patients were
65 years or older. Response durations were 35+, 29, 28+, 21+, 11, 8, 3+, 2, 1+ months. Themedian survival of all patients was 12 months, whereas the median survival of both nonres-
ponders and responders was 10 and 37+ months, respectively (P= 0.025). The main toxicityconsisted of local inflammation and induration at the injection sites, flu like symptoms with
fever, nausea/vomiting and diarrhoea. None of these side effects required hospitalization, andthey were acceptable even in patients with concomitant disease.
Subcutaneous IL-2 therapy is active and has limited toxicity in patients with advancedRCC. This outpatient regimen renders immunotherapy applicable in older patients and
patients with concomitant disease. Subcutaneous IL-2 therapy is attractive to combine withother treatment modalities like monoclonal antibodies, interferon or chemotherapy.
61

Introduction
Renal cell adenocarcinoma (RCC) is a tumor of renal tubular origin that has its peak ageincidence between 55 and 60 years (1), and nearly half of the patients have metastatic diseaseat presentation. The median survival of patients with metastatic RCC is approximately 12
months; the 2-year survival rate is less than 20% (2). Important prognostic indicators forsurvival are functional performance status, time to dissemination from initial diagnosis,
number of metastatic sites, prior cytotoxic chemotherapy, and recent weight loss (3).Conventional treatment modalities are not effective in treating metastatic RCC. Renal
cell carcinoma is resistant to chemotherapy (4), probably due to at least two separate factors;the presence of P-glycoprotein and elevated levels of gluthathione (5). Among biological
response modifiers interferon has shown some activity, but the responses are infrequent andtheir duration is usually short (6).
Recombinant interleukin-2 (rIL-2) has been used to treat RCC in a variety of dosagesand schedules. Response rates of 20 to 30%, with complete remissions in approximately 3 to
5% of patients, have been reported (7-11). These responses can be durable, some lasting 5years. Initial rIL-2 regimens were developed using chemotherapy guidelines in which the
maximum tolerable dose was given to patients. Toxicity of rIL-2, however, also is dose-related and severe when given by intravenous (IV) bolus or infusion (7-11). As a result, entry
criteria for initial phase II studies were strictly defined with regard to renal, pulmonary andcardiovascular function. In clinical practice, careful attention must be paid to the existence
of concomitant disease prohibiting IL-2 treatment. We report our phase II study usingsubcutaneous rIL-2 administrations to treat patients with advanced RCC, many of whom were
not eligible for IV-administered IL-2. The subcutaneous route was used to reducetoxicitiesassociated with IV rIL-2 administration. We have reported earlier on the first 29
patients treated in this study (12,13). This report updates our experience.
Patients and methods
PatientsSince December 1989, we have treated 47 patients with progressive, histologically proven
advanced or disseminated RCC and clinically measurable or evaluable disease. The study wasapproved by the University Hospital Groningen Medical Ethical Committee. Patients entered
the study after informed consent was obtained. Table 1 lists the patients’ characteristics. Table2 shows the concomitant diseases of 21 patients that would probably render them ineligible
for IV-administered rIL-2 treatment. However these concomitant diseases were not anexclusion criterium for subcutaneous treatment.
62

Table 1. Patients’ characteristics
N
Patients 47
Male/female 30/17
Age (years)
Mean 59
Range 42-76
Performance
WHO 0/1 27/12
2 8
Previous chemotherapy 1
Previous nephrectomy 37
Concomitant disease 21
Metastatic sites
Lung 35
Bone 7
Lymph nodes 7
Liver 4
Parotic gland 1
Skin 4
Number of sites1 18
2 25
> 2 4
Time from initial diagnoses
< 1 year 35
> 1 year 12
Treatment was initiated after patients were thaught to selfadminister rIL-2 injections.The first 29 patients were treated in a 6-week regimen (12). This regimen was amended to
4 weeks in attempt to decrease toxicities. The rIL-2 (Aldesleukin, EuroCetus B.V.,Amsterdam, TheNetherlands) was administered subcutaneously at 18.0 million IU
administered once daily for 5 conscutive days.
63

Table 2. Concomitant disease in 21 patients.
N
Previous myocardial infarction 2
Angina pectoris >= NYHA class II 5
Cardiac arrhythmias 4
Cardiac ischaemias 3
Aortic-femoral bypass 2
Valvular heart disease 2
Spinal cord lesion 2
Bilateral nephrectomy 2
Transient ischemic attacks 1
Previous cerebral vascular accident 1
Porphyria, acute intermittent 1
N = Number of diagnosisNYHA = New York Heart Association
After the first 5 days the dose on days 1 and 2 of the following cycles was reduced
to 9 million IU. Patients were treated either for 4 or 6 consecutive weeks. Treatment wasrepeated after a 3 week rest period in case of a 6-week course and after a 2-week rest period
when in the 4-week course. Acetaminophen (250-500 mg orally every 4-6 hours) was
administered concomitantly to prevent pyretic reactions.
Assessment of response and toxicityPrior to study entry, the stage of the patients diease was determined by full clinical exami-
nation, measurement of blood cell counts, serum electrolytes, creatinine clearance, liver and
thyroid function, chest radiograph, technetium pyrophosphate bone scan and computedtomographic scanning. During therapy, patients were examined on days 1, 7, 14 and 28, or
more frequently if clinically indicated. Toxicity was assessed during each visit according toWorld Health Organization criteria.
Radiologic evaluations to determine tumor measurements were repeated after each 4-
or 6-week treatment. A complete response was defined as disappearance of all tumor evidencefor a minimum of four weeks. A partial response was defined as a 50% or greater decrease
in the evaluable lesions. Response less than 50% or increases less than 25% were classified
64

as stable disease. Progression was defined as an increase of more than 25% or thedevelopment of new lesions.
Statistical analysisThe duration of response was calculated from the day the response was first documented to
the day of progressive disease. The overall survival was calculated from the start of treatment.Survival curves were plotted by using the Kaplan-Meier method (14), and statistical dif-
ferences were estimated using the log-rank test (15). Reported probability values are two-
sided.
Results
Out of the 47 patients, 45 received a full 4- or 6-week treatment course. One male patient
died of a myocardial infarction during the third week of treatment. Another patient with a
partial spinal cord lesion from a metastatic site in the spinal column had new paralyticsymptoms after 1 week of treatment, and IL-2 therapy was discontinued. This patient was
evaluated as early progressive disease.In all, 46 patients were evaluable for response. Two patients had a complete response,
seven patients had a partial response, 22 patients had stable disease, and 15 patients
progressed. Overall, the response rate was 20% (nine of 46 patients; 95% confidence limit,9% to 34%).
Response duration in the two patients with a complete response was 29 and 35+months. Patients with a partial response had response durations of 1+, 2, 3+, 8, 11, 21+ and
28+ months. The median length of survival of all patients was 12 months. The median length
of survival of nonresponders and responders was 10 and 37+ months, respectively (P= .025;Fig 1). Four of the nine patients with tumor responses were 65 years of age or older. No
difference was found between responders and nonresponders with regard to performance
status, prior nephrectomy, or sites of metastases. With regard to location of tumor response,seven of nine responses occurred in lung metastases; no responses were observed in the 10
patients with the primary tumor in situ.Side effects of rIL-2 treatment administered subcutaneously are shown in table 3.
Transient inflammation and local induration at the injection sites occurred in all patients. The
residual nodular lesions resembling subcutaneous lipomas disappeared slowly during a 2- to4- month period. In two patients with anticoagulant therapy, the injection sites at the upper
leg became hemorrhagic; however, it was not severe enough to require discontinuation oftherapy. Fever and chills occurred in all patients and, in most cases, was not controllable with
antipyretic treatment, leading to a grade I, II and III toxicity in 100 of 432 treatment weeks,
248 of 432 treatment weeks and 9 of 432 treatment weeks, respectively. Mild to
65

Table 3. Toxicity and side effects.
Number* Percentage
Local toxicity 47 100
Fever 47 100
Nausea/vomiting 45 96
Diarrhoea 26 57
Skin toxicity 10 21
Mucositis 2 4
Hypotension 12 26
Requiring fluids or pressors 0 0
Weight gain > 5% 5 11
Cardiac toxicity† 2 4
Creatinine > 200 µm/l§ 4 9
Thyroid dysfunction 7 15
Clinical evidence of infection 4 9
Neuropsychiatric symptoms 10 21
Bilirubin increase 1 2
ASAT increase ( > 2 x normal) 3 6
Thrombocytopenia0
0
* Number of patients experiencing at least one episode of toxic effect. † One lethal. § Two patients onhemodialysis excluded.
moderate nausea and vomiting occurred during 115 of 432 and 133 of 432 treatment weeks,
respectively. Mild diarrhea was observed during 82 of 432 treatment weeks. Seven patientsdeveloped dry skin desquamation, primarily cinfined to the palms and soles. Three patients
developed a generalized rash with pruritus.A blood systolic tension below 100 mm Hg occurred during 32 of 432 treatment
weeks (12 patients).
66

Figure 1. Survival curve of responders and nonresponders.
In four patients the systolic tension was below 90 mm Hg, but this was accompanied withsymptoms in only two patients; one with a complete thoracic spinal cord lesion leading to a
50% dose reduction in rIL-2 during the last 4 weeks, and another patient who was onhemodialysis following bilateral nephrectomy. A weight gain of more than 5% was observed
during 5 of 432 treatment weeks (5 patients).One 76-year-old patient with a history of vascular disease developed a myocardial in-
farction during the third week of treatment and died with signs and symptoms of brain-stemischemia. A 72-year-old patient developed atrial fibrillation with high frequency during the
third week of IL-2 treatment and was treated with verapamil.Although pretreatment creatinine clearance was decreased, (mean 73 mL/min; range
0-150 mL/min), serum creatinine levels above 200 µm/L occurred in only four patients whoall had elevated initial creatinine levels (125, 148, 154 and 278 µm/L; two patients onhemodialysis were excluded). In one patient progressive renal dysfunction led to a dose
reduction of 50% from the third week of therapy.
67

All patients had evidence of marked lymphocytosis and eosinophilia. Their peripheralblood lymphocytes rose from a mean of 1.6 (range, 0.2 to 6.0) to 4.4 (range, 1.0 to 5.9) x
109/L while eosinophils rose from 0.6 (range, 0.04 to 3.9) to 6.6 (range, 0.3 to 21.9) x 109/L.Thyroid dysfunction occurred in seven patients. Two patients developed a biochemical
hyperthyroidism followed by symptomatic hypothyroidism for which thyroid substitution wasindicated. Five patients had a biochemical hypothyroidism, which was symptomatic in one
patient. Three patients received thyroid substitution for 1.5 to 2 months until thyroid functionhad normalized spontaneously.
Infections for which antibiotic or antiviral treatment was indicated were found in fourpatients. One patient with a spinal cord lesion had recurrent urinary tract infections related
to the urinary catheter. The other patients developed a pulmonary infection, an epididymitis,and a herpes infection of the eye.
Neuropsychiatric symptoms included somnolence (three patients), disorientation (twopatients), difficulties with concentration (two patients), peripheral neuropathy (two patients),
and hallucinatory symptoms (one patient). No coma or seizures were observed. Computedtomography of the brain revealed metastases in two patients, with disorientation and depress-ion in one and headache and concentration difficulties in the other.
Discussion
The toxicity profile of high-dose IV rIL-2 requires adequate renal, cardiovascular andpulmonary function in patients selected for this therapy (7). Because the highest incidence of
RCC occurs in the same age group that has the highest incidence of cardiovascular andpulmonary diseases, a number of patients with RCC are not eligible for high-dose IV rIL-2
treatment. Therefore, investigators have looked for less toxic regimens. Initially, continuousinfusion appeared to be less toxic than the bolus injections (8), but a randomized study
comparing continuous infusion and bolus injections at equivalent doses found similar toxicity(9).
The primary complications of IV Il-2 (capillary leak syndrome, hypotension, organ
failure, bone marrow toxicity, and mental state abnormalities) are dose- and treatment-durationrelated (7-11). Bacterial sepsis, a complication of IV rIl-2 treatment observed in approxi-
mately 25% of patients, may be related to the central venous catheters and a reversiblechemotactic defect of neutrophils (16).
Subcutaneously administered rIL-2 injections can be administered on an outpatientbasis or managed by the patient at home, and they require minimal nursing assistance. Most
toxicities are mild to moderate and consist of painful swelling at the injection site, fever,chills, nausea, vomiting, diarrhea, pruritus and hypotension. These side effects rarely require
hospitalization or cessation of treatment (12,17-20). The low incidence of clinical infections
68

in this group of patients suggests that there is no indication for prophylactic antibiotic use inpatients treated with single-agent rIL-2 administered subcutaneously (21). Clinically relevant
neuropsychiatric symptoms during this outpatient regimen are rare, and their appearance mayindicate brain metastases (22). Treatment of patients with spinal cord lesions should be
carefully considered in view of the possibility of more pronounced hypotensive symptoms andspinal cord compression due to enlargement of metastatic sites caused by edema.
The 20% response rate of this subcutaneously administered rIL-2 regimen is in therange of the response rates observed in IV rIL-2 studies (7-11). Efficacy was pronounced in
nephrectomized patients with pulmonary metastases, in contrast to 10 patients without anephrectomy in whom no primary tumor responses where observed. Our data also confirm
the observation that IL-2 treatment is effective in the elderly patients (23). Toxicities inpatients aged 65 years and older were comparable to the toxicities observed in other patients,
except for the two patients who suffered cardiac toxicities. Subcutaneous rIL-2 can also beactive as second-line treatment; Lissoni et al (20) reported a 31% response rate in 13 patients
with advanced RCC who had progressive disease after interferon-alfa therapy. The lowtoxicity profile of subcutaneous rIL-2 makes this regimen especially attractive forcombinations aimed at increasing rIL-2 activity. Atzpodien and Kirchner (24) reported a
response rate of 31% in 32 RCC patients treated with subcutaneous rIL-2 and interferon-alfa.Recently, we studied the safety, immunostimulatory, and cytotoxic effects of low-dose
anti-CD3/T-cell receptor (CD3/TCR) monoclonal antibody OKT3 (Orthoclone, OrthoBiotechInc, Raritan, NJ) in combination with subcutaneous rIL-2. We reported a maximum tolerated
dose of 400 µg OKT3 but could not demonstrate enhanced immune activation, compared withthe activation found with rIL-2 alone (25). To overcome resistance to rIL-2 therapy, we are
studying the use of a bispecific monoclonal antibody BIS1, directed against the CD3/TCR andan epithelial carcinoma antigen EGP-2, in combination with subcutaneous rIL-2, to retarget
rIL-2-activated lymphocytes in vivo. We recently reported this combination to be feasible incompromised patients. Intravenous rIL-2 has been combined with a number of cytotoxic
agents in an attempt to modify its therapeutic spectrum (26-29). We expect that such regimenswill be at least as feasible with subcutaneous rIL-2.
Subcutaneous rIL-2 may be a worthwhile alternative for administration of this drug,especially in older patients with compromised functions of vital organs and in situations in
which combinations with toxic co-medications are contemplated.
69

References
1. Incidence of cancer in the netherlands 1989. First report of the netherlands cancer registry,Utrecht:Hoonte-Holland bv, 1992.
2. deKernion JB, Ramming KP and Smith RB. The natural history of metastatic renal cell carcinoma: acomputer analysis. J. Urol. 1978; 120: 148-152.
3. Elson PJ, Witte RS and Trump DL. Prognostic factors for survival in patients with recurrent ormetastatic renal cell carcinoma. Cancer Res. 1988; 48: 7310-7313.
4. Yagoda A. Chemotherapy of renal cell carcinoma: 1983-1989. Semin. Urol. 1989; 7: 199-206.5. Mickisch G, Bier H, Bergler W, Bak M, Tschada R and Alken P. P-170 glycoprotein, glutathione and
associated enzymes in relation to chemoresistance of primary human renal cell carcinomas. Urol Int1990; 45: 170-176.
6. Muss HB. Interferon therapy for renal cell carcinoma. Semin. Oncol. 1987; 14 (suppl 2): 36-42.7. Rosenberg SA, Lotze MT, Yang JC, Aebersold PM, Linehan WM, Seipp CA and White DE. Experience
with the use of high-dose interleukin-2 in the treatment of 652 cancer patients. Ann. Surg. 1989; 210:474-485.
8. West WH, Tauer KW, Yanelli JR, Marshall GD, Orr DW, Thurman GD and Oldham RK. Constantinfusion recombinant interleukin-2 in adoptive immunotherapy of advanced cancer. N. Engl. J. Med.1987; 316: 898-905.
9. Weiss GR, Margolin KA, Aronson FR, Sznol M, Atkins MB, Dutcher JP, Gaynor ER, Boldt DH,Doroshow JH, Bar MH, Hawkins MJ, Demchak PA, Gucalp R and Fisher RI. A randomized phase IItrial of continuous infusion interleukin-2 or bolus injection interleukin-2 plus lymphokine-activated killercells for advanced renal cell carcinoma. J. Clin. Oncol. 1992; 10: 275-281.
10. Parkinson DR, Fisher RI, Rayner AA, Paietta E, Margolin KA, Weiss GR, Mier JW, Sznol M, GaynorER, Bar MH, Gucalp R, Boldt DH, Mills B and Hawkins MJ. Therapy of renal cell carcinoma withinterleukin-2 and lymphokine-activated killer cells: Phase II experience with a hybrid bolus andcontinuous infusion interleukin-2 regimen. J. Clin. Oncol. 1990; 8: 1630-1636.
11. Margolin KA, Rayner AA, Hawkins MJ, Atkins MB, Dutcher JP, Fisher RI, Weiss GR, Doroshow JH,Jaffe HS, Roper M, Parkinson DR, Wiernik PH, Creekmore SP and Boldt DH. Interleukin-2 andlymphokine-activated killer cell therapy of solid tumors: analysis of toxicity and management guidelines.J. Clin. Oncol. 1989; 7: 486-498.
12. Sleijfer DT, Janssen RA, Buter J, De Vries EGE, Willemse PHB and Mulder NH. Phase II study ofsubcutaneous interleukin-2 in unselected patients with advanced renal cell cancer on an outpatient basis.J. Clin. Oncol. 1992; 10: 1119-1123.
13. Buter J, Janssen RA, Mulder NH, Jong PE, Leij de L and Sleijfer DTh. Recombinant interleukin-2 formetastatic renal cell carcinoma in hemodialysis patients. Eur. J. Cancer 1992; 28A: 1770-1771.
14. Kaplan EL and Meier P. Nonparametric estimation from incomplete observations. J. Am. Stat. Assoc.1958; 53: 457-481.
15. Peto R, Pike MC, Armitage J, Breslow NE, Cox DR, Howard SV, Mantel N, McPherson K, Peto J andSmith PG. Design and analysis of randomized clinical trials requiring prolongued observation of eachpatient. II. Analysis and examples. Br. J. Cancer 1977; 35: 1-39.
16. Klempner MS, Noring R, Mier JW and Atkins MB. An acquired chemotactic defect in neutrophils frompatients receiving interleukin-2 immunotherapy see comments. N. Engl. J. Med. 1990; 322: 959-965.
17. Whitehead RP, Ward D, Hemmingway L, Hemstreet GPIII, Bradly E and Konrad M. Subcutaneousrecombinant interleukin 2 in a dose escalating regimen in patients with metastatic renal celladenocarcinoma. Cancer Res. 1990; 50: 6708-6715.
18. Stein RC, Malkovska V, Morgan S, Galazka A, Aniszewski C, Roy SE, Shearer RJ, Marsden RA,Bevan D, Gordon-Smith EC and Coombes RC. The clinical effects of prolonged treatment of patientswith advanced cancer with low-dose interleukin-2. Br. J. Cancer 1991; 63: 275-278.
19. Leahy MG, Pitfield D, Popert S, Gallagher CJ and Oliver RTD. Phase I study comparing continuousinfusion of recombinant interleukin-2 by subcutaneous or intravenous administration. Eur. J. Cancer1992; 28A: 1049-1051.
20. Lissoni P, Barni S, Ardizzoia A, Crispino S, Paolorossi F, Archili C, Vaghi M and Tancini G. Second
70

line therapy with low-dose subcutaneous interleukin-2 alone in advanced renal cancer patients resistantto interferon- alpha. Eur. J. Cancer 1992; 28: 92-96.
21. Buter J, De Vries EGE, Sleijfer DT, Willemse PHB and Mulder NH. Infection after subcutaneousinterleukin-2. Lancet 1992; 339: 552.
22. Buter J, De Vries EGE, Sleijfer DT, Willemse PHB and Mulder NH. Neuropsychiatric symptoms duringtreatment with interleukin-2. Lancet 1993; 341: 628.
23. Negrier S, Mercatello A, Bret M, Thiesse P, Blay JY, Coronel B, Merrouche Y, Oskam R, Franks CR,Clavel M, Moskovtchenko JF and Philip T. Intravenous interleukin-2 in patients over 65 with metastaticrenal carcinoma. Br. J. Cancer 1992; 65: 723-726.
24. Atzpodien J and Kirchner H. The out-patient use of recombinant human interleukin-2 and interferonalfa-2b in advanced malignancies. Eur. J. Cancer 1991; 27 Suppl 4P S88-91;:
25. Buter J, Janssen RAJ, Martens A, Sleijfer DT, De Leij L and Mulder NH. Phase I/II of low doseintravenous OKT3 and subcutaneous interleukin-2 in metastatic cancer. Eur. J. Cancer 1993; 29A:2108-2113.
26. Demchak PA, Mier JW, Robert NJ, O’Brien K, Gould JA and Atkins MB. Interleukin-2 and high-dosecisplatin in patients with metastatic melanoma: a pilot study. J. Clin. Oncol. 1991; 9: 1821-1830.
27. Richards JM, Mehta N, Ramming K and Skosey P. Sequential chemoimmunotherapy in the treatmentof metastatic melanoma. J. Clin. Oncol. 1992; 10: 1338-1343.
28. Mitchell MS. Chemotherapy in combination with biomodulation: a 5-year experience withcyclophosphamide and interleukin-2. Semin. Oncol. 1992; 19: 80-87.
29. Yang JC, Shlasko E, Ritchey JL, Landry JG, White DE and Rosenberg SA. Combinationchemoimmunotherapy for metastatic colorectal cancer using 5-Fluorouracil, Leucovorin andInterleukin-2. Eur. J. Cancer 1993; 29A: 355-359.
71


Chapter 4
Phase I/II study of low dose intravenous OKT3 andsubcutaneous IL-2 in metastatic cancer
Jan Buter, Richard A.J. Janssen1, Alexander Martens1, Dirk Th. Sleijfer, Lou de Leij1,and Nanno H. Mulder.
Departments of Medical Oncology and1Clinical Immunology, Internal Medicine,University Hospital Groningen, The Netherlands.
Summary
In a Phase I/II study the safety, immunostimulatory and antitumour effects of a combined
OKT3/IL-2 treatment was studied in 15 cancer patients who failed IL-2 treatment. OKT3 wasgiven as a 2 hour IV infusion. Doses of 50, 100, 200 and 400 µg OKT3 were studied. Within
24 hours SC IL-2 was started five days/week for four weeks at a dose of 9-18x106 IU daily.
MTD was 400 µg OKT3 with neurotoxicity as dose limiting toxicity. Toxicity of subcutaneousIL-2 was acceptable. At the MTD 9 patients with RCC with measurable disease were treated
in a phase II setting. Eight patients were evaluable for response. Four patients had stabledisease and four had progressive disease. An increase of activated lymphocyte subpopulations
could not be found, although OKT3 was detectable on lymphocytes in vivo. Only if laboratory
studies shed light on methods to improve immunostimulating effects of OKT3 will furtherclinical studies be warranted.
Introduction
After disappointing results with aspecific stimulation of the immune system with BacillusCalmette-Guerin or specific stimulation with tumour derived vaccines (1), the use of
recombinant cytokines has opened a new approach in the immunotherapy of disseminatedcancer. Objective responses in selected tumours have been observed using interferon or
interleukin-2 (IL-2). Renal cell carcinoma (RCC) and malignant melanoma (MM) appear to
be the most susceptible to this strategy. Interferons have shown an overall response rate ofapproximately 16% in RCC, but responses were usually of short duration (2). IL-2 alone or
in combination with Lymphokine Activated Killer (LAK) cells generatedin vitro has resulted
in objective tumour regression with a response rate of approximately 20%-30% in RCC (3,4).
73

Intravenous IL-2 treatment however, is associated with severe toxicity for whichhospitalization and intensive care monitoring is necessary in a number of patients (3).
Recently treatment regimens with intermittent subcutaneous injections have been developed,
with acceptable toxicity, also resulting in a response rate of approximately 20% in RCCpatients (5-8). Despite this obvious improvement in applicability by eliminating most of the
toxicity of IL-2 treatment, the number of 80% non-responding patients remains a clinicalchallenge.
Resistance to IL-2 treatment could be due to lack of appropriate effector cells of the
immune system. Besides the IL-2 induced aspecific NK/LAK activity, current efforts inimproving immunotherapy have focussed on T cell mediated antitumour activity after antigen
recognition. Previously we found that during IL-2 therapy the NK cells are the predominantstimulated population, whereas T cells are only temporarily activated (9). In this study we aim
at increasing T cell immune reactivity in patients who failed IL-2 treatment. For this purpose
we used OKT3, a mouse monoclonal antibody directed against the CD3 antigen of the humanT cell receptor. (CD3/TCR). Anti CD3 moabs are both capable of activating and blocking the
T cell receptor, depending of the dose used. Low doses of anti-CD3 moabs cause activationand proliferation of resting T-cells in vitro and in animal studies, resulting in inducing IL-2
receptor expression, cytokine production and both antigen specific an non-specific cytotoxicity
(10,11). Combination of OKT3 and IL-2 in long term lymphocyte cultures results in a tenfoldincrease in the production of cytotoxic cells compared to cultures using IL-2 alone (12,13).
A certain anti-tumour effect of anti CD3 moabs has been reported (14,15). Bolus injectionsof 50-100 µg OKT3 caused neurotoxicity with symptoms of aseptic meningitis in 7 out of 13
patients (15).
When used at high doses, anti-CD3 moabs cause immunosuppressionin vivo, a property thatis extensively exploited in renal transplant patients for the suppression of graft rejection
(16,17).
The purpose of this study is to explore the safety, immunomodulatory and anti-tumourproperties of slow infusion with escalating, low doses OKT3, followed by a fixed regimen of
intermittent SC injections of IL-2 in a phase I/II setting.
Materials and methods
Patient selectionEligible patients had a histological confirmed diagnosis of disseminated RCC or MM for
whom no effective therapy was available after monotherapy with IL-2 had failed or thetumour had relapsed. Patients pretreated with other therapy were eligible as long as a
minimum of 3 weeks had elapsed since the completion of previous treatment. Additional
qualifications for eligibility included a performance status of WHO grade 2 or less. Patients
74

who required steroids for control of CNS localizations and patients with uncontrollable diseaseapart from the tumour were excluded from the study. For the phase II study measurable or
evaluable disease was required. The study protocol was approved by the Medical Ethical
Committee of the University Hospital Groningen, The Netherlands. All patients gave informedconsent before entry in the study.
OKT3The mouse monoclonal antibody OKT3 was obtained from the Orthoclone Pharmaceutical
Corporation, Raritan, NJ. It is available in vials containing 5 mg in 5 ml. A hundred folddilution was available for this study.
Interleukin-2Interleukin-2 was obtained from the EuroCetus company Amsterdam, the Netherlands. It is
available as Proleukin, with a biological activity of 18 million International Units permilligram. Vials of 1 mg were reconstituted with 1,2 ml sterile water and administered
subcutaneously within 24 hours after preparation, as has been described previously (7,8).
Monoclonal antibodiesThe monoclonal antibodies (Moab) Leu4 (anti-CD3); Leu3 (anti-CD4); Leu2 (anti-CD8);Leu19, (anti-CD56+16); anti-HLA-Dr and anti-IL-2Ralfa (CD25) were obtained from Becton
Dickinson, Mountain View, CA, USA and were directly conjugated with phycoerythrin (PE)or fluorescein-isothyocyanaat (FITC).
Immunostaining of cells and flow cytometryWhole EDTA-blood was stained within four hours after collection. To 100 µl of whole blood
20 µl of Mab preparation (containing 0.5 µg of assessed Mab) was added and the sample wasincubated at room temperature for fifteen minutes. Two ml of FACSlysing solution (Becton
Dickinson, Mountain View, CA, USA) was added and the cells were incubated for an
additional ten minutes. Subsequently, the solution was centrifuged and the cells were washedin phosphate buffered saline supplied with 0.092 mg/ml heparin and resuspended in 150 µl.
To analyse the binding of OKT3 on T-cells, whole blood aliquots of 100 µl were incubatedwith 10 µl of anti-Leu4-Fitc plus 50 µl of Goat Anti Mouse (GAM)-IgG2a-PE (Southern
Biotechnology Associates, Alabama, USA; 20 fold diluted) or with 10 µl of anti-Leu16-Fitc
plus 50 µl of GAM-IgG2a-PE. The samples were immediately analyzed on a FACSTAR(Becton Dickinson, Moutain View, CA, USA) with the laser tuned at 488 nm. Lymphocytes
were gated using standard FSC/SSC settings, which excluded the monocytes and granulocytesfrom analysis.
75

Soluble IL-2 receptor and soluble CD8Soluble IL-2 receptor (IL-2R) and soluble CD8 levels in serum were measured using a
commercial sandwich ELISA (T-cell Sciences, Inc, Cambridge Massachusetts).
Treatment and study designPrior to entry, patients were staged by full clinical examination, measurement of blood cell
counts, blood chemistry, thyroid function tests, chest radiograph and appropriate computed
tomographic scanning or ultrasound sonography. OKT3 dissolved in 100 ml NaCl 0.9 %, wasgiven as a 2 hour IV infusion. Starting dose of OKT3 was established on 50 µg since this
dose showed a certain toxicity as bolus injection in a previous study (15). Doses of 50, 100,200 and 400 µg were tested. The dose was escalated after at least two patients had shown no
toxicity exceeding WHO grade II at that dose. Within 24 hours after the infusion,
subcutaneous IL-2 was started 5 days/week for four weeks at a dose of 18 106 IU/day in thefirst week. The dose in the first two days of the following weeks was reduced to 9 106
IU/day. While on study patients were not allowed treatment with NSAID’s. After a short stayin the hospital, patients were treated at home and IL-2 injections were self-administered.
Acetaminophen 250-500 mg orally every 4-6 hours was given to prevent pyretic reactions.
Metocloperamide 20 mg suppository was given for nausea and vomiting. Toxicity was scoredaccording to WHO criteria during and after the OKT3 infusion and before each weekly IL-2
cycle. For toxicity greater than WHO grade II, IL-2 therapy was withheld until toxicity wasresolved. When a delay of more than 7 days was necessary, the patient was removed from the
study.
Blood samples were taken in the mornings before, 18 hours after the OKT3 infusionand on day 7, 14 and 28 during IL-2 treatment. Blood counts, electrolytes, renal and liver
function tests, lymphocyte subsets and lymphocyte activation markers were determined forevaluation of side effects and immunological changes. In 3 patients soluble IL-2 receptor and
soluble CD8 was measured. To be evaluable for response, patients with measurable disease
had to be followed for at least 4 weeks after the start of treatment. Radiological evaluationfor determination of tumour measurements was repeated after four week treatment or when
there was evidence of disease progression during a course. Complete response (CR) indicatedthe documented disappearance of all signs and symptoms of detectable tumour and no
development of new lesions. A partial response (PR) was defined as a decrease of at least
50% in the sum of the product of the two largest perpendicular diameters of all measurablelesions and no concomitant occurrence of new lesions. The situation in which no change or
decrease of less than 50% of the sum of the products of the two largest perpendiculardiameters of measurable lesions occurred was defined as stable disease. Disease progression
was defined as a 25% increase in the aforementioned lesions.
76

Results
Ten patients were entered in the phase I protocol. Patient’s characteristics are shown in table1. All patients were evaluable for toxicity. Maximum tolerated dose was 400 µg OKT3 with
neurotoxicity in 2 out of 4 patients (Table 2). Patient 2. (50 µg) developed neurological
symptoms with vertigo during treatment. Computed tomography of the brain showedcerebellar metastases, whereupon IL-2 treatment was discontinued. Patient 7. (400 µg) had a
psychotic reaction with confusion and desorientation 36 hours after the OKT3 infusion. Nolateralisation of symptoms was found and a CT scan of the brain showed no abnormalities.
All symptoms were transient and IL-2 treatment could be restarted after 5 days without
complications. Patient 9. (400 µg) was somnolent 4 to 36 hours after the infusion. Patients 4.(100 µg) and 6. (200 µg) had a mild headache responding to Acetaminophen.
Table 1. Patient’s characteristics.
Phase I Phase II
No. Patients 10 5
Age, yearsMedianRange
5729-73
5645-64
Male/female 8 / 2 3 / 2
Performance WHO )012
532
14
DiagnosisRenal cell carcinomaMetastatic melanoma
91
5
Prior chemotherapyPrior surgeryPrior radiotherapyPrior immunotherapy
19210
315
Metastatic sitesLungLiverBoneLocal recurrencePrimaryOthers
9
22
3
511121
77

Subcutaneous IL-2 treatment was well tolerated, but transient inflammation and localinduration at the injection sites occurred in all patients. Fever and chills were common and
in most cases not controllable with antipyretic treatment, leading to a grade I and II toxicity
in 3/33 and 13/33 weeks, respectively. A grade III toxicity was seen in 4/33 weeks. Nauseaand vomiting grade I and II occurred in 8/33 and 14/33 weeks, respectively and was in most
cases not controllable with anti-emetic therapy. Diarrhea grade I was observed in 3/33 weeks.Hypotension, defined as systolic tension below 100 mm Hg occured only once in 33 treatment
weeks. Hepatic and renal toxicity was mild. An increase in serum bilirubin level was not
found. Serum creatinine levels remained stable during treatment. Increases in serum Alkalinephosphatase and Lactic dehydrogenase were found frequently, but were transient in most
cases. Patient 3. developed a clinical and biochemical hypothyroidism for which substitutiontherapy was indicated. Two and a half month after discontinuation of IL-2 treatment, thyroid
function had normalized spontaneously. No objective responses were observed (Table 2).
Table 2. Toxicity and response of OKT3/ IL-2 treatment.
Patientno.
OKT3(µg)
Toxicity Onset ofsymptoms
(h)
Days of IL-2treatment
Response
1. 50 None 5 NE
2. 50 Vertigo 32 2 NE
3. 100 None 20 SD
4. 100 Headache 12 20 PD
5. 200 None 20 SD
6. 200 Headache 12 20 PD
7. 400 Confusion 36 20 SD
8. 400 None 20 PD
9. 400 Somnolence 4 20 SD
10. 400 None 20 PD
11. 400 None 20 SD
12. 400 None 20 PD
13. 400 None 20 SD
14. 400 headache 12 20 PD
15. 400 hypotension 48 5 NE
NE, not evaluable; SD, stable disease; PD, progressive disease.
78

Because four patients with metastatic RCC with measurable disease were treated at the 400µg OKT3 step, this number was extended with 5 other patients to study the efficiacy at the
MTD dose. Patient’s characteristics are shown in table 1. Toxicity consisted of hypotension
with renal dysfunction and headache in one patient each (Table 2). After 4 weeks treatment,eight patients were evaluable for response. Four patients had stable disease for 10, 7, 4 and
1 months and four patients showed progressive disease. Toxicity of subcutaneous IL-2 wascomparable to the toxicity seen in the other patients.
Immunological changes measured before and 18 hours after the OKT3 infusion are
shown in Tabel 3.
Table 3. Cell surface phenotype (% positive cells).
Patient OKT3 dose(µg)
Ly CD3 CD56+16 CD4 CD8
1 50 BeforeAfter
4433
7068
2124
5350
1818
2 50 BeforeAfter
1823
7573
810
4543
3234
3 100 BeforeAfter
2837
7681
1410
5662
1917
4 100 BeforeAfter
2845
6970
2020
3737
3432
5 200 BeforeAfter
2421
7157
1728
5240
1616
6 200 BeforeAfter
1717
6750
1830
3430
3016
8 400 BeforeAfter
2611
61ND
22ND
37ND
25N.D
9 400 BeforeAfter
2012
6041
3137
3020
2817
10 400 BeforeAfter
2814
5542
3237
4135
139
11 400 BeforeAfter
2834
5558
4036
3540
1614
12 400 BeforeAfter
134
5221
3613
128
3345
13 400 BeforeAfter
27ND
6532
1927
4629
157
14 400 BeforeAfter
2019
6466
4040
1921
2523
15 400 BeforeAfter
1913
4941
4648
2421
2621
Abreviations: Ly, Lymphocytes; ND, not determined;
79


Table 4. Soluble IL-2r and soluble CD8.
Patient OKT3 dose(µg)
SolubleIL-2R(U/ml)
SolubleCD8
(U/ml)
7 400 Before:After:
873901
Before:After:
561536
11 400 Before:After:
16591440
Before:After:
420415
14 400 BeforeAfter:
37752523
Before:After:
467411
Discussion
We studied thein vivo safety, immunostimulatory and antitumour effects of a combinedOKT3/IL-2 treatment in 15 cancer patients. MTD was 400 µg OKT3 with neurotoxicity as
dose limiting factor. Objective responses were not observed. Furthermore, no signs ofenhanced T cell function as indicated by the induction of CD25 or HLA-Dr expression were
found after administration of the OKT3, although the antibody could be detected on the T-lymphocyte surface. No enhanced rebound lymphocytosis during successive IL-2 treatment
was observed, compared to treatment with sc IL-2 alone. A rise in soluble IL2-receptor orsoluble CD8 indicating possible immune activation in other compartments than the peripheral
blood was not observed at the MTD.OKT3, a mouse IgG2 monoclonal antibody directed against the human CD3/TCR
complex, is known for its immunosuppressive activity associated with rapid depletion of peri-pheral blood lymphocytes, CD3/TCR modulation and prolonged graft survival when used
repeatedly in high doses (> 1 mg) in renal transplant recipients (17). Besidesimmunosuppressive effects anti-CD3 moabs have strong mitogenic activity in lymphocytes
when used at low doses (µg) inin vitro and in vivo. For its mitogenic activity at least threesignals seem to be necessary: CD3/TCR receptor occupation, cross linking of CD3 molecules
and additional accessory cell signals from monocytes. Mitogenic activity can be induced inthe absence of cross linking and accessory cell signals when exogenous IL-2 is provided (18).
The most likely mechanism for anti-CD3 antibody-mediated triggeringin vitro is the inductionof IL-2 receptors (19). Tumour regression after administration of low dose anti-murine CD3
was found in a murine model (14). In clinical use, signs of immune activation and cytokinerelease have been observed after first dose administration of OKT3 to renal transplant patients
(20,21). OKT3 coated T cell, found in lymph node biopsies from renal transplant recipientswithin 2 hours after bolus injection of the antibody, showed enhanced proliferation in the
81

presence of IL-2in vitro (22).
Possible reasons for the lack of enhanced T cell activation with the OKT3/IL-2combination in ou study could be that the OKT3 doses used are to low to activate T celfunction. Another explanation could be the previous treatment with IL-2 in all patients entered
in this study. T cell lytic function of patients treated with IL-2 has been found to be inhibitedand only partial reversible by subsequent T cell receptor activation using anti-CD3 mAb (23).
Recent clinical phase I studies in cancer patients with OKT3 alone or combined with low dosecontinuous infusion of IL-2 failed to enhance T cell phenotype or function at doses from 10 -
600 µg OKT3 (24,25). Further investigation is needed to explain the difference between the
in vitro andin vivo findings of the effects of low dose OKT3 in combination with IL-2 on theinducion of T cell activation. Only if such studies shed light on methods to improve
stimulating effects of OKT3 will further clinical studies be warranted.
Literature
1. Currie GA. Eighty years of immunotherapy: a review of immunological methods used for the treatmentof human cancer. Br. J. Cancer 1972; 26: 141-153.
2. Muss HB. Interferon therapy for renal cell carcinoma. Semin. Oncol. 1987; 14 (suppl 2): 36-42.3. Rosenberg SA, Lotze MT, Muul LM, Chang AE, Avis FP, Leitman S, Lineham WM, Robertson CN,
Lee RE, Rubin JT, Seipp CA, Simpson CG and White DE. A progress report on the treatment of 157patients with advanced cancer using lymphokine-activated killer cells and interleukin-2 or high-doseinterleukin-2 alone. N. Engl. J. Med. 1987; 316: 889-897.
4. West WH, Tauer KW, Yanelli JR, Marshall GD, Orr DW, Thurman GD and Oldham RK. Constantinfusion recombinant interleukin-2 in adoptive immunotherapy of advanced cancer. N. Engl. J. Med.1987; 316: 898-905.
5. Atzpodien J, Korfer A, Franks CR, Poliwoda H and Kirchner H. Home therapy with recombinantinterleukin-2 and interferon-α2b in advanced human malignancies. Lancet 1990; 335: 1509-1512.
6. Whitehead RP, Ward D, Hemmingway L, Hemstreet GPIII, Bradly E and Konrad M. Subcutaneousrecombinant interleukin 2 in a dose escalating regimen in patients with metastatic renal celladenocarcinoma. Cancer Res. 1990; 50: 6708-6715.
7. Stein RC, Malkovska V, Morgan S, Galazka A, Aniszewski C, Roy SE, Shearer RJ, Marsden RA,Bevan D, Gordon-Smith EC and Coombes RC. The clinical effects of prolonged treatment of patientswith advanced cancer with low-dose interleukin-2. Br. J. Cancer 1991; 63: 275-278.
8. Sleijfer DT, Janssen RA, Buter J, De Vries EGE, Willemse PHB and Mulder NH. Phase II study ofsubcutaneous interleukin-2 in unselected patients with advanced renal cell cancer on an outpatient basis.J. Clin. Oncol. 1992; 10: 1119-1123.
9. Janssen RAJ, Buter J, Straatsma E, Heijn AA, Sleijfer DTh, De Vries EGE, Mulder NH, The TH andDe Leij L. HLA-DR-expressing CD8bright cells are only temporarily present in the circulation duringsubcutaneous interleukin-2 therapy in renal cell carcinoma patients. Cancer Immunol. Immunother. 1993;36: 198-204.
10. Van Wauwe JP, De May JR and Goossens JG. OKT3: a monoclonal anti-human T-lymphocyte antibodywith potent mitogenic properties. J. Immunol. 1980; 124: 2708-2713.
11. Hirsch R, Gress RE, Pluznik DH, Eckhaus M and Bluestone JA. Effects of in vivo administration ofanti-CD3 monoclonal antibody on T cell function in mice. II. In vivo activation of T cells. J. Immunol.1989; 142: 737-743.
12. Ochoa AC, Gromo G, Alter BJ and Sondel PM. Long-term growth of lymphokine-activated killer (LAK)cells: role of anti-CD3,β-IL-1, interferon-τ and -β1. J. Immunol. 1987; 138: 2728-2733.
82

13. Ochoa AC, Hasz DE, Rezonzew R, Anderson PM and Bach FH. Lymphokine-activated killer activityin long-term cultures with anti-CD3 plus interleukin 2: Identification and isolation of effector subsets.Cancer Res. 1989; 49: 963-968.
14. Ellenhorn JDI, Hirsch R, Schreiber H and Bluestone JA. In vivo administration of anti-CD3 preventsmalignant progressor tumor growth. Science 1988; 242: 737-743.
15. Richards JM, Vogelzang NJ and Bluestone NJ. Neurotoxicity after treatment with muromonab-CD3. N.Engl. J. Med. 1990; 323: 487-488.
16. Hirsch R, Eckhaus M, Auchincloss JH, Sachs DH and Bluestone JA. Effects of in vivo administrationof anti-T3 monoclonal antibody on T cell function in mice. I. Immunosuppression of transplantationresponses. J. Immunol. 1988; 140: 3766-3772.
17. Ortho multicenter transplant study group. A randomized clinical trial of OKT3 monoclonal antibody foracute rejection of cadaveric renal transplants. N. Engl. J. Med. 1985; 313: 337-342.
18. Schwab R, Crow MK, Russo C and Weksler ME. Requirements for T cell activation by OKT3monoclonal antibody: role of modulation of T3 molecules and interleukin 1. J. Immunol. 1985; 135:1714-1718.
19. Tsoukas CD, Landgraf B, Bentin J, Valentine M, Lotz M, Vaughan JH and Carson DA. Activation ofresting T Lymphocytes by anti-CD3(T3) antibodies in the absence of monocytes. J. Immunol. 1985; 135:1719-1723.
20. Abramowicz D, Schandene L, Goldman M, Crusiaux A, Vereerstraeten P, Pauw de L, Wybran J,Kinnaert P, Dupont E and Toussant C. Release of tumor necrosis factor, interleukin-2, and gamma-interferon in serum after injection of OKT3 monoclonal antibody in kidney transplant recipients.Transplantation 1989; 47: 606-608.
21. Chatenoud L, Ferran C, Reuter A, Legendre C, Kreis H, Franchimont P and Bach JF. Systemic reactionto the anti-T-cell monoclonal antibody OKT3 in relation to serum levels of tumor necrosis factor andinterferon-α. N. Engl. J. Med. 1989; 320: 1420-1421.
22. Ellenhorn JDI, Woodle ES, Ghobreal I, Thistlethwaite JR and Bluestone JA. Activation of human Tcells in vivo following treatment of transplant recipients with OKT3. Transplantation 1990; 50: 608-612.
23. Weil-Hillman GW, Schell K, Segal DM, Hank JA, Sosman JA and Sondel P. Activation of human Tcells obtained pre- and post-interleukin-2 (IL2-2) therapy by anti-CD3 monoclonal antibody plus IL-2:implications for combined in vivo treatment. J. Immunol. 1991; 10: 267-277.
24. Urba WJ, Ewel C, Kopp W, Smith II JW, Steis RG, Ashwell JD, Creekmore SP, Rossio J, Sznol M,Sharfman W, Fenton R, Janik J, Watson T, Beveridge J and Longo DL. Anti-CD3 monoclonal antibodytreatment of patients with CD3- negative tumors: A phase IA/B study. Cancer Res. 1992; 52:2394-2401.
25. Sosman J, Ellis T, Bodner B, Kefer C and Fisher RI. Phase IB trial of anti-CD3 (OKT3) and low dosecontinuous infusion (CI) interleukin-2 (IL-2) in cancer patients. Proc. Am. Assoc. Cancer Res. 1992;33: 338. (Abstract)
83


Chapter 5
Phase I study of intravenously applied bispecific antibody inrenal cell cancer patients receiving subcutaneous IL-2.
B.J. Kroesen1, J. Buter2, D. Th. Sleijfer2, R.A.J. Janssen1, W.T.A. van der Graaf2,
T. H. The1, L. de Leij1, and N.H. Mulder2.
University Hospital Groningen, Depts. of Clinical Immunology1, and Medical Oncology2,
Oostersingel 59, 9713 EZ Groningen, The Netherlands.
Summary
In a phase I trial the toxicity and immunomodulatory effects of a combined treatment of
intravenous (i.v.) bispecific monoclonal antibody BIS-1 and subcutaneous (s.c.) interleukin-2
(IL-2) was studied in renal cell cancer patients. BIS-1 combines a specificity against CD3 onT lymphocytes with a specificity against a 40 kD pancarcinoma associated antigen, EGP-2.
Patients received BIS-1 F(ab’)2 fragments intravenously at doses of 1, 3, and 5 µg kg-1 bodyweight during a concomitantly given standard s.c. IL-2 treatment. For each dose, four patients
were treated with a 2 h BIS-1 infusion in the second and fourth week of IL-2 therapy. Acute
BIS-1 F(ab’)2 related toxicity with symptoms of chills, peripheral vasoconstriction andtemporary dyspnea was observed in 2/4 and 5/5 patients at the 3 and 5 µg kg-1 dose level,
respectively. The maximum tolerated dose (MTD) for BIS-1 F(ab’)2 was 5 µg kg-1. Elevatedplasma levels of tumour necrosis factorα (TNF-α) and interferonγ (IFN-γ) were detected at
the MTD. Flowcytometric analysis showed a dose-dependent binding of BIS-1 F(ab’)2 to
circulating T lymphocytes. Peripheral blood mononuclear cells (PBMC), isolated after treat-ment with 3 and 5 µg kg-1 BIS-1, showed increased specific cytolytic capacity against EGP-2+
tumour cells as tested in anex vivo performed assay. Maximal killing capacity of the PBMCs
as assessed by adding excess BIS-1 to the assay, was shown to be decreased after BIS-1infusion at 5 µg kg-1 BIS-1 F(ab’)2. A BIS-1 F(ab’)2 dose-dependant disappearance of
circulating mononuclear cells from the peripheral blood was observed. Within the circulatingCD3+CD8+ lymphocyte population, LFA-1α-bright and HLA-DR+ T-cell numbers decreased
preferentially. It is concluded that i.v. BIS-1 F(ab’)2, when combined with s.c. IL-2, has a
MTD of 5 µg kg-1. The treatment endows the T lymphocytes with a specific anti-EGP-2directed cytotoxic potential.
85

Introduction
Interleukin-2 (IL-2)-based immunotherapy has reproducible activity in selected tumours. Renalcell carcinoma (RCC) and melanoma are the malignancies most sensitive to this form of treat-
ment. Objective responses are observed in approximately 20 % of patients with RCC, with
durable complete remissions occurring in 5% (1). Subcutaneous (s.c.) administration of IL-2has been found to prevent an important part of the toxicity associated with the use of
intravenous (i.v.) IL-2 and has been shown to give rise to immunological and anti-tumoureffects similar to the i.v. treatment (2,3). Still, most RCC and melanoma patients and almost
all patients with other tumour types do not respond to IL-2 treatment.
A new form of immunotherapy in which the specific binding properties of monoclonalantibodies (MAbs) and the killing capacities of cytotoxic effector cells are combined, using
bispecific monoclonal antibodies (BsMAbs), has been the subject of several recent studies.BsMAb used in this treatment concept are composed of the antigen-binding subunits of two
different MAbs, giving rise to one antibody with two specificities. BsMAbs which combine
specificities against triggering molecules on cytotoxic effector cells on the one hand andtumour-associated antigens (TAAs) present on target cells on the other are able to redirect the
lytic capacity of the effector cell towards a chosen tumour target cell (4). This concept hasbeen studied in vitro and in vivo for a number of different effector and target cell populations
(5-10). Results indicate that BsMAb-redirected effector cells can specifically kill tumour cell
lines in vitro and established tumoursin vivo in animal models. A start has been made toexploit this treatment modality for the treatment of cancer patients. In glioma and carcinoma
patients, BsMAbs were shown to induce anti-tumour activity as well as inflammatory reactions
upon local transfer ofex vivo-activated autologous peripheral blood mononuclear cells(PBMCs) preincubated with a BsMAb reactive with the CD3 complex on T lymphocytes and
a TAA present on the tumour cells (11-13). To investigate the therapeutic possibilities of
BsMAb further, i.e. for systemic anti-tumour treatment, we have started a phase I study fori.v. administration of BsMAb. The BsMAb used, BIS-1, is reactive with both the CD3
complex on all T lymphocytes, and a pancarcinoma-associated antigen called epithelialglycoprotein (EGP-2) (14). Antibodies recognizing this carcinoma associated protein had been
clustered as SCLC cluster 2 and include CO17-1A, and AUA-1 (14-16). EGP-2 is a mem-
brane-bound 40 kDa glycoprotein which is highly expressed by most carcinomas and is notshed from the cell membrane (17). EGP-2 was also found to be present on all renal cell
carcinomas tested by us, although often to a low extend (own observation). Its expression onnormal tissue is restricted to simple epithelia (18), and the antigen is described in a number
of clinical studies as a target antigen for Mab-based immunotherapies (13,19,20). In the
present study BIS-1 was combined with s.c. IL-2 treatment. This combination was chosenbecause target cell lysis by BsMAb redirected CTL has been shown to be dependent on pre-
activation of lymphocytes (5,21,22). This implies that effective in vivo targeting of T
86

lymphocytes towards tumour cells by BsMAb should meet the condition of prior immuneactivation which, in the case of local treatment settings, can be done by ex vivo activation of
autologous immune cells (9,11). Immune activation in vivo, including T cell activation, can
be attained by s.c. IL-2 therapy (3). Furthermore, homing of lymphocytes into tumour tissuewhich appears to be a prerequisite for effective cellular immunotherapy, might be enhanced
by IL-2 (23,24).The present phase I trial studies the feasibility, toxicity and immunomodulatory effects
of i.v. administered BIS-1 in combination with s.c.-given IL-2 in patients with disseminated
RCC who were unresponsive to previous single-agent s.c. IL-2 treatment. F(ab’)2 fragmentsof BIS-1 were made and used in the present study to prevent possible aspecific toxicity,
resulting from the interaction of the Fc part of the BsMAb with FcR+ cells such as monocytesand the CD3-recognizing part of the antibody with T cells, resulting in a crosslinking of the
two celltypes.
Materials and methods
PatientsAll patients had a histologically confirmed diagnosis of disseminated RCC not responding to
single-agent s.c. IL-2. The patients had bidimensionally measurable tumour lesions, a perfor-mance status of≤ 2 (World Health Organization, WHO scale), an age of≥ 18 years, an
estimated life expectancy of more than 3 months, a rest period of at least 2 weeks afterprevious immunotherapy and an adequate haematologic function (white blood count≥ 4,000
mm-3 platelet count≥ 120,000 mm-3, haematocrit≥ 30%). Patients with uncontrollable disease
apart from the tumour, with renal dysfunction as indicated by serum creatinine level > 120µMol L-1 or with hepatic dysfunction as indicated by serum bilirubin levels > 30 mMol L-1
were excluded. Additional exclusion criteria were concurrent treatment with corticosteroidsor prior treatment with mouse antibodies. The study was approved by the University Hospital
Groningen Medical Ethical Committee. Written informed consent was obtained from all
patients before the start of treatment.
Preparation and purification of BIS-1The BIS-1-producing quadroma was made in our department by fusion of the hybridomas
RIV-9 and MOC-31, producing anti-CD3 (IgG3) and anti-EGP-2 (IgG1) antibodies respec-tively, according to a procedure as described by De Lauet al. (25). Large-scale production
of BIS-1 was done in a hollow fiber culture system (Endotronics, Minniapolis, MN, USA)
under good manufacturing practice (GMP) guidelines. Purification of the hybrid antibodies
87

(IgG3/IgG1) from parental-type antibodies (IgG3 and IgG1), also produced by the quadroma,was done by Protein A column chromatography. Hollow fiber culture supernatant was loaded
onto the column at pH 7.3 and the different IgG fractions were eluted successively by
lowering the pH stepwise. The BIS-1 containing fraction, eluted with 0.1 M sodium acetate,pH 4.0 was then digested by pepsin (Worthington, Freehold, NJ, USA) using a final BIS-
1:pepsin ratio of 100:1 (w/w). Digestion was performed at 37°C for 4 h, immediately followedby G150 sephadex gel filtration to separate BIS-1 F(ab’)2 from undigested IgG, fragmented
Fc portions and pepsin. The purified BIS-1 F(ab’)2 solution was adjusted to a concentration
of 0.2 mg ml-1 with 0.9% sodium chloride. HSA (Institute Merieux, Lyon, France) was addedto a concentration of 0.5% and the preparation was then passed through a 0.22 µm filter and
stored sterile at 4°C. Sterility of the BIS-1 F(ab’)2 preparation was confirmed by culturing in
Clausur medium. The BIS-1 F(ab’)2 preparation was pyrogen free as tested in aLimulusAmebocyte Lysate test and by intravenous administration of the preparation to rabbits.
Abnormal toxicity was tested by administration of the BIS-1 F(ab’)2 preparation to mice andguinea pigs both intravenously and intraperitoneally according to the protocol of the Dutch
Pharmacopee IX (1980) and was found to be absent. The ability of the BIS-1 F(ab’)2
preparation to redirect the lytic activity of T lymphocytes towards EGP-2 positive tumour cellswas assessed in a standard51Cr-release assay in whichin vitro-activated T lymphocytes
(effector lymphocytes, see below) were used as effector cells and GLC-1M13 (EGP-2-
positive), GLC-1 (EGP-2-negative) and P815 (FcR-positive) were used as target cells. Thetarget cell line P815 was used to check whether or not the BIS-1 (Fab’)2 preparation was
devoid of undigested Fc containing BIS-1 IgG.
TreatmentPatients received daily subcutaneous injections of 18x106 IU of IL-2 (Proleukin, EuroCetus
Amsterdam, Netherlands) in a 5 day weekly cycle for four consecutive weeks as prevouslydescribed (2). The dose in the first 2 days of the second, third and fourth weeks was reduced
to 9 x 106 IU day-1 followed by 3 days of 18 x 106 IU day-1. Acetaminophen 250-500 mg
orally every 4-6 h was given to suppress pyretic reactions. The BIS-1 F(ab’)2 BsMAb was ad-ministered in 100 ml sodium chloride as a 2 h i.v. infusion.
Study protocolConsecutive cohorts of at least four patients were treated at each dose level in a dose-escalat-ing phase I trial design. Dose levels of 1, 3 and 6 µg kg-1 body weight were planned to be
studied. The antibody was administered in the rebound phase of a preceeding 5 day s.c. IL-2cycle when the number of peripheral blood T lymphocytes was high (3). The first two patients
from a particular dose level received the antibody on days 8 and 22 and the following two
88

patients received the antibody on days 8 and 23, in order to study the effects of the antibodyboth before (day 8 and 22) and during (day 23) a cycle of IL-2 administration. On the day
of the antibody infusion, IL-2 was administered 4 h after the end of infusion. The end point
of the study was dose-limiting toxicity, defined toxicity exceeding WHO grade II. Themaximum tolerated dose (MTD) was defined as the dose level below that producing dose
limiting toxicity. Immunological parameters, including cytological and functional binding ofBIS-1 F(ab’)2, were monitored before and at the end of the antibody infusion. Quantification
of BIS-1 F(ab’)2 binding to T lymphocytes was done by a flow cytometry based procedure.
Functional binding of BIS-1 F(ab’)2 to T lymphocytes was assessed in a standard51Cr-releasecytotoxicity assay against the target cell lines GLC-1M13 (EGP-2-positive) and GLC-1 (EGP-
2-negative).
Toxicity and response monitoringBefore treatment, patients were staged with a full physical examination, determination of
WHO performance status, renal, liver, thyroid and haematological function, an ECG andradiological recording of disease extension. During treatment weight and temperature were
recorded daily and renal, liver and haematological functions were determined weekly. Thyroid
function was determined before and after the whole treatment. Blood samples were takenbefore the start and at the end of infusion of BIS-1 F(ab’)2 for analysing BIS-1 F(ab’)2 binding
to T lymphocytes and the cytotoxic capacity of isolated PBMCsin vitro. Vital functions were
measured every 30 minutes during the infusion, every 2 h thereafter and three times daily inthe 5 days during which the patients were hospitalised. Toxicity was scored according to stan-
dard WHO criteria (26). Dose modifications were planned as follows. In case of toxicityduring the BIS-1 F(ab’)2 infusion exceeding WHO grade II the infusion was abrogated. In
case of a weight gain > 5%, or an increase of serum creatinine level of more than 100% or
a decrease in systolic tension of 25% during the rest of treatment, the IL-2 was discontinued.Treatment could be reinstituted when toxicity had returned to below a grade I level. If IL-2
had to be withheld for more than 5 days the patient went off study. Response was monitoredby radiographic techniques as appropriate. Tumour evaluations were repeated after 4 weeks
of treatment and every 3 months thereafter. A complete response was defined as the disap-
pearance of all evidence of tumour for a minimum of four weeks; a partial response wasrecorded when a 50% or greater decrease in the sum of the products of all diameters of evalu-
able lesions was reached. Patients with a response less than partial or an increase of less than25% for at least 3 months were classified as having stable disease. Progression was defined
as an increase of more than 25% or the development of new lesions.
89

PBMC isolationPBMCs were obtained from heparinised peripheral blood. Isolation was done by density
centrifugation of diluted (1:1 in phosphate buffered saline PBS) blood on Lymphoprep
(Nycomed, Oslo, Norway) at 2,400 r.p.m. for 20 min. The PBMC fraction was washed twiceby resuspension in RPMI-1640 (GIBCO Europe, Breda, The Netherlands) and centrifugation
at 1,800 (first time) and 1,200 (second time) r.p.m. for 10 min. After isolation, PBMCs werecollected in complete medium consisting of RPMI-1640 supplemented with 2% heat-
inactivated human pooled serum, 2 mM glutamine and 60 µg ml-1 gentamicin.
Antibodies used for flow cytometryFor phenotyping of T lymphocytes and assessment of BIS-1 F(ab’)2 binding to T lymphocytes,
the following MAbs were used: fluorescein isothiocyanate (FITC)- or phycoerythrin (PE)-
labelled anti-Leu-4 (CD3), biotinylated anti-Leu-2a (CD8), FITC-labelled anti-LFA-1α(CD11a), PE-labelled HLA-DR (Beckton Dickinson, Mountain View, CA, USA), biotinylated
goat anti-mouse Ig (GαM-biotin) and biotinylated goat anti-rabbit Ig (GαR-biotin) (SouthernBiotechnologies Inc., Cambridge, MA, USA).
Flow cytometric analysisCD3 occupancy by BIS-1 F(ab’)2 was assessed using an indirect immunofluorescence stainingprocedure in which streptavidin-PE (SAPE) (Becton Dickinson) was used to amplify the BIS-1
F(ab’)2 detection with biotinylated goat anti-mouse antibodies (27). 100 µl aliquot of periphe-
ral EDTA blood or isolated PBMC samples were incubated with phosphate-buffered saline(PBS) or a saturating amount of BIS-1 F(ab’)2 (2 µg ml-1) at 4°C for 30 min. After one wash
with 2 ml of PBS and 50 µl GαM-biotin or, as a control for aspecific binding of the conjugate,GαR-biotin (each 40x diluted in PBS containing 1% pooled human serum) was added to the
cell pellet and incubated at 4°C for 30 min. After one wash with 2 ml PBS, 10 µl Streptavi-
din-PE was added to the cell pellet and the samples were incubated at 4°C for 30 min. Cellswere resuspended in 2 ml FACS-lysing solution (Beckton Dickinson, Mountain View, CA,
USA), incubated 10 min at room temperature, washed once with PBS and resuspended in afinal volume of 150 µl PBS for flow cytometric analysis. The CD3 occupancy was calculated
according to the following formula:
in which the sequential incubation steps are given between brackets, MFI is the mean
fluorescence intensity, SAPE is streptavidin-PE andt=x represents eithert=0 h (before the
infusion) or t=2 h (after the infusion).
90

Changes in leucocyte numbers as induced by the treatment were analyzed by a CoulterLeucocounter (Coulter Electronics, Hilaleah, FL, USA). Changes occurring within the
CD3/CD8 double-positive cell population as induced by the treatment were analyzed by three-
colour flow cytometry. CD8-biotin/Streptavidin-allophycoerythrin (APC) and CD3-PE or CD3-FITC were used to select for CD3/CD8 double positive T lymphocytes, and CD11a-FITC and
HLA-DR-PE conjugates were used to analyse the presence of LFA-1α and HLA-DR-positivecells within the CD3/CD8 cell population. Staining was performed on 100 µl peripheral EDTA
blood obtained from the patient just prior to (t=0 h) and directly after(t=2 h) BIS-1 infusion.
In the first step, CD8-biotin was allowed to bind at 4°C for 30 min followed by one washwith 2 ml of PBS. The second step included the addition of either streptavidin-APC, CD3-
FITC, HLA-DR-PE or streptavidin-APC, CD3-PE, CD11a-FITC to the resuspended cell pellet
and incubation for another 30 min at 4°C. The cell suspension was resuspended in 2 ml FACSlysing solution, incubated for 10 min at room temperature, washed once with 2 ml PBS and
resuspended in a final volume of 150 µl of PBS for analysis. The samples were analyzed ona Coulter Elite Cytometer (Coulter Electronics, Hilaleah, Fl, USA) using an argon laser (488
nm) for FITC and PE excitation and a He/Ne (623 nm) laser for excitation of APC.
Immunofluorescence emission was measured using a 525 nm bandpassfilter for FITC, a 575nm bandpass filter for PE and a 675 nm bandpass filter for APC.
Effector lymphocytesIn order to test the activity of the BIS-1 F(ab’)2 preparation, PBMCs isolated from healthyvolunteers were activated by incubating the cells for 3 days in complete medium supple-
mented with 5% (giving about 0.5 µg IgG ml-1 end concentration) culture supernatant of themitogenic anti-CD3 Mab WT-32 (28), followed by washing and incubation for two additional
days in complete medium supplemented with 60 IU ml-1 IL-2 (EuroCetus, Amsterdam, The
Netherlands). To assess functional binding of BIS-1 F(ab’)2 to T lymphocytes in the clinicalstudy, freshly isolated PBMCs drawn from the patients just before and after the 2 h antibody
infusion were used directly in the51Cr-release cytotoxicity assay.
Target cell linesGLC-1M13 (EGP-2-positive) and GLC-1 (EGP-2-negative) are small-cell lung cancer (SCLC)-
derived cell lines (29). P815 is a FcR-positive mouse mastocytoma cell line. These cell lineswere cultured according to routine procedures in RPMI-1640 based medium supplemented
with 14% heat inactivated fetal calf serum, 2 mM glutamine 60 µg ml-1 gentamicin (Schering,
Kenilworth, USA), 0.05 mM ß-mercaptoethanol and 1 mM sodium-pyruvate at 37°C in ahumidified atmosphere containing 5% carbon dioxide.
91

51Cr-release assay51Cr-release assays were performed according to standard procedures to assess BIS-1-
redirected T-cell cytotoxicity. All determinations were done in triplicate in the presence of 60
IUml IL-2. Before the assay, 5x106 target cells (GLC-1M13, GLC-1 or P815) were suspendedin 100 µl culture medium containing 3.7 MBq [51Cr]sodium chromate (Amersham, UK) and
incubated for 1 h at 37°C, in a humidified, 5% carbon dioxide-containing atmosphere.Unbound [51Cr]sodium chromate was removed by washing the cells three times with medium.
A 50 µl aliquot of medium containing 0.4 µg ml-1 BIS-1 F(ab’)2 (giving a final concentration
of 0.1 µg ml-1 during the assay) or not was pipetted into a 96 wells round-bottom microtitreplate (Greiner no. 650180) and incubated into 50 µl 2.5 x104 or 2.5 x105 effector lymphocytes
for 15 min at room temperature. Subsequently, 100 µl of medium containing 2.5 x103 51Cr-labelled target cells was added to each well to give effector to target (E/T) ratios of 1, 10 and
100 in a final volume of 200 µl. The microtiter plates were centrifuged at 500 r.p.m. for 2 min
and incubated at 37°C, 5% C02 for 4 h. After the incubation, the plates were centrifuged at1,000 r.p.m. for 5 min and 100 µl samples taken from the supernatant were counted in a
gamma counter for 5 min. Cell lysis was calculated from the percentage51Cr released,according to the formula:
Maximal release was determined from a sample to which 100 µl 2% Triton X-100 solution
was added instead of effector cells. Spontaneous release was determined from a sample towhich 50 µl medium was added instead of effector cells.
Cytokine releaseAntibody-based capture ELISAs were used to assess TNF-α (British Bio-technology, Oxford,UK) and IFN-γ (Eurogenetics, Leuven, Belgium) according to the manufacture’s instructions.
Blood plasma was isolated by centrifugation of EDTA containing peripheral blood samplesat 2,500 r.p.m. at 4°C for 5 min, immediately after collection. The cell fraction was discarded
and the plasma samples stored at -20°C until use.
StatisticsChanges in leucocyte count, phenotype and function were statistically analysed using the
Wilcoxson test for paired observations. A two-sided alpha level of 0.05 was considered
significant.
92

Table I. Patients characteristics.
N %
Patients 14
Female/male 6 / 8
Age (years)
Median 58
Range 48 - 70
WHO performance
0 3 21
1 7 50
2 4 29
Prior therapy
Nephrectomy 6 43
Chemotherapy 0 0
Immunotherapy 14 100
Tumour localizations
Primary 8 57
Lung 9 64
Bone 5 36
Other 4 29
Number of metastatic sites
1 2 14
2 8 57
3 or more 4 11
Results
In vitro effectiveness and characteristics of BIS-1 F(ab’)2The purified BIS-1 F(ab’)2 fragment preparation used in this study was analyzed by SDS-PAGE. No undigested IgG could be detected (data not shown). In agreement with this the
preparation induced no Fc-mediated cytotoxicity of activated cytotoxic T lymphocytes towards
93


Table II. Toxicity and response of treatment
No. Sex Doseµg/kg
Toxicity 1day 8
Toxicity 2day 22 or 23
Response
1. M 1 - - SD
2. M 1 - - PD
3. F 1 - - SD
4. F 1 - - PD
5. F 3 - - PD
6. M 3 Chills, fever Chills PD
7. F 3 - - SD
8. M 3 - Chills PR, 6 months
9. M 6->5a Chills, dyspnea, fever Chills PD
10. F 5 Chills, temporarydyspnea, fever
Chills SD
11. M 5 Chills - PD
12. F 5 Chills Chills PD
13. M 5 Chills, temporarydyspnea, fever
Chills, temporarydyspnea, fever
PD
14. M 5 - Chills, temporarydyspnea, fever
SD
a At day 8 infusion was abrogated at t = 1.5 h, giving an effective dose of approximately 5 µg kg-1. Atday 22 5 µg kg-1 was given in a 2 h infusion. F, female; M, male; PR, partial remission; SD, stabledisease; PD, progressive disease.
Phase I studyFrom October 1992 until June 1993, 14 patients with advanced RCC who showed no responseafter 4 weeks of s.c. IL-2 treatment were entered. The characteristics of the patients are listed
in Table 1. All patients were eligible for evaluation of toxicity. Side-effects arising from theBIS-1 F(ab’)2 administration are listed in Table 2. This dose-dependent toxicity could be dis-
criminated from the toxicity associated with IL-2 by its acute and rapidly transient characteris-tics. At the 1 µg kg-1 dose level no toxicity was observed. Toxicity occurred in two out of four
patients at the 3 µg kg-1 dose level and consisted of chills, peripheral vasoconstriction withrise in diastolic tension, temporary dyspnea and fever. Symptoms started suddenly in all
patients, approximately 100 min after the start of infusion and lasted 15-30 min, except for
95

the fever, which started approximately 30 min after the end of the infusion and lasted for 1-2h. No neurotoxicity was observed after administration of the BIS-1 F(ab’)2. In the first patient
at the 6 µg kg-1 dose level, severe rigors started 1 h after the start of infusion, and becameaccompanied by increasing dyspnea with signs of cyanosis, whereupon the infusion had to be
abrogated. Symptoms resolved gradually over the next 4-6 h except for fever. The patient hadreceived a total dose just over 5 µg kg-1. On day 22, a dose of 5 µg kg-1 could be ad-
ministrated to the same patient as a 2 h infusion, producing toxicity with chills to a grade Itoxicity. No further dose escalation was attempted. A total of 5 other patients were treated at
a 5 µg kg-1 dose level producing grade I-II toxicity in all patients. This dose was consideredthe MTD. No difference in toxicity was observed between the administration of the antibody
on day 8 and 22, before the start of a new IL-2 cycle, or on day 23, during an IL-2 cycle.There was no correlation between sex, age, performance status, prior nephrectomy or the
presence of lung metastases and toxicity.Toxicity during subcutaneous IL-2 treatment was similar to previous findings with s.c.
IL-2 monotherapy (2) and consisted of transient inflammation and local induration at theinjection sites in all patients. The residual nodular lesions resembling subcutaneous lipomasdisappeared slowly during a 2-4 month period. Flu-like symptoms with fever and chills
occurred in all patients, leading to a grade I, II toxicity in 21/56 and 29/56 treatment weeks,respectively. Nausea/vomiting grade I, II, and III occurred during 25/56, 20/56 and 1/56 weeks
respectively, while diarrhoea was observed during 5/56 weeks reaching grade I only.Hypotension was not observed. Transient elevations ofγ-glutamyl-transpeptidase and alkaline
phosphatase were observed in 34% and 21% of patients respectively. One patient receivingBIS-1 (at the 5 µg kg-1 dose level) had gradual progression of pre-existent renal dysfunction
at the end of IL-2 therapy, resulting in a creatinine elevation to grade III toxicity. Thyroiddysfunction was observed in one patient. Peripheral blood lymphocytes counts dropped
temporarily upon administration of the BIS-1 F(ab’)2 as will be discussed below, but thesenumbers returned to normal values 24 h after the infusion. During subsequent IL-2 treatment
mean peripheral blood lymphocyte count rose from 1.8 (s.d. 1.0) to a maximum of 4.8 (s.d.2.6) x 109 l-1, while eosinophil counts rose from 0.3 (SD 0.3) to 4.9 (SD 3.9) x 109 l-1. No
additional toxicity, especially no enhanced mucositis, diarrhoea or skin toxicity from the BIS-1(Fab’)2 antibody on top of the IL-2 related toxicity was observed during the rest of the IL-2
treatment course when compared to previous s.c. IL-2 monotherapy (2).
Response to treatmentAll 14 patients were assessable for response after 4 weeks of treatment. One partial response
in a patient with lung metastasis who received 3 µg kg-1 was observed and lasted 6 months.Five patients showed stable disease for at least 3 months and eight patients exhibited
progressive disease.
96


F(ab’)2. After PBMC isolation, in order to perform51Cr-release assays, the CD3 occupancyby BIS-1 F(ab’)2 was measured again and proved to be reduced from 4% to 2.5% (SD 0.6)
and from 6% to 3% (SD 0.5) for the doses 3 and 5 µg BIS-1 respectively. The CD3occupancy by BIS-1 F(ab’)2 was found to decrease in the next hours (not shown).
Functional analysis of BIS-1 bindingThe ability of in vivo BIS-1 F(ab’-)2-loaded T lymphocytes to exert specific anti-tumour
activity was assessed in anin vitro 51Cr-release assay. PBMCs isolated from peripheral blood
obtained just before (t = 0 h) and directly after (t = 2 h) infusion with BIS-1 F(ab’)2 wereincubated with51Cr-labelled EGP-2-positive and -negative target cells at E/T ratio’s of 1, 10
and 100. Both att = 0 h and att = 2 h, the assay was also performed in the presence of
additional BIS-1 F(ab’)2 (0.1 µg ml-1) added to the assay to assess the maximal redirected
Treatment-related cytokine releaseSince the observed toxicity in the patients treated at the 5 µg kg-1 BIS-1 F(ab’)2 dose level
(Table II) might be explained by the release of secondary cytokines, serum levels of TNF-αwere assessed in patients treated at 3 and 5 µg kg-1 before and at different time points after
cytotoxic capacity of the PBMC. Figure 3 shows the results of the EGP-2-redirected cytolyticcapacity of these freshly isolated PBMC at an E/T ratio of 100. PBMCs isolated after infusion
of 3 µg kg-1 BIS-1 F(ab’)2 showed significantly higher specific anti-tumour activity than
PBMCs isolated before the infusion (P<0.04) indicating that thein vivobound BIS-1 endowedthe T lymphocytes with a functional anti-EGP-2 redirected cytotoxic capacity (see fig. 3at
= 0- and t = 2-). At this dose, maximal redirected cytotoxic capacity, before and after the
infusion, as assessed by adding 0.1 µg ml-1 BIS-1 F(ab’)2 in vitro to the assay, was approxi-mately the same in all patients tested (see fig. 3at = 0+ andt = 2+). At 5 µg kg-1 however,
the maximal redirected cytotoxic capacity after the 2 h infusion was found to be significantlylower (P<0.005) than the maximal redirected cytotoxic capacity before infusion using the
same E/T ratio (see fig. 3bt = 0+ andt = 2+). Using the EGP-2-negative target cell line
GLC-1, no cytotoxicity could be measured at any of the assessed doses or time pointsindicating that possible LAK activity did not interfere with this assay (data not shown).
98



Table III. Immunophenotyping of peripheral blood lymphocytes before and after BIS-1 F(ab’)2 infusion
at 5 µg kg-1 body weight.
patient# day of
treatment
CD3a CD8b CD11ac HLA-DRc
bright dim ratio
11 d8 t = 0
t = 2
66
62
21
18
63
50
35
49
1.8
1.0
49
39
d23 t = 0
t = 2
56
58
19
17
72
44
28
36
2.6
1.2
67
52
12 d8 t = 0t = 2
5253
1513
5843
4256
1.40.8
2812
d23 t = 0t = 2
3331
1915
5637
4463
1.30.6
128
13 d8 t = 0
t = 2
58
54
26
28
68
68
32
32
2.1
2.1
16
10
d23 t = 0
t = 2
62
73
16
16
64
45
36
54
1.8
0.8
10
4
14 d8 t = 0t = 2
7683
1514
8567
1432
6.12.1
3926
d23 t = 0t = 2
6459
2122
7656
2443
3.61.6
3119
aPercent positive cells of total lymphocytes. bPercent positive cells of CD3 positive lymphocytes.cPercent positive cells of CD3/CD8 double-positive lymphocytes.Leucocyte numbers and
immunophenotyping
especially monocyte but also lymphocyte numbers were significantly reduced in the blood(P<0.01 at 3 µg kg-1 and P<0.005 at 5 µg kg-1 ). To analyze this phenomenon more
specifically, blood samples obtained from patient 11-14 were stained with CD3, CD8, CD11a(LFA-1α) and anti-HLA-DR before and after infusion with 5 µg kg-1 body weight BIS-1
F(ab’)2. Changes occurring within the CD3/CD8 double-positive T lymphocyte populationbetween the blood samples taken before and after the infusion were analysed. Within the
CD3/CD8 double positive T cell population, LFA-1α-bright and HLA-DR positive cellsdisappeared from the blood to a greater extend (P<0.02 and P<0.01 respectively) as a result
of BIS-1 F(ab’)2 infusion than the LFA-1α-dim positive or HLA-DR negative cells (Table III).
101


Discussion
The mechanisms ofin vivo IL-2 mediated anti-tumour responses are still not clarified.However, it is conceivable that to attain effective cellular immunotherapy a number of
prerequisites should be met. These include (1) effector cell activation, (2) presence or
migration of effector cells in or to the tumour site and (3) specific recognition and killing ofthe tumour target cells by the effector cells. During IL-2 treatment, NK effector cells as well
as T lymphocytes become activated (3) and the latter cells have been shown to migrate to thesite of the tumour (23,24) However, in RCC patients, who are in fact the best responding
patient group, an overall response rate of only approximately 20% to IL-2 therapy is attained(1). Resistance to IL-2 therapy might be due to an inability of the effector cells to specifically
recognise and/or kill the tumour cells. BsMAbs that are able to bind to both tumour cells andeffector cells might add such specificity to the IL-2 treatment. Furthermore, it is speculated
that, in addition to the IL-2 induced activation, the BsMAb might provide a necessary co-stimulatory signal by cross-linking the IL-2-activated T lymphocytes to tumour cells throughtheir CD3 complex. In this study we investigated the feasibility of a combination treatment
of i.v. applied BsMAb and s.c. IL-2 therapy. To prevent aspecific immune activation ortoxicity that could arise from binding of the BsMAb through its Fc part to FcR positive cells
like monocytes, F(ab’)2 fragments of BIS-1 were used in the present study. Acute toxicity,however, was encountered after administration of BIS-1 F(ab’)2 with chills, peripheral
vasoconstriction, dyspnea, fever and release of cytokines such as TNF-α and IFN-γ. Thesephenomena led to the conclusion that the MTD of BIS-1 F(ab’)2 given as a 2 h infusion is 5
µg kg-1. Recently, other investigators have reported severe toxicity of a similar nature withhigh systemic release of TNF-α and IFN-γ after administration of 1 mg of a F(ab’)2 BsMAb
in a patient with ovarian carcinoma. In this study no concomitant IL-2 was given (30). In thepresent study we also found elevated levels of TNF-α and IFN-γ. It remains to be resolved
Legend to figure 5. Absolute numbers of monocytes (x 106 ml-1) just before (t = 0) and directly after(t = 2) infusion with 1 (4 patients, n = 8) (fig.5a), 3 (4 patients, n = 8) (fig.5b) and 5 (6 patients, n = 12)(fig.5c) µg kg-1 BIS-1 F(ab’)2. Median as well as 25 and 75 percentiles are shown as a box plot whereaswhiskers range down to 5 and up to 95 percentile values. * indicates a significant reduction (P<0.005by the Wilcoxon test) compared to the values at t = 0.
Legend to figure 6. Absolute numbers of lymphocytes (x 106 ml-1) just before (t = 0) and directly after(t = 2) infusion with 1 (4 patients, n = 8) (fig.6a), 3 (4 patients, n = 8) (fig.6b) and 5 (6 patients, n = 12)(fig.6c) µg kg-1 BIS-1 F(ab’)2. Median as well as 25 and 75 percentiles are shown as a box plot whereaswhiskers range down to 5 and up to 95 percentile values. * indicates a significant reduction (P<0.005by the wilcoxon test) compared to the values at t = 0.
103

whether the observed toxicity in the higher doses of the present study is still the result ofaspecific stimulation of the monocyte/macrophage system or that it is induced by specific BIS-
1 F(ab’)2-mediated T cell activation, or both. The observed toxicity appears to be unrelatedto MOC31 binding alone, since the EGP-2-recognizing antibody MOC31 can be given to
patients in a dose of at least 50 mg kg-1 without any toxic side-effects (unpublished results).Anti-CD3 directed antibodies (complete Ig with an intact Fc portion) however, have shown
to be toxic in cancer patients with a MTD of also approximately 5 µg kg-1 (400 µg total dose).However, neurotoxicity with an onset of 12 h after infusion was dose limiting in this setting
(31). The observed toxicity appears therefore to be related to the combined (i.e. bispecific)binding activity of BIS-1 F(ab’)2. T-cell activation, which could possobly induce toxicity,
requires not only binding of BIS-1 F(ab’)2 to CD3 but also clustering of the CD3 molecules(32). Since the BIS-1 F(ab’)2 has only a monovalent binding site to the CD3 molecule,
clustering of CD3 molecules and therefore triggering of T-cell activation is thought to bepossible only by immobilisation of BIS-1 F(ab’)2 via its EGP-2 binding site. Since no EGP-2-
positive circulating (blood) cells are present, it is speculated that BIS-1 F(ab’)2 might havereacted with tumour cells, or possibly some normal epithelia, after leaving the blood
circulation. Subsequently, eitherin situ present or newly extravasated T lymphocytes couldhave been triggered through cross-linking of the CD3 complexes by BIS-1. A more likely
explanation is that BIS-1 F(ab’)2 bound preferentially to T lymphocytes in the circulation.After extravasation of some of these cells, possibly induced by IL-2, these BIS-1 F(ab’)2-
loaded cells may react with EGP-2 on tumour or epithelia. The tumour-T cell interactionmight subsequently trigger the production of secondary cytokines like TNF-α and IFN-γresulting in the enhanced extravasation of both lymphocytes and monocytes, as we observedin the present study.In vivo binding of BIS-1 F(ab’)2 to peripheral blood T lymphocytes was
evaluatedex vivoboth functionally by a51Cr-release assay and immunocytologically using a
sensitive indirect staining method for flow cytometry. For the51Cr-release assay, performedto evaluate also functional binding of BIS-1, PBMC obtained from the patients just prior to
and directly after the infusion of BIS-1 were used. Figure 3 shows thatin vivo BIS-1 F(ab’)2-loaded T lymphocytes were able to specifically lyse EGP-2-positive tumour cellsin vitro.
Although the E/T ratio of 100/1 is of little clinical relevance, it is indicative for the functional
binding of BIS-1 F(ab’)2 in vivo. At 3 µg kg-1 BIS-1 F(ab’)2 up to approximately 45% of themaximal obtainable cytotoxicity against EGP-2-positive target cells could be measured. Owing
to the partial loss of BIS-1 F(ab’)2 during isolation (see Figure 2), this finding is probably anunderestimation of the actualin vivo capacity to exert anti-tumour activity. The SCLC cell
lines GLC-1 and GLC-1M13 are relatively resistant to LAK activity (own observation) andas a result no cytotoxicity was measured in the absence of BIS-1 F(ab’)2. At 5 µg kg-1 the
target cell killing capacity of PBMCs after the infusion was found to be approximately 50%of the cytotoxicity observed with addition of an optimal concentration of BIS-1 to the assay.
However, this was mainly due to the substantially lower maximal inducible cytotoxicity after
104

the infusion with BIS-1 F(ab’)2 as compared to the maximal cytotoxic capacity before theinfusion at this dose.
This last phenomenon appears to be related to the observed rapid reduction of theamount of PBMCs in the peripheral blood during the infusion of 5 µg kg-1 BIS-1 F(ab’)2. Such
a reduction of PBMCs occurred to a much lesser extend at 3 µg kg-1 BIS-1 F(ab’)2 (seeFigures 5 and 6 ). However, the low number of circulating PBMCs itself can not explain the
reducing killing capacity of the isolated PBMCs since the cytotoxicity assays were performedat a fixed E/T ratio. Lymphocyte subset analysis of blood samples taken before and after
infusion with 5 µg kg-1 BIS-1 F(ab’)2 showed in addition to the general disappearance ofPBMCs, a preferential reduction in the percentage LFA-1α-bright and HLA-DR-positive cells
within the CD3/CD8 double positive lymphocyte population (see table III), whereas thepercentage CD3- and CD8-positive cells was not altered by the infusion. The LFA-1α-bright
positive T-cell population has been described as the main population responsible for cytolyticactivity (33,34). The importance of LFA-1 for the induction of target cell lysis is also
indicated from the observation that ICAM-1-negative target cells are relatively resistant tolysis by BsMAb-redirected cytolytic effector cells (35-38). Furthermore, LFA-1α-bright cellshave been shown to leave the circulation during acute immune responses (39). As discussed
above, extravasation of these cells might have been initiated by the TNF-α produced duringthe infusion with BIS-1. TNF-α is known to induce up-regulation of endothelial adhesion
molecules like ICAM-1 and E-selectin that are involved in the migration of leucocytes(40-43). Since LFA-1α-bright cells have high avidity for both ICAM-1 and -2 (44), this might
explain the reduction of especially CD3/CD8/LFA-1α-bright positive T lymphocytes from thecirculation which subsequently explains the observed decreased maximal target cell killing in
vitro after infusion with 5 µg kg-1 BIS-1 F(ab’)2. The production of IFN-γ in addition to TNF-α, as observed after treatment with 5 µg kg-1 BIS-1 F(ab’)2, can be taken as a further
indication of BIS-1 induced T-cell activation.We observed one partial response in 14 evaluable patients who where unresponsive
to initial s.c. IL-2 monotherapy. This is in line with the cytotoxic capacity of the redirectedcells observedin vitro, although a late response to IL-2 cannot be excluded. BsMAb-
redirected T lymphocytes, in contrast to genuine HLA-restricted cytotoxic T lymphocytes, areable to exert their lytic capacity only once towards a relevant target cell. Redirected killing
capacity can be restored, however, by adding new BsMAb (45). Therefore, to obtain betteranti-tumour responses, it might be necessary to give BIS-1 F(ab’)2 more than once to the
patient.In conclusion, BIS-1 F(ab’)2 can be given to cancer patients with a MTD of 5 µg kg-1
as a 2 h infusion, when combined with s.c. IL-2. BIS-1 F(ab’)2 can be detected on peripheralblood T lymphocytes both cytologically and functionally upon i.v. administration of the
BsMAb. At 5µg kg-1 BIS-1 F(ab’)2 a rapid induction of TNF-α and IFN-γ production isobserved and a transient leucopenia with a preferential depletion of LFA-1α-bright CD8
105

positive T lymphocytes from the blood is seen. The wide applicability of the EGP-2 antibodywarrants further investigations to fully exploit the full potential of this kind of immunothera-
py.
AcknowledgementThe authors acknowledge G. Mesander for excellent technical assistance with flow cytometricanalysis and J. Kosterink for advice concerning pharmaceutical aspects of BIS-1 F(ab’)2.
Large-scale production of BIS-1 and isolation of the bispecific antibody fraction was done incooperation with Dr. R. vd Griend (Biocult, Utrecht) and Dr W. de Vrij and Drs M.W.A. de
Jonge (MCA development, Groningen). This study was supported by a grant from the DutchCancer Society (Koningin Wilhelmina Fonds, 89-07).
References
1. Rosenberg SA, Lotze MT, Yang JC, Aebersold PM, Linehan WM, Seipp CA and White DE. Experiencewith the use of high-dose interleukin-2 in the treatment of 652 cancer patients. Ann. Surg. 1989; 210:474-485.
2. Sleijfer DT, Janssen RA, Buter J, De Vries EGE, Willemse PHB and Mulder NH. Phase II study ofsubcutaneous interleukin-2 in unselected patients with advanced renal cell cancer on an outpatient basis.J. Clin. Oncol. 1992; 10: 1119-1123.
3. Janssen RAJ, Buter J, Straatsma E, Heijn AA, Sleijfer DTh, De Vries EGE, Mulder NH, The TH andDe Leij L. HLA-DR-expressing CD8bright cells are only temporarily present in the circulation duringsubcutaneous interleukin-2 therapy in renal cell carcinoma patients. Cancer Immunol. Immunother. 1993;36: 198-204.
4. Bolhuis RLH, Sturm E and Braakman E. T cell targeting in cancer therapy. Cancer Immunol.Immunother. 1991; 34: 1-8.
5. Kerr L, Huntoon C, Donohue J, Leibson PJ, Bander NH, Ghose T, Luner SJ, Vessella R and McKeanDJ. Heteroconjugate antibody-directed killing of autologous human renal carcinoma cells by invitro-activated lymphocytes. J. Immunol. 1990; 144: 4060-4067.
6. Ferrini S, Prigione I, Miotti S, Ciccone E, Cantoni C, Chen Q, Colnaghi MI and Moretta L. Bispecificmonoclonal antibodies directed to CD16 and to a tumor- associated antigen induce target-cell lysis byresting NK cells and by a subset of NK clones. Int. J. Cancer 1991; 48: 227-233.
7. Mezzanzanica D, Garrido MA, Neblock DS, Daddona PE, Andrew SM, Zurawski CR, Segal DM andWunderlich JR. Human T-Lymphocytes targeted against an established human ovarian carcinoma witha bispecific F(ab’)2 antibody prolong host survival in a murine xenograft model. Cancer Res. 1991;51(20): 5716-5721.
8. Segal DM, Qian JH, Andrew SM, Titus JA, Mezzanzanica D, Garrido MA and Wunderlich JR. Cytokinerelease by peripheral blood lymphocytes targeted with bispecific antibodies, and its role in blockingtumor growth. Ann. N. Y. Acad. Sci. 1991; 636: 288-291.
9. Weiner GJ and Hillstrom JR. Bispecific anti-idiotype/anti-CD3 antibody therapy of murine B celllymphoma. J. Immunol. 1991; 147: 4035-4044.
10. Weiner LM, Holmes M, Adams GP, LaCreta FL, Watts P and Palazzo IG. A human tumor xenograftmodel of therapy with a bispecific monoclonal antibody targeting c-erb-2 and CD16. Cancer Res. 1993;52: 94-100.
106

11. Nitta T, Sato K, Yagita H, Okumura K and Ishii S. Preliminary trial of specific targeting therapy againstmalignant glioma. Lancet 1990; 335: 368-371.
12. Bolhuis RLH, Lamers CHL, Goey SH, Eggermont AMM, Trimbos JBMZ, Stoter G, Lanzevecchia A,di Re E, Miotti S, Raspagliesi F, Rivoltini L and Colnaghi MI. Adoptive immunotherapy of ovariancarcinoma with bs-Mab-targeted lymphocytes: a multicentre study. Int. J. Cancer 1992; supplement 7:78-81.
13. Kroesen BJ, ter Haar A, Spakman H, Willemse PHB, Sleijfer DTh, De Vries EGE and Mulder NH.Local antitumour treatment in carcinoma patients with bispecific monoclonal antibody redirected T-cells.Cancer Immunol. Immunother. 1993; 37: 400-407.
14. De Leij L, Helfrich W, Stein R and Mattes MJ. SCLC cluster 2 antibodies detect thepancarcinoma/epithelial glycoprotein EGP-2. Int. J. Cancer 1993; (In Press)
15. Herlyn M, Steplewski Z, Herlyn D and Koprowski H. Colorectal carcinoma specific antigen: detectionby means of monoclonal antibodies. Proc. Natl. Acad. Sci. U. S. A. 1979; 75: 1438-1452.
16. Beverly PCL, Souhami RL amd Bobrow L. Proceedings of the first international workshop on SmallCell Lung Cancer Antigens. In: Souhami RL, Beverley L, Bobrow L, eds. Lung Cancer. 4th Ed.Amsterdam: Elseviers Sience Publishers, 1988: 15-36.
17. Steplewski Z, Chang TH, Herlyn M and Koprowski H. Release of antibody-defined antigens by humancolorectal carcinoma and melanoma cells. Cancer Res. 1981; 41: 2723-2727.
18. Varki NM, Reisveld RA and Walker LE. Antigens associated with a human lung adenocarcinomadefined by monoclonal antibodies. Cancer Res. 1984; 44: 681-687.
19. Sindelar WF, Maher MM, Herlyn D, Sears HF, Steplewski Z and Koprowski H. Trial of therapy withmonoclonal antibody 17-1A in pancreatic carcinoma: prilimary results. Hybridoma Suppl. 1986; 1p:125-132.
20. Samonigg H, Wilders-Trussching M, Loibner H, Plot R, Rot A, Kuss I, Werner G, Stoger H, WrannM and Herlyn D. Immune response to tumor antigens in a patient with colorectal cancer afterimmunization with anti-idiotype antibody. Clin. Immunol. Immunopathol. 1992; 65: 271-277.
21. Bach FH, Geller RL, Nelson PJ, Panzer GG, Benfield MR, Inverardi L, Podack ER, Witson JC,Houchins JP and Alter BJ. A minimal stepwise activation analysis of functional maturation of Tlymphocytes. Immunol. Rev. 1989; 111: 35-57.
22. De Jong R, Brouwer M, Rebel VI, Van Seventer GA, Miedema F and Van Lier RAW. Generation ofalloreactive cytolytic T lymphocytes by immobilized anti-CD3 monoclonal antibodies. Analysis ofrequirements for human T-lymphocyte differentiation. Immunology 1990; 70: 357-364.
23. Fisher B, Packard BS, Carrasquillo JA, Carter CS, Topalian SL, Yang JC, Yolles P, Larson SM andRosenberg SA. Tumor localization of adoptively transferred indium-111 labeled tumor infiltratinglymphocytes in patients with metastatic melanoma. J. Clin. Oncol. 1989; 7: 250-261.
24. Pankonin G, Reipert B and Agar A. Interaction between interleukin-2 activated lymphocytes andvascular endothelium: binding to and migration across specialized and non-specialized endothelia.Immunology 1990; 7751-7760.
25. De Lau WJM, Van Loon AE, Heije K, Valerio D and Bast BJ. Production of hybrid hybridomas onHATs-neomycinr double mutants. J. Immunol. 1989; 117: 1-8.
26. WHO Handbook for reporting results of cancer treatment. 48th Ed. Den Haag: Martinus Nijhoff, 1979:27. Zola H, Neoh SH, Manzioris BX, Webster J and Loughan MS. Detection by immunofluorescence of
surface molecules present in low copy numbers. High sensitivity staining and calibration of flowcytometer. J. Immunol. Methods 1990; 135: 247-255.
28. Tax WJM, Willems HW, Reekers PPM, Capel PJA and Koene RH. Polymorphism and mitogenic effectof IgG monoclonal antibodies against T3 antigen on human T-Cells. Nature 1983; 304: 445-447.
29. De Leij L, Postmus EP, Buys CHCM, Elema JD, Ramaekers F, Poppema S, Brouwer M, Van der VeenAY, Mesander G and The TH. Characterization of three new variant cell lines derived from small cellcarcinoma of the lung. Cancer Res. 1985; 45: 6024-6033.
30. Tibben JG, Boerman OC, Claessens RAMJ, Corstens FHM, Van Deuren M, De Mulder PHM, Van derMeer JWM, Keijser KGG and Massuger LFAG. Cytokine release in an ovarian carcinoma patientfollowing intravenous administration of bispecific antibody OC/TR F(ab’)2. J. Natl. Cancer Inst. 1993;85: 1003-1004.
31. Buter J, Janssen RAJ, Martens A, Sleijfer DT, De Leij L and Mulder NH. Phase I/II of low doseintravenous OKT3 and subcutaneous interleukin-2 in metastatic cancer. Eur. J. Cancer 1993; 29A:
107

2108-2113.32. Schwab R, Crow MK, Russo C and Weksler ME. Requirements for T cell activation by OKT3
monoclonal antibody: role of modulation of T3 molecules and interleukin 1. J. Immunol. 1985; 135:1714-1718.
33. Morimoto C, Rudd CE, Letvin NL and Schlossmann SF. A novel epitope of the LFA-1 antigen whichcan distinguish killer effector and suppressor cells in human CD8 cells. Nature 1987; 330: 479-482.
34. Tsubota H, Lord CI, Watkins CM, Morimoto C and Letvin L. A cytotoxic T-lymphocyte inhibitsacquired immunodeficiency syndrome virus replication in peripheral blood lymphocytes. J. Exp. Med.1989; 169: 1421-1434.
35. Rivoltini L, Cattoretti FA, Mastroioanni A, Melani C, Colombo MP and Parmiani G. The high lysabilityby LAK cells of colon-carcinoma cells resistant to doxorubricin is associated with a high expression ofICAM-1, LFA-3, NCA and to a less-differentiated phenotype. Int. J. Cancer 1991; 47: 746-754.
36. Braakman E, Goedebuure PS, Vreugdehil RJ, Segal DM and Bolhuis RLH. ICAM- melanoma cells arerelatively resistant to CD3-mediated T-cell lysis. Int. J. Cancer 1990; 46: 475-480.
37. Webb DSA, Motowski Hand Gerrard ThL. Cytokine-induced enhancement of ICAM-1 expression resultsin increased vulnerability of tumor cells to monocyte mediated lysis. J. Immunol. 1991; 146: 3682-3686.
38. Stotter H, Wiebke EA, Tomita S, Belldegrun A, Topalian S, Rosenberg SA and Lotze MT. Cytokinesalter target cell susceptibillity to lysis. Evaluation of tumor infiltrating lymphocytes. J. Immunol. 1989;142: 1767-1773.
39. Hviid L, Theander TG, Abdulhadi NH, Abu-Zeid YA, Bayoumi RA and Jensen JB. Transient depletionof T cells with high LFA-1 expression from peripheral circulating during acute plasmodium falciparummalaria. Eur. J. Immunol. 1991; 21: 1249-1253.
40. Zimmermann GA, Prescot SA and McIntyre TM. Endothelial cell interactions with granulocytes.Tethering and signaling molecules. Immunology Today 1992; 13: 93-100.
41. Graeves MW. Early cellular and molecular events in inflamed skin: an integrated concept. J. Dermatol.Science 1992; 3: 1-5.
42. Vogetseder W, Feichtinger H, Schulz TF, Schwaeble W, Tabaczewski P, Mitterer M, Bock G, MarthCh, Dapunt O, Mikuz G and Dierich MP. Expression of 7F7-antigen, a human adhesion moleculeidentical to intracellular adhesion molecule-1 (ICAM-1) in human carcinomas and their stromalfibroblasts. Int. J. Cancer 1989; 43: 768-773.
43. Nickoloff BJ and GriffithCEM. T lymphocytes and monocytes bind to keratinocytes in frozen sectionsof biopsy specimens in normal and inflamed skin: modulation by recombinant gamma interferon andtumour necrosis factor. J. Am. Acad. Dermatol. 1989; 20: 617-629.
44. Diamond MS, Staunton DE, Marlin SD and Springer TA. Binding of the integrin Mac-1 (CD11b/CD18)to the third immunoglobulin-like domain of ICAM-1 (CD54) and its regulation by glycosilation. Cell1991; 65: 961-971.
45. Blank-Voorthuis CJAC, Braakman E, Ronteltap CPM, Tilly BC, Sturm E, Warnaar SO and BolhuisRLH. Clustered CD3/TCR complexes do not transduce activation signals following bispecificmonoclonal antibody triggered lysis by CTL via CD3. J. Immunol. 1993; 151 (6): 2904-2914.
108

Chapter 6
Recombinant interleukin-2 for metastatic renal cellcarcinoma in hemodialysis patients
J.Buter1, R.A.J.Janssen2, N.H.Mulder1, P.E. de Jong3, L. de Leij2 and D.Th. Sleijfer1.
Departments of Medical Oncology1, Immunology2 and Nephrology3, University Hospital,Oostersingel 59, 9713 EZ Groningen, The Netherlands.
Summary
The toxicity and efficacy of an outpatient therapy regimen with subcutaneous interleukin-2 in
two patients with advanced renal cell carcinoma who were on hemodialysis are described.Although objective responses were not seen in these patients, subcutaneous IL-2 induces
immunological changes, that are similar to those seen after intravenous IL-2 therapy and are
indicative for the in vivo induction of peripheral blood lymfokine activated killer cell (LAK)activity. This treatment has a mild toxicity and can be given to patients with major organ
dysfunction who are on hemodialysis.
Introduction
Cytotoxic and hormonal therapies have had little impact on metastatic renal cell carcinomas.
Interferon has shown some activity, but responses are infrequent and the duration of responses
is usually short (1). Recombinant interleukin-2 has been used as a treatment of renal cellcancer using a variety of dosages and schedules. This therapy, although effective, has been
associated with severe toxicity sometimes requiring intensive care monitoring and vasopressorsupport (2,3). Recently, we have described an effective, low-toxic schedule of IL-2 given
subcutaneously on an outpatient basis for patients with metastatic renal cell cancer (4). We
describe here the application of this regimen in two patients on hemodialysis with specialemphasis on toxicity and immunological parameters.
109

Methods
Monoclonal antibodiesThe monoclonal antibodies (Mab) Leu4-FITC, Leu3-FITC, Leu2-FITC/PE, Leu19-
PE/unlabelled, anti-HLA-Dr-FITC/PE and anti-IL-2Ralfa-FITC/PE were obtained from
Bencton Dickinson, Mountain View, CA, USA and were directly conjugated withphycoerythrin (pe) or fluorescein-isothyocyanaat (fitc).
Immunostaining of cells and flow cytometryWhole EDTA-blood was stained within four hours after collection. To 100 µl of whole blood
20 µl of monoclonal antibody preparation (containing 0.5 µg of assessed Mab) was added andthe sample was incubated at room temperature for fifteen minutes. Two ml of FACS-lysing
solution (Becton Dickinson, Mountain View, CA, USA) was added and the cells wereincubated for an additional ten minutes. Subsequently, the solution was centrifugated and the
cells were washed in phosphate buffered saline supplied with 0.092 mg/ml heparine (PBS/hep)
and resuspended in 150 µl. The samples were immediately analyzed on a FACstar (BectonDickinson, Moutain View, CA, USA) with the laser tuned at 488 nm. Lymphocytes were
gated using standard FSC/SSC settings, which excluded the monocytes and granulocytes fromanalysis.
Soluble IL-2 receptorSoluble IL-2 receptor (IL-2R) in serum was measured by a sandwich ELISA (T-cell Sciences,
Inc, Cambridge Massachusetts).
Case histories
The first patient, male, was born in 1934. In 1965 a nephrectomy of the right kidney was donebecause of nephrolithiasis. In September 1989, a nephrectomy of the left kidney was
performed because of a renal cell carcinoma, stage T3G2N0M0, followed by dialysis, whichwas complicated by ventricular and supraventricular ectopic arrhytmias.
In January 1990 multiple lung metastases were diagnosed, because of pulmonary
complaints related to progression of these lung metastases IL-2 therapy was started in April1990. IL-2 was given in a 5-day cycle of Cetus IL-2 (EuroCetus, Amsterdam, The
Netherlands), given subcutaneously every week for 6 consecutive weeks. During the first weekthe patient was hospitalized, whereas the rest of the treatment was on an outpatient basis.
During the first 5-day cycle 18x106 International Units IL-2 was given once daily, in the
following cycles the dose in the first two days was routinely reduced to 9x106 InternationalUnits. Other treatment consisted of paracetamol to prevent pyretic reactions, and
110

erythropoietin because of dialysis related anemia. During IL-2 treatment a supraventriculartachycardia occurred which could be terminated by intravenously administration of verapamil.
Toxicity of IL-2 administration consisted of transient inflammation and local induration at the
injection sites, fever and chills WHO grade II (four cycles), anorexia, nausea, vomiting anddiarrhea grade I (two cycles), an increase in serum levels of alkaline phosphatase (from 277
to 409 U/l, N ≤ 120), lactic dehydrogenase (from 212 to 416 U/l, N≤ 235) andgamma-glutamyl transferase (from 232 to 300 U/l, N≤ 65). The hemoglobin concentration
remained stable at an average of 85 g/l. The leukocyte count rose from 7.0 to a maximum of
16.2x109 cells/l (n = 4.0-11.0), eosinophils from 0.2 to a maximum of 2.7 x 109 cells/l (n =0-0.4). No thrombocytopenia was found. Immunological changes are listed in table 1. The
pretreatment blood pressure 130/90 mm Hg decreased to a lowest value of 90/60 mm Hg.Fluid retention, weight gain and nephrotoxicity caused by IL-2 could not be evaluated because
of the hemodialysis, which was continued initially two times a week for 5 3/4 hours, later on
three times a week for 4 hours because of uremic pericarditis. During the dialysis sessionsthere was a delta systolic blood pressure of 10±15 mm Hg (mean and SD, n = 15 ). After the
six weeks of treatment, restaging showed progressive disease, therefore IL-2 was discontinued.The patient died six weeks later as a result of tumor progression.
The second patient, male, born in 1915, underwent an nephrectomy in 1980 because
of a renal cell cancer of the left kidney, and a nephrectomy in June 1986, also because of arenal cell cancer, of the right kidney, T2N0M0, followed by hemodialysis. Thereafter, the
patient had been hospitalized because of hypertensive encephalopathy (1986), supraventriculartachycardia (1986) and a bleeding duodenal ulcer (1987). In 1989 slowly progressive lung
metastases were diagnosed, for which IL-2 was given in April 1990, in a 5-day cycle of Cetus
IL-2 in the same schedule as in the first patient. The patient also received paracetamol toprevent pyretic reactions.
Toxicity of IL-2 consisted of local inflammation and induration at the injection sites,fever WHO grade II (one cycle), nausea grade I (two cycles) and diarrhea grade I (four
cycles). There was an increase in serum levels of alkaline phosphatase (from 96 to 179 U/l),
lactic dehydrogenase (from 283 to 327 U/l) and gamma-glutamyl transferase (from 33 to 158U/l). The hemoglobin concentration decreased from 111 to 95 g/l. The initial leukocyte count
rose from 8.5 to a maximum of 27.3x109 cells/l, eosinophils rose from 0.8 to 11.4x109 cells/l.No thrombocytopenia was found. Immunological changes are listed in table 1. The
pretreatment blood pressure 115/80 mm Hg decreased to a lowest value of 75/50 mm Hg.
Hemodialysis was continued twice weekly for 5 3/4 hours. During the dialysis sessions therewas a delta systolic blood pressure of -15±20 mm Hg (mean and SD, n = 13). After six week
of treatment restaging showed stable disease. Further treatment was discontinued on requestof the patient because of symptomatic hypotension, increasing after each dialysis. The patient
died 21 weeks later because of brain metastases.
111

Tabel 1. Immunological changes during IL-2 therapy.
Patient
Variable 1 2
No. of CD3+ cells
103/ml
Baseline
PeakAfter treatment
350
880670
370
23801130
No. of CD56+CD3- cells103/ml
Baseline
Peak
After treatment
50
500
500
90
1210
780
CD3+HLA-Dr+†
5 (3%)‡
BaselinePeak
1434
1557
CD56+HLA-Dr+†4 (3%)
Baseline
Peak
27
74
25
52
CD3+CD25+†
3 (2%)
Baseline
Peak
19
36
8
56
Soluble IL-R
(69-477 U/ml)Baseline
Peak
2541
24775
1521
22268
Normal values in parentheses.
†Expressed as percentage of the CD3+ or CD56+ subset, respectively.
‡Mean (S.D.)
112

Discussion
The 30% response rate in patients treated with recombinant IL-2, has opened a newtherapeutic approach in the treatment of renal cell carcinoma. Severe toxicity with a treatment
related mortality of 2.5%, however, can complicate the administration of high dose
intravenous IL-2 (2). A major side effect is an apparent increase in capillary permeability anda decrease in vascular resistance, resulting in hypotension, azotemia, oliguria, weight gain and
interstitial pulmonary edema for which vasopressors and intubation with assisted ventilationwas indicated in several patients. Other toxicity consisted of fever, chills, nausea, vomiting,
diarrhea, bone marrow toxicity, hyperbilirubinemia and cardiac toxicity such as arrhythmias
and infarction.Because of the toxicity related to intravenous IL-2 treatment, this therapy appears only
suitable for fit patients in which special attention is given to renal, cardiovascular andpulmonar function. Renal cell carcinoma has a maximum incidence in patients 40-60 years
of age, a group in which also a maximum incidence of cardiovascular and pulmonary disease
occurs. So, a number of patients with renal cell carcinoma are not eligible for intravenousIL-2 treatment. Therefore, many investigators have looked for less toxic regimens (3-7).
Subcutaneously administered IL-2 alone or combined with interferon alfa, can inducetumor regression in up to 20 percent in renal cell carcinoma (4-7). Patients can be treated on
an outpatient basis, IL-2 is injected by themself, and toxicity consists of painful swelling at
the injection site, fever, chills, nausea, vomiting, diarrhea, pruritus and mild hypotension.None of these side effects requires hospitalization, and they are acceptable even in patients
with major organ dysfunction.Based on the strict entry criteria for intravenous IL-2 studies, the two patients
described here were clearly not eligible for such treatment. Because of the limited toxicity of
subcutaneous IL-2 (4), both patients were offered and instituted on this form of treatment.Although in both patients an objective tumor regression was not found after six weeks of
treatment, subcutaneously administered IL-2 induced an increase in circulating T-lymphocytes(CD3+) with an increased expression of HLA-Dr and IL2-R (CD25) antigens, indicating their
activation. There was a markedly increase in cells with the natural killer cell phenotype
(CD3-CD56+) with increased expression of HLA-Dr. This population is considered to containthe cells with lymphokine activated killer cell (LAK) activity (8-10). The increase in soluble
IL-2 receptor (IL-2R) also signifies an increased number of activated lymphocytes (10,11).These changes are similar to those seen after IL-2 therapy in other patients (4,8-10), and
suggest that subcutaneously given IL-2 induces peripheral blood LAK activity in these
patients.Toxicity of subcutaneous IL-2 in both patients was comparable with the toxicity in
other patients treated with the same schedule, except for the somewhat more pronouncedhypotension. IL-2 treatment can induce a syndrome consisting of azotemia, oliguria and
113

decreased excretion of sodium. This syndrome is ascribed to renal hypoperfusion and resultantprerenal azotemia, characterized by an increased BUN to creatinine ratio due to enhanced
resorption of ureum with sodium and water (12). Besides, an intrarenal defect caused by IL-2
has been described (13). In our anefritic patients, lacking the renin-angiotensin-aldosteronesystem to regulate bloodpressure, the influence of IL-2 on this parameter cannot be
determined, especially because hemodialysis is frequently associated with profoundhypotension due to autonomic and ventricular dysfunction (14).
This report illustrates that subcutaneously IL-2 can be given in an outpatient regimen
to patients with advanced renal cell cancer on hemodialysis, causing immunological changesthat are indicative for periferal blood LAK activity.
AcknowledgementsWe thank A. Heyn and R. Brons for their assistance with the FACS analysis.
References
1. Muss HB. Interferon therapy for renal cell carcinoma. Semin. Oncol. 1987; 14 (suppl 2): 36-42.2. Rosenberg SA, Lotze MT, Muul LM, Chang AE, Avis FP, Leitman S, Lineham WM, Robertson CN,
Lee RE, Rubin JT, Seipp CA, Simpson CG and White DE. A progress report on the treatment of 157patients with advanced cancer using lymphokine-activated killer cells and interleukin-2 or high-doseinterleukin-2 alone. N. Engl. J. Med. 1987; 316: 889-897.
3. West WH, Tauer KW, Yanelli JR, Marshall GD, Orr DW, Thurman GD and Oldham RK. Constantinfusion recombinant interleukin-2 in adoptive immunotherapy of advanced cancer. N. Engl. J. Med.1987; 316: 898-905.
4. Sleijfer DTh, Janssen RAJ, Willemse PHB, Martens A, Leij de L, De Vries EGE and Mulder NH.Low-dose regimen of interleukin-2 for metastatic renal carcinoma. Lancet 1990; 335: 1522-1523.
5. Atzpodien J, Korfer A, Franks CR, Poliwoda H and Kirchner H. Home therapy with recombinantinterleukin-2 and interferon-α2b in advanced human malignancies. Lancet 1990; 335: 1509-1512.
6. Whitehead RP, Ward D, Hemmingway L, Hemstreet GPIII, Bradly E and Konrad M. Subcutaneousrecombinant interleukin 2 in a dose escalating regimen in patients with metastatic renal celladenocarcinoma. Cancer Res. 1990; 50: 6708-6715.
7. Stein RC, Malkovska V, Morgan S, Galazka A, Aniszewski C, Roy SE, Shearer RJ, Marsden RA,Bevan D, Gordon-Smith EC and Coombes RC. The clinical effects of prolonged treatment of patientswith advanced cancer with low-dose interleukin-2. Br. J. Cancer 1991; 63: 275-278.
8. Weil-Hillman GW, Fisch P, Prieve AF, Sosman JA, Hank JA and Sondel PM. Lymphokine activatedkiller activity induced by in vivo interleukin 2 therapy: predominant role for lymphocytes with increasedexpression of CD2 and Leu19 antigens but negative expression of CD16 antigens. Cancer Res. 1989;49: 3680-3688.
9. Sosman JA, Kohler PC, Hank JA, Moore KH, Bechhofer R, Storer B and Sondel PM. Repetitive weeklycycles of interleukin-2. II. clinical and immunologic effects of dose, schedule, and addition ofindomethacin. J. Natl. Cancer Inst. 1988; 80: 1451-1461.
10. Urba WJ, Steis RG, Longo DL, Kopp WC, Maluish AE, Marcon L, Nelson DL, Stevenson HC andClark JW. Immunomodulatory properties and toxicity of interleukin-2 in patiewnts with cancer. CancerRes. 1990; 50: 185-192.
11. Rubin LA and Nelson DL. The soluble interleukin-2 receptor: biology, function, and clinical application.Ann. Intern. Med. 1990; 113: 619-627.
12. Belldegrun A, Webb DE, Austin III HA, Steinberg SM, White DE, Linehan WM and Rosenberg SA.
114

Effects of interleukin-2 on renal function in patients receiving immunotherapy for advanced cancer. Ann.Intern. Med. 1987; 106: 817-822.
13. Shalmi CL, Dutcher JP, Feinfeld DA, Chun KJ, Saleemi KR, Freeman LM, Lynn RI and Wiernik PH.Acute renal dysfunction during interleukin-2 treatment: suggestion of an intrinsic renal lesion. J. Clin.Oncol. 1990; 8: 1839-1846.
14. Heber ME, Lahari A, Thompson B and Raftery EB. Baroreceptor, not left ventricular function is thecause of hemodialysis hypotension. Clin. Nephrol. 1989; 32: 79-86.
115


Chapter 7a
Infection after subcutaneous interleukin-2
Jan Buter, Elisabeth G. E. de Vries, Dirk Th. Sleijfer, Pax H. B. Willemse
and Nanno H. Mulder.
Department of Medical Oncology, University Hospital Groningen, The Netherlands
Introduction
High-dose IL-2 therapy given either as intravenous (IV) bolus injections or continuous
infusion is associated with a high frequency of significant bacterial infections in cancerpatients. Sepsis was one of the major causes of IL-2 therapy related deaths in the initial
protocols (1-3). Most infections are related to indwelling central venous catheters that are in
place for several days. But also changes in the host defence mechanism with a chemotacticdefect in neutrophils have been reported in patients receiving IL-2 therapy (4). Recently, Jones
(5) reported a high frequency of bacteriological proven infection in patients receivingsubcutaneous IL-2 and Interferon-α in the absence of central venous catheters, which they
attribute to IL-2 treatment. They advise careful monitoring of treatment with subcutaneous IL-
2, and the investigation of the role of prophylactic antibiotics in this context. We reportedearlier an outpatient regimen with single-agent subcutaneous IL-2 in patients with
disseminated renal cell cancer (6). We retrospectively analyzed and report here our experienceconcerning the rate of infection in this regimen.
Patients and methods
Patients received daily subcutaneous injections of 18 x 106 International Units IL-2
(EuroCetus, Amsterdam, Netherlands) on day 1 to 5 in the first week, while the dose in thefirst two days of the following weeks was reduced to 9 x 106 International Units. Patients
were treated for 4 or 6 weeks. Treatment was repeated after 2 to 3 weeks rest period to a
maximum of 3 courses. Paracetamol 250-500 mg orally every 4 to 6 hours was given tosuppress pyretic reactions. Patients visited the outpatient clinic on day 1 and 5 of every
weekly cycle. Toxicity was assessed with a patient interview, physical examination, full bloodcounts, assessment of renal, liver, and coagulation functions. No routine blood cultures were
performed. In case of clinical signs of infection appropriate cultures were taken and antibiotic
117

treatment was initiated.
Results
A total of 42 patients, 24 men and 18 women, mean age 59 years (range 29-76) received 468
weeks of treatment. We found clinical evidence of infection for which antibiotics wereindicated on 6 occasions. ( 1.3% ) One patient with a spinal cord lesion and atonic bladder
was treated three times for recurrent urinary infections which were related to the urinarycatheter. A second patient received antibiotics for a local infection with group B hemolytic
streptococci in the leg which was compromised with a thrombotic venous occlusion. One
patient with multiple lung metastases was treated for a clinical pulmonary infection and onepatient was treated for a clinical epididymitis.
Discussion
Although no routine blood cultures were performed and asymptomatic bacteriaemia cannot
be excluded, the low incidence of clinical infection in this group of 42 patients and theabsence of symptoms that could be ascribed to bacteriaemia suggest that there is no indication
for the use of prophylactic antibiotics in patients treated with single-agent subcutaneous IL-2.Since no excess of infection in cancer patients receiving IFNα has been reported (7,8), the
relation between combination therapy with IL-2 and IFNα and infection needs further investi-
gation.
References
1. Rosenberg SA, Lotze MT, Muul LM, Chang AE, Avis FP, Leitman S, Lineham WM, Robertson CN,Lee RE, Rubin JT, Seipp CA, Simpson CG and White DE. A progress report on the treatment of 157patients with advanced cancer using lymphokine-activated killer cells and interleukin-2 or high-doseinterleukin-2 alone. N. Engl. J. Med. 1987; 316: 889-897.
2. Dutcher JP, Gaynor ER, Boldt DH, Doroshow JH, Bar MH, Sznol M, Mier J, Sparano J, Fisher RI,Weiss G and et al . A phase II study of high-dose continuous infusion interleukin-2 withlymphokine-activated killer cells in patients with metastatic melanoma. J. Clin. Oncol. 1991; 9: 641-648.
3. Snydman DR, Sullivan B, Gill M, Gould JA, Parkinson DR and Atkins MB. Nosocomial sepsisassociated with interleukin-2. Ann. Intern. Med. 1990; 112: 102-107.
4. Klempner MS, Noring R, Mier JW and Atkins MB. An acquired chemotactic defect in neutrophils frompatients receiving interleukin-2 immunotherapy see comments. N. Engl. J. Med. 1990; 322: 959-965.
5. Jones AL, O’Brien ME, Moore J, Cropley I, Lorentzos A, Jameson B and Gore ME. Infectiouscomplications of subcutaneous interleukin-2 and interferon-alpha. Lancet 1992; 339: 181-182.
6. Sleijfer DTh, Janssen RAJ, Willemse PHB, Martens A, Leij de L, De Vries EGE and Mulder NH.Low-dose regimen of interleukin-2 for metastatic renal carcinoma. Lancet 1990; 335: 1522-1523.
118

7. Muss HB. Interferon therapy for renal cell carcinoma. Semin. Oncol. 1987; 14 (suppl 2): 36-42.8. Creagan ET, Twito DI, Johansson SL, Schaid DJ, Johnson PS, Flaum MA, Buroker TR, Geeraerts LH,
Veeder MH, Gesme DH,Jr. and et al . A randomized prospective assessment of recombinant leukocyteA human interferon with or without aspirin in advanced renal adenocarcinoma. J. Clin. Oncol. 1991;9: 2104-2109.
119


Chapter 7b
Neuropsychiatric symptoms during treatment withinterleukin-2
Jan Buter, Elisabeth G. E. de Vries, Dirk Th. Sleijfer, Pax H. B. Willemse
and Nanno H. Mulder
Department of Medical Oncology, University Hospital Groningen, The Netherlands
Introduction
Neuropsychiatric changes are frequently observed during IL-2 therapy. These side effects aredose and schedule dependent. On intensive treatment regimens with intravenous administration
of high-dose IL-2, patients become frequently agitated, combative, disoriented, or somnolent,and occasionally comatose (1-3). Fenner recently (4) reported neuropsychiatric symptoms
during outpatient combination treatment with subcutaneous interleukin-2 at a dose of 3 x 5-20
MIU/m², and interferon-α with or without subsequent intravenous 5-fluorouracil for metastaticrenal cell carcinoma in 39 of 101 patients. Treatment limiting neuropsychiatric symptoms
were less frequent than in patients treated with high-dose intravenous IL-2, and symptomsresolved spontaneously after cessation of treatment, possibly indicating brain metastases. All
three drugs used have their own neurotoxicity, and it is therefore difficult to attribute toxicity
to one of them. We report the neuropsychiatric toxicity of an outpatient regimen ofsubcutaneous IL-2 monotherapy in patients with renal cell cancer (5).
Materials and methods
A total of 61 patients with progressive metastatic renal cell carcinoma were treated. Mean agewas 59 years (range, 41 to 75 years) and 37 patients were male. Patients received daily
subcutaneous injections of 18 x 106 International Units IL-2 (EuroCetus, Amsterdam,Netherlands) on day 1 to 5 in the first week, while the dose in the first two days of the
121

following weeks was reduced to 9 x 106 International Units. Patients were treated for at leastfour consecutive weeks per course. Treatment was repeated after a 2 or 3 week rest period
unless progressive disease was recorded. Paracetamol 250-500 mg orally every 4 to 6 hours
was given to suppress pyretic reactions. Neuropsychiatric toxicity was evaluated everytreatment week.
Results
104 treatment courses were administered. Clinically relevant neuropsychiatric symptoms wererecorded in 14% of courses in 14 patients. IL-2 treatment was discontinued in 2 patients
because of neurotoxicity. One patient died of brain stem ischemia after a myocardial infarctionand one patient had progression of a partial spinal cord lesion due to metastases in the first
week of IL-2 treatment, for which treatment was discontinued. Coma or seizures did not
occur. Disorientation was noted in 2 patients; 2 had difficulties with concentration; 1complained about hallucinatory symptoms on the second day of treatment for which IL-2 dose
was temporarily reduced for one day whereupon symptoms resolved spontaneously; andsomnolence occurred in 3, peripheral neuropathy in 2, and vertigo in 2 with hypotension (psyst
< 100 mm Hg). Computer tomography of the brain revealed brain metastases in 2 patients,
with disorientation and depressive symptoms in 1 and headache and concentration difficultiesin the other.
Discussion
Clinically relevant neuropsychiatric symptoms during this outpatient regimen with
subcutaneous IL-2 monotherapy were rare and required cessation of treatment in 2% ofcourses. Brain metastases are not uncommon in renal cell cancer and as we found overt
metastases in 14% of patients with neuropsychiatric symptoms on IL-2 these symptoms maybe indicative of metastases of the brain or other central nervous system localizations.
References
1. Rosenberg SA, Lotze MT, Yang JC, Aebersold PM, Linehan WM, Seipp CA and White DE. Experiencewith the use of high-dose interleukin-2 in the treatment of 652 cancer patients. Ann. Surg. 1989; 210:
122

474-485.2. Siegel JP and Puri RK. Interleukin-2 toxicity. J. Clin. Oncol. 1991; 9: 694-704.3. Denicoff KD, Rubinow DR, Papa MZ and Seipp CA. The neuropsychiatric effects of treatment with
interleukin-2 and lymphokine activated killer cells. Ann. Intern. Med. 1987; 107: 293-300.4. Fenner MH, Hänninen EL, Kirchner HH, Poliwoda H and Atzpodien J. Neuropsychiatric symptoms
during treatment with interleukin-2 and interferon-α. Lancet 1993; 341: 372.5. Sleijfer DT, Janssen RA, Buter J, De Vries EGE, Willemse PHB and Mulder NH. Phase II study of
subcutaneous interleukin-2 in unselected patients with advanced renal cell cancer on an outpatient basis.J. Clin. Oncol. 1992; 10: 1119-1123.
123


Chapter 8
Fluorouracil/Leucovorin/Interferon α-2a in patients withadvanced colorectal cancer.
Effects of maintenance therapy on remission duration.
Jan Buter, Harm A.M. Sinnige, Dirk Th. Sleijfer, Elisabeth G.E. de Vries, Pax .H.B.
Willemse, Winette T.A. van der Graaf, René C.J. Verschueren1 and Nanno H. Mulder
Departments of Medical Oncology and1Surgical Oncology University Hospital,
Oostersingel 59, 9713 EZ Groningen,The Netherlands.
Summary
Background: We reported earlier a phase II study of combination treatment with 5-
fluorouracil (5-FU), leucovorin (LV), and interferonα-2a (IFN) in patients with previously
untreated metastatic colorectal cancer (Sinnige et al., Eur J Cancer 1993; 29A: 1715-20).Therapy was on an outpatient basis and consisted of LV 60 mg p.o. q8h day 1-3, IFN 18x106
IU s.c. day 1-3, and bolus 5-FU 750 mg/m2 i.v. day 2-3. Treatment was repeated every 14days, till a maximum of 8 courses. A response rate of 54% (95% confidence interval (CI),
34%-72%) was observed. However, remission duration after cessation of therapy was short
with a median duration of 5 months (range 2 to 13+).Methods:Subsequently entered patientsreaching a remission on this induction treatment received maintenance therapy: the above
described 3-day regimen every 6 weeks until progression, for a maximum of 2 years.
Results: Fifty-three patients were enroled in the induction regimen and 18 out of 29responding patients received maintenance treatment. In 50 assessable patients 3 CR and 26
PR were observed for a response rate of 58% (CI, 43-72%). Median remission duration ofpatients receiving maintenance therapy was 9.4 months (CI, 8.4-10.3 months) compared to
4.7 months (CI, 3.2-6.2 months) of patients without maintenance therapy (p= .032). Median
overall survival of all patients was 16.6 months. Toxicity of maintenance therapy was confinedto WHO grade 2.
Conclusion: The high response rate of this 5-FU/LV/IFN regimen holds true in a larger
group of patients. Moreover, maintenance therapy prolongs median remission duration inresponding patients without adding significant toxicity.
125

Introduction
Colorectal carcinoma is one of the major causes of cancer-related deaths in the western world.The prognosis of untreated patients with advanced disease is poor with a median survival time
of 10 months (1). The results of chemotherapy in these patients have been disappointing.
Single-agent therapy with 5-fluorouracil (5-FU) results in response rates of 15% with mostresponses being partial and non-lasting. Effects on survival, if any, are minimal (2, 3).
Addition of leucovorin (LV) to 5-FU has shown to improve anticancer activity bothpreclinically and clinically by modulating the inhibition of the target enzyme thymidilate
synthetase (4, 5). Other modulation studies have shown improved anticancer activity from the
combination of interferonα-2a (IFN) and 5-FU. Several synergistic mechanisms for thiscombination have been proposed, including altered intracellular and serum pharmacokinetics
of 5-FU induced by IFN (6, 7). We studied the combination of 5-FU, LV and IFN. This
triple-drug combination showed improved cytotoxicity over the two-drug combinationsin vitro(8, 9). We reported earlier on the first 28 assessable patients with previously untreated
metastatic colorectal cancer in a phase II study with a response rate of 54% (95% confidenceinterval (CI), 34%-72%). Despite this high activity, remission duration after cessation of
therapy was short with a median remission duration of 5 months (range 2-13+) (10). Since
then, patient accrual has continued, but patients with an objective response now receivedmaintenance courses every six weeks to a maximum of 2 years or until progression. To
investigate the role of maintenance therapy on the remission duration and the overall survival,we compared the second cohort receiving maintenance courses with the first cohort receiving
the induction treatment only.
Patients and methods
Patients with histologically documented bi-dimensionally measurable or assessable advanced
colorectal carcinoma, a WHO performance status (PS) of 0 to 2, an age between 18 and 75
years, with no prior chemotherapy and no uncontrollable concomitant diseases were eligible.Additional eligibility criteria included a leucocyte count of > 3x109/L, platelet count >
100x109/L, serum creatinine < 200 µmol/L, and serum bilirubin < 100 mmol/L. Informedconsent was obtained from all patients before the start of treatment and the study was
approved by the Medical Ethical Committee of the University Hospital Groningen, The
Netherlands. Appropriate radiologic examinations were obtained within 4 weeks of study-entryto serve as a baseline for serial evaluation of the patient’s disease status. Serum levels of
carcino-embryonic antigen (CEA) were determined before the start of treatment. After aninterim analysis the protocol was amended and patients in the second cohort with an objective
126

Table 1 . Patients’ characteristics
N
Patients 53
Male/female 28/25
Age(years)
median 53
range 27-69
Performance status
0 16
1 31
2 6
Prior radiotherapy 4
Time from diagnosis (months)
median 4
range 0-74
Primary tumor
Colon 33
Rectum 20
Sites of disease*
Liver only 38
Liver and lung 3
Liver and other site 9
Lung only 2
Abdominal 16
*Can be more than one site
127

response (CR or PR) after eight induction courses were given maintenance therapy. Theirnumber was estimated on detecting a doubling of remission duration with a power of 0.80 and
a p-value < 0.05.
Therapy was on an outpatient basis and consisted of leucovorin 60 mg orally every 8hours on days 1 through 3, interferonα-2a (Roferon-α, Roche, Mijdrecht, The Netherlands)
18x106 IU subcutaneously on days 1 through 3, and 5-FU 750 mg/m2 as an intravenous bolusinfusion on days 2 and 3. Acetaminophen 500 mg orally every 4 to 6 hours was given for
pyretic reactions on IFN. To diminish the severity of mucositis, the patients were instructed
to use ice chips by mouth starting 5 minutes before 5-FU administration and continuing for30 minutes after the end of the 5-FU infusion (11). An oral hygiene program was used
consisting of frequent teeth cleaning and mouth rinses with saline followed by chlorhexidinegluconate 0.12%. Induction cycles were repeated every 14 days for 4 courses and treatment
was repeated in responding patients to a maximum of 8 courses. Maintenance treatment
consisted of the same 3 day schedule every 6 weeks until progression for a maximum of 2years.
Evaluation of response was performed after every four courses during the inductiontreatment and after every course during the maintenance treatment. A complete response (CR)
required disappearance of all evidence of tumor for a minimum of four weeks, a partial
response (PR) was registered when a 50% or greater decrease in the sum of the products ofall perpendicular diameters of evaluable lesions was reached; patients with a response less
than partial or an increase of less than 25% were classified as stable disease (SD). Progression(PD) was defined as an increase of more than 25% or the development of new lesions.
Remission duration was measured from the end of the remission-induction treatment until the
date of documented progression. Survival was measured from the first day of therapy to dateof death.
Toxicity was assessed before every new course according to WHO guidelines (12).Treatment was withheld for 1 week when toxicity from a prior course had not recovered to
a WHO grade 1 or less, except for hand-foot syndrome and alopecia. In case of grade 2 or
higher major organ toxicity and grade 3 or higher myelotoxicity, 5-FU dose was reduced with25%. In case of a delay for more than 2 weeks or more than 50% dose reduction the patient
went off study. Because of its short intermittent use, no dose modification for the IFN wasforeseen. CEA serum levels were measured before every course.
128

Statistical analysis
Estimates of survival and remission duration were calculated using the method of Kaplan and
Maier (13). Differences between responding patients with or without maintenance therapy wascalculated using the generalized Wilcoxon test (14). A two sided alpha level of 0.05 was
considered statistically significant. The association between performance status and responsewas assessed with the Mantel test for trend (15).
Table 2. Characteristics of responding patients with or without maintenance treatment.
No maintenance treatment Maintenance treatment
Patients 11 18
CR 2 1
PR 9 17
Male/female 5/6 11/7
Age (years)
Median 50 54
Range 27-64 41-69
Performance status
0 5 9
1 6 8
2 0 1
Site of origin
Colon 5 9
Rectum 6 9
Time from diagnosis(months)
Primary 10 13
Metastasis 9 4
129

Results
PatientsFrom November 1990 to November 1993, a total of 53 patients were enroled in the induction
regimen. Patients characteristics are listed in table 1. Liver metastases were the predominant
metastatic site (74% of patients). All patients are included in the analysis of remissionduration and survival. The characteristics of responding patients receiving maintenance
treatment (group B) or not (group A) are shown in table 2. Both groups were comparable forage, sex, primary tumor, and performance status.
Response
Three out of the 53 patients were not evaluable for response. Two of them died from
unrelated causes after one treatment course. One patient developed tumor-associatedobstruction ileus two weeks after a first course and died after surgery. Three CR and 26 PR
were observed. The response rate in 50 assessable patients was 58% (CI, 43%-72%). Anadditional 16 patients had SD and 5 patients had PD. Responses occurred in the liver (N=24),
lung (N=6), and three responses were observed in extrahepatic, intra-abdominal lesions.
Response rate was correlated to performance status. Objective response rate (CR + PR) was88% in 16 patients with a WHO performance status of 0 and 48% in 29 patients with PS 1,
and 20% in 5 patients with PS of 2 (p= .002). The overall response rate was higher forpatients with rectum (75%) than for patients with colon primaries (47%) (p= .043). No
difference in response rate was observed between patients with or without prior radiotherapy,
male or female gender, and late (> 1 year) or early (< 1 year) onset of metastasis afterdiagnosis of primary tumor.
Pretreatment CEA levels were elevated in 36/50 assessable patients. Responses were observedin 22/36 patients with elevated CEA levels and in 6/14 patients with normal pretreatment CEA
levels (N.S.). Serial measurements of CEA levels revealed an initial rise of CEA levels after
the onset of chemotherapy in several patients, probably due to shedding of the epitopes intothe circulation. Biochemical response of serum CEA levels correlated with the clinical
response, with only 2/22 responding patients having sustained elevated CEA levels (p= .036).
130

Toxicity
Toxicity during the induction therapy was significant and occurred in all patients, with
mucositis, mild nausea and vomiting, diarrhea and leucopenia as the most frequently observedside effects (table 3). Mucositis occurred in 229/354 (65%) courses, nausea and vomiting
grade 1 and 2 in 142/354 (40%), diarrhea in 134/354 (39%) courses, and leucopenia in 93/534(26%). Hand-foot syndrome (HFS) occurred in 24 patients and alopecia grade 3 in 11 patients.
HFS and alopecia were observed only after two or more courses. Neurological toxicity,
primarily cerebellar toxicity, occurred in 5 patients. In 14 patients 25% dose reduction of 5-FU was necessary because of persistent toxicity (43 courses). Hospital admission was
necessary for grade 3-4 mucositis (2 patients) and diarrhea (1 patient). Toxicity tended toaccumulate during the induction treatment. After the end of the induction treatment toxicities
resolved after a 4- to 6-week rest period.
131

Table 3. Toxicity occurring in 354 courses during induction treatment
Toxicity WHO grade (%)
1 2 3 4
Mucositis 35 23 7 1
Diarrhea 18 18 1 1
Vomiting 32 8 0 0
Leucopenia 14 8 4 1
Thrombocytopenia 1 0 0 0
Anemia 8 2 1 0
Maintenance treatment
Eighteen responding patients received maintenance treatment for a total 80 courses (median4, range 1-10). Toxicity during maintenance courses was low and consisted of mild mucositis
and diarrhea, confined to a WHO grade 1-2 level in all patients. The overall survival of all53 patients is shown in figure 1. With a median observation period of 19.7 months, no
differences were yet observed in the survival times of both cohorts. Median survival time of
all patients was 16.6 months (CI, 10.3-22.8 months). Median remission duration of patientsreceiving maintenance therapy was 9.4 months (CI, 8.4-10.3 months) compared to 4.7 months
(CI, 3.2-6.2 months) of the previous 11 responding patients without maintenance therapy (p=.033, figure 2).
Legend to figure 1. Survival probability of all patients.
Legend to figure 2 . Probability of progression free survival of patients with (dashed line) or without
(solid line) maintenance treatment (P=.033).
132

Figure 1.
Figure 2 .
133

Discussion
We reported earlier our experience with an outpatient combination treatment of 5-FU, oral LVand IFN in patients with previously untreated metastatic colorectal cancer (10). LV was
administered orally because of the preferential uptake of the activel-isomer that may prevent
possible competition of the inactived-isomer in the serum (16). The dose of LV 60 mg, every
8 hours for 3 days was shown to result in serum concentrations of LV sufficiently highenough to modulate 5-FU cytotoxicityin vitro (10). Among the first 28 assessable patients
a response rate of 54% (95% CI, 34%-72%) was observed. Despite this high activity, the
remission duration after cessation of chemotherapy was however disappointing with a medianduration of 5 months (range 2-13+ months). We therefore started maintenance courses for
responding patients to attempt prolongation of remission duration.We report here our cumulative experience of a total of 53 patients. The high response
rate of this regimen holds true in a larger group of patients, with a response rate of 58% (95%
CI, 43%-72%) among 50 evaluable patients. Response was correlated to initial performancestatus. The response rate is achieved at the cost of significant toxicity, for which dose
modifications were necessary in 26% of patients. Remission duration after the end of theinduction treatment was prolonged in the cohort of patients who received maintenance
treatment, when compared with the cohort of responders among the first 28 patients who only
received the induction treatment. Remission duration was 4.7 and 9.4 months for both groups,respectively (p= .033). With a median observation duration of responding patients of 19.7
months no conclusions can be drawn on survival time in both subgroups. The median survivaltime of all 53 patients was 16.6 months. Toxicity during maintenance therapy was confined
to grade 1-2 mucositis and was acceptable in all patients.
In conclusion, a high response rate of 54% of this outpatient regimen in patients withadvanced colorectal carcinoma in a single center phase II setting holds true in a larger group
of patients. Maintenance treatment in responding patients may prolong remission durationwithout adding significant toxicity. To study the effects of treatment on survival, randomized
controlled trials are necessary comparing induction/maintenance treatment to the standard
options of treatment in this stage of colon cancer.
134

References
1. Silverman DT, Murray JL, Smart CR, Brown CC, Myers MH. Estimated median survival times ofpatients with colorectal cancer based on experience with 9,745 patients.Am J Surg1977; 133: 289-97.
2. Moertel CG. Chemotherapy of gastrointestinal cancer.N Engl J Med1978; 299: 1049-52.3. Davis HL. Chemotherapy for large bowel cancer.Cancer1982; 50: 2638-46.4. Moran RG. Leucovorin enhancement of the effects of the fluoropyrimidines on thymidilate synthase.
Cancer1989; 63: 1008-12.5. Arbuck SG. Overview of clinical trials using 5-fluorouracil and leucovorin in the treatment of advanced
colorectal cancer.Cancer1989; 63: 1036-44.6. Wadler S, Schwartz EL. Antineoplastic activity of the combination of interferon and cytotoxic agents
against experimental and human malignancies: a review.Cancer Res1990; 50: 3473-86.7. Grem JL, McAtee N, Murphy RF, Balis FM, Steinberg SM, Hamilton JM, et al. A pilot study of
interferon alfa-2a in combination with fluorouracil plus high-dose leucovorin in metastaticgastrointestinal carcinoma.J Clin Oncol1991; 9: 1811-20.
8. Houghton JA, Morton CL, Adkins DA, Rahman A. Locus of interaction among 5-fluorouracil,leucovorin, and interferon-α2a in colon carcinoma cells.Cancer Res1993; 53: 4243-50.
9. Sinnige HAM, Timmer-Bosscha H, Peters GF, De Vries EGE, Mulder NH. Combined modulation ofleucovorin andα-2a interferon of fluoropyrimidine mediated growth inhibition.Anticancer Res1993;13: 1335-40.
10. Sinnige HAM, Buter J, De Vries EGE, Uges DRA, Roenhorst HW, Verschueren RCJ, et al. Phase I-IIstudy of the addition ofα-2a interferon to 5-fluorouracil/leucovorin. Pharmacokinetic interaction ofα-2ainterferon and leucovorin.Eur J Cancer1993; 29A: 1715-20.
11. Mahood DJ, Dose AM, Loprinzi CL, Veeder MH, Athmann LM, Thernau JM, et al. Inhibition offluorouracil-induced stomatitis by oral cryotherapy.J Clin Oncol1991; 9: 449-52.
12. WHO Handbook for reporting results of cancer treatment. Den Haag: Martinus Nijhoff, 1979.13. Kaplan EL, Maier P. Nonparametric estimation from incomplete observations.J Am Stat Assoc1958;
53: 457-81.14. Breslow NE. Analysis of survival data under the proportional hazards model.Int Statist Rev1975; 43:
45.15. Mantel N. Chi-square tests with one degree of freedom: Extensions of the Mantel-Haenszel procedure.
J Am Stat Assoc1963; 58: 690-700.16. Straw JA, Szapary D, Wynn WT. Pharmacokinetics of the diastereoisomers of leucovorin after
intravenous and oral administration to normal subjects.Cancer Res1984; 44: 3114-9.
135


Chapter 9
Dose escalation of dacarbazine combined with interferon-alfa,G-CSF and ondansetron in patients with metastatic melano-
ma
J. Buter, D. Th. Sleijfer, P.H.B. Willemse, W.T.A. van der Graaf, E.G.E. de Vries,H. Schraffordt Koops1 and N.H.Mulder.
Departments of Internal Medicine and1Surgery, University Hospital, Groningen, 9713 EZ
The Netherlands.
Summary
To define the activity of an individually escalated dacarbazine (DTIC) dose combined withinterferon alfa-2a (IFN), granulocyte-colony stimulating-factor (G-CSF), and ondansetron, 20
patients with metastatic melanoma, were treated with DTIC, ondansetron 8 mg iv. G-CSF 300
µg sc. and IFN 9x106 IU sc. Treatment every 21 days to a maximum of 6 courses. DTIC dosewas escalated with 250 mg/m² in case of acceptable toxicity to 1250, 1500 and 1750 mg/m2
in 14/19, 8/11 and 0/5 patients, respectively. Dose escalation prohibiting toxicities werethrombopenia (10 pts.), leucopenia (9 pts.) and nausea/vomiting (2 pts.). Four partial remis-
sions were observed, for a response rate of 20% (95% confidence interval, 6 to 44 %).
Duration of responses were 1, 2, 3, and 3 months. Median overall survival was 7.8 months.
Introduction
Approximately 20% of the patients with malignant melanoma will develop distant metastasesthat are not amenable to surgical therapy. The prognosis in this situation is poor with a
median survival of only a few months. No medical treatment is available that has substantialinfluence on the prognosis of these patients. Chemotherapy is only marginally active with no
influence on survival. Dacarbazine (DTIC) is the most active chemotherapeutic drug with a
137

low but consistent response rate of 17% (13 to 21%, 95% confidence interval) and a completeresponse rate of approximately 5% in single-agent regimens (1-4). Interferon-alpha (IFN) has
shown therapeutic activity in patients with metastatic malignant melanoma. Response rates are
reported between 10 and 20% (5,6). When combined with DTIC, IFN has shown to improveresponse rates and survival in patients with metastatic melanoma in several phase II trials for
response rates of 25 to 35 % (7-13). This could be confirmed in comparative studies. Toxicity,particularly myelotoxicity, was more prominent with combination treatment in all studies
(14-16).
Besides the combination of agents, their individual dose intensity is an importantparameter for the outcome of systemic treatment of patients with disseminated solid tumors
(17). In melanoma patients this was also shown for the alkylating drug melfalan (18). Atstandard DTIC dose of 800 mg/m² bolus i.v. on day 1 every 3 to 4 weeks, acute
nausea/vomiting (N/V) and leucopenia are dose limiting toxicities. With the recent availability
of new drugs that are capable of reducing side effects of chemotherapy, dose intensificationof DTIC might become possible in an attempt to improve therapeutic activity. Chemotherapy
induced nausea and vomiting can efficiently be reduced with the new 5 HT3-antagonistic anti-emetics. Secondly, the growth factor G-CSF has been approved for reducing chemotherapy
induced neutropenia. In a phase II trial we studied the feasibility and efficacy of individual
DTIC dose intensification, combined with IFN under support of G-CSF and ondansetron inpatients with metastatic melanoma.
Materials and methods
Twenty patients were entered, all had histologically proven disseminated malignant melanoma
with measurable disease and met the following criteria: Age of 18 - 75 year, World HealthOrganization (WHO) performance status 2 or less, expected survival of at least 3 months,
serum creatinine level < 150 µmol/L; serum bilirubin level < 25 µmol/L, WBC > 3.0x109/L,platelet count > 100x109/L, and no prior treatment with dacarbazine or interferon. Patients
with brain metastases, other malignancies or uncontrollable disease were excluded. The study
protocol was approved by the Medical Ethical Committee and informed consent was obtainedfrom all patients before entry. Initial diagnostic workup consisted of a complete history and
physical examination, full blood counts and assessment of renal and hepatic function, chestx-ray radiograph with additional computed tomography or sonography of abdominal masses
and from the liver in case of disturbed liver functions (1.5 times normal). Brain computed
tomography was done in case of clinical suspicion of brain metastases.The maximal individual tolerated DTIC dose was given in combination with IFN and
supportive treatment with G-CSF and ondansetron. Patients received a starting dose of DTIC
138

Table 1. Patients’ characteristics
N %
Patients 20
Female/male 7 / 13
Age, years (mean, range) 47 (30-68)
WHO performance status
0 9 45
1 6 30
2 5 25
Prior therapy
Surgery 20 100
Regional perfusion 3 15
Radiotherapy 3 15
Chemotherapy 2 10
Tumor localizations*
Lung 10 50
Liver 8 40
Soft tissue and visceral 13 65
Bone 3 15
Lymph nodes 3 15
Other 2 10
Number of metastatic sites
1 11 55
2 6 30
3 or more 3 15
* May be more than one site IU s.c.
1000 mg/m² intravenously as a one hour infusion preceded by ondansetron 8 mg i.v. on day
1. Granulocyte colony-stimulating factor 300 µg was administered subcutaneously on day 3through 13. Courses were repeated every 21 days to a maximum of 6 courses. Interferon-alfa-
2a was administered at a daily dose of 3 x 106 IU s.c. daily on day 1 to 3, and 9 x 106
thereafter during the whole treatment period. In the first seven patients IFN was started in
139

Table 2. Dose escalation of DTIC and toxicity
Intended
DTIC dose
(mg/m²)
No. patients
intended
No. patients
realized
Dose escalation prohibiting toxicity
Thrombocyto-
penia
Leucopenia Nausea and
vomiting
1250 19 14 4 4
1500 11 8 2 1
1750 5 0 4 4 2
course 4, whereas the following patients received IFN from the first course of treatment.
DTIC dose was escalated with 250 mg/m² in a next course in case of bone marrow toxicity
less than WHO grade 3 and organ toxicity less than WHO grade 2. In those patients in whichIFN was started in course 4, no dose escalation of DTIC was performed in that course.
Acetaminophen (250-500 mg orally every 4-6 hours) was given to suppress pyretic reactions.Patients were examined for toxicity on days 1, 15 and 22 of each course. Toxicity was
assessed using the WHO guidelines (19). For nausea and vomiting a modified grading was
used because of the prophylactic use of antiemetic medication. Grade 0 stated no complaints;grade 1, nausea only; grade 2, nausea and vomiting 1-2 times; grade 3, nausea and vomiting
3 times or more, requiring additive medication; grade 4, intractable vomiting requiringintravenous fluids.
DTIC dose was reduced to 75% of the previous dose in case of bone marrow toxicity
grade 4 in the preceding course or leucocytes of < 2.5 x109/L or thrombocytes < 100 x 109/Lon the day of DTIC infusion. When on the day of infusion, leucocytes were < 1.5 x109/L or
thrombocytes < 75 x109/L, the course was delayed for one week to a maximum of 3 weeks.Interferon dose was withheld for one day per week in case of intolerance.
Tumor measurements and radiological examinations were repeated after 3 courses and
at the end of treatment. After 3 courses, treatment was continued unless progressive diseasewas apparent. Complete response (CR) was defined as the disappearance of all signs of
disease for at least 4 weeks. A partial response (PR) was defined as a decrease by at least50% in the sum of the products of the largest perpendicular diameters of all measurable
lesions. Stable disease (SD) was defined as a situation with less than 50% decrease or less
than 25% increase and progressive disease (PD) as more than 25% increase in the sum of theaforementioned diameters.
Leucocyte numbers on days 1, 15 and 22 of course 1 to 3 in which the first 7 patients
140

did not receive IFN were compared with those of the following 7 patients who started with
Table 3. Percentage of courses with toxicity occurring in 66 assessable courses
Toxicity WHO grade
1 2 3 4
Nausea/vomiting 36 20 5
Diarrhoea 12 2
Fatigue 30 15 2
Leucopenia 32 11 12 2
Thrombocytopenia 6 10 12 8
Anemia 15 11 5 2
Neurotoxicity 23 12 2
IFN from the start of treatment to study the influence of IFN on G-CSF stimulation ofleucocytes.
StatisticsDifferences in leucocyte numbers were tested using the Mann-Whitney-U test.
Results
PatientsThe clinical characteristics of the patients entered in this protocol are summarized in table 1.
The 20 patients were treated with 1 to 6 courses (median 3) for a total of 65 courses. All
patients completed at least one course and all patients were evaluable for toxicity.
Toxicity and dose escalation of DTICDTIC dose could be escalated to 1250, 1500 and 1750 mg/m2 in 14 of 19, 8 of 11 and 0 of
5 patients, respectively (Table 2.). Dose escalation prohibiting toxicities were thrombopenia
(10 patients), leucopenia (9 patients), and nausea and vomiting (2 patients). In 8 other patientsno dose escalation was attempted because of tumor progression. Toxicities occurring during
a total of 65 courses are listed in table 3. Grade 3/4 thrombopenia and leucopenia occurredin 20% and 14% of the courses, respectively. Five patients received red blood cell transfusions
141

and 4 patients received prophylactic platelet transfusions in the course of their treatment.Nausea and vomiting grade 2 and 3 occurred in 22% and 6% of
Table 4. Leucocyte numbers with or without IFN, course 1-3
Leucocytes (x 109/L)
without IFN with IFN
Day Mean SD Mean SD
1000 mg/m2 DTIC
1 7.8 1.8 5.9 2.1
15 13.2 4.9 5.2 4.3
22 7.9 4.6 4.1 0.9
1250 mg/m2 DTIC
1 7.4 2.8 5.4 4.0
15 10.1 4.4 11.4 11.2
22 8.1 2.7 6.5 7.0*
1500 mg/m2 DTIC
1 8.2 1.4 3.5 0.3*
15 3.6 0.1 4.9 3.6
22 6.5 1.4 3.3 0.4
* P <.05, compared to no IFN, Mann-Whitney U test
the courses despite the prophylactic use of ondansetron. Diarrhoea was limited to grade 1-2
occurring in 14% of the courses. One patient became hypotensive during DTIC infusion withtemporary tachycardia. Subsequent ECG analysis showed a sinus rhythm with no signs of
ischemia and treatment could be continued under clinical observation. Flu-like symptoms and
fatigue occurred in 16 of the patients during IFN treatment. These symptoms were controllablewith acetaminophen in most patients. Neurotoxicity was recorded in 7 patients. Four patients
had mild headache and intermittent somnolence. Three other patients had severe headache,severe fatigue with mental depression, and confusion, in one patient each. IFN was withheld
temporary for toxicities in 4 patients, while treatment was discontinued in 2 patients.
To study possible interference of IFN with the stimulation effect of G-CSF onleucocyte numbers, the first 3 courses in the first 7 patients receiving no IFN were compared
with the first 3 courses of the following 7 patients who did receive IFN. Leucocyte numbersare listed in table 4. Leucocyte numbers in courses with IFN were lower on day 22 after
DTIC 1250 mg/m2 and on day 1 of DTIC 1500 mg/m2 (P < .05).
142

ResponseTwenty patients were evaluable for response. Four partial responses were observed. Five
patients had stable disease and 11 patients showed progression. Objective response rate was20%, ( 95% confidence interval, 6 to 44 %). Response durations were 1, 2, 3, and 3 months.
Responses occurred in the lung, lymph nodes, and skin metastases. Three out of the four
responders were women. Median survival of all patients was 7.8 months. Average relativedose intensity of DTIC (17) of all patients was 360 mg/m2/week. No differences in relative
DTIC dose intensity between responders and non-responders was observed.
Discussion
The treatment of metastatic melanoma is still unsatisfactory. DTIC, with response rates of
approximately 17%, is one of the most active drugs in this disease available (20).The working mechanism of DTIC is partly understood. DTIC has no cytotoxic activity by
itself; it has to be metabolized in liver cells to its active metabolites that probably mediatecytotoxic activity both as antimetabolites and as alkylating agents. O6-methyl-deoxyguanosine
formation in DNA is thought to be a critical cytotoxic event of DTIC activity (21,22).
Combination with IFN has been shown to improve response rates and survival of DTIC withreported response rates up to 35 % in several phase II (7-13) and comparative studies (14-16).
In most studies, DTIC has been administered at a dose of 800 to 1250 mg/m2 given as asingle infusion or fractionated over 2 to 5 days every 3 to 4 weeks. Acute nausea/vomiting
and myelotoxicity, especially leucopenia, are dose limiting in this setting. We studied the
possibility of escalating DTIC dose with support of two new drugs that are capable ofreducing chemotherapy induced side effects.
In this study, the growth factor G-CSF and the antiemetic ondansetron permittedindividual dose escalation of DTIC up to 1500 mg/m2 in a 3 week cycle regimen. However,
a dose of 1500 mg/m2 was only realized in 8 out of the total 20 patients, with thrombopenia
or leucopenia prohibiting dose escalation in 10 out of the remaining 11 patients. A startingdose of 1250 mg/m2 seems to be feasible for further study in this setting. Acute nausea and
vomiting was effectively controlled by ondansetron, given at a single i.v. bolus-injection of8 mg before the start of infusion. Although nausea/vomiting was not completely prevented,
grade 3 nausea and vomiting occurred in only 6% of the courses ( 4 patients) while no grade
4 nausea/vomiting was not observed. In the current study, IFN administered s.c. at a dailydose of 9 MU, was tolerated somewhat less well when compared with a previous standard
143

DTIC dose combination regimen with IFN (10), requiring dose modifications in 29% of thepatients. It is possible that in addition to the escalated DTIC dose this is caused by the
combination of biological agents.
Because biological response modifiers have shown to influence the stimulation effectof G-CSF on the maturation of neutrophils in vitro (23,24) and IFN has been shown to
suppress neutrophil colony formation in vitro (25,26), the patients leucocyte numbers werestudied during courses with and without concurrent IFN treatment. We observed some
marginal interference of IFN with the stimulation effect of G-CSF on leucocyte numbers
(table 4.). Leucocyte numbers on day 22 of 1250 mg/m2 and on day 1 of 1500 mg/m2 DTICdose level were lower in the IFN containing courses (P < .05). However, these difference
were not clinically important. The response rate of 20% ( 6% to 44 %, 95% confidence
interval) of the current study does not appear to be superior to the activity of other DTIC/IFNcombinations with standard DTIC doses (7-13). As to the sites of response, all four responses
occurred in the lung, soft tissue or lymph nodes, while no responses were observed in thebone, liver or visceral abdominal metastases. This reflects the normal pattern in this disease.
In conclusion: The use of G-CSF and ondansetron permits individual dose escalation
of DTIC up to 1500 mg/m2 every 3 weeks in patients with metastatic melanoma withthrombopenia and leucopenia as the main dose limiting factors. A clinical unimportant
interference of IFN with the stimulation of leucocytes by G-CSF was found. With the use ofG-CSF and ondansetron, a dose of 1250 mg/m2 every 3 weeks is recommended as a starting
dose for DTIC, when combined with IFN. Escalation of DTIC dose did not seem to improve
the response rate or survival of patients with metastatic melanoma in this study.
References
1. Nathanson L, Wolter J, Horton J et al . Characteristics of prognosis and response to an imidazolecarboxamide in malignant melanoma. Clin. Pharm. Ther. 1971; 12: 955-962.
2. Constanza ME, Nathanson L, Lenhard R et al. Therapy of malignant melanoma with an imidazolecarboxamide and bis-chloroethyl nitrosurea. Cancer 1972; 30: 1457-1461.
3. Constanza ME, Nathanson L, Lenhard R et al. Results with methyl-CCNU and DTIC in metastaticmelanoma. Cancer 1977; 40: 1010-1015.
4. Balch, CM., Houghton, AN and Peters, LJ. Cutaneous melanoma. In: Cancer, principles and practiceof oncology, edited by DeVita, V. T. , Hellman, S. and Rosenberg, S. A. Philadelphia: Lippincott,J. P., 1993, p. 1612-1661.
5. Creagan ET, Ahmann DL, Frytak SF, Long HL, Chang MN, Chang N and Itri LM. Phase II trials ofrecombinant leukocyte A interferon in disseminated malignant melanoma: Results in 96 patients. CancerTreat. Rep. 1986; 70: 619-624.
6. Thomson, D. B. and McLeod, G. R. C. Pilot efficacy study of recombinant leucocyte A interferon(rIFN-A) in patients with metastatic melanoma. In: Proceedings, satellite symposium to 3rd Europeanconference on clinical oncology and cancer nursing, Professional postgraduate Services, Macclesfield:Brookes,J. J. , 1985,
7. Avril MF, Beerblock K, Dreno B, Delaunay M, Bonerandi JJ, Guillaume JC, Souteyrand P, Kalis B,Chevrant-Breton J, Verret J et al. Treatment of metastatic melanoma with dacarbazine recombinant
144

interferon alfa 2A combination: results of multicentric study. Bull. Cancer (Paris) 1990; 77: 1183-1191.8. Bajetta E, Negretti E, Giannotti B, Brogelli L, Brunetti I, Sertoli MR, Bernengo MG, Sofra MC,
Maifredi G, Zumiani G et al. Phase II study of interferon alpha-2a and dacarbazine in advancedmelanoma. Am. J. Clin. Oncol. 1990; 13: 405-409.
9. McLeod GR, Thomson DB and Hersey P. Clinical evaluation of interferons in malignant melanoma. J.Invest. Dermatol. 1990; 95: 185S-187S.
10. Mulder NH, Willemse PHB, Schraffordt Koops H, De Vries EGE and Sleijfer DT. Dacarbazine (DTIC)and human recombinant interferon alpha 2a (Roferon) in the treatment of disseminated malignantmelanoma. Br. J. Cancer 1990; 62: 1006-1007.
11. Hersey P, McLeod GR and Thomson DB. Treatment of advanced malignant melanoma with recombinantinterferon alfa-2a in combination with DTIC: long-term follow-up of two phase II studies. Br. J.Haematol. 1991; 79 Suppl 1: 60-66.
12. Creagan ET, Schaid DJ, Ahmann DL and Frytak S. Disseminated malignant melanoma and recombinantinterferon: analysis of seven consecutive phase II investigations. J. Invest. Dermatol. 1990; 95:188S-192S.
13. Biological Response modifiers in melanoma (BREMIM) Italian Cooperative Group. Phase II study ofinterferon alfa-2a and dacarbazine in advanced melanoma. Eur. J. Cancer 1992; 28A: 1719-1720.
14. Falkson CI, Falkson G and Falkson HC. Improved results with the addition of interferon alfa-2b todacarbazine in the treatment of patients with metastatic malignant melanoma. J. Clin. Oncol. 1991; 9:1403-1408.
15. Sertoli MR, Queirolo P, Bajetta E, Negretti E, Calabresi F, Barduagni L, Giannotti B, Brogelli L,Bernengo MG, Sofra MC, Maifredi G, Zumiani G, Comella G, Bruzzoni R, DiLeo A, et al. Dacarbazine(DTIC) with or without recombinant interferon alpha-2a at different dosages in the treatment of stageIV melanoma patients. Prilimary results of a randomized trial. Proc. Am. Soc. Clin. Oncol. 1992; 11:1185. (Abstract)
16. Kirkwood JM, Ernstoff MS, Giuliano A, Gams R, Robinson WA, Costanzi J, Pouillart P, Speyer J,Grimm M and Spiegel R. Interferon alpha-2a and dacarbazine in melanoma. J. Natl. Cancer Inst. 1990;82: 1062-1063.
17. Hryniuk WM. Average relative dose intensity and the impact on design of clinical trials. Semin. Oncol.1987; 14: 65-74.
18. Cornbleet MA, McElwain TJ, Kumar PJ et al. Treatment of advanced malignant melanoma with highdose melphalan and ABMT. Br. J. Cancer 1983; 48: 329-334.
19. WHO Handbook for reporting results of cancer treatment, Den Haag:Martinus Nijhoff, 1979. Ed. 48th20. Hill GJ, Kremetz ET and Hill HZ. Dimethyltriazeno imidazole carboxamide and combination
chemotherapy for melanoma IV. Late results after complete responses to chemotherapy (CentralOncology Group Protocols 7130, 7131, and 7131A). Cancer 1984; 53: 1299-1305.
21. Lee SM, O’Conner P, Thatcher N, Crowther D, Margison GP and Cooper D. Formation and loss ofO6-methyldeoxyguanosine (O6-Med-G) in peripheral leucocytes of patients receiving dacarbazine (DTIC)or CB10-277. Proc. Am. Assoc. Cancer Res. 1993; 34: 2115. (Abstract)
22. Lee SM, Thatcher N, Dougal M and Margison GP. Dosage and cycle effects of dacarbazine (DTIC) andfotomustine on O6-alkylguanine-DNA alkyltransferase in human peripheral blood mononuclear cells. Br.J. Cancer 1993; 67: 216-221.
23. Katayama K, Koizumi S, Ueno Y, Ohno I, Ichihara T, Horita S, Miyawaki T and Taniguchi N.Antagonistic effects of interleukin 6 and G-CSF in the later stage of human granulopoiesis on vitro. Exp.Haematol. 1990; 18: 390-394.
24. Shirafuji N, Matsuda S, Tani K, Ozawa K, Nagata S, Asano S and Takaku F. Granulocytecolony-stimulating factor stimulates human mature neutrophilic granulocytes to produce interferon-α.Blood 1990; 75: 17-19.
25. Greenberg PL and Mosny SA. Cytotoxic effects of interferon in vitro on granulocytic progenitor cells.Cancer Res. 1977; 37: 1794.
26. Estrov Z, Lau AS, Williams BRG and Freedman MH. Recombinant interferon alpha-2a and juvenilchronic myelogenous leukemia: Cell receptor binding, enzymatic induction, and growth suppression invitro. Exp. Haematol. 1987; 15: 127.
145

Summary and conclusions
The natural process of cell growth, differentiation and apoptotic death is regulated by a varietyof peptide cell regulators. Produced by different cells, these cytokines work in a autocrine and
paracrine way in the process of physiological growth, inflammatory states and malignancy.
Recombinant DNA technology has made several cytokines available for clinical use. Inmedical oncology the recombinant cytokines have gained interest for their capability to
mediate the regression of cancer and to reduce the myelosuppressive side effects ofchemotherapy.
The present thesis deals with the clinical aspects of the use of cytokines as biological
response modifiers in the treatment of cancer. Inchapter 1 a review is given of the literatureon the role of two recombinant human cytokines, interleukin-2 and interferon-alfa in the
treatment of patients with disseminated solid tumors. IL-2 plays a central role in the inductionof the immune response and this cytokine is able to induce tumor responses in approximately
20% of patients with renal cell cancer or metastatic melanoma. Therapy with IL-2 is however
associated with substantial toxicity which is dependent on dose, schedule and route ofadministration. High dose intravenous application of this drug requires patient selection and
intensive monitoring, while subcutaneous administration can be conducted as outpatienttreatment. No apparent dose-response relationship is observed for IL-2, although different
mechanism may be responsible for the in vivo observed antitumor activity at various doses.
The addition of adoptively transferred activated cells has not consistently shown to improvethe activity of IL-2 mediated immunotherapy.
Unlike IL-2, Interferon-α has a direct growth inhibiting and modulating effect on tumorcells. IFN is active in several hematological diseases. Its role in the treatment of solid tumors
is limited to Kaposi’s sarcoma, renal cell carcinoma and melanoma although the synergistic
effects with the cytostatic 5-fluorouracil are encouraging. The reversibility of the side effectsof IFN, in contrast to those of many cytotoxic agents, makes it a worthwhile drug. A dose of
5 to 10 MU subcutaneously or intramuscular, at least three times a week has been found tobe optimal.
Chapters 2 and 3describe the efficacy and toxicity of sc administration of IL-2 in
patients with RCC. Renal cell cancer is a tumor of tubular origin that is resistant to standardtreatment modalities at the stage of metastatic disease. IL-2 has shown to be active in this
disease and it is an accepted drug for the treatment of metastatic RCC in Europe and theUSA. We found the subcutaneous route of administration to be associated with less severe
toxicity than the standard intravenous administration, while antitumor activity was maintained
in patients with RCC. Among 46 assessable patients with RCC we observed nine responses,for a response rate of 20% (9% to 34%, 95% confidence interval). Two patients had complete
responses that lasted 29 and 35+ months. Toxicity of sc administered IL-2 consisted of local
147

inflammation and induration at the injection sites, fever, chills, nausea/vomiting, diarrhoea andmild hypotension. Subcutaneous IL-2 is active in patients with renal cell cancer and the
toxicity profile enables treatment of patients with compromised organ function due to
concomitant disease.
With the improvement of the tolerability of IL-2, the resistance to this form oftreatment in the majority of patients emerges as even more of a challenge. The mode of action
of IL-2 mediated antitumor responses in vivo are not understood. IL-2 is thought to act
indirectly by stimulating and activating the cellular host defence mechanisms. Resistance toIL-2 treatment could therefor be the result of tumor dependent factors or alternatively be the
result of factors related to the effector-cells. Several investigators have indicated an importantrole of cytotoxic T-lymphocytes in IL-2 mediated antitumor activity.Chapter 4 studies the
addition of a monoclonal antibody (mAb) OKT3, targeting the CD3-part of the T-cell antigen-
receptor, to the sc IL-2 treatment in an attempt to improve T-cell activation. Whileimmunosuppressive at high doses, this mAb is a potent mitogen at low doses. In a phase I
dose escalating setting we found a maximal tolerable dose of 400 µg OKT3 with neurotoxicityas dose-limiting factor. No increase of activated lymphocyte populations was observed in the
range of 50 to 400 µg when compared with IL-2 monotherapy although the antibody was
detectable on lymphocytesin vivo.The observation of mixed responses, made in our patients on several occasions,
suggests clonal differences in metastases as a cause for IL-2 unresponsiveness. Due to
heterogeneity of the tumor, some cells seem to escape recognition by the immune system. Inchapter 5 we studied the use of a bispecific monoclonal antibody to improve cell-cell
interaction between activated effector-cells and tumor-cells in patients with renal cellcarcinoma. In a phase I trial the bispecific monoclonal antibody BIS-1, targeting both CD3
and a 40 kD carcinoma-associated glycoprotein EGP-2, was combined with sc interleukin-2
treatment. This BsMab was toxic producing chills, peripheral vasoconstriction and dyspnea,with maximum tolerated dose of 5 µg/kg when given as a slow infusion. We showed that the
BsMab binds to CD3 positive cells, with the development of BsMab-redirected tumor
cytotoxicity in anex vivoassay. T-cells and monocytes disappeared from the peripheral bloodafter infusion of the BsMab and elevated serum levels of TNF-α and IFN-γ were detected.
In chapter 6 two case histories are described on the outpatient therapy with sc IL-2in patients with advanced renal cell carcinoma who were on hemodialysis. It was shown that
sc IL-2 induced immunological changes, similar to those observed after iv IL-2 therapy
indicating in vivo induction of peripheral blood lymfokine activated killer cell (LAK) activity.We conclude that this treatment has a mild toxicity and can be given to patients with major
organ dysfunction who are on hemodialysis.Correspondence concerning two aspects of IL-2 related side effects are described in
chapter 7. Combination of drugs can be useful to improve activity, but it also makes it
148

difficult to ascribe observed toxicities to one specific drug. The single-agent treatment withIL-2 could give additional information on this issue. While a high frequency of bacterial
infection was observed with iv IL-2, and also in one study with combination of sc IL-2 and
IFN treatment, the frequency of clinical significant infections during single-agent sc IL-2treatment was low and did not indicate the requirement of prophylactic antibiotics in this
setting. Neurotoxicity of IL-2 is dose and schedule related. In our experience with sc IL-2neurotoxicity was rare and in most cases neurotoxicity was related to metastases in central
nervous system localizations.
Chapters 8 and 9describe two studies with recombinant IFN alfa-2a in combinationwith chemotherapy. Inchapter 8, interferon is added to a combination of oral leucovorin and
5-FU to improve antitumor activity against colorectal cancer. This threefold combination wasshown previously to be active with responses in 53% of 28 patients with colorectal cancer,
but remission duration was disappointing with a median remission duration of 4.7 months. A
clinical update of the regimen and the role of maintenance therapy in this setting is given inthis chapter. In 50 assessable patients a response rate of 58% (43% to 72%, 95% confidence
interval) was observed. The remission duration was improved in the patient cohort receivingmaintenance therapy every 6 weeks compared to the cohort who received only the induction
treatment, with median remission durations of 4.7 and 9.4 months, respectively. Overall
survival of all patients was 17.2 months.For patients with metastatic melanoma no treatment is available that has a substantial
influence on their prognosis. Dacarbazine (DTIC) is one of few chemotherapeutic drugs thatis marginally active. As a single-agent DTIC induces responses in 17% of patients. When
combined with IFN, response rates up to 35% can be reached. Acute vomiting and
myelosuppression, however are dose limiting toxicities of this drug at a standard dose of 800mg/m2 every 3 weeks. For several solid tumors, including melanomas, it has been shown that
dose-intensity is an important factor for the efficacy of chemotherapy. With the availabilityof two new drugs that are capable of reducing chemotherapy induced side effects it might be
possible to intensify the dose to improve therapeutic activity.Chapter 9 describes a study
with dose escalation of dacarbazine in combination with interferon alfa-2a under support ofthe recombinant human hematopoietic growth factor G-CSF and the 5HT3-antagonistic
antiemetic ondansetron in patients with metastatic melanoma. Individual DTIC-dose could beescalated up to 1500 mg/m2 with thrombocytopenia and leucopenia as dose limiting factors.
There was a marginal interference of IFN with the stimulation effect of G-CSF on leucocytes.
Nausea and vomiting was controllable with the use of ondansetron in most patients. Amongtwenty assessable patient, four partial responses were observed. Dose escalation of DTIC did
not appear to improve therapeutic activity.
149

Conclusions and perspectives
The use of recombinant cytokines as biological response modifiers in clinical medicine is
established although the action mechanisms are only poorly understood. In clinical oncologyimmunotherapy has only a small role in selective tumors for which no alternative treatments
are available. Despite the lack of clinical breakthroughs, the recombinant cytokines remain animportant new modality in the treatment of cancer. Biological therapy is based on the
capability of the immune system to recognize ’self’ from ’non-self’ by determinants on the
cell membrane. Also the cytotoxic effects of immune effector cells take place at the level ofthe cell membrane, in contrast to most cytotoxic drugs that are targeting nuclear DNA. As it
is not dependent on cell division or the penetration of drugs to the DNA, immunotherapymight be capable of eliminating those cells that escape chemotherapy because they are not
dividing at the time of therapy. When used in combination, chemotherapy might alter epitopes
on the cell membrane of tumor cells and thus make these cells more recognizable for theimmune system. Recent studies with combinations of platinum containing chemotherapy and
immunotherapy in patients with melanoma have been encouraging. Furthermore, it isspeculated that in minimal residual disease at least for some patients the tumor is controlled
by an interaction between tumor and the immune system. The reversibility of most side effects
of immunotherapy, unlike those of chemotherapy, makes it a worthwhile alternative in thetreatment in some forms of cancer. Since many aspects of immunotherapy remain
investigational, this form of treatment should be conducted in the setting of clinical trialprotocols.
150

Samenvatting en conclusies
Het natuurlijke proces van celgroei, differentiatie en geprogrammeerde celdood wordt bestuurddoor een groot aantal cel-regulerende eiwitten. Deze zogenaamde cytokinen worden
geproduceerd door verschillende cel-typen. Door hun autocriene en paracriene werking spelen
zij een belangrijke rol in het proces van fysiologische groei, ontsteking en maligniteit. Metbehulp van recombinant DNA technieken zijn verschillende cytokinen beschikbaar gekomen
voor klinisch onderzoek. In de medische oncologie zijn de cytokinen onderzocht vanwege hunantitumor activiteit en vanwege de capaciteit om de beenmergremmende bijwerkingen van
chemotherapie te verminderen.
In dit proefschrift worden de klinische aspecten van het gebruik van cytokinen alsbiologische response modifiers bij de systeem behandeling van kanker beschreven. In
hoofdstuk 1 wordt een overzicht gegeven van de literatuur over de rol van twee recombinantcytokinen, interleukine-2 en interferon-alfa bij de behandeling van gemetastaseerde solide
tumoren. Interleukine-2 speelt een centrale rol bij het ontstaan van een immuun respons. Dit
cytokine is in staat gebleken om tumor remissies te induceren bij ongeveer 15 tot 20% vande patiënten met een niercelcarcinoom of melanoom. De behandeling met IL-2 gaat echter
gepaard met aanzienlijke bijwerkingen die zowel afhankelijk zijn van de dosis, het therapie-schema, als de toedieningswijze. Behandeling met intraveneuze toediening van hoge doses IL-
2 vereist een strenge selectie van patiënten wat betreft hun hart- en longfunctie en intensieve
zorg tijdens de behandeling. Er is geen duidelijke dosis-respons relatie gevonden voor IL-2,hoewel mogelijk verschillende werkingsmechanismenen verantwoordelijk zijn voor het
klinische antitumor effect bij verschillende doseringen. De adoptieve toediening van in vitrogeactiveerde cellen heeft geen consistente verbetering van de IL-2 gemedieerde
immuuntherapie opgeleverd.
Interferon-alfa heeft, in tegenstelling tot IL-2, naast de stimulerende werking op hetimmuunsysteem ook een direct groeiremmend en modulerend effect op tumorcellen. Interferon
is actief gebleken bij verschillende hematologische ziekten. De rol bij de behandeling vansolide tumoren beperkt zich tot het Kaposi’s sarcoma, het niercelcarcinoom en het melanoom,
hoewel de synergistische effecten met 5-FU veelbelovend zijn. De reversibiliteit van de
bijwerkingen, in tegenstelling tot de bijwerkingen van veel cytostatica, maken IFN tot eenaantrekkelijk alternatief. Een dosering van 5 tot 10 miljoen eenheden subcutaan of
intramusculair is optimaal gebleken.De hoofdstukken 2 en 3 beschrijven de effectiviteit en bijwerkingen van subcutaan
toegediend IL-2 bij patiënten met een gemetastaseerd niercelcarcinoom. Het niercelcarcinoom,
dat ontstaan uit de cellen van de niertubulus, is resistent gebleken voor de standaardbehandelingsmogelijkheden zoals chemotherapie en radiotherapie in het stadium van
uitgezaaide ziekte. De systeembehandeling met IL-2 is werkzaam gebleken in deze situatieen in Europa en Amerika is het een geaccepteerd medicijn bij de behandeling van het
151

gemetastaseerde niercelcarcinoom. Bij 46 patiënten met valueerbare metastasen van eenniercelcarcinoom vonden bij 20% (95% betrouwbaarheid interval, 9% tot 34%) van de
patiënten een remissie. Twee patiënten hadden een complete remissie welke 29 and 35+
maanden duurden. De toxiciteit van sc IL-2 bestond uit locale ontsteking en zwelling op deinjectieplaatsen, koorts, rillingen, misselijkheid, overgeven, diarree en milde
bloeddrukverlaging. Wij concluderen dat sc IL-2 actief is bij patiënten met eenniercelcarcinoom en dat de relatief milde bijwerkingen behandeling van patiënten met een
verminderde orgaanfunctie mogelijk maakt.
Nu door de thuisbehandeling met subcutaan IL-2 de toepasbaarheid van dezebehandeling sterk is verbeterd, vormt het falen van de behandeling bij het merendeel van de
patiënten de belangrijkste klinische uitdaging. Het mechanisme van door IL-2 geïnduceerdeklinische antitumor effecten is nog onduidelijk. Interleukine-2 wordt verondersteld indirect te
werken door stimulatie en activatie van de cellulaire immunologische afweer. Resistentie voor
IL-2 behandeling kan theoretisch veroorzaakt worden door factoren van de tumorcel of doorfactoren van de effector cellen. Verschillende onderzoekers veronderstellen een belangrijke
rol voor de cytotoxische T-cel als effectorcel bij de door IL-2 gemedieerde antitumoractiviteit. Hoofdstuk 4 beschrijft de resultaten van de toevoeging van een monoclonaal
antilichaam OKT3, dat gericht is tegen het CD3 gedeelte van de T cel antigeen receptor, aan
de IL-2 behandeling in een poging de T-cel activatie te verbeteren. Hoewel het OKT3immuunsuppressief werkt bij hoge doseringen (mg), is het bij lage doseringen (µg) een
krachtig T-cel mitogeen gebleken. In een fase I dosis escalatie studie bij patiënten met eenniercelcarcinoom vonden we een maximaal tolerabele dosis van 400 µg, met neurotoxiciteit
als dosislimiterende factor. Hoewel het antilichaam aantoonbaar was op circulerende
lymphocyten, konden wij geen verhoging van geactiveerde lymphocyten populaties vinden bijdoseringen variërend van 50 tot 400 µg OKT3, in vergelijking met behandeling met IL-2
alleen.De observatie van zogenaamde ’mixed responses’, waarbij één haard kleiner wordt en
tegelijkertijd een andere haard groeit, die we bij onze patiënten een aantal malen hebben
gedaan, suggereert clonale verschillen in de metastasen. Door heterogeniciteit van de tumorworden sommige tumorcellen niet door het immuunsysteem herkend.Hoofdstuk 5 bestudeert
het gebruik van bispecifieke antilichamen om de interactie tussen tumorcel en effectorcel teverbeteren bij patiënten met een niercelcarcinoom. In een fase I studie werden 14 patiënten
met een niercelcarcinoom behandeld met Interleukine-2 en een bispecifiek monoclonaal
antilichaam BIS-1 dat gericht is tegen zowel het CD3 op T cellen als tegen een membraangebonden 40 kD tumor geassocieerd glycoproteine EGP-2. Dit bispecifieke antilichaam
veroorzaakte bijwerkingen met verschijnselen van rillingen, perifere vasoconstrictie endyspneu, met een maximaal tolerabele dosis van 5 µg/kg. We konden aantonen dat het
bispecifieke antilichaam bond aan CD3 positieve cellen, en dat deze cellen in het laboratorium
beter in staat bleken om EGP-2 positieve tumorcellen te lyseren. Tijdens de infusie van het
152

antilichaam verdwenen lymphocyten en monocyten tijdelijk uit het perifere bloed, en warenverhoogde spiegels van TNF-α en IFN-γ aantoonbaar. Bij een patient werd een gedeeltelijk
terugdringen van longhaarden gezien.
In hoofdstuk 6 zijn de casus beschreven van thuisbehandeling met sc IL-2 bij tweehemodialyse patiënten die progressieve metastasen van een niercelcarcinoom hadden. We
konden aantonen dat sc IL-2 immunologische veranderingen induceert die vergelijkbaar zijnmet de veranderingen die optreden tijdens intraveneuze IL-2 behandeling, en die wijzen op
de in vivo inductie van lymfokine activated killer cell (LAK) activiteit.
Correspondentie aangaande twee aspecten van bijwerkingen van IL-2 zijn beschrevenin hoofdstuk 7. Combinatie van verschillende medicijnen kan nuttig zijn om de effectiviteit
van therapie te verbeteren, maar het bemoeilijkt tegelijkertijd het toeschrijven vanbijwerkingen aan een van de gebruikte middelen. De mono-therapie met sc IL-2 kon hierover
aanvullende informatie verschaffen. In tegenstelling tot de intraveneuze behandeling en een
studie met een combinatie van subcutaan IL-2 en IFN, die gepaard gingen met een hogefrequentie van bacteriële infecties, was de frequentie van klinisch significante infecties tijdens
subcutaan IL-2 monotherapie laag en was er geen noodzaak om profylactisch antibiotica tegebruiken.
Neuropsychiatrische bijwerkingen die op kunnen treden bij therapie met IL-2 zijn
dosis- en therapievorm afhankelijk. In onze ervaring was neurotoxiciteit zeldzaam en in velegevallen gerelateerd aan metastasen gelokaliseerd in het zenuwstelsel.
De hoofdstukken 8 en 9 beschrijven twee studies met recombinant interferon-alfa incombinatie met chemotherapie.Hoofdstuk 8 beschrijft de resultaten van de toevoeging van
IFN aan een combinatie van leucovorin en 5-FU in een poging de therapeutische effectiviteit
van cytostatica bij patiënten met een gemetastaseerde tumor van de dikke darm te verhogen.Deze drievoudige combinatie bleek eerder actief te zijn bij de behandeling van 28 patiënten
met een tumor van de dikke darm waarbij 53% van de patiënten een remissie had. De duurvan de remissies was echter teleurstellend met een mediane duur van 4.7 maanden. Een
klinische vervolg van deze studie en de rol van onderhoudstherapie in deze setting worden
beschreven in dit hoofdstuk. In 50 patiënten met evalueerbare afwijkingen had 58% (43% tot72%, 95% betrouwbaarheidsinterval) van de patiënten een klinische remissie. De remissieduur
van het cohort patiënten dat onderhoudsbehandeling kreeg was verbeterd ten opzichte van hetcohort dat alleen de inductiebehandeling had gehad, met een mediane remissie duur van
respectievelijk 4.7 en 9.4 maanden. De mediane overleving van alle patiënten in deze studie
was 17.2 maanden.Voor patiënten met een gemetastaseerd melanoom is er geen behandeling beschikbaar
die een substantieel effect heeft op de prognose. Dacarbazine (DTIC) is een van de weinigecytostatica die enige activiteit vertoont. Als enkelvoudige therapie induceert DTIC remissies
bij 17% van de patiënten. In combinatie met IFN worden remissie percentages tot 35%
bereikt. De behandeling met DTIC gaat echter gepaard met dosis limiterende bijwerkingen
153

bestaande uit acuut braken en beenmergtoxiciteit bij een standaard dosering van 800 mg/m2
om de 3 weken. Voor verschillende solide tumoren, inclusief het melanoom is het belang van
dosis intensiteit voor de effectiviteit van chemotherapie beschreven. Met de beschikbaarheid
van twee nieuwe medicijnen die in staat zijn de bijwerkingen van chemotherapie te reducerenzou dosis intensificatie mogelijke kunnen zijn in een poging de therapeutische effectiviteit te
verhogen. Inhoofdstuk 9 worden de resultaten van een fase II onderzoek met individueledosis escalatie van dacarbazine in combinatie met interferon-alfa, de hematopoietische
groeifactor G-CSF en het 5HT3-antagonistische antiemeticum ondansetron bij patiënten met
een gemetastaseerd melanoom beschreven. De individuele DTIC dosis kon geintensifeerdworden tot 1500 mg/m2 eenmaal per 3 weken, waarna bijwerkingen van trombocytopenie en
leucopenie dosis limiterend werden. Er was een klein effect waarneembaar van de IFN op destimulatie van het G-CSF op het leucocyten getal. De bijwerkingen van misselijkheid en
overgeven waren bij de meeste patiënten goed controleerbaar met ondansetron. Vier van de
20 patiënten hadden een gedeeltelijke remissie van de tumor. Er werd geen relatie gevondentussen de dosisintensiteit en het optreden van een respons. Dosis escalatie van het DTIC lijkt
geen duidelijke verhoging van de effectiviteit te geven in dit regime.
154

Conclusies en perspectieven
Het gebruik van recombinante cytokines als biologische respons modifiers is nu ingevoerd in
de klinische geneeskunde, hoewel de werkingsmechanismen nog onduidelijk zijn. In demedische oncologie speelt de immuuntherapie een bescheiden rol bij sommige tumoren
waarvoor geen alternatieve behandelingsmogelijkheid voorhanden zijn. Ondanks het uitblijvenvan klinische doorbraken, vormen de recombinante cytokines een belangrijke nieuwe
modaliteit bij de behandeling van kanker. Immuuntherapie is gebaseerd op de mogelijkheid
van het immuunsysteem om ’zelf’ van ’niet-zelf’ te onderscheiden op basis van kenmerkenop de celmembraan. Ook het cytotoxisch effect van de effectorcellen van het immuunsysteem
speelt zich af op het niveau van de celmembraan, in tegenstelling tot de effecten van demeeste cytostatica die gericht zijn op het DNA in de celkern. Door onafhankelijk te zijn van
celdeling en de penetratie tot het DNA, zou immuuntherapie in staat kunnen zijn om juist die
tumor cellen te elimineren die aan de chemotherapie ontsnappen, omdat ze niet delen ten tijdevan de therapie. In combinatie met cytostatica, kunnen door chemotherapie epitopen op de
celmembraan van tumorcellen veranderen waardoor deze cellen mogelijk beter herkenbaarworden voor het immuunsysteem. Recente studies met combinaties van platinum bevattende
chemotherapie en immuuntherapie hebben bemoedigende resultaten laten zien bij patiënten
met een gemetastaseerd melanoom. Bij sommige patiënten met microscopische tumorrestenna therapie wordt verondersteld dat de tumor onder controle wordt gehouden door een
evenwicht tussen de tumor en het immuunsysteem. Stimulatie van de immunologische afweerin deze situatie nuttig kunnen zijn, hoewel het aantonen van een mogelijk effect zeer moeilijk
zal zijn. Het reversibele karakter van de bijwerkingen van immuuntherapie, in tegenstelling
tot de bijwerkingen van de meeste cytostatica, maken het een waardevol alternatief voorsommige vormen van kanker. Omdat vele aspecten van immuuntherapie nog onduidelijk zijn,
blijft het nodig om deze behandelingsvorm uit te voeren in de setting van klinischgecontroleerd onderzoek.
155