Embed Size (px)
Citation preview

Unit 35
Spinal Injuries

Overview
• Spinal column instability
• Mechanism of injury
• Types of spinal cord injuries
• Signs and symptoms of spinal injury
• Manual stabilization
• Spinal immobilization principles

Introduction
• Spinal cord injuries can leave patients with devastating neurologic injuries
• Injuries can lead to permanent disability, paralysis, and death
• Care provided by EMT has crucial impact on patient’s long-term outcomes
• EMT must recognize spine injuries
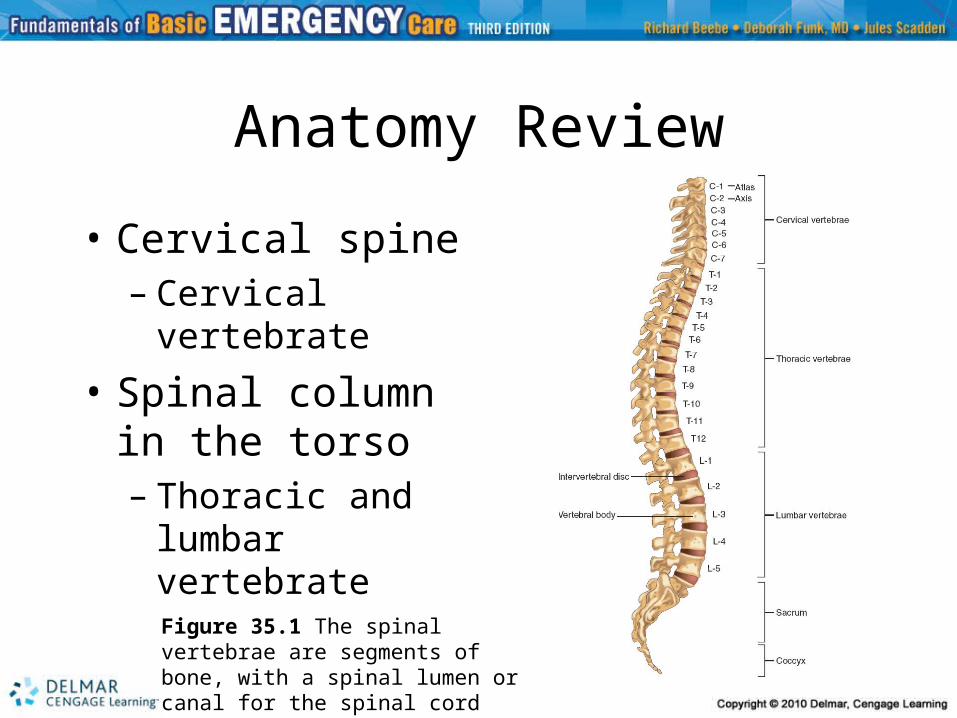
Anatomy Review
• Cervical spine– Cervical
vertebrate
• Spinal column in the torso– Thoracic and
lumbar vertebrate
Figure 35.1 The spinal vertebrae are segments of bone, with a spinal lumen or canal for the spinal cord

Anatomy Review
• Spinal cord– Anterior cord– Central cord – Posterior cord
• Nerve roots and dermatomes– Sensory and motor nerves– Dermatome: map of spinal nerves and
associated areas of sensation
Spinal Column Instability
• Injuries to cervical spine can be life threatening or have lifelong implications
• Hyperflexion: excessive forward bending of neck
• Hyperextension: excessive backward bending of neck
• Lateral bending: due to side impact

Spinal Column Instability (cont’d.)
• Axial loading: sudden downward pressure causing compression
• Axial distraction: cervical spine is pulled apart
Figure 35.11 Axial loading can occur from force applied from above, such as when the top of the head impacts with the windshield of a car
Mechanism of Injury
• Motor vehicle collision– Force may cause motion beyond normal range,
damaging spinal column
• Falls– Force of fall may fracture or burst bones
resulting in spinal cord injury
• Gun shot wounds– Bullet strike to spinal column will likely cause
trauma and spinal cord injury

Mechanism of Injury (cont’d.)
• Sports injuries– Collisions occurring during sports can result
in force, causing injury
• Associated injuries– EMT must consider spinal injury, if trauma
sustained by body part close to spine– Assume trauma occurring above clavicles, to
chest or abdomen, may also involve spine injury

Types of Spinal Cord Injuries
• Spinal cord injury may result in lacerations, compression, and stretching
• Primary spinal cord injury: occurs at time of incident
• Secondary spinal cord injuries: result from improper handling of patient with potential spinal cord injury
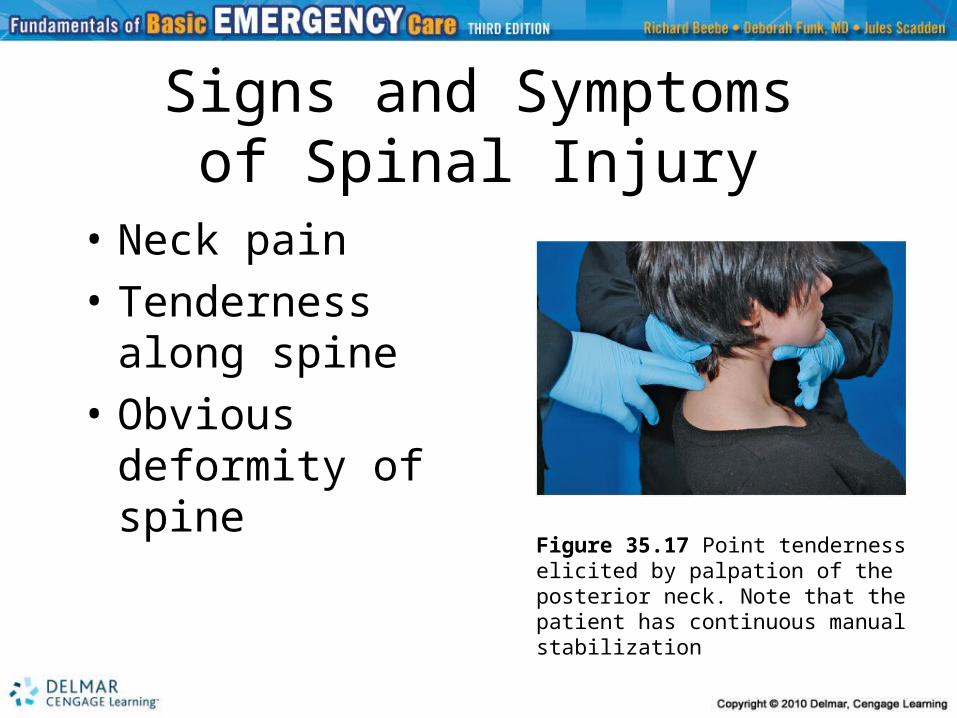
Signs and Symptomsof Spinal Injury
• Neck pain
• Tenderness along spine
• Obvious deformity of spine
Figure 35.17 Point tenderness elicited by palpation of the posterior neck. Note that the patient has continuous manualstabilization

Signs and Symptomsof Spinal Injury (cont’d.)
• Respiratory distress or arrest – Diaphragm may stop contracting – Signs: extreme shortness of breath,
respiratory difficulty, or apnea
• Neurogenic shock– Caused by loss of nervous system control
of blood pressure– Results in relative blood loss and
hypotension
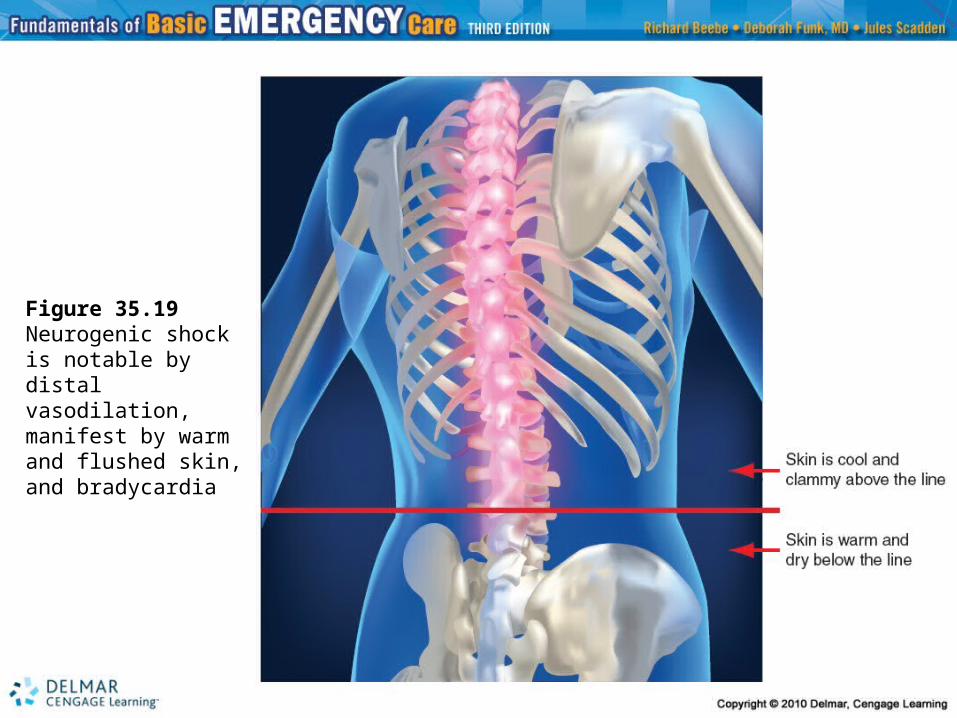
Figure 35.19 Neurogenic shock is notable by distal vasodilation,manifest by warm and flushed skin, and bradycardia
Signs and Symptomsof Spinal Injury (cont’d.)
• Paralysis– Depending on location of spinal cord injury,
areas affected by paralysis differ– Quadriplegia, paraplegia, and paresthesia
• Associated signs of spinal cord injury– Loss of control of bowels and/or bladder– Priapism: painful erection

Primary Assessment
• Always protect spine from further injury
• High-priority: full spine immobilization and immediate transport
• Low priority: proceed to secondary assessment at more measured pace

Considerations When Deciding on Spinal Immobilization
• Any patient with significant mechanism of injury and distracting injury should be treated for spine injury
• Assume spinal injury if patient is found unconscious and no one witnessed what caused patient’s condition
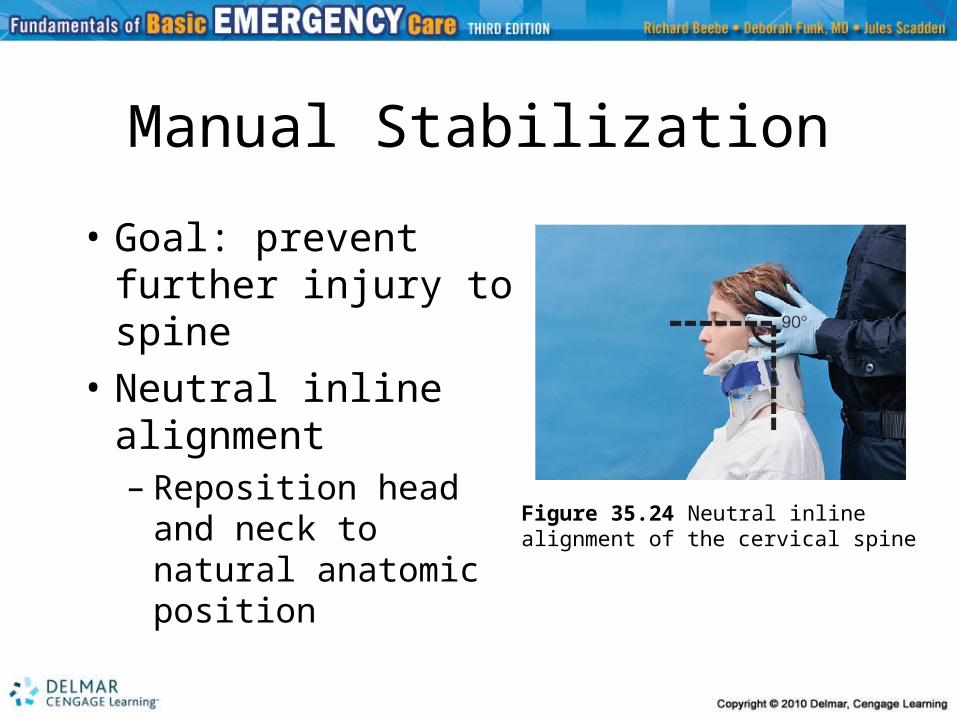
Manual Stabilization
• Goal: prevent further injury to spine
• Neutral inline alignment– Reposition head and
neck to natural anatomic position
Figure 35.24 Neutral inlinealignment of the cervical spine

Distal Neurologic Function
• Assesses peripheral neurologic function
• Check extremities for movement and sensation
• Look for signs of distal circulation
• Confirm distal circulation, sensation, and movement (CSM) before and after patient is placed on long backboard
Cervical SpineImmobilization Device
• Cervical collar: semi-rigid device used to maintain neutral inline alignment
• Application of the cervical spine immobilization device– Move chin cup up chest until chin is
trapped, then attach Velcro®

Special Problem of Helmets
• Important for EMT to know whether it is safer to take helmet off or leave on
• Keep helmet in place if well fitted and does not impede management of airway, breathing, and immobilization
• Remove loose fitting helmets

Spinal ImmobilizationPrinciples
• Immobilize entire length of spine using long backboard
• Head immobilization– Head secured last to prevent neck injury– Pediatric challenges
• Pediatric immobilization boards have dip in head section, allowing for child’s larger occiput
– Geriatric challenges• Use padding for curvature of spine
Moving Patientto Long Backboard
• Patient lying down– Four-person lift and slide– Long axis drag– Modified log roll– Orthopedic stretcher

Moving Patientto Long Backboard (cont’d.)
• Seated patient – Use intermediate device to move patient
• Rapid extrication– Remove seated patient quickly
• Short spinal immobilization device– Secures spine in upright position
• Standing patient – Perform standing takedown technique

Selective Spinal Immobilization
• Selective spinal immobilization criteria– Negative mechanism of injury does not
meet criteria • Isolated foot injury
– Uncertain mechanism of injury requires further assessment to meet criteria
• Slip and fall
– Positive mechanism of injury meets criteria• High velocity motor vehicle impact

Selective Spinal Immobilization (cont’d.)
• Assessment by clinical criteria– Determine neck pain, and extremity
sensation and motor function– Unreliable patient examination
• Use caution and immobilize patient
• Preexisting medical conditions– Elderly patient may have brittle bones

Transport
• Pay special attention and handle patient gently
• Provide extra padding
• Get patient safely to most appropriate hospital in reasonable amount of time
• Perform ongoing assessment

Conclusion
• EMT’s quick recognition of potential for spinal cord injury can help prevent further damage from occurring
• Careful immobilization while maintaining inline stabilization is key in managing patient who has sustained spinal injury