Embed Size (px)
Citation preview
Journal of Plastic, Reconstructive & Aesthetic Surgery (2008) 61, 1534e1538
CASE REPORT
Unilateral buttock reconstruction usingcontralateral inferior gluteal artery perforatorflap with the aid of multi-detector CT
H. Chang a, C. Heo a,*, J. Jeong a, R. Baek a, K. Minn a, C. Yoon b
a Department of Plastic and Reconstructive Surgery, The College of Medicine,Seoul National University, 28 Yeongun-dong, Chongno-gu, Seoul 110-744, South Koreab Department of Radiology, The College of Medicine, Seoul National University,28 Yeongun-dong, Chongno-gu, Seoul 110-744, South Korea
Received 29 August 2006; accepted 27 December 2006
KEYWORDSButtock reconstruction;Inferior gluteal arteryperforator flap (IGAPflap);Multidetector CT(MDCT)
* Corresponding author. Tel.: þ82 34058.
E-mail address: [email protected]
1748-6815/$-seefrontmatterª2008Bridoi:10.1016/j.bjps.2006.12.013
Summary The applicability of inferior gluteal artery perforator (IGAP) flaps in breast recon-struction following breast cancer has been well described. However, the use of IGAP flaps inbuttock augmentation has not been presented. We present the case of a female patient withbuttock asymmetry and a deficiency of volume, who underwent buttock reconstruction basedon a contralateral IGAP flap. Multidetector computed tomography (MDCT) was used to studydonor and recipient areas, and allowed easy interpretation as it provided anatomical imagesand three-dimensional anatomy reconstructions. Based on a knowledge of individual anatom-ical perforating vessel distributions, safe perforator flaps can be designed. Moreover, we areconvinced that buttock reconstruction using autologous tissue can be performed in a safeand reliable fashion using perforator flaps. Donor site morbidity was minimal and the muscleat the donor site was preserved. The contralateral buttock proved an excellent donor sitefor aesthetic unilateral buttock reconstruction and provided ample tissue in the describedcase.ª 2008 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
1 787 7222; fax: þ82 31 787
(C. Heo).
tishAssociationofPlastic,Reconstruc
The buttocks are an important element of sexual attrac-tion, and occupy a major place in the concept of beauty asrecognised by most cultures and ethnic groups. Conse-quently, for several decades, a number of surgeons havebeen attempting to correct alterations in the shape andvolume of this region by resection and skin adjustments,
tiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.
Unilateral buttock reconstruction using contralateral IGAP 1535
placement of gluteal prostheses, liposuction, lipoinjection,or other techniques.1 The authors report the case of a pa-tient with unilateral buttock deformity who underwent au-tologous reconstruction using a contralateral IGAP flap.
Case report
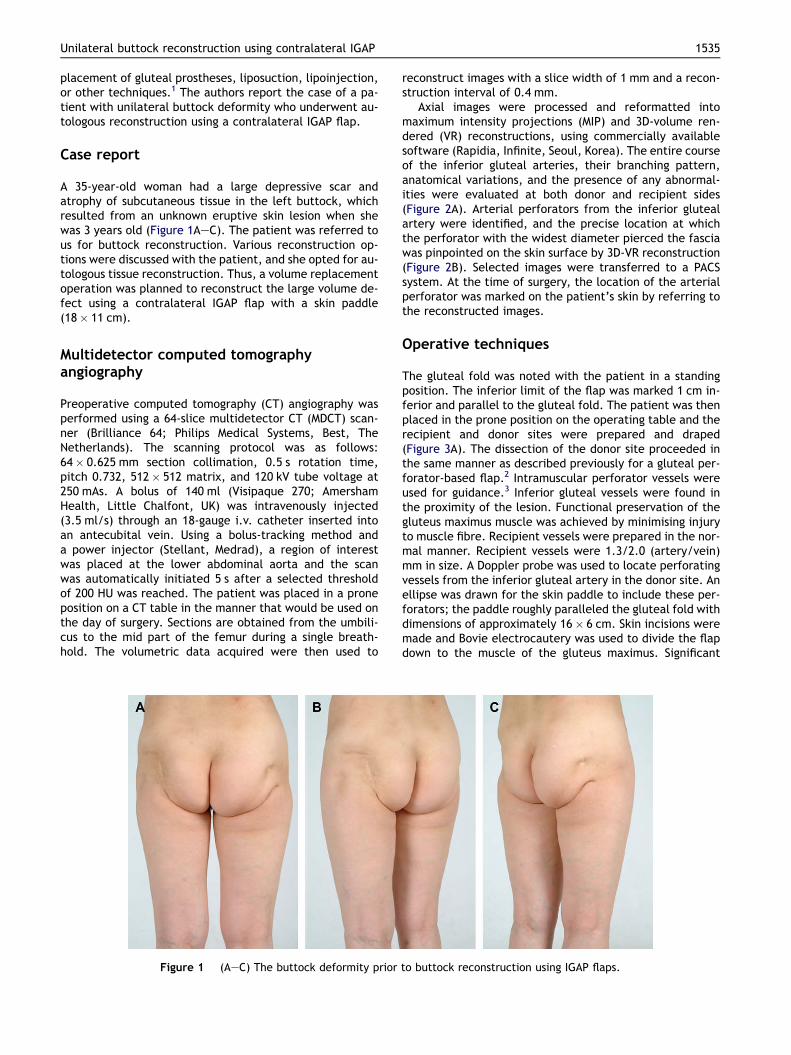
A 35-year-old woman had a large depressive scar andatrophy of subcutaneous tissue in the left buttock, whichresulted from an unknown eruptive skin lesion when shewas 3 years old (Figure 1AeC). The patient was referred tous for buttock reconstruction. Various reconstruction op-tions were discussed with the patient, and she opted for au-tologous tissue reconstruction. Thus, a volume replacementoperation was planned to reconstruct the large volume de-fect using a contralateral IGAP flap with a skin paddle(18� 11 cm).
Multidetector computed tomographyangiography
Preoperative computed tomography (CT) angiography wasperformed using a 64-slice multidetector CT (MDCT) scan-ner (Brilliance 64; Philips Medical Systems, Best, TheNetherlands). The scanning protocol was as follows:64� 0.625 mm section collimation, 0.5 s rotation time,pitch 0.732, 512� 512 matrix, and 120 kV tube voltage at250 mAs. A bolus of 140 ml (Visipaque 270; AmershamHealth, Little Chalfont, UK) was intravenously injected(3.5 ml/s) through an 18-gauge i.v. catheter inserted intoan antecubital vein. Using a bolus-tracking method anda power injector (Stellant, Medrad), a region of interestwas placed at the lower abdominal aorta and the scanwas automatically initiated 5 s after a selected thresholdof 200 HU was reached. The patient was placed in a proneposition on a CT table in the manner that would be used onthe day of surgery. Sections are obtained from the umbili-cus to the mid part of the femur during a single breath-hold. The volumetric data acquired were then used to
Figure 1 (AeC) The buttock deformity prior
reconstruct images with a slice width of 1 mm and a recon-struction interval of 0.4 mm.
Axial images were processed and reformatted intomaximum intensity projections (MIP) and 3D-volume ren-dered (VR) reconstructions, using commercially availablesoftware (Rapidia, Infinite, Seoul, Korea). The entire courseof the inferior gluteal arteries, their branching pattern,anatomical variations, and the presence of any abnormal-ities were evaluated at both donor and recipient sides(Figure 2A). Arterial perforators from the inferior glutealartery were identified, and the precise location at whichthe perforator with the widest diameter pierced the fasciawas pinpointed on the skin surface by 3D-VR reconstruction(Figure 2B). Selected images were transferred to a PACSsystem. At the time of surgery, the location of the arterialperforator was marked on the patient’s skin by referring tothe reconstructed images.
Operative techniques
The gluteal fold was noted with the patient in a standingposition. The inferior limit of the flap was marked 1 cm in-ferior and parallel to the gluteal fold. The patient was thenplaced in the prone position on the operating table and therecipient and donor sites were prepared and draped(Figure 3A). The dissection of the donor site proceeded inthe same manner as described previously for a gluteal per-forator-based flap.2 Intramuscular perforator vessels wereused for guidance.3 Inferior gluteal vessels were found inthe proximity of the lesion. Functional preservation of thegluteus maximus muscle was achieved by minimising injuryto muscle fibre. Recipient vessels were prepared in the nor-mal manner. Recipient vessels were 1.3/2.0 (artery/vein)mm in size. A Doppler probe was used to locate perforatingvessels from the inferior gluteal artery in the donor site. Anellipse was drawn for the skin paddle to include these per-forators; the paddle roughly paralleled the gluteal fold withdimensions of approximately 16� 6 cm. Skin incisions weremade and Bovie electrocautery was used to divide the flapdown to the muscle of the gluteus maximus. Significant
to buttock reconstruction using IGAP flaps.
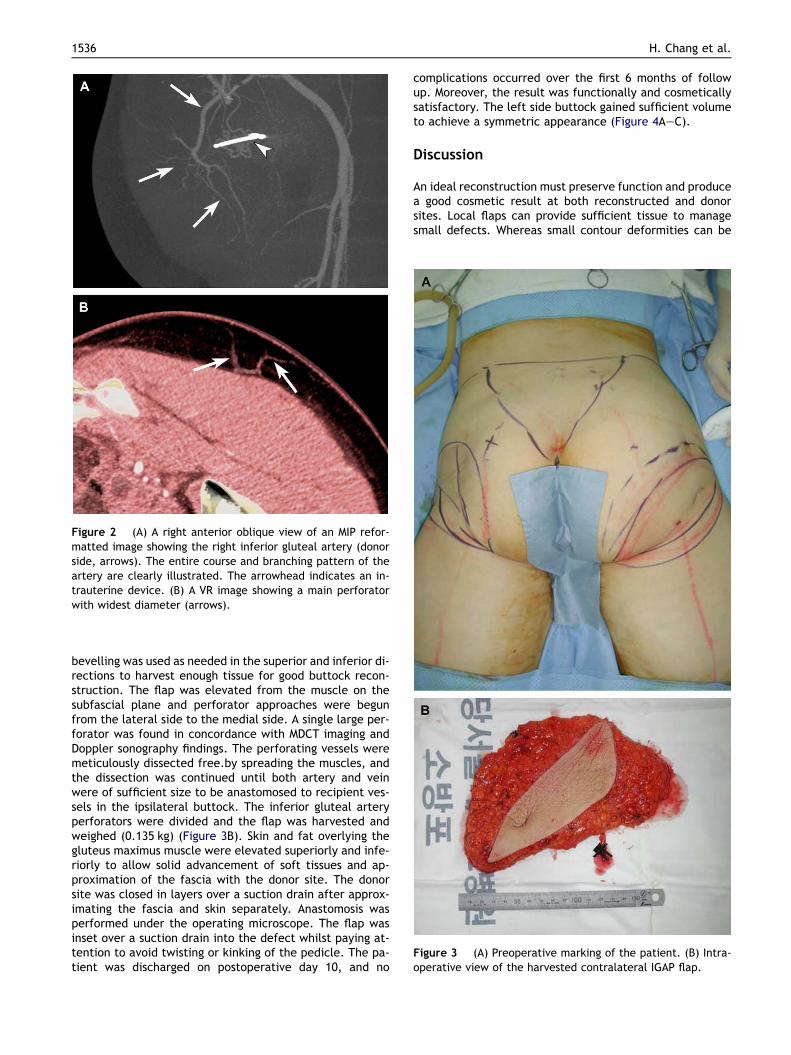
Figure 2 (A) A right anterior oblique view of an MIP refor-matted image showing the right inferior gluteal artery (donorside, arrows). The entire course and branching pattern of theartery are clearly illustrated. The arrowhead indicates an in-trauterine device. (B) A VR image showing a main perforatorwith widest diameter (arrows).
Figure 3 (A) Preoperative marking of the patient. (B) Intra-operative view of the harvested contralateral IGAP flap.
1536 H. Chang et al.
bevelling was used as needed in the superior and inferior di-rections to harvest enough tissue for good buttock recon-struction. The flap was elevated from the muscle on thesubfascial plane and perforator approaches were begunfrom the lateral side to the medial side. A single large per-forator was found in concordance with MDCT imaging andDoppler sonography findings. The perforating vessels weremeticulously dissected free.by spreading the muscles, andthe dissection was continued until both artery and veinwere of sufficient size to be anastomosed to recipient ves-sels in the ipsilateral buttock. The inferior gluteal arteryperforators were divided and the flap was harvested andweighed (0.135 kg) (Figure 3B). Skin and fat overlying thegluteus maximus muscle were elevated superiorly and infe-riorly to allow solid advancement of soft tissues and ap-proximation of the fascia with the donor site. The donorsite was closed in layers over a suction drain after approx-imating the fascia and skin separately. Anastomosis wasperformed under the operating microscope. The flap wasinset over a suction drain into the defect whilst paying at-tention to avoid twisting or kinking of the pedicle. The pa-tient was discharged on postoperative day 10, and no
complications occurred over the first 6 months of followup. Moreover, the result was functionally and cosmeticallysatisfactory. The left side buttock gained sufficient volumeto achieve a symmetric appearance (Figure 4AeC).
Discussion
An ideal reconstruction must preserve function and producea good cosmetic result at both reconstructed and donorsites. Local flaps can provide sufficient tissue to managesmall defects. Whereas small contour deformities can be

Figure 4 (AeC) Postoperative photographs taken 6 months after buttock reconstruction.
Unilateral buttock reconstruction using contralateral IGAP 1537
corrected by lipoinjection, dermal fat flaps and dermalimplants, large defects and deformities require the transferof more tissue.4e8 Babuccu et al. demonstrated changes inthe gluteal region with age and weight gain in young andmiddle-aged women from the perspective of aesthetic sur-gery.9 During the prepubertal period, the interglutealsulcus and infragluteal sulci do not actively change. How-ever, weight gain has a major influence on the shape ofthe gluteal region, and commensurate with the hormonesurge associated with puberty, the gluteal region expandsin all directions. Moreover, although age affects the shapeof the gluteal region during the pubertal period, duringthe postpubertal, menopausal, and postmenopausal pe-riods, weight becomes the major determinant as the but-tocks sag with weight gain. This causes infragluteal sulcito move in downward and lateral directions and a lengthen-ing of the intergluteal sulcus. In addition, gluteal shape issubject to the effects of demographics, such as, ethnicity,feeding habits and lifestyle. During assessments of glutealregion morphology, it is advisable to consider its dynamicnature, and thus in the present case, we decided to adapta contralateral IGAP flap for gluteal reshaping, which hasbeen reported to provide excellent result at donor and re-cipient sites to ensure gluteal harmony and aesthetic integ-rity.8 Preoperative marking speeds up surgical dissectionand aids the location of vessels intraoperatively. Moreover,preoperative ultrasonography and pencil Doppler can pro-vide an overall view of the distributions of individual perfo-rating vessels but do not provide a definite place in theplanning of free microvascular perforator flaps. Anatomicalvariations make microsurgical dissection significantly moredifficult and can even threaten the success of the flap bydamaging the delicate venae comitantes.10 However, ad-vances in CT technology, especially MDCT, enable noninva-sive vascular imaging with high spatial and temporalresolutions. Moreover, MDCT angiography allows preciseevaluations to be made of the origins, courses and relationsof small diameter vessels in both donor and recipient areas.In addition, the costs of MDCT and ultrasonography to thepatients are similar because of medical insurance in ourcountry. Recently several investigators have reported their
initial successful experiences of MDCT for the mapping ofdeep inferior epigastric perforators for breast reconstruc-tion.11,12 In our case preoperative MDCT angiography pro-vided an accurate vascular map of the inferior glutealperforator. To our knowledge, these are the first reportson the use of MDCT for this purpose. The reformatted im-ages obtained were easy to interpret because they clearlydemonstrated a multi-dimensional overview of the arterialanatomy. This technique precisely localised the arterialperforator, and was useful during surgical planning. Basedon individual anatomical demonstrations of perforating ves-sels, even individual perforator flaps could be designed us-ing this method. It also permits the option of performinga virtual anatomy dissection of the patient on a computer.In the present study, donor site dissection was performed asfor gluteal perforator-based flaps.2 Intramuscular perfora-tor vessels were used for guidance.3 Even though dissectionwithin the muscle was somewhat tedious, careful ligationof branches and the dissection of perforator vessels usinga retractor facilitated the safe and easy preparation ofthe recipient vessel. Inferior gluteal vessels were reliableand of large calibre, were present in the proximity of thelesion and were versatile enough to cover defects. More-over, functional preservation of the gluteus maximus wasachieved whilst minimising injury to muscle fibre.
Buttock reconstruction for aesthetic purposes is a diffi-cult issue in plastic surgery. Here, we describe the use ofautologous tissue transfer for buttock reconstruction ina safe and reliable fashion using IGAP flaps. Contralateralbuttock can provide ample tissue and may be an excellentchoice as a donor site. Moreover, MDCT allowed preciseimaging using three-dimensional anatomical reconstruc-tions and, thus, we advocate its use for perforator flapreconstruction.
References
1. Cuenca-Guerra R, Quezada J. What makes buttocks beautiful?A review and classification of the determinants of glutealbeauty and the surgical techniques to achieve them. AestheticPlast Surg 2004;28:340e7.

1538 H. Chang et al.
2. Koshima I, Moriguchi T, Soeda S, et al. The gluteal perforator-based flap for repair of sacral pressure sores. Plast ReconstrSurg 1993;91:678e83.
3. Park SH. Muscle-splitting approach to superior and inferior glu-teal vessels: versatile source of recipient vessels for free-tissuetransfer to sacral, gluteal, and ischial regions. Plast ReconstrSurg 2000;106:81.
4. Pereira LH, Radwanski HN. Fat grafting of the buttocks andlower limbs. Aesthetic Plast Surg 1996;20:409e16.
5. Raposo-Amaral CE, Cetrulo Jr CL, Guidi Mde C, et al. Bilaterallumbar hip dermal fat rotation flaps: a novel technique for au-tologous augmentation gluteoplasty. Plast Reconstr Surg 2006;117:1781.
6. Gonzalez R. Augmentation gluteoplasty: the XYZ method. Aes-thetic Plast Surg 2004;28:417e25.
7. Gurlek A, Demir CY, Askar I, et al. A transverse rectus ab-dominis myocutaneous (TRAM) flap for reconstruction ofa large deformity in the buttock: a new indication for
a TRAM flap. Scand J Plast Reconstr Surg Hand Surg 2005;39:95e9.
8. Josvay J, Sashegyi M, Kelemen P, et al. Clinical experience withthe hatchet-shaped gluteus maximus musculocutaneous flap.Ann Plast Surg 2005;55:179e82.
9. Babuccu O, Kargi E, Hosnuter M, et al. Morphology of the glu-teal region in the female population 5 to 83 years of age. Aes-thetic Plast Surg 2004;28:405e11.
10. Giunta RE, Geisweid A, Feller A. The value of preoperativeDoppler sonography for planning free perforator flaps. PlastReconstr Surg 2000;105:2381.
11. Masia J, Clavero JA, Larranaga JR, et al. Multidetector-rowcomputed tomography in the planning of abdominal perforatorflaps. J Plast Reconstr Aesthet Surg 2006;59:594e9.
12. Alonso-BurgosA,Garcia-TutorE,BastarrikaG,etal.Preoperativeplanning of deep inferior epigastric artery perforator flap recon-structionwith multislice-CTangiography: imaging findingand ini-tial experience. J Plast Reconstr Aesthet Surg 2006;59:585e93.