Embed Size (px)
Citation preview

UsaieimBjAipeaaaIcccoopwrdti
Urcin
FSRnEC©0d
C
Ultrasound-Guided Therapeutic Procedures inthe Musculoskeletal System
Jose Luis del Cura, MD, PhD
iedgiotmatbt
caTltrccfdfit
GBmSltsism
ltrasound allows the exploration of most of the musculo-keletal system, including lytic bone lesions. Its flexibility,vailability, and low cost make it the best tool to guide
nterventional therapeutic procedures in any musculoskel-tal system lesion visible on ultrasound. These techniquesnclude drainages of abscesses, bursitis, hematomas oruscular strains, treatment of cystic lesions (ganglions,aker’s cysts), arthrocentesis, injection of substances in
oints and soft tissues, and aspiration of calcific tendinitis.lthough the puncture of joints for arthrocentesis and
njection of substances are performed by clinicians usingalpation, the use of ultrasound guidance improves theffectiveness of the technique especially for small or poorlyccessible lesions and joints and for obese patients. Drain-ge can be performed using catheters or needles and canvoid a more aggressive approach most of the time.
ntracavitary urokinase helps when the aim is to drainlotted hematomas or fibrinous collections. Injection oforticoids is useful in the treatment of ganglia, Baker’systs, tendinitis, and noninfected arthritis. Calcific tendinitisf the shoulder can be effectively treated using percutane-us “lavage” with lidocaine. Calcifications usually disap-ear and symptoms improve in nearly 90% of the casesithin a year. Most of these techniques are low cost and
equire only a moderate skill. Ultrasound-guided proce-ures are useful tools to effectively treat some diseases of
he musculoskeletal system and should be routine in anymaging department.
ltrasound (US) can detect, locate, and identify a wideange of musculoskeletal lesions, including those lo-ated within the bone when the cortex is destroyed. Its an extraordinarily flexible, readily available tech-ique, with a low cost. Moreover, it does not use
rom the Servicio de Radiodiagnóstico, Hospital de Basurto, Bilbao,pain.eprint requests: Jose Luis del Cura, MD, PhD, Servicio de Radiodiag-óstico, Hospital de Basurto, Ave. Montevideo 18, 48013 Bilbao, Spain.-mail: [email protected] Probl Diagn Radiol 2008;37:203-18.2008 Mosby, Inc. All rights reserved.
363-0188/2008/$34.00 � 0
poi:10.1067/j.cpradiol.2007.08.001urr Probl Diagn Radiol, September/October 2008
onizing radiation. These features have made US anmergent tool in the evaluation of musculoskeletaliseases. Also, this imaging technique is excellent foruiding minimally invasive interventional proceduresn the musculoskeletal system when lesions are visiblen US. An important additional advantage of US ishat it works in real time. This permits continuousonitoring of any procedure, allowing visualization of
ny needle or instrument used all the time, making theechnique more safe and accurate. Afterwards, US cane used to control the outcome of the procedures ando monitor treated lesions.
The procedures that can be performed with USontrol are diverse: diagnostic techniques (biopsies,rthrocentesis) or therapeutic procedures (Table 1).hese techniques are, in general, very effective and are
ess costly than their diagnostic or therapeutic alterna-ives, and, for most of them, only a moderate skill isequired. Although currently this tool is being effi-iently used for the diagnosis and treatment of mus-uloskeletal diseases, many radiologists are still notully aware of its wide potential. What follows is aiscussion of the different US-guided techniques usedor the treatment of musculoskeletal diseases, theirndications, and possible difficulties and complica-ions.
eneral Requirementsefore starting any procedure, the lesion to be treatedust be identified, defined, and located with precision.o, a careful US study of the area where the lesion is
ocated is required. Usually, high-resolution (morehan 7 MHz) lineal array transducers are the mostuitable to carry out most of the explorations andnterventions in the musculoskeletal system. Occa-ionally, for lesions or structures deeply located, itay be necessary to use 3.5- or 5-MHz curved array
robes.1 Convex probes have the disadvantage of
203

mIUa
bstcc
tHnemlcr
adltptanbrortbn
hsv
apsUt
pppwmwaabcscmtpps
ib
Fss
Tp
2
aking the visualization of the needles more difficult.t is useful to complete the exploration with a DopplerS to identify nearby vessels, to plan the procedure
nd avoid damaging them.2
Any lesion must comply with two requirements toe treated or diagnosed with a US-guided procedure: ithould be visible on US, and it should be accessiblehrough an acoustic window, so that the needle usedan be seen in its entire path and the process can beontrolled in real time.
Diverse devices have been designed to attach to theransducer head for help in guiding the procedures.owever, although sometimes helpful, they are notecessary because a freehand technique can be used invery case. Using a freehand technique requires only aoderate skill and is more flexible in approaching the
esion. A needle guide is more expensive and time-onsuming and restricts the paths available.3 For thateason, we always use a freehand technique.
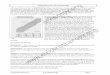
The procedure should be planned in advance tovoid vessels, nerves, or any structure that could beamaged. As a general rule, the shortest path to theesion is the most adequate one. On the other hand,he ideal path of the needle is the one that is mostarallel to the surface of the transducer. This orien-ation will increase the echogenicity of the needlend will enable a better visualization. When theeedle is parallel to the surface, it appears as aright echogenic line, sometimes with associatedeverberation artifacts4 (Fig 1). If the direction isblique, the echogenicity of the needle becomeseduced, and when the angle is very oblique, onlyhe tip of the needle can be seen, showing up as aright echogenic dot. When visualization of the
ABLE 1. US-guided therapeutic interventions that can beerformed in musculoskeletal system
ArthocentesisJoint and soft-tissue injections
CorticosteroidsHyaluronic acid
DrainageAbscessesBursitisHematomasMuscular strainsTennis leg
Treatment of cystic lesionsGangliaPopliteal cysts
Aspiration of calcific tendinitis
eedle is difficult, moving it quickly in and out can c
04
elp to identify its position.4 A single focal zonehould be selected to avoid artifacts and to make theisualization of the needle more precise.
All procedures can be performed with localnesthesia. We use 1% lidocaine injected into theuncture site. The puncture site and the needle usedhould be carefully sterilized to maintain asepsis.sually, it is not necessary to use sterile covers for
he transducer.To avoid bleeding that can result from any of the
rocedures, it is advisable to have the coagulationarameters within acceptable levels. Before eachrocedure, we arrange for some coagulation tests,hich include prothrombin time, international nor-alized ratio (INR), and a platelet count. In patientsith coagulopathies or those subject to an antico-
gulant treatment, these analyses should be obtainedt least 24 hours before the procedure. However,leeding diathesis is rarely an absolute contraindi-ation. For biopsy or puncture with a fine needle ofuperficial lesions, where an adequate hemostasisan be achieved by direct pressure, these require-ents can be omitted. In the remaining lesions and
echniques, if the patient has less than 60,000latelets, the procedure can be performed after alatelet transfusion. If INR is above 1.5, we pre-cribe the administration of fresh plasma.
Before the procedure, the patient should be dulynformed of the procedure, its purpose, and the possi-le complications derived, and the patient’s informed
IG 1. Percutaneous treatment of shoulder calcific tendinitis in theupraspinatus tendon. Reverberation artifacts (arrows) can be ob-erved behind the needle.
onsent should be obtained.
Curr Probl Diagn Radiol, September/October 2008

ATifmuirthsepgoj
I
etsi
erspecsua
C
it
w
T
srmaci
pcr
Fa(nj
C
rthrocentesishe puncture of joints for arthrocentesis and the
njection of substances is a routine procedure per-ormed by orthopedists and rheumatologists. Inost cases, they carry it out without image aid,
sing palpation for guidance. However, the reliabil-ty of the intra-articular location of the injection iselatively low.5,6 Similarly, the failure of arthrocen-esis performed without imaging control is quiteigh, especially in obese patients and small effu-ions. The puncture of joints guided by US is anasy technique and enables the success of therocess to be assured. The use of sonographicuidance is particularly useful for small effusions,bese patients, or in cases of poorly accessibleoints such as the hip.3-8
ndicationsArthrocentesis is indicated in the case of joint
ffusion. Arthrocentesis allows joint fluids to be ex-racted in order to diagnose the type of arthritis. Ineptic arthritis, it is useful for obtaining fluid to culturen order to determine the pathogen agent.3,4
Therapeutic arthrocentesis is indicated for painfulffusions to decompress the joint. It will generally beequested when the arthrocentesis performed by theurgeon has failed, which is often the case in obeseatients and when the effusion is very dense, dueither to a highly fibrinous or hemorrhagic content. Itan also be used to drain purulent fluid in cases ofeptic arthritis or bursitis. Arthrocentesis can be alsosed to inject drugs (usually corticosteroids) into therticulation for treatment.7,8
ontraindicationsThe alterations of the coagulation are not a contra-
ndication. For these patients, the previously men-ioned precautions should be followed.
An injection of corticosteroids is contraindicatedhen septic arthritis is suspected.
echnique (Fig 2)The joint fluid is frequently dense, particularly in
eptic arthritis. Therefore, it is convenient to useelatively thick needles. We use 16- to 20-G needles inost cases. For superficially located joints, local
nesthetic is not necessary. For deeper ones or when itan be anticipated that the procedure will be lengthy,
t is advisable to minimize pain by anesthetizing the surr Probl Diagn Radiol, September/October 2008
ath. In young children and especially when an arthro-entesis of the hip is to be performed, sedation may beequired.
The path selected for the puncture should be the
IG 2. Knee arthrocentesis using a freehand technique. (A) A vascularccess catheter is introduced with sonographic guidance into the joint.B) Effusion is aspired from the joint using the vascular catheter of theeedle. (C) US image showing the catheter (arrows) placed inside theoint.
hortest that allows having the needle as parallel as
205

phaas
lTaTirwpftpmToes5
oo8eiotkoI
sopvh
R
ircr
C
cmafl
jrmsa
JStrH
Fa need
2
ossible to the surface of the transducer. Once the jointas been reached with the tip of the needle, the fluid isspirated. In superficial joints, the technique is simplend does not pose any difficulties, but in the hip, somepecific considerations should be made.
In the hip, aspiration should be performed in theocation where the fluid is better visualized on US.his location is within the anterior capsule andnterior to the surface of the neck of the femur.3,4
he puncture should be performed with the patientn the supine position and the hip in externalotation, with the transducer and the needle alignedith the axis of the neck of the femur. In adultatients and especially in obese ones, the distancerom the puncture site can be quite long and,herefore, before performing the arthrocentesis, therocedure should be thoroughly planned, the patheasured, and a sufficiently long needle selected.he tract of the needle in the hip is relativelyblique and, therefore, the control of the procedure,specially in obese patients, is more difficult. Inome patients, it may be necessary to use a 3.5- to-MHz curved array transducer.
Sometimes, the density of the fluid or the presencef clots, fibrine films, or septa may make the drainagef effusions difficult. In these cases, the use of 6- to-F catheters placed in a recess of the joint cavity maynable the joint to be drained. It is also possible tonject fibrinolytics inside the joint to achieve the lysisf the fibrine or the clots to facilitate the drainage ofhe effusion (Fig 3). We use fibrinolytics in thenee, which is the joint where this problem is mostften encountered. In these cases, we inject 100,000
IG 3. (A) Drainage of a septic arthritis in knee using a trocar catheterrow). Due to the dense nature of the effusion, use of urokinase was
U of urokinase dissolved in 20 to 30 mL saline c
06
olution. After 1 to 2 hours, we aspirate the joint orpen the drainage, enabling the fluid to flow. Thisrotocol has enabled the aspiration of septated oriscous effusions in nearly every case where weave used it.
esultsThe decompression of the joint always results in an
mmediate relief of symptoms, even if there is aecurrence of the effusion, especially when it is asso-iated with an intra-articular injection of corticoste-oids (if indicated).
omplicationsIn septic arthritis, manipulation of the joint can
ause spreading of the infection. It is advisable not toove the needle too much within the joint in septic
rthritis and limit the procedure to the aspiration of theuid in the most direct way possible.
In noninfectious effusions, the manipulation of aoint, especially if catheters are used, implies a higherisk of infection. Whenever intra-articular catheters,anipulations, or repeated punctures are used, they
hould be associated with prophylactic broad spectrumntibiotic treatment.
oint and Soft-Tissue Injectionsimilar to arthrocentesis, joint and soft-tissue injec-
ions are also routinely performed by orthopedists andheumatologists under palpation, without image aid.owever, the accuracy of the location of the injection
ws). (B) The catheter can be finally seen placed inside the joint (opened to completely drain it.
r (arro
annot be guaranteed. US guidance is excellent to
Curr Probl Diagn Radiol, September/October 2008

ci
I
iatslsl
epta
T
istti
UWpoti
pfb(
taat
R
cin
Fmr
Fl(
C
onfirm that the injection is placed in the point wheret is most effective.
ndicationsAn intra-articular injection of steroids can be useful
n the treatment of various types of noninfectiousrthritis, for managing the pain caused by degenera-ive, traumatic, or inflammatory arthritis. Other sub-tances, such as hyaluronic acid, can be intra-articu-arly injected.9 Image guidance will assure that theseubstances are effectively delivered inside the articu-ation.7,8,10,11
Treatment of extra-articular musculoskeletal dis-ase, such as tendinitis, synovitis, or fasciitis, can beerformed by direct injection of corticoids in or next tohe diseased structure and US is an excellent tool toccurately guide these injections.12
echniqueFor the injection of substances, intra-articularly or
n soft tissues, thinner needles (22-25 G) are the mostuitable as they are less painful. Although local anes-hetics are not strictly necessary, it is advised to usehem, given that injections may be painful, especiallyn low-capacity joints and in thinner parts of the body.
Injections should be performed under continuousS guidance, similar as described for arthrocentesis.hen injecting articulations, the needle tip should
referably be directed to the locations where fluid isbserved. In doing so, the intra-articular position ofhe needle tip can be more easily confirmed before
IG 4. Treatment of a traumatic effusion in ankle (A). A needle is plaore fluid can be observed (B). After draining the effusion, 40 mg tr
ecovered completely.
njection (Fig 4). a
urr Probl Diagn Radiol, September/October 2008
In the treatment of tendinitis or fasciitis, we like tolace the needle tip in the periphery of the tendons orascias, to avoid intrasubstance injections which cane painful and which can debilitate theses structuresFig 5).
When corticosteroids are to be injected, differentypes can be used, alone or in combination with localnesthetics. We usually use 40 mg triamcinolonecetonide, a long-acting steroid, as a standard injec-ion.
esultsThese injections are usually very effective in the
ontrol of pain caused by articular or soft-tissuenflammatory or degenerative diseases. The effects areoticed a short time after the injection. The intra-
nder sonographic guidance into the joint, aiming to the place whereinolone acetate was injected. The pain disappeared and the patient
IG 5. Injection of corticosteroid in the treatment of lateral epicondy-itis. A needle (arrow) is directed to the surface of the inflamed tendonasterisk).
ced uiamc
rticular corticosteroid injection usually reduces the
207

js
C
mtcfu
D
fot
I
waaapt
C
f
T
atmveaacactt
sdTtowsficiOsdtittWeal
cmtuu
ihfas
Ffa
2
oint effusions in a few days and improves clinicalymptoms.13
omplicationsLocal skin atrophy has been described after treat-
ent with certain types of corticosteroids such asriamcinolone14 (Fig 6). Septic arthritis is a potentialomplication. Thus, a sterile technique must be strictlyollowed. If repeated corticosteroid injections aresed, cartilage destruction may be accelerated.8
rainage of Muscular AbscessesMuscular abscesses can result as complications
rom surgery or trauma. They can also occur as a resultf foreign bodies. Moreover, they can be the result ofhe extension of nearby or distant infectious processes.
ndicationsDrainage of muscular abscesses can be performed
ith two objectives: First, to obtain fluid for culturend identification of the specific pathogen causing thebscess; an abscess can also be drained to cure it andvoid surgery or to improve the symptoms of theatient and their condition before performing an elec-ive surgery.
ontraindicationsIn situations of bleeding diatheses, the criteria to
IG 6. Skin atrophy in the lateral side of the elbow in a patient treatedor lateral epicondylitis with US-guided injection of triamcinolonecetate. The lesion spontaneously disappeared in a month.
ollow are as previously explained above. r
08
echniqueMuscular abscesses can be drained by directly
spirating them with a needle or by placing a percu-aneous drainage catheter. The aspiration by needleay be enough for small-sized abscesses with low
iscosity fluid. In these cases, the puncture alsonables fluid to be obtained for bacteriological culturend total aspiration of the abscess in combination withppropriate antibiotic treatment can be sufficient toure the infection. Large-bore needles (14- to 18-G)re recommended, especially those with vascular ac-ess catheters, through which the drainage of collec-ions can be performed quite efficiently after removinghe inner metallic needle.
Drainage catheters are necessary for larger ab-cesses. These are catheters with side holes in theiristal end that enable the discharge of purulent fluid.hey can be placed using the Seldinger technique or
he trocar system.4 The Seldinger technique consistsf puncturing the collection with a needle throughhich a guide wire is passed and passing through it
uccessive dilators until the drainage catheter isnally placed in the cavity. The trocar catheter is aatheter mounted on a hollow rigid metallic guide,nside which a sharp metallic needle is introduced.nce mounted, the whole device looks similar to a
harp needle covered by the catheter. It is intro-uced in the collection by direct puncture throughhe skin and, once the collection is reached, thenner needle is removed and the catheter is slidhrough the metallic guide until the distal part withhe side holes is placed inside the collection (Fig 7).
e always use the trocar technique because itnables drainage to be performed in one single stepnd has the advantage of being easier to perform foress skilled radiologists.
The catheter can be connected to a bag or aollector to allow drainage of the purulent fluid. Weaintain the drainage until the patient is afebrile, until
heir blood formula shows no signs of infection, andntil the drain is less than 10 mL/d for three consec-tive days.
Muscular abscesses have the inconvenience of be-ng too viscous. Also, they often contain sphacelus orematic clots which obstruct the catheters. It is there-ore necessary to control them frequently and, if theyre obstructed, disobstruct with the injection of aterile saline solution through the catheter. For those
easons, enough bore catheters should be used. WeCurr Probl Diagn Radiol, September/October 2008

ut
R
anaeip
tpiTsfp
C
pip(t
ccpto
DH
FF
C
sually use 8- to 10-F and, occasionally, 12-F cathe-ers.
esultsIn a large number of cases, the percutaneous drain-
ge achieves the healing of the abscess and avoids theeed for surgery. In our experience, this is achieved inpproximately 80% of cases. In the rest, the drainagenables the infection to be controlled and also reducests size, making surgery easier and enabling it to beerformed as an elective intervention.
There are various factors that we have observed andhat are associated with a higher risk of failure of theercutaneous drainage. One is the association withnfectious lesions in the adjacent bone (osteomyelitis).he other is the presence of intracavitary elements,uch as foreign bodies, myositis ossificans, or boneragments, where germs can remain, resulting in re-
IG 7. Drainage of a muscular abscess in the thigh (A). A trocar (arrowinally, a catheter (open arrow) can be seen in the collection (D).
eated recurrence of the infection (Fig 8). o
urr Probl Diagn Radiol, September/October 2008
omplicationsOften the puncture of the infected tissue spreads the
athogen to the blood, resulting in a bacteremia. It ismportant to carry out the procedure after treating theatient with a specific or a broad spectrum antibioticwhen the pathogen is unknown) and to maintain suchreatment subsequently.
As in any other intervention procedure, and espe-ially when large-bore catheters are used, bleeding canomplicate the puncture. The need to prevent theuncture of large vessels has been previously men-ioned as well as the precautions that need to bebserved in cases of bleeding diatheses.
rainage of Hematomasematomas of soft tissue are generally of traumatic
introduced under sonographic guidance into the collection (B and C).
s) isrigin, although they appear more easily in patients
209

wbwct
I
rtHtptsdt
iao
prphtiead
C
FA ted fo
Fsc vity in
2
ith bleeding diatheses, especially in those who areeing treated with anticoagulant drugs. In patientsith soft-tissue or muscular hematomas, the drainage
an relieve the associated symptoms and reduce theime required to heal the lesion.
ndicationsSmall-sized and asymptomatic hematomas do not
equire treatment and they only need a conservativereatment until they are spontaneously reabsorbed.owever, hematomas can sometimes produce symp-
oms such as pain, fever, and malaise. Sometimes theyroduce a mass effect that compresses adjacent struc-ures. In the limbs, this can cause a compartmentyndrome or skin necrosis. In all of these cases, therainage of hematomas can help improve the symp-
IG 8. Muscular abscess in thigh before (A) and after drainage (B). A rebscess recurred twice and elective surgery was scheduled. An infec
IG 9. Drainage of a hematoma in vastus medialis muscle of quadronographic guidance into the collection. (B) After successful drainagatheter was removed after 2 days and patient resumed sporting acti
oms of the patient. Moreover, hematomas can be i
10
nfected quite easily, resulting in the formation ofbscesses. In that case, they should be treated as anyther abscess.
In traumatic hematomas or muscular strains, thehysiological process of healing of muscular lesionsequires the broken fibers to be located in closeroximity but the presence of fluid collections orematomas separates them and prevents the forma-ion of the scar.15 In these situations and especiallyn those resulting from the practice of sports, thevacuation of the hematomas speeds up the healingnd cicatrization process of lesions and reduces theowntime (Fig 9).
ontraindicationsThe drainage of hematomas where active bleeding
ing calcification (arrow) can be seen in the abscess after the drainage.cus of myositis ossificans was removed from the cavity.
in a handball player. (A) A 8-F trocar (arrows) is introduced underhe collection, a catheter can be seen (open arrow) in the cavity. The
3 weeks.
main
icepse of t
s present is absolutely contraindicated and a hema-
Curr Probl Diagn Radiol, September/October 2008

tdspofiam
TH
Tdmm(cctsu2dhrd
cf
M
Qttssrtdn
fpiflr
R
drpd7
dAcett
C
doa
rtIbbfllcaodsscapaa
rrseo
T
C
oma should not be drained in patients with bleedingiatheses due to the risk of bleeding. Occasionally, ithould be deemed necessary to drain a hematoma in aatient where this lesion results from treatment withral dicumarinics. In that case, the hemostasis shouldrst be sufficiently reestablished, and oral dicumarinicnticoagulant treatment should be changed into treat-ent with heparin.
echniqueematomas
he drainage technique of hematomas is similar to thatescribed for abscesses. The contents of the hemato-as can be variable and often fluid collections areixed with clots. Sometimes, large-bore catheters
10-12 F) should be used if the contents are mostlyoagulated. However, and despite the use of largeatheters, they tend to become blocked by clots andherefore drainage of this type of hematoma will not beuccessful unless fibrinolytic substances are used. Wese intracavitary urokinase at a dose of 100,000 to50,000 IU dissolved in 20 to 40 mL saline solution,epending on the volume of the hematoma, every 8ours. We maintain the treatment until the hematomaesolves or no reduction in the collection can beetected in 1 to 3 days.
Hematomas of longer evolution may appear as fluidollections. In these cases, the drainage can be per-ormed simply by puncturing with a needle.4
uscular Strains
uick drainage of fluid collections formed betweenhe broken fibers of a muscular strain will acceleratehe cicatrization process. This is particularly useful inports practitioners who need a quick return to theirporting activity. In these cases, the aim is not toeduce the volume of the hematoma but to speed uphe cicatrization process. These collections can berained using a needle guided by US. An 18- to 20-Geedle is sufficient to drain the liquid.
Punctures can be repeated if new collections areormed. In large lesions where there is an abundantroduction of fluid during the first days after thenjury, a fine catheter (5-6 F) can be useful to drain theuid until the scar is formed, after which it can be
emoved. uurr Probl Diagn Radiol, September/October 2008
esultsIn hematomas treated with the protocol previously
escribed, clinical improvement and the total or partialesolution can be achieved in all patients. In ouratients, drainage has been maintained for 1 to 13ays, with 40% of patients having drainage less than2 hours.
Among the strains, the results obtained in rupturesue to the tearing of the muscular insertion of thechilles tendon (tennis leg) are remarkable. In these
ases, drainage with a catheter for 24 to 72 hoursnables the formation of a scar within that period andhe sporting activity can be restarted within 4 weeks ofhe event, even for serious lesions (Fig 10).
omplicationsThe manipulation of hematomas and the use of
rainage catheters in their management involve a riskf infection. Thus, a prophylactic broad-spectrum oralntibiotic treatment should always be associated.
Another possible complication is bleeding. It is aare complication if the previously described precau-ions are followed in patients with bleeding diatheses.t may become difficult to assess if the fluid drainedelongs to the drainage of the hematoma or to a newleeding. With this in mind, it is useful to observe theuid drained. An old hematoma has a dark color and is
ess viscous, whereas fresh blood has a more intenseolor and tends to clot once outside. It is also useful tossess the change in size of the collection: the volumef liquid drained should correlate with a similarecrease in volume of the hematoma. If not, bleedinghould be suspected. If the presence of bleeding isuspected, the drainage tube should be closed untilonfirmation is obtained as to whether or not there isctive bleeding. Computed tomography and angiogra-hy are useful techniques to evaluate the presence ofctive bleeding and, if needed, to treat it by means ofn embolization.
A partial resolution of a hematoma should not beegarded as a technical failure because the aim is toelieve symptoms and reduce the healing period. Themall residues of hematoma which have not beenvacuated will subsequently be reabsorbed spontane-usly.
reatment of GangliaGanglia are cystic lesions located preferably in the
pper limbs. They are the most frequent soft-tissue
211

ttbeutdrpnpt
I
stit
pr
C
o
T
gDTvTg11
Fw( and
2
umors in hands and wrists, which are the sites wherehey are usually located. They are not true neoplasms,ut cystic spaces with fibrous walls and withoutpithelial lining filled with gelatinous fluid. They aresually asymptomatic and generally do not requirereatment. When treatment is needed, surgery is theefinite treatment, although it has significant recur-ence rates (1-34%). Given its benign nature, manyatients refuse surgery to treat these lesions. Percuta-eous treatment of the ganglia under US guidance canrovide immediate relief to the symptoms and, even-ually, cure them.14,16,17
ndicationsTreatment of ganglia is indicated when they are
ymptomatic. Symptoms observed can be inflamma-ion, compression of nearby structures, or pain result-ng from an increased internal pressure. In these cases,
IG 10. “Tennis leg” in a paddle player. (A) A hematoma can be seenas introduced under sonographic guidance into the collection. (C) T
D) Two weeks later, a scar (arrows) could be seen sealing the strain
he aim of the treatment is to reduce the internal t
12
ressure in the lesion. Occasionally, treatment isequired for cosmetic reasons also.
ontraindicationsThis procedure has no contraindications, except that
f the steroids injected.
echniqueBefore treating these lesions, a thorough sono-
raphic study is required to confirm its fluid nature andoppler is used to confirm that is not a vascular lesion.hen, under US guidance, the needle is slowly ad-anced until the tip reaches the interior of the cavity.he content of the ganglion is extremely dense andelatinous and therefore large-bore needles (14- to8-G) should be used to drain them. We usually use4-G vascular access needles and aspirate the contents
een gastrocnemius and soleus muscles. (B) A 6-F trocar (open arrow)ays later, a scar had formed (arrows) and the catheter was removed.the patient resumed sporting activity.
betwwo d
hrough the catheter of the needle (Fig 11). To com-
Curr Probl Diagn Radiol, September/October 2008

pw
ibbt
R
t
tdmm
C
ccdef
TPtnaatBntcsttttpe
I
cpmgptc
C
Fwsf
C
letely empty the collection, it is useful to wash outith saline solution.The complete treatment of the ganglion requires the
njection of corticosteroids in the lesion. As mentionedefore, various types of corticosteroids and formulas cane used. In this case, we also used a 40 mg solution ofriamcinolone acetate, a long-acting corticosteroid.
esultsThe technique is very effective in the short term, but
IG 11. Treatment of a ganglia. (A) A ganglia can be observed in therist. (B) A vascular access catheter is introduced into the cyst under
onographic guidance. (C) The gelatinous content of the ganglia isully aspirated. Afterwards, 40 mg triamcinolone acetate was injected.
here is a high rate of recurrence (21-60%) and s
urr Probl Diagn Radiol, September/October 2008
herefore in most cases it cannot be considered aefinite treatment but a nonaggressive technique toanage the ganglia. In case of recurrence, the treat-ent can be repeated.
omplicationsLocal skin atrophy following treatment with triam-
inolone, especially when an extravasation of theorticosteroid occurs after the puncture has beenescribed is the main complication of ganglia.14 How-ver, skin atrophy usually resolves spontaneously in aew weeks.
reatment of Popliteal Cystsopliteal or Baker’s cysts are distended bursae within
he popliteal space, particularly of the semimembra-ous-gastricnemius bursa. They are usually caused byn increase in synovial fluid volume and pressuressociated with diverse pathologies of the knee ofraumatic, degenerative, or inflammatory origin.18
aker’s cysts are generally asymptomatic and requireo treatment. However, they may cause symptoms dueo inflammation, rupture, intracystic hemorrhage, in-reased internal pressure, or compression of nearbytructures. These symptoms may be chronic, such ashe presence of a mass in the popliteal space or painhat increases with movement. Sometimes the symp-oms caused by compression of nearby veins mimichrombophlebitis of the leg.19 When symptomatic,ercutaneous treatment under US guidance is veryffective to improvement.
ndicationsTreatment is indicated in patients with acute or
hronic pain or functional limitation caused by aopliteal cyst. Also, in patients with symptoms thatimic deep venous thrombosis caused by rupture or
rowth of a popliteal cyst, decompression should beerformed as soon as possible. The purpose should beo improve local complications produced by the ex-essive growth of the cyst.
ontraindications
Contraindications are related to the use of cortico-
teroids as part of the procedure.213

T
waoorpicbocoe
irdteaa
R
espdfip
iwt
C
tna
popi
ASCtseaatcytad
F4 ars a
2
echniqueThe puncture of the popliteal cysts can be made
ith a similar technique as the one described forrthrocentesis. Generally, we use 18- to 20-G needlesr vascular access catheters (Fig 12). Fluid collectionsutside the cysts produced in the limb as a result of theupture of the popliteal cysts can also be aspirated. Inatients with deep venous thrombosis symptoms, fluids frequently dense and fibrin, septa, or clotted bloodan be found inside the cysts.18 In these cases, largerore needles should be used. When fluid is very denser clotted, we frequently drain the cysts using a trocaratheter and inject urokinase into the cyst, as previ-usly described, to dissolve the clots and facilitatemptying the content.
After draining the cyst, it is advisable to perform anntracystic injection of corticosteroids to avoid recur-ence and treat the chronic symptoms. As previouslyescribed when dealing with the therapeutic arthrocen-esis, different types of corticosteroids can be usedither on their own or in combination with localnesthetics. We usually inject 40 mg triamcinolonecetonide.
esultsTreatment is very effective in the short term,
specially in patients with deep venous thrombosisymptoms. The improvement is immediate and theatient can leave the room and walk with almost noiscomfort. Although recurrence of the cysts is quiterequent, an improvement of the symptoms is achievedn most cases. The treatment can be repeated if new
IG 12. Treatment of a Baker’s cyst. (A) A needle (arrows) is introdu0 mg triamcinolone acetate is injected. The injected substance appe
ainful episodes occur. i
14
In our experience, patients with multiple collectionsn limbs caused by ruptured popliteal cysts and thoseho suffer from inflammatory arthritis are more prone
o have recurrences.
omplicationsCyst recurrence is not a real complication, because
he aim of the procedure is to improve the symptomsot to cure the cyst. Recurrence is relatively frequent,lthough it is often asymptomatic.
In the case of manipulation of the cyst, repeatedrocedures, or use of catheters for its drainage, the riskf infection increases. In these cases, we associaterophylactic treatment with broad spectrum antibiot-cs.
spiration of Calcific Tendinitis in thehoulderalcific tendinitis is the deposit of calcium in the
endons of the rotator cuff, and especially, in theupraspinatus tendon. It can be bilateral. Its pathogen-sis is unknown. Calcifications usually appear indults between 30 and 60 years of age. In general, it isself-limited process in which the calcifications tend
o be reabsorbed and disappear. Reabsorption of thealcifications is observed in 9% of patients after 3ears and in 27% after 10 years.20 However, in 50% ofhe patients, these calcifications cause chronic painnd functional limitation of the shoulder.20,21 Pain andisability caused by calcific tendinitis can be very
to the cyst under sonographic guidance. (B) Once the cyst is empty,s a fluid with echogenic dots filling the cyst (open arrows).
ced in
mportant, especially in episodes of acute exacerba-
Curr Probl Diagn Radiol, September/October 2008

tc
m
tst
Fsac
C
ion. These symptoms can be highly incapacitating andan last for months or years.
Conservative treatment (nonsteroidal anti-inflam-
IG 13. Aspiration of a calcific tendinitis of right supraspinatus tendoonographic monitoring. (B) A 20-G needle (arrows) is directed to thend aspirated and a “liquid hole” appears and progressively replacean be seen settled down in the syringe.
atory drugs, corticosteroids injections, rehabilita- p
urr Probl Diagn Radiol, September/October 2008
ion) has a limited effect. To definitively improvehoulder function and pain, it is necessary to removehe calcifications.22 Among some of the alternatives
) Procedure is performed with the patient seated and with continuousification (asterisk). (C) Once in the calcification, lidocaine is injectedcalcification (open arrow). (D) After finishing the procedure, calcium
n. (Acalc
s the
roposed to surgery, the most used are high-intensity
215

sptct
I
dwrwomrhcog
C
tc
T
cssasvtpfat
caucswidian
Fd
2
hock waves. This treatment is quite effective butainful and requires specific equipment, making thereatment relatively expensive. A simpler and muchheaper alternative is the removal of the calcificationshrough percutaneous aspiration or “lavage.”
ndicationsThe use of percutaneous aspiration of calcific ten-
initis is indicated in symptomatic patients. Thoseithout symptoms or functional limitations do not
equire treatment nor is it necessary to treat thoseherein a perforation of the surface of the tendon hasccurred with the release of calcium to the subacro-ial-subdeltoid bursa. In this case, the spontaneous
esolution process is underway and the puncture willave a limited effect on its natural evolution. Thisondition can be diagnosed when calcium is observedutlining the rotator cuff tendons on shoulder radio-raphs.
ontraindicationsThis procedure itself has no contraindications, only
hose related to the drugs injected (local anesthetics,
IG 14. (A) Calcific tendinitis of supraspinatus tendon before treatmeisappeared and the patient is asymptomatic.
orticosteroids). s
16
echniqueThe technique consists of a “lavage” of the
alcification using a 1% lidocaine solution. Beforetarting, a sonographic exploration of the shoulderhould be performed to identify the calcificationsnd plan the best access path. We place the patienteated with his arm behind his back to enable betterisualization of the rotator cuffs. In rare cases wherehe affected tendon is the subscapular, the arm islaced in external rotation. The technique is per-ormed with the patient seated to keep the syringelways below the calcification to permit the calciumo settle by gravity on the bottom of the syringe.
For the procedure, we use a 20-G 4-cm needleonnected to a syringe filled with lidocaine. Afternesthetizing the skin, the needle is introducednder continuous US guidance aiming for the cal-ification until the tip reaches the subacromial-ubdeltoid bursa. After the bursa is anesthetizedith a small quantity of lidocaine, the needle is
ntroduced through the tendon until the calciumeposit is reached (Fig 13). Once the needle isnside the calcification, it is very important not tottempt initially to aspirate the calcium because theeedle can become obstructed by calcium. Instead,
) One year after US-guided percutaneous aspiration, calcification has
nt. (Btrong pressure must be applied to the syringe
Curr Probl Diagn Radiol, September/October 2008

pstsestwipucplbc
mdci
raaa
R
ttiiid1sn
C
nipd
st
pprh
rpatcuc
CUimtw
ppm
C
lunger with short and repeated impulses until amall quantity of fluid appears inside the calcifica-ion. When injecting fluid initially, the patient mightuffer moderate pain. Releasing the syringe afterach impulse, the liquid tends to flow back into theyringe, dragging the calcium with it, appearing inhe syringe as a cloud. Progressively, a liquid cavityill substitute the calcification. This cavity will
ncrease in size with each injection and reduce whenressure ceases. The procedure should be repeatedntil the lidocaine flows back without draggingalcium. Then, aspiration of the cavity can beerformed to remove residual fluid and calcium. Inarge-sized calcifications, the syringe may have toe changed several times because the liquid turnsompletely cloudy.
Sometimes, particularly in small calcifications, itight not be possible to obtain calcium. However, this
oes not represent a failure of the treatment since thealcification frequently will disappear spontaneouslyn the following weeks.
Before extracting the needle, we inject corticoste-oids in the subacromial-subdeltoid bursa to avoiddhesive capsulitis. We use 40 mg triamcinolonecetonide. Following the procedure, the patient isllowed to move the limb freely.
esultsThe calcifications reduce their density and size in
he radiography, especially in the first month afterreatment, and frequently they even disappear. Clinicalmprovement during the first weeks is usually signif-cant.22-26 Afterwards, resorption of the calcificationss slower. One year after treatment, calcification hasisappeared or is minimal in the majority of cases (Fig4).23 Approximately 70% of our patients have noymptoms at all and another 20% have experienced aotable improvement.
omplicationsThe patient can suffer pain when introducing the
eedle into the tendon and when the fluid is firstnjected into the calcification. In the first days after theuncture, the patient usually experiences moderateiscomfort in the shoulder.25
We have observed fainting spells and even convul-ive reactions in a small number of patients. We think
hat this is due to the position in which we placed oururr Probl Diagn Radiol, September/October 2008
atients (seated and looking toward the person who iserforming the procedure). For this reason, we cur-ently administrate a rapid-acting anxiolytic one-halfour before the procedure.
A significant number of patients have a tempo-ary recurrence of the symptoms 2 months after theuncture. This recurrence can even last for weeks,fter which the pain usually disappears. We thinkhat this may be the result of the inflammatoryhanges produced by the cicatrization of the resid-al cavity formed in the tendon after removing thealcium.
onclusionsltrasound is the simplest and most efficient imag-
ng method to guide intervention procedures in theusculoskeletal system. These procedures are easy
o perform, inexpensive, and available to any unit,hatever its size. Its efficiency rate is very high.The involvement of radiologists in this type of
rocedure is very important, both as a service to theatient and to maintain our position in the use of theusculoskeletal US.
REFERENCES1. Carson BW, Wong A. Ultrasonographic guidance for injec-
tions of local steroids in native hip. J Ultrasound Med1999;18:159-60.
2. Longo JM, Bilbao JI, Barettino MD, et al. Percutaneousvascular and nonvascular puncture under US guidance: Roleof color Doppler imaging. Radiographics 1994;14:959-72.
3. De Smet AA. Ultrasound-guided injections and aspirations ofthe extremities. Semin Roengenol 2004;39:145-54.
4. Cardinal E, Chhem RK, Beauregard C. Ultrasound-guidedinterventional procedures in the musculoskeletal system. Ra-diol Clin North Am 1998;36:597-604.
5. Balint PV, Kane D, Hunter J, et al. Ultrasound guidedversus conventional joint and soft tissue fluid aspiration inrheumatology practice: A pilot study. J Rheumatol 2002;29:2209-13.
6. Raza K, Lee CY, Pilling D, et al. Ultrasound guidance allowsaccurate needle placement and aspiration from small joints inpatients with early inflammatory arthritis. Rheumatology2003;42:976-9.
7. Koski JM. Ultrasound guided injections in rheumatology.J Rheumatol 2000;27:2131-8.
8. Newman JS. Diagnostic and therapeutic injections of the footand ankle. Semin Roengenol 2004;39:85-94.
9. Migliore A, Tormenta S, Martin LS, et al. Open pilot study ofultrasound-guided intra-articular injection of hylan G-F 20(Synvisc) in the treatment of symptomatic hip osteoarthritis.
Clin Rheumatol 2005;24:285-9.217

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
0. Pekkafali MZ, Kiralp MZ, Basekim CC, et al. Sacroiliac jointinjections performed with sonographic guidance. J UltrasoundMed 2003;22:553-9.
1. Naredo E, Cabero F, Beneyto P, et al. A randomized compar-ative study of short term response to blind injections versussonographic-guided injection of corticoisteroids in patientswith painful shoulder. J Rheumatol 2004;31:308-14.
2. Tsai WC, Hsu CC, Chen CP, et al. Plantar fasciitis treated withlocal steroid injection: comparison between sonographic andpalpation guidance. J Clin Ultrasound 2006;34:12-6.
3. Koski JM, Anttila P, Hamalainen M, et al. Hip jointultrasonography: Correlation with intra-articular effusion andsynovitis. Br J Rheumatol 1990;29:189-92.
4. Breidahl WH, Adler RS. Ultrasound-guided injection of gan-glia with coricosteroids. Skeletal Radiol 1996;25:635-8.
5. Van Holsbeeck M, Introcasso JH. Musculoskeletal ultra-sonography. Radiol Clin North Am 1992; 30:907-925.
6. DeFriend DE, Schranz PJ, Silver DA. Ultrasound-guidedaspiration of posterior cruciate ligament ganglion cysts. Skel-etal Radiol 2001;30:411-4.
7. Chiou HJ, Chou YH, Wu JJ, et al. Alternative and effectivetreatment of shoulder ganglion cyst: Ultrasonographicallyguided aspiration. J Ultrasound Med 1999;18:531-535.
8. Labropoulos N, Shifrin DA, Paxinos O. New insights into the
development of popliteal cysts. Br J Surg 2004;91:1313-8.18
9. Handy JR. Popliteal cysts in adults: A review. Semin ArthritisRheum 2001;31:108-18.
0. Speed CA, Hazleman BL. Calcific tendinitis of the shoulder.N Eng J Med 1999;340:1582-4.
1. Hurt G, Baker C. Calcific tendinitis of the shoulder. OrthopClin N Am 2003;34:567-75.
2. Aina R, Cardinal E, Bureau NJ, et al. Calcific shouldertendinitis: Treatment with modified US-guided fine-needletechnique. Radiology 2001;221:455-61.
3. Farin PU, Rasanen H, Jaroma H, et al. Rotator cuffcalcifications: Treatment with ultrasound-guided percutane-ous needle aspiration and lavage. Skeletal Radiol 1996;25:551-4.
4. Farin PU, Jaroma H, Soimakallio S. Rotator cuffcalcifications: Treatment with US-guided technique. Radiol-ogy 1995;195:841-3.
5. Pfister J, Gerber H. Chronic calcifying tendinitis of theshoulder—Therapy by percutaneous needle aspiration andlavage: A prospective open study of 62 shoulders. ClinRheumatol 1997;16:269-74.
6. Bradley M, Bhamra MS, Robson MJ. Ultrasound guidedaspiration of symptomatic supraspinatus calcific deposits. Br J
Radiol 1995;68:716-9.Curr Probl Diagn Radiol, September/October 2008