Embed Size (px)
Citation preview

Biofeedback and Self-Regulation, Vol. 19, No. 4, 1994
Twenty-Five Years of Progress: Twenty-Five More? 1
Frank Andrasik Center for Behavioral Medicine, The University of West Florida
This address outlines important steps for ensuring the future of biofeedback and applied psychophysiology. These steps are contained in the acronym PHUTRE, wherein PH stands for Political activism of the Hard and fast variety, U represents United front, T encompasses Transfer of knowledge (from clinician to researcher, researcher to clinician, and from both to students in training), R refers to our Research base, and E represents the Excitement that our fieM has the potential to generate.
Descriptor Key Words: AAPB, membership; AAPB, future; applied psychophysiology; bio- feedback; cognitive behavior therapy; hypertension; headache, minimal contact treatment; health care, political activism; transfer of knowledge.
Around the time I graduated from Meadowdale High School, in Dayton, Ohio, Drs. Gaarder, Murphy, Brown, and others were meeting to discuss the fascinating topic of voluntary regulation of autonomic functions, which then led to the establishment of the Biofeedback Research Society. I had no idea that 25+ years after retiring as Senior Class President I would be given another chance to preside, especially in an international scientific or- ganization. I must confess, at that time of my life, I had not heard about these new concepts, nor did I much care. I was quite involved with my schooling, sports, and other age- and gender-appropriate activities. In fact, it was not until 1975 that I began to study biofeedback and applied psy-
1This paper is based on the Presidential Address delivered at the annual meeting of AAPB, Atlanta, Georgia, March, 1994. Please address correspondence to Frank Andrasik, Ph.D., Center for Behavioral Medicine, The University of West Florida, 11000 University Parkway, Pensacola, Florida 32514.
311
0363-3586/94/1200-0311507.00/0 © 1994 Plenum Publishing Corporation

312 Andras ik
chophysiology intensely. The excitement I felt back then, however, is just as real today.
When I first sat down to prepare my remarks for this talk, I thought it would be helpful to spend some time reviewing our past. However, since time for this presentation is limited and Dr. Johann Stoyva, who knows this history much better than I, will be addressing this topic, I decided it would be best to leave this material for him. In this text, I want to focus my comments on the paths I believe we need to follow in the years to come in order to ensure that we indeed do have a future.
I have organized my comments around the acronym P H U T R E , with apologies to Mr. Webster and the French. Each letter or letter grouping represents an aspect I believe to be critical to our future and to our con- tinued existence.
P - -POLITICAL ACTIVISM
H- -HARD AND FAST TYPE
It has never been so clear to me as now that our future depends in large part on our success in the political arena. The main concern at the moment is ensuring inclusion in impending national health care legislation. We are told that a bill of some type will arrive at President Clinton's desk in October of this year. "Hard and fast" in the dictionary sense is inter- preted to mean strongly binding. The typical meaning of fast applies as well, as speed of action is crucial.
Participants at the Long-Range Planning Retreat in San Antonio in the Fall of 1992 knew full well the historical significance and the contro- versial side of levying a mandatory assessment to establish a fund restricted for lobbying in the political arena, even though this type of action was not unprecedented. During Past-President Budzynski's term, 1974, approxi- mately $1,200 was donated by members to defeat attempted federal regu- lation of biofeedback devices. Long-Range Planning participants predicted that an immediate 15% drop in membership would result from the special legislative assessment; drop-off was actually something closer to 10%. This is one time when you hope your prediction abilities are inaccurate! Our group, true to its origins, resists external control, viewing this to be the antithesis of what we are all about. Many who did comply with the assess- ment said loudly, "never again"; the 10% of nonrenewing members ap- peared to express their disagreement behaviorally by withdrawing from our society. The Fund for the Future has been judicious in expending the pre- clous dollars raised that year, but a continued cash infusion was still judged

Twenty-Five Years 313
to be necessary. This time contributions were requested on a voluntary ba- sis. Of the approximate 1,200 members who have paid their 1994 dues thus far and who were asked to consider making a voluntary contribution (stu- dents, foreign members, hardship cases, etc. have always been excused), approximately 25% have made a voluntary contribution. The total collected to date amounts to $12,267.00; the per capita amount averages about $38.00, which is very close to the per capita amount generated by the 1993 mandatory assessment. Thus, a sizable minority continue to see merit in pursuing a political course and behaviorally support the notion at a similar level.
Once the special legislative assessment became a reality, I placed a number of calls to sister organizations, those with a size and mission similar to ours. Most had not considered such an approach. A few had given it consideration, but were not yet ready to commit. Nearly all applauded our courage.
While the 58+ thousand dollars raised in 1993 may seem sizable from some perspectives, it is a mere drop in the bucket for a concerted national lobbying program. With so little ammunition and so many targets we knew we had to select wisely and to take a steady aim. The fall board meeting last year was scheduled in Washington, DC so that a lobbying trip could be made to the hill and expenses economized. I had never participated in such an event and must confess that I looked to the day with a healthy level of skepticism. I now confess that it proved to be a rewarding, educa- tional, and actually enjoyable experience. Senior health care aides were our primary targets and they had many constituents competing for their time. A message has to be clear and focused to be effective in this type of situ- ation; ours was. The "addicting" side of politics became evident as I found myself experiencing adrenaline surges throughout the visit. By day's end, I was more convinced than ever that this new mode of behavior is something we must continue. Leaders in organizations similar in scope and mission have begun to praise our efforts. Some political types have even gone so far as to state that our approach could weil serve as a model for o ther similar organizations.
Through the efforts of members of the Fund for the Future and our Legislative committee, our in-house legislative intern, and special volun- teers, we were able to arrange a presentation to the Technical Advisory Committee of the Health Care Finance Agency (HCFA) just a few days prior to the annual meeting. This is a first in the 25-year history of AAPB and is a significant milestone for us. Dr. Keith Sedlacek, our selected spokesperson, reported that the presentation went weil indeed. This politi- cal activism on our part has opened a previously closed door.

314 A n d r a s i k
A common criticism of the Fund for the Future has been that our membership numbers and bank account statement are too small to even bother with a political agenda. To that, I say firmly: Our accomplishments argue otherwise. CHAMPUS coverage has been expanded, some changes favorable to biofeedback have been made in the CPT code manual, pro- gress has been made with HCFA, and the door has been opened to 60+ congressional offices. My economics professor would proclaim that this was a good bang for the buck!
At the start of the conference we were provided a commemorative yearbook that includes statements from all past presidents. In reading the histories submitted by the Past-Presidents it is learned that in nearly every year something happens that, even if not emanating from political forces, has strong political implications. Thus, I was not surprised when a summer issue of the Annals of Internal Medicine published a metaanalysis that did not speak favorably about cognitive behavior therapy (which included analy- sis of biofeedback) for management of essential hypertension. However, I was somewhat surprised when the rebuttal I submitted as President of AAPB was rejected by the Editor without comment. I believe this rebuttal deserves to be archived, and I present it here. 2 From the text of this letter, I quote:
Reconsideration of Eisenberg et al. (1993)
Being someone who is favorably disposed to alternative approaches to medical problems, I was disappointed to read the report by Eisenberg, Delbanco, Berkey, Kaptchuk, Kupelnick, Kuhl, and Chalmers (1993) in the June issue of Annals of Internal Medicine. Upon careful study of this report and the two quantitative analyses of pharmacological treatment referenced by these authors (Collins, Peto, MacMahon, Hebert, Fiebach, Eberlein, Godwin, Qizilbash, Taylor, & Henneckens, 1990; MacMahon, Peto, Cutler, Collins, Sorlie, Neaton, Abbott, Godwin, Dyer, & Stamler, 1990) and used as a base of comparison for the cognitive behavioral treatments reviewed, I arrived at somewhat different conclusions.
The main findings of Eisenberg et al., for purposes of this discussion, were that (a) cognitive behavioral treatments (CBT) for hypertension produced statistically significant reductions in both DP and SP (9.0 and 13.4 mm Hg, respectively) relative to wait-list or no-treatment conditions when baseline BP was assessed during a single session; (b) these differences were much smaller in magnitude and not statistically significant when baseline BP was based on readings collected over multiple sessions (4.0 and 4.1 mm Hg, respectively); (c) CBT for hypertension was not statistically significant from attention-placebo for either method of determining baseline BP (differences of 4.5 and 6.5 mm Hg for single session BL and 1.3 and 2.8 for multiple session BL); and (d) these effects did not rival those for similar statistical analyses conducted for randomized controlled trials of pharrnacotherapy
2A reporter for a national magazine who was preparing an article about the findings and implications of Eisenberg et al. recognized the need for a counter view and phoned me as President of AAPB to obtain this information.

Twenty-Five Years 315
versus p lacebo (mean DP reduc t ions of 5-6 mm Hg) (Coll ins et al., 1990; MacMahon et al., 1990).
First, as best I can determine, the BP reductions mentioned in (d) above were based on studies using single-session BP values. Comparison of these medication effects must be limited to the like data sets from Eisenberg et al., which does not always seem to be the case in the manuscript. BP reductions for CBT compare very favorably to those for medication when conducted on a level playing field. In fact, reductions for all comparisons except CBT versus placebo for multiple session BL seem to rival or surpass the effects reported for the medication analyses. Thus, for like comparisons and even for one unlike comparison (single-session BL for medication versus multiple session BL for CBT) CBT appears to hold its own.
Second, it is reported by Eisenberg et al. that approximately 85% of all patients in the CBT trials were concurrently receiving antihypertensive medication and it can be assumed that a great deal of BP lowering had already taken effect. We know by the law of initial values that starting points have a large bearing on the subsequent amount of change that is possible (Wilder, 1967). The lower the BP at the start of the study, the lower the likelihood of it changing substantially. Also, in light of the large number of patients taking concurrent medication, comparison (a) ment ioned above seems more appropriately viewed as "medicat ion" versus 'med ica t ion plus CBT," rather than wait-list/no t reatment versus CBT. When judged from this standpoint, the incremental reductions beyond effects due to medication alone seem rather sizable. Eisenberg et al.'s conclusion that "data from our metaanalysis suggest that cognitive interventions alone are not capable of blood pressure reductions of this magnitude" (p. 969) [in reference to a medication effect of 5-6 mm Hg for DP] does not seem supported.
Third, it is accepted that attrition is high in investigations of medication alone. Attrition was low on average for the CBT trials (mean approximately 10%). It does not appear that any of the a forement ioned analyses took dropouts into account ( incorpora t ion of end-poin t analysis). The h igher expec ted rate of attrition in studies of medication alone could bias outcomes in favor of these medication studies.
Fourth, one potential outcome of CBT is that it can lessen the need for concurrent medication (Glasgow, Engel, & D'Lugoff, 1989). Would anyone argue that it is not significant if, upon a successful course of CBT, medication can be safely reduced with no rise in BP? Analysis of BP alone would not reveal this important clinical effect.
Fifth, treatment in the medication studies was prolonged, intensive, and aggressive (spanning many years and involving up to three lines of medication). The mean duration of CBT was just over 2 months, which is hardly a similar dose of treatment. A study of CBT (uncontrolled, and therefore not included in Eisenberg et al.) that treated patients more aggressively to ensure that they achieved target training goals (similar to titrating medications until the desirable blood level is achieved) produced highly significant medication and BP reductions that endured (Fahrion, Norris, Green, Green, & Snarr, 1986).
In summary, it seems premature to accept the conclusions of Eisenberg et al. I would argue that CBT for hypertension continues to hold promise and merits additional rigorous, intensive study. 3
3A more recent meta-analysis (Linden & Chambers, 1994), directly comparing pharmacological and psychological treatments, found BP reductions were of a similar magnitude when adjustments were made for baseline differences.

316 A n d r a s i k
Again, it was a major disappointment that we were not allowed to defend ourselves in the court where we were being tried.
U - - U N I T E D FRONT
In a few moments Past-President Stoyva will discuss some of the forces that have served to distract us from our mission and to drive us apart these past 25 years. It is time, it has to be time, to put aside our differences and pick up the olive branch. While Political Activism is the key to the door, strength and unity are needed to ensure that our passage through the doorway is noticed.
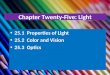
AAPB Membership Figures
2400
2200
2000
1800
~ 1600
1400
1200
1000
78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93
Year
Fig. 1. Total number of members of AAPB for each year from 1978 through 1993.

Twenty-Five Years 317
Our membership has fluctuated over the years, with a precipitous drop coincident with initiation of the mandatory assessment. Data for 1978, the most distant year with complete and accurate membership records, re- vealed our member base to be 1,790. Preceding years were smaller. It took us about 20 years to reach our peak membership, but just a few short years to fall back to the membership levels of the late 1970s (see Figure 1). It is important to note that this downturn in membership base was in evidence prior to enactment of the special legislative assessment. Other possible con- tributions to this downturn in membership were immediately evident to me upon assuming the Presidency, for it was at this time that I began to hear, loudly and clearly, complaints from certain segments of our membership that AAPB was becoming closed-minded and not the comfortable, accept- ing home it once was.
At a recent workshop presented by one of the pioneers of brief ther- apy, Simon H. Budman (1994) reminded a t tendees of the concept of "lock-in" and how it can have a strong influence on behavior. He re- counted several poignant examples of lock-in, three of which are shared here.
The first concerns the competition between the beta and VHS video formats. It is clear that VHS is the victor; does anyone admit to having a beta camera or player? Was VHS selected because it was clearly superior? Most would say no. A second example of lock-in concerns the design of the computer/typewriter keyboard, on which I prepared this address. Re- member that when the keyboard was originally laid out, typewriters were of the manual variety and the quicker typists could easily jam the typing elements. The keyboard was purposely designed to slow down the fastest typist in order to prevent the keys from locking in place. This slowed down keyboard is the one we continue to use today. Is it the best keyboard lay- out? A third example concerns many of our notions about delivery of clini- cal services; the once-a-week 50-minute hour, the prescription to practice X amount per day, and the like. Research addressing such locked-in as- sumptions is not abundant. I will return to the clinical examples of lock-in later.
How does this apply to us? I believe our organization is experienc- ing lock-in phenomena in various ways today. One notable example is the area of E E G research and application. Some may say perhaps the p roper term for what is going on here is "lock-out." We have t ended to lock-in certain applications as legitimate and to discount or lock-out oth- ers too quickly. We are guilty of similar lock-in and lock-out p h e n o m e n a concerning E M G research and application. Few doubt the value of E M G conditioning as an aid to general relaxation, but the lock p h e n o m e n a be- gin to surface when the focus is expanded to o the r appl icat ions and

318 Andrasik
claims. The board of AAPB acknowledges the legitimacy of concerns from our disenfranchised segments and is taking important steps to ad- dress this very aspect at the 1994 annual meeting. We must find ways to become more inclusive, ra ther than exclusive, and then never forget its importance. Recalling our history, I find this present divisiveness some- what puzzling. Remember , this is the group where sober university and medical scientists brushed elbows with those wearing flowing white robes and beads at the early meetings. Are we still divergent in our views, or have we become less tolerant?
I am reminded of the writing of Shunryu Suzuki, who in the text, Zen Mind, Beginner's Mind (1970), stated: "In the beginner's mind there are many possibilities, but in the expert's there are few." Perhaps we need to "regress," if you will, to our past when we were less expert but still mindful of Past-President Neal Miller's admonition to be bold in what we attempt, but cautious in what we claim.
T- -TRANSFER OF KNOWLEDGE
I am convinced that we have better mousetraps in many areas of ap- plication. Yet, we all know some inventors whose closets are filled with these new and improved mousetraps. We have to find ways to let individu- als know of our better mousetraps, a process that I have termed Transfer of Knowledge. This transfer must take place both within and outside our ranks. Knowledge must be t ransferred internally from clinician to re- searcher, from researcher to clinician, and from both to the students who will follow in our tracks. Past-President Green (1994) aptly pointed out in his yearbook statement why knowledge must be transferred from clinician to researcher:
A striking change in the Biofeedback Research Society began in the mid-1970s and came to fruition about the time of my year of service. Therapists interested in biofeedback formed an Applications Division. This was a great step forward for the Biofeedback Society of America, not only for clinicians, but also for researchers. This may sound contradictory, but I've noticed that the best clinicians are also the best observers of human experience. As a result, they of ten get remarkable "unexplainable" results that are useful as germinal material in designing research studies. Researchers who have clinician friends, or who do clinical work themselves, often find that clinical findings can focus research investigations into productive channels.
Bridging the gap between research and practice is another internal transfer issue that must be resolved, and thankfully some authors are be- ginning to address this thorny issue (Barlow, Hayes, & Nelson, 1984). AAPB has long recognized the importance of nurturing its students. I am

Twenty-Five Years 319
convinced that we do more for students than any other professional society, but we must not rest on this laurel.
Finally, our knowledge has to be transferred to those outside our ranks---to non-AAPB professionals, to potential consumers who need our services, and to funding gatekeepers. Some members cautioned it would be unwise to mention marketing in my address. Marketing is not and does not need to be a four-letter word, especially when the product is legitimate. We can learn much from our colleagues with experience in this area (Frederiksen, Solomon, & Brehony, 1984; Schulz, 1993). Some of these functions have begun through our political activism, but much, much more needs to be accomplished.
R--RESEARCH BASE
The empirical data we have deposited in the bank are our main source of currency in the scientific and political marketplace. Regulatory agencies and governing bodies have made it painfully clear that large- scale clinical trials are given the highest dollar value. This is why it is especially significant that such a trial sponsored by AAPB and prepared by Drs. Richard Scherman, John Arena, Ed Blanchard, Doug Degood, Alan Glaros, Steve Wolf, and myself received approval for funding by the newly created Office of Alternative Medicine at the National Insti- tutes of Health (NIH). Although others within our ranks were successful with their applications too (Drs. Douglas DeGood, Steve Fahrion, and Angele McGrady), this is the first large-scale AAPB-initiated research project that extends data collection into "real world," actual clinical set- tings. This was a dream shared by Past-Presidents Miller and Schwartz. It is my hope and expectation that this study will be just the first of many to come.
I believe it may be instructive to examine select areas where demon- strable progress has been made. It is clear that significant inroads have been made in several areas, with muscle rehabilitation, incontinence, Ray- naud's, and phantom limb pain serving as the better examples. In fact, these areas should serve as models for ways to conduct programmatic research. It strikes me that it is no accident that research has progressed to a higher level in these areas. Why is the progress so solid here? First, researchers have devoted considerable time to investigating the biopsychosocial deter- minants of these disorders. It has always interested me how the number of treatment outcome investigations tends to far exceed the number of as- sessment investigations. How is it, or rather why is it, that treatment tends to outpace assessment? An obvious answer is that clients need to be treated

320 Andrasik
and cannot and will not wait until all assessment parameters are defined. However, we must redouble our efforts to gain bet ter understanding of the disorders we treat.
Second, there is something about these disorders that has seemed to capture the interest of some of our most talented researchers. This is due in part to the complexity of these disorders, the complexity of the required instrumentation, and the extensive knowledge required just to enter the arena. This is not meant in any way to discount the expertise of researchers in other areas. The best within our ranks may be found in every area of application. The concentration of our best seems most dense in these areas. Study of research progression in these areas would be instructive to all. 4
Earl ier I ment ioned how lock-in p h e n o m e n a have influenced our clinical practice, too. Managed care demands that we reexamine our clinical assumptions and subject them to empirical scrutiny. An important area of research has to be evaluation of alternative ways to deliver our treatments, and that in fact is one of the main thrusts that has continued in our re- search. With the exception of very specialized applications, the world simply will not long buy t reatments that require frequent, intensive, one-on-one sessions for protracted periods. Dr. Anderson Rowan and I (Rowan & An- drasik, 1993) recently completed a review of studies employing reduced therapist contact in the t reatment of recurrent headache disorders. The typical reduced therapist contact t reatment involves from 3 to 5 face-to-face sessions with a therapist and supplements the limited number of t reatments by providing clients written and audio instructional materials. It might sur- prise you to realize that we were able to iocate 23 published investigations of the effectiveness of reduced therapist contact self-regulatory t reatments for adult and pediatric headache. It may surprise you further to learn, that with few exceptions, reduced contact approaches were equivalent in effec- tiveness to the more intensive, in-office t reatments . Similar research is needed in other areas of application.
E- - -EXCITEMENT
Dr. Harold Varmus, the new Director of the National Institutes of Heal th and therefore one of the most powerful figures in science, recently provided this commentary on the behavioral sciences:
4Headache, an area near and dear to this author's heart, is also one where we have made significant advances. However, it has been omitted from the examples mentioned here because of the fundamental controversies about the nature of the disorder itself (see the presentation by Edmeads, 1994, at the conference) and uncertainty about mechanisms mediating effectiveness.

Twenty-Five Years 321
g~ õ
J
J
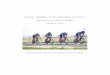
Fig. 2. Number of published articles on biofeedback for each year from 1974 through 1993 as indexed in PsychLit and Medline.
I begin with the premise that behavior is an incredibly important element in medicine. People's habits, their willingness to quit smoking, their willingness to take steps to avoid transmission of HIV are all behavioral questions. But what l'm looking for are new ideas, real discoveries. When I read about genetics, I see breakthroughs every day. And while I'm trying to learn more about behavioral science, I must say that I don't feel I get tremendous intellectual stimulation from most of the things I read. (New York Times, November 23, 1993)
I be l ieve tha t r e sea rch in b i o f e e d b a c k and a pp l i e d p sychophys io logy
can p rov ide tha t exc i t emen t and that the expans ion poss ib i l i t ies a r e a l r e a d y
evident . E x a m i n a t i o n o f addresses by p a s t - p r e s i d e n t s c lear ly po in t s o u t the
exci t ing r e sea rch pa ths to the fu ture , so t h e r e is no n e e d to r e e x a m i n e t h e m here .
I used to sha re the grave conce rns expres sed by m e m b e r s w h o la- m e n t e d ou r e rod ing da t a base and loss o f r e s e a r c h e r s f rom the o r g a n i z a -
t ion. Th is conce rn is still p resen t , bu t is l e s s e n e d in intensi ty . T h e r e is
s imply too much t a len t and c o m m i t m e n t for this to h a p p e n . W h a t c o n c e r n s
me m o r e is ensur ing tha t individuals and agenc ies ou t s ide A A P B b e c o m e k n o w l e d g e a b l e of wha t we do. T rans fe r and d i s semina t ion o f this knowl - edge is the i m m e d i a t e task.

Andrasik
322
~tlr~~~ QI ~ t~t~ti
Sl
~ear
Fig. 3. Total number of doctoral disserta~ä°ns on bio[eedback for each year [rom 1971 through 1991.
ublished books wholly or sig- I~i~ 4 Total number o[.p abac k for each year from - ~';" "ntl-' devoted to 131otcw,~ 1oo3
mt~ca ~ 1971 througn ,~~ •

Twenty-Five Years 323
SUMMARY
We have two basic choices before us. The first is simply to conduct business as usual. If we choose this course we may weil survive for another 25 years, but I do not see how we can survive weil. Data we have recently summarized (modeled after the earlier reports prepared by Hatch & Saito, 1990; Shirakura, Saito, Tsuru, Iga, Tsutsumi, Yamamoto, Hiraki, Iwasaki, & Kobayashi, 1992) clearly point to the declining impact of biofeedback. Note the precipitous declines in the total number of biofeedback articles published irrespective of the data base searched (Figure 2), the decline in doctoral dissertation research on biofeedback (Figure 3), and the decline in the number of books devoted wholly or significantly to biofeedback (Fig- ure 4). Mere survival, however, should not be acceptable to us. It goes against our very fabric. We must, and I am confident we will, set our sights much higher. By doing this, our future truly will be so bright that we taust put on shades. 5
Thank you for allowing me to serve you this past year and to address you at the 1994 twenty-fifth anniversary conference.
REFERENCES
Barlow, D. H., Hayes, S. C., & Nelson, R. O. (1984). The scientist practitioner: Research and aecountabiliO~ in elinieal and educational settings. New York: Pergamon.
Budman, S. H. (1994, January). Brief therapy in action: A practical model of treatment for the 1990s and beyond. Gulf Breeze, FL.
Collins, R., Peto, R., MaeMahon, S., Hebert, P., Fiebach, N. H., Eberlein, K. A., Godwin, J., Qizilbash, N., Taylor, J. O., & Hennekens, C. H., (1990). Blood pressure, stroke, and coronary heart disease. Part 2. Short-term reduetions in blood pressure: Overview of randomized drug trials in their epidemiological context. Lancet, 335, 827-838.
Edmeads, J. (1994, March). Mechanisms ofheadpain. Invited address presented at the annual meeting of the Association for Applied Psychophysiology and Biofeedback, Atlanta, Georgia.
Eisenberg, D. M., Delbanco, T. L., Berkey, C. S., Kaptchuk, T. J., Kupelnick, B., Kuhl, J., & Chalmers, T. C. (1993). Cognitive behavioral techniques for hypertension: Are they effective? Annals of lnternal Medicine, 118, 964-972.
Fahrion, S., Norris, P., Green, A., Green, E., & Snarr, C. (1986). Biobehavioral treatment of essential hypertension: A group outcome study. Biofeedback and Self-Regulation, 11, 257-277.
Frederiksen, L. W., Solomon, L. J., & Brehony, K. A. (1984). Marketing health behavior: Principles, techniques, and applications, New York: Plenum.
Glasgow, M. S., Engel, B. T., & D'Lugoff, B. C. (1989). A controlled study of a standardized behavioral stepped treatment for hypertension. Psychosomatic Medicine, 51, 10-26.
Green, E. (1994). President, 1978-1979. Twenty-fifth anniversary yearbook. Wheat Ridge, CO: Association for Applied Psychophysiology and Biofeedback.
5At this point, the presenter donned a pair of sunglasses and concluded his talk.

324 Andrasik
Hatch, J. P., & Salto, I. (1990). Growth and development of biofeedback: A bibliographic update. Biofeedback and Self-Regulation, 15, 37-46.
Linden, W., & Chambers, L. (1994). Clinical effectiveness of non-drug treatment for hypertension: A meta-analysis. Annals of Behavioral Medicine, 16, 35-45.
MacMahon, S., Peto, R., Cutler, J., Collins, R., Sorlie, P., Neaton, J., Abbott, R., Godwin., J., Dyer, A., & Stamler, J. (1990). Blood pressure, stroke, and coronary heart disease. Part 1. Prolonged differences in blood pressure: Prospective observational studies corrected for the regression dilution bias. Lancet, 335, 765-774.
Rowan, A. B., & Andrasik, F. (1993). Efficacy and cost-effectiveness of minimal therapist contact treatments of chronic headaches: A literature review. Manuscript submitted for publication.
Schulz, R. A. (1993, November). New directions in promoting health care and performance. Presented at the applied psychophysiology and biofeedback conference, Banff, Alberta, Canada.
Shirakura, K., Salto, I., Tsuru, T., Iga, T., Tsutsumi, Y., Yamamoto, K., Hiraki, K., Iwasaki, T., & Kobayashi, S. (1992). In K. Shirakura, I. Saito, & S. Tsutsui (Eds.), Current biofeedback research in Japan (pp. 7-14). Tokyo: Shinkoh Igaku Shuppan.
Suzuki, S. (1970). Zen mind, beginner's mind. New York: John Weatherhill. Wilder, J. (1967). Stimulus and response: The law of initial value. Bristol: J. Wright.