Embed Size (px)
Citation preview
TUMOUR MARKERS

What is a tumour marker? Almost anything that forms part of a malignant cell or that is produced by that cell may, in certain situations, be useful as a tumour marker: • structural molecules • secretion products and enzymes • non-specific markers of cell turnover ALL HAVE COUNTERPARTS IN NON-MALIGNANT CELLS
How do we use tumour markers? • Screening/early detection • Diagnosis/case finding • Staging/prognosis • Detecting recurrence • Monitoring therapy
What are the characteristics of an ideal tumour marker?
• Detectable only if tumour is present • Identifies the type of tumour • Circulating concentration correlates with the mass of tumour present • Responds rapidly to treatment-induced remission • Responds rapidly to relapse • Should predict outcome • In patients with stable disease
Carcinoembryonic antigen (CEA)
• CEA is a highly glycosylated cell surface glycoprotein involved in intercellular adhesion • CEA is shed from the cell surface into the circulation and can be detected in serum. • It is thought that infiltrating tumour growth breaks down the normal barriers that usually prevent CEA from entering the circulation.
Malignancies associated with elevated CEA levels
Over-expressed primarily by adenocarcinomas: Colon Rectum Breast Lung
Benign conditions associated with elevated CEA levels Pulmonary emphysema Bronchitis Acute ulcerative colitis Rectal polyps Hepatitis Alcoholic cirrhosis Obstructive jaundice Smokers Renal disease

CEA Normal range: <5ng/ml Smokers: <10ng/ml Suspect malignancy at >20ng/ml Suspect metastatic spread at >50ng/ml T1/2: 3 days (1-5 days)
Dukes’ Grade % patients CEA >5ng/ml A 4 B 26 C 44 D 65

Cancer Antigen 125 (CA125)
Glycoprotein, with unknown biological function Marker developed through immunization of mice with cells from an ovarian carcinoma line, to produce the OC 125 monoclonal antibody
Epithelial cells • Fallopian tubes • Endometrium • Endocervix • Normal ovary
Mesothelial cells • Pleura • Pericardium • Peritoneum
‘Normal’ serum concentration: <35 kU/L Elevated in menstruation T1/2: 5 days (1-5 days)
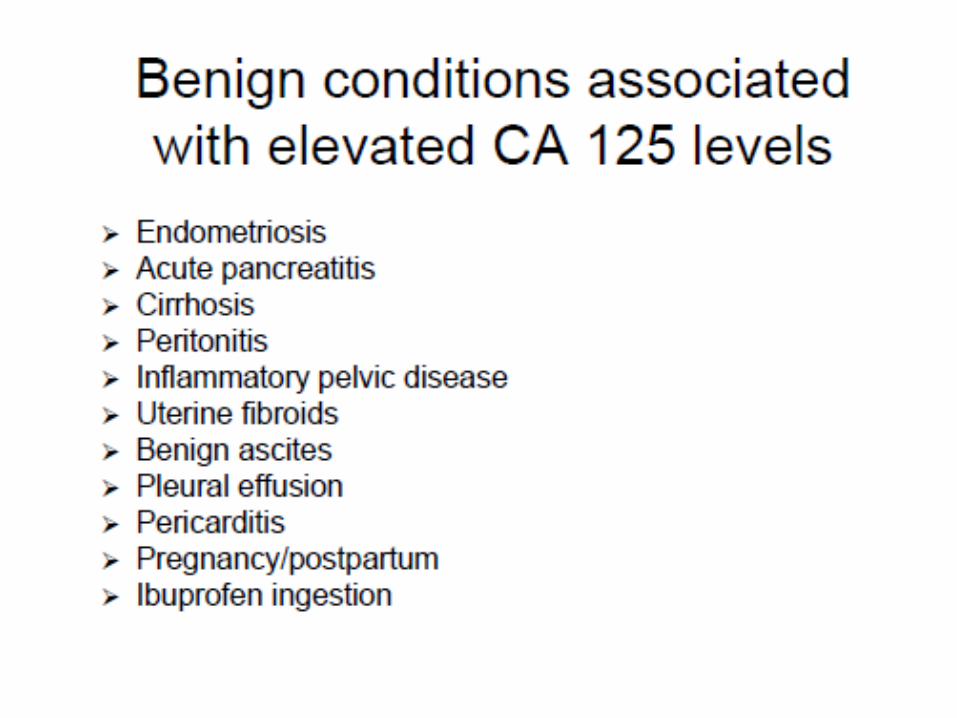
CA125
Malignancies associated with elevated CA 125 80-85% ovarian serous adenocarcinomas 50% Stage I >90% Stage II Breast Cervix Endometrium Uterus Fallopian tubes Liver Biliary tract Stomach Colon Pancreas Lung

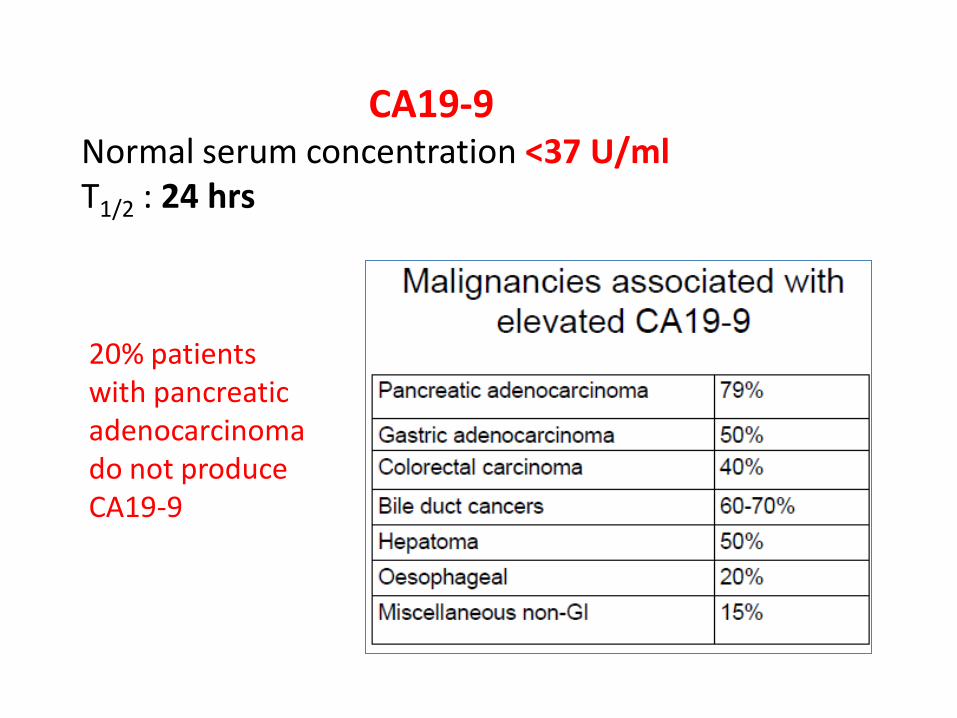
CA19-9 Normal serum concentration <37 U/ml T1/2 : 24 hrs
20% patients with pancreatic adenocarcinoma do not produce CA19-9


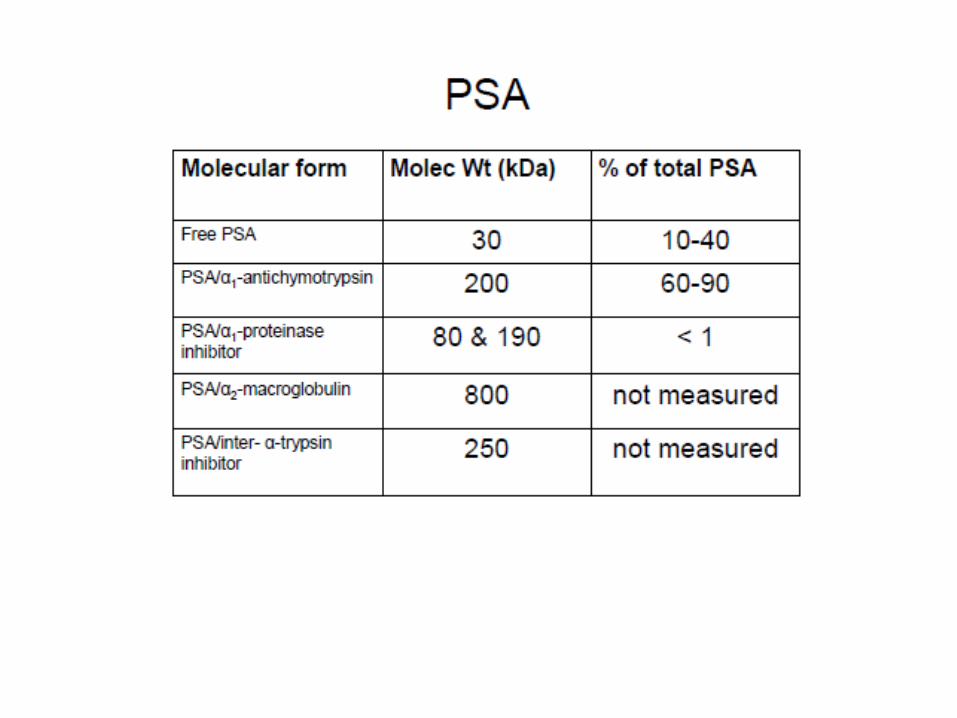
Prostatic Specific Antigen (PSA)
Serine protease Liquefy seminal coagulum Production is androgen-dependent Produced almost exclusively by epithelial component of prostate gland Raised in: Benign prostatic hypertrophy Acute and chronic prostatitis Urinary retention
T½ = 2.5 days (radical prostatectomy)




Alpha–fetoprotein (AFP)
Glycoprotein Performs some of the functions of albumin in the foetal circulation Adult normal values <10 U/L T1/2 = 5 days
Physiological conditions with elevated AFP
Pregnancy Age <1 year (adult levels achieved between 6 months and 1 year)



Human Chorionic Gonadotropin (βhCG)
Multiple forms in serum (intact heterodimer, free alpha, free beta chains, various degradation products) Function is to maintain progesterone production during first 2 weeks of pregnancy Reference: <5 U/L T1/2 = 16-24 hours May be biphasic, second T1/2 = 12.8 days Elevated βhCG: Physiological condition: pregnancy Benign condition: pituitary adenoma Malignancies:
Gestational trophoblastic disease NSGCT SGCT testis (20%)

Serum Tumour Markers - Summary
• Tumour markers can contribute to patient management but be aware of their limitations
• The main application of tumour markers is in monitoring of disease response to treatment
• Measurement of α-fetoprotein and human chorionic gonadotrophin is mandatory in the management of germ cell tumours
• Carcinoembryonic antigen (CEA) is recommended for postoperative follow-up of patients with stage II and III colorectal cancer

Serum Tumour Markers - Summary
• Prostate specific antigen (PSA) may be used for detecting disease recurrence and monitoring treatment in patients with prostate cancer
• In some high risk patients, measurement of α-fetoprotein, CA125, or CA19-9 may aid early detection of primary liver (hepatocellular) cancer, ovarian cancer, or pancreatic cancer respectively
• Opportunistic screening with panels of tumour markers is not helpful
• Measurement of CA125 in men or PSA in women is inappropriate






























