Embed Size (px)
Citation preview

Case report
Tumor seeding of the jejunostomy site after transhiatal esophagectomyfor esophageal carcinoma
N. Y. Hsu1, T. Y. Lin2, C. T. Hsu2, P. P. Tsai3
Division of Chest Surgery, Departments of 1Surgery, 2Pathology, and 3Radiology, China Medical CollegeHospital, Taichung, Taiwan, Republic of China
SUMMARY. A 65-year-old male patient with squamous cell carcinoma of the esophagus had a transhiatalesophagectomy after a prophylactic tube jejunostomy. The tube was removed 3 weeks after surgery. Ten monthslater, a painless 2-cm abdominal mass was noted at the previous jejunostomy site. Subsequent segmental resectionof the jejunum disclosed metastatic squamous cell carcinoma of the esophagus. It is possible that tumor seeding maydevelop at the jejunostomy site after transhiatal esophagectomy for esophageal carcinoma.
INTRODUCTION
Transhiatal esophagectomy (THE) has been advo-cated as an alternative to the classic transthoracicapproach for either benign or malignant disease andis a safe, well-tolerated operation if performed withcare and for the proper indications.1,2 Although anoverview of intraoperative and post-operative com-plications of THE has been presented,3 tumor seedingat the jejunostomy site after THE for esophagealcarcinoma has never been reported; to the best of ourknowledge, this is the ®rst reported case.
CASE REPORT
A 65-year-old male patient was admitted with a6-month history of progressive dysphagia whenswallowing bulky food. Upper gastrointestinalradiographs with barium contrast revealed a 3-cmulcerative tumor in the lower third of the esoph-agus, and a diagnosis of squamous cell carcinomawas made from a subsequently obtained esophago-scopic biopsy specimen. THE was performedthrough midline laparotomy, and reconstructionwith the gastric tube through the retrosternal route
was completed after a cervical esophagogastros-tomy was carried out. In addition, a prophylactictube jejunostomy (using an 18F catheter) wasconstructed at the left upper abdominal site by astandard Stamm procedure. Squamous cell carcino-ma of the esophagus was identi®ed in the resectedspecimen. Pathologic review showed moderatelydi�erentiated squamous cell carcinoma with inva-sion to the deep muscular layer of the esophagus.The patient had an uneventful post-operativecourse. Because the patient's oral intake provedadequate, the feeding tube was removed at a post-operative visit 3 weeks later.
However, the patient returned 10 months latercomplaining of a painless abdominal mass on theprevious jejunostomy wound site. An examinationshowed it was 2 ´ 2 cm with a hard consistency andwas ®xed below the abdominal wall.
The patient denied nausea, vomiting, change inbowel habits or weight loss over the last 10 months.Physical examination was normal except for theabdominal mass. The esophagogram revealed a patentanastomotic site and an intact gastric tubemucosa. Anabdominal computed tomographic scan demonstrateda ®lling defect in the lumen of the jejunostomy withextension and invasion into the abdominal wall(Fig. 1). No abdominal adenopathy was seen. Anexploratory laparotomy was performed, and a tumorarising from the jejunum lumen around the jejunos-tomy site and ®xed to the abdominal wall was found.Subsequent en bloc resection including the tumor-bearing segment of the jejunum and a portion of
Address correspondence to: N. Y. Hsu, Division of Chest Surgery,Department of Surgery, China Medical College Hospital, No. 2,Yuh-Der Road, Taichung, Taiwan, Republic of China.Tel: (+886) 4 2052121 ext. 1974; Fax: (+886) 4 202 9083;e-mail: [email protected]
157
Diseases of the Esophagus (1999) 12, 157±159Ó 1999 ISDE/Blackwell Science Asia
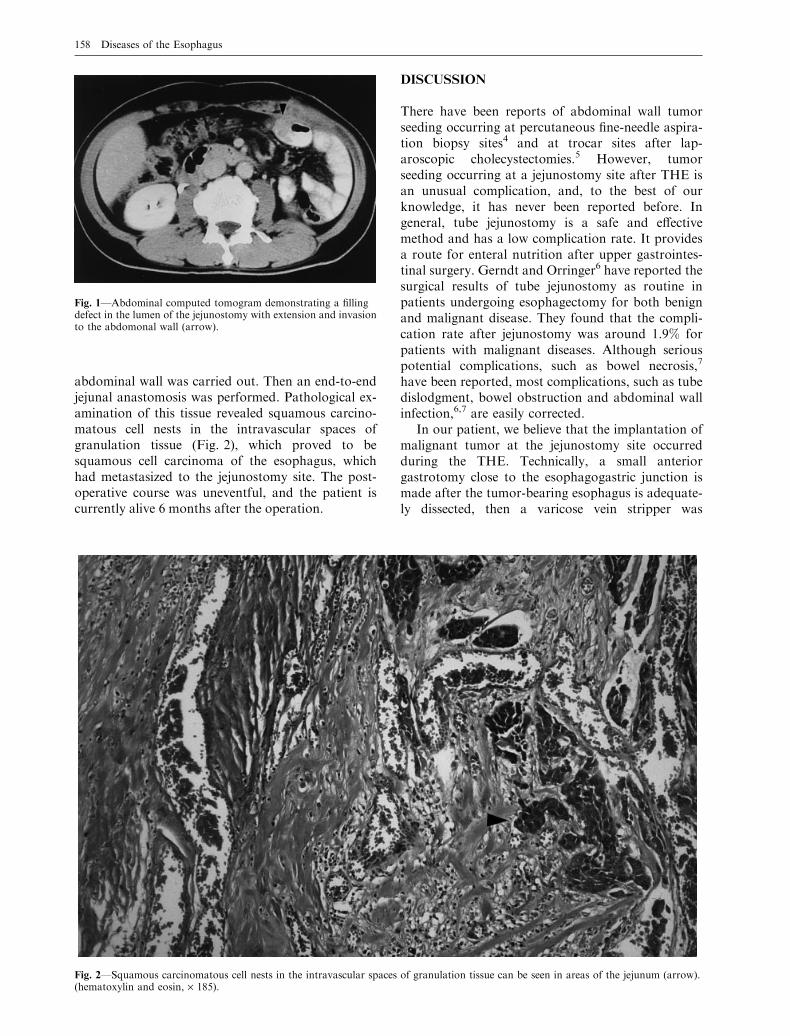
abdominal wall was carried out. Then an end-to-endjejunal anastomosis was performed. Pathological ex-amination of this tissue revealed squamous carcino-matous cell nests in the intravascular spaces ofgranulation tissue (Fig. 2), which proved to besquamous cell carcinoma of the esophagus, whichhad metastasized to the jejunostomy site. The post-operative course was uneventful, and the patient iscurrently alive 6 months after the operation.
DISCUSSION
There have been reports of abdominal wall tumorseeding occurring at percutaneous ®ne-needle aspira-tion biopsy sites4 and at trocar sites after lap-aroscopic cholecystectomies.5 However, tumorseeding occurring at a jejunostomy site after THE isan unusual complication, and, to the best of ourknowledge, it has never been reported before. Ingeneral, tube jejunostomy is a safe and e�ectivemethod and has a low complication rate. It providesa route for enteral nutrition after upper gastrointes-tinal surgery. Gerndt and Orringer6 have reported thesurgical results of tube jejunostomy as routine inpatients undergoing esophagectomy for both benignand malignant disease. They found that the compli-cation rate after jejunostomy was around 1.9% forpatients with malignant diseases. Although seriouspotential complications, such as bowel necrosis,7
have been reported, most complications, such as tubedislodgment, bowel obstruction and abdominal wallinfection,6,7 are easily corrected.
In our patient, we believe that the implantation ofmalignant tumor at the jejunostomy site occurredduring the THE. Technically, a small anteriorgastrotomy close to the esophagogastric junction ismade after the tumor-bearing esophagus is adequate-ly dissected, then a varicose vein stripper was
Fig. 1ÐAbdominal computed tomogram demonstrating a ®llingdefect in the lumen of the jejunostomy with extension and invasionto the abdomonal wall (arrow).
Fig. 2ÐSquamous carcinomatous cell nests in the intravascular spaces of granulation tissue can be seen in areas of the jejunum (arrow).(hematoxylin and eosin, ´ 185).
158 Diseases of the Esophagus

advanced through the gastrotomy site to strip theesophagus.8 After the esophagus is extracted inv-ersely and passed through the gastrotomy site, agastric cardiectomy is performed and the specimen isremoved. Therefore, when the esophagus is extractedinversely, the ulcerative tumor is exposed to theoperative ®eld, which may cause tumor cell contam-ination of the surgeon's gloves. Unfortunately, sub-sequent iatrogenic implantation of malignant cellsthrough the surgeon's gloves may occur while a smallenterotomy is created for the completeness of astandard Stamm jejunostomy. Furthermore, we thinkthat tumor cell contamination of the surgeon's glovesprobably did not occur during dissection of thetumor-bearing esophagus in our patient, because theesophageal tumor did not invade to adventitia layerof the esophagus.
Although there have been similar reports of tumorimplantation in minimally invasive procedures, suchas laparoscopy,5 thoracoscopy,9 and even conven-tional incisions,10 the exact mechanics responsible forthe seeding remain controversial.11 However, anunderstanding of the importance of the non-touchprinciple of surgical oncology, attention to technicaldetails and awareness of potential risk will perhapsprevent this problem.
References
1. Orringer M B, Marshall B, Stirling M C. Transhiatalesophagectomy for benign and malignant disease. J ThoracCardiovasc Surg 1993; 105: 265±276.
2. Bumm R, Feussner H, Bartels H et al. Radical transhiatalesophagectomy with two-®eld lymphadenectomy and endo-dissection for distal esophageal adenocarcinoma. World J Surg1997; 21: 822±831.
3. Katariya K, Harvey J C, Pina E, Beattie E J. Complications oftranshiatal esophagectomy. J Surg Oncol 1994; 57: 157±163.
4. Lundstedt C, Stridbeck H, Andersson R, Tranberg K G,Andren-Sandberg A. Tumor seeding occurring after ®ne-needle biopsy of abdominal malignancies. Acta Radiol 1991;32: 518±520.
5. Clair D G, Lautz D B, Brooks D C. Rapid development ofumbilical metastases after laparoscopic cholecystectomy forunsuspected gallbladder carcinoma. Surgery 1993; 113: 355±358.
6. Gerndt S J, Orringer M B. Tube jejunostomy as an adjunct toesophagectomy. Surgery 1994; 115: 164±169.
7. Myers J G, Page C P, Steward R M, Schwesinger W H, SirinekK R, Aust J B. Complications of needle catheter jejunostomy in2,022 consecutive applications. Am J Surg 1995; 170: 547±551.
8. Bell G,Watt I, Anderson J R. Transhiatal esophagectomy usinga varicose vein stripper. Surg Gyn Obs 1992; 175: 461±463.
9. Fry W A, Siddiqui A, Pensler J M, Mostafavi H. Thoraco-scopic implantation of cancer with a fatal outcome. AnnThorac Surg 1995; 59: 42±45.
10. Enneking W F, Maale G E. The e�ect of inadvertent tumorcontamination of wounds during the surgical resection ofmusculoskeletal neoplasms. Cancer 1988; 62: 1251±1256.
11. Murthy S M, Goldschmidt R A, Rao L N, Ammirati M,Buchman T, Scanlon E F. The in¯uence of surgical trauma onexperimental metastasis. Cancer 1989; 64: 2035±2044.
Jejunostomy site tumor seeding 159





























