Embed Size (px)
DESCRIPTION
silahkan
Citation preview
Tumor muskuloskeletal
Sarcoma
• A type of cancer that begins in bone or in the soft tissues of the body, including cartilage, fat, muscle, blood vessels, fibrous tissue, or other connective or supportive tissue.
• Mesenchym

Soft Tissue Tumor• Fibrous tumor• Fibrohistiocytic tumor• Lipomatous tumor• Smooth muscle tumor• Skeletal muscle tumor• Tumors of blood and lymphatic vessels• Perivascular tumor• Synovial tumor• Neural tumor• Paraganglionic tumor• Pluripoten mesenchymal tumor
Surgical Oncology, 2003
Incidence
• It represents 1% of adult (age >16 years) malignancies and 15% of pediatric cancers. This malignancy can occur in any part of the body, though approximately 50% of all soft-tissue sarcomas present in an extremity
Surgical Oncology, 2003
Incidence
• Overall, the three most common subtypes of soft tissue sarcoma are liposarcoma, malignant fibrous histiocytoma(MFH), and leiomyosarcoma.
• Among extremity soft tissue sarcomas,liposarcoma and MFH predominate.
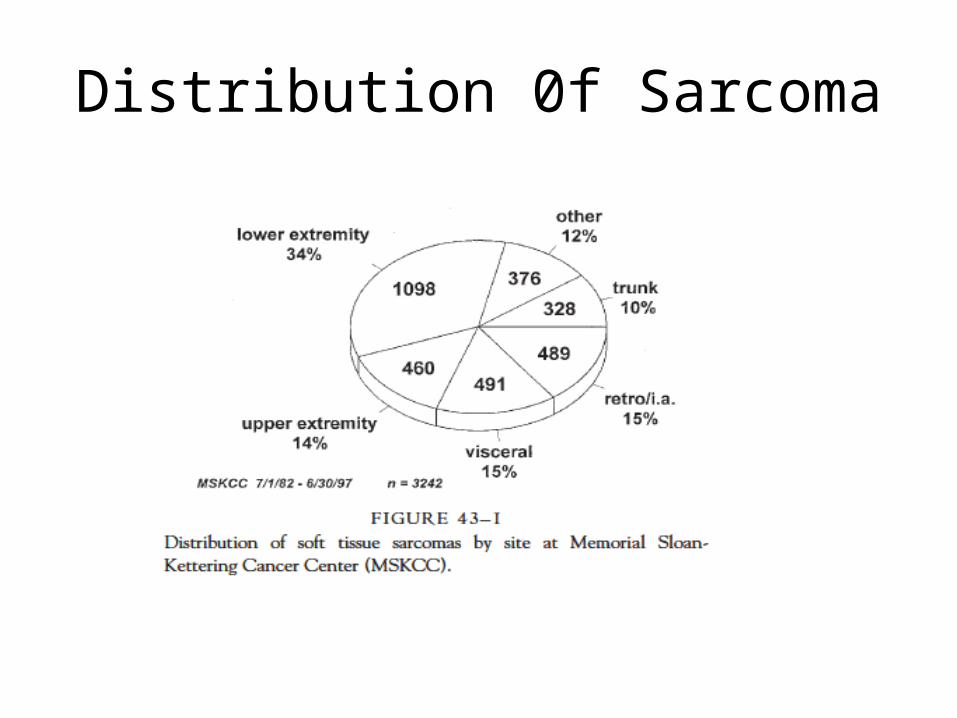
Distribution 0f Sarcoma

Devita, 2008
• Overall, the three most common histopathologic subtypes are MFH, liposarcoma, and leiomyosarcoma.
• Histopathologic type is anatomic site dependent: The common subtypes in the extremities are liposarcoma, MFH, synovial sarcoma, and fibrosarcoma.
Devita, 2008
Overview
• Sarcoma histologic type is generally an important determinant of prognosis and also an important predictor of distinctive patterns of behavior
• Sarcomas are characterized by local invasiveness. The pattern of metastasis of most sarcomas is hematogenous. Lymph node metastases are uncommon, except for selected cell types usually associated with childhood sarcoma.28
Grading
• The pathologic features that define grade include cellularity, histologic type and subtype and/or differentiation, pleomorphism, necrosis, and number of mitoses.
• Grading needs to be complemented with radiologic and molecular parameters.
Etiology
• Genetic• Radiation• Lymphedema• Chemical agents exposure
Differential Diagnosis
• benign lesions, as well as primary or metastatic carcinoma, melanoma, and lymphoma.
Clinical presentation
• a mass is usually large, is often painless, and may be associated by the patient with an episode of injury. The majority present at a size larger than 5 cm.
• There is frequently a perceived antecedent trauma. Pain is usually a late symptom. Lesions may be misdiagnosed as hematomas or strained muscle. (Washington, 2007)
Primary bone tumor on pediatric
• Primary bone tumors in children are rare conditions
• Th e most common benign lesion of bone is undoubtedly the solitary osteocartilaginous exostosis ( osteochondroma).
Sign & Symptoms
• Pain that is constant, unrelated to activity, and is worse at night.
• Swelling• Pathologic fracture
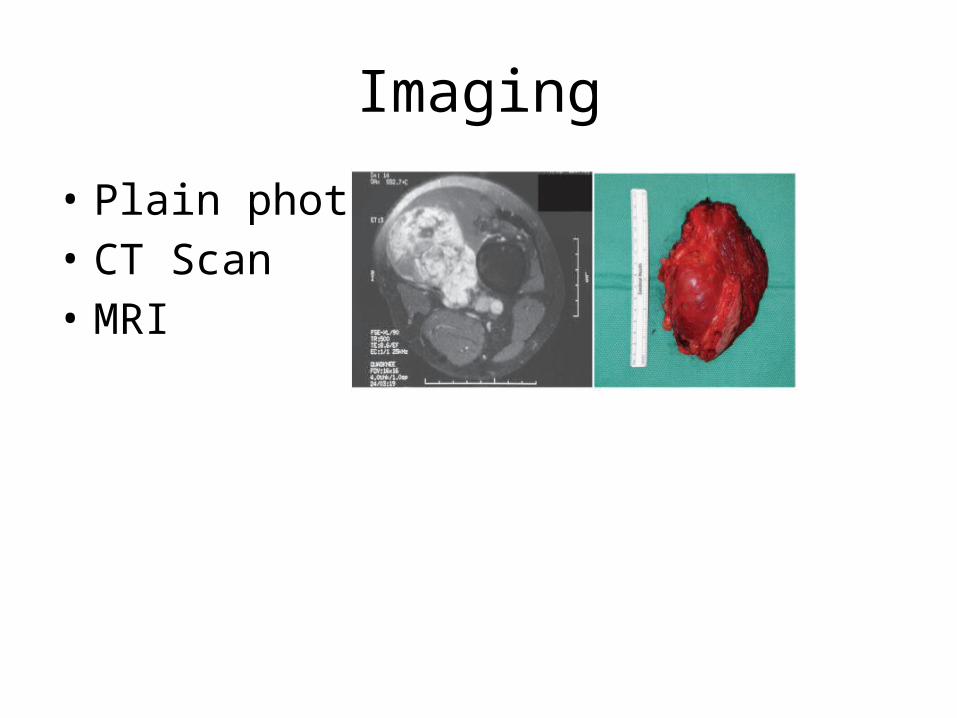
Imaging
• Plain photo• CT Scan• MRI
Biopsy
• Incisional biopsy : gold standard. (Washington, 2007)
Incision should parallel to the long axis of the extremity.
• Core needle biopsy• Excisional biopsy• FNAB : cytopathologic evaluation only, FNA
usually cannot give the grade

• If the lesion under investigation is small (<5cm), an excisional biopsy should be performed, serving as both a diagnosticand therapeutic procedure.
• If the lesion is large, a Tru-Cut (or if nondiagnostic, an incisional) biopsy is the procedure of choice.
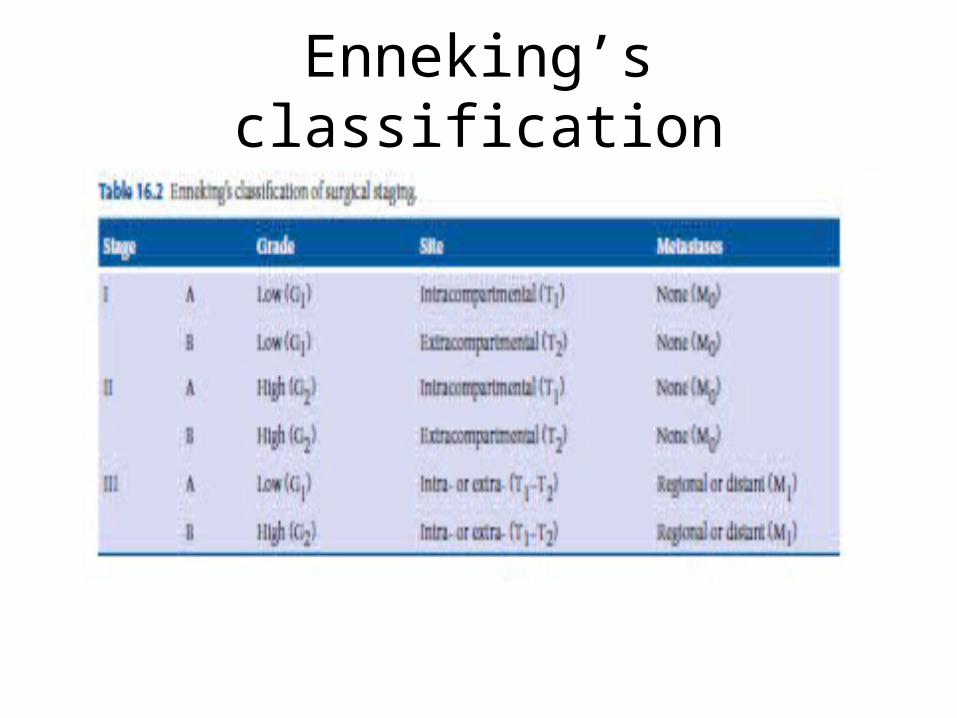
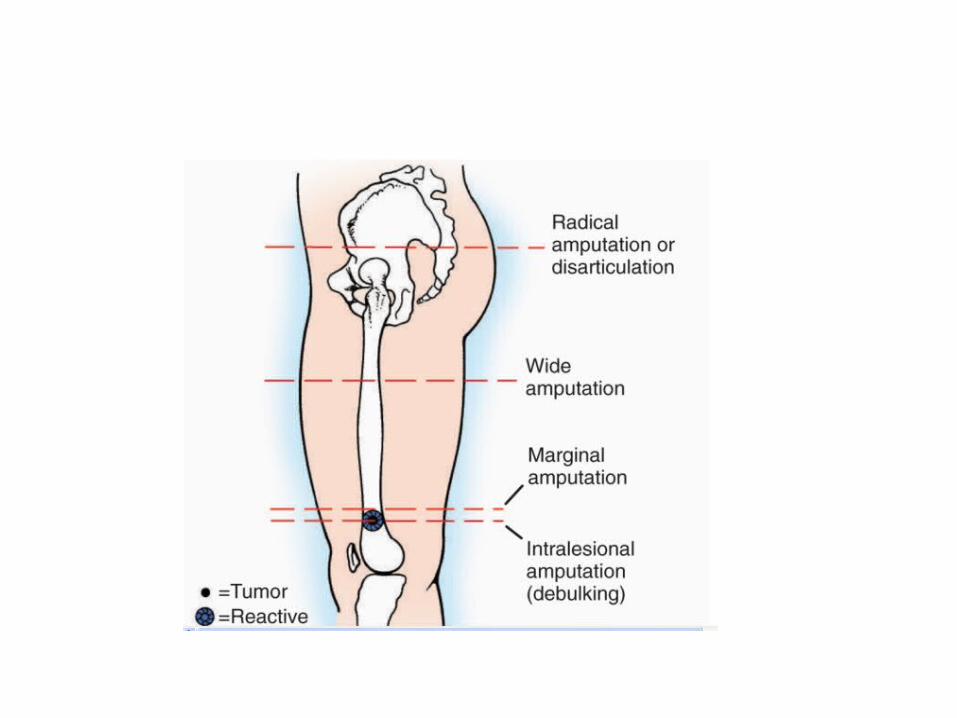
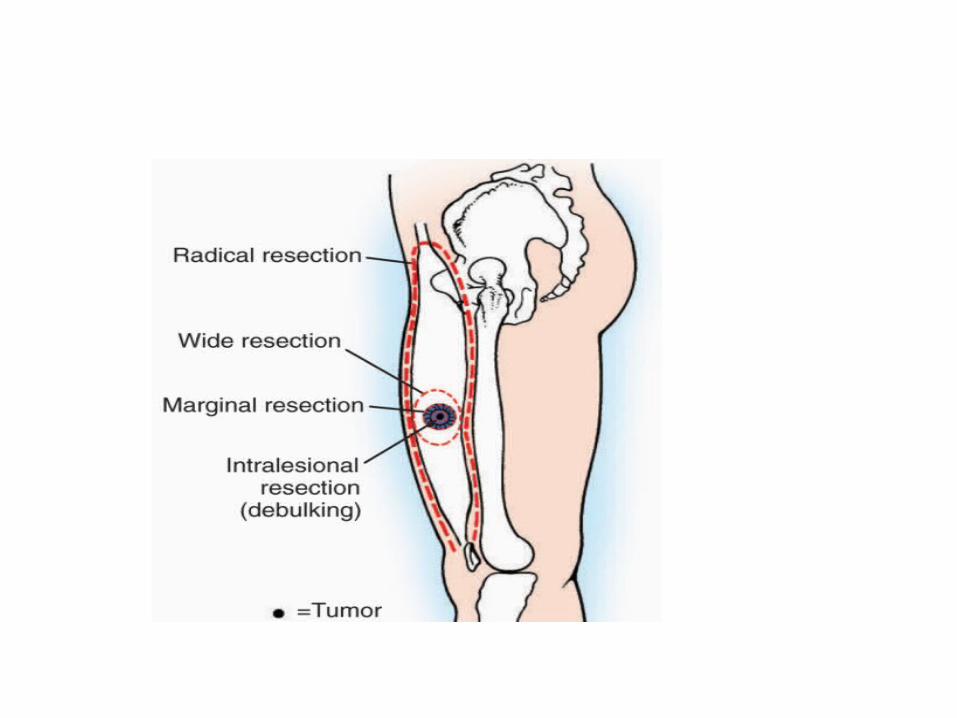
Enneking’s classification
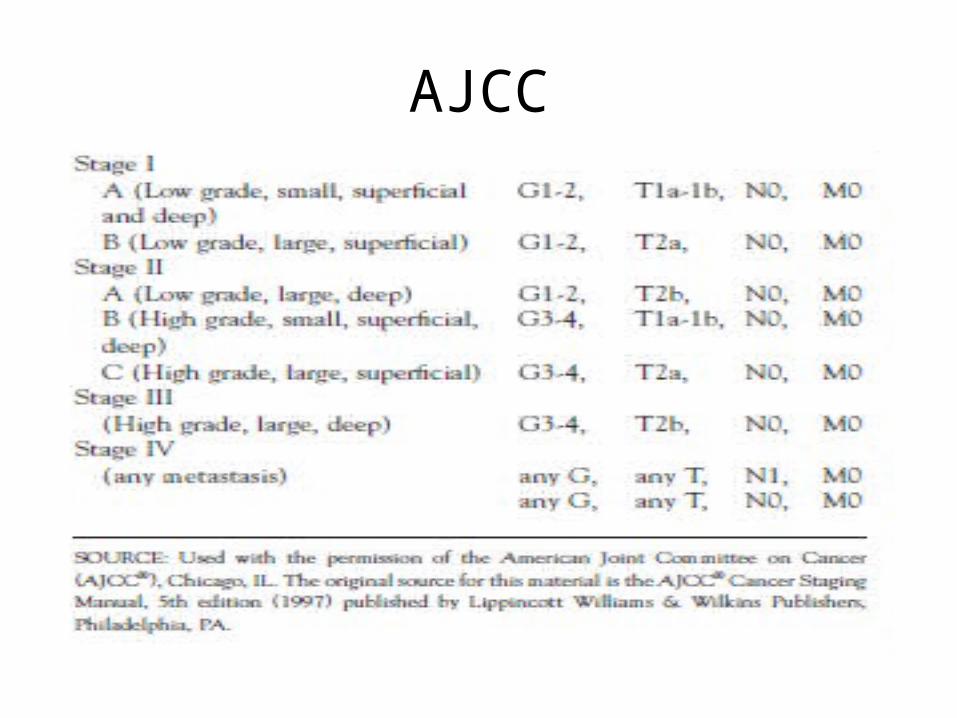
AJCC
Surgical Oncology, 2003
Metastases
• Soft tissue sarcoma of the extremity metastasizes almost exclusively to the lung.
• Current treatment of choice is thoracotomy with wedge resection of all pulmonary nodules.
Surgical Oncology, 2003
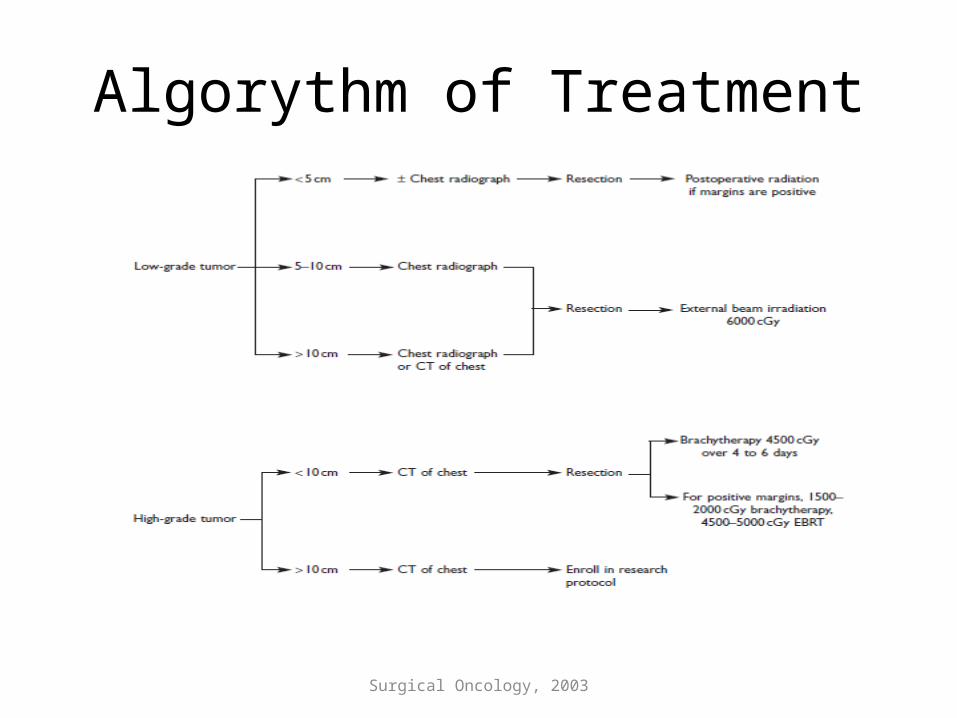
Algorythm of Treatment
Goals of treatment for resectable disease:
• Complete removal with negative margins• Maximal preservation of function• Remove prior biopsy scar en bloc• Postoperative irradiation reduces recurrence
Unresectable lesions or tumors:
• Associated with widely disseminated disease: treat with primary irradiation 6500cGy

Washington, 2007
Surgical Treatment
A. Resection• Smaller, grade I tumors can be excised with a
minimum 1-cm margin, usually without adjuvant radiation.
• Larger tumors may benefit from a larger margin or radiation to prevent recurrence.
• Grade II and III tumors, in general, require radiation therapy in addition to excision to avoid more-radical surgery. Depending on the size and grade of tumor, compartment resection may be indicated.
Surgical Oncology, 2003
Washington, 2007
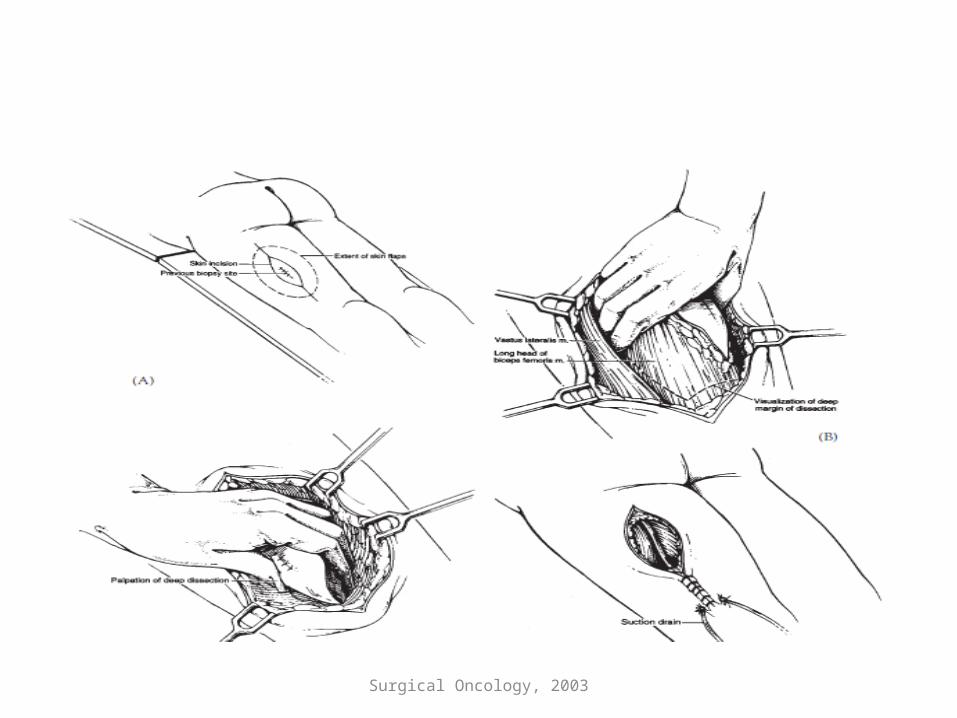
B. Limb-sparing resection• Limb-sparing resection combined with
radiation therapy offers survival equivalent to that achieved with amputation (Ann Surg 1982;196:305). The resection field should be marked with clips to guide radiation therapy.

Recurency
• Soft tissue sarcoma of the extremity recurs in approximately onethird of all patients, including those with high- and low-grade tumors of all sizes, with a median disease-free interval of 18 months.
Key Topic in Orthopedic, 1995
Benign Bone Tumor
• Cartilage tumor : enchondroma, chondroblastoma and chondromyxoid fibroma.
• Fibrous tissue : solitary bone cyst, Aneurysmal bone cyst,Non-ossifying fibroma, Fibrous dysplasia,Giant cell tumour
• Bone tumor : Osteoid osteoma, Osteoblastoma
Clinical Finding
• progressive pain at rest and at night
Campbell's,2007
Location• epiphyseal (adult) a giant cell tumor, whereas an
epiphyseal lesion in children is likely to be a chondroblastoma.
• Diaphyseal lesions includes Ewing sarcoma, histiocytosis, lymphoma, fibrous dysplasia, and adamantinoma (especially in the tibia).
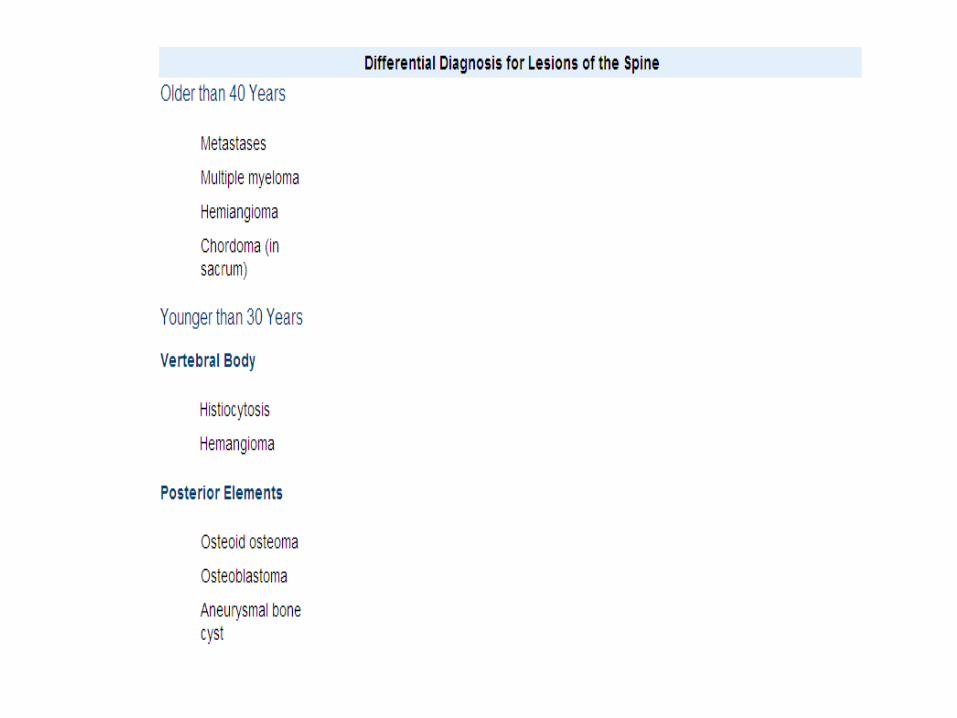
• Most vertebral lesions in adult patients are metastases, myelomas, or hemangiomas. In the sacrum, chordoma is at the top of the list of differential diagnoses. In younger patients with a vertebral body lesion, the most likely diagnosis is histiocytosis;
Metastases of Unknown Origin
• In a patient older than age 40 with a new, painful bone lesion, multiple myeloma and metastatic carcinoma are the most likely diagnoses even if the patient has no known history of carcinoma.
• Prostate cancer and breast cancer are the two most common primary sources for bone metastases.
• If a patient has no known primary tumor, however, the most likely sources are lung cancer and renal cell carcinoma
Imaging
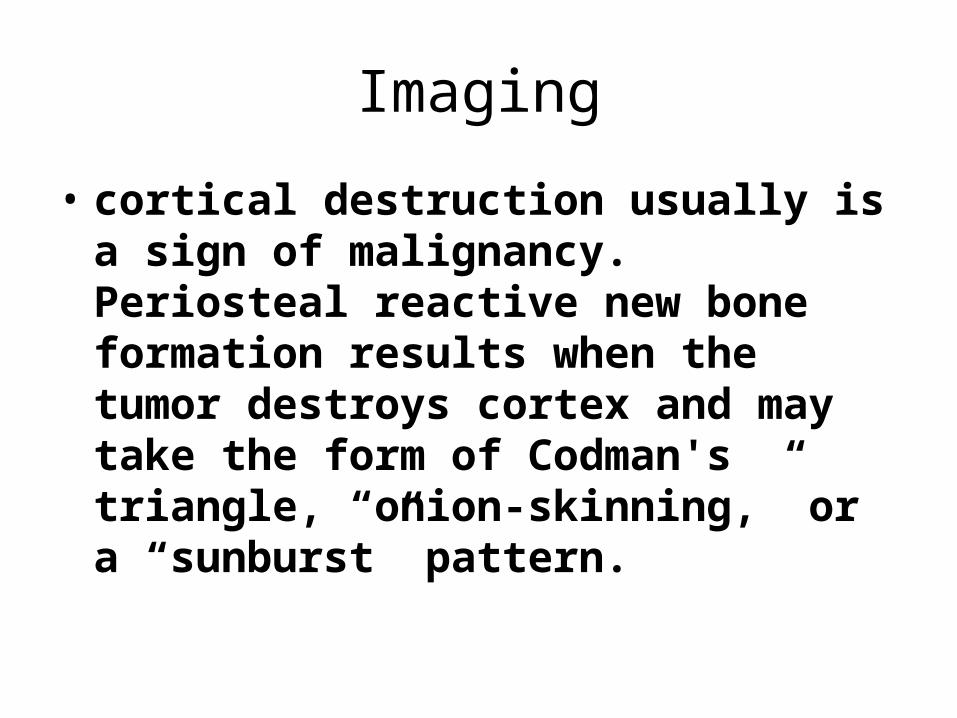
• cortical destruction usually is a sign of malignancy. Periosteal reactive new bone formation results when the tumor destroys cortex and may take the form of Codman's triangle, “onion-skinning,” or a “sunburst” pattern.
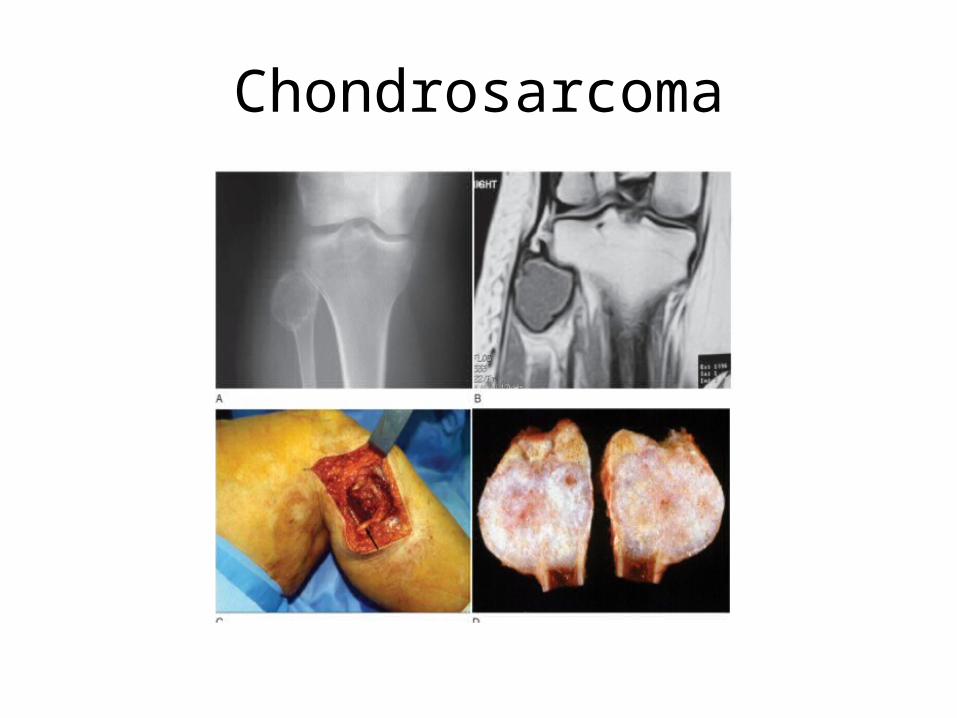
Chondrosarcoma

Campbell's, 2007
AJCC for Bone Sarcoma
Campbell's, 2007
Treatment
• The goal of treatment in a patient with a primary malignancy of the musculoskeletal system is to make the patient disease free.
• The goal of treatment of a patient with metastatic carcinoma to bone is to minimize pain and to preserve function.
• The optimal treatment of the tumor often requires a combination of radiation therapy, chemotherapy, and surgery.
Radiation
• Most primary bone malignancies are relatively radioresistant. Exceptions are the marrow cell tumors, including multiple myeloma, lymphoma, and Ewing sarcoma, which are each exquisitely sensitive.
• Carcinomas metastatic to bone, with the exception of renal cell carcinoma, also frequently are sensitive to radiation treatment.
• For most other bone tumors, radiation has a limited role because local control is achieved better with surgery.
Chemotherapy
• chemotherapy has a well-defined role in the treatment of other high-grade malignancies of bone, such as malignant fibrous histiocytoma, and high-grade soft-tissue malignancies of childhood, such as rhabdomyosarcoma.
• The role of chemotherapy is less well defined for adult soft-tissue malignancies.
• In general, chemotherapy is not useful for cartilaginous lesions and most other low-grade malignancies.
Surgery
• now allow limb salvage to be a reasonable option for most patients with bone or soft-tissue sarcomas.
• Specifically, preoperative radiation therapy for soft-tissue sarcomas and neoadjuvant chemotherapy for bone sarcomas have helped surgeons to resect successfully some tumors that in the past would have been deemed unresectable.