Embed Size (px)
Citation preview

Trends in molecular diagnosticsTrends in molecular diagnosticsDetection of target Detection of target genes of interestgenes of interest
QuantificationQuantification
Infectious diseasesInfectious diseasesHIVHepatitis C & BTB / MAC CytomegalovirusHerpes simplexVaricella zosterCT/GCHPV
Profiling mutations Profiling mutations associated with disease associated with disease outcomeoutcome
Hepatitis C genotypeHIV drug resistance genotypeHost genetic factorsThrombophiliaCyP450 – drug metabolismHLA type

Key developmentsKey developments
TechnologyTechnology
Uptake in diagnostic arena Alternative methods to PCR – SDA, TMA, LCR, NASBA, bDNAAvailability of Analyte Specific Reagents (ASR)Trend to real time or kinetic formatsAutomationContamination and inhibitor control

? What is driving commercial NAT ? What is driving commercial NAT platform developmentplatform development
Reduce sources of errorReduce sources of error
Reduce tedious processesReduce tedious processes
Improve time to resultImprove time to result
Improved analytical rangeImproved analytical range
Improve limit of detectionImprove limit of detection
Improve specificityImprove specificity

Pre amplification Pre amplification -- extractionextraction
•Volumetric errors amplified•Tedious – manual, repetitive•Specimen integrity


Post amplification & detectionPost amplification & detectionEndpoint detectionEndpoint detection
•Volumetric error•Fragment size vs. probe hybridisation•Time to result•Automation calibration issues•Result calculations

Signal amplification Signal amplification -- bDNAbDNA
TMA PCR bDNA
Target RNA or DNA
Add primers & enzymes
Add primers & enzymes
Copies(RNA) Copies
(DNA)
1 detection probe per copy
1 detection probe per amplified copy
Multiple detection probes per target
Add probes and branched DNA
Virus, bacterium or cell
Comparison of Amplification Methods
HIV, HBV, HCV, CMVStandard curveAmplify signal of label – no amplicon issuesOvernightHigh throughputLimited extraction

Kinetic / real time product Kinetic / real time product detectiondetection

Monitoring in Real timeMonitoring in Real time
Agarose Gel Blotting FRET

Real time PCRReal time PCR

Real Time PCR with 5Real Time PCR with 5’’ Nuclease AssayNuclease AssayProduct detection during amplificationProduct detection during amplification
Fluorescence EmissionQuenched
||||||||||||| ||||||||||||
R Q
hγ
R
|||||||||||||||||||||| |||||
Q
Fluorescence Emission
Detected
hγ
Q
||||||||||||||||||||||||||||||||||
R
Primer Probe

HIV viral load testsHIV viral load testsManufacturer Principle Results Availability Analytical range
Roche RT-PCR (gag)(COBAS HIV MONITOR v1.5)
copies/mL (6 hours to result)
Widely <50 – 100,000<400 – 750,000
Bayer HIV Branched DNA 3.0 (bDNA) (pol)
copies./mL(results 2x less than Roche)
(36 hours to result)
NSW, Vic <50 – 800,000
Biomerieux HIV-1 QT NASBA (gag)
Copies/mL(6 hours to result)
NSW <400 – 1,000,000<80 – 500,000
Roche Real time (Taqman)(gag)
Copies/mL(4-6 hours to result)
Widely <40 – 10,000,000
Biomerieux EasyQ HIV-1 real time TMA (gag)
Copies/mL & IU/mL(4-5 hours to results)
1 lab <40 – 10,000,000
Abbott Celera Realtime PCR m2000 (pol integrase)
copies/mL Widely <40 – 10,000,000
Artus Realtime PCR –Rotorgene
Copies/mL Unregistered <40 – 10,000,000

Selected ApplicationsSelected Applications
Primary HIV diagnosis & enhanced surveillancePrimary HIV diagnosis & enhanced surveillance
Infant HIV diagnosisInfant HIV diagnosis
HIV treatment & progressionHIV treatment & progressionmonitoringmonitoring


HIV TestingHIV TestingDirect Detection of VirusDirect Detection of Virus
p24 antigen detection – serologyp24 only assays – qualitative and quantitativep24 in combination with antibody Serum
Virus isolation - cultureNucleic acid detection - (NAT))HIV DNA or RNA ?
DNA qualitative – proviral (cellular)resolution of inconclusive serologydiagnosis in infants - maternal antibodiesacute infection (pre-seroconversion)
RNA quantitative – monitoring / serial viral loaddrug resistance monitoring subtyping – treatment and surveillance
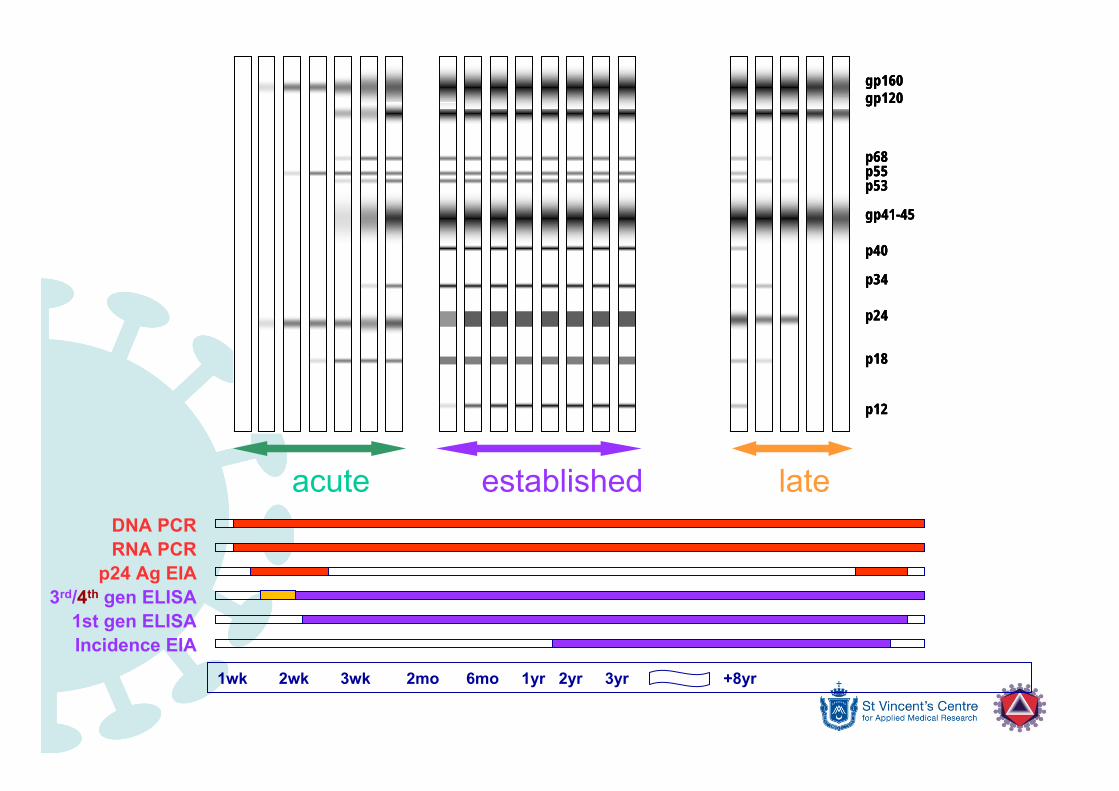
DNA PCRRNA PCR
p24 Ag EIA3rd/4th gen ELISA
1st gen ELISAIncidence EIA
1wk 2wk 3wk 2mo 6mo 1yr 2yr 3yr +8yr
gp160gp120
p68p55p53
gp41-45
p40
p34
p24
p18
p12
gp160gp120
p68p55p53
gp41-45
p40
p34
p24
p18
p12
gp160gp120
p68p55p53
gp41-45
p40
p34
p24
p18
p12
acute established late

Minipool NAT testing in blood Minipool NAT testing in blood donorsdonors
1 2 3 4
1 2 3 4
4 mini pools of 6 samples each4 mini pools combined and tested(total = 24 samples in single test)
1 2 3 4
1
1

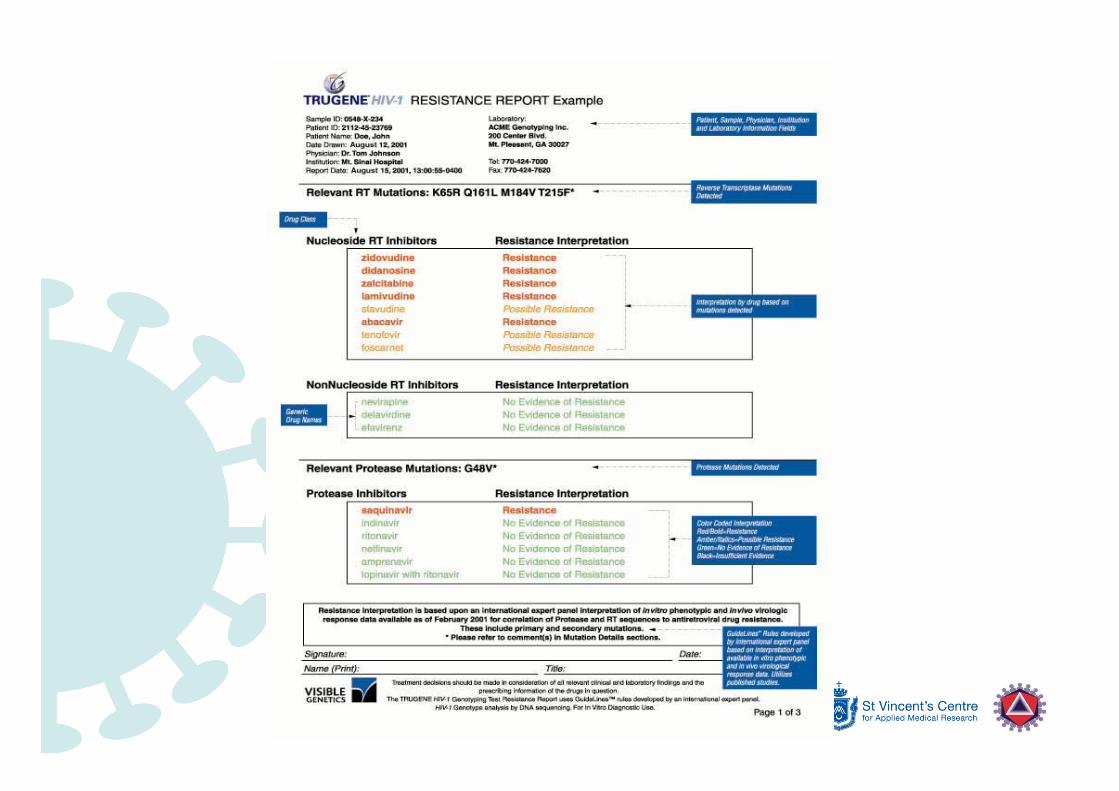
HIV drug resistance testingHIV drug resistance testing

Breakthrough of Breakthrough of resistanceresistance

DNA sequencingDNA sequencing


Neonatal HIV diagnosisNeonatal HIV diagnosis

Neonatal HIV diagnosisNeonatal HIV diagnosisSerologic assays
Maternal antibodies persist up to 18 months postpartumAntibody tests not helpful in newborn diagnosisSero-reversion (pos → neg) in serial samplesHIV-1 p24 antigen limited value – complexed by Ab
Virologic assaysVirus culture from PBMCMaternal HIV-1 RNA in obstetric setting is useful in predicting risk of perinatal transmission HIV DNA and RNA useful in infant
Detection in infant is diagnostic for perinatal HIV infectionUseful in timing of transmission (in utero, intrapartum, post partum)Monitoring response to therapy in infected infant

Positive 48h(likely intrauterineInfection - early)
1 2 3 4 5 6 7 8 9 10 11 12
48h
14d1-2mo
Positive 14d(likely intrapartum
Infection - late)
3-6mo
HIV RNA/CD4
? considercease ZDV px
aggressive ARV
13 14 15
HIV infection reasonablyexcluded in non-breast fed infant
if negative in 2 or more≥≥1month and 1month and ≥≥4months4months
6-12mo
>2 negative HIV Ab tests (<1month apart)Loss Ab/ neg DNA =
un-infected>15-18mo
Infant still Ab+ at12mo – retest 15-18mo
HIV Ab+ >18mo =
HIV infection
Months post partum

CASE STUDYCASE STUDY

gp160
gp120
p68
p55/51
gp41
p40
p34
p24
p18
α-huIgG
BA,RIBA,RIHIV serology• HIV-1/2 Ab/Ag 4th gen EIA – reactive • HIV-1/2 3rd generation EIA - reactive• HIV-1/2 rapid test (X2) – reactive• HIV-1 western blot – POSITIVE
HIV direct detection• HIV-1 p24 antigen – not detected• HIV proviral DNA PCR – not detected• HIV RNA (gag) – PCR – not detected
N P

BA,RIBA,RI
30 30 y/o African male Ghanay/o African male GhanaImmigration detention centre NSWImmigration detention centre NSWHeterosexualHeterosexualExposure Exposure FSW 1 year agoFSW 1 year agoCurrently 1Currently 1°° syphilissyphilisRecurrent episodes malaria Recurrent episodes malaria –– treated as outpatient treated as outpatient several times over last few yearsseveral times over last few years

What next?What next?Follow up sample and detailed history!Follow up sample and detailed history!HIV serology testing strategies HIV serology testing strategies • Supplementary EIAs
CD4 lymphocyte count CD4 lymphocyte count • 480 (normal)
HIVHIV--2 serology 2 serology • Negative to specific gp 36 antigens
HIV RNA HIV RNA (pol)(pol)• Not detected by bDNA RNA test
HIV culture HIV culture -- virus isolationvirus isolation• CD8 depleted, IL2 enriched, PHA stimulated
PBMC co-culture
gp140
gp105
p68
p56
gp36
p34
p26
p16





























