Embed Size (px)
Citation preview

Robert E. Beasley, MD, FSIR, FSCAIDirector of Vascular/Interventional Radiology
Mount Sinai Medical Center
Miami Beach, FL
Treatments of Superficial Venous Disease: Endovenous Laser Ablation

Disclosures
Speaker/Trainer/Advisory Board:
• Abbott Vascular
• BARD
• BSCI
• Cardinal Health/Cordis
• Cook Medical
• CSI
• Endologix
• Gore
• Lake Region Medical
• Medtronic
• Penumbra
• Phillips/Volcano
• Spectranetics
• Terumo/Bolton

• Vein problems are the most common chronic condition in North America
• 40% of Americans have varicose veins1
• Up to 56% men; up to 60% women2
• More people lose work time from vein disorders than from arterial disease3
• More than 20 million people in the United States suffer from varicose veins or spider veins
Prevalence of Varicose Veins
1 Vascular Medicine, Weinberg, May 20102 Phlebology, Robertson, 2008
3Vascular Disease Foundation Newsletter, Spring 2005; Vol. 5, N2

• Inherited genetic predisposition
• Normal aging process
• Hormonal changes that relax vein walls, which put woman at a greater risk than men
• Conditions that put excess pressure on leg veins – including standing for long periods of time, obesity and pregnancy
• History of blood clots and conditions that increase pressure in the abdomen, such as tumors, constipation and tight garments
• Previous venous surgery
• Exposure to ultraviolet rays
What Causes Varicose Veins?

• -32.1% of English women cotton workers had varicose veins compared with 5.8% of Egyptian women workers
• -Various studies documented VV prevalences:
8% in Singapore
1.2% in India
6.1% in Tanzania,
2-16% in Cook Islands, etc.
The prevalence of venous disease is highest in western, industrialized societies

• 134 families examined, including 67 patients and 67 controls and their parents
• Risk of developing VVs 90% if both parents affected
• 47% (25% for males and 62% for females) if one parent affected
• 20% if neither parent affected
Cornu-Thenard A et al, Importance of the Familial Factor in Varicose Disease, J Dermatol Surg Oncol 1994; 20:318-326
Heredity affects incidence ofChronic Venous Disease
• Framingham 2yr incidence:P0-1: 45.7/1000
P2-3: 53.2/1000
P>3: 59.2/1000
• 405 women with VVs
13% had 1 pregnancy
30% had 2 pregnancies
57% had 3 or more
(Mullane DJ, Am J OB Gyn, 1952,63:620)
Pregnancy confers an independent risk: More pregnancies more varicose veins
• Most studies show that prolonged standing or sitting increases the prevalence and severity of venous disease
• 2854 factory workers, in those with varicose veins:
65.5% stood
29.2% sat
6.3% walked
Santler R, Hautarzt 1956;10:460
Work may be hazardous to your venous health

• Compression Stockings
• Compression therapy is frequently the first and most conservative step in the management of varicose veins. In fact, insurers often require that patients undergo conservative compression therapy prior to becoming eligible for reimbursement for the EVLT or other more aggressive varicose vein treatments. Compression stockings are also often used following those same treatments to promote healing by lessening pain, swelling and bruising.
It is important to recognize that compression stockings can alleviate some symptoms of varicose veins but they cannot treat their underlying cause, failed valves (also called venous reflux). Even with faithful use of compression stockings, the disease may progress to the point that more advanced treatment is necessary.
Conservative Care

Endovenous Laser Treatments (EVLT)
Radiofrequency Ablation (RFA)
Phlebectomy
Sclerotherapy
Stripping & Ligation
Minimally Invasive Options
Before After

Endovenous Laser
Treatment (EVLT) is a
30 – 45 minute, in-office
procedure requiring
only local anesthetic
and enables patients to
return to normal activity
immediately – with little
or no pain.
Endovenous Laser Treatment (EVLT)

EVLT for the elimination of varicose veins is quickly becoming the gold-standard in the treatment of varicose veins.
EVLT uses laser energy, which is simply a highly concentrated beam of light. Medical lasers work by delivering this light energy to the targeted tissue with extreme precision, so as not to affect the surrounding tissue. Lasers have proven their safety and effectiveness through years of use in all types of medical procedures, from eye surgery to dermatology. In the hands of a skilled physician, lasers offer far less risk for complications than conventional surgery.
In EVLT, a thin fiber is inserted into the damaged vein through a very small entry point in the skin. A laser light is emitted through the fiber, as the fiber is pulled back through the vein, it delivers just the right amount of energy. The targeted tissue reacts with the light energy, causing the vein to close and seal shut.
The veins that are closed are superficial veins that handle less than five percent of the body's blood flow. The blood is automatically routed to other, healthy veins.
Endovenous Laser Treatment (EVLT)
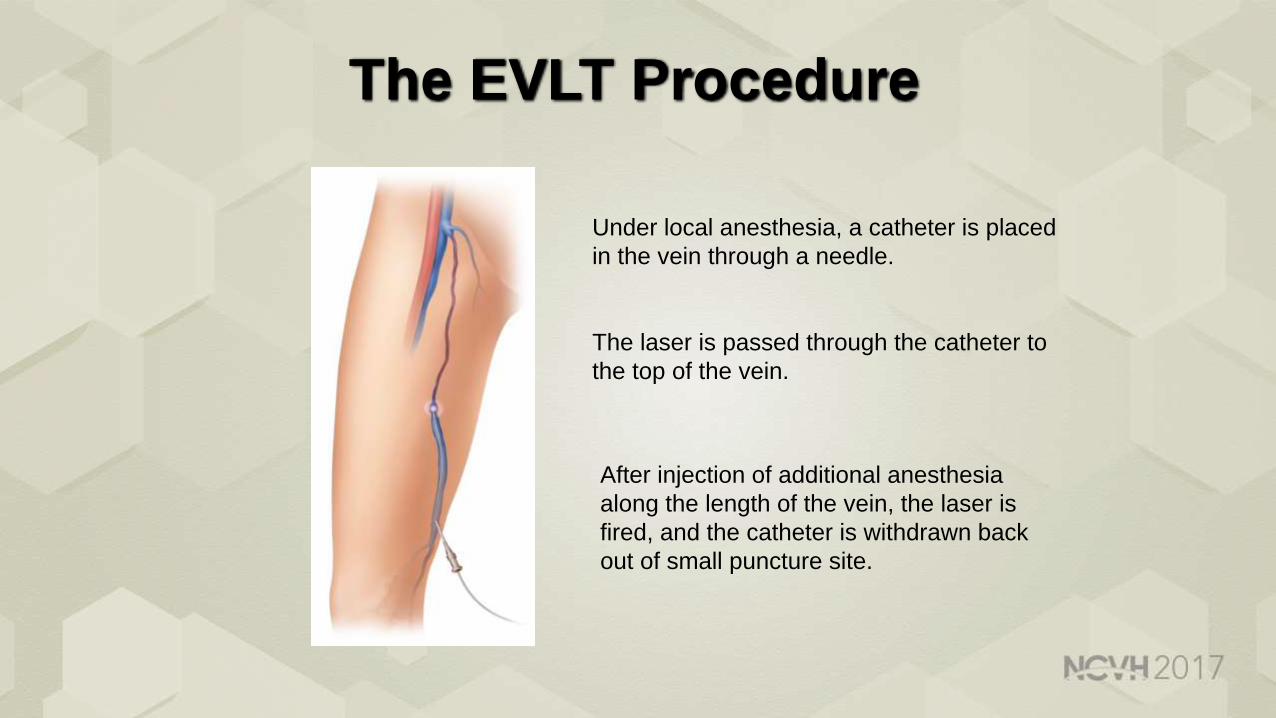
The EVLT Procedure
Under local anesthesia, a catheter is placed
in the vein through a needle.
The laser is passed through the catheter to
the top of the vein.
After injection of additional anesthesia
along the length of the vein, the laser is
fired, and the catheter is withdrawn back
out of small puncture site.

VEIN MAPPING

What Is VenaCure EVLT Treatment?
VenaCure EVLT laser treatment eliminates unsightly varicose veins with:▪ No hospital stay▪ Minimal-to-no scarring▪ No lengthy recovery ▪ Minimal-to-no side effects
The VenaCure EVLT system uses targeted laser energy to seal the vein shut and help patients look and feel better fast.
Patient prepped for the procedure

Venous Access

Venous Access
Ultrasound-guided Access Microintroducer
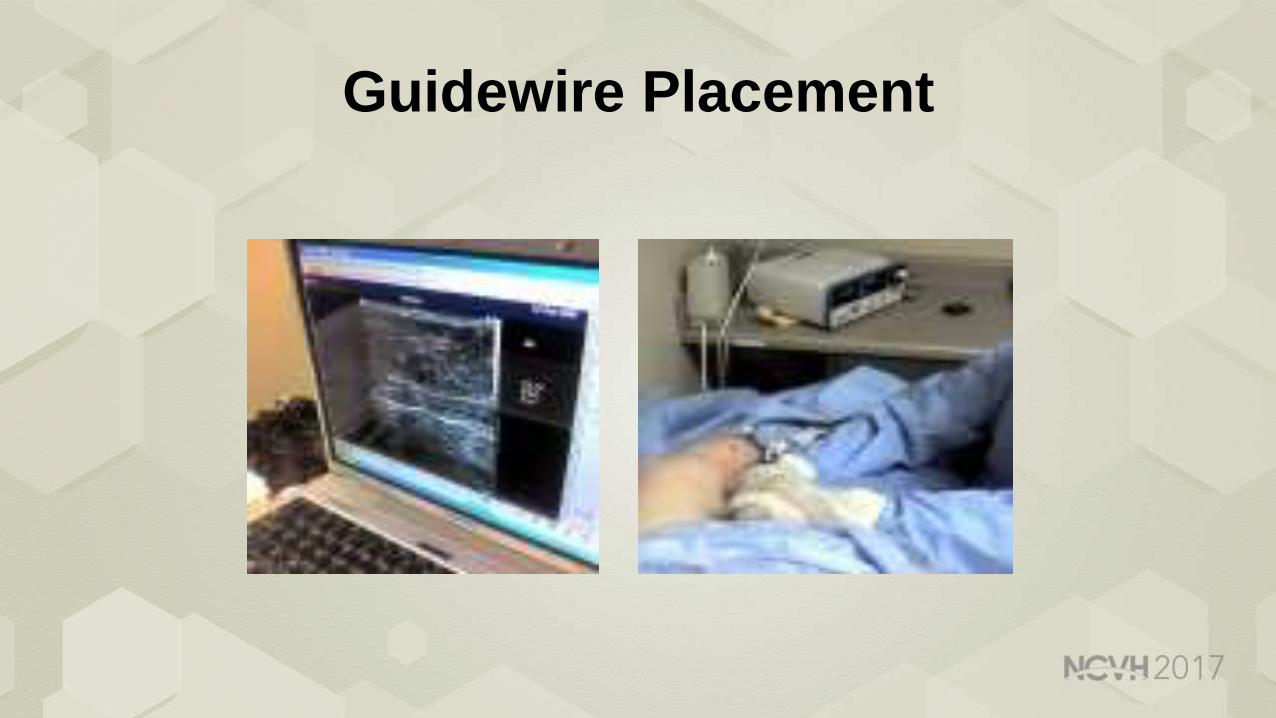
Guidewire Placement
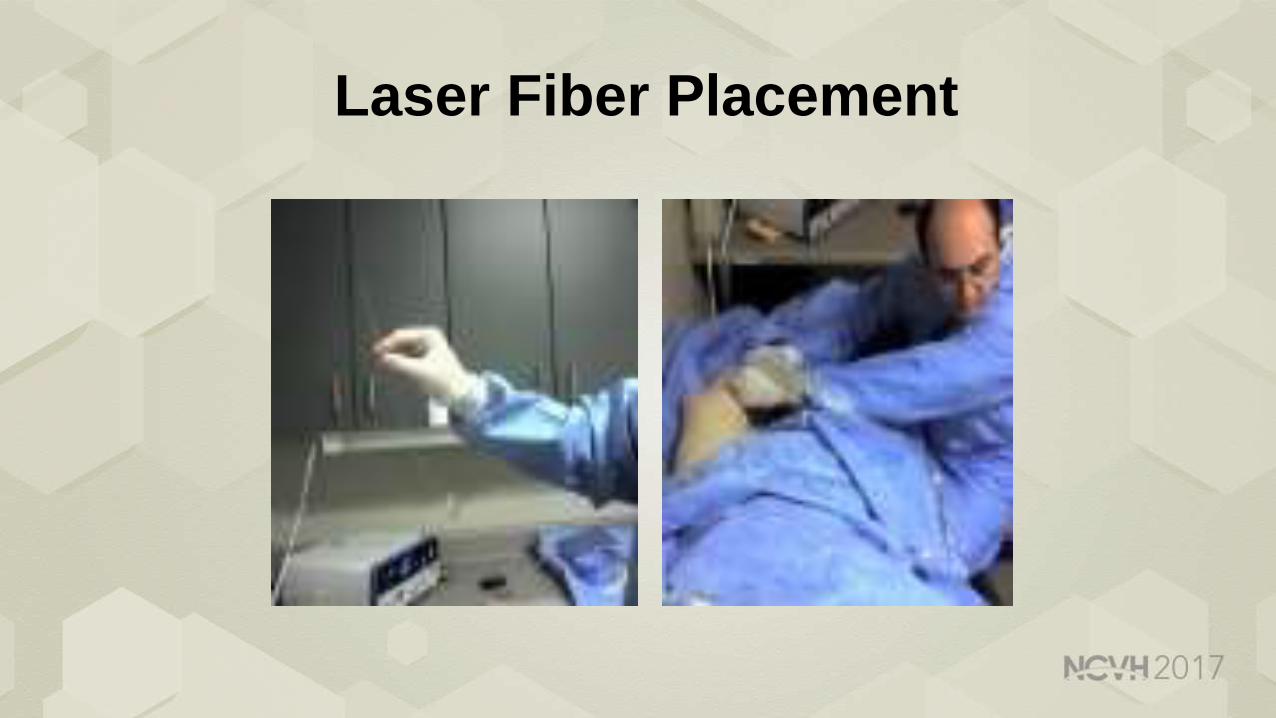
Laser Fiber Placement

Laser Fiber Placement
Guidewire and Laser Fiber Placement
Guidewire and Laser Fiber Placement
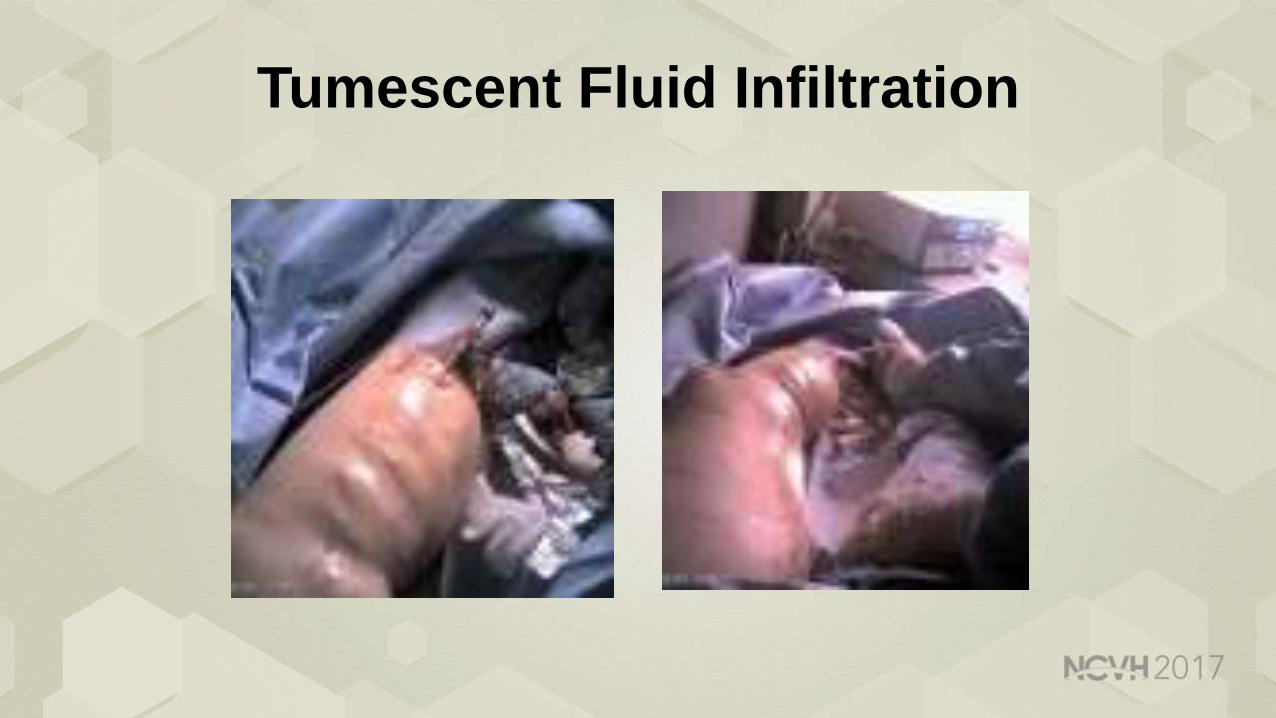
Tumescent Fluid Infiltration

Tumescent Infiltration

Endovenous Laser Treatment
Laser in sheath Laser On

Safe procedure◦ Complications are minor and self-limiting
Less painful◦ The majority of patients experienced mild discomfort (1.5, range 0-5) in the
early post-operative period Less limiting ◦ Resumes work after 1.2 days
Relatively easy procedure (30 – 45 min)◦ Local anesthesia
Treatment of varicose veins under local anesthesia is safe and yields satisfactory clinical and duplex outcome
Treatment of varicose veins can be performed safely with comparable results to general anesthesia in selected patients
Journal of Vascular Surgery, 2009Hongkong Medical Journal, 2009
Phlebology, 2009
Endovenous Laser Treatment
EVLT Evidence for Wound Healing
MORE THAN 20 NEW STUDIES SINCE 20101. Abdul-Haqq R, et al. Endovenous ablation of great saphenous vein and perforator veins improves venous stasis ulcer healing. Ann Vasc Surg.
2013 Oct;27(7):932-9.
2. Agale SV. Chronic Leg Ulcers: Epidemiology, Aetiopathogenesis, and Management. Ulcers, Vol 2013 (2013), Article ID 413604, 9 pages.
3. Amir O, Liu A, Chang ALS. Stratification of highest-risk patients with chronic skin ulcers in a Stanford retrospective cohort includes diabetes, need
for systemic antibiotics, and albumin levels. Ulcers. 2012, Article ID 767861, 7 pages.
4. Fife CE, Carter MJ. Wound Care Outcomes and Associated Cost Among Patients Treated in US Outpatient Wound Centers: Data from the US
Wound Registry. Wounds. 2012 Jan;24(1):10-7.
5. Gloviczki P, et al. The care of patients with varicose veins and associated chronic venous diseases: Clinical Practice Guidelines of the Society for
Vascular Surgery and the American Venous Forum. J Vasc Surg. 2011 May;53(5 Suppl):2S-48S.
6. Harlander-Locke M, et al. Combined treatment with compression therapy and ablation of incompetent superficial and perforating veins reduces
ulcer recurrence in patients with CEAP 5 venous disease. J Vasc Surg. 2012 Feb;55(2):446-50.
7. Kostas TI, et al. Chronic venous disease progression and modification of predisposing factors. J Vasc Surg. 2010 Apr;51(4):900-7.
8. L.E.K. Consulting 2014 Market Analysis. Market Sizing and Assessment of Outsourced Outpatient Wound Care.
9. Ma H, O’Donnell TF Jr, Rosen NA, Iafrati MD. The real cost of treating venous ulcers in a contemporary vascular practice. J Vasc Surg Venous
Lymphat Disord. 2014 Oct;2(4):355-61.
10. Marrocco CJ, et al. Endovenous ablation for the treatment of chronic venous insufficiency and venous ulcerations. World J Surg. 2010
Oct;34(10):2299-304.
11. Nesbitt C, Bedenis R, Bhattacharya V, Stansby G. Endovenous ablation (radiofrequency and laser) and foam sclerotherapy versus open surgery
for great saphenous vein varices. Cochrane Database Syst Rev. 2014 Jul 30;7:CD005624.
12. O’Donnell TF Jr, et al. Clinical practice guidelines of the Society for Vascular Surgery (SVS) and the American Venous Forum (AVF): Management
of venous leg ulcers. J. Vasc Surg. 2014 Aug;60(2 Suppl):3S-59S.
13. O’Meara S, Cullum N, Nelson EA, Dumville JC. Compression for venous leg ulcers (Review). Cochrane Database Syst Rev. 2012 Nov
14;11:CD000265.
14. Pannier F, Rabe E. Progression of Chronic Venous Disorders-Results from the Bonn Vein Study. J Vasc Surg. March 2011;53(1):254-5. (Abstract
Presented at AVF Forum 23rd Annual Meeting)
15. Pannier F, Rabe E. Progression in venous pathology. Phlebology. 2015 Mar;30(1 Suppl):95-7.
16. Rabe E, et al. Incidence of Varicose Veins, Chronic Venous Insufficiency, and Progression of Disease in the Bonn vein Study II. J Vasc Surg.
March 2010; 51(3):791.
17. Rabe E, Pannier F. Societal costs of chronic venous disease in CEAP C4, C5, C6 disease. Phlebology. 2010 Oct;25 Suppl 1:64-7.
18. Review and Comment of the 2011 Clinical Practice Guidelines of the Society for Vascular Surgery and the American Venous Forum.
Phlebolymphology. 2012;19(3):107-120.
19. Robertson L, et al. Incidence of chronic venous disease in the Edinburgh Vein Study. J Vasc Surg Venous Lymphat Disord. 2013 Jan;1(1):59-67.
20. Shenoy MM. Prevention of venous leg ulcer recurrence. Indian Dermatol Online J. 2014 Jul;5(3):386-9.
21. Shepherd AC, Lane RT, Davies AH. The natural progression of chronic venous disorders: An overview of available information from longitudinal
studies. Phlebolymphology. 2012;19(3):138-147.
22. Teo TK, et al. Endovenous laser therapy in the treatment of lower-limb venous ulcers. J Vasc Interv Radiol. 2010 May;21(5):657-62.
23. Ye K, et al. Long-term outcomes of stent placement for symptomatic nonthrombotic iliac vein compression lesions in chronic venous disease. J
Vasc Interv Radiol 2012; 23:497-502.2010 2011 2012 2013 2014 2015
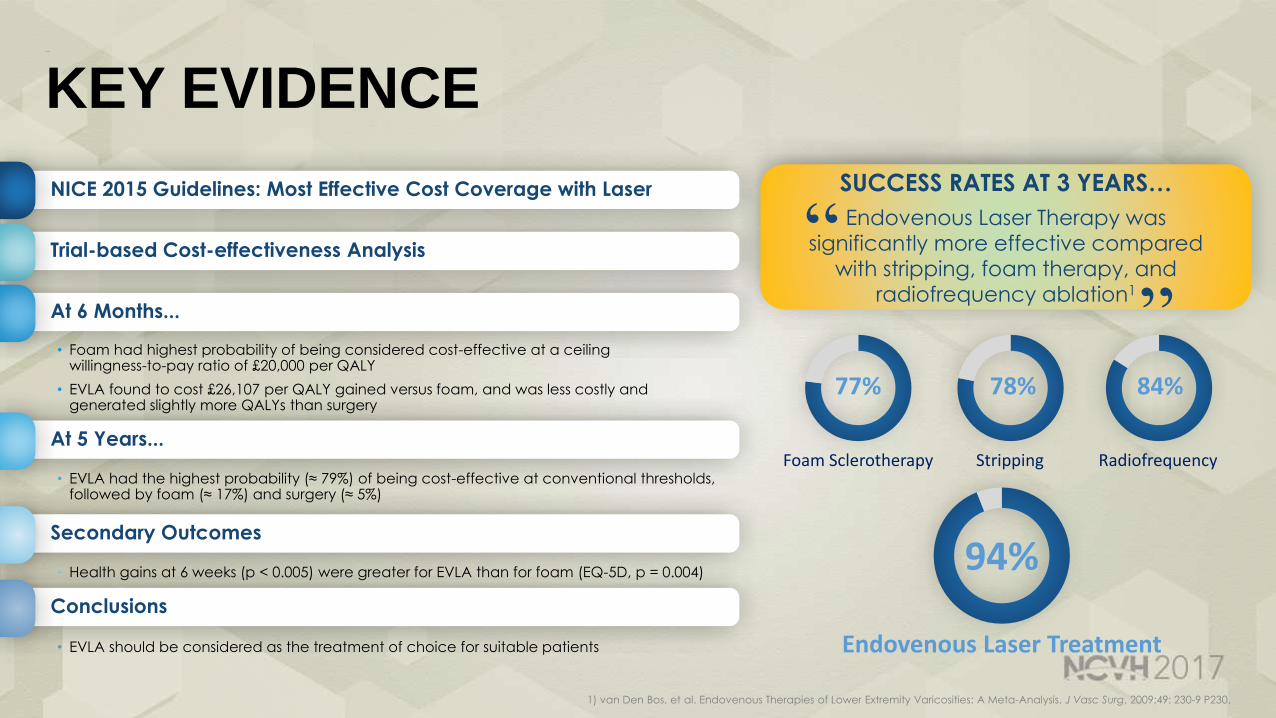
KEY EVIDENCE
1) van Den Bos, et al. Endovenous Therapies of Lower Extremity Varicosities: A Meta-Analysis. J Vasc Surg, 2009;49: 230-9 P230.
78%
Stripping
77%
Foam Sclerotherapy
84%
Radiofrequency
94%
Endovenous Laser Treatment
SUCCESS RATES AT 3 YEARS…
Endovenous Laser Therapy was
significantly more effective compared
with stripping, foam therapy, and
radiofrequency ablation1
“ “
NICE 2015 Guidelines: Most Effective Cost Coverage with Laser
Trial-based Cost-effectiveness Analysis
At 6 Months...
• Foam had highest probability of being considered cost-effective at a ceiling willingness-to-pay ratio of £20,000 per QALY
• EVLA found to cost £26,107 per QALY gained versus foam, and was less costly and generated slightly more QALYs than surgery
At 5 Years...
• EVLA had the highest probability (≈ 79%) of being cost-effective at conventional thresholds, followed by foam (≈ 17%) and surgery (≈ 5%)
Secondary Outcomes
• Health gains at 6 weeks (p < 0.005) were greater for EVLA than for foam (EQ-5D, p = 0.004)
Conclusions
• EVLA should be considered as the treatment of choice for suitable patients
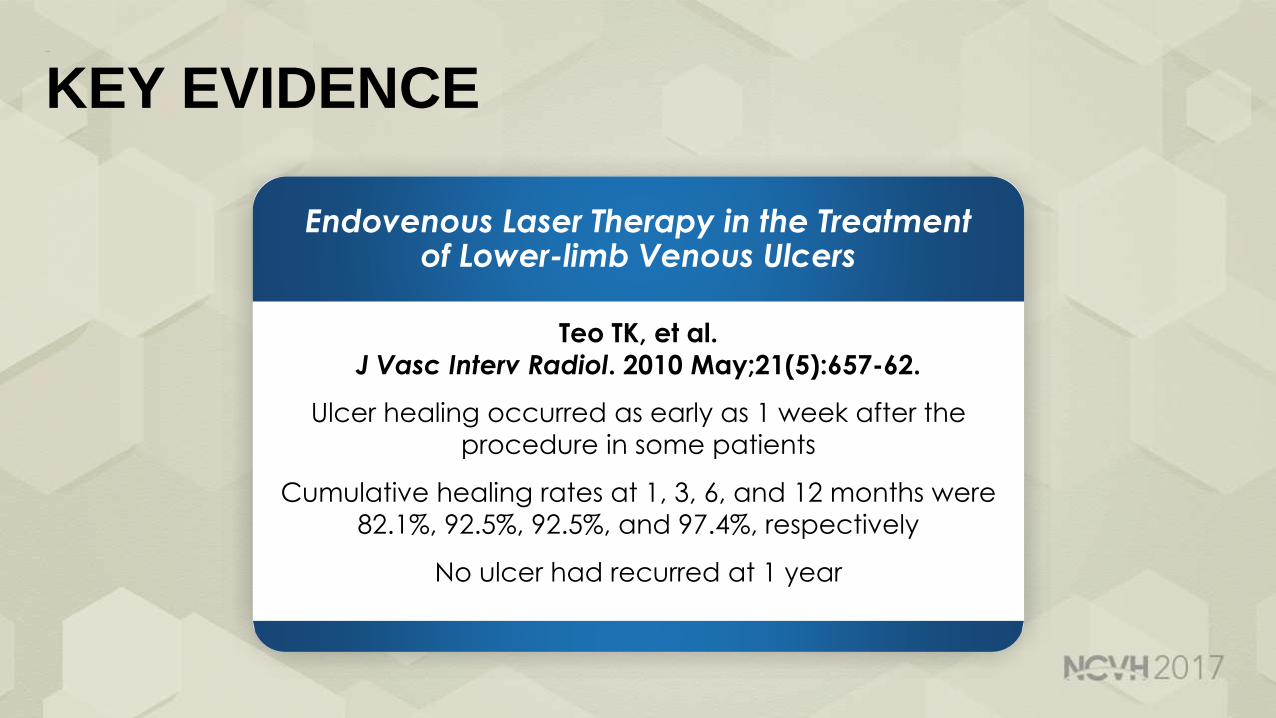
KEY EVIDENCE
Endovenous Laser Therapy in the Treatment of Lower-limb Venous Ulcers
Teo TK, et al.
J Vasc Interv Radiol. 2010 May;21(5):657-62.
Ulcer healing occurred as early as 1 week after the
procedure in some patients
Cumulative healing rates at 1, 3, 6, and 12 months were
82.1%, 92.5%, 92.5%, and 97.4%, respectively
No ulcer had recurred at 1 year

KEY EVIDENCE
Role of Endovenous Laser Treatment in the Management of Chronic Venous Insufficiency
Sharif MA, et al.
Ann Vasc Surg. 2007 Sep;21(5):551-5.
EVLT was used to treat 23 limbs in 20 patients C5 or greater on the
CEAP classification
The cumulative 3- and 12-month healing rates were 87% (20/23) and 100% (23/23)
“These results demonstrate that EVLT, carried out in an outpatient setting, is
effective in the treatment and prevention of chronic venous ulcers, with good
patient satisfaction and no major complication”

SUMMARY
OVER 20 KEY EVLT STUDIES have been published IN THE LAST 5 YEARS
EVLT is CONSISTENTLY CONCLUDED AS BEING MOST EFFECTIVE in the treatment and prevention of chronic venous ulcers
EVLT has NO MAJOR COMPLICATIONS
EVLT has GOOD PATIENT SATISFACTION

THANK YOU!

Robert E. Beasley, MD, FSIR, FSCAIDirector of Vascular/Interventional Radiology
Mount Sinai Medical Center
Miami Beach, FL
Treatments of Superficial Venous Disease: Endovenous Laser Ablation




















![Behcet’s Disease: Radiologic Diagnosis · with Behcet’s disease is the rupture of a large aortic or arterial aneurysm [17]. Venous occlusion: Deep and superficial veins thrombophlebitis](https://img.dokumen.tips/doc/110x75/5ace29797f8b9a875a8eac4b/behcets-disease-radiologic-behcets-disease-is-the-rupture-of-a-large-aortic.jpg)








