Embed Size (px)
Citation preview

Treatment Satisfaction of Internal versus External Cardioversion in Patients with Chronic Atrial Fibrillation—A Randomized, Prospective, 28-Day Follow-Up Study
KARL-HEINZ LADWIG, M.D., PH.D.,*† GÜNTER LEHMANN, M.D.,‡ BIRGITT MARTEN-MITTAG,* HEIDI SIMON, M.D.,* ECKHARD ALT, M.D.‡§
*Institut und Poliklinik für Psychosomatische Medizin, Med. Psychologie und Psychotherapie des Klinikums rechts der Isar der Tech-nischen Universität, Munich; †National Research Centre for Environment and Health, Institute of Epidemiology Munich-Neuherberg;‡Deutsches Herzzentrum and §Medizinische Klinik des Klinikums rechts der Isar der Technischen Universität, Munich, Germany
Summary
Background and hypothesis: The use of internal cardiover-sion (IC) in chronic atrial fibrillation (AF) may be limited byprocedure-related distress. This procedure may be efficaciousbut is not necessarily perceived as satisfactory by the patientbecause of the frequent procedure-related distress.
Methods: We compared treatment satisfaction in 55 pa-tients with chronic AF referred for cardioversion (CV). Satis-faction with conventional external cardioversion (EC, n = 27)and low-energy IC (n = 28) was compared immediately afterthe approach and at 28-day follow-up.
Results: Four hours after CV, satisfaction scores (rangingfrom 0 to 7) were higher with EC (mean 6.1 standard deviation[SD] ± 1.4) versus IC (m = 5.4 SD ± 1.8) (p = 0.09). At 28days, treatment satisfaction decreased in EC (m = 5.5 SD ±2.1) and increased in the IC group (5.7 SD ± 1.8) because of adecrease in the trustful attitude subscale (p = 0.026) followedby tolerance for distressing factors (p = 0.059). The analysis ofvariance for repeated measures revealed a significant time bymethod interaction effect (p = 0.04). Patients prone to develop-ing low treatment satisfaction (LTS) at follow-up were more
anxious (p = 0.007) before treatment. They suffered morefrom sleeping disorders (p = 0.009) and considered their dis-ease condition to be worse than that in their counterparts (p =0.027). Low treatment satisfaction at 28 days was associatedwith anxiety (p = 0.017), depression (p = 0.01), and the per-ception of heart-related symptoms (p = 0.001). Multivariateanalysis revealed the failure to maintain sinus rhythm (p =0.001) as the most powerful contributor to LTS.
Conclusions: The novel IC approach causes acute proce-dure-related distress but has no enduring negative psychologi-cal side effects. Despite a greater patient perception of dis-tressing procedure-related factors during IC compared withEC, the IC approach provides a greater 28-day benefit in termsof tolerability and acceptance on the part of the patients.Failure to maintain sinus rhythm rather than the method ap-plied contributes most to LTS.
Key words: atrial fibrillation, cardioversion, treatment satis-faction
Introduction
Restoration of sinus rhythm is a desirable therapeutic goalin patients with chronic atrial fibrillation (AF). Initially intro-duced in the early 1960s,1 the electrical external cardioversion(EC) in patients with persistent (non-self-terminating) AF isnow recognized as a simple, efficient, and safe technique ifperformed under proper anticoagulation and R-wave synchro-nization.2 In an effort to reduce energy requirements and toprolong maintenance of sinus rhythm, the novel technique oflow-energy internal cardioversion (IC) of AF, using biphasicshocks and two electrode catheters positioned in the right atri-um and the coronary sinus, has been recently devised. Themethod has been proven to be safe and of benefit with respectto primary success rate and long-term effects.3–6
The introduction of new therapeutic approaches in the treat-ment of patients is generally justified by greater efficiency and
Clin. Cardiol. 26, 10–16 (2003)
This study was supported by a grant from the Medical Faculty ofthe Technical University of Munich (KKF-F20-97).
Address for reprints:
K.H. Ladwig Ph.D., M.D. habil, Priv. Doz.Institut u. Poliklinik für Psychosomatische MedizinPsychotherapie u. Med. PsychologieKlinikum rechts der Isar der TUM Langerstrasse 381675 Munich, Germanye-mail: [email protected]
Received: June 1, 2001Accepted: January 8, 2002

K.-H. Ladwig et al.: Treatment satisfaction of IC vs. EC in chronic AF 11
safety. Medical devices that replace established treatmentshould also provide a greater benefit in terms of tolerabilityand acceptance on the part of the patients and thus achieve abetter illness-related quality of life. The latter concept hasgained some attraction in the clinical research of therapeuticconcepts in the context of AF.7–11 Until now, technology as-sessment of low-energy IC compared with the clinical stan-dard, which is EC, has not been extended to the concept oftreatment satisfaction. The impact of the external versus inter-nal approach on the subsequent illness-related quality of lifelikewise has not been the subject of clinical research so far.
In contrast to the EC procedure that requires the adminis-tration of a short-acting narcotic, the IC approach allows ap-plication with low sedation. Although of benefit to the patient,conscious awareness and perception of shock application maycause procedure-related distress which may substantially af-fect treatment satisfaction. We, therefore, performed a ran-domized, prospective trial to determine the effect of EC versusIC in terms of treatment satisfaction in patients with persistentchronic AF. We also sought to identify predictors of low treat-ment satisfaction.
Patients and Methods
The design of the present investigation was a random-ized, prospective follow-up study of patients with chronic AFscheduled for electrical cardioversion. In all, 57 patients wereconsecutively enrolled into the study between January 1, 1997,and December 31, 1997. Written informed consent was ob-tained from all patients. The study was approved by the EthicsCommittee of the Medical Faculty of the Technical Universityof Munich.
Exclusion criteria were evidence of digitalis toxicity, elec-trolyte imbalance, or hyperthyroidism. Furthermore, patientswith a history of a long QT syndrome, a mechanical atrioven-tricular valve prosthesis, and a history of thromboembolismwere excluded from the study, as were patients with an acutemyocardial infarction or cardiopulmonary surgery within thepreceding 6 weeks.
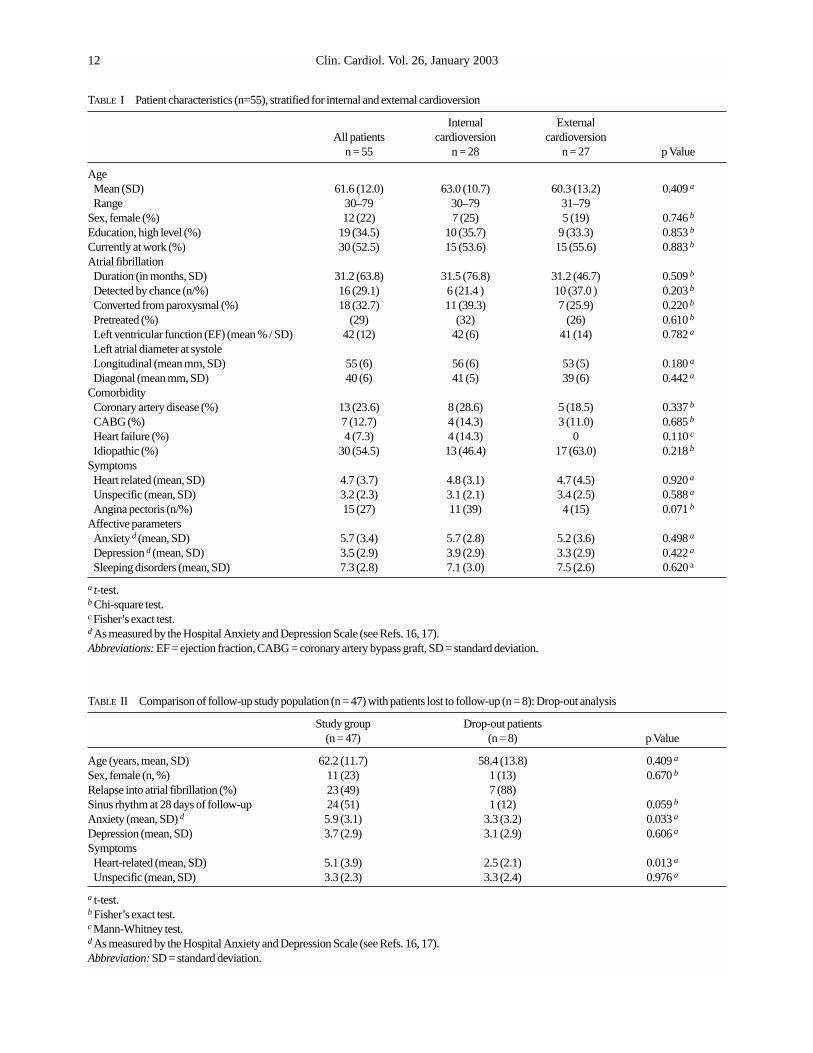
Of the 57 patients enrolled, 2 refused to participate. Thus, atbaseline investigation, the study group comprised 55 patientswith a mean age of 61.6 years (standard deviation [SD] 12.0;range 30–79 years). There were 43 (78%) male and 12 (22%)female patients. Internal cardioversion was performed in 28patients and EC in 27 patients. The randomization achievedbalanced characteristics of the patients with respect to so-ciodemographic, clinical, and psychological factors (Table I).
The follow-up investigation at 28 days post interventionwas carried out in 47 patients. Patients in the study group ex-hibited a higher prevalence of heart-specific symptoms and ahigher mean level of anxiety than did the eight (14.5%) drop-out patients (Table II).
An extensive clinical examination was performed in all pa-tients. Prior to their hospital stay, all patients were treated withwarfarin for at least 4 weeks before admission to achieve ef-fective anticoagulation. Warfarin was withheld 48 h prior to IC
in order to reduce the risk of bleeding from puncture sites andwas substituted by intravenous administration of heparin (fordetails see Ref. No. 12).
Treatment
Under the supervision of an anesthetist, patients undergoingEC were given a short-acting narcotic (methohexital). Directcurrent EC was performed by means of two paddles, placed on the anterior chest wall and in an axillary position. One to a maximum of three R wave-triggered shocks of increasing energy (200, 360, and again 360 J) were applied. In case offailure of the second 360 J energy shock, 150 mg amiodaronewas administered intravenously, and a final attempt with 360 Jwas made.
The protocol for the IC included the delivery of biphasicshocks of 3 ms pulse duration, each with phases separated by0.2 ms and synchronized to the R wave through an externaldefibrillator. Energy was transmitted via custom-built 6-Fcatheters with an active surface of 2.5 cm2. The first catheter,forming the anode, was positioned in the lower right atrium toachieve firm contact with the right atrial free wall. The secondcatheter was placed at random either in the coronary sinus orthe left pulmonary artery. One to a maximum of five R wave-triggered shocks of increasing energy (3–15 J) were applied.Analogously, in case of failure of the last shock, 150 mg amio-darone was administered intravenously and a final attemptwith 15 J was made.
Prior to the IC cardioversion treatment, patients were ini-tially presedated with 5 mg of diazepam orally. If patients re-ported discomfort in the gradual step-up protocol with a lowstarting intensity of 60 V (0.1 J) as test shock, 2.0 to 12 mg mi-dazolam were administered intravenously. Criteria for discon-tinuation were complications, such as proarrhythmia or majorbleeding, persistent patient discomfort, and shock energies> 15 J (for further technical details of the treatment protocolsee Ref. No. 5).
In the 14 patients in whom the initially assigned cardiover-sion (CV) modality failed (9 IC,5 EC), the alternative CVmethod was performed on the following day. Referring to theintent-to-treat approach, treatment satisfaction was evaluatedwith reference to the originally assigned CV method.
Assessment of treatment satisfaction: Treatment satisfac-tion was based on an investigator-developed instrument in-cluding 7 dichotomised items (range 0–7) that assess two di-mensions of the treatment approach (range 0–1): (1) a generaltrustful attitude toward the procedure (“advise it for everyone,repeat it at any time, provides feelings of security and shelter,optimistic outcome expectancy in the context of the diseaseprocess”); and (2) awareness of distressing factors togetherwith the treatment approach (“experiencing the approach wasmore distressing than expected, perceive feelings of anxietywhen recollecting the treatment procedure, was aware ofcomplicating factors during treatment”).
The items were selected after semistructured interviewswith patients with coronary disease and were peer reviewed bycardiologists of the department. The internal consistency of
Clin. Cardiol. Vol. 26, January 200312
TABLE I Patient characteristics (n=55), stratified for internal and external cardioversion
Internal External All patients cardioversion cardioversion
n = 55 n = 28 n = 27 p Value
Age Mean (SD) 61.6 (12.0) 63.0 (10.7) 60.3 (13.2) 0.409 a
Range 30–79 30–79 31–79Sex, female (%) 12 (22) 7 (25) 5 (19) 0.746 b
Education, high level (%) 19 (34.5) 10 (35.7) 9 (33.3) 0.853 b
Currently at work (%) 30 (52.5) 15 (53.6) 15 (55.6) 0.883 b
Atrial fibrillationDuration (in months, SD) 31.2 (63.8) 31.5 (76.8) 31.2 (46.7) 0.509 b
Detected by chance (n/%) 16 (29.1) 6 (21.4 ) 10 (37.0 ) 0.203 b
Converted from paroxysmal (%) 18 (32.7) 11 (39.3) 7 (25.9) 0.220 b
Pretreated (%) (29) (32) (26) 0.610 b
Left ventricular function (EF) (mean % / SD) 42 (12) 42 (6) 41 (14) 0.782 a
Left atrial diameter at systoleLongitudinal (mean mm, SD) 55 (6) 56 (6) 53 (5) 0.180 a
Diagonal (mean mm, SD) 40 (6) 41 (5) 39 (6) 0.442 a
ComorbidityCoronary artery disease (%) 13 (23.6) 8 (28.6) 5 (18.5) 0.337 b
CABG (%) 7 (12.7) 4 (14.3) 3 (11.0) 0.685 b
Heart failure (%) 4 (7.3) 4 (14.3) 0 0.110 c
Idiopathic (%) 30 (54.5) 13 (46.4) 17 (63.0) 0.218 b
SymptomsHeart related (mean, SD) 4.7 (3.7) 4.8 (3.1) 4.7 (4.5) 0.920 a
Unspecific (mean, SD) 3.2 (2.3) 3.1 (2.1) 3.4 (2.5) 0.588 a
Angina pectoris (n/%) 15 (27) 11 (39) 4 (15) 0.071 b
Affective parametersAnxiety d (mean, SD) 5.7 (3.4) 5.7 (2.8) 5.2 (3.6) 0.498 a
Depression d (mean, SD) 3.5 (2.9) 3.9 (2.9) 3.3 (2.9) 0.422 a
Sleeping disorders (mean, SD) 7.3 (2.8) 7.1 (3.0) 7.5 (2.6) 0.620 a
a t-test.b Chi-square test. c Fisher’s exact test.d As measured by the Hospital Anxiety and Depression Scale (see Refs. 16, 17).Abbreviations: EF = ejection fraction, CABG = coronary artery bypass graft, SD = standard deviation.
TABLE II Comparison of follow-up study population (n = 47) with patients lost to follow-up (n = 8): Drop-out analysis
Study group Drop-out patients (n = 47) (n = 8) p Value
Age (years, mean, SD) 62.2 (11.7) 58.4 (13.8) 0.409 a
Sex, female (n, %) 11 (23) 1 (13) 0.670 b
Relapse into atrial fibrillation (%) 23 (49) 7 (88)Sinus rhythm at 28 days of follow-up 24 (51) 1 (12) 0.059 b
Anxiety (mean, SD) d 5.9 (3.1) 3.3 (3.2) 0.033 a
Depression (mean, SD) 3.7 (2.9) 3.1 (2.9) 0.606 a
SymptomsHeart-related (mean, SD) 5.1 (3.9) 2.5 (2.1) 0.013 a
Unspecific (mean, SD) 3.3 (2.3) 3.3 (2.4) 0.976 a
a t-test.b Fisher’s exact test.c Mann-Whitney test.d As measured by the Hospital Anxiety and Depression Scale (see Refs. 16, 17).Abbreviation: SD = standard deviation.

K.-H. Ladwig et al.: Treatment satisfaction of IC vs. EC in chronic AF 13
the total scale was 0.81 Cronbach’s alpha (general trustful atti-tude subscale 0.77; distress subscale 0.62) and thus achievedsufficient consistency.
Treatment satisfaction was assessed about 4 h after the car-dioversion treatment and again after 28 days. The 28-day end-point measurement was carried out on a self-administeredquestionnaire which was remailed by the patients.
Psychodiagnostic Assessment
Anxiety and depression were evaluated using the 14-itemHospital Anxiety and Depression Scale,15 with publishednorms obtained from a German standard population.16 In ad-dition, patients’ emotional distress level, vital exhaustion, andsleeping disorders17 were measured.
An AF-related symptom checklist contained eight symp-toms (palpitation, heart racing, fluttering, dizziness, missingheart beats, shortness of breath, short episodes of loss of con-sciousness, restlessness) and ranged from 0 to 16. Nonspecificsymptoms were assessed with the Zerssen symptom check listin an abridged version,13 ranging from 0 to 10. Psychodiag-nostic and symptom assessment was carried out in about 4 hbefore the treatment procedure.
Statistical Analysis
Mean values are presented as mean ±SD. Group differencesin normally distributed continuous variables were analyzed bythe t-test for three independent groups. The Mann-Whitney testwas used to analyze group differences for continuous variableswhere the assumption of normal distribution was violated.Categorical variables were tested for equal distribution usingthe Pearson test (chi square) and, depending on sample size,Fisher’s exact test, respectively.
To test for changes from baseline to follow-up in non-nor-mally distributed continuous variables, we applied Wilcoxon’ssigned rank test. Changes in treatment satisfaction scores overtime and CV method applied were analyzed by one-factoranalysis of variance for repeated measures.
We used stepwise logistic regression analysis as a multivari-ate model to identify the independent contribution of variousvariables to predict 28-day patient satisfaction. Differenceswere considered significant with a probability value of <0.05.Statistical analysis was carried out on Statistical Package forSocial Sciences, version 9.0 (SPSS, Inc., Chicago, Ill., USA).
Results
In all, 55 patients were randomly assigned to either the IC (n = 28) or the EC (n = 27) treatment group. After a follow-upperiod of 28 days, 47 patients (23 patients in the IC group, 24patients in the EC group) were reexamined. Sinus rhythm wasmaintained in 24 of 47 patients.
1. The overall treatment satisfaction immediately followingthe procedure (ranging between 0 = low and 7 = high) reached
a mean value of 5.8 (SD ± 1.7). Initial mean treatment satisfac-tion was higher in the EC group (6.1 SD ± 1.4) than in the ICgroup (5.4 SD ± 1.8). Differences in mean scores betweengroups were of borderline significance (Mann-Whitney test, p = 0.09). Subscale analysis revealed that the difference wasdue to the greater awareness of distressing factors during theprocedure in the IC group (p = 0.049), while there were no sig-nificant differences between both groups concerning a generaltrustful attitude toward the CV approach.
At 28 days, the preferences between the treatment groupshad changed: now, mean treatment satisfaction increased to5.7 ± 1.8 in the IC group and decreased to 5.5 (SD ± 2.1) in theEC group. The analysis of variance for repeated measures re-vealed a significant time by method interaction effect (p =0.04) (Fig. 1).
The turnover of treatment satisfaction scores over the 28-day follow-up period is mainly based on a downgrading of sat-isfaction scores in the EC group. As can be seen in Figure 2,both subscales significantly dropped over the time span in the
FIG. 1 Mean treatment satisfaction scores for external cardiover-sion (EC, ■ ) and internal cardioversion (IC, ■■ ) at two study points:4 h post treatment and 28 days post treatment (scores in means andstandard error of the means). Analysis of variance for repeated mea-sures (p = 0.04).
4 Hours3
4
5
6
7
28 Days
Trea
tmen
t sa
tisfa
ctio
n
4 HoursTA TDF TA TDF
0.5
1.0
1.5
p = 0.059**
p = 0.049*
p = 0.026**
28 Days
Sco
re (m
ean
[SD
])
FIG. 2 Mean treatment satisfaction scores at Day 0 and at Day 28,stratified into the subscales: (a) general trustful attitude toward thetreatment approach (TA) and (b) tolerance for distressing treatmentfactors (TDF) * = Mann-Whitney test; ** = Wilcoxon’s signed ranktest. ■ = External cardioversion, ■ = internal cardioversion.
Clin. Cardiol. Vol. 26, January 200314
EC group (general trustful attitude, p = 0.026 and tolerance to-ward distressing factors p = 0.059). Correspondingly, bothsubscale scores increased moderately in the IC group.
The mean overall treatment satisfaction score at study endwas 6.5 (SD ± 1.0) in the patient group with maintained sinusrhythm (n = 24) and was 4.5 (SD ± 2.1) in the group with re-currence of AF (n = 23) (p = 0.0001). The result proves thatdifferences in treatment satisfaction attributed to the differentapproaches are less pronounced by far than differences causedby the final therapeutic result achieved.
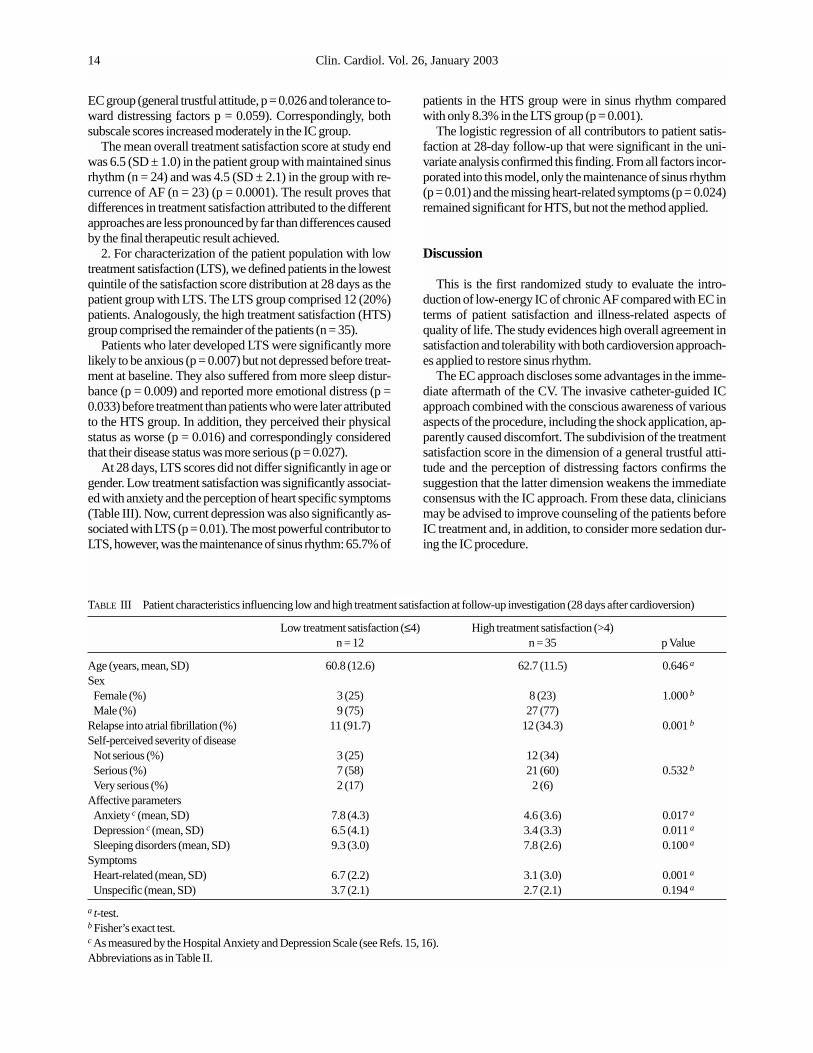
2. For characterization of the patient population with lowtreatment satisfaction (LTS), we defined patients in the lowestquintile of the satisfaction score distribution at 28 days as thepatient group with LTS. The LTS group comprised 12 (20%)patients. Analogously, the high treatment satisfaction (HTS)group comprised the remainder of the patients (n = 35).
Patients who later developed LTS were significantly morelikely to be anxious (p = 0.007) but not depressed before treat-ment at baseline. They also suffered from more sleep distur-bance (p = 0.009) and reported more emotional distress (p =0.033) before treatment than patients who were later attributedto the HTS group. In addition, they perceived their physicalstatus as worse (p = 0.016) and correspondingly consideredthat their disease status was more serious (p = 0.027).
At 28 days, LTS scores did not differ significantly in age orgender. Low treatment satisfaction was significantly associat-ed with anxiety and the perception of heart specific symptoms(Table III). Now, current depression was also significantly as-sociated with LTS (p = 0.01). The most powerful contributor toLTS, however, was the maintenance of sinus rhythm: 65.7% of
patients in the HTS group were in sinus rhythm comparedwith only 8.3% in the LTS group (p = 0.001).
The logistic regression of all contributors to patient satis-faction at 28-day follow-up that were significant in the uni-variate analysis confirmed this finding. From all factors incor-porated into this model, only the maintenance of sinus rhythm(p = 0.01) and the missing heart-related symptoms (p = 0.024)remained significant for HTS, but not the method applied.
Discussion
This is the first randomized study to evaluate the intro-duction of low-energy IC of chronic AF compared with EC interms of patient satisfaction and illness-related aspects ofquality of life. The study evidences high overall agreement insatisfaction and tolerability with both cardioversion approach-es applied to restore sinus rhythm.
The EC approach discloses some advantages in the imme-diate aftermath of the CV. The invasive catheter-guided IC approach combined with the conscious awareness of variousaspects of the procedure, including the shock application, ap-parently caused discomfort. The subdivision of the treatmentsatisfaction score in the dimension of a general trustful atti-tude and the perception of distressing factors confirms thesuggestion that the latter dimension weakens the immediateconsensus with the IC approach. From these data, cliniciansmay be advised to improve counseling of the patients beforeIC treatment and, in addition, to consider more sedation dur-ing the IC procedure.
TABLE III Patient characteristics influencing low and high treatment satisfaction at follow-up investigation (28 days after cardioversion)
Low treatment satisfaction (≤4) High treatment satisfaction (>4)n = 12 n = 35 p Value
Age (years, mean, SD) 60.8 (12.6) 62.7 (11.5) 0.646 a
Sex Female (%) 3 (25) 8 (23) 1.000 b
Male (%) 9 (75) 27 (77)Relapse into atrial fibrillation (%) 11 (91.7) 12 (34.3) 0.001 b
Self-perceived severity of diseaseNot serious (%) 3 (25) 12 (34)Serious (%) 7 (58) 21 (60) 0.532 b
Very serious (%) 2 (17) 2 (6)Affective parametersAnxiety c (mean, SD) 7.8 (4.3) 4.6 (3.6) 0.017 a
Depression c (mean, SD) 6.5 (4.1) 3.4 (3.3) 0.011 a
Sleeping disorders (mean, SD) 9.3 (3.0) 7.8 (2.6) 0.100 a
SymptomsHeart-related (mean, SD) 6.7 (2.2) 3.1 (3.0) 0.001 a
Unspecific (mean, SD) 3.7 (2.1) 2.7 (2.1) 0.194 a
a t-test.b Fisher’s exact test.c As measured by the Hospital Anxiety and Depression Scale (see Refs. 15, 16).Abbreviations as in Table II.

K.-H. Ladwig et al.: Treatment satisfaction of IC vs. EC in chronic AF 15
At 28 days, however, the IC approach gained relativelymore patient support and reached an even higher treatment sat-isfaction level compared with the EC group. Apparently, theperception of acute distressing factors of the procedure con-tained no enduring properties. Treatment satisfaction with theEC method decreased significantly, indicating that patientsachieve an impression of distressing factors even treated witha short-acting narcotic. These findings may be helpful in thetherapeutic decision process for the considerably high propor-tion of patients in whom sinus rhythm cannot be maintained.
Treatment satisfaction research19–25 has shown that veryfew patients express dissatisfaction or are critical of their care.Especially in the face of highly technical treatments,22 patientsmay not believe in the legitimacy of their own expectationseven when they are at odds with their own individual experi-ence. Thus, the ceiling effect of overall treatment satisfactionobserved in the present study may be due to patients’ per-ceived dependence on the therapy applied. This effect may ex-plain why a relatively high level of treatment satisfaction ispresent even in patients in whom sinus rhythm was not main-tained after CV.
Patients with LTS are sometimes difficult to manage on aclinical basis. Therefore, it is useful to gain some deeper in-sights into those patients denying the benefits of the therapy.18
Social class, marital status, gender, and age (in line with otherempirical studies19, 22) did not promote LTS. Hall et al.24 foundthat patients who labeled themselves as sicker were less satis-fied with their medical care. This finding is supported by thedata of the present study. Less satisfied patients also consid-ered their disease status to be more severe.
Little work has examined possible associations betweenpatients’ psychological status and treatment satisfaction.22
The data reveal that LTS was significantly associated withemotional distress, anxiety, and sleeping disturbances. Thestrong association between LTS and failure to maintain sinusrhythm and the subsequent characterization of these patientsas emotionally distressed raises the question whether theremay be an interaction between high prevalence of affectivedysfunction and the failure to maintain sinus rhythm. This in-teraction deserves particular attention and will be subject tofurther analysis.
The most powerful contributor to treatment satisfaction,however, was the success of the approach applied. In patientsin whom sinus rhythm could not be restored or maintained,LTS was prevalent in 73% of cases at study end. The successparameter contributed far more to the discrimination betweenthe LST and HST groups than any other factor, including thetwo different approaches under evaluation. It is notable thateven rather distressing factors during the IC procedure, such asthe perception of high levels of intracardiac pain,25–27 do nothave influence on the 28-day patient mean satisfaction level.
A limitation of the study should be noted. Eight (14.5%) pa-tients who were less affected by symptoms of psychologicaldysfunction and by heart-related pain at study entry were lostto follow-up. Thus, the conclusions of the study might be morerelevant to symptomatic patients.
Conclusion
The novel technique of IC can be applied with low seda-tion, which is of benefit for the patient but may cause psycho-logical harm because of procedure-related distress. Beyondthe visceral pain component, internal shock application mayalso lead to an affective response in the patients. In fact, thepresent study confirms a short-term distress effect in patientsundergoing the IC procedure, which has, however, no endur-ing properties. Nevertheless, a considerable proportion of pa-tients reported low treatment satisfaction because of adverseshock perception. It therefore appears advisable to increasesedation routinely over > 5 mg of diazepam.
At 28 days after the CV, patients have a less distressing rec-ollection of the approach, which results in a somewhat higherlevel of treatment satisfaction with the IC compared with theEC approach. Thus, the present study reveals that the introduc-tion of the novel IC approach has no persistent negative psy-chological side effects. Clinicians may, however, be advisedfrom these data to improve patient counseling before IC treat-ment so that the patient does not underestimate the acute pro-cedure-related distress.
No relevant affective differences between treatment groupswere observed. However, when the study group was dividedinto patients with and without successfully restored sinusrhythm, pronounced differences in almost all behavioral out-come measurements emerged. The high level of disease-relat-ed suffering in patients with chronic AF deserves further atten-tion. These findings further improve the awareness of AF as aserious “disease” and support a more aggressive managementof this condition.28
References
1. Lown B, Amarasingham R, Neumann J: New method for terminating car-diac arrhythmias—use of synchronized capacitator discharge. J Am MedAssoc 1962;182:548–555
2. Levy S, Breithardt G, Campbell RWF, Camm AJ, Daubert J-C, Allessie M,Aliot E, Capucci A, Cosio F, Crijns H, Jordaens L, Haver RNW, LombardiF, Lüderitz B, on behalf of the Working Group on Arrhythmias of theEuropean Society of Cardiology: Atrial fibrillation: Current knowledge andrecommendations for management. Eur Heart J 1998;19:1294–1320
3. Murgatroyd FD, Slade AKB, Sopher SM, Rowland E, Ward DE, Camm J:Efficacy and tolerability of transvenous low energy cardioversion of parox-ysmal atrial fibrillation in humans. J Am Coll Cardiol 1995;25:1347–1353
4. Schmitt C, Alt E, Plewan A, Ammer R, Leibig M, Karch M, Schömig A:Low energy intracardiac cardioversion after failed conventional externalcardioversion of atrial fibrillation. J Am Coll Cardiol 1996;28:994–999
5. Alt E, Ammer R, Schmitt C, Evans F, Lehmann G, Pasquantonio J, SchömigA: A comparison of treatment of atrial fibrillation with low-energy intracar-diac cardioversion and conventional external cardioversion. Eur Heart J1997;18:1796–1804
6. Neri R, Palermo P, Cesario AS, Baragli D, Amici E, Gambelli G: Internalcardioversion of chronic atrial fibrillation in patients. PACE 1997;20:2237–2242
7. Jung W, Tebbenjohanns J, Wollpert C, Lüderitz B: Safety, efficacy, andpain perception of internal atrial defibrillation in humans (abstr). Circulation1995;92(suppl I):I-472
8. Kay GN, Bubien RS, Epstein AE, Plumb VJ: Effect of catheter ablation ofthe atrioventricular junction on quality of life and exercise tolerance inparoxysmal atrial fibrillation. Am J Cardiol 1988;62:741–744
9. Lancaster TR, Singer DE, Sheehan MA, Oertel MA, Maraventano SW,Hughes RA, Kistler JP: The impact of long-term warfarin therapy on quali-ty of life. Evidence from a randomized trial. Boston Area Anticioagulation
Clin. Cardiol. Vol. 26, January 200316
Trial for Atrial Fibrillation Investigators. Arch Intern Med 1991;151:1944–1949
10. Brignole M, Gianfranchi L, Menozzi C, Bottoni N, Bollini R, Lollo G,Oddone D, Gaggioli G: Influence of atrioventricular junction radiofrequen-cy ablation in patients with chronic atrial fibrillation and flutter on quality oflife and cardiac performance. Am J Cardiol 1994;74:242–246
11. Jung W, Lüderitz B: Quality of life in patients with atrial fibrillation. J Cardiovasc Electrophysiol 1998;9(suppl):S177–S186
12. Lehmann G, Horcher J, Dennig K, Plewan A, Ulm K, Alt E, Schömig A:Atrial mechanical performance following internal or external cardioversionof atrial fibrillation: An echocardiographic study. Chest 2002;121:13–18
13. von Zerssen D: Die Beschwerden-Liste. Göttingen: Hogrefe, 197614. McHorney CA, Ware JE, Raczek AE: The MOS 36-item short form health
status survey (SF36). II: Psychometric and clinical tests of validity in mea-suring physical and mental health constructs. Med Care 1993;31:247–263
15. Zigmond AS, Snaith RP: The hospital anxiety and depression scale. ActaPsychiatr Scand 1983;67:361–370
16. Herrmann CH, Buss U, Snaith RP: Psychologisches Screening vonPatienten einer kardiologischen Akutklinik mit einer deutschen Fassung der“Hospital anxiety and depression (HAD)” Scala. Psychother PsychosomMed Psychol 1991;41:83–92
17. Appels AP, Mulder P: Excess fatigue as a precursor of myocardial infarc-tion. Eur Heart J 1988;9:758–764
18. Abramowitz S, Cote AA, Berry E: Analyzing patient satisfaction: A multi-analytic approach. Quality Rev Bull 1987;13:122–130
19. Hopton JL, Howie JGR, Porter MD: The need for another look at the patientin general practice satisfaction surveys. J Fam Pract 1993;10:82–87
20. Langewitz W, Keller A, Denz M, Woessmer-Buntschu B, Kiss A: The pa-tient satisfaction questionnaire: A suitable tool for quality control in thephysician-patient relationship? Psychother Psychosom Med Psych 1995;45:351–357
21. Sitzia J, Wood N: Patient satisfaction: A review of issues and concepts. SocSci Med 1997;45:1829–1843
22. Fox JG, Storms DM: A different approach to sociodemographic predictorsof satisfaction with health care. Soc Sci Med 1981;15:557–564
23. Schmeling-Kludas C: Treatment satisfaction and cooperation in the hospitaland general practice: Attitude of an internal medicine patient sample andphysicians responsible for their treatment? Psychother Psychosom MedPsych 1995;45:193–201
24. Hall JA, Milburn MA, Daltroy LH: Why are sicker patients less satisfiedwith their medical care? Tests of two explanatory models. Health Psychol1998;17:70–75
25. Boriani G, Biffi M, Bronzetti G, Ayers GM, Zannoli R, Branzi A, CapucciA, Magnani B: Efficacy and tolerability in fully conscious patients oftransvenous low-energy internal atrial cardioversion for atrial fibrillation.Am J Cardiol 1998;81:241–244
26. Jung J, Heisel A, Fries R, Koellner V: Tolerability of internal low-energyshock strengths currently needed for endocardial atrial cardioversion. Am JCardiol 1997;80:1489–1490
27. Timmermanns C, Rodriguez LM, Ayers GM, Lambert H, Smeets JL,Vlaeyen JW, Albert A, Wellens HJ: Effect of butorphanol tartrate on shock-related discomfort during internal atrial defibrillation. Circulation 1999;99:1837–1842
28. Waktare JEP, Camm AJ: Acute treatment of atrial fibrillation: Why andwhen to maintain sinus rhythm. Am J Cardiol 1998;81(5a):3C–15C





















