Embed Size (px)
Citation preview

ORIGINAL PAPER
Treatment of ischial pressure sores. Our experience of 99 patientswith 108 sores
Charalambos A. Georgiou & Pierre S. Nguyen &
Zdravska Batchvarova & Cécile Philandrianos &
Jacques Bardot & Dominique Casanova
Received: 24 May 2014 /Accepted: 18 August 2014 /Published online: 19 September 2014# Springer-Verlag Berlin Heidelberg 2014
AbstractBackground Ischial pressure sores concern patients in the sittingposition and particularly the rehabilitated patients. Spontaneoushealing may be very difficult without surgery, and ischial pres-sure sores have the highest recurrence rate among otherdecubitus. Furthermore, there is no consensus concerning theideal surgical technique in order to definitely treat the patients.This is a retrospective analysis of the surgical treatment of ischialpressure sores aiming to identify the ulcer recurrence rate persurgical technique and describe the early complications.Methods This was a retrospective study that was conducted inMarseille, France, between 1988 and 2007. The medical re-cords concerning patients with ischial pressure sores werecollected and analyzed. The main objective was to identifythe ulcer recurrence rate after ischial pressure sore surgicaltreatment. The secondary objective was the identification anddescription of early complications.Results Ninety-nine patients were finally selected and analyzedfor 108 ischial pressure sore treatments. Primary endpoint anal-ysis identified 25 recurrences for 108 sores (23.14 %). Ham-string V-Y advancement flap had 71 % recurrence rate. Wounddehiscence was the primary complication. Six out of sevenhamstring V-Yadvancement flaps had early complications.
Conclusions Pressure sore treatment can be difficult and chal-lenging. In this retrospective study, we have found that thehamstring V-Y advancement flaps have a much higher recur-rence rate and a higher rate of complications. Our results maybe limited by the retrospective nature of this study but theyimply that the V-Yadvancement flaps should not be used as afirst choice for ischial pressure sore treatment.Level of Evidence: Level IV, therapeutic study.
Keywords Ischial pressure sores . Decubitus . Pressureulcers . Hamstring flaps . Gluteus maximusmyocutaneousflaps . V-Yadvancement flaps
Introduction
Pressure sores consist a frequent pathology that the plasticsurgeon is solicited to deal with in the everyday practice.Ischial pressure sores concern usually patients in the sittingposition and particularly the rehabilitated patients that needthis position in their professional and social life. Very oftenthis kind of sore is deep, and the bone prominence of theischion is exposed. Its dimensions can be easilyunderestimated, as the skin defect may be very small makingthe sore sinusoid, and very often, spontaneous healing forthese chronic ulcers may be very difficult without surgery.
Care workers consider this kind of decubitus as the mostdifficult to cure because of the high recurrence rate [1]. Al-though Conway and Griffith [2] initially estimated this rate atapproximately 75 %, it has been more recently decreased to20 % [3] as a result of multidisciplinary patient care, preven-tive equipment, and better treatment protocol. Nevertheless,ischial pressure sores have the highest recurrence rate amongother pressure sores.
Furthermore, there is no consensus concerning the idealsurgical technique in order to definitely treat the patients.
C. A. Georgiou : P. S. Nguyen : Z. Batchvarova : J. Bardot :D. CasanovaPlastic, Reconstructive and Aesthetic Surgery Department,La Conception University Hospital, 147 Boulevard Baille,13005 Marseille, France
C. A. Georgiou (*)Plastic Reconstructive and Aesthetic Surgery Department, St RochUniversity Hospital of Nice, 5 Pierre Devoluy, 0600 Nice, Francee-mail: [email protected]
C. PhilandrianosPlastic, Reconstructive and Aesthetic Surgery Department, HôpitalNord, University Hospital, Chemin des Bourrely, 13915 Marseille,France
Eur J Plast Surg (2014) 37:667–672DOI 10.1007/s00238-014-1014-9
Many authors propose myocutaneous or muscular flaps so asto fill adequately the wound cavity and cover the surface of thesore at the same time [4]. For some authors, the flap that ismost suitable is the gluteous maximus myocutaneous flap [5,6]. For others posterior thigh-based flaps such as hamstringmyocutaneous advancement in a V-Y manner are preferred[7–9]. Even gracilis myocutaneous flap as well as tensorfasciae latae flap were proposed as possible solutions for thetreatment of this kind of sores [10]. More recently, perforatorfasciocutaneous flaps were proposed [11, 12]. However, thechoice between fasciocutaneous and myocutaneous or mus-cular flaps remains debatable [13, 14] even though evidenceexists that flaps containing muscle may implement local cel-lular differentiation and healing [15]. In every case thoughwound dimensions, previous surgeries, and scars must influ-ence the choice having as a principle the golden rule of tissueeconomy in order to address future recurrences.
We have conducted a retrospective analysis of the surgicaltreatment of ischial pressure sores aiming to identify the ulcerrecurrence rate per surgical technique and describe the earlycomplications.
Material and methods
This was a retrospective and descriptive study that was con-ducted in two centers (Hôpital Nord and Hôpital La Concep-tion) in Marseille, France, between 1988 and 2007. We col-lected and analyzed all of the medical records concerningpatients with pressure sores. Among them, we selected themedical records of patients with ischial pressure sores. Wethen proceeded to a descriptive analysis of patient character-istics, ulcer characteristics, treatment, and evolution. The mainobjective was to identify the ulcer recurrence rate after ischialpressure sore surgical treatment. Recurrence was defined asthe pressure sore (Stage >II) located at the initial sore’s loca-tion after complete healing and after permitting the sitedposition. The secondary objective of this study was the iden-tification and description of early complications. Complica-tions included wound dehiscence, hematoma, partial or totalflap loss, and postoperative skin fistulas. Early was defined asthe complications that occurred within the first postoperatorymonth.
All of the patients were treated with the same care protocolthat was identical for the two centers. It included:
1. An initial preoperative phase. In this phase, the candidatesfor surgery were hospitalized and prepared for operation.Preparation included nutrition, fluid resuscitation, anemia,and other deficiency correction. At the same time, localcare was intensified in order to acquire a clean wound. Forneglected cases, surgical debridement took place so as toacquire a suitable wound for coverage.
2. Second phase concerned the main surgery for coverage orwound closure. For all patients, a superficial excision ofwound walls and bursal sac as well as bone contouringtook place before closing or covering the wound. Thenwound closure or coverage followed according to classicsurgical techniques:
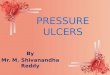
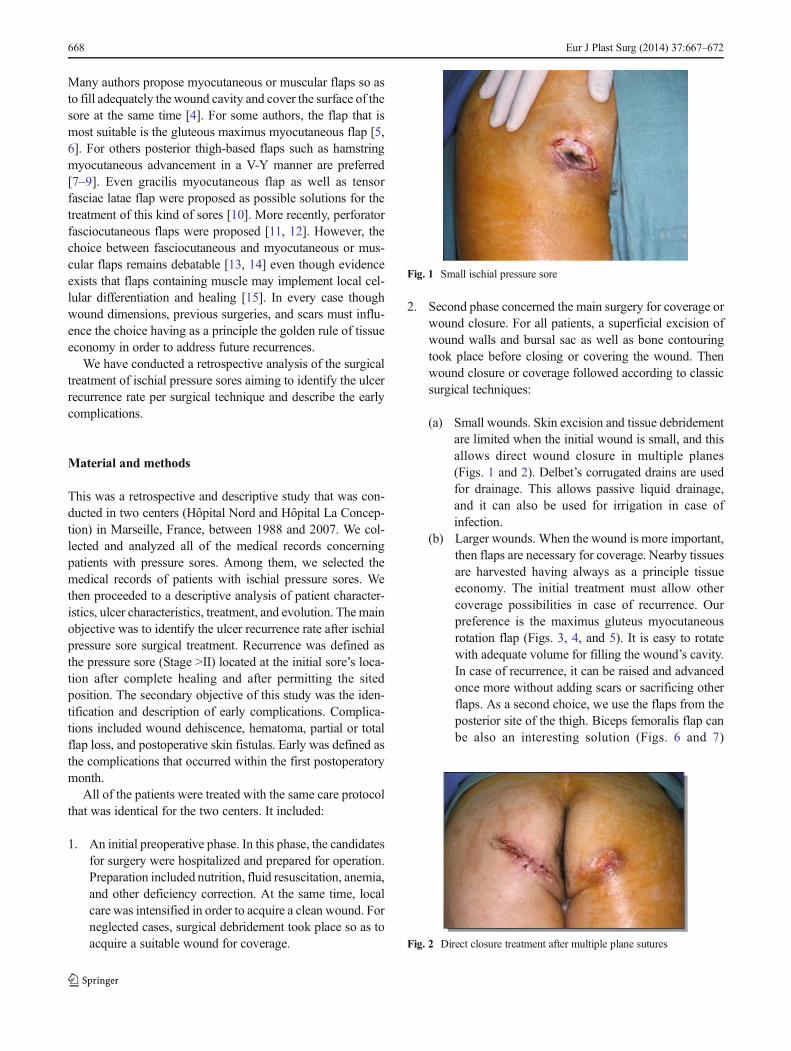
(a) Small wounds. Skin excision and tissue debridementare limited when the initial wound is small, and thisallows direct wound closure in multiple planes(Figs. 1 and 2). Delbet’s corrugated drains are usedfor drainage. This allows passive liquid drainage,and it can also be used for irrigation in case ofinfection.
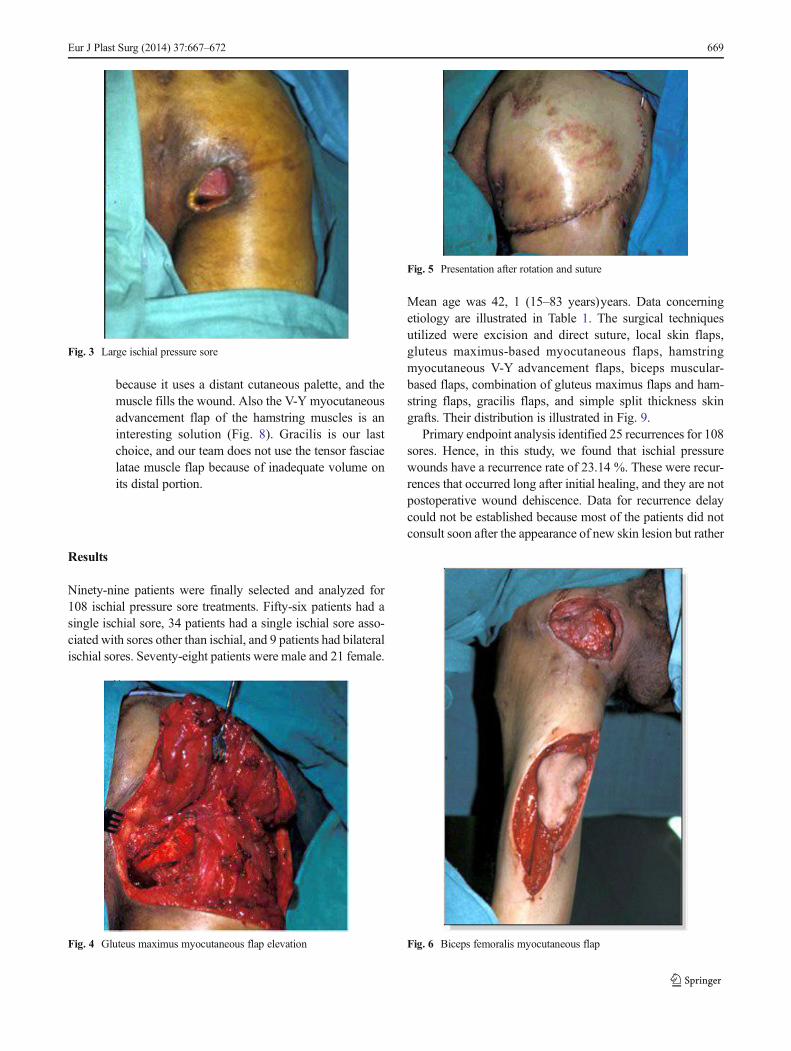
(b) Larger wounds. When the wound is more important,then flaps are necessary for coverage. Nearby tissuesare harvested having always as a principle tissueeconomy. The initial treatment must allow othercoverage possibilities in case of recurrence. Ourpreference is the maximus gluteus myocutaneousrotation flap (Figs. 3, 4, and 5). It is easy to rotatewith adequate volume for filling the wound’s cavity.In case of recurrence, it can be raised and advancedonce more without adding scars or sacrificing otherflaps. As a second choice, we use the flaps from theposterior site of the thigh. Biceps femoralis flap canbe also an interesting solution (Figs. 6 and 7)
Fig. 1 Small ischial pressure sore
Fig. 2 Direct closure treatment after multiple plane sutures
668 Eur J Plast Surg (2014) 37:667–672
because it uses a distant cutaneous palette, and themuscle fills the wound. Also the V-Y myocutaneousadvancement flap of the hamstring muscles is aninteresting solution (Fig. 8). Gracilis is our lastchoice, and our team does not use the tensor fasciaelatae muscle flap because of inadequate volume onits distal portion.
Results
Ninety-nine patients were finally selected and analyzed for108 ischial pressure sore treatments. Fifty-six patients had asingle ischial sore, 34 patients had a single ischial sore asso-ciated with sores other than ischial, and 9 patients had bilateralischial sores. Seventy-eight patients were male and 21 female.
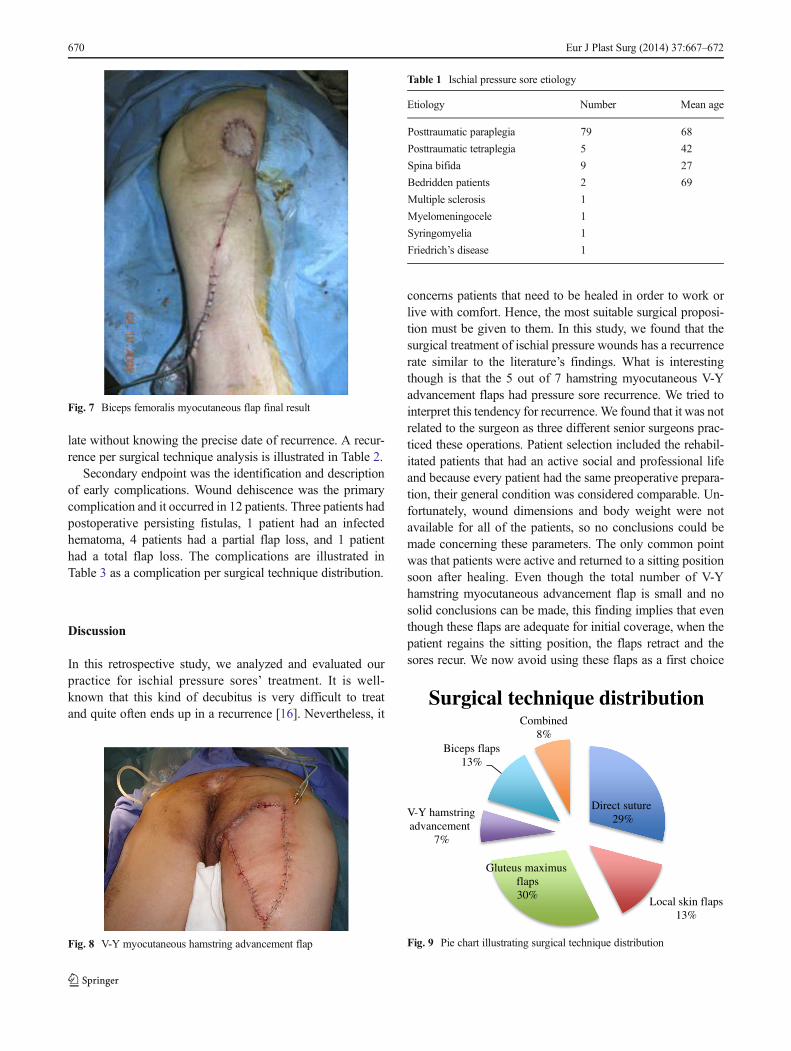
Mean age was 42, 1 (15–83 years)years. Data concerningetiology are illustrated in Table 1. The surgical techniquesutilized were excision and direct suture, local skin flaps,gluteus maximus-based myocutaneous flaps, hamstringmyocutaneous V-Y advancement flaps, biceps muscular-based flaps, combination of gluteus maximus flaps and ham-string flaps, gracilis flaps, and simple split thickness skingrafts. Their distribution is illustrated in Fig. 9.
Primary endpoint analysis identified 25 recurrences for 108sores. Hence, in this study, we found that ischial pressurewounds have a recurrence rate of 23.14 %. These were recur-rences that occurred long after initial healing, and they are notpostoperative wound dehiscence. Data for recurrence delaycould not be established because most of the patients did notconsult soon after the appearance of new skin lesion but rather
Fig. 3 Large ischial pressure sore
Fig. 4 Gluteus maximus myocutaneous flap elevation
Fig. 5 Presentation after rotation and suture
Fig. 6 Biceps femoralis myocutaneous flap
Eur J Plast Surg (2014) 37:667–672 669
late without knowing the precise date of recurrence. A recur-rence per surgical technique analysis is illustrated in Table 2.
Secondary endpoint was the identification and descriptionof early complications. Wound dehiscence was the primarycomplication and it occurred in 12 patients. Three patients hadpostoperative persisting fistulas, 1 patient had an infectedhematoma, 4 patients had a partial flap loss, and 1 patienthad a total flap loss. The complications are illustrated inTable 3 as a complication per surgical technique distribution.
Discussion
In this retrospective study, we analyzed and evaluated ourpractice for ischial pressure sores’ treatment. It is well-known that this kind of decubitus is very difficult to treatand quite often ends up in a recurrence [16]. Nevertheless, it
concerns patients that need to be healed in order to work orlive with comfort. Hence, the most suitable surgical proposi-tion must be given to them. In this study, we found that thesurgical treatment of ischial pressure wounds has a recurrencerate similar to the literature’s findings. What is interestingthough is that the 5 out of 7 hamstring myocutaneous V-Yadvancement flaps had pressure sore recurrence. We tried tointerpret this tendency for recurrence. We found that it was notrelated to the surgeon as three different senior surgeons prac-ticed these operations. Patient selection included the rehabil-itated patients that had an active social and professional lifeand because every patient had the same preoperative prepara-tion, their general condition was considered comparable. Un-fortunately, wound dimensions and body weight were notavailable for all of the patients, so no conclusions could bemade concerning these parameters. The only common pointwas that patients were active and returned to a sitting positionsoon after healing. Even though the total number of V-Yhamstring myocutaneous advancement flap is small and nosolid conclusions can be made, this finding implies that eventhough these flaps are adequate for initial coverage, when thepatient regains the sitting position, the flaps retract and thesores recur. We now avoid using these flaps as a first choice
Fig. 7 Biceps femoralis myocutaneous flap final result
Fig. 8 V-Y myocutaneous hamstring advancement flap
Table 1 Ischial pressure sore etiology
Etiology Number Mean age
Posttraumatic paraplegia 79 68
Posttraumatic tetraplegia 5 42
Spina bifida 9 27
Bedridden patients 2 69
Multiple sclerosis 1
Myelomeningocele 1
Syringomyelia 1
Friedrich’s disease 1
Direct suture29%
Local skin flaps13%
Gluteus maximus flaps30%
V-Y hamstring advancement
7%
Biceps flaps13%
Combined8%
Surgical technique distribution
Fig. 9 Pie chart illustrating surgical technique distribution
670 Eur J Plast Surg (2014) 37:667–672
and prefer the gluteus maximus-based flaps that are a morereliable solution.
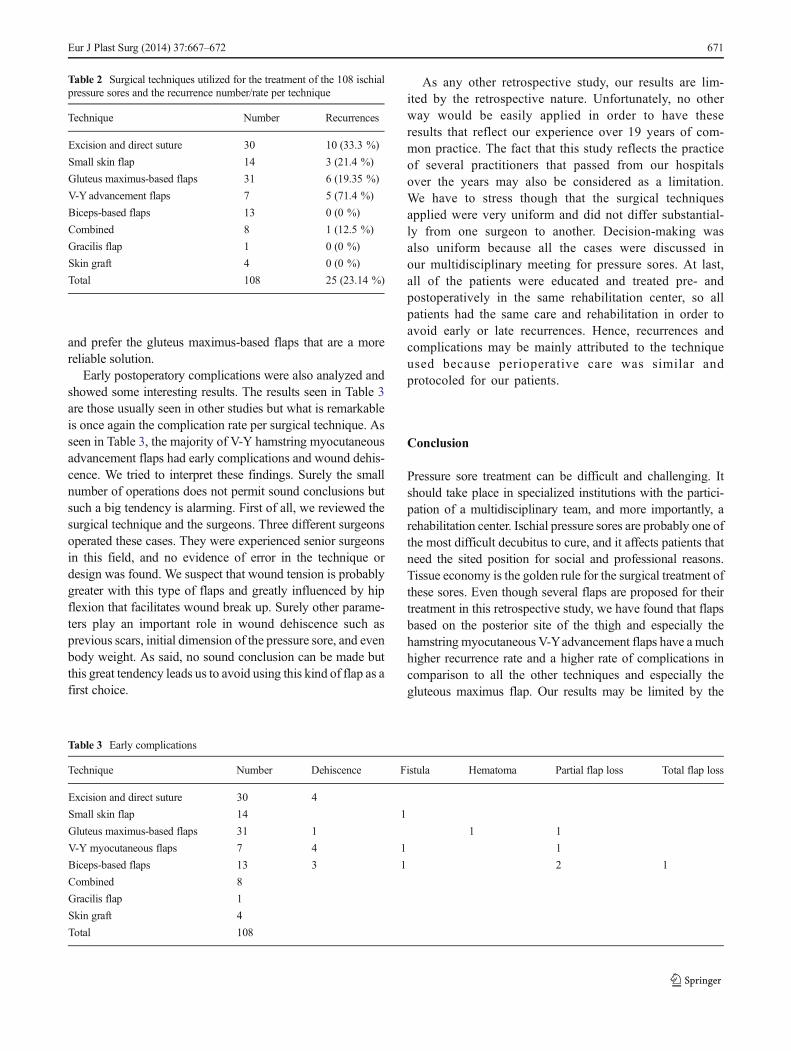
Early postoperatory complications were also analyzed andshowed some interesting results. The results seen in Table 3are those usually seen in other studies but what is remarkableis once again the complication rate per surgical technique. Asseen in Table 3, the majority of V-Y hamstring myocutaneousadvancement flaps had early complications and wound dehis-cence. We tried to interpret these findings. Surely the smallnumber of operations does not permit sound conclusions butsuch a big tendency is alarming. First of all, we reviewed thesurgical technique and the surgeons. Three different surgeonsoperated these cases. They were experienced senior surgeonsin this field, and no evidence of error in the technique ordesign was found. We suspect that wound tension is probablygreater with this type of flaps and greatly influenced by hipflexion that facilitates wound break up. Surely other parame-ters play an important role in wound dehiscence such asprevious scars, initial dimension of the pressure sore, and evenbody weight. As said, no sound conclusion can be made butthis great tendency leads us to avoid using this kind of flap as afirst choice.
As any other retrospective study, our results are lim-ited by the retrospective nature. Unfortunately, no otherway would be easily applied in order to have theseresults that reflect our experience over 19 years of com-mon practice. The fact that this study reflects the practiceof several practitioners that passed from our hospitalsover the years may also be considered as a limitation.We have to stress though that the surgical techniquesapplied were very uniform and did not differ substantial-ly from one surgeon to another. Decision-making wasalso uniform because all the cases were discussed inour multidisciplinary meeting for pressure sores. At last,all of the patients were educated and treated pre- andpostoperatively in the same rehabilitation center, so allpatients had the same care and rehabilitation in order toavoid early or late recurrences. Hence, recurrences andcomplications may be mainly attributed to the techniqueused because perioperative care was similar andprotocoled for our patients.
Conclusion
Pressure sore treatment can be difficult and challenging. Itshould take place in specialized institutions with the partici-pation of a multidisciplinary team, and more importantly, arehabilitation center. Ischial pressure sores are probably one ofthe most difficult decubitus to cure, and it affects patients thatneed the sited position for social and professional reasons.Tissue economy is the golden rule for the surgical treatment ofthese sores. Even though several flaps are proposed for theirtreatment in this retrospective study, we have found that flapsbased on the posterior site of the thigh and especially thehamstring myocutaneous V-Yadvancement flaps have a muchhigher recurrence rate and a higher rate of complications incomparison to all the other techniques and especially thegluteous maximus flap. Our results may be limited by the
Table 2 Surgical techniques utilized for the treatment of the 108 ischialpressure sores and the recurrence number/rate per technique
Technique Number Recurrences
Excision and direct suture 30 10 (33.3 %)
Small skin flap 14 3 (21.4 %)
Gluteus maximus-based flaps 31 6 (19.35 %)
V-Y advancement flaps 7 5 (71.4 %)
Biceps-based flaps 13 0 (0 %)
Combined 8 1 (12.5 %)
Gracilis flap 1 0 (0 %)
Skin graft 4 0 (0 %)
Total 108 25 (23.14 %)
Table 3 Early complications
Technique Number Dehiscence Fistula Hematoma Partial flap loss Total flap loss
Excision and direct suture 30 4
Small skin flap 14 1
Gluteus maximus-based flaps 31 1 1 1
V-Y myocutaneous flaps 7 4 1 1
Biceps-based flaps 13 3 1 2 1
Combined 8
Gracilis flap 1
Skin graft 4
Total 108
Eur J Plast Surg (2014) 37:667–672 671

retrospective nature of this study and by the number of pa-tients, but they imply that other flaps than the hamstringmyocutaneous V-Y advancement flaps should be used as afirst choice for ischial pressure sore treatment. More powerful,prospective and randomized studies should take place in orderto definitely resolve this issue.
Conflict of interest None
Ethical standards This study has been approved by the appropriateethics committee and have therefore been performed in accordance withthe ethical standards set forth in the 1964 Declaration of Helsinki and itslater amendments.
All persons gave their informed consent prior to their inclusion in thestudy. Details that might disclose the identity of the subjects under studywere omitted.
References
1. Homma K, Murakami G, Fujioka H, Fujita T, Imai A, Ezoe K (2001)Treatment of ischial pressure ulcers with a posteromedial thighfasciocutaneous flap. Plast Reconstr Surg 108:1990–1996, discus-sion 1997
2. Conway H, Griffith BH (1956) Plastic surgery for closure ofdecubitus ulcers in patients with paraplegia; based on experiencewith 1,000 cases. Am J Surg 91:946–975
3. Kierney PC, Engrav LH, Isik FF, Esselman PC, Cardenas DD, RandRP (1998) Results of 268 pressure sores in 158 patients managedjointly by plastic surgery and rehabilitation medicine. Plast ReconstrSurg 102:765–772
4. Cariou JL, Bovet JL, Schoofs M, Baudet J, Panconi B. Notreexpérience de la couverture des escarres ischiatiques par lambeauxmusculo-cutanés. Ann Chir Plast Esthet 28: 337–47
5. Rubayi S, Burnett CC (1999) The efficacy of single-stage surgicalmanagement of multiple pressure sores in spinal cord-injured pa-tients. Ann Plast Surg 42:533–539
6. Mathes SJ, Nahai F (1979) Clinical atlas of muscle andmusculocutaneous flaps. CV Mosby, St. Louis, p 94–98
7. Baker DC, Barton FE, Converse JM (1978) A combined biceps andsemitendinosus muscle flap in the repair of ischial sores. Br J PlastSurg 31:26–28
8. Hurteau JE, Bostwick J, Nahai F, Hester R, Jurkiewicz MJ (1981) V-Yadvancement of hamstring musculocuataneous flap for coverage ofischial pressure sores. Plast Reconstr Surg 68:539–542
9. Hurwitz DJ, Swartz WM, Mathes SJ (1981) The gluteal thigh flap: areliable, sensate flap for the closure of buttock and perineal wounds.Plast Reconstr Surg 68:521–532
10. Wingate GB, Friedland JA (1978) Repair of ischial pressure ulcerswith gracilis myocutaneous island flaps. Plast Reconstr Surg 62:245–248
11. Scheufler O, Farhadi J, Kovach SJ et al (2006) Anatomical basis andclinical application of the infragluteal perforator flap. Plast ReconstrSurg 118:1389–1400
12. Geddes CR, Morris SF, Neligan PC (2003) Perforator flaps: evolu-tion, classification, and applications. Ann Plast Surg 50:90–99
13. Yamamoto Y, Tsutsumida A, Murazumi M, Sugihara T (1997) Long-term outcome of pressure sores treated with flap coverage. PlastReconstr Surg 100:1212–1217
14. Foster RD, Anthony JP, Mathes SJ, Hoffman WY (1997) Ischialpressure sore coverage: a rationale for flap selection. Br J PlastSurg 50:374–379
15. Chan JK-K, Harry L, Williams G, Nanchahal J (2012) Soft-tissuereconstruction of open fractures of the lower limb: muscle versusfasciocutaneous flaps. Plast Reconstr Surg 130:284e–295e
16. Tavakoli K, Rutkowski S, Cope C et al (1999) Recurrence rates ofischial sores in para- and tetraplegics treated with hamstring flaps: an8-year study. Br J Plast Surg 52:476–479
672 Eur J Plast Surg (2014) 37:667–672