Treatment of diabetic ketoacidosis and hyperosmolar
hyperglycemic state in adults Authors Abbas E Kitabchi, PhD, MD,
FACP, FACE Burton D Rose, MD Section Editor David M Nathan, MD
Deputy Editor Jean E Mulder, MD Disclosures All topics are updated
as new evidence becomes available and our peer review process is
complete. Literature review current through: Dec 2012. | This topic
last updated: jun 26, 2012. INTRODUCTION Diabetic ketoacidosis
(DKA) and hyperosmolar hyperglycemic state (HHS, also called
nonketotic hyperglycemia) are two of the most serious acute
complications of diabetes. They are part of the spectrum of
hyperglycemia and each represents an extreme in the spectrum. The
treatment of DKA and HHS in adults will be reviewed here. The
epidemiology, pathogenesis, clinical features, and diagnosis of
these disorders are discussed separately. (See "Epidemiology and
pathogenesis of diabetic ketoacidosis and hyperosmolar
hyperglycemic state" and "Clinical features and diagnosis of
diabetic ketoacidosis and hyperosmolar hyperglycemic state in
adults".) DEFINITIONS DKA and HHS differ clinically according to
the presence of ketoacidosis and the degree of hyperglycemia [1-3].
The definitions proposed by the American Diabetes Association for
DKA and HHS are shown in the table (table 1) [1]. In DKA, metabolic
acidosis is often the major finding, while the serum glucose
concentration is generally below 800 mg/dL (44 mmol/L) [1-3].
However, serum glucose concentrations may exceed 900 mg/dL (50
mmol/L) in patients with DKA who are comatose [3,4]. In HHS, there
is little or no ketoacid accumulation, the serum glucose
concentration frequently exceeds 1000 mg/dL (56 mmol/L), the serum
osmolality may reach 380 mosmol/kg, and neurologic abnormalities
are frequently present (including coma in 25 to 50 percent of
cases) [1,2,5,6].
Significant overlap between DKA and HHS occurs in more than
one-third of patients [7]. The typical total body deficits of water
and electrolytes in DKA and HHS are compared in the table (table
2). (See "Clinical features and diagnosis of diabetic ketoacidosis
and hyperosmolar hyperglycemic state in adults", section on
'Definitions'.) TREATMENT Treatment overview and protocols The
treatment of DKA and HHS is similar, including the administration
of insulin and correction of the fluid and electrolyte
abnormalities that are typically present, including hyperglycemia
and hyperosmolality, hypovolemia, metabolic acidosis (in DKA), and
potassium depletion (table 3) [1,8-10]. The factors responsible for
these metabolic abnormalities are discussed separately. (See
"Clinical features and diagnosis of diabetic ketoacidosis and
hyperosmolar hyperglycemic state in adults".) Therapy also requires
frequent patient monitoring and identification and treatment of
precipitating events. Infection (most commonly pneumonia and
urinary tract infection) is a common precipitating
event. Thus, cultures should be obtained if there are suggestive
clinical findings, recognizing that infection may be present in the
absence of fever [1,9,10]. An algorithmic approach developed for
the ADA is shown in the flow diagrams for treating DKA (algorithm
1) and HHS (algorithm 2) [1,3]. Initial evaluation Both DKA and HHS
are medical emergencies that require prompt recognition and
management. An initial history and rapid but careful physical
examination should focus on: Airway, breathing, and circulation
(ABC) status Mental status Possible precipitating events (eg,
source of infection, myocardial infarction) Volume status
The initial laboratory evaluation of a patient with suspected
DKA or HHS should include determination of: Serum glucose Serum
electrolytes (with calculation of the anion gap), BUN, and plasma
creatinine Complete blood count with differential Urinalysis and
urine ketones by dipstick Plasma osmolality Serum ketones (if urine
ketones are present) Arterial blood gas if the serum bicarbonate is
substantially reduced Electrocardiogram
Additional testing, such as cultures of urine, sputum, and
blood, serum lipase and amylase, and chest x-ray, should be
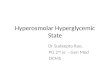
performed on a case-by-case basis. Monitoring The serum glucose
should initially be measured every hour until stable, while serum
electrolytes, blood urea nitrogen, creatinine, osmolality, and
venous pH (for DKA) should be measured every two to four hours,
depending upon disease severity and the clinical response [1,10].
Repeat arterial blood gases are unnecessary during the treatment of
DKA; venous pH, which is about 0.03 units lower than arterial pH
[11], is adequate to assess the response to therapy and avoids the
pain and potential complications associated with repeated arterial
punctures (figure 1). Monitoring serum bicarbonate is another
alternative if blood chemistries can be returned in a timely
fashion. Acidosis in DKA Direct measurement of beta-hydroxybutyrate
in the blood is the preferred method for monitoring the degree of
ketonemia and has become more convenient with the development of
bedside meters capable of measuring whole blood
beta-hydroxybutyrate [12]. However, this approach is not available
in many hospitals. Nitroprusside tablets or reagent sticks react
with acetoacetate and acetone (produced by the decarboxylation of
acetoacetic acid), but do not identify beta-hydroxybutyrate. (See
"Clinical features and diagnosis of diabetic ketoacidosis and
hyperosmolar hyperglycemic state in adults", section on 'Serum
ketones'.)
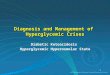
During insulin therapy, beta-hydroxybutyrate is converted to
acetoacetate. Thus, if the nitroprusside method is used for
monitoring of ketones in the blood or urine, an increasingly
positive test due to this conversion may erroneously lead the
clinician to believe that ketosis has worsened (figure 2) [13]. As
a result, assessments of urinary or serum ketone levels by the
nitroprusside method should not be used as an indicator of response
to therapy. If the results of blood chemistries can be returned in
a timely fashion, an alternative to monitoring venous pH and serum
beta-hydroxybutyrate is monitoring the serum bicarbonate
concentration (to assess correction of the metabolic acidosis) and
the serum anion gap (to assess correction of the ketoacidemia). The
serum anion gap provides an estimate of the quantity of unmeasured
anions in the plasma, such as albumin and, in DKA, ketoacid anions.
It is calculated by subtracting the major measured anions (chloride
and bicarbonate) from the major measured cation (sodium): Serum
anion gap = Serum sodium - (serum chloride + bicarbonate) (See
"Approach to the adult with metabolic acidosis", section on 'Serum
anion gap and differential diagnosis'.) Monitoring the anion gap
will give a good estimate of serum ketoacid anion levels in DKA.
Normalization of the anion gap reflects disappearance of ketoacid
anions in the serum and correction of the ketoacidosis. However,
ketonemia and ketonuria may persist for more than 36 hours due to
the slower removal of acetone, in part via the lungs [14,15]. Since
acetone is biochemically neutral, such patients do not have
persistent ketoacidosis. The factors that can affect the anion gap
during the treatment of DKA are reviewed below. (See 'Anion gap'
below.) Fluid replacement Initial fluid therapy in DKA and HHS is
directed toward expansion of the intravascular volume and
restoration of renal perfusion [16]. Adequate rehydration with
subsequent correction of the hyperosmolar state may result in a
more robust response to low dose insulin therapy [17,18]. The
average fluid loss is 3 to 6 liters in DKA and up to 8 to 10 liters
in HHS, due largely to the glucose osmotic diuresis (table 2)
[1,2,8,10]. In addition to inducing water loss, glucosuria results
in the loss of approximately 70 meq of sodium and potassium for
each liter of fluid lost. The aim of therapy is to replete the
extracellular fluid volume without inducing cerebral edema due to
too rapid reduction in the plasma osmolality. (See 'Cerebral edema'
below and "Treatment and complications of diabetic ketoacidosis in
children", section on 'Cerebral edema'.) Fluid repletion is usually
initiated with isotonic saline (0.9 percent sodium chloride). This
solution will replace the fluid deficit, correct the extracellular
volume depletion more rapidly than one-half isotonic saline, lower
the plasma osmolality (since it is still hypoosmotic to the
patient), and reduce the serum glucose concentration both by
dilution and by increasing urinary losses as renal perfusion is
increased [16,19]. The optimal rate at which isotonic saline is
given is dependent upon the clinical state of the patient. Isotonic
saline should be infused as quickly as possible in patients who are
in shock. In the absence of cardiac compromise, isotonic saline is
infused at a rate of 10 to 15 mL/kg lean body weight per hour
(about 1000 mL/hour in an average-sized person) during the first
few hours, with a maximum of 50 mL/hour). If the patient is
hemodynamically stable, one-half isotonic saline is preferred since
the addition of potassium to isotonic saline will result in a
hypertonic solution that will delay correction of the
hyperosmolality. The serum potassium should be maintained between
4.0 and 5.0 meq/L. (See'Effect of potassium supplementation'
above.) Potassium repletion is more urgent in patients with massive
potassium deficits who are hypokalemic prior to therapy [34,35].
Such patients require aggressive potassium replacement (20 to 30
meq/hour), which usually requires 40 to 60 meq/L added to one-half
isotonic saline. Since insulin will worsen the hypokalemia, insulin
therapy should be delayed until the serum potassium is above 3.3
meq/L to avoid possible arrhythmias, cardiac arrest, and
respiratory muscle weakness [1,34,35].
Serum sodium Hyperglycemia in uncontrolled diabetes mellitus has
a variable effect on the serum sodium concentration, as factors are
present that can both lower and raise the measured value [36]: By
raising the serum osmolality, hyperglycemia results in osmotic
water movement out of the cells, thereby lowering the serum sodium
concentration by dilution. The direct effect of hyperglycemia is
counteracted by the glucosuria-induced osmotic diuresis. The
diuresis results in water loss in excess of sodium and potassium,
which will tend to raise the serum sodium concentration and plasma
osmolality unless there is a comparable increase in water
intake.
The serum sodium concentration at presentation varies with the
balance of these mechanisms. (See "Clinical features and diagnosis
of diabetic ketoacidosis and hyperosmolar hyperglycemic state in
adults", section on 'Serum sodium'.) Reversing the hyperglycemia
with insulin will lower the plasma osmolality, which will cause
water to move from the extracellular fluid into the cells, thereby
raising the serum sodium concentration [1,5,10,36,37]. Thus, a
patient with a normal initial serum sodium concentration will
usually become hypernatremic during therapy with insulin and
isotonic saline. The degree to which this is likely to occur can be
estimated at presentation by calculation of the "corrected" serum
sodium concentration, that is, the serum sodium concentration that
should be present if the serum glucose concentration were lowered
to normal with insulin alone [36]: Corrected serum Na = Measured
serum Na + [SG 42] Where SG is the increment above normal in the
serum glucose concentration (in mg/dL). The SG should be divided by
2.3 if measured in mmol/L. Bicarbonate and metabolic acidosis The
indications for bicarbonate therapy in DKA are controversial [38]
and evidence of benefit is lacking [39-41]. In a randomized trial
of 21 DKA patients with an admission arterial pH between 6.90 and
7.14 (mean 7.01), bicarbonate therapy did not change morbidity or
mortality [39]. However, the study was small, limited to patients
with an arterial pH 6.90 and above, and there was no difference in
the rate of rise in the arterial pH and serum bicarbonate between
the bicarbonate and placebo groups. No prospective randomized
trials have been performed concerning the use of bicarbonate in DKA
with pH values less than 6.90. The specific indications for
bicarbonate administration are important because there are three
potential concerns with such therapy: Overzealous use of alkali can
lead to a rise in pCO2 (since there is less of an acidemic stimulus
to hyperventilation), resulting in a paradoxical fall in cerebral
pH as the lipidsoluble CO2 rapidly crosses the blood-brain barrier.
Neurologic deterioration has been reported in this setting, but is
probably a rare event [42]. The administration of alkali may slow
the rate of recovery of the ketosis [43,44]. In a study of seven
patients, the three patients who were treated with bicarbonate had
a rise in serum ketoacid levels during bicarbonate infusion,
resulting in a six-hour delay in improvement of ketosis [43].
Animal studies suggest that bicarbonate therapy increases hepatic
ketogenesis. However, in the randomized trial cited above,
bicarbonate therapy had no effect on the rate of decline in serum
ketone levels [39].
Alkali administration can lead to a posttreatment metabolic
alkalosis, since metabolism of ketoacid anions with insulin results
in the generation of bicarbonate and spontaneous correction of most
of the metabolic acidosis. (See 'Anion gap' below.)
There are, however, selected patients who may benefit from
cautious alkali therapy [42]. These include: Patients with an
arterial pH less than 7.00 in whom decreased cardiac contractility
and vasodilatation can further impair tissue perfusion. At an
arterial pH above 7.00, most experts agree that bicarbonate therapy
is not necessary, since insulin therapy alone will result in
resolution of most of the metabolic acidosis [45]. Patients with
potentially life-threatening hyperkalemia, since bicarbonate
administration in acidemic patients drives potassium into cells,
thereby lowering the serum potassium concentration [46]. (See
"Treatment and prevention of hyperkalemia in adults".)
We recommend administering bicarbonate if the arterial pH is
less than 6.90. We give 100 meq of sodium bicarbonate in 400 mL
sterile water with 20 meq of potassium chloride, if the serum
potassium is less than 5.3 meq/L, administered over two hours. The
venous pH should be monitored every two hours, and bicarbonate
dosed as above, until the pH rises above 7.00. Anion gap There is a
variable relationship between the elevation in serum anion gap and
the fall in serum bicarbonate concentration because of the
excretion of ketoacid anions in the urine [47,48]. (See "The anion
gap/HCO3 ratio in patients with a high anion gap metabolic
acidosis".) Ketoacid anions have been called "potential
bicarbonate," since their metabolism following the administration
of insulin results in the generation of bicarbonate and reversal of
the acidosis. The effect of ketoacid anion excretion on the course
of ketoacidosis varies with the accompanying cation: The excretion
of ketoacid anions with hydrogen or ammonium is associated with an
equivalent loss of protons, correcting both the anion gap and the
acidemia. It has been estimated that approximately 30 percent of
the ketoacids produced in DKA are excreted in the urine in patients
with relatively normal renal function; the conversion of
acetoacetic acid to acetone can neutralize another 15 to 25 percent
of the acid load [49]. The excretion of ketoacid anions with sodium
or potassium represents the loss of bicarbonate precursors (ie,
"potential bicarbonate") and is therefore equivalent to bicarbonate
loss. The net effect is that the anion gap is reduced but the
acidosis persists.
As a result of the urinary loss of "potential bicarbonate,"
almost all patients with DKA (except those with advanced renal
failure) develop a normal anion gap acidosis (also known as a
"non-gap acidosis") during treatment [47,50,51]. Suppose, for
example, that a patient has a serum bicarbonate of 8 meq/L and an
anion gap of 24 meq/L (approximately 16 meq/L above normal).
Insulin therapy promotes correction of the ketoacidosis by
inhibiting lipolysis, which decreases the supply of free fatty
acids to the liver for ketogenesis, by inhibiting ketogenesis in
the liver, and by promoting peripheral ketone metabolism. (See
"Insulin action", section on 'Insulin and ketone body
metabolism'.)
The net effect is that the 16 meq/L of ketoacid anion will be
metabolized, which will regenerate some of the HCO3 lost in the
initial buffering reaction. However, the plasma HCO3 may only rise
by about 8 meq/L (to 16 meq/L), with the rest of the HCO3
replenishing the cell and bone buffer stores. At this point, the
patient will have metabolic acidosis with a normal AG, due to the
combination of the previous production of the intact ketoacid and
the subsequent loss of the ketoacid anion in the urine. If no
ketoacid anions had been excreted in the urine (as in a dialysis
patient), then insulin therapy would have returned both the anion
gap and serum bicarbonate concentration to baseline. (See "The
anion gap/HCO3 ratio in patients with a high anion gap metabolic
acidosis", section on 'Ketoacidosis'.) Phosphate depletion Whole
body phosphate depletion is common in uncontrolled diabetes
mellitus, although the serum phosphate concentration may initially
be normal or elevated due to movement of phosphate out of the cells
[8,52]. As with potassium balance, phosphate depletion is rapidly
unmasked following the institution of insulin therapy, frequently
leading to hypophosphatemia that is usually asymptomatic. The fall
in serum phosphate concentration during the treatment of DKA is
acute, self-limited, and usually not associated with marked
phosphate depletion or adverse effects. Clinically evident
hemolysis as well as rhabdomyolysis with myoglobinuria are rare
complications of the hypophosphatemia [53-55]. (See "Signs and
symptoms of hypophosphatemia".) Prospective randomized trials of
patients with DKA have failed to show a beneficial effect of
phosphate replacement on the duration of ketoacidosis, dose of
insulin required, rate of fall of serum glucose, or morbidity and
mortality [56-58]. In addition, phosphate replacement may have
adverse effects such as hypocalcemia and hypomagnesemia [56,59-61].
Based upon these observations, we do NOT recommend the routine use
of phosphate in the treatment of DKA or HHS. However, to avoid
cardiac and skeletal muscle weakness and respiratory depression due
to hypophosphatemia, careful phosphate replacement may be indicated
in patients who develop cardiac dysfunction, hemolytic anemia, or
respiratory depression, and in those with a serum phosphate
concentration below 1.0 mg/dL (0.32 mmol/L) [62]. When needed, 20
to 30 meq/L of potassium phosphate can be added to replacement
fluids. COMPLICATIONS The most common complications of the
treatment of DKA and HHS, hypoglycemia and hypokalemia, have been
reduced significantly since the administration of low dose insulin
and careful monitoring of serum potassium [63]. Hyperglycemia may
result from interruption or discontinuation of intravenous insulin
without prior coverage with subcutaneous insulin. Cerebral edema
Cerebral edema in uncontrolled diabetes mellitus (usually DKA, with
occasional reports in HHS) is primarily a disease of children and
almost all affected patients are below the age of 20 years [64].
Symptoms typically emerge with 12 to 24 hours of the initiation of
treatment for DKA, but may be present prior to the onset of
therapy. Issues related to cerebral edema in DKA, including
pathogenesis, are discussed in detail separately in the pediatric
section but will be briefly reviewed here. (See "Cerebral edema in
children with diabetic ketoacidosis".) Headache is the earliest
clinical manifestation, followed by lethargy, and decreased
arousal. Neurologic deterioration may be rapid, with seizures,
incontinence, pupillary changes, bradycardia, and respiratory
arrest. These symptoms progress if brainstem herniation occurs, and
the rate of progression may be so rapid that papilledema is not
seen.
Cerebral edema is associated with a mortality rate of 20 to 40
percent [1]. Thus, an essential part of therapy in DKA is careful
monitoring for changes in mental or neurologic status that would
permit early identification and therapy of cerebral edema. The 2009
ADA guidelines on hyperglycemic crises in diabetes in adults
suggested that the following preventive measures may reduce the
risk of cerebral edema in high-risk patients [1]: Gradual
replacement of sodium and water deficits in patients who are
hyperosmolar. The usual regimen for the first few hours is isotonic
saline at a rate of 10 to 15 mL/kg lean body weight per hour (about
1000 mL/hour in an average-sized person) with a maximum of 7.3,
serum bicarbonate >15 mEq/l, and minimal ketonuria and
ketonemia. Normal laboratory values vary; check local lab normal
ranges for all electrolytes.IV: intravenous; SC: subcutaneous. *
After history and physical exam, obtain capillary glucose and serum
or urine ketones (nitroprusside method). Begin one liter of 0.9
percent NaCl over one hour and draw arterial blood gases, complete
blood count with differential, urinalysis, serum glucose, BUN,
electrolytes, chemistry profile and creatinine levels STAT. Obtain
electrocardiogram, chest X-ray, and specimens for bacterial
cultures, as needed. Serum Na+ should be corrected for
hyperglycemia (for each 100 mg/dl glucose >100 mg/dl, add 1.6
mEq to sodium value for corrected serum sodium value). An
alternative IV insulin regimen is to give a continuous intravenous
infusion of regular insulin at 0.14 units/kg per hour; at this
dose, an initial intravenous bolus is not necessary.
Copyright 2006 American Diabetes Association From Diabetes Care
Vol 29, Issue 12, 2006. Modifications from Diabetes Care Vol 32,
Issue 7, 2009. Reprinted with permission from the American Diabetes
Association.