Embed Size (px)
Citation preview

C A S E R E P O R TJ Orthopaed Traumatol (2006) 7:23–25DOI 10.1007/s10195-006-0116-y
P. BaumannG.U. Exner
Treatment of a neglected pseudarthroticmultifragmentary intra-articular supracondylarfemoral fracture using a modularreconstruction system
Received: 7 March 2005Accepted: 28 November 2005
P. Baumann (�) • G.U. ExnerUniversitätsklinik BalgristForchstrasse 340, 8008 Zürich, SwitzerlandE-mail: [email protected]
Abstract The standard treatment ofacute distal femoral fractures con-sists of open anatomic reconstruc-tion and fixation. Internal fixationmay be accomplished with angularplates, condylar screw fixation,antegrade or retrograde nailing.Inveterated condylar fractures arerarely seen in our society and pres-ent challenging management prob-lems. A 64-year-old man presentedwith a pseudarthrotic dislocatedmultifragmentary supracondylarfracture and a knee flexion contrac-ture two years following the acci-dent, mobilized only with a wheel-chair. Because of the severly osteo-
porotic bone, degenerative articularchanges and the flexion contrac-ture, we chose resection of the frag-ments and implantation of a recon-struction system (MUTARS)instead of osteosynthesis. Elevenweeks postoperatively, the patientwas able to walk without crutches.Nine months after surgery, he hasflexion up to 90° and full exten-sion, and has regained an activelife.
Key words Intra-articular supra-condylar femoral fracture •
Pseudarthrosis • Modular recon-struction system MUTARS
Introduction
A 64-year-old man sustained a multifragmentary articularsupracondylar fracture of the right femur two years beforeadmittance to our institution. We describe our treatmentand the functional result with implantation of a tumor-reconstruction knee prosthesis (MUTARS system).
Case report
A 64-year-old man sustained a multifragmentary articularsupracondylar fracture of the right femur. Socially disin-tegrated after the recent death of his wife, he refused anymedical treatment in spite of inability to walk and theneed of a wheelchair.
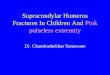
When he came to our treatment two years after theaccident, he presented a pseudarthrosis of the dislocatedfragments (Fig. 1) with a flexion contracture of the kneejoint (range of motion for flexion/extension, 135°/60°/0°).
Reduction and osteosynthesis were felt to result intoinsufficient rehabilitation because of the suspected severecartilage damage and muscle contractures as well assevere osteopenia. Therefore reconstruction with a modu-lar system usually used after tumor resection surgery waschosen (MUTARS system).
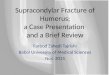
Range of motion exercises were begun immediatelypostoperatively. Six weeks after reconstruction, thepatient regained ambulation and radiographs wereobtained (Fig. 2). Eleven weeks postoperatively he wasable to walk without crutches. On physical examinationnine months after surgery, he was walking without crutch-es, had flexion up to 90° and full extension. The patient isvery satisfied and socially reintegrated.

24
Discussion
Distal femoral fractures represent about 7% of all femurfractures. The typical distal femoral fracture is associatedwith high-energy trauma in younger individuals, and
occurs in the elderly with osteoporotic bone [11]. Thefractures are frequently associated with other skeletal orsoft-tissue injuries, especially those involving youngerpatients [1]. The standard treatment for acute distalfemoral fractures consists of open anatomic reconstruc-tion and fixation [1]. Several possible operative tech-niques have been described, including open reduction,angular plate or dynamic condylar screw fixation, as wellas antegrade or retrograde nailing [1–5].
Some reports described the treatment of supracondylarfemoral fractures with implantation of a primary totalknee endoprosthesis. Davila et al. [6] reported the satis-factory use of a megaprosthesis as treatment for persistentnonunion of supracondylar femur fractures in two patientsafter failed fixation. In 1992, Bell et al. [7] reported thetreatment of 10 supracondylar femoral fractures (accord-ing to Müller’s classification type C) and 3 Müller type Afractures in elderly patients (average age, 84 years) with aprimary knee endoprosthesis. In a short follow-up of 6months, 11 regained a good functional outcome, and mostpatients regained their pre-injury level of independence[7]. Kress et al. [8] described the treatment of nonunionswith total knee arthroplasty using non-cemented femoralstems: two patients had supracondylar femur fractures.
The MUTARS system is a modular kinematic rotatinghinge total knee prosthesis initially designed for limbreconstruction after tumor surgery. It consists of a titani-um cemented long stem, or a non-cemented CoCrMostem. A substantial component of the system to implantthe prosthesis uncemented is the hexagonal design of thestem [4]. The medullary canal can easily be preparedusing a special rasp.
Fig. 1a, b Diagnostic imaging 2 years after fracture of the right femur. a Three-dimensional computed tomographs show a multifragmen-tary articular fracture of the femur with pseudarthrosis. The distal femur is laterally and ventrally dislocated; a large piece of sclerotic bonecan be seen intra-articulary. b Standard radiographs of the complex multifragmentary articular supracondylar fracture. The distal femur isventrally and laterally luxated. The bone appears osteopenic
Fig. 2 Radiographs at six weeks postoperatively document thereconstruction with the MUTARS system. The patella is intact andwell centered
a b

25
Our patient sustained a complex multifragmentaryarticular supracondylar fracture of the right femur twoyears before admittance to our institution. Management ofthe displaced and older complex supracondylar femurfracture (type C according to Müller’s classification [10])is fraught with problems, including insufficient vascularsupply, poor bone quality and difficulty in obtaining andmaintaining reduction. The preoperative CT scan in ourcase showed a complex multifragmentary articular frac-ture with pseudarthrosis and luxation of the distal femur.The bone was impacted and of poor quality. The femur
and tibia were osteoporotic, making screw or plate fixa-tion difficult.
In our patient, we expected a high risk of fixationfailure, nonunion, instability and re-fracture with openreduction and plate or screw fixation, or with intra-medullary nailing. With implantation of the MUTARSprosthesis, early postoperative mobilization and motionexercises could be started. At follow-up 9 months aftersurgery, the patient appears to have an excellent func-tional result and, with his regained mobility, he is social-ly reintegrated.
1. Kinzl L (2000) Femur: distal. In: RüediTP, Murphy WM (eds) AO principles offracture management. Thieme, StuttgartNew York, p 469
2. Bolhofner B, Carmen B, Clifford P(1996) The results of open reductionand internal fixation of distal femurfractures using biologic (indirect)reduction technique. J Orthopaed Trau-matol 10:372–377
3. Huang HT, Huang PJ, Su JY (2003)Indirect reduction and bridge plating ofsupracondylar fractures of the femur.Injury 34:135–140
4. Ingman AM (2002) Retrograde intra-medullary nailing of supracondylar fe-moral fractures: design and developmentof a new implant. Injury 33:707–712
5. Kumar A, Jasani V, Butt MS (2000)Management of distal femoral fracturesin elderly patients using retrograde tita-nium supracondylar nails. Injury31:169–173
6. Davila J, Malkani A, Paiso JM (2001)Supracondylar distal femoral nonunionstreated with a megaprosthesis in elderlypatients: a report of two cases. J Ortho-paed Traumatol 15(8):574–578
7. Bell KM, Johnstone AJ, Court-BrownAM, Hughes SPF (1992) Primary kneearthroplasty for distal femoral fracturesin elderly patients. J Bone Joint Surg Br74:400–402
8. Kress K, Scuderi GR, Windsor RE et al(1993) Treatment of nonunion about theknee utilizing custom total knee arthro-plasty with Pressfit intramedullarystems. J Arthroplasty 8:49–55
9. Gosheger G, Winkelmann W. (2000)Mutars® - ein modulares Tumor- undRevisionssystem. Orthopäde 29[Suppl1]:54–55
10. Murphy WM, Leu D (2000) Fractureclassification. In: Rüedi TP, Murphy WM(eds) AO principles of fracture manage-ment. Thieme, Stuttgart New York, p 53
11. O’Brien P, Meek RN, Blachut PA,Broekhuyse HM (2001) Fractures of thedistal femur. In: Rockwood CA, GreenDP (eds) Fractures in Adults. LippincottWilliams & Williams, p 1731
References