Embed Size (px)
Citation preview
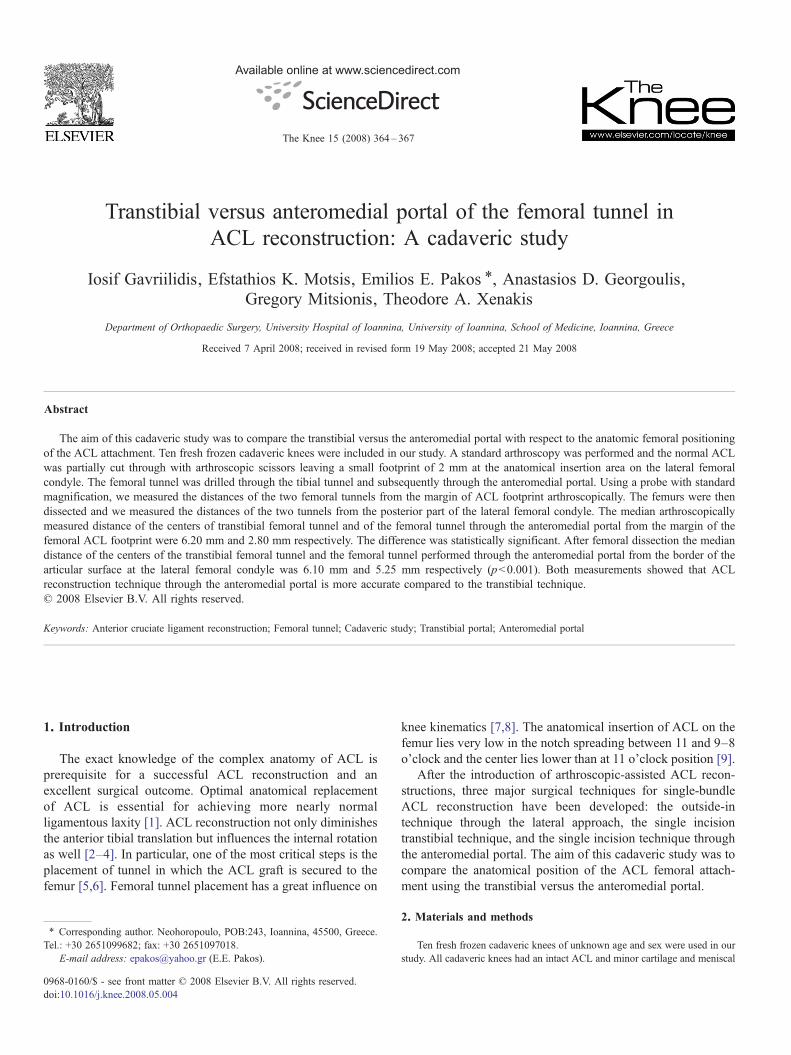
Available online at www.sciencedirect.com
4–367
The Knee 15 (2008) 36Transtibial versus anteromedial portal of the femoral tunnel inACL reconstruction: A cadaveric study
Iosif Gavriilidis, Efstathios K. Motsis, Emilios E. Pakos ⁎, Anastasios D. Georgoulis,Gregory Mitsionis, Theodore A. Xenakis
Department of Orthopaedic Surgery, University Hospital of Ioannina, University of Ioannina, School of Medicine, Ioannina, Greece
Received 7 April 2008; received in revised form 19 May 2008; accepted 21 May 2008
Abstract
The aim of this cadaveric study was to compare the transtibial versus the anteromedial portal with respect to the anatomic femoral positioningof the ACL attachment. Ten fresh frozen cadaveric knees were included in our study. A standard arthroscopy was performed and the normal ACLwas partially cut through with arthroscopic scissors leaving a small footprint of 2 mm at the anatomical insertion area on the lateral femoralcondyle. The femoral tunnel was drilled through the tibial tunnel and subsequently through the anteromedial portal. Using a probe with standardmagnification, we measured the distances of the two femoral tunnels from the margin of ACL footprint arthroscopically. The femurs were thendissected and we measured the distances of the two tunnels from the posterior part of the lateral femoral condyle. The median arthroscopicallymeasured distance of the centers of transtibial femoral tunnel and of the femoral tunnel through the anteromedial portal from the margin of thefemoral ACL footprint were 6.20 mm and 2.80 mm respectively. The difference was statistically significant. After femoral dissection the mediandistance of the centers of the transtibial femoral tunnel and the femoral tunnel performed through the anteromedial portal from the border of thearticular surface at the lateral femoral condyle was 6.10 mm and 5.25 mm respectively (pb0.001). Both measurements showed that ACLreconstruction technique through the anteromedial portal is more accurate compared to the transtibial technique.© 2008 Elsevier B.V. All rights reserved.
Keywords: Anterior cruciate ligament reconstruction; Femoral tunnel; Cadaveric study; Transtibial portal; Anteromedial portal
1. Introduction
The exact knowledge of the complex anatomy of ACL isprerequisite for a successful ACL reconstruction and anexcellent surgical outcome. Optimal anatomical replacementof ACL is essential for achieving more nearly normalligamentous laxity [1]. ACL reconstruction not only diminishesthe anterior tibial translation but influences the internal rotationas well [2–4]. In particular, one of the most critical steps is theplacement of tunnel in which the ACL graft is secured to thefemur [5,6]. Femoral tunnel placement has a great influence on
⁎ Corresponding author. Neohoropoulo, POB:243, Ioannina, 45500, Greece.Tel.: +30 2651099682; fax: +30 2651097018.
E-mail address: [email protected] (E.E. Pakos).
0968-0160/$ - see front matter © 2008 Elsevier B.V. All rights reserved.doi:10.1016/j.knee.2008.05.004
knee kinematics [7,8]. The anatomical insertion of ACL on thefemur lies very low in the notch spreading between 11 and 9–8o'clock and the center lies lower than at 11 o'clock position [9].
After the introduction of arthroscopic-assisted ACL recon-structions, three major surgical techniques for single-bundleACL reconstruction have been developed: the outside-intechnique through the lateral approach, the single incisiontranstibial technique, and the single incision technique throughthe anteromedial portal. The aim of this cadaveric study was tocompare the anatomical position of the ACL femoral attach-ment using the transtibial versus the anteromedial portal.
2. Materials and methods
Ten fresh frozen cadaveric knees of unknown age and sex were used in ourstudy. All cadaveric knees had an intact ACL and minor cartilage and meniscal
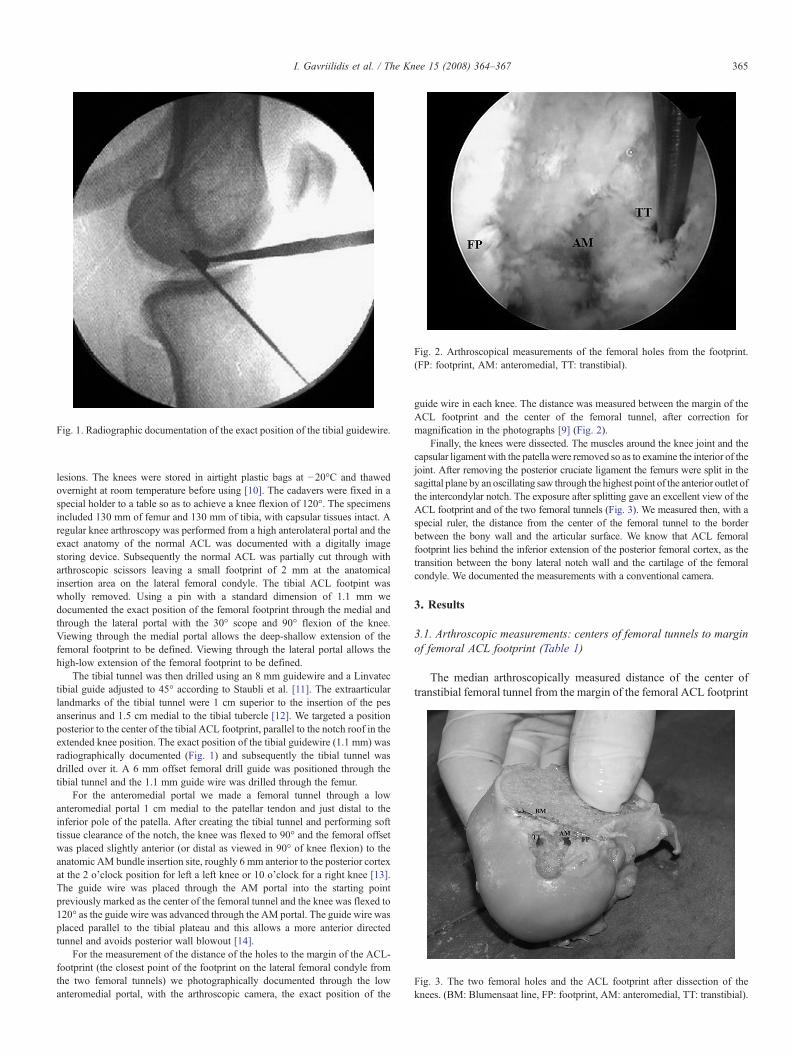
Fig. 1. Radiographic documentation of the exact position of the tibial guidewire.
Fig. 2. Arthroscopical measurements of the femoral holes from the footprint.(FP: footprint, AM: anteromedial, TT: transtibial).
Fig. 3. The two femoral holes and the ACL footprint after dissection of theknees. (BM: Blumensaat line, FP: footprint, AM: anteromedial, TT: transtibial).
365I. Gavriilidis et al. / The Knee 15 (2008) 364–367
lesions. The knees were stored in airtight plastic bags at −20°C and thawedovernight at room temperature before using [10]. The cadavers were fixed in aspecial holder to a table so as to achieve a knee flexion of 120°. The specimensincluded 130 mm of femur and 130 mm of tibia, with capsular tissues intact. Aregular knee arthroscopy was performed from a high anterolateral portal and theexact anatomy of the normal ACL was documented with a digitally imagestoring device. Subsequently the normal ACL was partially cut through witharthroscopic scissors leaving a small footprint of 2 mm at the anatomicalinsertion area on the lateral femoral condyle. The tibial ACL footpint waswholly removed. Using a pin with a standard dimension of 1.1 mm wedocumented the exact position of the femoral footprint through the medial andthrough the lateral portal with the 30° scope and 90° flexion of the knee.Viewing through the medial portal allows the deep-shallow extension of thefemoral footprint to be defined. Viewing through the lateral portal allows thehigh-low extension of the femoral footprint to be defined.
The tibial tunnel was then drilled using an 8 mm guidewire and a Linvatectibial guide adjusted to 45° according to Staubli et al. [11]. The extraarticularlandmarks of the tibial tunnel were 1 cm superior to the insertion of the pesanserinus and 1.5 cm medial to the tibial tubercle [12]. We targeted a positionposterior to the center of the tibial ACL footprint, parallel to the notch roof in theextended knee position. The exact position of the tibial guidewire (1.1 mm) wasradiographically documented (Fig. 1) and subsequently the tibial tunnel wasdrilled over it. A 6 mm offset femoral drill guide was positioned through thetibial tunnel and the 1.1 mm guide wire was drilled through the femur.
For the anteromedial portal we made a femoral tunnel through a lowanteromedial portal 1 cm medial to the patellar tendon and just distal to theinferior pole of the patella. After creating the tibial tunnel and performing softtissue clearance of the notch, the knee was flexed to 90° and the femoral offsetwas placed slightly anterior (or distal as viewed in 90° of knee flexion) to theanatomic AM bundle insertion site, roughly 6 mm anterior to the posterior cortexat the 2 o'clock position for left a left knee or 10 o'clock for a right knee [13].The guide wire was placed through the AM portal into the starting pointpreviously marked as the center of the femoral tunnel and the knee was flexed to120° as the guide wire was advanced through the AM portal. The guide wire wasplaced parallel to the tibial plateau and this allows a more anterior directedtunnel and avoids posterior wall blowout [14].
For the measurement of the distance of the holes to the margin of the ACL-footprint (the closest point of the footprint on the lateral femoral condyle fromthe two femoral tunnels) we photographically documented through the lowanteromedial portal, with the arthroscopic camera, the exact position of the
guide wire in each knee. The distance was measured between the margin of theACL footprint and the center of the femoral tunnel, after correction formagnification in the photographs [9] (Fig. 2).
Finally, the knees were dissected. The muscles around the knee joint and thecapsular ligament with the patella were removed so as to examine the interior of thejoint. After removing the posterior cruciate ligament the femurs were split in thesagittal plane by an oscillating saw through the highest point of the anterior outlet ofthe intercondylar notch. The exposure after splitting gave an excellent view of theACL footprint and of the two femoral tunnels (Fig. 3). We measured then, with aspecial ruler, the distance from the center of the femoral tunnel to the borderbetween the bony wall and the articular surface. We know that ACL femoralfootprint lies behind the inferior extension of the posterior femoral cortex, as thetransition between the bony lateral notch wall and the cartilage of the femoralcondyle. We documented the measurements with a conventional camera.
3. Results
3.1. Arthroscopic measurements: centers of femoral tunnels to marginof femoral ACL footprint (Table 1)
The median arthroscopically measured distance of the center oftranstibial femoral tunnel from the margin of the femoral ACL footprint
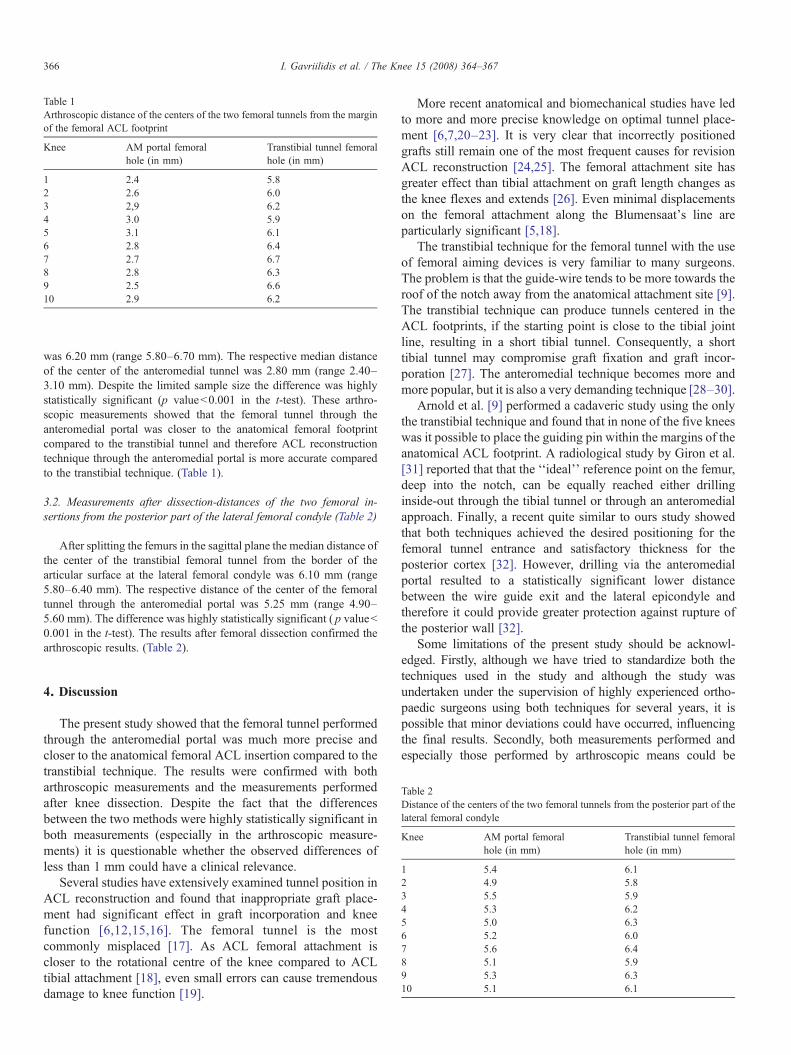
Table 1Arthroscopic distance of the centers of the two femoral tunnels from the marginof the femoral ACL footprint
Knee AM portal femoralhole (in mm)
Transtibial tunnel femoralhole (in mm)
1 2.4 5.82 2.6 6.03 2,9 6.24 3.0 5.95 3.1 6.16 2.8 6.47 2.7 6.78 2.8 6.39 2.5 6.610 2.9 6.2
366 I. Gavriilidis et al. / The Knee 15 (2008) 364–367
was 6.20 mm (range 5.80–6.70 mm). The respective median distanceof the center of the anteromedial tunnel was 2.80 mm (range 2.40–3.10 mm). Despite the limited sample size the difference was highlystatistically significant (p valueb0.001 in the t-test). These arthro-scopic measurements showed that the femoral tunnel through theanteromedial portal was closer to the anatomical femoral footprintcompared to the transtibial tunnel and therefore ACL reconstructiontechnique through the anteromedial portal is more accurate comparedto the transtibial technique. (Table 1).
3.2. Measurements after dissection-distances of the two femoral in-sertions from the posterior part of the lateral femoral condyle (Table 2)
After splitting the femurs in the sagittal plane the median distance ofthe center of the transtibial femoral tunnel from the border of thearticular surface at the lateral femoral condyle was 6.10 mm (range5.80–6.40 mm). The respective distance of the center of the femoraltunnel through the anteromedial portal was 5.25 mm (range 4.90–5.60 mm). The difference was highly statistically significant ( p valueb0.001 in the t-test). The results after femoral dissection confirmed thearthroscopic results. (Table 2).
Table 2Distance of the centers of the two femoral tunnels from the posterior part of thelateral femoral condyle
Knee AM portal femoralhole (in mm)
Transtibial tunnel femoralhole (in mm)
1 5.4 6.12 4.9 5.83 5.5 5.94 5.3 6.25 5.0 6.36 5.2 6.07 5.6 6.48 5.1 5.99 5.3 6.310 5.1 6.1
4. Discussion
The present study showed that the femoral tunnel performedthrough the anteromedial portal was much more precise andcloser to the anatomical femoral ACL insertion compared to thetranstibial technique. The results were confirmed with botharthroscopic measurements and the measurements performedafter knee dissection. Despite the fact that the differencesbetween the two methods were highly statistically significant inboth measurements (especially in the arthroscopic measure-ments) it is questionable whether the observed differences ofless than 1 mm could have a clinical relevance.
Several studies have extensively examined tunnel position inACL reconstruction and found that inappropriate graft place-ment had significant effect in graft incorporation and kneefunction [6,12,15,16]. The femoral tunnel is the mostcommonly misplaced [17]. As ACL femoral attachment iscloser to the rotational centre of the knee compared to ACLtibial attachment [18], even small errors can cause tremendousdamage to knee function [19].
More recent anatomical and biomechanical studies have ledto more and more precise knowledge on optimal tunnel place-ment [6,7,20–23]. It is very clear that incorrectly positionedgrafts still remain one of the most frequent causes for revisionACL reconstruction [24,25]. The femoral attachment site hasgreater effect than tibial attachment on graft length changes asthe knee flexes and extends [26]. Even minimal displacementson the femoral attachment along the Blumensaat's line areparticularly significant [5,18].
The transtibial technique for the femoral tunnel with the useof femoral aiming devices is very familiar to many surgeons.The problem is that the guide-wire tends to be more towards theroof of the notch away from the anatomical attachment site [9].The transtibial technique can produce tunnels centered in theACL footprints, if the starting point is close to the tibial jointline, resulting in a short tibial tunnel. Consequently, a shorttibial tunnel may compromise graft fixation and graft incor-poration [27]. The anteromedial technique becomes more andmore popular, but it is also a very demanding technique [28–30].
Arnold et al. [9] performed a cadaveric study using the onlythe transtibial technique and found that in none of the five kneeswas it possible to place the guiding pin within the margins of theanatomical ACL footprint. A radiological study by Giron et al.[31] reported that that the ‘‘ideal’’ reference point on the femur,deep into the notch, can be equally reached either drillinginside-out through the tibial tunnel or through an anteromedialapproach. Finally, a recent quite similar to ours study showedthat both techniques achieved the desired positioning for thefemoral tunnel entrance and satisfactory thickness for theposterior cortex [32]. However, drilling via the anteromedialportal resulted to a statistically significant lower distancebetween the wire guide exit and the lateral epicondyle andtherefore it could provide greater protection against rupture ofthe posterior wall [32].
Some limitations of the present study should be acknowl-edged. Firstly, although we have tried to standardize both thetechniques used in the study and although the study wasundertaken under the supervision of highly experienced ortho-paedic surgeons using both techniques for several years, it ispossible that minor deviations could have occurred, influencingthe final results. Secondly, both measurements performed andespecially those performed by arthroscopic means could be

367I. Gavriilidis et al. / The Knee 15 (2008) 364–367
questioned in terms of accuracy. However, the correction formagnification in photographs used for the measurement of themargin of the ACL footprint from the center of the femoral tunnelprobably eliminated the resulting bias.
Location of the femoral tunnel is very important, because itdoes not only determine graft tension, but it also affects theligamentization process of graft healing [33]. The posteriorplacement of the graft and the lateral removal of the femoraltunnel restores more natural knee kinematics [7,34]. The pro-blem with AM portal is the limited visibility and also the ex-cessive angulation of the tunnel in the sagittal plane [35] whichmay erode the anterior portion of the knee resulting in bonetunnel enlargement [36]. So the surgeon must be very ex-perienced and confident with the arthroscope, if he wants tosucceed in reaching the anatomic positioning of femoral tunnel.
Conflict of interest statement
No funding or external support was received by any of theauthors in support of or in any relationship to the study.
The authors are not aware of any conflict of interests arisingfrom the publication of the manuscript.
References
[1] Garofalo R, Moretti B, Kombot C, Moretti L, Mouhsine E. Femoral tunnelplacement in anterior cruciate ligament reconstruction: rationale of the twoincision technique. J Orthop Surg 2007;2:10.
[2] Ristanis S,GiakasG, PapageorgiouCD,Moraiti T, StergiouN, et al. The effectsof anterior cruciate ligament reconstruction on tibial rotation during pivotingafter descending stairs. Knee Surg Sports Traumatol Arthrosc 2003;11:360–5.
[3] Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciateligament anatomy and function relating to anatomical reconstruction. KneeSurg Sports Traumatol Arthrosc 2006;14:982–92.
[4] Tashman S, Collon D, Anderson K, Kolowich P, Anderst W. Abnormalrotational knee motion during running after ACL reconstruction. Am JSports Med 2004;32:975–83.
[5] Zavras TD, Race A, Bull AM, Amis AA. A comparative study of ‘isometric’points for anterior cruciate ligament graft attachment. Knee Surg SportsTraumatol Arthrosc 2001;9:28–33.
[6] Musahl V, Plakseychuk A, VanScyoc A, Sasaki T, Debski RE, McMahonPJ, et al. Varying femoral tunnels between the anatomical footprint andisometric positions: effect on kinematics of the anterior cruciate ligament-reconstructed knee. Am J Sports Med 2005;33:712–8.
[7] Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL. Knee stabilityand graft function following anterior cruciate ligament reconstruction:comparison between 11 o’clock and 10 o’clock femoral tunnel placement.Arthroscopy 2003;19:297–304.
[8] Scopp JM, Jasper LE, Belkoff SM, Moorman III CT. The effect of obliquefemoral tunnel placement on rotational constraint of the knee reconstructedusing patellar tendon autografts. Arthroscopy 2004;20:294–9.
[9] Arnold MP, Kooloos J, van Kampen A. Single incision technique missesthe anatomical femoral anterior cruciate ligament insertion: a cadaver study.Knee Surg Sports Traumatol Arthrosc 2001;9:194–9.
[10] WooSLY,OrlandoCA,Camp JF,AkesonWH.Effects of postmortem storageby freezing on ligament tensile behavior. J Biomech 1986;19:399–404.
[11] Staubli HU, Rauschning W. Tibial attachment area of the anterior cruciateligament in the extended knee position. Anatomy and cryosections in vitrocomplemented by magnetic resonance arthrography in vivo. Knee SurgSports Traumatol Arthrosc 1994;2:138–46.
[12] Morgan CD, Kalman VR, Grawl DM. Definitive landmarks for reprodu-cible tibial tunnel placement in anterior cruciate ligament reconstruction.Arthroscopy 1995;11:275–88.
[13] Harner CD, Honkamp NJ, Ranawat AS. Anteromedial portal technique forcreating the anterior cruciate ligament femoral tunnel. Arthroscopy 2008;24:113–5.
[14] O’Donell JB, Scerpella TA. Endoscopic anterior cruciate ligament recons-truction: Modified technique and radiographic review. Arthroscopy 1995;11:577–84.
[15] Friedman RL, Feagin Jr JA. Topographical anatomy of the intercondylarroof: a pilot study. Clin Orthop Relat Res 1994;306:163–70.
[16] Yaru NC, Daniel DM, Penner D. The effect of tibial attachment site ongraft impingement in an anterior cruciate ligament reconstruction. Am JSports Med 1992;20:217–20.
[17] Topliss C, Webb J. An audit of tunnel position in anterior cruciate ligamentreconstruction. Knee 2001;8:59–63.
[18] Khalfayan EE, Sharkey PF, Alexander AH, Bruckner JD, Bynum EB. Therelationship between tunnel placement and clinical results after anteriorcruciate ligament reconstruction. Am J Sports Med 1996;24:335–41.
[19] Harner CD, Giffin JR, Dunteman RC, Annunziata CC, Friedman MJ.Evaluation and treatment of recurrent instability after anterior cruciateligament reconstruction. J Bone Jt Surg Am 2000;82:1652–64.
[20] Markolf KL, Hame S, Hunter DM, Oakes DA, Zoric B, Gause P, et al.Effects of femoral tunnel placement on knee laxity and forces in an anteriorcruciate ligament graft. J Orthop Res 2002;20:1016–24.
[21] Sakane M, Fox RJ, Woo SL, Livesay GA, Li G, Fu FH. In situ forces in theanterior cruciate ligament and its bundles in response to anterior tibialloads. J Orthop Res 1997;15:285–93.
[22] SimmonsR,Howell SM,HullML. Effect of the angle of the femoral and tibialtunnels in the coronal plane and incremental excision of the posterior cruciateligament graft: an in vitro study. J Bone Jt Surg Am 2003;85-A:1018–29.
[23] Sudhahar TA, Glasgow MM, Donell ST. Comparison of expected vs. actualtunnel position in anterior cruciate ligament reconstruction. Knee 2004;11:15–8.
[24] Passler HH, Hoher J. Intraoperative Qualitatskontrolle bei der Bohrkanal-platzierung vom vorderen kreuzbandersatz. Unfallchirurg 2004;107:263–72.
[25] Eichhorn J, Girdano N. Computerassistierte Rekonstruction des vorderenkreuzbandes mit dem Navigations-system. Arthroskopie 2005;18:24–6.
[26] Muneta T, Yamamoto H, Sakai H, Ishibashi T, Furuya K. Relationshipbetween changes in length and force in invitro reconstructed anteriorcruciate ligament. Am J Sports Med 1993;21:299–304.
[27] Heming JF, Rand J, SteinerME.Anatomical limitations of transtibial drilling inanterior cruciate ligament reconstruction.AmJ SportsMed 2007;35: 1708–15.
[28] Chhabra A, Kline AJ, Nilles KM, Harner CD. Tunnel expansion afteranterior cruciate ligament reconstruction with autogenous hamstrings: acomparison of the medial portal and transtibial techniques. Arthroscopy2006;22:1107–12.
[29] Hantes M, Zachos V, Basdekis G, Zibis A, Daliana Z, Malizos K. Dif-ferences in graft orientation using the transtibial and anteromedial portaltechnique in ACL reconstruction: an MRI prospective study. J Bone Jt SurgBr 2006;88(suppl I):93.
[30] Paessler H, Rossis J, Mastrokalos D, Kotsovolos I. Anteromedial vs trans-tibilal technique for correct femoral tunnel placement during arthroscopicACL reconstruction with hamstrings: an in vivo study. J Bone Jt Surg Br2004;86(suppl III):234.
[31] Giron F, Buzzi R, Aglietti P. Femoral tunnel position in anterior cruciateligament reconstruction using three techniques.A cadaver study. Arthroscopy1999;15:750–6.
[32] Albuquerque RF, Amatuzzi MM, Pacheco AP, Angelini FJ, Campos Jr O.Positioning of the femoral tunnel for arthroscopic reconstruction of the anteriorcruciate ligament: comparative study of 2 techniques. Clinics 2007;62: 613–8.
[33] Howell SM, Taylor MA. Failure of reconstruction of the anterior cruciateligament due to impingement by the intercondylar roof. J Bone Jt Surg Am1993;75:1044–55.
[34] Amis AA, Jakob RP. Anterior cruciate ligament graft positioning, tensioningand twisting. Knee Surg Sports Traumatol Arthrosc 1998;6:S2–S12.
[35] Segawa H, Koga Y, Omori G, Sakamoto M, Hara T. Influence of the femoraltunnel location and angle on the contact pressure in the femoral tunnel inanterior cruciate ligament reconstruction. Am J Sports Med 2003;31:444–8.
[36] Friederich NF, Müller W, O'Brien WR. Clinical application of biomechanicand functional anatomical findings of the knee joint. Orthopade 1992;21:41–50.



![The transtibial versus the anteromedial portal …...arthroscopic single-incision BPTB ACL reconstruction was initially described through the TT technique [23], where the femur is](https://img.dokumen.tips/doc/110x75/5f856acc944e8872860b1a93/the-transtibial-versus-the-anteromedial-portal-arthroscopic-single-incision.jpg)