Embed Size (px)
Citation preview

TRANSPLANTATION OF THE GLUTEUS MAXIMUS MUSCLE
(A PRELIMINARY REPORT)*
J. DEWEY BISGARD, M.D.
CHICAGO
T HE disabiIity resuIting from the Ioss of gIutea1 muscIe function and the frequency of its occurrence in
the residuum of anterior poIiomyeIitis has inspired severa pIastic operations designed for the functiona substitution or partia1 repjacement of this important muscIe group. In their endeavors to reestabIish these functions of extension and abduction in the affected extremities Lange,’ Ober,2 Legg,3 Hey Groves,4 Yer- gason,” and DicksonG have utiIized the sacrospinaIis (erector spinae), the tensor fascia femoris, and the semitendinosus muscIes by various ingenious pIastic opera- tions. These observers have reported reIa- tive functiona improvement in their cases as manifested by an increased stabiIity of the hip joint with greater certainty of gait (Iess Iimp) and increased endurance in walking.
remaining proxima1 portion through a subcutaneous tunne1 over the sacrum for transmission of its action to its newIy estabIished insertion, the greater tro- chanter of the opposite side. This operation was done in two cases which presented suitabIe indications, but insuffrcient time has eIapsed to permit a fina evaIuation of the functiona resuIts. However, in both instances paIpation at the present time eIicits contraction of the transpIanted segments simuItaneousIy with abduction of the extremities and in one, increased stability of the respective hip joint.
A supplementary report with end results wiI1 be published at a Iater date. At this time a brief description of the operative technique wiI1 be given.
OPERATIVE TECHNIQUE
The possibiIity of transpIanting a portion of the gIuteus maximus muscle from the norma uninvoIved side to exert its muscIe puI1 for partia1 repIacement of the action of its paraIyzed contraIatera1 feIIow and gluteus medius was considered, and its rationaIe and technica detaiIs verified and evoIved by anatomica dissection. It was found that the muscIe beIIy couId be spIit IongitudinaIIy at the bifurcation of the inferior gIutea1 nerve and independent nerve and bIood suppIies preserved in both segments (the inferior and superior gIutea1 vesseIs providingdua1 circuIatory channeIs). Thus, anatomicaIIy, it appeared that it was possibIe to Ieave undisturbed the dista1 one- haIf or one-third of the muscIe to carry on its norma function and to transpIant the
With the patient in a prone position an incision is carried from 4 inches beIow the greater trochanter to the posterior inferior spine of the ilium of the normal (donor) side and the fascia overlying the gIuteus maximus muscIe is exposed by a wide subcutaneous dissection. The part of the muscuIar insertion which joins the tensor fascia Iata is incised so as to include a strip of this fascia 1 or 5 inches in length. The muscIe beIIy is then split and the proxima1 portion dissected up to its origin where the inferior gIutea1 nerve is identified. At this point great care is exercised to carry the furtfler division of the muscIe between the branches of this nerve to insure innervation of both segments. The transpIant is then freed with smaI1 shavings of bone by an
* From the University of Chicago Department of Surgery, Division of Orthopedics.
373

3 14 American Journal of Surgery Bisgard-GIuteus Maximus Muscle FEBRUARY. 1933
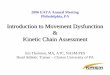
osteotome from its iliac and part of its is estabIished between the two incisions. sacra1 origins. At this stage the transpIant The free end of the transpIant incIuding is quite free with the exception of its nerve its fascia Iata proIongation is drawn
reflected to show blood and nerve \
and vascuIar pedicIes. The
FIG. I.
base (origin) through this tunne1 over the sacrum is then rotated through an arc of 180’ and is firmIy anchored into the greater and re-attached to the sacrum by a few trochanter of the recipient extremity. sutures of heavy siIk. A smaI1 incision is This probabIy is best accompIished by made over the greater trochanter of the passing the fascia through a driI1 hole paralytic hip and a subcutaneous tunne1 in the trochanter.
[ConcIuded on p. 334.1