Embed Size (px)
Citation preview

Total Etch-The Rational Dentin Bonding Protocol
Raymond L. Bertolotti, D.D.S., Ph.D., F.A.D.M.
Phosphoric acid etching of dentin is critically reexamined in view of current adhesive resin development. Research and clinical experience both suggest that ‘‘total etch,” the simultaneous etching of dentin and enamel, is a rational protocol with many modem adhesive resins.
ACID ETCHING OF DENTIN
hosphoric acid etching of enamel’ has been P widely accepted since its introduction in 1 19557 Phosphoric acid etching of dentin
was introduced by Fusayama and co-workers in 1977.2 Numerous studiess7 have reported clinical success with adhesive resins applied to phosphoric acid etched dentin. The resins used were apparently capable of forming a good “seal” with the etched dentin. On the total etched tooth, the same resins were used as both an enamel bond and a dentin bonding agent (DBA). Despite over 13 years of clinical success with Fusa- yama’s Clearfil F (Kuraray) system, as well as success with other adhesive systems, phosphoric acid etching of dentin remains controversial.
The controversy concerning phosphoric acid ap- pears to have resulted from adverse experiences, which occurred when some nonadhesive resins were applied to etched dentin. As pointed out by Kanca8 and Bran- n s t r ~ r n , ~ many of the early studies that reported phos- phoric acid to be a pulpal irritant may have been incorrectly interpreted. For example, in an often refer- enced publication, Macko et all0 placed a zinc oxide- eugenol restorative material in paired cavities with and without prior phosphoric acid etching. The etched cavities demonstrated slight-to-moderate pulpal inflam- mation (in the absence of clinical pain) after placement of a zinc oxide-eugenol restoration. Phosphoric acid was the only variable and the resulting idammation was attributed to probable irritation by the acid. Eugenol has subsequently been shown to be a pulpal irritant. I t is now known that phosphoric acid removes the smear layer, increasing dentin permeability. l2 It is reasonable to attribute the inflammation of the acid treated teeth to the eugenol permeating the dentin. HumeI3 observed that the smear layer is effective in reducing eugenol permeation to the pulp. These observations support the
Private practitioner, San Leandro. California. Address reprint requests to Raymond L. Bertolotti, Fifth Quarter Dental
Seminars. 425 Estudillo Avenue, San Leandro, CA 94577. 1991 Decker Periodicals Publishing, Inc.
Kanca hypothesis that eugenol, not the phosphoric acid, was the cause of pulpal irritation in the Macko study.
Several other studies directly investigated the effects of phosphoric acid on vital teeth. Brannstrom et all4 found that phosphoric acid in silicate cement did not irritate the pulp as long as bacterial invasion was prevented. Johnson et all5 investigated 7-day exposure of dentin to phosphoric acid and reported no more pulpal irritation than resulted in a distilled water control group.
Many restorative protocols have attempted to avoid dentin exposure to phosphoric acid. These protocols usually involve placement of calcium hydroxide or glass ionomer liners, or perhaps a dentin adhesive resin, prior to enamel etching. Yet total avoidance of dentin exposure to phosphoric acid is clinically impossible. To do so would be time consuming, if indeed at all pos- sible.
In the early 1980s, it is likely that widespread use of liners under composites, especially glass ionomers, which were subsequently acid etched to enhance com- posite adhesion,I6 led to untoward sensitivity. As ex- plained by Fusayama, l6 the glass ionomer liner can be lifted from the cavity floor by polymerization shrinkage of the overlying bonded composite, thereby exposing dentinal tubules. The fluid in the tubules moves as a result of pressure changes in the void, inducing sen- sitivity to temperature changes or to bite pressure. Without the lining, sensitivity would have been less likely, since the dentin bonding strength of resins, especially to smear layer removed dentin, is typically much higher than that of glass ion~mers . ’~.’~ Clinical experience has shown that thin, flat, glass ionomer liners in “ideal“ Class I or Class I1 cavity preparations often result in sensitivity, while glass ionomer bases in deep preparations rarely result in sensitivity. This ob- servation is easily explained by the ability of glass ionomer to resist lift-off in deep “holes” where mechani- cal retention is a factor. Geometry may also explain the absence of clinical sensitivity in Class 111, IV, and V cavities, with or without liners, in contrast to common sensitivity in Class I and I1 restorations.
Most of Fusayama’s etched dentin research has in- volved carious dentin. The carious dentin is less per- meable to phosphoric acid than is normal dentin.lg One
1

JOURNAL OF ESTHETIC DENTISTRY/VOLUME 3, NUMBER 1 January/Febmary 1991
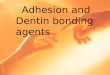
Figure 1. A, Nonadhesive resin tags into etched vital dentin. [Photograph supplied by Professor M. Iwaku.)
might expect the effect of phosphoric acid on carious dentin to be more mild than on normal dentin, possibly causing reason to question the research results in ap- plication to normal dentin. This concern for the effect of phosphoric acid on ‘‘normal‘‘ dentin was investigated by TatsumL2’ who found that vital monkey dentin remineralized rather quickly after demineralization by phosphoric acid. Inokoshi et a 1 2 1 have shown that phos- phoric acid, as well as nitric acid, affects only about the outer 10 microns of the dentinal tubules in vital teeth.
In extracted teeth, those most often used for dentin bonding research, the effects of etching are much more profound. Resin tags of 300 microns are not uncom- mon in nonvital teeth, while typical tags in vital teeth are about 10 microns22 as illustrated in Figure 1. There is clearly reason to question the validity of dentin bond values reported for extracted teeth.
THE DENTAL MANUFACTURER’S DECISION
It is now evident that dental materials manufac- turers have made their decisions about acid etching of dentin. One need only examine the content of many current generation dentin “conditioners.” Acids such as nitric are a popular ingredient. Nitric acid is a strong acid, even stronger than phosphoric acid. It easily removes smear layers too. Yet nitric acid is not general- ly feared, probably because the DBAs (e.g.,Tenure, Den-Mat; Mirage Bond, Chameleon; Restobond 3, Lee Pharmaceuticals), which utilize these nitric acid “con- ditioners” are in fact highly adhesive. No sensitivity results from smear layer removal and application of the DBA. There have been no nitric acid studies analogous to the early phosphoric studies that reported sen-
Figure 1. B, Adhesive resin tags into etched vital dentin. (Photograph supplied by Professor M. Iwaku.)
sitivity. A recent showed that the “oxylates” in some conditioners containing both nitric acid and an oxylate “mordant” are not necessary. Pure 2.5 percent nitric acid is just as effective in cleansing the dentin and creating bonds to the DBA. The dissociation con- stants, listed in Table 1, indicate the relative acidities of several acids used to modify teeth.
Most clinically successful DBAs seem to follow a similar protocol. Etch or “condition” to remove the smear layer, apply an adhesion promoter, then a quick curing low viscosity resin. It is important that the low viscosity resin quickly polymerize in the opened den- tinal tubules before pulpal pressure fils the tubules with For a good bond, the DBA must be poly- merized before the polymerization shrinkage of the overlying composite can separate the DBA from the dentin.
CLINICAL EXPERIENCE
Two long-term clinical trials of phosphoric acid etched dentin are of particular interest. Iwaku et a15 reported a 5- to 6-year longitudinal clinical study in which they found only one adverse pulp response out of 93 cases. This adverse response appeared to be
Table 1. Dissociation Constants of Some Acids Used in Tooth Etching and “Conditioning”
Acid P16
Hydrochloric Nitric Maleic Phosphoric Citric
-1.4 -1.4
1.8 2.3 3.1
*used in enamel microabrasion.
2

Total Etch
caused by missed carious dentin. In another study, Shintani et a14 reported no pulpal problems in 213 cases after 4 years where total etch followed by either Scotchbond (3M Dental) or Clearfiil F were used. These and similar studies have been largely ignored, being overwhelmed with studies that avoided exposure of dentin to phosphoric acid.
With the clinically successful "total etch" protocol in mind, the present author surveyed approximately 3,200 North American and Australian clinicians who had attended a seminar on the concept of total etching. Advocated was total etching with 38 percent liquid phosphoric acid for 15 to 30 seconds. Specifically dis- cussed was the application of New Bond (Kuraray), a DBA designed for phosphoric acid etched dentin, fol- lowed by placement of composite within 1 minute. [New Bond is an improved version of Clearfii F.) While not tabulated, the majority are presumed to have used a light-cured composite resin, contrary to the popularity of self-cured composite resins used with New Bond in Japan. Six hundred and twenty responses (about 19 percent) were received.
Eighty-eight percent of respondents said they had tried total etching with phosphoric acid on both dentin and enamel, and 12 percent said they had not. New Bond was the most often used DBA with 69 percent of respondents affirming its use. Twelve percent said they had not used New Bond and 19 qualified their answer to use in specific situations. Dual Cured Scotchbond drew 20 percent users, 70 percent nonusers. Eight per- cent of respondents used Photo Bond (Kuraray) while 88 percent did not. Thirty-five percent of respondents indicated use of "other" bonding agents not specifically advocated for use during the seminar. Space was provided for the names of these agents. Sixty-five per- cent of respondents did not use "other" bonding agents. In answer to the question, "Did you experience more problems than with your previous, nonphosphoric acid technique of dentin bonding?" 8 percent of respondents replied in the affirmative. Eighty-one percent said they had not experienced more problems, and 11 percent were unsure. Those who responded with a yes were given an opportunity to describe the problem as follows: sensitivity/debond/other. They were also asked if direct versus indirect (inlay, etc.) procedures affected the results. They were given a blank space in which to comment on a yes response. Five percent of respon- dents answered in the affirmative, 14 percent said no, and 81 percent were unsure. Nine percent said yes to the question, "Did the brand of dentin bonding material make a difference?" They were given space to explain. Thirty-nine percent said no and 52 percent were not sure. Of particular interest is that 98 percent of the respondents who have tried phosphoric etching of den- tin (with a variety of DBAs) continued to use the pro- cedure "frequently" or "exclusively." It is worth noting that all of the 2 percent who didn't continue had not used New Bond.
Sensitivity, the most common traditional fear, was rare. The most frequently reported "problem" was debonds, but the majority of the debonds occurred with use of enamel bonding resins, rather than DBAs. Often named were Enamel Bond (3 M Dental) and Visar Seal (Den-Mat). Several bonding agents were reported to be clinically successful with this etching procedure, the most frequently reported being Tenure, then Dual Cure Scotchbond, and finally Photo Bond. The results show that the fears of dentin etching with phosphoric acid were not clinically apparent as long as a proper DBA is used. The successful DBAs are known to contain the requisite adhesion promoters and quick curing, low vis- cosity resins. Sensitivity was reported by a small minority. These usually occurred when an "enamel bonding" resin rather than a DBA was used. Specifi- cally named in more than one instance were Scotchbond 2 (black bottle) and Visar Seal. These resins do not contain the necessary adhesion promoter required by the total etch protocol. Scotchbond 2 has an adhesion promoter (HEMA) in the matching (gold bottle) "conditioner." I t is absent when the conditioner is omitted and replaced with phosphoric acid. However, personal experience has shown that Scotchbond 2 is clinically successful with total etch if both the con- ditioner (not washed off) and the resin follow the phos- phoric acid etching, washing, and drying. Visar Seal, as well as Enamel Bond, lacks the requisite dentin ad- hesion promoter. I t is sold for enamel bonding or for use over the same manufacturer's DBA (Tenure).
When these survey results are combined with the experience of contemporary Japanese dentists, many of whom view phosphoric acid etching of dentin as "routine" with the Fusayama technique, it is hard to rationalize many of the current restorative resin pro- tocols. They appear to be needlessly complicated and are likely inferior to more simple approaches.
RATIONAL RESTORATION OF PREPARED CAVITIES
The bonding of resins to dentin and enamel will now be discussed in view of current knowledge and dental products.
Prepared enamel and dentin are quite different. Phosphoric acid etched enamel is generally free of microleakage when etched and bonded with resin. Den- tin is not generally free of microleakage when etched and bonded with a wide variety of etchants and resins. However, the microleakage of some resins on dentin may be less than that experienced with the cement's glass i0nome3~ or zinc phosphate.26 Nitric acid etching of enamel and dentin, a relatively new concept, has not been as thoroughly researched as phosphoric acid etching. Nitric acid was not apparently researched in the early studies leading to the phosphoric acid etching
3

JOURNAL OF ESTHETIC DENTISTRY/VOLUME 3, NUMBER 1 January/Februnry 1991
Irigure 2. A, Caries Detector.
fears. Bond strengths and etch morphology appear to be comparable for 37 percent phosphoric and 2.5 per- cent nitric a ~ i d . ~ ~ . ~ ' One might speculate that the nitric acid concentration or etching time could be improved with further research.
Current generation dentin bonding agents general- ly remove the dentin smear layer or modify it. Dentin conditioners which remove the smear layer are general- ly washed off, while conditioners which modify the smear are generally not washed off. Commercial ex- amples are Gluma #2 (Bayer) and Tenure Conditioner (Den-Mat), which are washed off, removing the smear, and Scotchbond 2 Primer (3M) and All Bond primer (Bisco), which are not washed off, leaving a modified smear.
Many bonding protocols using separate enamel etchants and dentin conditioners are difl[icult, if not im- possible, to accomplish. Restricting phosphoric acid etchant, even in the gel form, to enamel or the dentin primer to dentin are impossible in a clinical setting. The consequences can be less than ideal bonding of the dentin or the enamel. More rational is to use a dentin and enamel protocol that does not restrict application of materials to selected areas.
Given the evidence that acids and composites do not irritate the pulp, one needs to critically examine the need for bases. For indirect restorations, undercuts must be eliminated. It appears prudent to use glass ionomer materials for these situations. Glass ionomer is cariostatic, adheres sufliciently well to be retained in small or retentive areas (but not in thin, flat layers on the pulpal floor) and it seals well. A recently intro- duced light-curing glass ionomer, Vitrabond (3M Den- tal) appears to be especially well suited to this use because of its convenient application, tenacious bond to dentin, and fluoride release. However, it is not con- venient for thick application and, due to its HEMA con- tent, has potential to adhere to resin temporaries. When adhesion to a resin temporary is anticipated to
Figure 2. B, Tentative caries removal guided by tactical means.
be a problem, glass ionomer base cements without HEMA would be preferred. A base may also be desired for thermal insulation under deep metallic restorations. Routine bases appear to be unnecessary, if not un- desirable, with current generation DBAs. Especially to be avoided are large calcium hydroxide bases, which become soft upon water exposure, making them unable to provide support for the overlying restoration. To be- come convinced, one need only remove a failed restora- tion to discover a calcium hydroxide base with the consistency of "cottage cheese." Calcium hydroxide may, however, be prudent as a limited area pulp cap material when covered by another base such as glass ionomer when calcification is desired. On the other hand, many endodontists feel that the calcium hydroxide makes endodontic therapy more difficult. However, direct exposure of the pulp to phosphoric acid does not appear to result in any clinical problems.28 Due to the difficulty in achieving bonds to deep den- tin,29 it is prudent to utilize a moisture-tolerant base in deep restorations. In the clinical experience of the author, Vitrabond has performed well as a pulp cap- ping material when used in a limited area and the remaining dentin etched with phosphoric acid prior to application of the DBA.
Caries removal should be guided by a caries detect- ing solution (e.g., Caries Detector, Kuraray), which dif- ferentiates the bacteria invaded, nonmineralizable, senseless outer carious dentin from the inner carious dentin, which will remineralize and should not be removed.30 Caries Detector use is illustrated in Figure 2. Hardness, the traditional guide to caries removal, results in over-cutting pdpally in nearly all cases. After caries removal and possibly limited basing, total etch is a strong candidate for optimal re~tora t ion .~~ The final restoration may be indirect resin, porcelain, bonded cast bonded amalgam,33 or direct resin. The DBA should be one known to work with total etch. The Clearfil system has the benefit of over 13 years of cM-
4

Total Etch
Figure 2. C, Application of Caries Detector.
Figure 2. D, Bacterial invaded dentin revealed after washing.
cal experience with total etch. Recent experience with total etch and a variety of adhesive DBAs, particularly Tenure and Dual Cure Scotchbond suggests that they also work The first DBA manufactured outside Japan with total etch instructions, utilizing phosphoric acid dentin etchant is All Bond. It, too, appears promis- ing.
The profession must not continue to ignore the suc- cessfd adhesive resin techniques, including etched den- tin, fist described by Fusayama’s group. To continue to unnecessarily remove mineralizable tooth structure without guidance of a caries detector, to develop and use needlessly complex bonding protocols, and to use bases and h e r s routinely does not appear prudent in view of our current knowledge and clinical experience.
Figure 2. E, Appearance after removal of stained dentin and reapplication of Caries Detector.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
REFERENCES Buonocore MG. A simple method of increasing the ad- hesion of acrylic filling materials to enamel surfaces. J Dent Res 1955:34:849-853. Fusayama T, Nakamura M, Kurosaki N, Iwaku M. Non- pressure adhesion of a new adhesive restorative system. J Dent Res 1979:58: 1364-1370. FusayamaT. New concepts in operative dentistry. Chicago: Quintessence, 1980. Shintani H. Satou N, Satou J. Clinical evaluation of two posterior composites retained with bonding agent. J Pros- thet Dent 1989;62:627-632. Iwaku M. Inokoshi S . HosodaH, FusayamaT. Conservative dentistry with a caries detector and a chemically adhesive composite, a longitudinal study of a new system. Br Dent
Bertolotti FU. Acid etching of dentin. Quintessence Int
Kanca J 111. One year evaluation of a dentin-enamel bond- ing system. J Esthet Dent 1990;2:100-103. Kanca J 111. An alternative hypothesis to the cause of pulpal inflammation in teeth treated with phosphoric acid. Quin- tessence Int 1990:21:83-86. Brannstrom M. Dentin and pulp in restorative dentistry. London: Wolfe Medical, 1982. Macko DL, Rutberg M, Langeland K. Pulp response to the application of phosphoric acid to dentin. Oral Surg 1978:45;930-940. Inokoshi S, Fujitani M, Hosoda H. Pulpal response to Panavia EX. In: Adhesive Prosthodontics, Academy of Den- tal Materials. Nqmegen: Eurosound. 1986:47-55. Pashley DH, Michelich V, Kehl T. Dentin permeability: ef- fects of smearlayerremoval. JProsthetDent 1981:46:531- 537. Hume W. An analysis of the release and the diffusion through dentin of eugenol from zinc oxide-eugenol mix- tures. J Dent Res 1984:63:881-884. Brannstrom M, Vojinovic 0, Novenvall KJ . Bacteria and pulpal reaction under silicate cement restorations. J Pros- thet Dent 1979;4 1 :290-295.
J 1983:155:19-22.
1990;2 1 : 77-78.
5

JOURNAL OF ESTHETIC DENTISTRY/VOLUME 3, NUMBER 1 January/February 1991
15. Johnson RH. CMstensen GJ, Stigers R, Lasewell HR. Pul- pal irritation due to the phosphoric acid component of sili- cate cement. Oral Surg 1970;29:447-454.
16. Fusayama T. Factors and prevention of pulp irritation by adhesive composite resin restorations. Quintessence Int 1987: 18:633440.
17. Wilson AD, McLean JW. Glass Ionomer Cement. Chicago: Quintessence, 1988.
18. Himoura K, Moore BK. Phillips RW. Tensile bond strength between glass ionomer cement and composite resin. J Am Dent Assoc 1987;114: 167-172.
19. Ogawa K, Yamashita Y, Ichijo T, Fusayama T. The ultra- structure and hardness of the transparent layer of human carious dentin. J Dent Res 1983;62:7-10.
20. Tatsumi T. Physiological remineralization of artificially decalcified monkey teeth under adhesive composite res- toration. J Stom Soc Jpn 1989;56:47-74.
21. Inokoshi S, Hosoda H, Harnirattisai C, et al. A study on the resin impregnated layer of dentin. Jpn J Conserv Dent 1990:33:427-442.
22. Iwaku M. Nakamichi K, Horie K, et al. Tags penetrating dentin of a new adhesive resin. Bull Tokyo Med Dent Univ 1981:28:45-51.
23. Blosser RL, Bowen RL. Effects of purified ferric oxa- late/nitric acid as a pretreatment for the NTG-Gh4A and PMDM bonding system. Dent Mater 1988;4225-231.
24. Torstenson B, Nordenwall J, Brannstrom M. Pulpal reac-
tion and microorganisms under Clearfii composite resin in cavities with acid etched dentin. Swed Dent J 1982:
25. Shortall A, Fayyad M, Williams JD. Marginal seal of injec- tion molded ceramic crowns cemented with three adhesive systems. J Prosthet Dent 1989;6 1:24-27.
26. Tjan AHL. DUM JR. Grant BE. Microleakage ofcast crowns cemented with a new adhesive resin. J Dent Res 1990;69 Special issue, Abstract number 120.
27. Bowen RL, Cobb EN. A method for bonding to dentin and enamel, J Am Dent Assoc 1983; 107:734-746.
28. Godfrey JL. Bonded porcelain inlays: a better alternative to amalgam. Austral Dent Assoc News Bull 1990; 169:25- 27.
29. Tagami J, Tao L. Pashey DH. Correlation among dentin depth, permeability and bond strength of adhesive resins. Dent Mater 1990:6:45-50.
30. Fusayama T. Clinical guide for removing caries using a caries-detecting solution. Quintessence Int 1988: 19:397- 401.
31. Fusayama T. Optimal cavity wall treatment for adhesive restorations. J Esthet Dent 1990:2:95-99.
32. Uchiyama Y. Adhesion in prosthetic restorations. Adhesive Prosthodontics, Academy of Dental Materials. Nijmegen: Eurosound, 1986:2 1-31.
33. Lacy AM, Staninec MA. The bonded amalgam restoration. Quintessence Int 1989;20:52 1-524.
6: 167-1 76.
6