Embed Size (px)
Citation preview

PHENOTYPES OF THROMBOEMBOLIC
PULMONARY EMBOLISM
TIMOTHY A. MORRIS, MD
PROFESSOR OF MEDICINE
UCSD MEDICAL CENTER
SAN DIEGO, CA
Timothy A. Morris, MD is a Professor of Medicine and the Clinical Service Chief for the Division of Pulmonary and Critical Care Medicine at University of California San Diego (UCSD) Medical Center, Hillcrest facility. His center was ranked in the top 10 hospitals for pulmonary medicine in 2014. It was ranked under the Mayo clinic because of low scores in the “Showing Up to Work Despite the Bitter Cold” category. His outpatient, inpatient and ICU practice includes direct care of patients as well as gently supervising the care provided by housestaff and fellows. He is the longstanding Medical Director of the Pulmonary Function Laboratory and the Department of Respiratory Care, which has been recognized for its quality and leadership by the American Association for Respiratory Care. Despite his notoriety, he takes his own garbage cans to the curb weekly. Dr. Morris received his MD degree from Georgetown University School of Medicine in 1987, just prior to when his current fellows were born. He may have delivered one or two of them. He trained in internal medicine at Georgetown University Medical Center and received the Dudley P. Jackson Award as the Outstanding Resident for Excellence in Teaching. He did his fellowship in Pulmonary and Critical Care Medicine at UCSD, during which time he was awarded the American Lung Association of California Research Fellowship Grant and the ACCP Young Investigator Award. As a faculty member, he has received eleven annual Outstanding Teaching Awards from the UCSD Department of Medicine. He is the lead editor of the educational textbook, the Manual of Clinical Problems in Pulmonary Medicine. He served as President of the California Thoracic Society and as a member of numerous steering committees of the ACCP networks. The California Thoracic Society gave him their annual “Outstanding Clinician Award” in 2008. Dr. Morris’ NIH-funded research is in the area of pulmonary embolism. He is an author of the upcoming ACCP Consensus Guidelines on therapy for pulmonary embolism. He was a two-time recipient of the Distinguished Scholar in Thrombosis Award, American College of Chest Physicians for 2003-2007. He received the First Place Award for Best Research Abstract presented at CHEST by the American College of Chest Physicians in 2006. In 2009, he was awarded the “Certificate of Achievement from as the Clinical Expert in Pulmonary Embolism” by The American Thoracic Society and The CHEST Foundation: Award in Venous Thromboembolism by The American College of Chest Physicians. Fairly certain that nobody would be reading this text very carefully, he italicized the phrases “Best Person Ever” and “Worlds Most Interesting Man 2010-2015” to make the paragraph look fuller. Dr. Morris has two children, both of whom are in college. He marvels at this fact, since he remembers driving them to grammar school about a month ago. He constantly embarrasses them.
1

OBJECTIVES:
Participants should be better able to:
1. Describe newly identified populations at high risk for developing acute pulmonary embolism;
2. Understand the advantages of SPECT VQ scanning;
3. Evaluate findings that suggest a high risk of mortality in patients diagnosed with acute pulmonary embolism;
4. Understand the long term effect of pulmonary embolism on symptoms, physiology and quality of life
FRIDAY, MARCH 13, 2015 10:30 AM
2

Phenotypes of Thrombotic Pulmonary Embolism
Timothy A. Morris, MD FACCP Professor of Medicine Clinical Service Chief
Division of Pulmonary and Critical Care Medicine University of California, San Diego
Disclosure Information Timothy Morris, MD
• The content of this presentation does not relate to any product of a commercial interest; therefore, there are no relevant financial relationship to disclose.
• I will discuss the no off label use and/or investigational use in my presentation
3

Phenotypes
• Risk populations • Hard to image populations • Less acutely vulnerable populations • More acutely vulnerable populations • Chronically vulnerable populations
Phenotypes
• Risk populations – High risk – General population
• Hard to image populations • Less acutely vulnerable populations • More acutely vulnerable populations • Chronically vulnerable populations
4

The incidence of VTE is…
A. Higher in cirrhosis than heart transplant B. Higher after heart transplant than cirrhosis C. Equally high in cirrhosis and heart transplant D. Low in both E. I’d like to buy a vowel
The incidence of VTE is…
A. Higher in cirrhosis than heart trans
B. Higher after heart transplant than cirrhosis
C. Equally high in cirrhosis and heart transplant
D. Low in both E. I’d like to buy a vowel
A. B. C. D. E.
0% 0% 0%0%0%
5

VTE one year after heart transplantation
1. Rolando J. Alvarez-Alvarez , Eduardo Barge-Caballero , Sergio A. Chavez-Leal , María J. Paniagua-Martin , Raquel Ma. Venous thromboembolism in heart transplant recipients: Incidence, recurrence and predisposing factors. The Journal of Heart and Lung Transplantation, 2014
6

VTE overall after heart transplantation
1. Rolando J. Alvarez-Alvarez , Eduardo Barge-Caballero , Sergio A. Chavez-Leal , María J. Paniagua-Martin , Raquel Ma. Venous thromboembolism in heart transplant recipients: Incidence, recurrence and predisposing factors. The Journal of Heart and Lung Transplantation, 2014
7

Incidence of VTE in Liver Disease
venous thromboembolism 1% (0.7% - 1.3%)
Pulmonary embolism 0.28% (0.13% - 0.49%)
Statins for VTE prevention: maybe for males?
Lassila R, et al. The association of statin use with reduced incidence of venous thromboembolism: a population-based cohort study. BMJ Open 2014;4:e005862. doi:10.1136/bmjopen-2014-005862
8

Phenotypes
• Risk populations • Hard to image populations
– Pregnancy – Co-existing lung disease – Contrast sensitivity
• Less acutely vulnerable populations • More acutely vulnerable populations • Chronically vulnerable populations
Quiz question
In a __ year old ___ with ___ suspected of PE, the correct test is:
A.Contrast enhanced CT B.Contrast enhanced CT C.Contrast enhanced CT D.Contrast enhanced CT E.Answers A, B, C and D are all correct
9

Pregnancy-Related Death
Chang J, Elam-Evans LD, Berg CJ, Herndon J, Flowers L, Seed KA, Syverson CJ. Pregnancy-related mortality surveillance--United States, 1991--1999. MMWR
Surveill Summ. 2003;52(2):1-8.
VTE Risk in Pregnancy and Post-partum
1. Pomp ER, Lenselink AM, Rosendaal FR, et al. Pregnancy, the postpartum period and prothrombotic defects: risk of venous thrombosis in the
MEGA study. J Thromb Haemost 2008; 6: 632–7
10

Trend in CT vs VQ for Pregnant Patients
1. Revel M-P, Cohen S, Sanchez O, et al. Pulmonary embolism during pregnancy: diagnosis with lung scintigraphy or CT angiography. Radiology 2011;258:590-598
In pregnant patients suspected of having PE, indeterminate findings are…
A. More common in CT scans than in VQ scans B. More common in VQ scans than in CT scans C. About equally common in both scans D. Refuse to answer
11

In pregnant patients suspected of having PE, indeterminate findings
are… A. More common in CT scans
than in VQ scans B. More common in VQ scans
than in CT scans C. About equally common in both
scans D. Refuse to answer
A. B. C. D.
9%3%
15%
74%
CT vs VQ in Pregnancy: Utility
1. Revel M-P, Cohen S, Sanchez O, et al. Pulmonary embolism during pregnancy: diagnosis with lung scintigraphy or CT angiography. Radiology 2011;258:590-598
12

Example of Indeterminate CT in Pregnant Woman
• No contrast in PA • Smaller SVC (exhalation?)
Good
• Contrast in PA • Larger SVC (inhalation?)
Bad
1. Revel M-P, Cohen S, Sanchez O, et al. Pulmonary embolism during pregnancy: diagnosis with lung scintigraphy or CT angiography. Radiology 2011;258:590-598
CT vs VQ in Pregnant Women: Radiation
1. Revel M-P, Cohen S, Sanchez O, et al. Pulmonary embolism during pregnancy: diagnosis with lung scintigraphy or CT angiography. Radiology 2011;258:590-598
13

PEDS Title page
PEDS Trial: PE after a negative CTPA
or VQ/CUS
14

In my institution, we use SPECT VQ to diagnose PE in…
A. Almost nobody (< 1% of cases) B. A small number of cases (1% - 10%) C. A substantial minority (10% - 40%) D. As much as CT scanning (>40%)
In my institution, we use SPECT VQ to diagnose PE in…
A. Almost nobody (< 1% of cases)
B. A small number of cases (1% - 10%)
C. A substantial minority (10% - 40%)
D. As much as CT scanning (>40%)
A. B. C. D.
74%
0%6%
21%
15

Planar Perfusion Scan
Det
ecto
r
SPECT Data
16

SPECT Scanning
http://tomo3d-ea.gforge.inria.fr/tomo3d-ea.html
SPECT “Voxel” Dataset
http://tomo3d-ea.gforge.inria.fr/tomo3d-ea.html
17

SPECT V/Q
SPECT V/Q scan
planar V/Q scan
Contrast CT scan
Reinartz P, Wildberger JE, Schaefer W, Nowak B, Mahnken AH, Buell U. Tomographic imaging in the diagnosis of pulmonary embolism: a comparison between V/Q lung scintigraphy in SPECT technique and multislice spiral CT. J Nucl Med. 2004;45(9):1501-8.
VQ SPECT Accuracy
Jann Mortensen & Henrik Gutte. SPECT/CT and pulmonary embolism Eur J Nucl Med Mol Imaging (2014) 41 (Suppl 1):S81–S90
18

VQ SPECT Sensitivity
Kan. The accuracy of V/Q SPECT in the diagnosis of pulmonary embolism: a meta-analysis. Acta Radiologica. 2014 Abstract
VQ SPECT Specificity
Kan. The accuracy of V/Q SPECT in the diagnosis of pulmonary embolism: a meta-analysis. Acta Radiologica. 2014 Abstract
19

VQ SPECT Negative Likelihood Ratio
Kan. The accuracy of V/Q SPECT in the diagnosis of pulmonary embolism: a meta-analysis. Acta Radiologica. 2014 Abstract
VQ SPECT Positive Likelihood Ratio
Kan. The accuracy of V/Q SPECT in the diagnosis of pulmonary embolism: a meta-analysis. Acta Radiologica. 2014 Abstract
20

Phenotypes
• Risk populations • Hard to image populations • Less acutely vulnerable populations
– Outpatient therapy – No therapy
• More acutely vulnerable populations • Chronically vulnerable populations
Pulmonary Embolism Severity Index
Add age+points Severity classes I. ≤65 II. 66–85 III.86–10 IV.106–125 V. > 125
1. Donze J, Le Gal G, Fine MJ, Roy PM, Sanchez O, Verschuren F, Cornuz J, Meyer G, Perrier A, Righini M, Aujesky D. Prospective validation of the Pulmonary Embolism Severity Index. A clinical prognostic model for pulmonary embolism. Thromb Haemost. 2008;100(5):943-948
21

PESI Scores and Mortality
PESI Class Mortality
I 0 - 1.6%
II 2.0% - 3.5%
III 6.5% - 7.7%
IV 10.4% - 12.2%
V 17.9% - 24.5%
1. Donze J, Le Gal G, Fine MJ, Roy PM, Sanchez O, Verschuren F, Cornuz J, Meyer G, Perrier A, Righini M, Aujesky D. Prospective validation of the Pulmonary Embolism Severity Index. A clinical prognostic model for pulmonary embolism. Thromb Haemost. 2008;100(5):943-948
No treatment for very low risk patients?
22

I withhold anticoagulation in incidentally discovered subsegmental PE patients…
A. Never, on the basis of strong RCT evidence B. Never, because of my overall judgment C. Sometimes, on the basis of strong RCT evidence D. Sometimes, because of my overall judgment
I withhold anticoagulation in incidentally discovered subsegmental
PE patients… A. Never, on the basis of strong
RCT evidence B. Never, because of my overall
judgment C. Sometimes, on the basis of
strong RCT evidence D. Sometimes, because of my
overall judgment A. B. C. D.
16%
48%
20%16%
23

Do subsegmental PEs need to be treated?
• No high quality randomized controlled trials of anticoagulation therapy versus no intervention in patients with SSPE or incidental SSPE.
• Well-conducted research is required before informed practice decisions can be made.
Yoo HHB, Queluz THAT, El Dib R. Anticoagulant treatment for subsegmental pulmonary embolism. Cochrane Database of Systematic
Reviews 2014, Issue 4. Art. No.: CD010222. DOI: 10.1002/14651858.CD010222.pub2.
24

Phenotypes
• Risk populations • Hard to image populations • Less acutely vulnerable populations • More acutely vulnerable populations
– How to stratify – What to focus on – What helps and what doesn’t
• Chronically vulnerable populations
PESI Scores and Mortality
PESI Class Mortality
I 0 - 1.6%
II 2.0% - 3.5%
III 6.5% - 7.7%
IV 10.4% - 12.2%
V 17.9% - 24.5%
1. Donze J, Le Gal G, Fine MJ, Roy PM, Sanchez O, Verschuren F, Cornuz J, Meyer G, Perrier A, Righini M, Aujesky D. Prospective validation of the Pulmonary Embolism Severity Index. A clinical prognostic model for pulmonary embolism. Thromb Haemost. 2008;100(5):943-948
25

Other prognostic factors
• Co-existing DVT1
– Positive US: hazard ratio of 2.0 • Right ventricular strain2
– Echocardiography or CT: RR 2.4 (95% CI 1.3-4.4) – BNP: RR of 9.5 (95% CI 3.2-28.6) – Pro-BNP RR 5.7 (95% CI 2.2-15.1) – Troponin: RR 8.3 (95% CI 3.6-19.3)
1. Jimenez D, Aujesky D, Diaz G, Monreal M, Otero R, Marti D, Marin E, Aracil E, Sueiro A, Yusen RD. Prognostic significance of deep vein thrombosis in patients presenting with acute symptomatic pulmonary embolism. Am J Respir Crit Care Med.
2010;181(9):983-991. 2. Sanchez O, Trinquart L, Colombet I, Durieux P, Huisman MV, Chatellier G, Meyer G. Prognostic value of right ventricular
dysfunction in patients with haemodynamically stable pulmonary embolism: a systematic review. Eur Heart J. 2008;29(12):1569-1577.
The best indicator of mortality in PE patients on CT scanning is…
A. The clot burden (total amount) B. Right ventricle dimensions C. Pulmonary artery dimensions D. Forward movement of CT contrast dye E. Presence of a “saddle embolus”
26

The best indicator of mortality in PE patients on CT scanning is…
A. The clot burden (total amount)
B. Right ventricle dimensions C. Pulmonary artery
dimensions D. Forward movement of CT
contrast dye E. Presence of a “saddle
embolus”
A. B. C. D. E.
14%
57%
23%
3%3%
27

“Moderate” correlation between CT
clot burden and RV function on echo
1. Rodrigues. Relationship of clot burden and echocardiographic severity of right ventricular dysfunction after acute pulmonary embolism. Int J Cardiovasc Imaging, 2014
28

CT clot burden doesn’t predict 30d mortality
A.G. Bach et al. / European Journal of Radiology xxx (2014) xxx–xxx
CT RV findings don’t predict 30d mortality
1. A.G. Bach et al. / European Journal of Radiology xxx (2014) xxx–xxx
2 mm (6.6%)
difference
29

CT pulmonary trunk and 30d mortality
• Survivors – Median 28.7 mm – Interquartile 26.3 mm – 32.2 mm
• Non-survivors – Median 30.6 mm – Interquartile 27.8 mm – 32.4 mm
1. A.G. Bach et al. / European Journal of Radiology xxx (2014) xxx–xxx
30

Saddle PE more unstable, but similar mortality
1. Pathak. Comparison between Saddle versus Non-Saddle Pulmonary Embolism: Insights from Nationwide Inpatient Sample. International Journal of Cardiology 180 (2015) 58–59
CT contrast reflux might predict 30d mortality
• Contrast from arm vein refluxes into IVC
1. A.G. Bach et al. / European Journal of Radiology xxx (2014) xxx–xxx
31

CT contrast reflux might predict 30d mortality
1. A.G. Bach et al. / European Journal of Radiology xxx (2014) xxx–xxx
32

Prognosis of PE with T-wave inversions
P. Kukla et al. / Heart & Lung 44 (2015) 68e71
33

Heart-type fatty acid-binding protein
and 30-d mortality for acute PE
1. Ruan. Prognostic Value of Plasma Heart-Type Fatty Acid-Binding Protein in Patients With Acute Pulmonary
EmbolismHeart-Type Fatty Acid-Binding Protein: A Meta-analysis. Chest. 2014;146(6):1462-1467. doi:10.1378/chest.13-
1008
Thrombolytics
34

I use thrombolytics for hemodynamically stable PE patients with RV strain…
A. Almost always B. More often than not C. About half the time D. Unusually E. Almost never
I use thrombolytics for hemodynamically stable PE patients
with RV strain… A. Almost always B. More often than not C. About half the time D. Unusually E. Almost never
A. B. C. D. E.
11%
5%
58%
21%
5%
35

Hemodynamically stable pts
Wan S, Quinlan DJ, Agnelli G, Eikelboom JW. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism: a meta-analysis of the randomized controlled trials. Circulation. 2004;110(6):744-9.
Hemodynamically stable pts
Wan S, Quinlan DJ, Agnelli G, Eikelboom JW. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism: a meta-analysis of the randomized controlled trials. Circulation. 2004;110(6):744-9.
36

Meta-analysis: lytics vs heparin
Wan S, Quinlan DJ, Agnelli G, Eikelboom JW. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism: a meta-analysis of the randomized controlled trials. Circulation. 2004;110(6):744-9.
Intracranial Bleed During VTE Rx
Dalen JE, Alpert JS, Hirsh J. Thrombolytic Therapy for Pulmonary Embolism: Is It Effective? Is It Safe? When Is It Indicated? Arch Intern Med. 1997;157:2550-6.
37

Clinical Decisions
Mortality
1.61%
Increase due to
more bleeding
Decrease due
to faster lysis
??% Risk
from
PE
Resolution Rates After PE
Urokinase pulmonary embolism trial. Phase 1 results: a cooperative study. Jama. 1970;214(12):2163-72.
Will this save the patient?
38

Chatterjee, Thrombolysis for Pulmonary Embolism and Risk of All-Cause Mortality, Major Bleeding, and Intracranial Hemorrhage A Meta-analysis. JAMA. 2014;311(23):2414-2421. doi:10.1001/jama.2014.5990
Problem: Major effect was the result of 6 small trials
39

Chatterjee, Thrombolysis for Pulmonary Embolism and Risk of All-Cause Mortality, Major Bleeding, and Intracranial Hemorrhage A Meta-analysis. JAMA. 2014;311(23):2414-2421. doi:10.1001/jama.2014.5990
Chatterjee, Thrombolysis for Pulmonary Embolism and Risk of All-Cause Mortality, Major Bleeding, and Intracranial Hemorrhage A Meta-analysis. JAMA. 2014;311(23):2414-2421. doi:10.1001/jama.2014.5990
40

Antoni Riera-Mestre , Cecilia Becattini , Michela Giustozzi , Giancarlo Agnelli. Thrombolysis in hemodynamically stable patients with acute pulmonary embolism: A meta-analysis. Thrombosis Research, Volume 134, Issue 6, 2014, 1265 - 1271
Major bleeding
Favors thrombolysis & heparin
Favors heparin alone
41

Antoni Riera-Mestre , Cecilia Becattini , Michela Giustozzi , Giancarlo Agnelli. Thrombolysis in hemodynamically stable patients with acute pulmonary embolism: A meta-analysis. Thrombosis Research, Volume 134, Issue 6, 2014, 1265 - 1271
Intracranial bleeding
Favors thrombolysis & heparin
Favors heparin alone
Antoni Riera-Mestre , Cecilia Becattini , Michela Giustozzi , Giancarlo Agnelli. Thrombolysis in hemodynamically stable patients with acute pulmonary embolism: A meta-analysis. Thrombosis Research, Volume 134, Issue 6, 2014, 1265 - 1271
All-cause mortality
Favors thrombolysis & heparin
Favors heparin alone
42

IVC filters
IVC filter picture
43

IVC Filters to Prevent PE*
p=0.03
*Decouses NEJM 1998
IVC Filters and mortality
Stein PD, Matta F, Keyes DC, Willyerd GL. Impact of vena cava filters on in-hospital case fatality rate from pulmonary embolism. Am J Med. 2012;125:478-484.
44

Fewer deaths in PE patients with IVC filters
Isogai. Effectiveness of Inferior Vena Cava Filters on Mortality as an Adjuvant to Antithrombotic Therapy. The American Journal of Medicine 2014
Right hydronephrosis
Bos. Et al. Strut Penetration: Local Complications, Breakthrough Pulmonary Embolism, and Retrieval Failure in Patients with Celect Vena Cava Filters. J Vasc Interv Radiol 2014
IVC filter complications?
IVF filer strut compression of the proximal right ureter
45

Low rate of long-term IVC filter problems
Bos. Et al. Strut Penetration: Local Complications, Breakthrough Pulmonary Embolism, and Retrieval Failure in Patients with Celect Vena Cava Filters. J Vasc Interv Radiol 2014
Phenotypes
• Risk populations • Hard to image populations • Less acutely vulnerable populations • More acutely vulnerable populations • Chronically vulnerable populations
46

Question
To prevent recurrence, PE should be treated for a)6 weeks b)3 months c)6 months d)Forever e)Depends on the clinical risks prior to the PE f) Depends on the clinical course after PE Dx
To prevent recurrence, PE should be treated for
a. 6 weeks b. 3 months c. 6 months d. Forever e. Depends on the clinical
risks prior to the PE f. Depends on the clinical
course after PE Dx
a. b. c. d. e. f.
0% 0%
12%
80%
0%
7%
47

Risk of Recurrence All provoked VTE
Iorio A, Kearon C, Filippucci E, Marcucci M, Macura A, Pengo V, Siragusa S, Palareti G. Risk of recurrence after a first episode of symptomatic venous thromboembolism provoked by a transient risk factor: A systematic review. Arch Intern Med 2010;170:1710-1716.
Provocation
Surgery (within 3 mo) • Type
– Orthopedic – General – Urologic – Gynecologic – Abdominal
• General anesthesia
Other (within 1wk – 3 mo) • Immobilization
– trauma, traveling, bedridden
• Pregnancy, childbirth • Estrogen
– (contraception or HRT)
• Trauma, fracture, plaster cast, • Nonspecific transient illness
Iorio A, Kearon C, Filippucci E, Marcucci M, Macura A, Pengo V, Siragusa S, Palareti G. Risk of recurrence after a first episode of symptomatic venous thromboembolism provoked by a transient risk factor: A systematic review. Arch Intern Med 2010;170:1710-1716.
48

Risk of Recurrence
Iorio A, Kearon C, Filippucci E, Marcucci M, Macura A, Pengo V, Siragusa S, Palareti G. Risk of recurrence after a first episode of symptomatic venous thromboembolism provoked by a transient risk factor: A systematic review. Arch Intern Med 2010;170:1710-1716.
Risk of Recurrence
Iorio A, Kearon C, Filippucci E, Marcucci M, Macura A, Pengo V, Siragusa S, Palareti G. Risk of recurrence after a first episode of symptomatic venous thromboembolism provoked by a transient risk factor: A systematic review. Arch Intern Med 2010;170:1710-1716.
49

Post-Rx D-dimer negative
Kearon C, et al. D-Dimer Testing to Select Patients With a First Unprovoked Venous Thromboembolism Who Can Stop Anticoagulant Therapy: A Cohort Study. Ann Intern Med. 2015;162:27-34.
PE secondary to a transient (reversible) risk factor
• Treatment for at least 3 months • Usually not long-term
– Use your judgment about non-surgical provocation
Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, Nelson ME, Wells PS, Gould MK, Dentali F, Crowther M, Kahn SR, American College of Chest P. Antithrombotic therapy for vte disease: Antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest 2012;141:e419S-494S.
50

Question
The duration of treatment after unprovoked PE… a)Depends entirely on the patient’s values b)Depends entirely on D-dimer levels after Rx c)Depends entirely on the degree of resolution d)The optimal duration is unknown
The duration of treatment after unprovoked PE…
a. Depends entirely on the patient’s values
b. Depends entirely on D-dimer levels after Rx
c. Depends entirely on the degree of resolution
d. The optimal duration is unknown
a. b. c. d.
0% 0%0%0%
51

Unprovoked VTE: Long-term risk
Prospective Cohort Study
(provoked vs non-provoked) Prandoni P, Noventa F, Ghirarduzzi A, Pengo V, Bernardi E, Pesavento R, Iotti M, Tormene D, Simioni P, Pagnan A. The risk of recurrent venous thromboembolism after discontinuing anticoagulation in patients with acute proximal deep vein thrombosis or pulmonary embolism. A prospective cohort study in 1,626 patients. Haematologica 2007;92:199-205.
Follow-up to Duration of Anticoagulation Trial
(provoked and non-provoked) Schulman S, Lindmarker P, Holmstrom M, Larfars G, Carlsson A, Nicol P, Svensson E, Ljungberg B, Viering S, Nordlander S, Leijd B, Jahed K, Hjorth M, Linder O, Beckman M. Post-thrombotic syndrome, recurrence, and death 10 years after the first episode of venous thromboembolism treated with warfarin for 6 weeks or 6 months. J Thromb Haemost 2006;4:734-742.
Long-term Rx after Unprovoked VTE
Ridker PM, et al. New England Journal of Medicine 2003;348:1425-1434. Kearon C, et al. New England Journal of Medicine 1999;340:901-907. Palareti G, et al. New England Journal of Medicine 2006;355:1780-1789.
52

Bleeding during long term Rx for unprovoked VTE*
* Underpowered Ridker PM, et al. New England Journal of Medicine 2003;348:1425-1434. Kearon C, et al. New England Journal of Medicine 1999;340:901-907. Palareti G, et al. New England Journal of Medicine 2006;355:1780-1789.
After an acute PE, if CTEPH does not develop, persistent perfusion defects…
A. are rare B. are not rare but are clinically insignificant C. cause symptoms and reduce quality of life D. Are a major cause of death
53

After an acute PE, if CTEPH does not develop, persistent perfusion defects…
A. are rare B. are not rare but are
clinically insignificant C. cause symptoms and
reduce quality of life D. Are a major cause of
death A. B. C. D.
21%
3%
15%
61%
Acute PE
Full recovery
CTEPH
Acute PE
Full recovery
CTEPH
Partial recovery
54

CTEPH-Related Clinical Factors
• Idiopathic etiology of the PE1
• Right heart strain during acute PE1, 2
– (e.g. PA pressures <50 mmHg)
• Age1
• Previous splenectomy3, 4
• Ventriculo-atrial shunts3-5
– (treatment of hydrocephalus)
• Chronic inflammatory disorders 3-5
– (e.g osteomyelitis, inflammatory bowel disease)
1.Pengo V, Lensing AW, Prins MH, Marchiori A, Davidson BL, Tiozzo F, Albanese P, Biasiolo A, Pegoraro C, Iliceto S, Prandoni P. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350(22):2257-2264.
2.Ribeiro A, Lindmarker P, Johnsson H, Juhlin-Dannfelt A, Jorfeldt L. Pulmonary embolism: one-year follow-up with echocardiography doppler and five-year survival analysis. Circulation. 1999;99(10):1325-1330.
3.Bonderman D, Jakowitsch J, Adlbrecht C, Schemper M, Kyrle PA, Schonauer V, Exner M, Klepetko W, Kneussl MP, Maurer G, Lang I. Medical conditions increasing the risk of chronic thromboembolic pulmonary hypertension. Thromb Haemost. 2005;93(3):512-516.
4.Bonderman D, Turecek PL, Jakowitsch J, Weltermann A, Adlbrecht C, Schneider B, Kneussl M, Rubin LJ, Kyrle PA, Klepetko W, Maurer G, Lang IM. High prevalence of elevated clotting factor VIII in chronic thromboembolic pulmonary hypertension. Thromb Haemost. 2003;90(3):372-376.
5.Lang I, Kerr K. Risk factors for chronic thromboembolic pulmonary hypertension. Proc Am Thorac Soc. 2006;3(7):568-570.
CTEPH-Related Clinical Factors
• Idiopathic etiology of the PE1
• Right heart strain during acute PE1, 2
– (e.g. PA pressures <50 mmHg)
• Age1
• Previous splenectomy3, 4
• Ventriculo-atrial shunts3-5
– (treatment of hydrocephalus)
• Chronic inflammatory disorders 3-5
– (e.g osteomyelitis, inflammatory bowel disease)
1.Pengo V, Lensing AW, Prins MH, Marchiori A, Davidson BL, Tiozzo F, Albanese P, Biasiolo A, Pegoraro C, Iliceto S, Prandoni P. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350(22):2257-2264.
2.Ribeiro A, Lindmarker P, Johnsson H, Juhlin-Dannfelt A, Jorfeldt L. Pulmonary embolism: one-year follow-up with echocardiography doppler and five-year survival analysis. Circulation. 1999;99(10):1325-1330.
3.Bonderman D, Jakowitsch J, Adlbrecht C, Schemper M, Kyrle PA, Schonauer V, Exner M, Klepetko W, Kneussl MP, Maurer G, Lang I. Medical conditions increasing the risk of chronic thromboembolic pulmonary hypertension. Thromb Haemost. 2005;93(3):512-516.
4.Bonderman D, Turecek PL, Jakowitsch J, Weltermann A, Adlbrecht C, Schneider B, Kneussl M, Rubin LJ, Kyrle PA, Klepetko W, Maurer G, Lang IM. High prevalence of elevated clotting factor VIII in chronic thromboembolic pulmonary hypertension. Thromb Haemost. 2003;90(3):372-376.
5.Lang I, Kerr K. Risk factors for chronic thromboembolic pulmonary hypertension. Proc Am Thorac Soc. 2006;3(7):568-570.
55

• Lupus anticoagulant6 • Elevated Factor VIII4
• Non-O blood groups7
• Lipoprotein (a)8
• Heart-type fatty acid-binding protein9
CTEPH-Related Laboratory Factors
4.Bonderman D, Turecek PL, Jakowitsch J, Weltermann A, Adlbrecht C, Schneider B, Kneussl M, Rubin LJ, Kyrle PA, Klepetko W, Maurer G, Lang IM. High prevalence of elevated clotting factor VIII in chronic thromboembolic pulmonary hypertension. Thromb Haemost. 2003;90(3):372-376.
6.Auger WR, Permpikul P, Moser KM. Lupus anticoagulant, heparin use, and thrombocytopenia in patients with chronic thromboembolic pulmonary hypertension: a preliminary report. Am J Med. 1995;99(4):392-396.
7.Bonderman D, Wilkens H, Wakounig S, Schafers HJ, Jansa P, Lindner J, Simkova I, Martischnig AM, Dudczak J, Sadushi R, Skoro-Sajer N, Klepetko W, Lang IM. Risk factors for chronic thromboembolic pulmonary hypertension. Eur Respir J. 2008.
8.Ignatescu M, Kostner K, Zorn G, Kneussl M, Maurer G, Lang IM, Huber K. Plasma Lp(a) levels are increased in patients with chronic thromboembolic pulmonary hypertension. Thromb Haemost. 1998;80(2):231-232.
9.Lankeit M, Dellas C, Panzenbock A, Skoro-Sajer N, Bonderman D, Olschewski M, Schafer K, Puls M, Konstantinides S, Lang IM. Heart-type fatty acid-binding protein for risk assessment of chronic thromboembolic pulmonary hypertension. Eur Respir J. 2008;31(5):1024-1029.
• Lupus anticoagulant6 • Elevated Factor VIII4
• Non-O blood groups7
• Lipoprotein (a)8
• Heart-type fatty acid-binding protein9
CTEPH-Related Laboratory Factors
4.Bonderman D, Turecek PL, Jakowitsch J, Weltermann A, Adlbrecht C, Schneider B, Kneussl M, Rubin LJ, Kyrle PA, Klepetko W, Maurer G, Lang IM. High prevalence of elevated clotting factor VIII in chronic thromboembolic pulmonary hypertension. Thromb Haemost. 2003;90(3):372-376.
6.Auger WR, Permpikul P, Moser KM. Lupus anticoagulant, heparin use, and thrombocytopenia in patients with chronic thromboembolic pulmonary hypertension: a preliminary report. Am J Med. 1995;99(4):392-396.
7.Bonderman D, Wilkens H, Wakounig S, Schafers HJ, Jansa P, Lindner J, Simkova I, Martischnig AM, Dudczak J, Sadushi R, Skoro-Sajer N, Klepetko W, Lang IM. Risk factors for chronic thromboembolic pulmonary hypertension. Eur Respir J. 2008.
8.Ignatescu M, Kostner K, Zorn G, Kneussl M, Maurer G, Lang IM, Huber K. Plasma Lp(a) levels are increased in patients with chronic thromboembolic pulmonary hypertension. Thromb Haemost. 1998;80(2):231-232.
9.Lankeit M, Dellas C, Panzenbock A, Skoro-Sajer N, Bonderman D, Olschewski M, Schafer K, Puls M, Konstantinides S, Lang IM. Heart-type fatty acid-binding protein for risk assessment of chronic thromboembolic pulmonary hypertension. Eur Respir J. 2008;31(5):1024-1029.
56

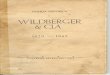
Improvement Relative to Initial Perfusion Defect
M ur phy 1968
Secker Wal ker 1970
Pal l a 1986
Pr edi l et to 1990
Donnamar i a 1993M enendez 1998
War tski 2000
0
10
20
30
40
50
60
70
80
90
0 100 200 300 400Time after PE (Days)
Rel
ativ
e Im
prov
emen
t in
Perfu
sion
.
Echocardiogram
Ribeiro et al. Circulation 1999; 99:1325-1330
57

Excellent review!
Clinical Consequences of Residual Defects
Sanchez O, Helley D, Couchon S, Roux A, Delaval A, Trinquart L, Collignon MA, Fischer AM, Meyer G. Perfusion defects after pulmonary embolism: risk factors and clinical significance. J Thromb Haemost. 2010;8(6):1248-55.
• More dyspnea • Lower 6 min walk distance • Higher PAP • More CTEPH
58

Quality of Life after Acute PE
1. Josien van Es , Paul L. den Exter , Ad A. Kaptein , Cornelie D. Andela , Petra M.G. Erkens , Frederikus A. Klok . Quality of life after pulmonary embolism as assessed with SF-36 and PEmb-QoL. Quality of life after pulmonary embolism as assessed with SF-36 and PEmb-QoL
59

Effect of lysis on QoL was not statistically significant
1. Stewart. Contribution of fibrinolysis to the physical component summary of the SF-36 after acute submassive pulmonary embolism. J Thromb Thrombolysis 2014
Phenotypes • Risk populations
– Add heart transplant to list • Hard to image populations
– Consider VQ SPECT • Less acutely vulnerable populations
– Withhold therapy?? • More acutely vulnerable populations
– Thrombolytics only in the sickest – IVC filters?
• Chronically vulnerable populations – Consider persistent perfusion defects after PE
60