Embed Size (px)
Citation preview

TI-RADS classification of thyroid nodules based on a score modified according to ultrasound criteria for malignancyOriginal
Rev. Argent. Radiol. 2014;78(3): 138-148138
AbstractObjective: The classification system of the thyroid nodules (TN) TI-RADS (Thyroid Imaging Reporting and Data System) proposed by Horvath et al. in 2009 is rarely used. The aim of this study was to evaluate a score modified according to ultrasound (US) criteria for malignancy in order to obtain a better application of this classification in daily practice.Materials and methods: 3650 TNs were classified according to a score of potential malignancy. US criteria for suspected malignancy were defined according to published studies and guidelines from various medical international societies. Each criterion was assigned a point for the final score of malignant probability of the TN. If suspected cervical lymph nodes were detected, a point was added.Results: The score in all benign (TI-RADS 2) or probably benign (TI-RADS 3) thyroid nodules was zero. In the TI-RADS 3 group only 2.2% of the TNs were malignant. The scores of TI-RADS 4a, 4b and 4c were one, two and three to four points, respectively. The malignancy rates were 9.5%, 48% and 85%, respectively. TI-RADS 5 TN had a score of five or more points with a malignancy of 100% in this study.Conclusion: A TI-RADS classification based on a score according to the number of suspicious US criteria defined for malignancy can be applied in daily practice.© 2014 Sociedad Argentina de Radiología. Published by Elsevier Spain, S.L.U. All rights reserved.
KeywordsThyroid nodule; TI-RADS; Ultrasound; Thyroid scintigraphy
Introduction
Thyroid nodules (TNs) may show highly diverse ultrasound patterns1,2, which often impairs an accurate classification regarding malignancy. For this reason, in 2009 Horvath et al3 proposed an evaluation system for TNs called TI-RADS (Thyroid Imaging Reporting and Data System), similar to the Breast Imaging Reporting and Data System (BI-RADS)4,5. In 2011, Kwak et al6, complemented this classification adding one subtype.However, both systems are difficult to apply. Even if the TI-RADS classification is quoted in the medical literature, it is rarely used in daily practice, perhaps because of some un-certainty on the part of the various specialists that use such classification.The aim of this study was to evaluate an easy-to-use TI-RADS classification based on a modified score according to the US criteria for malignancy present in each case.
Materials and methods
We reviewed the 7960 thyroid ultrasound scans performed between 2003 and 2013 and stored on the Picture Archiving and Communication System/Radiology Information System (PACS/RIS). The scans had been performed, or reviewed prior to reporting (if performed by a resident physician), by special-ists with 5 to 30 years’ experience in thyroid ultrasound. The US examination of a detected TN consisted in an evaluation of its echogenicity, internal content (presence of cystic lesions and/or calcifications), margins, shape and vascular pattern. Based on studies and guidelines from various national and international medical societies of different specialties7-16, ul-trasound criteria for suspected malignancy were established (table 1). Each criterion was assigned a point, and an ad-ditional point was added when one or more cervical lymph nodes suspicious for malignancy were detected. Thus, a final score of malignant probability of a TN was obtained.
TI-RADS classification of thyroid nodules based on a score modified according to ultrasound criteria for malignancyJ. Fernández Sánchez *
Radiology and Nuclear Medicine, Robert-Bosch-Krankenhaus, University Hospital, Tübingen University, Stuttgart, Germany

TI-RADS classification of thyroid nodules based on a score modified according to ultrasound criteria for malignancy
Rev. Argent. Radiol. 2014;78(3): 138-148
J. Fernández Sánchez
139
For TI-RADS assessment, we selected from the PACS imag-ing archiving system appropriately documented TNs (sagittal and axial ultrasound images of TNs, obtained by convention-al --B mode-- imaging and by color Doppler for the evalua-tion of perfusion) of which fine needle aspiration (FNA) had been performed and/or which had been scanned by thyroid scintigraphy and/or elastosonography and/or other imaging method (magnetic resonance imaging [MRI], positron emis-sion tomography – computed tomography [PET/CT]) and/or which had undergone histological assessment after surgery and/or which had at least a one-year clinical follow-up with ultrasound scans.As this was primarily a retrospective study, no approval was requested from the Ethics Committee.The statistical analysis was based on the calculation of predic-tive values of the TI-RADS classification categories.
Results
Of the 7960 thyroid ultrasound scans evaluated, one or sev-eral TNs were detected in 6127 and no focal lesions were de-tected in 1833. Of the latter (n = 1833), 1454 cases showed diffuse abnormality of the thyroid parenchyma, either due to Hashimoto’s thyroiditis or to thyroid autoimmune disease (Grave-Basedow disease), while the remaining 379 patients with no focal lesion had a normal sized gland, with an ultra-sound pattern that was hyperechogenic (in regard to muscle) and homogeneous, and with normal vascularity on color Doppler. These normal ultrasound scans of the thyroid, with an incidence of 4.7% in our series (379/7960 cases) were classified as TI-RADS 1, similar to BI-RADS classification of the breast (BI-RADS 1 = normal breast)4,5
Of the 6127 patients with one or several TNs, 1148 met the
study requirements. Of all TNs, 3650 were appropriately doc-umented and had been evaluated by the reference diagnostic methods. Therefore, they were used for the evaluation of TI-RADS classification in this study.Of these 3650 TNs, 1302 (35.6%) showed benign sono-graphic features: 73/1302 simple cysts2,17, 104/1302 TNs with a central cyst (type 1, according to Kim et al classification for partially cystic TNs)16, 56/1302 TNs with non-interrupted homogeneous peripheral calcification18 and 1069/1302 spongiform TNs2, 19,20. Based on their ultrasound pattern and the absence of ultrasound criteria for malignancy, these TNs had a score of zero. Furthermore, additional tests (FNA [n = 88] and/or histological examination after surgery [n = 132] and/or thyroid scintigraphy [n = 585] and/or elastosonogra-phy [n = 95] and/or MRI/PET/CT [n = 12] and/or clinical and sonographic follow-up of at least one year [n = 554] did not reveal malignancy. Thus, these 1302 TNs were classified as TI-RADS 2.The remaining 2194 TNs (60.1%) of the total of 3650 TNs with no ultrasound criteria for malignancy (score of zero) appeared as: hyperechoic with or without small cystic ab-normalities (527/2194); and solid with peripheral vascularity and a mixed pattern of hypo, iso or hyperechoic spots and/or small cystic changes and/or macrocalcifications (1667/2194). Only 48 (2.2% of 2194) were malignant (histologically con-firmed after surgery). In the remaining 2146, additional tests (FNA [n = 177) and/or histological examination after surgery [n = 569] and/or thyroid scintigraphy [n = 687] and/or elasto-sonograhy [n = 128] and/or MRI/PET/CT [n = 18] and/or clini-cal and ultrasound follow-up of at least one year [n = 843] did not reveal malignancy. This type of TN was classified as TI-RADS 3 (i.e., low probability of malignancy).In turn, 154/3650 TNs (4.2%) were assigned one or more points of potential malignancy (table 2). One-hundred and five of those TNs had a score of 1 and 10 of them were ma-lignant (10/105; 9.5%). In 12 of 25 TNs with a score of 2, thy-roid carcinoma was histologically detected (12/25; 48%) and in the case of TNs with a score of 3-4, malignancy increased up to 85% (12/14).With the aim of unifying terminology and considering the malignancy rates published by Horvath et al3 and Kwak et al6, thyroid nodules were classified as TI-RADS 4a when they had a score of 1 (malignancy below 10%), as TI-RADS 4b when they had a score of 2 (malignancy 10-50%) and as TI-RADS 4c when they had a score of 3-4 (malignancy 50-85%). In the remaining 120 TNs with a score of 4, no carcinoma was detected by the reference methods.TNs with a score of 5 or higher were classified as TI-RADS 5 (probably malignant, similar to the BI-RADS system). In our study, these TNs were histologically diagnosed as differenti-ated thyroid carcinoma (10/10; 100%). Histologically, thyroid
Table 1: Sonographically suspicious criteria for malignancy. Each criterion is assigned a point in the final score. If suspi-cious cervical lymph nodes are detected, an additional point is added to the score for categorizing nodules on TI-RADS classification.
• Hypoechogenicity• Microcalcifications• Partially cystic nodule with eccentric location of the fluid portion and lobulation of the solid component• Irregular margins• Perinodular thyroid parenchyma invasion• Taller-than-wide shape• Intranodular vascularity

Rev. Argent. Radiol. 2014;78(3): 138-148
TI-RADS classification of thyroid nodules based on a score modified according to ultrasound criteria for malignancy
140
carcinomas were papillary (n = 25), follicular (n = 15), oxy-philic (n = 2) or medullary (n = 2).In 3/6127 cases thyroid papillary carcinoma was diagnosed prior to ultrasound examination due to surgical excision of metastatic cervical adenopathy. As in BI-RADS classification, these cases were classified as TI-RADS 6.Table 3 summarizes findings in the scoring system and the corresponding category according to TI-RADS classification, while table 4 shows the positive predictive value of TI-RADS categories in this study.
Discussion
TNs are common. The prevalence of TNs in autopsies ranges between 8.2 and 64.6%21,22, while detection by ultrasound has increased from 19% to 68% with the technological devel-opment of ultrasound equipment23-25. However, TNs continue to be difficult to evaluate and this is why there are a large number of medical guidelines. So much so that, according to a research literature review conducted on PubMed/Medline for the preparation of this manuscript, only in the (approximately) last 10 years, over 250 articles have been published, including studies, recommendations by medical societies and reviews on guidelines for the detection of TNs, 9,11,13,14,26-35.TNs show different ultrasound patterns, with a hypo, iso or hyperechoic structure which, in turn, may be associated not only with cystic changes of variable shape and size, but also with macro and/or microcalcifications. In addition, the mar-gins and shape of TNs may be different.This diversity (much larger than that of focal lesions in other organs or glands, such as the liver or breast) poses serious difficulties for a proper classification. With the aim of solving this problem, in 2009, Horvath et al3 proposed a classification known as TI-RADS (similar to the sys-tem used for breast lesions, BI-RADS)4,5 and later Kwak et al6 added a subtype (4c). However, not all the ultrasound features of nodules proposed by Horvath et at can be applied with cer-tainty in daily practice6, and as regards Kwak et al, they did not use TN perfusion on color Doppler within their classification. Thus, our study also assessed the presence of suspicious cervi-cal lymph nodes (differentiating them from Kwak classification as regards the evaluation criteria for scoring).Though quoted in the medical literature, TI-RADS classi-fication is hardly used in daily practice. This may be due, in the first place, to an unawareness of this system by the wide range of specialists performing thyroid ultrasound scans
Table 3: TI-RADS classification of thyroid nodules based on a scoring system according to ultrasound criteria for malig-nancy.
TI-RADS 1: Normal thyroid gland. No focal lesion.TI-RADS 2: Benign nodules. Noticeably benign pattern (0% risk of malignancy)Score of zeroTI-RADS 3: Probably benign nodules (<5% risk of malig-nancy)Score of zeroTI-RADS 4:• 4a – Undetermined nodules (5-10% risk of malignancy)Score of 1.• 4b – Suspicious nodules (10-50% risk of malignancy)Score of 2.• 4c – Highly suspicious nodules (50-85% risk of malignancy)Score of 3-4TI-RADS 5: Probably malignant nodules (>85% risk of ma-lignancy)Score of 5 or higherTI-RADS 6: Biopsy-proven malignancy
Table 2: Nodules with a score of 1 or higher in relation to histologically proven malignancy following surgery.
Score according Cases (n) Malignancyto the number of sonographically suspicious criteria for malignancy
1 105 10/105 (9.5%)2 25 12/25 (48%)3-4 14 12/14 (85%)5 or higher 10 10/10 (100%)
Table 4: Positive predictive value of TI-RADS classification stages.
TI-RADS Category PV +
T2/T3 0%T4a 9.5%T4b 48%T4c 85%T5 100%
PV+: positive predictive value

TI-RADS classification of thyroid nodules based on a score modified according to ultrasound criteria for malignancy
Rev. Argent. Radiol. 2014;78(3): 138-148
J. Fernández Sánchez
141
(from family or primary physicians to internists, endocrinolo-gists, surgeons, radiologists and nuclear medicine specialists), but it may also be attributed to some uncertainty on the part of the professional performing the US scan (who may be afraid of misclassifying a TN) or to his/her convenience (as for some professionals it is easier to report, for example, a “nodular goiter” or an “enlarged thyroid gland with an hy-
poechoic nodule”, even if this report is not of great help for the ordering physician).From this perspective, we propose a TI-RADS classification based on a scoring system in which each ultrasound abnor-mality suspicious for malignancy is assigned a score. If one or more cervical lymph nodes suspicious for malignancy are detected, an additional point is added (table 1).
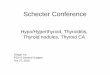
Figure 1 TI-RADS 1: normal thyroid gland. Figure 2 TI-RADS 2: simple thyroid cyst.
Figure 3 TI-RADS 2: solid nodule with central cyst. Figure 4 TI-RADS 2: nodule with homogeneous peripheral calcification.

Rev. Argent. Radiol. 2014;78(3): 138-148
TI-RADS classification of thyroid nodules based on a score modified according to ultrasound criteria for malignancy
142
In this study, 4.7% of thyroid ultrasound scans did not show focal lesion and the thyroid gland showed a hyperechoic, ho-mogeneous and normal ultrasound pattern with no changes in vascularity. These cases constituted category 1 in TI-RADS classification (fig. 1), while 35.6% of TNs with well-defined criteria for benignity (simple cyst, solid nodule with central
cyst, nodule with homogeneous peripheral calcification and spongiform nodule), with benignity being confirmed by vari-ous methods (figs. 2-5), were classified as TI-RADS 2.Only 2.2% of TNs with peripheral vascularity and hyperechoic (with or without cystic changes) or diverse US pattern (hypo, iso or hyperechoic, with cystic changes and/or macrocalcifica-
Figure 5 TI-RADS 2: spongiform nodule. Figure 6 TI-RADS 3: hyperechoic nodule.
Figure 7 TI-RADS 3: slightly hyperechoic nodule with small cysts and peripheral vascularity
Figure 8 The nodule on Figure 7 corresponds to a toxic adeno-ma on thyroid scintigraphy with 99mTC-sodium pertechnetate.

TI-RADS classification of thyroid nodules based on a score modified according to ultrasound criteria for malignancy
Rev. Argent. Radiol. 2014;78(3): 138-148
J. Fernández Sánchez
143
Figure 9 TI-RADS 3: several nodules in the same gland with a similar ultrasound pattern: hyper or isoechoic nodules, with small cystic changes and small hypoechoic spots, as well as microcalcifications (arrow) and peripheral perfusion. In the thyroid scintigraphy (lower row on the right) TNs appear as toxic adenomas in a patient with hyperthyroidism.
Figure 10 Patient with nodular goiter. In a hyperechoic nodule with small cysts, consistent with TI-RADS 3, a small papillary thyroid carcinoma (pT1b) was histologically detected after surgery.
Figure 11 TI-RADS4a: markedly hypoechoic nodule, of normal shape and abnormal vascularity. Score of 1.
Figure 12 TI-RADS 4b: nodule with microcalcifications and poorly defined irregular margins. Score of 2.

Rev. Argent. Radiol. 2014;78(3): 138-148
TI-RADS classification of thyroid nodules based on a score modified according to ultrasound criteria for malignancy
144
Figure 13 TI-RADS 4b: nodule with two sonographically suspi-cious criteria for malignancy: hypoechogenicity and internal vascularity.
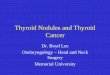
Figure 14 TI-RADS 4c: nodule with microcalcifications, irregu-lar borders and taller than wide shape (greater in its antero-posterior diameter than in its transverse diameter). Score of 3.
Figure 15 TI-RADS 4c: hypoechoic nodule of irregular margins with a taller than wide shape. Score of 3.
Figure 16 TI-RADS 5: hypoechogenic nodule with microcal-cifications and poorly defined margins, with perinodular tis-sue invasion (arrow). Taller than wide shape. Presence of a cervical lymph node suspicious for malignancy (see: Fig. 17). Overall score of 6.

TI-RADS classification of thyroid nodules based on a score modified according to ultrasound criteria for malignancy
Rev. Argent. Radiol. 2014;78(3): 138-148
J. Fernández Sánchez
145
tions) proved to be malignant. These TNs with a score of 1 and probably benign US findings are classified as TI-RADS 3 (fig. 6) (probability of malignancy < 5%) according to Hor-vath et al3 and Kwak et al6. In this respect, it should be noted that many of the TI-RAD 3 nodules are functioning or toxic thyroid adenomas (figs. 7-9) and that malignancy within this category is not only a rare occurrence, but also a generally unexpected histological finding following nodular goiter sur-gery (fig. 10). In our study, 9.5% of TNs meeting one criterion for malignancy were diagnosed as thyroid carcinoma.TNs with a score of 1 were assigned category 4a in TI-RADS classification (fig. 11), while TNs with a score of 2 were clas-sified as TI-RADS 4b (figs. 12 and 13). In the latter case, the incidence of malignancy increased up to 48%. In turn, TNs with a score of 3 or 4 showed an increased incidence of thy-roid carcinoma of up to 85%, and were therefore included within TI-RADS 4c (figs. 14 and 15). In this category, Kwak et al6 report a probability of malignancy of 50-95%.Finally, TNs with a score of 5 or higher were classified as TI-RADS 5 (figs. 16 and 17). In our study, all TNs with these ultrasound features proved to be malignant, but Horvath et al3 and Kwak et al6 report for this category a probability of malignancy of 85-99%.The TI-RADS classification based on the scoring system is shown in table 3. The advantage of this method is that it is more practical and easy to apply. The first step in the US clas-sification of TNs consists in evaluating the potential presence of criteria for suspected malignancy. When their presence is
detected, points must be added to the score as appropriate. Thus, if a TN has a score of 0, it is either definitely benign (TI-RADS 2) with the aforementioned US patterns (simple cyst, solid nodule with central cyst, nodule with homogeneous peripheral calcification and spongiform nodule) or prob-ably benign (TI-RADS 3). As from a score of 1, TNs begin to have, depending on the final score, from an undetermined categorization to a high probability of malignancy. For TNs classified as TI-RADS 4a, management will depend on the pa-tient’s general clinical condition. In the event of an incidental finding in a patient with a medical history that suggests no risk of developing thyroid carcinoma (for example, no family history of thyroid carcinoma, no exposure to previous radia-tion to the neck for malignancies, etc.), an ultrasound scan is enough for TNs less than 1 cm in size, while nodules larger than 1 cm should be examined by thyroid scintigraphy using 99mTC-sodium pertechnetate to evaluate their uptake36,37. The possible protocol-based management of TI-RADS 4a, with an additional evaluation by FNA, depends on medical history, clinical examination and ultrasound and scintigraphy findings (further prospective studies would be required). On the contrary, TNs classified as TI-RADS 4b and 4c should al-ways undergo FNA, except if contraindicated or in the event of high risk. Based on the results of this study, TI-RADS 5 nod-ules invariably require histological examination after surgery.Limitations to this study include the lack of cytological or histologi-cal confirmation for all cases. However, those performing ultra-sound diagnosis of TNs in daily practice are aware of the impos-sibility of performing FNA or surgery in all nodules. This is also impracticable in clinical trials for ethical reasons. In fact, owing to technological advances in ultrasound imaging and to the imple-mentation of new techniques (such as color Doppler or elastogra-phy) and other diagnostic methods (e.g., scintigraphy or PET/CT), it has been possible to reduce the number of these interventions.Even if some thyroid carcinomas have slow progression, when further diagnostic methods show signs of benignity in medi-cal practice, this is considered to be enough, because the likelihood that they may become malignant is low. For this reason, despite the unavailability of cytological or histological confirmation for all 3650 nodules, benignity as defined by those methods was considered to be valid. Furthermore, in 966 TI-RADS 2 and 3 cases, FNA or surgery was effectively performed, and in all cases of TI-RADS 3, 4a, 4b, 4c and 5 malignancy, histological confirmation was performed.TI-RADS is a merely sonographic classification. The final evalu-ation and therapeutic decision-making in the presence of a TN cannot be limited to the results of a thyroid ultrasound. In addition to the standard laboratory tests for the evaluation of thyroid function, measurement of thyroglobulin, calcitonin and diverse anti-thyroid antibodies is also important, as well as the thyroid scintigraphy using 99mTC-sodium pertechnetate.
Figure 17 TI-RADS 5: suspicious hypoechoic lymph node, with round shape and abnormal vascularity. Overall score of 6 for the nodule of fig. 16.

Rev. Argent. Radiol. 2014;78(3): 138-148
TI-RADS classification of thyroid nodules based on a score modified according to ultrasound criteria for malignancy
146
Conclusion A TI-RADS classification of TNs based on a score according to the most relevant sonographically suspicious criteria for malignancy can be better and more easily applied in daily practice. Based on the criteria for malignancy and the score assigned in this study, the probability of malignancy for TNs with a score of 1 is 10%, while for those with a score of 2 is almost 50% and for those that have been assigned a score of 3 or 4, the probability of malignancy is 85%. All TNs with a score of 5 or higher are malignant.A TI-RADS classification based on the scoring system de-scribed above should allow for and lead to unification of ter-minology and codes for TN classification among all physicians who evaluate the results of a thyroid ultrasound (whether they are primary physicians, endocrinologists, radiologists or specialists in nuclear medicine).
Conflicts of interestThe author declares no conflicts of interest.
References
1. Raggiunti B, Capone F, Franchi A, Fiore G, Filipponi S, Colagrande V, et al. Ultrasoundelastography: Can it provide valid information for dif-ferentation of benign and malignant thyroid nodules? J Ultrasound. 2011;14:136---41.
2. Moon WJ, Jung SL, Lee JH, Na DG, Baek JH, Lee YH, et al. Benign and malignant thyroid nodules: US differentiation --- multicenter retrospective study. Radiology. 2008;247:762---70.
3. Hovarth E, Majlis S, Rossi R, Franco C, Niedmann JP, Castro A, et al. An ultrasonogram reporting system for thyroid nodules stratifying cancer risk for clinical management. J Clin Endocrinol Metab. 2009;94:1748---51.
4. Liberman L, Menell JH. Breast imaging reporting and data system (BI-RADS). Radiol Clin North Am. 2002;40: 409---30.
5. Burnside ES, Sickles EA, Bassett LW, Rubin DL, Lee CH, Ikeda DM, et al. The ACR BI-RADS experience: learning from history. J Am Coll Radiol. 2009;6:851---60.
6. Kwak JY, Han KH, Yoon JH, Moon HJ, Son EJ, Park SH, et al. Thyroid imaging reporting and data system for US features of nodules: a step in establishing better stratification of cancer risk. Radiology. 2011;260:892---9.
7. Papini E, Guglielmi R, Bianchini A, Crescenzi A, Taccogna S, Nardi F, et al. Risk of malignancy in nonpalpable thyroid nodules: predictive value of ultra-sound and color-Doppler features. J Endocrinol Metab. 2002;87:1941---6.
8. Iannuccilli JD, Cronan JJ, Monchik JM. Risk for malignancy of thyroid nod-ules as assessed by sonographic criteria: the need of biopsy. J Ultrasound Med. 2004;23: 1455---64.
9. Frates MC, Benson CB, Charboneau JW, Cibas ES, Clark OH, Coleman BG, et al. Management of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference statement. Radiology. 2005;237:794---800.
10. Cappelli C, Castellano M, Pirola I, Gandossi E, De Martino E, Cumetti D, et al. Thyroid nodule shape suggests malignancy. Eur J Endocrinol. 2006;155:27---31.
11. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, et al. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer; Revised American Thyroid Association management guidelines for patients with thyroid nodules and differenti-ated thyroid cancer. Thyroid. 2009;19:1167---214.
12. Lee MJ, KimEK, Kwak JY, Kim MJ. Partially cystic thyroid nodules on ultra-
sound: probability of malignancy and songraphic differentiation. Thyroid. 2009;19:341---6.
13. Gharib H, Papini E, Paschke R, Duick DS, Valcavi R, Hegedüs L, et al., Ameri-can Association of Clinical Endocrinologists. Assoziazone Medici Endocri-nologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules: executive summary of recommendations. J Endocrinol Invest. 2010;33:51---6.
14. Moon WK, Baek JH, Jung SL, Kim DW, Kim EK, Kim JY, et al. Ultrasonog-raphy and ultrasound-based mangement of thyroid nodules: consensus statement and recommendations. Korean J Radiol. 2011;12:1---14.
15. Domínguez JM, Baudrand R, Cerda J, Campusano C, Fardella C, Arteaga E, et al. An ultrasound model to discriminate the risk of carcinoma. Acad Radiol. 2011;18:242---5.
16. Kim DW, Park JS, In HS, Choo HJ, Ryu JH, Jung SJ. Ultrasoundbased diag-nostic classification for solid and partially cystic thyroid nodules. AJNR Am J Neuroradiol. 2012;33:1144---9.
17. Ko MS, Jeong KS, Shong YK, Gonng GY, Baek JH, Lee JH. Collapsingn be-nign cystic nodules of the thyroid gland: sonographic differentation from papillary thyroid carcinoma. AJNR Am J Neuroradiol. 2012;33:124---7. 148 J. Fernández Sánchez
18. Kim BM, Kim MJ, Kim EK, Kwak JY, Hong SW, Son EJ, et al. Sonographic differentiation of thyroid nodules with eggshell calcifications. J Ultrasound Med. 2008;27:1425---30.
19. Bonavita JA, Mayo J, Babb J, Bennett G, Oweity T, Macari M, et al. Pattern recognition of benign nodules at ultrasound of the thyroid: which nodules can be left alone? AJR Am J Roentgenol. 2009;193:207---13.
20. Virmani V, Hammond I. Sonographic patterns of benign thyroid nodules: verification at our institution. AJR Am J Roentgenol. 2011;196:891---5.
21. Hull OH. Critical analysis of two hundred twenty-one thyroid glands; study of thyroid glands obtained at necropsy in Colorado. AMA Arch Pathol. 1955;59:291---311.
22. Dean DS, Gharib H. Epidemiology of thyroid nodules. Best Pract Res Clin Endocrinol Metab. 2008;22:901---11.
23. Carroll BA. Asymptomatic thyroid nodules: incidental sonographic detec-tion. AJR Am J Roentgenol. 1982;138:499---501.
24. Wiest PW, Hartshorne MF, Inskip PD, Crooks LA, Vela BS, Telepak RJ, et al. Thyroid palpation versus high-resolution thyroid ultrasonography in the detection of nodules. J Ultrasound Med. 1998;17:487---96.
25. Guth S, Theune U, Aberle J, Galach A, Bamberger CM. Very high preva-lence of thyroid nodules detected by high frequency (13 MHz) ultrasound examination. Eur J Clin Invest. 2009;39:699---706.
26. Camargo R, Corigliano S, Friguglietti C, Gauna A, Harach R, Munizaga F, et al. Latin American thyroid society recommendations for the management of thyroid nodules. Arg Bras Endocrinol Metabol. 2009;53:1167---75.
27. Perros P, American Thyroid Association. 2009 American Thyroid As-sociation guidelines on thyroid nodules. Clin Oncol (R Coll Radiol). 2010;22:469---71.
28. Boelaert K. Thyroid gland: Revised guidelines for the management of thy-roid cancer. Nat Rev Endocrinol. 2010;6: 185---6.
29. Unnikrishnan AG, Kalra S, Baruah M, Nair G, Nair V, Bantwal G, et al. En-docrine Society of India management guidelines for patients with thyroid nodules: A position statement. Indian J Endocrinol Metab. 2011;15:2---8.
30. Milas Z, Shin J, Milas M. New guidelines for the management of thy-roid nodules and differentiated thyroid cancer. Minerva Endocrinol. 2011;36:53---70.
31. Wémeau JL, Sadoul JL, d´Herbomez M, Monpeyssen H, Tramalloni J, Leteur-tre E, et al. Guidelines of the French society of endocrinology for the man-agement of thyroid nodules. Ann Endocrinol (Paris). 2011;72:251---81.
32. Levine RA. Current guidelines for the management of thyroid nodules. Endocr Pract. 2012;18:596---9.
33. Rosário PW, Ward LS, Carvalho GA, Graf H, Maciel RM, Maciel LM, et al. Thyroid nodules and differentiated thyroid cancer: update on the Brazilian consensus. Arg Bras Endocrinol Metabol. 2013;57:240---64.
34. Hofman MS. Thyroid nodules: time to stop over-reporting normal findings and update consensus guidelines. BMJ. 2013;347:f5742.
35. Paschke R, Hegedüs L, Alexander E, Valcavi R, Papini E, Gharib H. Thy-roid nodules guidelines: agreement, disagreement and need for future research. Nat Rev Endocrinol. 2011;7:354---61.
36. Meller J, Becker W. The continuing importance of thyroid scintigraphy in the era of high-resolution ultrasound. Eur J Nucl Med Mol Imaging. 2002;29:S425---38.
37. Mansi L, Moncayo R, Cuccurullo V, Dottorini ME, Rambaldi PF. Nuclear medicine in diagnosis, staging and follow-up of thyroid