Embed Size (px)
Citation preview

1174 BRIEF REPORTS BRIEF REPORTS
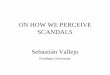
Figure 8. The handles are moved downward and the hooks are levered outof the airway.
sheep) did not allow for any quanti-fication of blood loss. Likewise, post-operative dissection to documentsoft-tissue damage from either tech-nique was not performed in thisstudy. However, prior to the datagathering phase of the study, tra-cheal endoscopy was used to observethe laryngeal structures during theperformance of multiple cricothyro-tomies. During this purely observa-tional phase, we did not observe anyevidence of complicating trauma tothe laryngeal structures from the in-vestigational device.
CONCLUSIONS
The use of this novel device for cri-cothyrotomy resulted in faster andeasier intubations over a standardsurgical technique. This device maybe a significant addition to standardemergency airway equipment. Thisdevice warrants further investiga-tion to determine its utility in clini-cal practice.—AARON E. BAIR, MD(e-mail: [email protected]), Divi-sion of Emergency Medicine, Depart-ment of Internal Medicine, U.C.Davis Medical Center, Sacramento,CA; and JOHN C. SAKLES, MD, Uni-versity of Cincinnati, Cincinnati, OH
This project is dedicated to the late B.Tomas Brofeldt, MD, inventor of therapid four-step technique, whose infec-tious enthusiasm, intellectual curiosity,and constant advocacy continue to be asource of inspiration. A special thanks toNathan Kuppermann, MD, MPH, for his
statistical support and assistance withthe preparation of the manuscript.
Presented at the SAEM annual meeting,Washington, DC, May 1997.
Key words. cricothyrotomy; crico-thyroidotomy; surgical airway ac-cess; failed intubation; airway man-agement.
References
1. Melick C, Rosen P. Cricothyrotomyand tracheotomy. In: Dailey RH, SimonB, Young GP, Stewart RD (eds). The Air-way: Emergency Management. St. Louis:Mosby–Year Book, 1992.2. Sakles SC, Laurin EG, Rantapaa AA,Panacek EA. Airway management in theemergency department: a one-year studyof 610 tracheal intubations. Ann EmergMed. 1998; 31:325–32.
3. Chang RS, Hamilton RJ, Carter WA.Declining rate of cricothyrotomy intrauma patients with an emergencymedicine residency: implication in skillstraining. Acad Emerg Med. 1998; 5:247–51.4. Weiss S. A new emergency cricothy-rotomy instrument. J Trauma. 1983; 23:155–8.5. Toye FJ, Weinstein JD. Clinical ex-perience with percutaneous tracheos-tomy and cricothyrotomy in 100 patients.J Trauma. 1986; 26:1034–40.6. Ciaglia P, Firsching R, Syniec C. Elec-tive percutaneous dilational tracheos-tomy. Chest. 1985; 87:715.7. Brofeldt BT, Panacek EA, RichardsJR. An easy cricothyrotomy approach:the rapid four-step technique. AcadEmerg Med. 1996; 3:1060–3.8. Holmes JF, Panacek EA, Sakles JC,Brofeldt BT. Comparison of 2 cricothy-rotomy techniques: standard methodversus rapid 4 step technique. AnnEmerg Med. 1998; 32:440–6.9. Davis DP, Bramwell KJ, Vilke GM,Rosen PB. Cricothyrotomy technique:standard technique versus the rapid fourstep technique. J Emerg Med. 1999; 17:17–21.10. Griggs WM. Cricothyrotomy concern[letter]. Acad Emerg Med. 1997; 4:1006–7.11. Mace S. Cricothyrotomy. In: RobertsJR, Hedges JR (eds). Clinical Proceduresin Emergency Medicine. Philadelphia: W.B. Saunders, 1997.12. McCormack HM, Horne DJ,Sheather S. Clinical applications of vi-sual analogue scales: a critical review.Psychol Med. 1988; 18:1007–1019.13. McDowell I, Newell C. Pain mea-surements. In: Measuring Health: AGuide to Rating Scales and Question-naires. New York: Oxford UniversityPress, 1996.14. Stata Corp. Stata Statistical Soft-ware: Release 5.0. College Station, TX:Stata Corporation, 1997.15. Davis DP, Bramwell KJ, HamiltonRS, Chan TC, Vilke GM. Cricothyrotomyspeed and safety: a comparison betweenstandard open technique and rapid four-step technique using a novel device [ab-stract]. Acad Emerg Med. 1998; 5:483.
Thrombolytics and Stroke: What DoEmergency Medicine Residents Perceive?
The use of thrombolytics in acutestroke remains controversial, andthe attitudes of emergency medicine(EM) residents on this topic are un-clear. It might be hypothesized thatas young physicians in training,they would be very likely to be ex-posed to thrombolytic therapy (as bydefinition, they work in teachinghospitals) and would therefore be
quite likely to embrace this innova-tive approach with some enthusi-asm. On the other hand, it is possi-ble that they would have a moreskeptical perspective and be rela-tively more resistant to the intensemarketing efforts that this therapyhas engendered.
The purpose of this direct-mailsurvey was to determine the percep-

ACADEMIC EMERGENCY MEDICINE • November 1999, Volume 6, Number 11 1175
tions, experience, and knowledge ofthrombolysis for acute stroke amongEM residents.
METHODS
Study Design. This was a surveyof EM residents to determine atti-tudes regarding the use of throm-bolytics and stroke. Because of itsvoluntary nature, this study wasconsidered exempt from informedconsent.
Study Participants. One thou-sand six hundred sixteen direct-mailsurveys were sent to all PGY1 andPGY3 allopathic EM residents andto all osteopathic EM residents(PGY2–4).
Survey Content and Adminis-
tration. The survey asked aboutresidents’ experience with thrombo-lytics for stroke, their knowledgeabout thrombolytics and stroke, andtheir attitudes and confidence aboutadministering thrombolytics. Thesurvey was first mailed in early1997 and a second mailing was sentto all nonrespondents approximatelythree months later. Residents couldmail or fax the complete two-pagesurvey back; forms were coded to al-low identification of respondents.
Data Analysis. Descriptive andcontingency table analyses werecompleted using SPSS Base 8.0 soft-ware (SPSS Inc., Chicago, IL). Bi-variant chi-square tests of indepen-dence among dichotomous variablesof interest were followed by assess-ment of the strength of associationusing phi (f) coefficients. The phi co-efficient is expressed on a scale of 0to 1 and has an interpretation sim-ilar to the Pearson correlation coef-ficient, r. Values of f above 0.90 in-dicate a very strong relationshipbetween variables, 0.70 to 0.89 astrong relationship, 0.50 to 0.69 amoderate relationship, 0.39 to 0.49a low relationship, and below 0.30 aweak relationship.
RESULTS
After the initial mailing, 471 sur-veys were returned for an initial re-sponse rate of 29.2%. Following thesecond mailing, which offered the
chance to win a $250 prize, an ad-ditional 230 responses were re-ceived, for an overall gross responserate of 43.4%. For purposes of anal-ysis, all PGY1s and PGY2s were an-alyzed as ‘‘junior’’ residents; allPGY3s and PGY4s were classified as‘‘seniors.’’ The PGY1 and PGY3 re-spondents totaled 85.4% of all re-sponders, reflecting the relativelysmall number of osteopathic pro-grams nationally, and the paucity ofPGY4 allopathic positions.
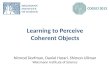
Of the respondents, 34.1% hadpersonally taken care of a patient forwhom thrombolytic therapy wasused for stroke; the response waspositively correlated with residencyyears (x2 = 33.54, p < 0.001; f =0.22). Seventy-three percent consid-ered their knowledge of thrombolytictherapy to be very good or somewhatgood, and 26.7% considered theirknowledge to be weak, and this per-ception was also positively corre-lated with residency year (x2 =57.05, p < 0.001; f = 0.29). Most re-spondents, 88.2%, stated that theywould personally take tissue plas-minogen activator (tPA) therapy ifthey had a stroke, and this was neg-atively correlated as well; the juniorresidents were significantly morelikely to state that they would per-sonally take tPA than the senior res-idents (x2 = 4.19, p < 0.05; f = 20.8).With regard to consultants, 53.6%stated that they would administerthrombolytics after a phone consul-tation with a neurologist; 7.6%would administer treatment withouta consult, and 34.7% would requirea neurologic evaluation prior to tPAadministration. Only 3.9% wouldnot give tPA for stroke under anycircumstances (Fig. 1). Just lessthan half the total group (44.1%)correctly identified the intracranialbleeding rate of patients given tPAfor stroke at 7%.
With regard to confidence in ra-diographic imaging reading beforegiving thrombolytics, 64.9% wouldnot give tPA unless the CT scan wasread by a radiologist. Fourteen per-cent would administer after emer-gency physician (EP) interpretationonly, almost 14% would require aneuroradiologist reading, and 6.8%would accept interpretation by aneurologist. About a fourth (25.4%)considered thrombolytics for strokea ‘‘major advance’’; 4.6% considered
it ‘‘no advance,’’ with more juniorresidents more likely to consider it a‘‘major advance’’ than senior resi-dents (x2 = 7.05, p < 0.01; f = 20.18).
DISCUSSION
Thrombolytic use for acute strokeremains a controversial area. Recentstudies indicate that there are con-siderable uncertainties as to whenand how this form of treatmentshould be used.1–3 Although the useof tPA for stroke has been approvedby the FDA since 1996, continuingcontroversy regarding the NINDS4
and ECASS5 studies may have con-tributed to the modest scale ofthrombolytic use in stroke.
The position of EPs as well asEM residents regarding the use oftPA in stroke is unclear. Althoughdata regarding the ability of EPs toaccurately evaluate head CTs inthrombolytic candidates have re-cently been published,6 we know ofno data describing the attitudes ofEM residents toward the differentissues presented by this techniqueor their knowledge of this subject.
Our study, which included re-sponses from more than one of everysix EM residents in the country, an-swers some of these questions. Con-sistent with our goal of comparingchanges in attitude that might occurduring residency training, our targetpopulation emphasized the two larg-est resident classes likely to show adifference, PGY1 and PGY3 (allo-pathic) and PGY2 and PGY4 (osteo-pathic). Almost nine of ten agreedthat they would take tPA personallywith a stroke, and less than 4%would not give it to a patient underany circumstances. Residents seemto be well aware of the subject withalmost three fourths saying theirknowledge was good or very good, al-though only approximately a thirdhad actually taken care of a patienttreated with thrombolytics forstroke. The finding that enthusiasmfor the therapy decreases with in-creasing postgraduate year may berelated to the recognition that fewstroke patients are candidates fortreatment.
LIMITATIONS AND FUTUREQUESTIONS
Our survey format has a few signif-

1176 BRIEF REPORTS BRIEF REPORTS
Figure 1. Survey responses regarding experience in using tissue plasminogen activator (tPA) in stroke, knowledgeregarding tPA use, and willingness to be treated with tPA.
icant limitations. First, there is nocertainty that our respondents pre-cisely represented the entire groupof domestic EM residents. However,the fact that the number of respon-dents represent approximately 15%of all EM residents in the countrymakes it unlikely that those re-sponding were markedly differentfrom nonrespondents. Supportingthis, there was no difference in thegroup who responded to the initialmailing and those who respondedonly to the second attempt, with itssignificant incentive. Further, it islikely that residents with strongfeelings (either positive or negative)would be more likely to respond toour survey than those who are moreagnostic. We were unable to assesswhat, if any, effect this would haveoverall. Also, in this rapidly evolvingand controversial field, it is possiblethat resident attitudes and experi-ences would change rapidly. Hence,it would seem reasonable to resur-vey a similar group within the nextfew years to better ascertain how
opinion and practices are changing.Finally, the narrow scope of our re-spondents (all EM residents) cau-tions against ascribing a similar per-spective and knowledge base toother classes of physicians. For ex-ample, ED attendings in the sameprograms might differ markedlyfrom their own residents; EPs innonteaching facilities would likelyvary even more.
CONCLUSIONS
Emergency medicine residents acrossthe country are quite involved withthe issues surrounding thrombolyt-ics and stroke; their knowledge andconfidence increase with increasingyears in training, but their optimismfor using such therapy does not.—BLOSSOM KUNNEL, DO, and MI-CHAEL HELLER, MD, EmergencyMedicine Residency of the LehighValley, Department of EmergencyMedicine, St. Luke’s Hospital, Beth-lehem, PA
Key words. thrombolytics; stroke;emergency medicine residents.
References
1. Spranger M, Steiner T, Schwab S, etal. Acute ischemic stroke: revasculariz-ing therapy. Stroke Council of the Amer-ican Heart Association. J Neur. 1998;245:567–72.2. Alberts MJ. tPA in acute ischemicstroke: United States experience and is-sues of the future. Neurology. 1998; 51(3suppl 3):S53–S55.3. DelZoppo GJ. Clinical trials in acutestroke: why have they not been success-ful? Neurology. 1998; 51(3 suppl 3):S59–S61.4. National Institute of NeurologicalDisorders and Stroke (NINDS) rt-PAStroke Study Group. Tissue plasminogenactivator for acute ischemic stroke. NEngl J Med. 1995; 333:151–7.5. Hacke W, Kaste M, Fieschi C, et al.Intravenous thrombolysis recombinanttissue plasminogen activator in acute he-mospheric stroke: The European Coop-erative Acute Stroke Study (ECASS).JAMA. 1995; 274:1017–25.6. Schriger DL, Kalafut M, Starkman S,et al. Cranial CT interpretation in acutestroke: physician accuracy in determin-ing eligibility for thrombolytic therapy.JAMA. 1998; 239:1293–7.