Embed Size (px)
Citation preview

1
Therapy of Small-cell Lung Cancer (SCLC) With a Topoisomerase-I-
inhibiting Antibody-Drug Conjugate (ADC) Targeting Trop-2,
Sacituzumab Govitecan
Jhanelle E. Gray1*, Rebecca S. Heist2*, Alexander N. Starodub3*, D. Ross Camidge4*,
Ebenezer Kio3, Gregory Masters5, W. Thomas Purcell4, Michael J. Guarino5, Jamal
Misleh5, Charles J. Schneider5, Bryan J. Schneider6, Allyson J. Ocean6, Tirrell
Johnson7, Leena Gandhi2, Kevin Kalinsky8, Ronald J. Scheff6, Wells A. Messersmith4,
Serengulam V. Govindan9, Pius Maliakal9, Boyd Mudenda9, William A. Wegener9,
Robert M. Sharkey9, and David M. Goldenberg9
1H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL; 2Massachusetts
General Hospital Cancer Center, Harvard Medical School, Boston, MA; 3Indiana
University Health Center for Cancer Care, Goshen, IN; 4University of Colorado Cancer
Center, Aurora, CO; 5Helen F. Graham Cancer Center & Research Institute, Newark,
DE; 6Weill Cornell Medicine, New York, NY; 7UF Health Cancer Center, Orlando, FL; 8Columbia University Medical Center-Herbert Irving Comprehensive Cancer Center,
New York, NY; 9Immunomedics, Inc., Morris Plains, NJ
*These authors contributed equally.
Corresponding author: Jhanelle E. Gray, H. Lee Moffitt Cancer Center & Research Institute, 12902 Magnolia Drive, FOB 1, Tampa, FL 33612. 813-745-6895 (phone); 813-745-3027 (Fax); [email protected] (email), or David M. Goldenberg, Immunomedics, Inc., 300 The American Road, Morris Plains, NJ 07950. 973-605-8200 (phone); 973-605-8311 (fax), [email protected] (email).
Running Title: Sacituzumab Govitecan for Small-cell Lung Cancer
Disclosure of Potential Conflicts of Interest: D.M. Goldenberg has stock (including
patents) in Immunomedics, Inc., and is a Board member. S.V. Govindan, P, Maliakal, B.
Mudenda, W.A. Wegener, and R.M. Sharkey are employees of Immunomedics, Inc.,
with stock options.
Presented in part at the Annual Meeting of the American Society of Clinical Oncology, Chicago, IL, June 3-7, 2016, and at the Annual Meeting of the American Association for Cancer Research, Washington, D.C., April 1-5, 2017.
Clinical Trial Identifier: NCT01631552
Statement of significance: A novel antibody-drug conjugate has been tested for safety and efficacy in patients with metastatic small-cell lung cancer after receiving a median of two prior therapies. The results indicate that this is an active agent in this very advanced patient population, warranting further clinical development.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

2
Note: Supplementary data for this article are available at Clinical Cancer Research Online (http://clincancerres.aacrjournals.org/)
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

3
Translational Relevance
No new therapeutic has been approved for the treatment of metastatic (stage IV)
small-cell lung cancer (mSCLC) in twenty years. In this trial, we evaluated a novel
antibody-drug conjugate (ADC), sacituzumab govitecan (IMMU-132), comprised of an
antibody targeting Trop-2 and containing the active metabolite of irinotecan, SN-38 (a
topoisomerase-I inhibitor). Repeated treatment cycles had manageable toxicity with
tumor reduction in the majority of patients, including objective responses in 17% at the
optimal dose schedule and with a median response duration of 5.7 months, based on
an intention-to-treat analysis. These patients had a median of two prior therapies.
Activity was observed in patients who were chemosensitive or chemoresistant to first-
line chemotherapy, and also in patients who failed second-line topotecan therapy. Thus,
sacituzumab govitecan is a promising new therapeutic for advanced mSCLC.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

4
Abstract
Purpose: We evaluated a Trop-2-targeting antibody conjugated with SN-38 in
metastatic small-cell lung cancer (mSCLC) patients.
Experimental Design: Sacituzumab govitecan was studied in patients with
pretreated (median, 2; range, 1-7) mSCLC who received either 8 or 10 mg/kg i.v. on
days 1 and 8 of 21-day cycles. The primary endpoints were safety and objective
response rate (ORR); duration of response, progression-free survival (PFS), and overall
survival (OS) were secondary endpoints.
Results: Sixty percent of patients showed tumor shrinkage from baseline CTs.
On an intention-to-treat basis (N= 50), the ORR was 14% (17% for 10 mg/kg group); the
median response duration, 5.7 months; the clinical benefit rate (CBR>4 months), 34%;
median PFS, 3.7 months; median OS, 7.5 months. There was a suggested
improvement in PR, CBR, and PFS with sacituzumab govitecan in second-line patients
who were sensitive to frontline therapy, but no difference between frontline
chemosensitive vs chemoresistant patients in the overall population. There was a
statistically significant higher OS in those patients who received prior topotecan vs no
topotecan therapy in a small subgroup. Grade >3 adverse events included neutropenia
(34%), fatigue (13%), diarrhea (9%), and anemia (6%). Trop-2 tumor staining was not
required for patient selection. No antibodies to the drug conjugate or its components
were detected on serial blood collections.
Conclusions: Sacituzumab govitecan appears to have a safe and effective
therapeutic profile in heavily-pretreated, mSCLC patients, including those who are
chemosensitive or chemoresistant to frontline chemotherapy. Additional studies as a
monotherapy or combination therapy are warranted.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

5
Introduction
Small-cell lung cancer (SCLC), originating from neuroendocrine progenitor cells,
comprises approximately 15% of all lung cancers, yet has one of the lowest 5-year
survival rates at 6% (1, 2). This is because of its highly aggressive nature, with about
two-thirds of patients already having metastatic disease at diagnosis (3). While palliative
first-line therapy of stage IV SCLC (mSCLC) has a high initial response rate of 60-75%,
the outcome is poor, with a median progression-free survival (PFS) of only 5.5 months
and a median overall survival (OS) of <10 months with platinum-based chemotherapy
(3). Responses to second-line therapy have been poorer, such as <10%, with a median
survival of only 4 to 5 months following second- or third-line chemotherapy (1, 3-5).
Unfortunately, those patients with platinum-resistant mSCLC (i.e., response duration <3
months) fare even worse (6). In the USA, the only approved drug in this second-line
setting of chemosensitive patients (duration of response >3 months), since 1998, is
topotecan, indicated for recurrent patients who were sensitive (duration of response
exceeding 3 months) (7-9). Still, irinotecan, taxanes, vinorelbine, gemcitabine, and
pemetrexed also are given frequently to patients with chemosensitive recurrent disease
(10-14). A review of recent randomized phase II and III clinical trials, including
topotecan in a control arm, showed 13 to 17% responses in second-line with topotecan,
but with as much as a 20% response rate among patients with chemosensitive disease,
while only 4% for those whose tumors were chemoresistant (15). However, these
responses and/or disease stabilization in second-line do not translate into improved
survival. For example, Hagmann and colleagues (16) reported a 22.5% response, a
median PFS of 2.4 months, and a median OS of 5 months with topotecan. In a third-line
setting, no objective responses were achieved, while a median PFS of 1.3 months and
a median OS of 2.5 months were reported (16). Other established single-agent
chemotherapies or retreatment with platinum plus etoposide combinations also have
been disappointing, yielding similar survival outcomes as topotecan alone (16). A
possible exception is amrubicin, a topoisomerase II inhibitor that was approved in Japan
in 2002, where studies reported a median survival of 7 to 12 months when given in
second-line, and appears to be useful in the therapy of relapsed SCLC (17-19). A
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

6
phase III trial conducted in the US, Europe, and Australia showed that while amrubicin
did not improve survival, it demonstrated activity and an acceptable safety profile
compared to topotecan (20). Thus, progress in the management of patients with SCLC,
especially those with metastatic disease, has been quite modest over the past 20 years.
Nearly all patients relapse early and succumb to their disease within a year.
The purpose of this study was to evaluate a novel antibody-drug conjugate
(ADC), comprising a topoisomerase-I-inhibiting camptothecin, SN-38 (7-ethyl-10-
hydroxycamptothecin, the active metabolite of irinotecan), linked to a humanized
antibody targeting Trop-2, a glycoprotein that is elevated in many epithelial cancers and
shown to be an attractive and selective target for antibody-based therapy (21). The
prodrug of SN-38, irinotecan, has been studied already in patients with SCLC, but
clinical trials in the USA and Europe have not demonstrated a benefit compared to an
etoposide-containing regimen (12, 22, 23). Therefore, developing an ADC to target the
thousand-fold more active metabolite of irinotecan, SN-38, was hypothesized as being
more active and potentially having a better therapeutic index (21). Also, preclinical
studies in human tumor xenografts indicated that a much higher dose of SN-38 could be
delivered to the tumor via this ADC compared to irinotecan (24). This improved
therapeutic index and encouraging activity were corroborated in the phase I “basket”
trial of sacituzumab govitecan given to patients with diverse metastatic cancers (25), as
well as other phase II trials in triple-negative breast cancer (TNBC) (26), urothelial
cancer (27), and non-small-cell lung cancer (28). We now report that sacituzumab
govitecan (IMMU-132) has activity and manageable toxicity in patients with advanced
and heavily-pretreated mSCLC.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

7
Patients and Methods
Patients
Patients >18 years of age with mSCLC who had relapsed or were refractory to at
least one prior standard line of therapy for metastatic disease, and with measurable
tumors by CT, were enrolled. They were required to have Eastern Cooperative
Oncology Group (ECOG) performance status of 0 or 1, adequate bone marrow, hepatic
and renal function, and other eligibility as described in the phase I trial (25). Previous
therapy had to be completed at least 2 weeks before enrollment.
Study Design and Treatment
The overall objective of this portion of the study was to evaluate safety and
antitumor activity of sacituzumab govitecan in patients with mSCLC. Sacituzumab
govitecan was administered intravenously at an initial infusion rate of 50 mg/h that was
escalated progressively to be completed within 3 h (subsequent infusions completed
within 60-90 min). Premedications (e.g., diphenhydramine, acetaminophen, and
dexamethasone) were prescribed optionally to reduce the risk of infusion reactions.
Doses of 8 or 10 mg/kg were given on days 1 and 8 of a 21-day cycle, with
contingencies to delay (maximum of 3 weeks). Toxicities were managed by supportive
hematopoietic growth-factor therapy for blood cell reduction at any time during
treatment, dose delays and/or modification as specified in the protocol (e.g., 25% of
prior dose), or by standard medical practice. Treatment was continued until disease
progression, initiation of alternative anticancer therapy, unacceptable toxicity, or
withdrawal of consent.
Study Oversight
The protocol and amendments were approved by each institution’s review board
and conducted in accordance with the Declaration of Helsinki and the International
Conference on Harmonization of Good Clinical Practice Guidelines. All patients gave
prior written informed consent. All authors confirmed their adherence to the protocol,
and vouched for the accuracy of the data and analyses.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

8
Study Assessments and Outcome
The primary endpoint was the proportion of patients with an objective response,
assessed by CT imaging (or MRI if contrast-allergic) approximately every 8 weeks until
disease progression, by each institution’s radiology group or a contracted local
radiology service. Objective responses were assessed by Response Evaluation Criteria
in Solid Tumors, version 1.1 (RECIST 1.1) (29). Partial (PR) or complete responses
(CR) required radiologic confirmation within 4 to 6 weeks after the initial response.
Clinical benefit rate (CBR) is defined as the percentage of patients with an objective
response or stable disease (SD) ≥4 months. Survival was monitored every 3 months
until death or withdrawal of consent.
Safety evaluations were conducted during scheduled visits or more frequently if
warranted. Blood count and serum chemistries were checked routinely before
administration of sacituzumab govitecan and when clinically indicated.
Adverse events (AEs) were coded by MedDRA Preferred Term and System
Organ Class (SOC) version 10, with severity assessed by NCI-CTCAE v4.03. All
patients who received sacituzumab govitecan were evaluated for toxicities.
Statistical Analyses
The protocol provided that objective response rates (ORR) were determined for
patients who received ≥2 doses (1 cycle) and had their initial 8-week CT assessment.
Subset analyses were performed based on patients meeting these requirements, while
overall response assessments are reported on an ITT basis. Duration of response is
defined according to RECIST 1.1 criteria, with those having an objective response
measured from time of the first evidence of response until progression, while stable
disease duration is measured from the start of treatment until progression. PFS and OS
are defined from the start of treatment until an objective assessment of progression was
determined (PFS) or death (OS). Duration of response, PFS, and OS were estimated by
Kaplan-Meier methods, with 95% confidence intervals (CI), using MedCalc Statistical
Software, version 16.4.3 (Ostend, Belgium).
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

9
Approximately 50 assessable patients were to be enrolled to provide adequate
safety and efficacy data for evaluation, with an objective response rate ≥15%, based
upon protocol-defined assessability, considered sufficient clinical activity to warrant
further investigation. After initial review of both 8 and 10 mg/kg dosing, 10 mg/kg doses
were selected for further clinical development and received by the majority of patients in
this study, as also was used in the TNBC and non-small-cell lung cancer investigations
(22, 24).
Tumor Trop-2 Immunohistochemistry (IHC) and Immunogenicity of Sacituzumab
Govitecan and Components
Available archival tumor specimens were stained for Trop-2 by IHC, as reported
previously (25, 26). Positivity required at least 10% of the tumor cells to be stained, with
an intensity scored as 1+ (weak), 2+ (moderate), and 3+ (strong). Antibody responses
to sacituzumab govitecan, the IgG antibody, and SN-38 were monitored in serum
samples taken at baseline and then prior to each even-numbered cycle by enzyme-
linked immunosorbent assays performed by the sponsor (25). Assay sensitivity is 50
ng/mL for the ADC and the IgG, and 170 ng/mL for anti-SN-38 antibody.
Results
Patients
A total of 53 mSCLC patients were enrolled between November 2013 and June
2016 after receiving a median of 2 prior lines of therapy (range, 1 to 7). All patients had
received cisplatin or carboplatin plus etoposide, and were considered chemosensitive
(N=27, 51%) or chemoresistant (N=26, 49%) to their platinum-containing frontline
therapy, based on a duration of response of >3 months or <3 months, respectively
(Table 1). While 22 (42%) had only one prior line of therapy, 14 (26%) and 17 (32%)
received 2 and >3 prior lines of therapy, respectively, including topotecan and/or
irinotecan (N=18, 34%), taxanes (N=9, 17%), and immune checkpoint inhibitors (N= 5,
9%). Most patients had extensive disease, with metastases to multiple organs, including
lungs (66%), liver (59%), lymph nodes (76%), chest (34%), adrenals (25%), bone
(23%), and pleura (6%) (Table 1). Other sites of disease included pancreas (N = 4),
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

10
pelvis (N = 2), brain (N = 2), skin (N = 2), and esophageal wall, ovary, and sinus (1
each).
Treatment Exposure, Safety and Tolerability
Of the 53 patients, 15 were treated at 8 mg/kg and 38 at 10 mg/kg. As of the
cutoff date for this report, 51 patients have now discontinued treatment, while two
started treatment about 7 months ago and are still continuing. More than 590 doses
(over 295 cycles) have been administered, with a median of 10 doses (≥ 5 cycles) per
patient, including 2 patients who received >60 doses (>30 cycles), and a median
treatment duration of 2.5 months (range, 1 to 23). No infusion-related reactions were
reported. Ten patients received hematopoietic cytokine support for neutropenia (five
only once, five repeatedly), but only after grade 3 events had occurred, so this use did
not influence the neutropenia or febrile neutropenia rates reported here. Neutropenia
was also the primary indication for dose reductions, which occurred in 18 patients (15 at
10 mg/kg, 3 at 8 mg/kg), and once reduced by 25%, additional reductions were
infrequent. No treatment-related deaths were observed.
The most frequent AEs (all grades) included gastrointestinal toxicity (diarrhea,
nausea/vomiting, abdominal pain, anorexia, constipation), fatigue, neutropenia, anemia,
and alopecia (Table 2). Although 18 patients (34%) had grade ≥3 neutropenia, only
one patient (2%) had febrile neutropenia. Other grade 3 or 4 AEs were limited to fatigue
(N=7, 13%), diarrhea (N=5, 9%), anemia (N=3, 6%), and hypoxia (N=2, 4%).
Efficacy
Three patients were disqualified after receiving their first dose due to protocol
violations, because further review found previously undiagnosed brain metastases in
two and a mixed NSCLC and SCLC histology in the other patient. Therefore, the
intention-to-treat (ITT) population included 50 patients. Of these, 43 patients received
≥2 treatment doses (1 cycle) and had at least one post-baseline CT response
assessment. The remaining 7 left the study prior to their first response assessment, six
patients during cycle one (4 unrelated adverse events, withdrew consent, disease
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

11
progression) and one patient with concurrent multiple comorbidities after cycle 2
(sudden death).
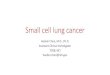
Treatment outcomes for the 43 patients with CT response assessments are
graphed in Fig. 1, including a waterfall plot of the best percentage change in the
diameter sum of the target lesions, showing 26 (60%) experienced a reduction of tumor
size from baseline (Fig. 1A), a graph showing the duration of the responses for those
achieving PR or SD status (Fig. 1B), and a plot tracking the response changes of the
patients with PR and SD over time (Fig. 1C).
Seven patients had partial responses (PR; ≥30% reduction, confirmed), resulting
in an overall ORR of 14% (7/50) based on ITT, and 17% (6/36) for patients in the 10
mg/kg dose group (Table 3). The median time to response was 2.0 months (range, 1.8
to 3.6 months) and the Kaplan-Meier estimated median duration of response was 5.7
months (95% CI: 3.6, 19.9), with 2 responses still ongoing 7.2 and 8.7 months after
starting treatment (Fig. 1B). Twenty-one patients had stable disease (SD) as best
response (21/50, 42%), including 6 patients with >30% tumor reduction at one response
assessment but not maintained on the subsequent CT, and 3 other patients with ≥20%
tumor reduction at one or more response assessments. The Kaplan-Meier estimated
median duration of SD was 5.6 months (95% CI: 5.2, 9.7), including 10 patients with SD
≥4 months, resulting in a clinical benefit rate (CBR: PR+SD≥4 months) of 34% (17/50)
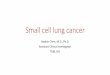
(Table 3). On an ITT basis (N=50), the median PFS and OS were 3.7 months (95% CI:
2.1, 4.3) and 7.5 months (95% CI: 6.2, 8.8), respectively (Table 3, Fig. 2). Interestingly,
the median PFS for the 10 patients with SD ≥4 months was close to that obtained by the
7 PR patients (5.6 vs 7.9 months, respectively), and the median OS was also
comparable (8.3 vs 9.2 months, respectively).
Of 4 patients who received prior treatment with an immune checkpoint inhibitor
(CPI) and had CT-assessable responses, one progressed, but the other 3 achieved
stable disease, including one patient with 54% tumor reduction at first assessment who
withdrew consent without additional treatment or assessments, one who achieved 17%
tumor shrinkage lasting 8.7 months, and a third whose tumor size remained unchanged
for 3.7 months.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

12
Table 3 summarizes other subgroups from the 43 CT-assessable patients. For
example, there was no substantial difference in ORR, PFS or OS between those
patients who were chemosensitive vs chemoresistant to their frontline platinum-based
chemotherapy, but the CBR was 50% and 26%, respectively, when all patients given
sacituzumab govitecan in different therapy lines were analyzed. However, when studied
in second-line in a small subgroup, there was a suggestion of improved outcome in PR,
CBR, and PFS for frontline chemosensitive vs chemoresistant patients. There was no
substantial difference in these metrics for those treated in this study in the 2nd- vs 3rd-
line or higher setting. Interestingly there was a statistically significant higher OS with
other response metrics compared in a small subset of patients who received prior
topoisomerase-I inhibitor therapy vs no such prior therapy.
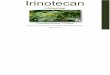
Significant tumor reduction in a patient given sacituzumab govitecan after
relapsing to frontline carboplatin plus etoposide therapy is presented in Fig. 3, showing
shrinkage of the adrenal metastasis by CT and 2+ Trop-2 staining of the SCLC archival
specimen by IHC. Another example with considerable tumor reduction is given in
Supplementary Fig. S1.
Immunohistochemical Staining of Tumor Specimens
Archival tumor specimens were obtained from 29 patients, but four were
inadequate for review, leaving 25 assessable tumors, of which 92% were positive, with
two (8%) having strong (3+) and thirteen (52%) moderate (2+) staining. Twenty-three of
these 25 patients had an objective response assessment. Five patients had PR as their
best response, four with 2+ staining, while the other was 1+ (Supplementary Table
S1). An analysis of PFS and OS vs IHC score showed no clear relationship
(Supplementary Fig. S2 A and B), with Kaplan-Meier estimates for PFS and OS for
patients with IHC scores of 0 and 1+ combined (N = 10) vs 2+ and 3+ combined (N =
13), indicating no significant differences (PFS, P = 0.27; OS, P = 0.72) based on IHC
score (Supplementary Fig. S2C and D).
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

13
Immunogenicity of ADC, SN-38, or hRS7 Antibody
No neutralizing antibodies to sacituzumab govitecan, the antibody, or SN-38
were detected in patients who maintained treatment for even up to 22 months.
Discussion
The relapse of SCLC to frontline chemotherapy continues to be divided into two
categories, resistant relapse, occurring within three months of the first platinum-based
therapy, and sensitive relapse, which occurs after at least 3 months post treatment (5,
6, 22, 23). Although there is still some ambiguity regarding the best management of
recurrent SCLC, topotecan, a topoisomerase-I inhibitor similar to the SN-38 used in the
ADC studied here, is the only product approved for 2nd-line chemosensitive relapse in
the USA, as supported by numerous trials (7-9). However, the efficacy and adverse
events of topotecan have varied considerably in prior studies, as demonstrated in a
meta-analysis of over a thousand patients contained in 14 articles, reporting that
topotecan had an objective response rate of 5% in chemoresistant frontline patients and
17% in chemosensitive patients (15). This review found grade >3 neutropenia,
thrombocytopenia, and anemia in 69%, 1%, and 24% of patients, respectively;
approximately 2% of patients died from this chemotherapy (15). Thus, topotecan shows
some promise in this second-line setting in patients who relapsed after showing
sensitivity to a platinum-based chemotherapy, but with considerable hematological
toxicity. However, even this conclusion was challenged recently by Lara et al. (30),
asserting that platinum-sensitivity is not strongly associated with improved PFS and OS
following treatment with topotecan, which is its currently-approved indication.
It is in this setting that the results reported here with sacituzumab govitecan in
advanced-disease patients (stage IV) following a median of 2 (range, 1 to 7) prior
therapies are promising. Sixty percent of the 43 CT-assessable patients showed a
reduction of tumor measurements from baseline, according to RECIST 1.1, with an ITT-
based ORR of 14% (7/50) and a median duration of response of 5.7 months (95% CI:
3.6, 19.9). Stable disease was found in 42% of patients, where 12% of these SD
patients had >30% tumor shrinkage as best response, although not confirmed on the
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

14
second scan. The clinical benefit rate at >4 months was 34% (17/50). Median PFS and
OS were 3.7 and 7.5 months, respectively. It is interesting that the median OS for the
ten patients with SD ≥4 months was 8.3 months (95% CI: 7.5, 22.4), which is not
statistically different from the median OS of 9.2 months (95% CI: 6.2, 20.9) for patients
with a PR (P=0.56).
In the group receiving 10 mg/kg as their starting dose (N = 36), there was a
confirmed objective response in six (17%), with an additional five patients having a
single CT showing >30% tumor reduction. Also, the clinical benefit rate for this group at
the 10 mg/kg dose was 39%. This supports the preferred dose of 10 mg/kg also found
in other cancer types treated with this ADC (22, 24). Noteworthy also is the lack of
patient selection based on immunohistochemical staining of tumor Trop-2, although
there may be a suggestion that stronger staining correlated with better response, but no
significant difference in PFS or OS was found with regard to IHC score (Fig. S2).
Clearly, more studies correlating tumor expression of Trop-2 and clinical outcome are
needed.
As mentioned, PFS and OS did not differ substantially between patients with SD
>4 months or PR. Patients with >30% tumor reduction on one CT or with SD generally
are not considered in ORR assessments. However, the results here indicate no
difference in duration of response between patients with confirmed PR or SD lasting for
more than 4 months (Fig. 1B). Indeed, the dynamic tracking of the individual patient
responses for PR or SD (especially when the SD last ≥4 months, which is a similar time
frame for confirming PR) suggests a clinical benefit for both groups by remaining below
the baseline tumor size for several months (Fig. 1C). Although there was a trend for the
PFS of patients with confirmed PR to be longer than the group of patients with SD
lasting ≥4 months (P = 0.16), the OS for these 2 groups was not significantly different (P
= 0.56). Therefore, while the number of patients in this initial analysis is relatively small,
the data suggest that more consideration should be given to disease stabilization as an
important indicator of clinical activity when an appropriate duration is achieved. This is
consistent with a report of SCLC patients enrolled into phase II trials by the Southwest
Oncology Group, showing that disease control rate at 8 weeks is a better predictor of
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

15
subsequent survival than RECIST tumor response findings (31). Cesano et al. also
emphasized that disease stabilization is a useful predictor of survival following second-
line chemotherapy in SCLC patients (32).
Evaluating patients with a CT assessment of response based on prior platinum-
regimen chemosensitivity (N = 24) or chemoresistance (N = 19) showed no response
differences with sacituzumab govitecan treatment; ORR was 17% and 16%,
respectively (Table 3), for the entire study population. PFS and OS results were 3.8 and
8.3 months for patients who were chemosensitive in frontline, compared to a PFS and
OS of 3.6 months and 6.2 months, respectively, for the chemoresistant group. In a small
population of patients given sacituzumab in second-line, however, evidence of improved
results in those who were chemosensitive to frontline therapy is suggested (Table 3),
but these results need to be confirmed in a larger study. If confirmed, this would differ
from topotecan, which is indicated in the USA only in those SCLC patients who showed
a >3-month response to frontline cisplatin and etoposide chemotherapy (6, 12, 22, 23).
Although both topotecan and SN-38 are inhibitors of the DNA topoisomerase I
enzyme, which is responsible for relaxing a supercoiled DNA helix when DNA is
synthesized by stabilizing the DNA complex and causing accumulation of single strand
DNA breaks (33), sacituzumab govitecan showed activity in a small group of patients
who relapsed after topotecan therapy (7/15 showed target lesion shrinkage, with 2 PR).
Thus, if corroborated in future trials, topotecan resistance or relapse may not be a
contraindication for administering sacituzumab govitecan, and because of being
similarly active in patients who were chemoresistant to cisplatin and etoposide (ORR of
16%), may be of particular value as a second-line therapeutic in patients with metastatic
SCLC regardless of chemosensitivity status.
In the twenty years since the approval of topotecan in the second-line setting, no
new agent has been licensed for metastatic SCLC therapy in second-line or later
therapy in the USA and Europe. However, there has been progress more recently with
inhibitors of the T-cell checkpoint receptors programmed cell-death protein (PD-1) and
cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) (34). Antonia et al. conducted a
phase I-II trial of nivolumab with or without CTLA-4 antibody ipilimumab in patients with
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

16
recurrent SCLC. Nivolumab alone achieved a 10% response rate, while the combination
had response rates of 19 to 23%, and a disease-control rate of 32% (34). However, a
recent study of ipilimumab with or without chemotherapy in SCLC failed to confirm an
advantage of combining this anti-CTLA4 antibody with chemotherapy (35). Since we
observed that sacituzumab govitecan may have activity in patients whose cancer has
progressed on therapy with immune checkpoint inhibitors, we are studying this further,
especially because of evidence showing such responses after relapse or
unresponsiveness to therapy with an immune checkpoint inhibitor in patients with other
cancer types (26, 27, 36, 37).
Despite recent progress in immunotherapy, this still is a lethal disease, especially
in the population that is chemoresistant to first-line therapy. The current results of
sacituzumab govitecan in heavily-pretreated patients with advanced, relapsed, stage IV,
SCLC, despite the limitations of a one-arm trial, suggest that this ADC may gain a role
in the therapy of both chemosensitive and chemoresistant SCLC patients, both before
or after topotecan, and thus needs to be studied further in such settings. It is
encouraging that another ADC, rovalpituzumab tesirine, an investigational DLL3-
targeting conjugate, also has shown activity in recurrent SCLC (38).
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

17
Disclosure of Potential Conflicts of Interest
D.M. Goldenberg has stock (including patents) in Immunomedics, Inc., and is a
Board member. S.V. Govindan, P, Maliakal, B. Mudenda, W.A. Wegener, and R.M.
Sharkey are employees of Immunomedics, Inc., with stock options.
Authors’ Contributions
Conception and design: A.N. Starodub, D.R. Camidge, W.A. Wegener, D.M.
Goldenberg
Development of methodology: S.V. Govindan, P. Maliakal, W.A. Wegener
Acquisition of data (acquired and managed patients, provided facilities, etc.): J.E. Gray,
R.S. Heist, A.N. Starodub, D.R. Camidge, E. Kio, G. Masters, W.T. Purcell, M.J.
Guarino, J. Misleh, C.J. Schneider, B.J. Schneider, A.J. Ocean, T. Johnson, L. Gandhi,
K. Kalinsky, R.J. Scheff, W.A. Messersmith
Analysis and interpretation of data (e.g., statistical analysis, biostatistics, computational
analysis): P. Maliakal, B. Mudenda, W.A. Wegener, R.M. Sharkey, J.E. Gray, R.S.
Heist, K. Kalinsky, A.N. Starodub, D.R. Camidge
Writing, review, and/or revision of the manuscript: All authors
Administrative, technical, or material support (i.e., reporting or organizing data,
constructing databases): P. Maliakal, B. Mudenda, W.A. Wegener, R.M. Sharkey
Study supervision: D.M. Goldenberg
Acknowledgments
We thank the patients and their families for participating, the clinical support
staffs at the investigational sites, and Heather Horne and the data management team at
Immunomedics for their contributions.
Funding
This study was supported by Immunomedics, Inc.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

18
References
1. Alvarado-Luna G, Morales-Espinosa D. Treatment for small cell lung cancer,
where are we now? A review. Transl Lung Cancer Res 2016;5:26-38.
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin
2017;67:7-30.
3. Fruh M, De Ruysscher D, Popat S, Crino L, Peters S, Felip E. Small-cell lung
cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-
up. Ann Oncol 2013;24 Suppl 6:vi99-105.
4. Hurwitz JL, McCoy F, Scullin P, Fennell DA. New advances in the second-line
treatment of small cell lung cancer. Oncologist 2009;14:986-94.
5. Schneider BJ. Management of recurrent small cell lung cancer. J Natl Compr
Canc Netw 2008;6:323-31.
6. Cheng S, Evans WK, Stys-Norman D, Shepherd FA. Chemotherapy for relapsed
small cell lung cancer: a systematic review and practice guideline. J Thorac Oncol
2007;2:348-54.
7. O'Brien ME, Ciuleanu TE, Tsekov H, Shparyk Y, Cucevia B, Juhasz G, et al.
Phase III trial comparing supportive care alone with supportive care with oral topotecan
in patients with relapsed small-cell lung cancer. J Clin Oncol 2006;24:5441-7.
8. Perez-Soler R, Glisson BS, Lee JS, Fossella FV, Murphy WK, Shin DM, et al.
Treatment of patients with small-cell lung cancer refractory to etoposide and cisplatin
with the topoisomerase I poison topotecan. J Clin Oncol 1996;14:2785-90.
9. von Pawel J, Schiller JH, Shepherd FA, Fields SZ, Kleisbauer JP, Chrysson NG,
et al. Topotecan versus cyclophosphamide, doxorubicin, and vincristine for the
treatment of recurrent small-cell lung cancer. J Clin Oncol 1999;17:658-67.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

19
10. Furuse K, Kubota K, Kawahara M, Takada M, Kimura I, Fujii M, et al. Phase II
study of vinorelbine in heavily previously treated small cell lung cancer. Japan Lung
Cancer Vinorelbine Study Group. Oncology 1996;53:169-72.
11. Smit EF, Fokkema E, Biesma B, Groen HJ, Snoek W, Postmus PE. A phase II
study of paclitaxel in heavily pretreated patients with small-cell lung cancer. Br J Cancer
1998;77:347-51.
12. Sandler AB. Irinotecan in small-cell lung cancer: the US experience. Oncology
(Williston Park) 2001;15:11-2.
13. van der Lee I, Smit EF, van Putten JW, Groen HJ, Schlosser NJ, Postmus PE, et
al. Single-agent gemcitabine in patients with resistant small-cell lung cancer. Ann Oncol
2001;12:557-61.
14. Jalal S, Ansari R, Govindan R, Bhatia S, Bruetman D, Fisher W, et al.
Pemetrexed in second line and beyond small cell lung cancer: a Hoosier Oncology
Group phase II study. J Thorac Oncol 2009;4:93-6.
15. Horita N, Yamamoto M, Sato T, Tsukahara T, Nagakura H, Tashiro K, et al.
Topotecan for relapsed small-cell lung cancer: systematic review and meta-analysis of
1347 patients. Sci Rep 2015;5:15437.
16. Hagmann R, Hess V, Zippelius A, Rothschild SI. Second-line therapy of small-
cell lung cancer: topotecan compared to a combination treatment with adriamycin,
cyclophosphamide and vincristine (ACO) - a single center experience. J Cancer
2015;6:1148-54.
17. Hasegawa Y, Takeda K, Kashii T, Kawano Y, Katayama H, Sumitani M, et al.
Clinical experiences of Amrubicin hydrochloride (Calsed) monotherapy in previously
treated patients with small-cell lung cancer. Jpn J Lung Cancer 2005;45:811-5.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

20
18. Inoue A, Sugawara S, Yamazaki K, Maemondo M, Suzuki T, Gomi K, et al.
Randomized phase II trial comparing amrubicin with topotecan in patients with
previously treated small-cell lung cancer: North Japan Lung Cancer Study Group Trial
0402. J Clin Oncol 2008;26:5401-6.
19. Hirose T, Nakashima M, Shirai T, Kusumoto S, Sugiyama T, Yamaoka T, et al.
Phase II trial of amrubicin and carboplatin in patients with sensitive or refractory
relapsed small-cell lung cancer. Lung Cancer 2011;73:345-50.
20. von Pawel J, Jotte R, Spigel DR, O'Brien ME, Socinski MA, Mezger J, et al.
Randomized phase III trial of amrubicin versus topotecan as second-line treatment for
patients with small-cell lung cancer. J Clin Oncol 2014;32:4012-9.
21. Goldenberg DM, Cardillo TM, Govindan SV, Rossi EA, Sharkey RM. Trop-2 is a
novel target for solid cancer therapy with sacituzumab govitecan (IMMU-132), an
antibody-drug conjugate (ADC). Oncotarget 2015;6:22496-512.
22. Lara PN, Jr., Natale R, Crowley J, Lenz HJ, Redman MW, Carleton JE, et al.
Phase III trial of irinotecan/cisplatin compared with etoposide/cisplatin in extensive-
stage small-cell lung cancer: clinical and pharmacogenomic results from SWOG S0124.
J Clin Oncol 2009;27:2530-5.
23. Zatloukal P, Cardenal F, Szczesna A, Gorbunova V, Moiseyenko V, Zhang X, et
al. A multicenter international randomized phase III study comparing cisplatin in
combination with irinotecan or etoposide in previously untreated small-cell lung cancer
patients with extensive disease. Ann Oncol 2010;21:1810-6.
24. Sharkey RM, McBride WJ, Cardillo TM, Govindan SV, Wang Y, Rossi EA, et al.
Enhanced delivery of SN-38 to human tumor xenografts with an anti-Trop-2-SN-38
antibody conjugate (sacituzumab govitecan). Clin Cancer Res 2015;21:5131-8.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

21
25. Starodub AN, Ocean AJ, Shah MA, Guarino MJ, Picozzi VJ, Jr., Vahdat LT, et al.
First-in-human trial of a novel anti-Trop-2 antibody-SN-38 conjugate, sacituzumab
govitecan, for the treatment of diverse metastatic solid tumors. Clin Cancer Res
2015;21:3870-8.
26. Bardia A, Mayer IA, Diamond JR, Moroose RL, Isakoff SJ, Starodub AN, et al.
Efficacy and safety of anti-Trop-2 antibody-drug conjugate, sacituzumab govitecan
(IMMU-132), in heavily pretreated patients with metastatic triple-negative breast cancer.
J Clin Oncol 2017;Epub ahead of print. March 13, 2017.
27. Faltas B, Goldenberg DM, Ocean AJ, Govindan SV, Wilhelm F, Sharkey RM, et
al. Sacituzumab govitecan, a novel antibody-drug conjugate, in patients with metastatic
platinum-resistant urothelial carcinoma. Clin Genitourin Cancer 2016;14:e75-9.
28. Heist RS, Guarino MJ, Masters G, Purcell WT, Starodub AN, Horn L, et al.
Therapy of advanced non-small-cell lung cancer with an SN-38-anti-Trop-2 drug
conjugate, sacituzumab govitecan. J Clin Oncol 2017;EPub ahead of print:May 26.
29. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al.
New response evaluation criteria in solid tumours: revised RECIST guideline (version
1.1). Eur J Cancer 2009;45:228-47.
30. Lara PN, Jr., Moon J, Redman MW, Semrad TJ, Kelly K, Allen JW, et al.
Relevance of platinum-sensitivity status in relapsed/refractory extensive-stage small-cell
lung cancer in the modern era: a patient-level analysis of Southwest Oncology Group
Trials. J Thorac Oncol 2015;10:110-5.
31. Lara PN, Jr., Moon J, Redman MW, Semrad TJ, Kelly K, Allen J, et al. Disease
control rate at 8 weeks predicts subsequent survival in platinum-treated extensive stage
small-cell lung cancer: Results from the Southwest Oncology Group (SWOG) database.
Clin Lung Cancer 2016;17:113-8.e1-2.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

22
32. Cesano A, Lane SR, Poulin R, Ross G, Fields SZ. Stabilization of disease as a
useful predictor of survival following second-line chemotherapy in small cell lung cancer
and ovarian cancer patients. Int J Oncol 1999;15:1233-8.
33. Takimoto CH, Arbuck SG. Camptothecins. In: Chabner BA, Long DL, editors.
Cancer Chemotherapy and Biotherapy. Second ed. Philadelphia: Lippincott-Raven;
1966. p. 463-84.
34. Antonia SJ, Lopez-Martin JA, Bendell J, Ott PA, Taylor M, Eder JP, et al.
Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer
(CheckMate 032): a multicentre, open-label, phase 1/2 trial. Lancet Oncol 2016;17:883-
95.
35. Reck M, Luft A, Szczesna A, Havel L, Kim SW, Akerley W, et al. Phase III
randomized trial of ipilimumab plus etoposide and platinum versus placebo plus
etoposide and platinum in extensive-stage small-cell lung cancer. J Clin Oncol 2016.
36. Heist RS, Guarino MJ, Masters G, Purcell T, Starodub AN, Horn L, et al. Therapy
of advanced non-small cell lung cancer with an SN-39-anti-Trop-2 drug conjugate,
sacituzumab govitecan (IMMU-132). J Clin Oncol 2017;in press.
37. Tagawa ST, Ocean AJ, Lam E, Saylor P, Bardia A, Hajdenberg JJ, et al. Therapy
for chemo-pretreated metastatic urothelial cancer (mUC) with antibody-drug conjugate
(ADC), sacituzumab govitecan (IMMU-132). J Clin Oncol 2017;35:abstract 327.
38. Rudin CM, Pietanza MC, Bauer TM, Ready N, Morgensztern D, Glisson BS, et
al. Rovalpituzumab tesirine, a DLL3-targeted antibody-drug conjugate, in recurrent
small-cell lung cancer: a first-in-human, first-in-class, open-label, phase 1 study. Lancet
Oncol 2017;18:42-51.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

23
Table 1. Baseline demographics and disease characteristics (N = 53)
Age Years (median; range) 63 (44 - 82)
Gender, N (%) Female 30 (56) Male 23 (44)
Race, N (%) White 47(88) Black 3 (6) Other 3 (6)
ECOG, N (%) 0 6 (11) 1 47(89)
Sites of metastases, N (%) Lung 35 (66) Liver 31 (59) Lymph nodes 40 (76) Chest 18 (34) Adrenals 13 (25) Bone 12 (23) Pleural effusion 3 (6) Pancreas 4 (7) Pelvis 2 (4) Brain 2 (4) Skin 2 (4) Others 3 (6)
Prior Lines of Therapy, N (%) 1 22 (42) 2 14 (26) ≥3 17 (32)
Sensitivity to 1st -line chemotherapy, N (%) Sensitive 27 (51) Resistant 26 (49)
Prior Therapy, N (%) Platinum and Etoposide 53 (100) Topotecan and/or
Irinotecan 18 (34)
Taxanes 9 (17) Checkpoint inhibitors (CPI) 5 (9)
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

24
Table 2. Adverse events (N=53)*
All Grades Grades 3 and 4
N % N %
Diarrhea 28 53 5 9
Nausea 27 51 - -
Fatigue 25 47 7 13
Neutropenia 23 43 18 34
Vomiting 18 34 - -
Abdominal pain 16 30 - -
Anorexia 15 28 - -
Anemia 14 26 3 6
Alopecia 12 23 - -
Constipation 11 21 - -
Hypomagnesemia 10 19 - -
Dehydration 9 17 - -
Dyspnea 9 17 - -
Cough 8 15 - -
Hypoxia 3 6 2 4
Febrile neutropenia 1 2 1 2
*Patients with adverse events, regardless of causality, occurring in >15%
(all grades) or ≥2% (grade ≥3) of patients.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

25
Table 3. IMMU-132 response assessment for ITT population (N = 50) or subset analyses in patients who had ≥2 IMMU-132 doses with at least one CT response determination (N = 43)
All patients (N = 50) 10 mg/kg (N = 36) 8 mg/kg (N = 14) Best overall response, N (%) PR 7 (14%) 6 (17%) 1 (7%) SD 21 (42%) 17 (47%) 4 (29%) PD 15 (30%) 7 (19%) 8 (57% IE 7 (14%) 6 (17%) 1 (7%) Duration of response, months, median (95% CI) 5.7 (3.6, 19.9) 4.0 (3.6, 5.7) 19.9 (N = 1) CBR (PR+SD ≥4 months), N (%) 17 (34%) 14 (39%) 3 (21%) PFS, months, median (95%CI) 3.7 (2.1, 4.3) 3.7 (2.8, 5.3) 2.0 (1.7. 3.8) OS, months, median (95% CI 7.5 (6.2, 8.8) 6.2 (5.0, 8.3) 8.1 (7.0, 22.4)
Subgroup analyses Response to Frontline Therapy (all patients) Sensitive (N = 24) Resistant (N = 19)
PR, N (%) 4 (17%) 3 (16%)
CBR (PR+SD ≥4 months), N (%) 12 (50%) 5 (26%)
PFS, months, median (95% CI) 3.8 (2.8, 6.0) 3.6 (1.8, 3.8) NS
OS, months, median (95% CI) 8.3 (7.0, 13.2) 6.2 (4.0, 10.5) NS
Response to Frontline Therapy (IMMU-132 as 2nd line) Sensitive (N = 10) Resistant (N = 9)
PR, N (%) 2 (20%) 1 (11%)
CBR (PR+SD ≥4 months), N (%) 5 (50%) 2 (22%)
PFS, months, median (95% CI) 4.9 (2.8, 7.6) 2.0 (1.8, 3.6) NS
OS, months, median (95% CI) 8.1 (7.5, 10.5) 8.0 (4.0, 10.5) NS
IMMU-132 Line of Therapy Received
2nd Line (N = 19) ≥3 Lines (N = 24)
PR, N (%) 3 (16%) 4 (17%)
CBR (PR+SD ≥4 months), N (%) 7 (37%) 9 (38%)
PFS, months, median (95% CI) 3.6 (2.0, 5.3) 3.7 (1.8, 5.5) NS
OS, months, median (95% CI) 8.1 (7.5, 10.5) 7.0 (6.2, 20.9 NS
≥3 Lines Pts Treated with Prior TPI
Prior TPI (N = 15) No Prior TPI (N = 9)
PR, N (%) 2 (13%) 1 (11%)
CBR (PR+SD ≥4 months), N (%) 6 (40%) 3 (33%) PFS, months, median (95% CI) 3.6 (3.3, 5.5) 3.7 (1.7, 4.3) NS
OS, months, median (95% CI) 8.8 (6.2, 20.9) 5.5 (3.2, 8.3) P = 0.04
Abbreviations: PR, partial response; SD, stable disease; PD, progressive disease; CI, confidence interval. PFS, progression-free survival; OS, overall survival, CBR, clinical benefit rate (PR+SD ≥4 months); TPI, topoisomerase I inhibitors, topotecan and irinotecan; IE, inevaluable; NS, not statistically significant.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

26
Figure Legends
Fig. 1. Graphic representation of anti-tumor response and duration in response-
assessable patients. A. Best percentage change in the sum of the diameters for the
selected target lesion and best overall response descriptor according to RECIST 1.1
criteria. Patients are identified with respect to the sacituzumab govitecan starting dose
and whether they were sensitive or resistant to prior first-line therapy. B. Duration of
response from the start of treatment for those patients who achieved stable disease or
better. Timing when tumor shrinkage achieved ≥30% is shown, along with sacituzumab
govitecan starting dose and sensitivity to first-line therapy. C. Dynamics of response for
patients who achieved stable disease or better. Two patients with confirmed partial
responses who are continuing treatment are shown with dashed line.
Fig. 2. Kaplan-Meier curves for 50 patients (ITT). A: Progression-free survival with 41
patients having progressed, 7 lost to follow-up while progression-free, and 2 currently
continuing progression-free. B: Overall survival with 37 deaths, 8 patients currently
alive, and 5 patients lost to follow-up.
Fig. 3. This 64-year-old male diagnosed with advanced SCLC received carboplatin as
1st line therapy from July 2013 to November 2013, with etoposide added in November
and December 2013. The disease relapsed in May 2014. Prior to starting sacituzumab
govitecan, the tumor lesions at baseline (May 2014) included subcarinal lymph node (20
mm) and right adrenal gland tumors (A: 43 x 34 mm diameter adrenal mass), as well as
multiple unmeasurable lesions in the right and left lobes of the liver, thickening of the
right hilum, a left upper lobe pulmonary nodule, and esophageal thickening. The
response evaluation after 2 months of therapy showed 50% reduction according to
RECIST 1.1 (B, adrenal mass shrinks to 14 mm, subcarinal lymph node shrinks to 17
mm). By the second response assessment, the adrenal mass was no longer visible,
while the subcarinal node experienced its maximum shrinkage ~11 months from the
start of treatment (to 11 mm), yielding maximum shrinkage of 82%. The patient
experienced a 21-month duration of response (July 2014 to March 2016). C.
Immunohistology of a biopsy from the adrenal mass stained for Trop-2 and scored as
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

27
2+, but with sparse distribution among the tumor cells. Arrow shows group of cells with
3+ membrane staining.
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

Figure 1
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

Figure 2
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

Figure 3
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933

Published OnlineFirst July 5, 2017.Clin Cancer Res Jhanelle E. Gray, Rebecca S. Heist, Alexander N Starodub, et al. Targeting Trop-2, Sacituzumab GovitecanTopoisomerase-I-inhibiting Antibody-Drug Conjugate (ADC) Therapy of Small-cell Lung Cancer (SCLC) With a
Updated version
10.1158/1078-0432.CCR-17-0933doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2017/07/04/1078-0432.CCR-17-0933.DC1
Access the most recent supplemental material at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/early/2017/07/04/1078-0432.CCR-17-0933To request permission to re-use all or part of this article, use this link
Research. on February 16, 2021. © 2017 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on July 5, 2017; DOI: 10.1158/1078-0432.CCR-17-0933