Embed Size (px)
Citation preview

The Way of the Future Redux Donald F. Fortin, MD, Robert M. Califf, MD, David B. Pryor, MD,
and Daniel B. Mark, MD, MPH
M edical practice is undergoing perhaps its most dramatic change of this century. A revolution in
the prevailing medical paradigm driven largely by pay- ors and large insurers is resulting in an aggressive chal- lenge to the value of complex, high-technology medical care and the specialists who use such care.l At the same time, government and industry investment in biotech- nology is fueling an explosion in the development of complex new therapies with expanded possibilities of patient benefit.2 As the health care system struggles to adapt to the constraints of capitated payments and man- aged care, it will be oriented toward vertical integration with a focus on primary care.3 In this environment we believe that the preservation of high-quality care for patients with complex diseases will be critically depen- dent on having access to information that defines the val- ue of medical technology and identifies areas in which generalists or specialists should provide ongoing care. This era has arrived more than 20 years after it was ini- tially predicted by the founders of our group.4 Because of its prominence in terms of quantifiable outcomes and cost, cardiovascular medicine is at the forefront of this revolution.
Whereas medicine has recently experienced a quan- tum leap in access to information technologies, the med- ical profession continues to lag far behind the business community in the collection and use of information. Over 20 years ago, the stated goal of the Duke Databank for Cardiovascular Disease was to create a resource to support daily clinical practice so that “no clinical deci- sions will be made on the care of any patient with coro- nary artery disease, myocardial infarction, or heart block until the data bank has been searched and outcomes of patients with the same descriptors as the new patient have been given to the physician. When Duke Medical Center can immediately bring to bear all its experience on each cardiovascular patient entering its doors, it will have a clear lead over all other physicians.“4 Our tenet is that unless cardiology can achieve the goal delineat- ed above, in an era in which the domain of the cardio- vascular specialist (and other specialists) will be increas- ingly circumscribed by default, patients will be deprived of significant opportunities for improved outcomes be- cause a rational basis will not be available for deter- mining when and how specialty care can produce ben- efit.
From the Duke Databank for Cardiovascular Disease, Division of Car- diology, Duke University Medical Center, Durham, North Carolina. Manuscript received and accepted Au ust 10, 1995.
Address for reprints: Robert M. Ca iff, 9 MD, Duke Databank for
Cardiovascular Disease, 2024 West Main Street, Bay A-108, Durham, North Carolina 27705.
WHERE WE CAME FROM Acute myocardial infarction was the first medical
problem for which a dedicated patient care unit (coro- nary care unit) was established at Duke University Med- ical Center. Reviews of medical records of coronary care unit patients demonstrated that physicians consistently remembered only their most recent patients, had no access to the experiences of other doctors and patients, and often had difficulty assimilating the significance of complex patient characteristics over time. This experi- ence led to the initial recognition of the limitations of physician personal experience and recollection as a guide for future management decisions. The Duke Databank for Cardiovascular Disease was begun in 1969 with the goal of putting computers to work on this problem. This computerized database was envisioned as a tool that would permit the physician to “use all of his experience to care for the patient, not just the portion of his expe- rience that he can remember.“4 However, the database that emerged was procedure oriented, with patients entering the system at the time of diagnostic catheteri- zation or coronary bypass surgery. We now recognize that this pragmatic orientation was not ideal, given that coronary atherosclerosis is a chronic disease of the arte- rial wall with short periods of escalating signs and/or symptoms (often requiring procedures) and long periods of quiescence. Our focus on studying and managing the procedures distracted us from concentrating on manag- ing the lifetime problem of controlling and coexisting with coronary artery disease.
Although the Duke Databank has become part of the institutional fabric at our medical center, its original goal of providing the practicing clinician with useful infor- mation about the institutional experience with each type of patient has never been fully realized. In the 1970s because of the shortcomings of available clinical trials, the Databank was used primarily to conduct observa- tional treatment comparisons5-7 that formed the basis of institutional practice patterns, In the 198Os, the system expanded to incorporate information about noninvasive testing,8-10 and observational treatment comparisons were extended to include coronary angioplasty.” Throughout its lifetime, the database has served as a tool to allow quantification of procedural information for administra- tive and research purposes and it has fundamentally changed the nature of our practice,5 but it has been large- ly unsuccessful in its effort to support and enhance clin- ical decision-making in real time.
The failure to realize the original goals of the Data- bank is not solely the fault of its caretakers. Early gen- erations of the database had to cope with 4 technologic limitations (unwieldy operating systems, crude database software, difficult computer communications, and expen- sive hardware), 3 social ones (a physician community
EDITORIALS 1 177

that was blissfully ignorant of computer-related matters, concerns about the security of confidential patient infor- mation amassed in computerized medical databases, and a health care system that had no recognition of the val- ue of such a white elephant), and analytic insufficiency (poorly understood methods for analyzing aggregated information).
Computer hardware and software have made quan- tum improvements in the last decade and enhancements continue at a breathtaking pace. 12,r3 What was once pos- sible only with a room-sized mainframe computer can now be accomplished much more efficiently (and quick- ly) by a workstation that fits comfortably atop a desk and has a price that is comparably reduced. Computer-oper- ating systems (the software interface between the com- puter “brain” or microprocessor and the user) have pro- gressed from arcane frustrating programs that only a computer expert could fully exploit to simple graphic interfaces that require little training (and no program- ming knowledge) to use effectively.
An equally important technical development has been that of the local area network (LAN). Before develop- ment of LANs, it was very difficult to get one comput- er to “talk” to another one. The LAN technology links personal computers and workstations transparently, there- by permitting access to a wealth of desired information (clinical, laboratory, administrative) from multiple geo- graphically dispersed locations (such as the hospital unit, the physician’s office, the outpatient clinic, and even the physician’s home).
The most recent technologic advance has been the ascendancy of client-server type data management sys- tems that allow huge quantities of information to be sort- ed and processed at specialized servers (large capacity workstations running relational database software), while permitting clients (or end users) to access any portion of the database from a remote, inexpensive (yet powerful) microcomputer. These advances in computer hardware and software have now created the technologic substrate necessary for the fulfillment of the Duke Databank’s original mission.
The social obstacles to implementation of this mis- sion have also been substantially reduced. Entire gener- ations of new physicians who grew up using computers are now entering the practice of medicine. In the mean- time, many older physicians have acquired a personal computer for home or office use. In short, the ascendant role of computers in society at large has brought the med- ical profession to a point where it is now willing and able to use computers to assist in clinical practice.
A major unresolved social problem is growing con- cern about the security of computerized medical records. Although paper records are easy to abuse individually, they cannot be manipulated in aggregate without tremen- dous difficulty and expense. Electronic records can be much more easily mishandled on a large scale, making the construction of stiff security measures an imperative for computerized databases.14 These measures can lim- it access to specific data elements and prohibit the aggre- gation of large data sets without the specific informed consent of the patients and providers contributing their information to the data repositories. Whereas such mea-
sures represent an important first step, a number of issues may have to be settled legislatively, including the estab- lishment of a code of health information that properly balances patient privacy with disclosure and use of data, and the imposition of penalties for violation of the code. This problem of security and unauthorized access to computerized information is a major problem for soci- ety in general and will require constant surveillance.
Major financially motivated challenges to the tech- nologic focus of medicine have produced immense pres- sure to demonstrate the value of cardiovascular medi- cine, and consequently have stimulated tremendous system-wide interest in computerized information. Until recently, the development of an information infrastruc- ture for the practice of medicine was considered by most clinicians to be too expensive with unclear rewards. As a result, the only universal information about medical practice comes from databases of medical billing infor- mation. The content of these databases is defined by pay- ors, and they therefore contain inadequate information about the medical status of the patient.15 Analyses of these data to answer clinical questions are accompanied by the potential for huge analytic uncertainty because the severity of illness of the patient cannot be adjusted for adequately. Without the ability to link basic infor- mation about patient characteristics and clinical man: agement with outcomes, practitioners and hospitals will experience a financial “implosion”: the inability to demonstrate the value of services provided through rel- evant and accurate information will lead to immense pressure from payors and administrators to do less (i.e., the problem of confusing evidence of no benefit with no evidence one way or another). We believe that recog- nizing this need will push the practitioner to view the computer as an indispensable tool in clinical practice.
The opportunities and problems created by the abil- ity to repeatedly analyze aggregated data are a by-prod- uct of the widespread availability of tremendous com- puter power. The randomized trial is a relatively new evaluative tool that has found widespread applicability in clinical medicine. The use of powerful statistical tech- niques to adjust for or “subtract out” baseline differences due to treatment selection biases when randomization has not been employed is an even newer, more complex and less well understood area of clinical biostatistics and epidemiology. Despite their limitations and frequent abuse,i6-i* these methods can now be used to compare outcomes among providers of health care19-21 and to assess the feasibility and likely outcomes of changes in the health care system. 22,23 An increasing number of training programs have been initiated to allow a broad- er segment of the medical profession to understand and use these. methods. The immense power of data collec- tion, storage, and retrieval made possible by the current generations of computer hardware and software cannot be appropriately capitalized upon without proper ana- lytic methods.
WHAT DO DATABASES OFFER IN CURRENT CARDIOVASCULAR PRACTICE?
One of the main reasons for creating a database for a cardiology practice is ‘to standardize the manner in
1178 THE AMERICAN JOURNAL OF CARDIOLOGYe VOL. 76 DECEMBER 1, 1995

which patient information is compiled, so that the obser- vations of one practitioner can be readily accessed and understood by another. Traditional medical records per- mit considerable variation in the observations that are recorded and the vocabulary physicians use, and they also encourage unstructured (free text) observations and conclusions. One physician’s terminology for a particu- lar entity or result often does not match another physi- cian’s understanding of the same terms. The computer- based medical record allows much less variation in terminology and diverts free text to appropriate subjec- tive portions of the record. Thus, computerized records can be more consistent and comprehensive than the tra- ditional paper medical record.
A cardiology database can be used to collect such routine data as patient demographics, risk factors, and results of history/physical examination. It can also com- pile procedural details including the patient’s status before and after a procedure, the anatomic and functional results of the procedure, and the personnel and equip- ment involved. By including data about complications during in-hospital and long-term follow-up, complete profiles about patients being cared for can be developed. Although the paper medical record has been used for this purpose, it is impractical to maintain an up-to-date copy of the record in multiple places (e.g., hospital, clin- ic), leading to both redundancy and incompleteness. In this area, the computerized record has clear advantages. However, the technology to take full advantage of the superior format of electronic records is relatively recent and is still evolving.
The level of detail contained in the database will determine not only its utility, but also the number of per- sonnel needed to manage it and, ultimately, its cost. Ear- ly generations of the database should focus on a parsi- monious set of key data elements. As secure funding becomes available, the database can be expanded to include the collection of data that is desirable but not essential. The challenge at each stage in the process is to meet the needs of users without allowing-the process to become unwieldy. After the basic database is in place, the first level of expansion might target detailed infor- mation about physicians in the community who refer pa- tients to the group; keeping these practitioners apprised of the status of their patients as well as of the introduc- tion of new procedures and technologies for which their patients may be eligible is an important component of a successful referral cardiology program. Another useful application is to link the cardiology database with the hospital’s information system. Making data about the procedures performed available to the hospital’s finan- cial office can help streamline the billing process and shorten the time to reimbursement. Procedural results and complications recorded in the database can be trans- mitted to the hospital’s quality assurance office, thereby helping to streamline the recredentialing process and to flag quality problems at an early stage.
One major \ motivation for integrating clinical and financial data is to permit appropriate and insightful analyses of the true costs to a hospital or provider sys- tem of caring for a given type of patient. Currently, most comparisons of clinical competence and financial effi-
ciency involve patient subgroups defined by administra- tive codes such as the diagnosis-related groups (DRG) system. Procedural DRGs typically include patients with varying demographics, clinical presentation (e.g., unsta- ble angina, acute myocardial infarction, stable angina), and unquantified comorbid illness who are lumped together because they are treated with the same proce- dure (e.g., percutaneous revascularization, DRG 112). Thus, comparing practitioners, practices, or hospitals on the basis of DRGs has obvious inadequacies, since the expected outcomes and expenditures vary importantly as a function of the severity of illness and comorbidity of the patient. To “level the playing field” for these com- parisons, sophisticated information systems with appro- priate clinical data must be linked with financial systems.
On the surface, having a practitioner enter data into a computerized record at the time of patient contact may appear inefficient and not worth the effort required. In light of the need to interface these data geographically, across time and within larger health systems, however, such practitioner commitment may be thought of as the tip of the iceberg. Beneath the incremental work required of the clinician at the time of patient contact (which replaces the dictated record most practitioners currently use) is a huge amount of work that must be done with the resulting data to produce evidence of quality and effi- ciency. Without a computerized record, this work is dif- ficult and time-consuming, and currently is not done in a fashion that emphasizes the full advantages and com- plexities of modem cardiovascular care. Once data have been entered as part of the patient care process, howev- er, these “below the surface” functions become expo- nentially more efficient, resulting in a substantially more powerful system at a competitive cost.
THE FUTURE The shift from cost-based reimbursement to managed
care has produced strong incentives for insurers and providers to develop vertically integrated health care sys- tems that cover the broad range of medical needs of a population. In vertically integrated health systems, em- phasis is shifted from the outcomes of specific proce- dures to the larger issue of the effectiveness of the sys- tem in providing the best health outcomes for the patient with identified heart disease over a period of years. A cardiology database that meets the needs of this type of health care structure must cover inpatient and outpatient care as well as diagnostic testing. Inpatients visit a vari- ety of highly specialized areas within a hospital in a short period of time; each area could benefit from immediate and sometimes simultaneous access to the medical record, which is impossible with the traditional paper record. Over a period of years, the patient with clinical- ly manifest ischemic heart disease will visit a variety of practitioners, have a number of diagnostic tests, and face a number of therapeutic decisions that offer the oppor- tunity for improving prognosis or quality of life. These medical encounters will typically occur in a geographi- cally and temporally dispersed manner.
In the idealized future practice of cardiovascular medicine, practitioners will be linked via computerized records that comprehensively account for patient char-
EDITORIALS 1179

acteristics, test results, therapies, and outcomes. Infor- mation will be collected at the point of care and will include not only the traditional medical record data, but also key images (e.g., angiograms, echocardiograms) and other relevant information. The practitioner per- forming diagnostic testing .will have immediate access to information about the patient’s history while the physician in the office or on the inpatient unit will be able to view the images from diagnostic testing direct- ly, even when they are obtained remotely. This electron- ic repository of information will be accessed via the physician’s workstation, which could physically be lo- cated at any place within reach of a telephone line.
The electronic medical record will form the basis for assessing current practice and developing new practices by the individual practitioner, the practice group, and the health care system. Once the investment has been made in the initial information infrastructure, a tremendous savings will be possible due to reduced need for per-
Hypothetical Surgical Scorecard
Practice A Practice 0
1 2 3
Years
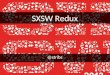
FIGURE 1. Ana ‘r
sis of operative mortality statistics and empiri- cal marginal va ue curves for 2 hypothetical practices. Practice A selects low-risk patients for operation with a predicted oper- ative mortality of :2%. Observed mortality is lower than pre- dicted, indicating that the technical performance of surgery is excellent in
s ractice A. Practice B selects higher-risk patients for
gphan their observed operative mortality is somewhat an predicted [A]. By these commonly used standards,
the surgery in practice A is superior to the surgery in practice B. 6 depicts improvement in 3-year survival for patients in each practice selected for surge
x These mar inol value curves
indicate that despite the higher on expecte f gerative mor- o tality rate in practice B, selection of patients wi more to gain from surgery is providing patients from practice B with more benefit than patients from practice A.
sonnel to store records, review charts, and produce paper reports that are difficult to read, subject to recording and interpretation bias, and impossible to analyze with mod- em analytic tools. An integrated computer system will help to stem the current trend toward reducing the num- bers of personnel providing direct patient care and increasing the personnel assigned to bureaucratic tasks.
With large groups of practitioners linked electroni- cally in this way, the potential is created for the resulting aggregated data to be analyzed in ways that help inform future medical decisions. Making medical care decisions consistent with individual patient preferences and values will continue to require the artful interaction of the prac- titioner and the patient, but when complex arrays of infor- mation must be considered to predict future outcomes and select among multiple alternatives, the computer will be an invaluable resource. Patients undergoing initial or follow-up evaluation due to a change in clinical status will be managed with the help of sophisticated risk algo- rithms or predictive models that are based on the avail- able clinical, laboratory, and diagnostic test data. Mea- suring outcomes and feeding such data back into the system will allow those risk algorithms or models to be validated, refined, and updated. Use of such validated models will provide a means for health care systems to project the clinical and economic consequences of cur- rent practice policies regarding the use of behavioral, pharmacologic, and mechanical intervention for a cohort of patients. These models will also make it possible for practitioners and administrators to examine the implica- tions of changes in practice policies on both outcomes and costs.
Advances in biotechnology have provided many ex- citing new therapeutic possibilities, but have also pushed the need for clinical trials to test these possibilities beyond the logistical and financial resources available. The clinical database of the future will permit the per- formance of clinical trials on a scale not imagined in the past. Because large numbers of patients are needed to detect reliably the incremental effects of most new treat- ments on outcomes, many future trials of cardiovascu- lar therapies will need to be quite large. Electronic med- ical records will provide ready access to most of the important baseline characteristics and concomitant infor- mation routinely collected in a clinical trial. Thus, the cost of adding the unique data elements required for a particular trial to such a system would be far less than the current cost of data collection for most multicenter trials. The resulting reduction in the cost of conducting a trial will allow more resources to be applied to answer- ing critical questions about practice. In addition, elec- tronic medical records will permit routine construction of registries covering patients not enrolled in the ran- domized trial, thereby providing key information about the generalizability of the resulting findings.
The database of the future will be used to evaluate the effectiveness of practitioners, groups, hospitals, and sys- tems. Currently, practitioners receive reports from others about their performance. In the future, this information will be available on-line to each practitioner. Periodic aggregation of these data will allow for early identifica-
1180 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 76 DECEMBER 1, 1995

tion and practice management of problems on medical scorecards. Practitioners will be able to examine and, if necessary, change their own practice behavior before out- side persons or groups (payors or government agencies) pass judgment. Future medical scorecards will likely take 3 forms: procedure-based outcome reports, process of care and outcome reports for practice groups, and assess- ments of the value of decision-making.
For practitioners performing procedures, a running record can be made available to allow them to be aware of their individual performances in terms of success rates and complications. The institutional or health care sys- tem performance can also be made available as each case is done. In addition to the medical outcomes, the costs of common procedures will be available on the individ- ual and institutional scorecard. Sophisticated regression equations can be built into the computerized system to provide immediate information about observed out- comes versus those expected in view of the severity of illness of the patients being treated.
Practice groups will increasingly be judged on the outcome of the patient over a period of time. A grow- ing number of therapies have been shown to be effec- tive in preventing recurrent symptomatic episodes or death in patients with documented ischemic heart dis- ease. Databases can be used to remind practitioners when these therapies are indicated, to measure the degree to which desirable practices are being used, and to evalu- ate the results of those practices in groups of patients as measured by mortality rates, hospitalizations, morbidi- ty, and cost. Individual practitioners and groups will be able to develop guidelines for decision-making and to track the success of those guidelines by measuring the degree to which they are used and the outcomes of the patients treated with the guidelines.
In the future, evaluation of medical practice will con- sider explicitly the value of medical decisions and prac- tices. Competence in the performance of specific proce- dures at a competitive price will be a prerequisite for practice groups, but, increasingly, the decision about who is evaluated and treated in a particular manner will be the key point of interest. For example, a cardiovascular practice may perform angioplasty and surgery with excellent outcomes and costs, even with adjustment for severity of underlying illness, but if patients are chosen for revascularization who derive little benefit, the excel- lent outcomes may be no better than what would have been expected with less aggressive and less expensive care. Using results of currently available or soon-to-be available clinical trials and observational studies of myo- cardial revascularization, it is now possible to project the expected survival experience for individual coronary dis- ease patients treated with medical therapy alone, surgi- cal revascularization, or percutaneous revascularization. If we take a population of patients treated by a particu- lar group, an “empirically-derived marginal value curve” could be calculated in which the impact of the choice of revascularization on survival could be estimated. In the hypothetical example in Figure 1, the group practice with the higher operative mortality is actually providing the greatest benefit to its patients.
None of this will change the critical importance of the clinician as a humanitarian who must work closely with the patient to make individual decisions and who must use the finest “bedside” skills to assist the patient in dealing with disease and prevention of its secondary consequences. Indeed, the availability of information that makes choices more explicit will, in many ways, produce a more challenging situation for the practition- er. In some cases, this information will point to difficult and risky therapeutic options that demand knowledge of the values and preferences of the patient and family. In other cases, the patient may wish the physician to carry the burden of a complex decision problem. We believe that the medical profession has a vital responsibility to collect and analyze data about its own practices and make decisions using accurate information and state-of- the-art methodology. Abdication of this responsibility will leave the medical profession virtually powerless to define the direction of medical care in the interest of the patient. In the not too distant future, practitioners will be able to justify judicious use of high technology and specialty care for their patients using clinically relevant outcome information that can serve as a common thread in a health care system with many conflicting agendas.
1. Ginzberg E. High-tech medicine and rising health care costs. JAMA 1990; 263:182&1822. 2. Dzau VJ, Gibbons GH, Cooke JP, Omoigui N. Vascular biology and medicine in the 1990s: scope, concepts, potentials, and perspectives. Circulation 1993;87: 705-719. 3. Iglehart JK. Managed competition. N Engl J Med 1993:3X3:1208-1212. 4. Rosati RA, Wallace AG, Stead EA Jr. The way of the future. Arch Intern Med 1973;131:285-287. 5. Califf RM, Pryor DB, Greenfield JC Jr. Beyond randomized clinical trials: apply- ing clinical experience in the treatment of patients with coronary artery disease. Circulation 1986:74:1191-l 194. 6. Hlatky MA, Lee KL, Harrell FE Jr, Califf RM, Pryor DB, Mark DB, Rosati RA. Tying clinical research to patient care by use of an observational database. SmMed 1984;3:375-387. 7. Califf RM, Harrell FE Jr, Lee KL, Rankin JS. Hlatky MA, Mark DB, Jones RH, Muhlbaier LH, Oldham HN Jr, Plyor DB. The evolution of medical and surgical ther- apy for coronaq artery disease: a 15.year perspective. JAMA 1989;261:2077-2086. 8. Harrell FE Jr, Califf RM, Pryor DB, Lee KL, Rosati RA. Evaluating the yield of medical tests. JAMA 1982;247:2543-2546. 9. Mark DB, Hlatky MA, Ha&l FE Jr, Lee KL, Califf RM, Pryor DB. Exercise treadmill score for predicting prognosis in coronary artery disease. Ann Intern Med 1987;106:793-800. 10. Pryor DB, Shaw LK, McCants CB, Lee KL, Mark DB, Harrell FE Jr, Muhlbaier LH, Califf RM. Value of the history and physical in identifying patients at increased risk for coronary artery disease. Ann Infern Med 1993;118:81-90. Il. Mark DB, Nelson CL, Califf RM, Ha&l FEJ, Lee KL, Jones RH, Fortin DF, Stack RS, Glower DD, Smith LR, DeLong ER, Smith PK, &eves JG, Jollis JG, Tcheng JE, Muhlbaier LH, Lowe IE, Phillips HR, Pryor DB. The continuing evo- lution of therapy for coronary artery disease: initial results from the era of coro- nary angioplasty. Circulation 1994;89:2015-2025. 12. Tcheng JE, Fortin DF, Pryor DB, CaIiff RM. A guide to the technology of information manawment. In: Roubin G. Phillios HR III. O’Neill WW. Califf RM. Stack RS, eds. Gerventional Cardiovascular’Medicine: Principles and Practice. New York: Churchill Livingstone, 1993:945-950. 13. Fortin DF, Blunden PB, Pryor DB, Tcheng JE, Califf RM. The Duke Databank for Cardiovascular Disease. In: Roubin G, Phillips HR III, O’Neill WW, Califf RM, Stack RS. eds. Interventional Cardiovascular Medicine: Princioles and Practice. New York: Churchill Livingstone, 1993:959-966. 14. Donaldson MS, Lohr KN (eds). Health Data in the Information Age: Use, Dis- closure and Privacy. Washington, D.C., Committee on Regional Hea& Data Net- works, Institute of Medicine, National Academy Press, 1994. 15. Jollis JG, Ancukiewicr M, DeLong ER, Pryor DB, Muhlbaier LH, Mark DB. Discordance of databases designed for claims payment versus clinical information systems: implications for outcomes research. Ann Intern &fed 1993;119:844-850. 16. Feinstein AR. An additional basic science for clinical medicine. II. The limi- tations of randomized trials. Ana Znrem Med 1983;99:544-550. 17. Byar DP. Why data bases should not replace randomized clinical trials. Bio- metrics 1980;36:337-342.
iDlTORlALS 1 181

18. Mantel N. Cautions on the use of medical databases. .StatMed 1983;2:355-362. pitals treating Medicare beneficiaries and short-term mortality. N Engl JMed 1994 19. Top01 EJ, Califf RM. Scorecard cardiovascular medicine: its impact and future 331:1625-1629. directions. Ann Intern Med 1994;120:65-70. 22. Pryor DB, Lee KL. Methods for the analysis and assessment of clinical data 20. Hannan EL, O’Donnell JF, Kilbum H, Bernard HR, Yazici A. Investigation of bases: the clinician’s perspective. Stat Med 1991;10:617-628. the relationship between volume and mortality for surgical procedures performed 23. Goldman L, Weinstein MC, Williams LW. Relative impact of targeted versu in New York State hospitals. JAMA 1989;262:503-510. population-wide cholesterol interventions on the incidence of coronary heart dis 21. Jollis JG, Peterson ED, DeLong ER, Mark DB, Collins SR, Muhlbaier LH, Pry ease. Projections of the coronary heart disease policy model. Circulaiion 1989;82 or DB. The relation between the volume of coronary angioplasty procedures at hos- 254260.
IMPLICATIONS FOR COST-EFFECTIVENESS The integration of new information technologies into the practice of medicine will
have a substantial impact on the cost of care in 3 ways. First, many institutions and physician practices will be able, for the tirst time, to assess their true cost of caring for a particular type of patient or clinical problem. By understanding clearly the med- ical resource inputs (and their costs) for a particular episode of care, they will be able to maximize efficiency and reduce waste without necessarily reducing quality. This will allow provider groups to compete more effectively for patient care contracts and will reduce the chances of their bidding at a level that is below their break-even cost.
Second, combining cost data with clinical data will make it possible to compare the value added for dollars spent on different programs. Using predictive models such as those developed by our group, for example, we could calculate the relationship between the added cost of each patient treated with coronary artery bypass grafting (CABG) and the added benefit expected for that patient (e.g., extra angina-free sur- vival). Comparison of the profile of different programs might show that Program A has less total cost and a lower average cost per CABG patient but also adds signifi- cantly less benefits per dollar spent through Program B. Thus, the higher-cost pro- gram in this hypothetical scenario (Program B) is providing more value.
Finally, whereas replacing existing information systems at hospitals and physician offices will add expense to the medical care system, an information system that sat- isfies the needs of the providers will likely pay for itself. Having ready access to detailed practice and cost data may allow the administration to perform its functions more efficiently and effectively. This could lend support to a reversal of the recent trend in hospitals to cut back on patient care stalf while preserving or even increas- ing administrative staff. An integrated medical information system should help reduce the overhead costs of medical practice by ensuring that important data are captured by the system and that such data are entered into the system only once. Medical records, billing, quality assurance, and competing for new business/retaining old busi- ness are among the administrative functions that will be made substantially more effi- cient with an integrated information system.
Robert M. Califf, MD
1182 THE AMERICAN JOURNAL OF CARDIOLOGY@ VOL. 76 DECEMBER 1, 1995