Embed Size (px)
Citation preview
CASE & REVIEW
The trigeminal trophic syndrome: An unusual causeof nasal ulceration
Seetha U. Monrad, MD,a Jeffrey E. Terrell, MD,c and David M. Aronoff, MDb
Ann Arbor, Michigan
Trigeminal trophic syndrome (TTS) is an unusual complication after peripheral or central damage to thetrigeminal nerve, characterized by anesthesia, paresthesias, and ala nasi ulceration. We describe a patientwith classic TTS after trigeminal rhizotomy who underwent several extensive evaluations for nasal ulcer-ation and received prolonged immunosuppressive therapy for a presumed autoimmune disorder before thecorrect diagnosis was made. An understanding of the predisposing factors and clinical presentation of TTSis important to ensure a timely diagnosis of this difficult-to-treat illness. Differentiation of TTS frommalignancy, infection, or vasculitis is possible on the basis of clinical history, tissue biopsy, and serologicevaluation. (J Am Acad Dermatol 2004;50:949-52.)
CASE REPORTA 52-year-old woman presented with progressive
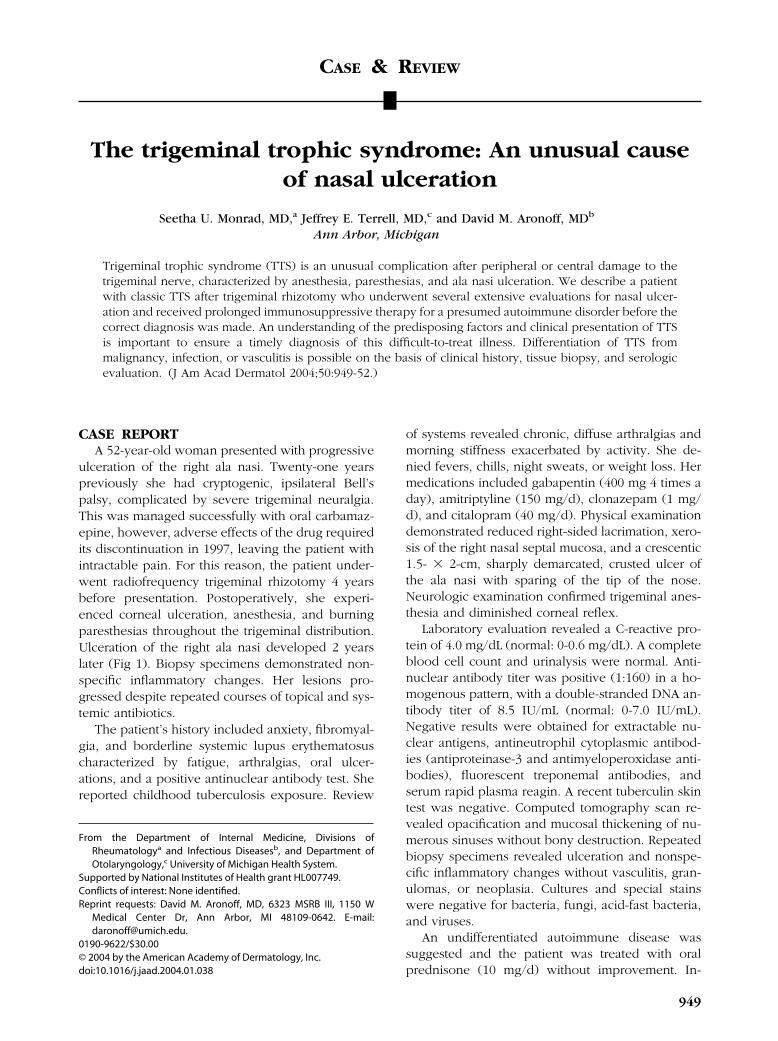
ulceration of the right ala nasi. Twenty-one yearspreviously she had cryptogenic, ipsilateral Bell’spalsy, complicated by severe trigeminal neuralgia.This was managed successfully with oral carbamaz-epine, however, adverse effects of the drug requiredits discontinuation in 1997, leaving the patient withintractable pain. For this reason, the patient under-went radiofrequency trigeminal rhizotomy 4 yearsbefore presentation. Postoperatively, she experi-enced corneal ulceration, anesthesia, and burningparesthesias throughout the trigeminal distribution.Ulceration of the right ala nasi developed 2 yearslater (Fig 1). Biopsy specimens demonstrated non-specific inflammatory changes. Her lesions pro-gressed despite repeated courses of topical and sys-temic antibiotics.
The patient’s history included anxiety, fibromyal-gia, and borderline systemic lupus erythematosuscharacterized by fatigue, arthralgias, oral ulcer-ations, and a positive antinuclear antibody test. Shereported childhood tuberculosis exposure. Review
From the Department of Internal Medicine, Divisions ofRheumatologya and Infectious Diseasesb, and Department ofOtolaryngology,c University of Michigan Health System.
Supported by National Institutes of Health grant HL007749.Conflicts of interest: None identified.Reprint requests: David M. Aronoff, MD, 6323 MSRB III, 1150 W
Medical Center Dr, Ann Arbor, MI 48109-0642. E-mail:[email protected].
0190-9622/$30.00© 2004 by the American Academy of Dermatology, Inc.doi:10.1016/j.jaad.2004.01.038
of systems revealed chronic, diffuse arthralgias andmorning stiffness exacerbated by activity. She de-nied fevers, chills, night sweats, or weight loss. Hermedications included gabapentin (400 mg 4 times aday), amitriptyline (150 mg/d), clonazepam (1 mg/d), and citalopram (40 mg/d). Physical examinationdemonstrated reduced right-sided lacrimation, xero-sis of the right nasal septal mucosa, and a crescentic1.5- � 2-cm, sharply demarcated, crusted ulcer ofthe ala nasi with sparing of the tip of the nose.Neurologic examination confirmed trigeminal anes-thesia and diminished corneal reflex.
Laboratory evaluation revealed a C-reactive pro-tein of 4.0 mg/dL (normal: 0-0.6 mg/dL). A completeblood cell count and urinalysis were normal. Anti-nuclear antibody titer was positive (1:160) in a ho-mogenous pattern, with a double-stranded DNA an-tibody titer of 8.5 IU/mL (normal: 0-7.0 IU/mL).Negative results were obtained for extractable nu-clear antigens, antineutrophil cytoplasmic antibod-ies (antiproteinase-3 and antimyeloperoxidase anti-bodies), fluorescent treponemal antibodies, andserum rapid plasma reagin. A recent tuberculin skintest was negative. Computed tomography scan re-vealed opacification and mucosal thickening of nu-merous sinuses without bony destruction. Repeatedbiopsy specimens revealed ulceration and nonspe-cific inflammatory changes without vasculitis, gran-ulomas, or neoplasia. Cultures and special stainswere negative for bacteria, fungi, acid-fast bacteria,and viruses.
An undifferentiated autoimmune disease wassuggested and the patient was treated with oralprednisone (10 mg/d) without improvement. In-
949

950 Monrad, Terrell, and Aronoff J AM ACAD DERMATOL
JUNE 2004
creasing doses of oral azathioprine (up to 150 mg/d)were prescribed but the lesion progressed, spread-ing toward the right inner canthus. On numerousoccasions the patient developed cellulitis, requiringantibiotics. The patient initially denied, but later ad-mitted to, manipulating the wound, at times subcon-sciously. She routinely “cleaned out” the ulcer toremove blood clots and eschars that obstructed herbreathing at night.
Trigeminal trophic syndrome (TTS) was diag-nosed based on the histopathology and the triad oftrigeminal anesthesia, facial paresthesias, and cres-centic ala nasi ulceration. The patient was urged tostop manipulating her ulcer and to keep it under asterile dressing. Unfortunately, she died soon after-wards from an accidental overdose of narcotic anal-gesics used to control the chronic trigeminal neural-gia. Postmortem examination revealed no systemicdisease or alternative diagnosis.
DISCUSSIONTTS is an unusual condition after damage to the
sensory root of the trigeminal nerve, with subse-quent progressive ulceration in the affected der-matome. Initially described by Wallenberg,1,2 TTSfirst appeared in the English-language literature 32years later in independent publications by Loveman3
and McKenzie.4 More than 100 cases have subse-quently been described.2,5
The most common presentation of TTS followstrigeminal ablation by rhizotomy or alcohol injectioninto the gasserian ganglion.2,5,6 Other causes of tri-geminal sensory nerve damage implicated in TTS arelisted in Table I. The period of latency betweentrigeminal injury and ulceration ranges from weeksto decades and the syndrome is more common inwomen and the elderly.2
The ala nasi is the most usual location of ulcer-ation, although lesions may occur on the scalp, fore-head, ear, palate, and jaw.5 The tip of the nose is
Fig 1. Female patient with crescentic ulceration of alanasi.
spared, as a result of innervation by the medialbranch of the anterior ethmoidal nerve.7,8 Alar ulcer-ation occurs in noncartilagenous areas, adopting acrescentic shape that helps differentiate it from ul-cers secondary to neoplastic or other inflammatoryprocesses. Destruction of the adjacent lip and cheekmay result in a characteristic sneer.5 Histologically,chronic ulceration is identified with minimal inflam-matory infiltrate (in the absence of a secondary su-perinfection) and no giant cells, granulomas, or vas-culitic lesions.9,10
The mechanism of ulceration is primarily trau-matic, usually self-induced. Often patients have par-esthesias in the affected area, prompting touching,rubbing, or picking to relieve the perceived irrita-tion.5,9 In some cases, anesthesia creates a sensationof nasal congestion and impaired airflow, precipitat-ing repetitive nasal manipulation.5 The self-mutilat-ing behavior may become compulsive; patients aresometimes unaware of their actions and denywound manipulation. Although self-induced traumais the primary cause of ulceration, there may bespecific neurologic injuries responsible for the in-tractable paresthesias and poor wound healing ofTTS. It is notable that herpes zoster, an importantnoniatrogenic trigger of TTS, can result in similarself-induced ulcers when recalcitrant pruritus fol-lows the initial rash.11 Investigations into the neuro-logic abnormalities underlying postherpetic itch11
may result in a better understanding of the cause ofTTS lesions.
The differential diagnosis of TTS is broad and adefinitive diagnosis relies on excluding other causesof nasal/facial ulceration (Table II). Treatment ofTTS is difficult and involves prevention of the com-pulsive behaviors in response to facial paresthesias.6
Table I. Causes of trigeminal nerve damageimplicated in cases of trigeminal trophic syndrome
Trigeminal rhizotomyAlcohol or glycerol injection of gasserian ganglionCortical and brainstem infarctionsVertebrobasilar insufficiencyAcoustic neuromaAstrocytomaIntracranial meningiomaSpinal cord degenerationMycobacterium leprae neuritisHerpes zoster opthalmicusSyringobulbiaPostencephalitic parkinsonismTraumaIdiopathic
Data compiled from references2,4-7,9.

Monrad, Terrell, and Aronoff 951J AM ACAD DERMATOL
VOLUME 50, NUMBER 6
Educating the patient about the self-induced natureof the ulceration is important.2 Protective devices orprostheses to cover the affected area, meticulousfingernail care, and cotton glove use may help.2
Topical therapy with saline nasal sprays and mois-turizers is of unproven benefit and promotes woundmanipulation. Systemic and topical antibioticsshould be applied to treat secondary infections.
Numerous pharmacologic therapies aimed at di-minishing paresthesias and compulsive behaviorshave been applied with anecdotal success, includingpimozide12,13; carbamazepine14; chlorpromazine15;amitriptyline and diazepam16; vitamin B supple-ments17; and clonazepam.9 Notably, our patient devel-oped TTS while receiving gabapentin, citalopram,amitriptyline, and clonazepem. Immunosuppressiveagents provide no benefit.18 Other interventions in-clude transcutaneous electrical stimulation19; ionto-pheresis and nerve blockade20; ionizing radiation3;ipsilateral cervical sympathectomy4,21; and stellateganglionectomy.4,22 Surgical reconstruction with in-nervated skin flaps has been successfully per-formed.9,10,23
In conclusion, TTS is an uncommon disordercomplicating peripheral or central damage to the
Table II. Diseases mimicking trigeminal trophic synd
Disease
InfectiousHerpes simplex and zoster virusesInvasive molds (mucormycosis, aspergillosis,
sporotrichosis)Other fungi (blastomycosis, paracoccidiodomycosis)Cutaneous anthrax (Bacillus anthracis)Syphilis (Treponema pallidum subsp. pallidum)
Yaws (T pallidum subsp. pertenue)
Mycobacterium tuberculosisLeprous trigeminal neuritis (M leprae)Cutaneous leishmaniasis
NeoplasticBasal cell, squamous cell carcinoma, sinonasal
(angiocentric) T/NK cell lymphomaAutoimmune
Wegener granulomatosis
Pyoderma gangrenosum
PsychiatricFactitious trauma
trigeminal nerve, characterized by crescentic ala nasiulceration in the setting of anesthesia and paresthe-sias. Treatment of TTS is aimed at suppressing par-esthesias, preventing manipulation, and coveringdefects with innervated skin flaps. It is important todifferentiate this syndrome from autoimmune disor-ders, infectious diseases, and neoplastic processesthat may mimic TTS.
REFERENCES1. Wallenberg A. Klinische Beitrage zur Diagnostik akuter
Herderkrankungen des Verlangerten Marks und der Bruke. Dt ZNervenheilk 1901;19:227-31.
2. Litschel R, Winkler H, Dazert S, Sudhoff H. Herpes zoster-associ-ated trigeminal trophic syndrome: a case report and review. EurArch Otorhinolaryngol 2003;260:86-90.
3. Loveman AB. An unusual dermatosis following section of thefifth cranial nerve. Arch Dermatol Syph 1933;28:369-75.
4. McKenzie KG. Observations on the results of the operative treat-ment of trigeminal neuralgia. Can Med Assoc J 1933;29:492-6.
5. Weintraub E, Soltani K, Hekmatpanah J, Lorincz AL. Trigeminaltrophic syndrome: a case and review. J Am Acad Dermatol 1982;6:52-7.
6. Dicken CH. Trigeminal trophic syndrome. Mayo Clin Proc 1997;72:543-5.
7. Bauer F. Trophic ulceration of the ala nasi following trigeminaldenervation. J Laryngol Otol 1966;80:422-5.
Diagnostic aids
ions typically painful; Tzanck smear; culturemunosuppressed patient; bone/sinus destruction present;ulture/biopsypsy/culture; serologycupational exposure; painless black eschar; culture/biopsyrology; dark-field microscopy; direct fluorescent antibodyestvel to endemic area; serology; dark-field microscopy;irect fluorescent antibody testosure history; caseating granulomas, organisms on biopsyosure history; trigeminal nerve biopsyosure history; identification of amastigotes by histology orirect microscopy; growth of promastigotes in culture;olymerase chain reaction
sue invasion; may cross midline; biopsy diagnostic
opulmonary, renal disease; erosion through skin unusual;ranulomas, vasculitis on biopsy; antineutrophilicytoplasmic antibodiesions painful; undermined, violaceous borders; biopsy maye useful
ions usually tender; may be bilateral; absence ofeurologic signs
rome
LesIm
cBioOcSe
tTra
dExpExpExp
dp
Tis
Singc
Lesb
Lesn

952 Monrad, Terrell, and Aronoff J AM ACAD DERMATOL
JUNE 2004
8. Cliff IS, Demis DJ. Giant ulcer of the face following surgery fortrigeminal neuralgia. Arch Intern Med 1967;119:218-22.
9. Goodnight JW, Calcaterra T. Trigeminal trophic syndrome: a re-port of two cases and review. Am J Otolaryngol 1994;15:219-22.
10. Munnoch DA, Morris AM. Trigeminal neuralgia, trophic ulcer-ation and the plastic surgeon. J R Coll Surg Edinb 1998;43:185-8.
11. Oaklander AL, Cohen SP, Raju SV. Intractable postherpetic itchand cutaneous deafferentation after facial shingles. Pain 2002;96:9-12.
12. Duke EE. Clinical experience with pimozide: emphasis on its usein postherpetic neuralgia. J Am Acad Dermatol 1983;8:845-50.
13. Mayer RD, Smith NP. Improvement of trigeminal neurotrophiculceration with pimozide in a cognitively impaired elderly wom-an–a case report. Clin Exp Dermatol 1993;18:171-3.
14. Bhushan M, Parry EJ, Telfer NR. Trigeminal trophic syndrome:successful treatment with carbamazepine. Br J Dermatol 1999;141:758-9.
15. Kavanagh GM, Tidman MJ, McLaren KM, Goldberg A, Benton EC.The trigeminal trophic syndrome: an under-recognized compli-cation. Clin Exp Dermatol 1996;21:299-301.
16. Finlay AY. Trigeminal trophic syndrome. Arch Dermatol 1979;
115:1118.17. Philpott OS. Trophic ulcer complicating operative proceduresfor the relief of trigeminal neuralgia. Rocky Mt Med J 1941;38:626-9.
18. Datta RV, Zeitouni NC, Zollo JD, Loree TR, Hicks WL Jr. Trigeminaltrophic syndrome mimicking Wegener’s granulomatosis: a casereport with a review of the literature. Ann Otol Rhinol Laryngol2000;109:331-3.
19. Westerhof W, Bos JD. Trigeminal trophic syndrome: a successfultreatment with transcutaneous electrical stimulation. Br J Der-matol 1983;108:601-4.
20. Tada J, Ueda M, Abe Y, Fujiwara H, Arakawa K, Arata J. Trigeminaltrophic syndrome—a report of three patients. J Dermatol 1991;18:613-5.
21. Walton S, Keczkes K. Trigeminal neurotrophic ulceration–a re-port of four patients. Clin Exp Dermatol 1985;10:485-90.
22. Harris W. An analysis of 1,433 cases of paroxysmal trigeminalneuralgia (trigeminal-tic) and the end-results of Gasserian alco-hol injection. Brain 1940;63:209-44.
23. Abyholm FE, Eskeland G. Defect of the ala nasi following trigem-inal denervation: case report. Scand J Plast Reconstr Surg 1977;
11:87-90.