Embed Size (px)
Citation preview

The Role of Neuroimaging in Selecting Treatments
for Patients with Acute StrokeDavid Greer, MD, Jamary Oliveira-Filho, MD, and Walter J. Koroshetz, MD
AddressNeurointensive Care and Acute Stroke Service, Massachusetts General Hospital, 55 Fruit Street, VBK 915, Boston, MA 02114, USA.
Current Neurology and Neuroscience Reports 2001, 1:26–32Current Science Inc. ISSN 1528-4042Copyright © 2001 by Current Science Inc.
IntroductionImaging in stroke now has the potential to reveal thepathophysiologic basis of the ischemic threat, includingthe underlying vascular lesion, the anatomic distributionor severity of the ischemia, and the anatomic distributionand stage of the ischemic brain injury. This informationshould guide the physician in his or her attempts tolimit the extent of the ischemic brain injury, to institutethe most appropriate secondary stroke prevention, and toassess the effectiveness of specific treatments. Recentprogress in stroke imaging establishes the basis for apathophysiologic-based evolution of stroke treatment.
However, stroke imaging technology and our understand-ing of clinical-radiologic correlation are still in an earlystage. As we learn more about how emergency brain imag-ing predicts response to a specific treatment, its role inguiding treatments for acute stroke patients will expand.
The potential role of imaging in selecting patients foracute stroke treatment falls into two major categories: 1)accurate identification of the ischemic stroke patient eligi-ble for a specific treatment; and 2) estimation of potentialrisk of a specific treatment risk versus its expected benefitin the individual patient.
Brain Imaging in Identification of Patients with Acute Ischemic Stroke.Identifying ischemia or abnormal brain perfusionPositron emission tomography (PET) is the gold standard toidentify brain ischemia [1,2]. The value of PET is twofold: 1)it provides maps of quantitative cerebral blood flow (CBF);and 2) it provides maps of metabolic consequences oflowered CBF, ie, ischemia (increased oxygen extractionfraction, lowered metabolic rate of oxygen, or glucoseutilization). No other technique has quite the analyticpower of PET, but unfortunately it is not a practical tool inthe emergency setting. How can we obtain such informationclinically? A variety of brain imaging techniques areavailable that can quickly identify the presence of loweredbrain perfusion in an emergency situation, including singlephoton emission computed tomography (SPECT), xenoncomputed tomography (CT), bolus-tracking magneticresonance imaging (MRI), and bolus-tracking radiographiccomputed tomography (RCT). Given its good spatialresolution, ability to provide quantitative blood flowinformation, and potential accessibility, xenon CT hasshown considerable promise as a clinically useful tool toidentify patients with ischemia [3]. SPECT imaging has beenstudied in acute stroke setting and is estimated to have a79% sensitivity for locating site of infarct, with specificity of95% [4]. CT, but primarily magnetic resonance (MR)techniques, also offer the advantage of being able to detecttissue consequences of ischemic injury, hypodensity on CT,and decreased diffusion of water by diffusion weightedimaging (DWI).
The armamentarium available for treating acute stroke patients is growing as clinical trials show benefit of intravenous thrombolysis, intra-arterial clot lysis, and antiplatelet agents. Patients with dissection or severe atheromatous stenosis of major cerebrovascular vessels are commonly treated with anticoagulation to prevent recurrent artery-to-artery embolus or arterial thrombosis. These advances in acute stroke treatments demand an accurate means to quickly identify those patients most likely to benefit (or not benefit) from a specific therapy. Fortunately, advances in imaging cerebrovascular lesions, decreased brain perfusion, and even ischemic tissue injury now make it possible to consider tailoring therapy to the individual patient’s cerebrovascular problem. Experience and controlled clinical data in this endeavor is meager. Here we describe the ability of various emergency neuroimaging tools to provide information on the state of brain blood flow, metabolism, and vascular anatomy. Most importantly, we present the rationale and limited available evidence relevant to how the neuroimaging information might be used to select optimal treatments for individual patients.

Neuroimaging in Selecting Treatments for Patients with Acute Stroke • Greer et al. 27
By tracking passage of a bolus of dye, estimates of rela-tive cerebral blood volume (rCBV) and relative cerebralblood flow (rCBF) relative mean tranist time (rMTT) canbe obtained using RCT [5] (currently limited to singlebrain slice) or echoplanar MRI (possible to image perfu-sion in whole brain) [6]. MR perfusion weighted imaging(PWI) may provide excellent ability to identify patientswith ischemia. However, bolus tracking PWI currently suf-fers from its inability to provide quantitative CBF infor-mation. The rMTT or relative time to peak (rTTP) brainmaps detect delays in perfusion of one brain regioncompared with others. Although this makes the techniqueextremely sensitive in identifying acute stroke patients, itdoes not identify those specific levels of low CBF that actu-ally threaten the survival of brain tissue. rCBV maps, on theother hand, seem to be highly specific in identifying tissuedestined for infarction [6], but rare patients may havesymptomatic ischemia on rMTT maps with normal rCBVmaps. Maps of regions that have lost the high-flow compo-nent as measured by PWI also may provide more specificitywith regard to the portion of the abnormal rMTT lesion athighest risk of infarction [7]. Large-scale prospective stud-ies of unselected patients to determine specificity and sen-sitivity of PWI have not yet been published.
Perhaps the simplest and most widely available studyof brain perfusion can be obtained with a helical CT scan-ner during performance of computed tomographic angiog-raphy (CTA). A nonquantitative computed tomographicperfusion (CTP) image is obtained by scanning the entirebrain after the bolus of intravenous contrast (whole brainCTP) [8]. Regions with low CBV will not receive asmuch contrast dye and will appear dark compared with thenormal brain (Fig 1). CTP increases the sensitivity of theRCT to identify patients with evidence of ischemia. Inour experience, up to 90% of patients with acute middlecerebral artery (MCA) territory stroke have an identifiableCTP abnormality. This technique, as well as the othercurrently available perfusion imaging techniques, is lesssensitive in patients with small vessel stroke.
Identifying early evidence of ischemic injuryMagnetic resonance DWI identifies an early stage ofischemic injury [9,10] and provides a means to trace itsdevelopment in patients [11–13]. Ischemic brain exhaus-tion of ATP stores causes anoxic depolarization and a rundown of ionic gradients, followed by water movement intothe cells. This movement of water from the more mobileextracellular space into the colloidal matrix of the intra-cellular milieu causes a decrease in the apparent diffusioncoefficient (ADC) of brain water and a regional increase insignal intensity on DWI. This imaging signature occursbefore infarction occurs and precedes the anoxic depolar-iza t ion that occurs a f ter ischemia [14] . In bothanimal models [16•] and humans [17•], if the brain isreperfused quickly, the tissue hyperintense on DWI may besalvaged. However, without successful reperfusion the DWI
abnormal tissue in stroke patients always goes on to infarc-tion. Serial studies show that in most patients imagedwithin 6 hours of onset, the DWI lesion is still enlarginghours later [11–13].
The sensitivity of DWI in identifying acute strokepatients is dependent upon the duration and degree of theischemia. It will approach the high 90% range in strokepatients as the interval between symptom onset and scantime approaches 6 hours [18•,19]. In a recent study of 24patients scanned with a mean time from onset of 3.43hours, an MTT abnormality on PWI and a DWI lesion wereseen in all of them [20]. It is rare to encounter a patientwith a symptomatic large intracranial vessel occlusion andnegative DWI. In reviewing 782 consecutively scannedpatients presenting with a stroke-like deficit, Ay et al. [21•]found 27 patients had a normal DWI while still symptom-atic. Only six patients had documented stroke on follow-up imaging. The two groups posing the most difficultywere patients with small brainstem lacunar strokes andpatients with major artery branch occlusions in which thePWI demonstrated decreased rCBF and increased rMTTbut normal rCBV. The regions with low rCBF but normalDWI were initially sympomatic and did eventually go onto infarct, representing “penumbra without core” [21•].
Acute stroke imaging is currently mandatory to excludepatients with intracranial hemorrhage from thrombolytictreatment. The value of combined diffusion/perfusionMR in positiviely identifying stroke patients has led tothe question of whether MR can detect intracranialhemorrhage well enough to substitute for CT. A number ofstudies have pointed to the excellent sensitivity of MR to
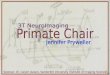
Figure 1. Schematic showing the rationale of using the mismatch between the perfusion weighted imaging (PWI) lesion volume on mean transit time (MTT) maps and the lesion volume on diffusion weighted imaging (DWI) to select patients for thrombolysis. Serial magnetic resonance imaging studies in acute stroke indicate that the DWI lesion increases over hours after a stroke. The PWI lesion volume decreases in this same time period. The region of final infarct is determined at the crossover point. Successful reperfusion therapy causes the perfusion lesion to suddenly decrease in size so that the crossover point occurs at a smaller DWI lesion volume and a smaller final stroke size. The benefit of reperfusion therapy constantly shrinks over time but varies among stroke patients.

28 Stroke
detect intracranial hemorrhage [20,22]. A head-to-headcomparison evaluating sensitivity and specificity versusRCT has not yet been published.
Noncontrast CT is the now the standard imaging tech-nique in acute stroke primarily because of its sensitivity tohemorrhage and subacute stroke. RCT detects hypodensitydue to increased water and decreased blood in the tissue,usually a sign of irreversible brain injury. In many patients,especially those with large strokes, CT hypodensity occurswithin a few hours of stroke onset. In an MR/CT compari-son study, Gonzalez et al. [18•]. found CT sensitivity of45% compared with 100% for DWI. However, from thesame center, Lev et al. [23] reported that varying the win-dow and level settings of the computerized CT images toprovide an almost black and white image significantly aidsin identification of patients with MCA territory stroke. Ifthe image is made almost black and white, with a centerlevel setting of 20 Houndsfield units (HU) and a windowsetting of 80 HU, the sensitivity of detection rises from the57% with standard settings to 71% with high-contrastsettings. There was no loss of specificity [23].
Identification of the vascular lesionIntra-arterial clot lysis is the most obvious treatment inneed of an accurate, rapid means of selecting patients.In the Prolyse® for Acute Cerebral Thromboembolism(PROACT) study of MCA occlusion, improved outcomewas demonstrated in the treated group [24]. However, inthe study, hundreds of patients underwent direct angiog-raphy only to find that they did not have an MCA occlu-sion. A rapid, sensitive, noninvasive technique thatdetects major vascular occlusions will be essential forselecting patients for treatment with intra-arterial devicesthat remove occlusive clots.
A rapid means of detecting a vascular stenosis alsoaids in the emergency evaluation of patients with transientischemic attacks (TIA) or minor stroke. It enablesidentification of those patients with symptomatic largevessel atherosclerosis or arterial dissection who have a highrisk of secondary or progressive stroke. In this context,emergency imaging of the vascular lesion enables rapidselection of patients who may benefit from aggressive mon-itoring, anticoagulaton, or revascularization procedures.
Patients with nonischemic neurologic deficit mimickingan acute, major cerebral artery syndrome form the thirdgroup in whom rapid, reliable evaluation of the cerebrovas-cular system is valuable. Nonstroke diagnoses can be pursuedafter a reliable study reveals widely patent cerebral vessels.
Selective injection of the cerebral arteries serves asthe gold standard in identifying the vascular stenosis orocclusion underlying the ischemic insult, but it is invasive,expensive, involves risk, and is not consistently available inemergency settings. Magnetic resonance angiography(MRA), CTA, and transcranial doppler ultrasound are non-invasive means of identifying vascular lesions that are lessexpensive and easily made available in the emergency
setting. The most recent advance in doppler ultrasoundcame with the addition of ultrasound contrast to transcra-nial color doppler. The vascular detail of MRA can beenhanced by intravenous injection of gadolinium with theflow-sensitive time of flight (TOF) sequences. The institu-tion of fast, helical CT scanners has enabled RCT to imagean intravenously administered bolus of CT contrast as itpasses through the cerebrovascular system. CTA, asopposed to MRA, is closer to direct angiographpy, as it isbased upon lumenal contrast signal as opposed to a flowvelocity as in MRA and doppler ultarsound. Three-dimen-sional, computer-generated vascular reconstructionsprovide exquisite vascular detail from CTAs.
In a report of 21 patients with acute nonhemorrhagicstroke studied prospectively with both CTA and digital sub-traction angiography (DSA), two raters correctly assessedall trunk occlusions of the basilar artery, internal carotidartery, and MCA, although assessment of more distal MCAbranch occlusions was less reliable. Additionally, there wasan 88% agreement rate in judging the degree of collateralvessel circulation in 17 occlusions. The size of 21 (62%) of34 hemispheric infarctions was also correctly predicted[25]. In a different study of 145 patients with symptoms ofacute stroke, arterial stenoses or occlusions were found tobe present on 43% of CT angiograms. For 27 cases inwhich both CTA and MRA were obtained, findings were inagreement for 98% of the vessels; agreement was 99% forthe 28 cases in which both CTA and DSA were acquired[26]. Therefore, current data attests to the extremely highaccuracy of CTA in detecting lesions in large intracranialvessels. In addition, whole brain CT perfusion studies canbe obtained simultaneously. The increased scanning speedof the newly marketed multidetector CT (MDCT) increasesthe extent of the vasculature that can be scanned. Now,much like MRA, a single multidetector CTA study canimage from the aorta through Circle of Willis to the topof the brain in less than 5 minutes. Information on thepresence of major extracranial and intracranial cerebralartery occlusion or stenosis can now be available to theemergency stroke physician.
Evaluation of the Risks and Benefits of Reperfusion TherapyCurrently, the only Food and Drug Administration-approved therapy in acute stroke patients is intravenousrecombinant tissue-plasminogen activator (rt-PA) within 3hours of stroke onset [27]. However, the PROACT studydemonstrated efficacy of intra-arterial clot lysis in patientswith MCA occlusion with treatment beginning by 6 hoursfrom onset but ending 2 hours later [24]. Some argue thatthe second European rt-PA (ECASS2) study containsevidence to indicate that some patients may benefit fromIV rt-PA in the 3- to 6-hour window. These trials focusattention on the need to develop a means to assess the riskand benefit of reperfusion therapy in the individual patient

Neuroimaging in Selecting Treatments for Patients with Acute Stroke • Greer et al. 29
at varying time periods from onset. Advanced imagingtechniques offer the potential to map the individual strokepatient’s salvageable versus irreversibly damaged tissue tobetter assess the risk/benefit ratio. However, its role inguiding therapy remains investigational.
The irreversibly injured tissueThe first European study of rt-PA (ECASS1) within 6 hoursof stroke onset showed that patients with CT hypodensityor effacement of sulci in greater than one third of the terri-tory of the MCA (1/3 MCA) had a significantly increasedchance of symptomatic hemorrhage [28]. This is the firstexample of how stroke progression on brain imagingmight guide selection of patients for thrombolysis.However, no evidence currently exists to extend this guide-line to the treatment of patients within 3 hours of onset orto patients with posterior circulation or anterior cerebralartery (ACA) territory stroke. It is also clear that classifica-tion of early CT scans by the 1/3 MCA rule is difficult[29,30]. Optimal windowing of CT scans helps in identify-ing the abnormal region [23], but whether this changesthe clinical significance of finding greater than 1/3 theMCA territory involved is not known. Reversibility ofischemic tissue hypodense on CT is thought to occurrarely, if at all.
Computed tomographic scanning of the entire brainafter contrast dye injection allows evaluation of a crudeCBV and assessment of the collateral circulation. The extentof leptomeningeal collaterals on CTA has been found tocorrelate with the collateral flow pattern at angiography[31•] and outcome after intravenous thrombolysis[32•,33•]. The size of the CTP lesion has been found tocorrelate with outcome after intra-arterial thrombolysis[23]. This technique has the potential to identifypatients who will have poor outcome even in the caseof successful thrombolysis, but requires considerablymore extensive validation.
As discussed previously, DWI is more sensitive thannoncontrast CT in detecting early ischemic injury [18•].Not surprisingly, Barber et al. [34] reported that DWI con-curred with CT in identifying all patients having greaterthan 1/3 MCA territory involvement on CT. More problem-atic in this study is how to act in the case of the one patientin which DWI, but not CT, showed involvement in greaterthan 1/3 MCA territory. Deciding not to reperfuse patientswith large DWI lesions is complicated by the fact that DWIis not inherently an irreversible tissue signature [16•,17•].With early reperfusion, DWI hyperintensity can reverse,either transiently, with necrosis of the tissue coming onafter recurrence of the DWI signal intensity, or perma-nently, with scattered neuronal necrosis at pathology.
The tissue at risk for infarction but salvageable by rep-erfusion is the target for presently available acute stroketherapy (Table 1). The tissue signature of this region onPET is increased oxygen ejection fraction (OEF), decreasedCBF, normal cerebral metabolic rate of oxygen (CMRO2),
and normal-labeled flumazenil binding [1,2,35].Combined DWI/PWI in patients identifies tissue that hasabnormal perfusion (low rCBF, increased rMTT) buthas not progressed to DWI hyperintensity. This tissue issalvageable by reperfusion. Serial MRI studies in acutestroke show that without reperfusion, a portion of theregion with abnormal rMTT/rCBF and normal DWI goeson to infarction. Most importantly, a rMTT lesion that ismore extensive than the initial DWI lesion is an indicatorof an enlarging stroke [6,13,36,37]. In contrast, in patientswith lesions on rMTT/rCBF maps that match the DWIlesion, the final stroke size and its distribution is often verysimilar to that of initial DWI lesion. Most importantly, ithas been demonstrated that in patients with PWI > DWIlesions, successful reperfusion is associated with blockingthe enlargement, or even substantially reducing, theDWI lesion [17•,30,38].
These observations have led to the hypothesis that therelationship between the PWI and DWI abnormal regions,and not necessarily the time from onset, should be used toselect patients for acute reperfusion therapy [39,40].Patients with major brain regions demonstrating abnormalPWI (low rCBF and increased rMTT) but normal DWI, socalled “PWI>DWI mismatch,” may be helped by reperfu-sion therapy independent of the time from onset ofischemic symptoms. This pattern (PWI > DWI) is associ-ated with an enlarging territory of injury over time. It ismore commonly seen in patients with a large intracranialartery occlusion, less commonly with distal branch occlu-sion [34,41]. A PWI abnormality that is much smaller thanthe extent of the DWI hyperintensity indicates that reperfu-sion has already occurred; this may preclude any benefitof instituting thrombolysis. The latter is also a pattern thathas been described to occur more commonly after intra-venous rt-PA treatment [30] as a sign of drug-inducedreperfusion. Because DWI hyperintensity does not signifyirreversible damage, there remains the chance that apatient with a matched lesion (PWI=DWI) is still a reason-able candidate for thrombolysis (given that the CT doesnot also show a hypointensity that matches the perfusionabnormality). A similar algorithm can be developed usingxenon CT with the target for reperfusion being regions withnormal noncontrast CT characteristics but dangerously lowquantitative CBF. A similar algorithm can be tested usingnoncontrast CT combined with contrast CT perfusion[31•]. In this instance, the target for reperfusion is theregion with moderate CT perfusion abnormality but nor-mal signal intensity on noncontrast CT.
Limitations and Future Goals of Acute Brain Imaging Investigation in Selecting Patients for Acute Reperfusion TherapyBased on current published evidence, the only establishedrole of emergency brain imaging is to exclude patients withbrain hemorrhage from thrombolysis. The presence of low

30 Stroke
density on CT involving greater than 1/3 MCA territory is abad prognostic factor for hemorrhage that must be takeninto consideration in the decision of whether to treat withintravenous rt-PA within 3 hours of onset. It is clear, how-ever, that with further clinical data and current methods weshould be able to better use acute brain imaging informa-tion. The introduction of better methods will also have amajor impact on this field.
It is important to understand the limitations of the cur-rent stroke imaging techniques. A potential disadvantageof the bolus t racking PWI s trategy i s the purelyempiric nature of the association between the rCBF andtruly ischemic levels of blood flow reduction. A means toquantify blood flow with MRI using arterial spin-labelingtechniques or even with bolus tracking may be valuable.Changes in the microcirculatory flow pattern may betterpredict tissue at risk [6]. Xenon CT gives quantitative bloodflow. MDCT measurements of CBF with bolus tracking ofradiograph contrast may be easier to quantify than MRmeasurements because the increase in Houndsfield units isproportional to the concentration of the dye.
Finally, the decision not to attempt reperfusion becauseof the degree of injury rests on a technique that reliablymarks tissue as irreversibly injured. Quantitation of bloodflow, ADC, or CT Houndsfield units may be essential inestablishing this important threshold. The presence ofDWI hyperintensity does not mark the tissue as irreversiblydamaged, however, irreversibly ischemic injury can only
occur after the tissue becomes DWI bright [17•]. Subtle,but definite injury patterns of CT hypodensity on the non-contrast scan need to be investigated, just as the DWIlesion has been, in relation to the perfusion abnormalityand change over time.
Another future goal of stroke neuroimaging is to iden-tify the tissue signature of regions with high probability ofhemorrhage after reperfusion. Very-low blood flow onxenon CT, rapid progression of CT hypodensity, leakage oflarge molecules (gadolinium, iodinated contrast) from thevasculature into the tissue, or iron-sensitive paramagneticsusceptibility MR sequences are potential indicators in thisregard. The latter may also help in identifying patientswith previous microhemorrhages due to amyloid angio-pathy, who have a higher risk of hemorrhage after treat-ment with thrombolytic drugs.
ConclusionsEmergency brain imaging in the acute stroke setting is nowmandatory. Advanced techniques in CT and MR brainimaging can now rapidly provide pathophysiologic infor-mation regarding the vascular lesion, the extent of thebrain perfusion abnormality, and extent of an early stage oftissue injury. Learning how the imaging characteristicspredict outcome after specific acute stroke therapy isnow a major focus of stroke research. Understanding thisrelationship will eventually guide clinical decision making
Table 1. Proposed tissue signatures of ischemic brain tissue that is salvageable by reperfusion therapy
Computed tomographyMagnetic resonance imaging
Xenon computed tomograhy
Positron emission tomography
Indicator of tissue viability
Normal signal intensity (Houndsfield units) on noncontrast CT
Normal ADC on DWI* Normal signal intensity on noncontrast CT
Normal CMRO2; normal flumazenil binding
Indicator of integrity of the vascular bed
Normal or moderate perfusion (decreased but present contrast signal in the tissue) on bolus tracking of CT dye through whole brain CTP
Normal CBV on bolus tracking MR perfusion†
Moderate but not severe CBF reduction (> 10–15 mL/100 gm/min)
Normal CBV
Indicator of abnormal perfusion
a) Increased MTT and decreased CBF on single slice CT perfusion
a) Increased rMTT and decreased rCBF on bolus tracking MR perfusion
Moderate CBF reduction on quantitative xenon CT
Moderate decrease in CBF; increased OEF
b) Moderate CT perfusion abnormality on whole brain CTP
b) Symptoms correlate with brain territory of occluded/stenotic vessel on MRA
c) Symptoms correlate with brain territory of occluded/stenotic vessel on CTA
*Some levels of ADC reduction may be reversible with early reperfusion therapy.†CBV reduction may be associated with normal ADC for a short time period and, therefore, reversible with reperfusion. Most likely region to be salvaged with reperfusion is one with abnormal rCBF and rMTT but normal CBV and normal DWI.ADC—anodal duration contraction; CBF—cerebral blood flow; CBV—cerebral blood volume; CMRO2—cerebral metabolic rate of oxygen; CT—computed tomography; CTA—computed tomographic angiography; CTP—computed tomagraphic perfusion; DWI—diffusion weighted imaging; MR—magnetic resonance; MRA—magnetic resonance angiography; MTT—mean transit time; OEF—oxygen ejection fraction.

Neuroimaging in Selecting Treatments for Patients with Acute Stroke • Greer et al. 31
and allow optimization of treatment decisions on an indi-vidual patient basis. Because of the relatively recent intro-duction of these techniques, evidence-based guidelines onthe use of imaging to select patients are still rudimentary.
References and Recommended ReadingPapers of particular interest, published recently, have been highlighted as:• Of importance•• Of major importance
1. Baron J: Mapping the ischemic penumbra with PET: implications for acute stroke treatment. Cerebrovasc Dis 1999, 9:193–201.
2. Heiss WD, Kracht L, Grond M, et al.: Early (11C) flumazenil/H20 positron emission tomography predicts irreversible ischemic cortical damage in stroke patients receiving acute thrombolytic therapy. Stroke 2000, 30:366–369.
3. Firlik AD, Rubin G, Yonas H, Wechsler LR: Relation between cerebral blood flow and neurological deficit resolution in acute ischemic stroke. Neurology 1998, 51:177–182.
4. Baird AE, Austin MC, McKay WJ, Donnan GA: Sensitivity and specificity of 99mTc-HMPAO SPECT cerebral perfusion measurements during the first 48 hours for the localization of cerebral infarction. Stroke 1997, 28:976–980.
5. Cenic A, Nabavi DG, Craen RA, et al.: Dynamic CT measurement of cerebral blood flow: A validation study. Am J Neuroradiol 1999, 20:63–73.
6. Sorensen AG, Copen WA, Ostergaard L, et al.: Hyperacute stroke: simultaneous measurement of relative cerebral blood volume, relative cerebral blood flow and mean tissue transit time. Radiology 1999, 210:519–527.
7. Ostergaard L, Sorensen G, Chesler D, et al.: Combined diffu-sion-weighted and perfusion-weighted flow heterogeneity magnetic resonance imaging in acute stroke. Stroke 2000, 31:1097–1103.
8. Hunter GJ, Hamberg LM, Ponzo JA, et al.: Assessment of cerebral perfusion and arterial anatomy in hyperacute stroke with three-dimensional functional CT: early clinical results. Am J Neuroradiol 1998, ???:29-37.
9. Moseley ME, Cohen Y, Mintorovitch J, et al.: Early detection of regional cerebral ischemia in cats: comparison of diffusion-and T-weighted MRI and spectroscopy. Magn Reson Med 1990, 14:330–346.
10. Busza AL, Allen KL, King MD, et al.: Diffusion-weighted imaging studies of cerebral ischemia in gerbils. Potential relevance to energy failure. Stroke 1992, 23:1602–1612.
11. Baird AE, Benfield A, Schlaug G, et al.: Enlargement of human cerebral ischemic lesion volumes measured by diffusion-weighted magnetic resonance imaging. Ann Neurol 1997, 41:581–589.
12. Schwamm LH, Koroshetz WJ, Sorensen AG, et al.: Time course of lesion development in patients with acute stroke. Serial diffusion and hemodynamic-weighted magnetic resonance imaging. Stroke 1998, 29:2269-2276.
13. Beaulieu C, deCrespigny A, Tong DC, et al.: Longitudinal magnetic resonance imaging study of perfusion and diffusion in stroke: evolution of lesion volume and correlation with clinical outcome. Ann Neurology 1999, 46:568–578.
14. Harris NG, Zilkha E, Houseman J, et al.: The relationship between the apparent diffusion coefficient measured by magnetic resonance imaging, anoxic depolarization and glutamate efflux during experimental cerebral ischemia. J Cereb Blood Flow Metab 2000, 20:28–36.
15. Lin W, Li F, Silva MD, et al.: Temporal evolution of ischemic injury evaluated with diffusion and perfusion and T2-weighted MRI. Neurology 2000, 54:689–696.
16.• Li F, Liu KF, Silva MD, et al.: Transient and permanent resolution of ischemic lesions on diffusion-weighted imaging after brief periods of focal ischemia in rats. Correlation with histopathology. Stroke 2000, 31:946–954.
Rats were exposed to short (10 minutes) or long (30 minutes) periods of middle cerebral artery occlusion. Serial magnetic resonance imaging studies were performed to track early reversal of diffusion weighted imaging (DWI) abnormality. Transient or permanent resolution of initial DWI lesions was seen in the short and long ischemia groups, respectively. Transient resolution of DWI lesions was associated with widespread neuronal necrosis. In regions with permanent resolution of DWI lesions, approximately 17% ofneurons were still found to be dead.17.• Kidwell T, Saver J, Mattiello J, et al.: Thrombolytic reversal
of acute human cerebral ischemic injury shown by diffusion/perfusion magnetic resonance imaging. Ann Neurol 2000, 47:462–469.
The authors performed diffusion weighted imaging (DWI)/perfusion weighted imaging (PWI) before and after intra-arterial thrombolysis in seven patients. Perfusion magnetic resonance (MR) studies in five of five patients showed larger regions with delayed contrast delivery than DWI abnormality. After thrombolysis all patients improved clinically; repeat MR studies showed complete resolution of the PWI abnormality in four; decrease in the DWI lesion in five. The follow-up DWI study 7 days later showed reappearance of part of the initial DWI lesion in three patients. This is the first study in humans to show reversal of DWI lesions after reperfusion, as well as the secondary reappearance of DWI lesions. Also demonstrates that reperfusion blocks growth of infarct as measured by serial DWI scans.18.• Gonzalez RG, Schaefer PW, Buonanno FS, et al.:
Diffusion-weighted MR imaging: diagnostic accuracy in patients imaged within 6 hours of stroke symptom onset. Radiology 1999, 210:155–162.
Blinded review of magnetic resonance (MR) and computed tomography (CT) in 22 consecutively imaged patients presenting with acute stroke syndrome. Fourteen had final stroke, eight had final nonstroke diagnoses. In the first 6 hours, diffusion weighted imaging (DWI) had 100% sensitivity and 85% specificity in detecting the stroke patients. This compared with 45% sensitivity and 100% specificity for standard noncontrast CT, and18% sensitivity and 100% specificity for T2- weighted MR. The contrast to noise ratios were much better (77%) for DWI as compared with 5.5% for CT and 9.8% for T2-weighted imaging.19. Lovblad KO, Laubach HJ, Baird AE, et al.: Clinical experience
with diffusion weighted MR in-patients with acute stroke. Am J Neuroradiol 1998, 19:1061–1066.
20. Schellinger PD, Jansen O, Fiebach JB, et al.: A standardized MRI stroke protocol: comparison with CT in hyperacute intracerebral hemorrhage. Stroke 1999, 30:765–768.
21.• Ay H, Buonanno FS, Rorodorf G, et al.: Normal diffusion weighted MRI during stroke-like deficits. Neurology 1999, 52:1784–1792.
Twenty seven of 782 consecutively imaged patients presenting with acute stroke-like syndromes were found to have normal diffusion weighted imaging (DWI) in brain regions responsible for the symptom. Nonischemic diagnoses were eventually rendered in 37%; transient ischemic attack or prolonged reversible deficit in 24%; 25% had infarction seen on follow-up imaging. Small brainstem lacunes were especially difficult to identify on the initial image. Magnetic resonance-demonstrated ischemia (prolonged mean transit time and low cerebral blood flow) but normal cerebral blood volume and normal DWI in symptomatic brain regions on the initial scan but infarct on the follow-up scan, so called “penumbra without core.”22. Patel MR, Edelman RR, Warach S: Detection of hyperacute
primary intraparenchymal hemorrhage by magnetic resonance imaging. Stroke 1996, 27:2321–2324.
23. Lev M, Segal AZ, Farkas J, et al.: CT perfusion imaging of hyperacute middle cerebral artery stroke predicts outcome of intraarterial thrombolytic treatment. In Proc Am Soc Neurorad-iol San Diego, CA.1999,
24. Furlan A, Higashida R, Wechsler L, et al.: Intra-arterial prourokinase for acute ischemic stroke. JAMA 1999, 282:2003–2011.

32 Stroke
25. Knauth M, von Kummer R, Jansen O, et al.: Potential of CT angiography in acute ischemic stroke. Am J Neuroradiol 1997, 18:1001-1010.
26. Shrier D, Tanaka H, Numaguch Y, et al.: CT angiography in the evaluation of acute stroke. Am J Neuroradiol 1997, 18:1011–1020.
27. The National Institute Of Neurological Disorders and Stroke rt-PA Stroke Study Group: Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995, 333:1581–1587.
28. Hacke W, Kaste M, Fieschi C, et al.: Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke: the European Cooperative Acute Stroke Study (ECASS). JAMA 1995, 274:1017–1025.
29. Grotta JC, Chiu D, Lu M, et al.: Agreement and variability in the interpretation of early CT changes in stroke patients qualifying for intravenous rtPA therapy. Stroke 1999, 30:1528–1533.
30. Marks MP, Tong DC, Beaulieu C, et al.: Evaluation of early reperfusion and IV t PA therapy using diffusion-and perfusion-weighted MRI. Neurology 1999, 52:1792–1798.
31.• Lee HK, Lee SJ, Cho SJ, et al.: Triphasic perfusion computed tomography in acute middle cerebral artery stroke. A correlation with angiographic findings. Arch Neurol 2000, 57:990–999.
Eight patients undewent computed tomography perfusion (CTP) studies followed by direct angiography. Regions of severe loss of contrast on CTP were found to correlate with regions of no or few collaterals on angiography. Regions with moderate loss of contrast signal on CTP were found to correlate with regions of slow leptomeningeal collaterals. Low density on noncontrast CT was confined to the zone of severe perfusion deficit on CTP. The NIHSS correlated with the extent of the total perfusion deficit.32.• Wildermuth S, Knauth M, Brandt T, et al.: Role of CT
angiography in patient selection for thrombolytic therapy in acute hemispheric stroke. Stroke 1998, 29:935-938.
Computed tomographic angiography (CTA) was performed in 40 consecutive patients with NIHSS greater than or equal to 8, scanned at less than 6 hours from onset of symptoms. Thirty-four patients had a documented vessel occlusion on CTA. Collateral flow was estimated as absent (no visible arteries apparent beyond the occlusion), good (filling of the sylvian branches), or moderate (collaterals visible). Twenty patients were treated with intravenous rt-PA and 20 with heparin. The extent of eptomeningeal collaterals seen on the CTA cor-related significantly with the outcome after thrombolytic therapy (RS=0.46, P<0.05).
33.• Lee KH, Lee SJ, Cho SJ, et al.: Usefulness of triphasic perfusion computed tomography for intravenou thrombolysi withtissue type plasminogen activator in acute ischemic stroke. Arch Neurol 2000, 57:1000–1008.
Seventeen patients had computed tomography perfusion studies and were treated with rt-PA within 3 to 7 hours after stroke onset. Patients with a moderate degree of perfusion deficit (see reference above) spanning 50% or more of the middle cerebral artery territory had a better chance of early improvement.34. Barber PA, Darby DG, Desmond PM, et al.: Identification of
major ischemic change. Diffusion-weighted imaging versus computed tomography. Stroke 1999, 30:2059–2065
35. Heiss WD, Thiel A, Grond M, Graf R: Which targets are relevant for therapy of acute ischemic stroke? Stroke 1999, 30:1486–1489.
36. Neurmann-Haefelin T, Wittsack HJ, Wenserski F, et al.: Diffusion- and perfusion-weighted MRI: the DWI/PWI mismatch region in acute stroke. Stroke 1999, 30:1591–1597.
37. Karonen JO, Nuutinen J, Kuikka JT, et al.: Combined diffusion and perfusion MRI with correlation to single-photon emission CT in acute ischemic stroke. Ischemic penumbra predicts infart growth. Stroke 1998, 29:939–943.
38. Schellinger PD, Janse O, Fiebach J, et al.: Monitoring intravenous recombinant tissue plasminogen activator thrombolysis for acute ischemic stroke with diffusion and perfusion MRI. Stroke 2000, 31:1318–1328.
39. Albers GW: Expanding the window for thrombolyitc therapy in acute stroke. The potential role of acute MRI for patient selection. Stroke 1999, 30:2230–2237.
40. Schlaug G, Benfield A, Baird AE, et al.: The ischemic penumbra. Operationally defined by diffusion and perfusion MRI. Neurology 1999, 53:1528–1537.
41. Rordorf G, Koroshetz WJ, Copen WA, et al.: Regional ischemia and ischemic injury in patients with acute middle cerebral artery stroke as defined by early diffusion-weighted perfusion-weighted MRI. Stroke 1998, 29:939–943.