Embed Size (px)
Citation preview

2013
2013; 35: 287–294
The role of ePortfolios in supporting continuingprofessional development in practice
JENNIFER A. GORDON & CRAIG M. CAMPBELL
Royal College of Physicians and Surgeons of Canada, Canada
Abstract
ePortfolios, based on models of reflective practice, are viewed as important tools in facilitating and supporting lifelong learning
across the medical education continuum. MAINPORT, the ePortfolio designed by the Royal College of Physicians and Surgeons of
Canada, supports the continuing professional development (CPD) and lifelong learning of specialist physicians practicing in
Canada by providing tools to develop CPD plans, set and track progress of established learning goals, document and reflect
on learning activities, and create the foundation for physicians to manage their learning. In this article, the authors summarize the
key design principles of the Royal College’s ePortfolio: learner-centered; interoperable; ease of access. The current core
functionality as well as future planned functionality for MAINPORT are described under three domains: recording and reflecting
on completed CPD activities; managing learning in practice; accessing learning resources and programs. The future MAINPORT
will evolve to become a foundational tool to support the shift towards competency-based medical education across the continuum
of medical education; from residency to retirement. MAINPORT will facilitate the ability of physicians to demonstrate their
expertise over time and how their learning has enabled improvements to their practice in contributing to improved health
outcomes for patients.
Introduction
Over the past two decades, systems of continuing professional
development (CPD), in response to concerns regarding
persistent gaps in physician performance (Grol et al. 2002),
adherence to health care indicators (McGlyn et al. 2003) and
quality of care measures (Institute of Medicine 1999; Forster
et al. 2004), have changed their focus from a primary
emphasis on knowledge dissemination strategies to facilitating
a culture of lifelong learning and self-improvement. This
cultural shift has been facilitated by CPD systems defining
values, educational principles, and measureable outcomes
and informed by a growing scientific evidence base on the role
of learning on behaviour change, performance improvement
and health outcomes (Davis et al. 1999; Grimshaw et al. 2002;
Overeem et al. 2007).
The cultural shift in CPD has been equally enabled by
technological innovations that have assisted physicians, for
example, to access CPD resources when addressing identified
practice needs, share stories and practice innovations within
inter-professional teams or communities of practice
(Parboosingh 2002), to use simulations (McGaghie et al.
2006; Gurusamy et al. 2008) and other self-assessment
strategies, and leverage data about how performance
and health outcomes can inform future learning (van der Veer
et al. 2010).
One of the technological innovations to support learning
in practice is the ePortfolio which may be defined as ‘a
purposeful aggregation of digital items – ideas, evidence,
reflections, feedback, etc., which ‘presents’ a selected
audience with evidence of a person’s learning and/or ability’
(Sutherland et al. 2007).
ePortfolios have been introduced across a range of health
professions within undergraduate (Finlay et al. 1998; Scholes
et al. 2004; Driessen et al. 2005; Ross et al. 2009; Hall et al.
2012), postgraduate (Teunissen et al. 2008; Wassef et al. 2012)
and CPD (duBoulay 2000; Austin et al. 2005; Davies et al. 2005;
Galbraith et al. 2008; Green et al. 2009; Kardos et al. 2009;
Tompkins et al. 2010) to support learning, reflection, self-
assessment, and the provision of feedback. The development
and implementation of ePortfolios within these contexts have
been viewed as important tools in facilitating the transition
towards competency-based medical education spanning the
continuum from residency to retirement. Several recent
systematic reviews have examined the educational effective-
ness of ePortfolios for learning and assessment within under-
graduate and postgraduate health education (Driessen et al.
2007; Buckley et al. 2009; Tochel et al. 2009). However, in
Practice points
. ePortfolios support lifelong learning across the con-
tinuum of education from residency to retirement
. ePortfolios can support reflection, assessment, and the
management of learning
. The design and functionality of ePortfolios may vary
based on needs and goals, but must be learner-centered
. Technology standards have facilitated interoperability,
data transfer, and reporting
Correspondence: Jennifer Gordon, Royal College of Physicians and Surgeons of Canada, Ottawa, Ontario K1S 5N8, Canada. Tel: (613) 730 6211;
fax: 613-730-2410; email: [email protected]
ISSN 0142–159X print/ISSN 1466–187X online/13/040287–8 � 2013 Informa UK Ltd. 287DOI: 10.3109/0142159X.2013.773395
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Reg
ina
on 0
9/07
/13
For
pers
onal
use
onl
y.

comparison to the initial phases of medical education, there
has been a relative paucity of literature on the role, utility or
functionality of ePortfolios to support or enable practice
reflection, lifelong learning and assessment of physicians in
practice.
Within professional practice contexts, portfolios were
introduced, initially using paper formats (Wilkinson et al.
2002), to provide a tool for health professionals to document
(for study credit) their participation in conferences, courses
or self-directed learning activities stimulated by practice. Over
time, electronic portfolios have supplanted paper versions
and transitioned from tools to document participation in
learning activities into tools that support multiple functions
including the ability to set and monitor goals, plan CPD
activities, manage learning projects, access learning resources
and document the outcomes of self-directed learning, self-
assessment and performance assessment for practice.
In Canada, the Royal College of Physicians and Surgeons of
Canada (www.royalcollege.ca), a not-for-profit professional
organization with a membership of 44,000 medical and
surgical specialists and resident affiliates, is responsible for
establishing the training requirements, accreditation standards
and national certification examinations for 67 specialties and
subspecialties. In 2001, the Royal College introduced a
mandatory Maintenance of Certification (MOC) Program to
support, enhance, and promote lifelong learning of Fellows
and other health care professionals in Canada. Participation in
the MOC Program, a mandatory requirement for maintaining
membership and the continued use of the Fellowship desig-
nation FRCPC or FRCSC, was supported by the provision of an
ePortfolio, MAINPORT.
In this article, the authors provide a brief review of the
theoretical models of practice reflection that have often
influenced the design and structure of ePortfolios; describe
the structure, design principles and key functional elements
included within MAINPORT, share data about how physicians
have used MAINPORT in practice; and discuss strengths,
barriers and plans for future development. This article is based
in part on the presentations included at the MedBiquitous
conference in May 2012.
Practice reflection: Theoreticalframeworks
Underlying theoretical frameworks that guided the original
development of ePortfolios by the Royal College were initially
based on models of practice reflection described by Schon
(1987) and Moon (2004). Donald Schon’s model of practice
reflection described a process where physicians are stimulated
by their ‘practice experiences (based on an awareness of a
need) to pause and reflect during (reflection-in-action) and/or
after (reflection-on-action) a process to frame and resolve the
issue identified. The learning process that seeks to gather,
analyze and apply evidence (both scientific and tacit) enables
physicians to learn from experience and guide the application
of new knowledge to reduce the risk of being ‘surprised’ in the
future. This process of pausing and learning before acting has
been recently described as self-monitoring by Eva and Regehr,
as an important component of physician self-assessment
(Eva & Regehr 2005). Moon defined reflection as ‘a form of
mental processing with a purpose and/or anticipated out-
comes that is applied to relatively complex or unstructured
ideas for which there is not an obvious solution’ (Moon 2004).
Moon’s model of reflection begins with noticing (an issue,
need or dilemma) followed by making sense, making meaning
that leads to transformative learning. A summary of the
evidence on the importance and impact of reflection and
reflective practice was the basis for a recent systematic review
(Mann et al. 2007). This literature review concluded that
‘Reflection is demonstrated among practicing professionals. It
appears that it fulfills several functions, including helping to
make meaning of complex situations and enabling learning
from experience’.
Reflection and reflective practice models emphasize the
importance of a purposeful critical analysis of experience or
knowledge to achieve greater understanding and meaning as
part of a continuous re-construction of practice (Parboosingh
2002). This process is central to how ePortfolios can facilitate
and support the capture the outcomes of reflection and
potentially facilitate the effectiveness of lifelong learning
defined as:
a continuously supportive process that stimulates
and empowers individuals to acquire all the know-
ledge, values, skills, and understanding they will
require throughout their lifetimes and to apply them
with confidence, creativity, and enjoyment in all
roles, circumstances, and environments. (Bankey
2007)
Definitions of reflection and lifelong learning emphasize
both the processes and skills required to continually seek,
acquire, renew, and upgrade knowledge, skills, competencies
and attitudes. Lifelong learning and reflection can be
stimulated by engaging in formal activities (where learners
have limited control over the learning objectives or methods),
informal or incidental activities (where learners have control
over the purpose of learning but the methods of learning
cannot be pre-planned) and self-directed learning (where the
learner controls the purpose and methods).
Structure and purpose ofePortfolios
Although there are numerous variations to the design and
structure of ePortfolios, the majority of ePortfolios fall within
one or more the following types (van Tartwijk & Driessen
2004):
Assessment portfolios: are usually organized to facilitate
learners with the opportunity to demonstrate achievement of
curricular objectives and for supervisors or evaluators to
review and assess specific learner achievements (products,
presentations, assessment scores, clinical outcomes).
Showcase portfolios: are intended to facilitate the ability of
learners to select, collect and display their best work or
evaluations from that work. Similar to portfolios in the visual
arts, showcase portfolios provide a record of personal devel-
opment and achievement that is dynamic and reflects a virtual
curriculum vitae.
J. A. Gordon & C. M. Campbell
288
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Reg
ina
on 0
9/07
/13
For
pers
onal
use
onl
y.

Development portfolios: enable learners to plan and keep
track of their own learning activities and personal develop-
ment plans. These development portfolios may be structured
around competencies and requirements to demonstrate pro-
gression and performance improvement towards mastery.
Reflective portfolios: provide learners and others with the
opportunity to reflect on experiences, learning activities,
critical incidents to make sense of one’s work with the
opportunity to receive feedback from others (mentors,
coaches, supervisors, etc.).
These basic types of portfolios are not mutually exclusive;
ePortfolios can be developed to integrate a combination of
these purposes depending on organizational needs.
MAINPORT incorporates several components from each of
the above-described types of ePortfolios. Regardless of the
type or purpose, typically, ePortfolio systems support most,
but not necessarily all, of the following processes (Becta 2008):
(1) Capturing and storing evidence
(2) Reflecting
(3) Giving and receiving of feedback
(4) Planning and setting goals
(5) Collaborating
(6) Presenting to a specific audience
ePortfolios for CPD at the RoyalCollege: Design characteristicsand functional elements
The development of the Royal College’s first ePortfolio, PC
Diary, was originally based on the Schon’s model of practice
reflection (Schon 1987) and designed to encourage specialists
to ‘consciously reflect on their practice experiences, identify
items of learning that they perceived had expanded or
consolidated their expertise and plan their professional devel-
opment’ (Campbell et al. 1996). With the implementation of
the Royal College’s mandatory Maintenance of Certification
(MOC) Program in 2001, all Fellows in full-time or part-time
practice or engaged in related professional development
activities, were required to document their learning activities
in a web-based ePortfolio, now called MAINPORT. The
structure and functionality of the Royal College’s MOC
Program and MAINPORT changed in 2011 to respond to the
findings from a survey completed by 2914 Fellows as part of a
formal MOC Program evaluation initiated in 2008 as well as
from an extensive review of the CPD research literature
applicable at that time.
The new MOC Program framework was simplified to reflect
how physicians learn and arranged an expanded number of
learning activities accepted for MOC credit under three
sections: group learning, self-learning, and assessment. Also,
a new revised credit system provided greater incentives for
MOC Program participants to engage in some self-learning and
all assessment activities. The new, re-designed MAINPORT
provided a more streamlined and user-friendly experience for
physicians with a number of new functional elements,
reflecting features from several of the types of ePortfolios
described above. Specifically, the new MAINPORT simplified
the documentation process for CPD activities and learning
outcomes for credit while providing tools to develop CPD
plans, set and track progress of established learning goals. It
also provided a learning space to access e-learning resources
(online journals and websites) that could be personalized and
created the foundation for physicians to manage their learning
in practice. These changes were intended to support the
transition toward competency-based CPD (Campbell et al.
2010).
Design characteristics
The key design principles of the Royal College’s MAINPORT
are summarized in Table 1.
Learner-centered
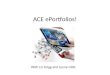
MAINPORT was designed so that its initial landing page
provided a high-level integrated ‘Dashboard’ (Figure 1). The
Dashboard presents a visual summary of the number of MOC
credits earned within the physician’s current MOC Program
cycle, the CPD activities completed, the learning activities in
progress or awaiting completion, and a listing of the CPD goals
being pursued. The Dashboard also offers an interface that is
intuitive to promote quick navigation and ease of use. The
provision of links to resources available from the Royal College
is complemented by the opportunity for each physician to
create a list of personal URL links to online resources such as
journals, websites or databases used by the physician. The
ePortfolio supports a learner-centered approach by offering
the user an ability to personalize the Dashboard to facilitate
access to learning resources commonly used in practice.
Interoperable
A key strategy for the current MAINPORT was to reduce the
burden of documentation by physicians. To accomplish this
design principle, multiple automation capabilities were
enabled including the sharing or transfer of data between
multiple technological systems. MAINPORT was designed to
receive data, including reflections documented by physicians,
from external third-party sources, directly into individual
MAINPORT accounts. One example of an automated
data transfer implemented to date includes the direct trans-
fer of data from InfoPOEMs (CMA website 2012) derived
from a physician’s review and recording of their reflections
Table 1. ePortfolio design principles.
� Learner-driven: the learner is responsible for the content of the
ePortfolio.
� User-friendly: an interface that is intuitive to promote ease of use.
� Flexibility: ability of learners to personalize access to tools, resources,
programs.
� Interoperability: to facilitate automation of data transfer from multiple
sources.
� Ease of Access: real-time access from multiple platforms including
mobile devices.
� Security: ensuring confidence in the security and privacy of data.
� Personal Growth and Professional Development: a ‘story of learning’
and expertise.
ePortfolios for CPD
289
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Reg
ina
on 0
9/07
/13
For
pers
onal
use
onl
y.

Figure 1. MAINPORT dashboard screen capture.
J. A. Gordon & C. M. Campbell
290
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Reg
ina
on 0
9/07
/13
For
pers
onal
use
onl
y.

on a summarized article provided by the Canadian
Medical Association. Other automated data transfer capabilities
include the reporting of completion of the Royal College’s
accredited online Bioethics self-assessment programs, as well
as participation in various accredited conferences held by
Royal College accredited CPD providers. The capability to
automatically transfer data from these external sources to each
physician’s MAINPORT account was made possible through
the MedBiquitous Activity Report standard (MedBiquitous
2012) that supported this design element of MAINPORT. The
data transfer process is based on a webservice API call, using a
standard XML format, to allow external CPD providers’ systems
to connect with MAINPORT via the Internet. These connec-
tions enable the Royal College to facilitate online, real-time
interactions with external organizations and reduce the docu-
mentation burden for physicians, saving them time and
focusing their documentation on what they learned, changed
or are planning to learn more about to enhance their practice.
In addition to helping reduce the documentation burden on
the physician, automation also provides a method of external
validation of the completion of an activity or attendance at an
event as compared to traditional physician self-reporting of
participation.
Ease of access
Beyond facilitating access to various online resources, the re-
designed MAINPORT ePortfolio enabled mobile access from
multiple platforms including the provision of BlackBerry and
Android apps in July 2012 and the development of a native
iPhone app in September 2012. The planned development
of mobile apps, based on demand from physicians, has not
only facilitated access to MAINPORT but encouraged phys-
icians to record and reflect as they learn. Key functionality of
the apps enables users to submit, modify or delete CPD
activities as well as review incomplete activities in their
MAINPORT accounts. Since the launch of the iPhone app in
September 2012, over 7000 Fellows have downloaded the app
and over 3000 Fellows have used the app to reflect and record
over 12,000 learning activities. The facilitation of recording
learning activities from mobile devices may contribute to the
inclusion of learning activities that would not have been
previously recorded in MAINPORT reflecting a more complete
summary of the lifelong learning of physicians over time.
Key functionality
The current core functionality as well as future-planned
functionality for MAINPORT are summarized in Table 2. The
key functional components of MAINPORT can be summarized
under three category headings:
Recording and reflection on completed activities
The ability to self-report participation in CPD activities and
reflect on the learning outcomes achieved provides evidence
of participation in learning activities and how learning
improves and contributes to competence, performance or
health outcomes. The documentation of lifelong learning
demonstrates the profession’s willingness to be transparent
and accountable for the privilege of professional self-regula-
tion, a benefit currently held by physicians practicing in
Canada. This functional component of recording and reflecting
on completed activities illustrates several common elements
among Showcase portfolios and Reflective portfolios.
MAINPORT assists reflection through the use of a common
set of questions within each documentation template, guiding
learners to record the details of their CPD activities for MOC
Program credit.
In the future, the structure of the documentation templates
will need to allow physicians to grant access to peers,
colleagues, mentors or coaches to provide feedback
(Driessen et al. 2007) and assist physicians to identify future
learning plans. Expansion of the current interoperability
standards will promote increased automation, and is expected
to even further reduce the burden of documentation for
individual physicians.
Table 2. ePortfolio functional components.
Current Future
The ability to: The ability to:
� Report on completed learning activities and reflect on learning outcomes
for practice
� Develop a practice-specific CPD learning plan
� Identify CPD goals, design and track learning activities to accomplish
stated goals
� Link CPD activities to CanMEDS roles
� Store ideas for future learning
� Manage learning activities in progress
� Access multiple search engines, online resources, and self-assessment
programs
� Personalize resources
� Access MAINPORT in either English or French
� Establish private and public layers
� Provide access to peers, mentors, coaches, and assessors for the
purposes of feedback (formative or summative)
� Expand automation strategies
� Describe professional practice domains using a ‘scope of practice’ tool
� Document cases and procedures completed in practice
� Link learning activities to scope of practice, competencies or milestones
� Develop tools to report on assessments of knowledge, competence, or
performance
� Access a calendar of events specific to one’s professional practice
� Link ePortfolio with social media and discussion forums to create online
communities of practice
� Expand the role of ePortfolio in supporting learning and assessment
across the continuum of medical education; from the beginning of
residency until retirement
ePortfolios for CPD
291
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Reg
ina
on 0
9/07
/13
For
pers
onal
use
onl
y.

Managing learning in practice
Learning in practice is stimulated by formal, informal and self-
directed activities through a process that is dynamic and
iterative. Physicians continually identify questions, issues or
concerns (Barrie et al. 1997; Ebell 1999) ‘at the point of care’
but only pursue a fraction of these identified needs. The
Holding Area of MAINPORT provides physicians with an
opportunity to store the questions they intend to pursue, the
articles that they are planning to review, the assessments they
are planning to complete etc., and revisit, revise or delete these
entries at any time in the future. In addition, the Holding Area
allows physicians to start a learning project and save the
activity for completion at a future date. Finally, MAINPORT
provides a CPD planning tool to enable physicians to reflect on
their key roles and responsibilities across multiple dimensions
of practice to identify key learning goals or initiatives. These
functions reflect some of the common elements of
Development portfolios and Showcase portfolios by enabling
learners to plan and keep track of learning activities and to
keep a record of specific goals, personal development, and
achievements relevant to their practice.
In the future, the planning and recording of learning
activities and outcomes (Moore et al. 2009) will be enhanced
by the development of a ‘scope of practice’ tool to allow
physicians to describe their professional practice and link
learning activities to specific competencies or milestones.
Identification of gaps from participation in various assessments
can then be framed into specific learning goals to create an
action plan either independently or with the help and
assistance of a mentor or coach (Wilkinson 2002).
Accessing learning resources and programs
Beyond the recording and management of learning is the
ability for MAINPORT to provide users access to search
engines and online resources. These resources support how
physicians scan their environment for new ideas or innov-
ations in development, search for evidence in response to
specific questions, and access online self-assessment programs
across multiple specialty and content domains. The ability to
centralize search engines and online resources with tools to
support the planning, management and recording of learning
activities creates the opportunity to build a learning space that
can be personalized.
In the future, accessing learning resources will become
increasingly specialty-specific and will be facilitated by the
adoption of a calendar of CME/CPD events, the population
of specialty-specific self-assessment programs and the ability
to integrate social media tools to access online communities
of practice.
Use of MAINPORT in supportinglifelong learning
By the end of 31 January 2012, which was the MOC Program
reporting deadline to record 2011 CPD activities, the
MAINPORT site (www.mainport.org) had 158,091 visits by
32,234 unique MOC Program participants. In comparison to
2010, the 2011 overall participation rates of Fellows practicing
in Canada rose from 89% to 92%. Participation of Fellows
practicing outside of North America stayed approximately the
same, moving from 59% to 54%.
There were significant changes in the percentage of
Fellows who used Section 2: Self-Learning during 2011 than
in 2010, with relatively stable participation in the other two
sections (Table 3). The total number of credits reported in
MAINPORT rose substantially from 4,506,187 in 2010 to
6,052,191 in 2011.
Further analysis will explore if the new MAINPORT has
changed usage patterns (frequency and type of reporting) and
how participants have used tools to plan, set goals, and access
online learning resources.
Discussion and final thoughts
Over the past decade, there has been a progressive cultural
shift in how the CPD of physicians has been conceptualized,
supported, and enabled. As residency education programs and
CPD systems transition towards a competency-based medical
education model, it is anticipated that ePortfolios will play an
important role in supporting physician learning and assess-
ment (Campbell et al. 2010; Harris et al. 2010; Iobst et al. 2010)
to address the changing learning needs and expectations of
physicians, regulatory authorities, and the public (Federation
of Medical Regulatory Authorities of Canada).
Table 3. Comparison of participation across the MOC program framework: 2010 and 2011.
Reporting YearSection 1:
Group learningSection 2:
Self-learningSection 3:
AssessmentTotal credits
reported
2010 97% 59% 37% 4,506,187
2011 94% 84% 30% 6,052,191
In 2011, the specialties with the highest numbers of unique Fellows reporting in MAINPORT included:
Psychiatry 14538 Obstetrics and Gynecology 4996
Anesthesia 9127 General Surgery 4848
Internal Medicine 8200 Ophthalmology 3611
Diagnostic Radiology 7794 Orthopedic Surgery 3187
Pediatrics 5523 Anatomical Pathology 2115
J. A. Gordon & C. M. Campbell
292
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Reg
ina
on 0
9/07
/13
For
pers
onal
use
onl
y.

However, a number of conceptual and practical barriers
remain to the adoption and integration of ePortfolios to
enhance their ability to support learning in practice. Further
research will need to address the following questions: What
structure or functionality of ePortfolios best supports learning
and reflection? What level of documentation provides suffi-
cient evidence of learning in practice? What is the role of a
mentor or coach in promoting ePortfolio use among residents
and physicians in practice? How can ePortfolios best support
both formative and summative assessment of achievement of
competencies, milestones or quality of care metrics? What is
the appropriate balance between facilitating reporting of
participation in learning activities with the need for physicians
to individually or collectively reflect and record meaningful
outcomes for practice? What skills are required by residents
and physicians in practice to manage their knowledge base
and plan their lifelong learning to address their professional
practice needs?
An ePortfolio which describes the learning activities
completed, the self-learning opportunities pursued, and the
areas of practice assessed and improved reflects the purpose
of CPD in demonstrating ‘progression of competence’ towards
the attainment of expertise. The future of ePortfolios in
supporting lifelong learning across the continuum of medical
education will require a greater degree of personalization, the
embedding of specialty-specific information that is pushed to
users based on their scope of practice, the provision of
continuous performance metrics, and the inclusion of data
from peers to inform the learning process and guide the
development of strategies that contribute to safe, evidence-
informed, and quality health care.
Declaration of interest: The authors report no conflicts of
interest. The authors alone are responsible for the content and
writing of the article.
Notes on contributors
Ms. JENNIFER A GORDON, MEd, is the Assistant Director of Continuing
Professional Development at the Royal College of Physicians and Surgeons
of Canada. Ms. Gordon oversees the Maintenance of Certification (MOC)
Program and the MAINPORT ePortfolio.
Dr. CRAIG M CAMPBELL FRCPC is an Associate Professor in the Faculty
of Medicine at University of Ottawa. He serves as Executive Director,
Office of Professional Affairs at the Royal College of Physicians and
Surgeons of Canada in Ottawa.
References
Austin Z, Marini A, Desroches B. 2005. Use of a learning portfolio for
continuing professional development: A study of pharmacist in Ontario
(Canada). Pharm Educ 5(3/4):175–181.
Bankey R. 2007. Technical report on lifelong learning. Ottawa: The Royal
College of Physicians and Surgeons of Canada.
Barrie AR, Ward AM. 1997. Questioning behaviour in general practice: A
pragmatic study. BMJ 215:1512–1515.
British Educational Communications and Technology Agency, JISC InfoKit.
2008. Understanding how e-portfolios work – Impact of e-portfolios on
learning (Hartnell-Young et al 2007). [Accessed 25 March 2013]
Available from http://www.jiscinfonet.ac.uk/infokits/e-portfolios/
Buckley S, Coleman J, Davison I, Khan KS, Zamora J, Malick S, Morley D,
Pollard D, Ashcroft T, Popovic C, et al. 2009. The educational effects of
portfolios on undergraduate student learning: A Best Evidence Medical
Education (BEME) systematic review. BEME Guide No. 11. Med Teach
Apr 31(4):282–298.
Campbell CM, Parboosingh JT, Gondocz ST, Babitskaya G, Lindsay E,
De Guzman RC, Klein LM. 1996. Study of Physicians’ Use of a Software
Program to Create a Portfolio of Their Self-directed Learning. Academic
Medicine 71(10):S49–S51.
Campbell CM, Silver I, Sherbino J, Cate OT, Holmboe E. 2010. Competency-
based continuing professional development. Med Teach; 32:657–662.
Davies H, Khera N, Stroobant J. 2005. Portfolios, appraisal, revalidation and
all that: A user’s guide for consultants. Arch Dis Child 90:165–170.
Davis D, O’Brien MA, Freemantle N, Wolf FM, Mazmanian P, Taylor-Vaisey
A. 1999. Impact of formal continuing medical education: Do
conferences, workshops, rounds and other traditional continuing
education activities change behavior or health care outcomes? JAMA
282(9):867–874.
Driessen EW, van Tartwijk J, Overeem K, Vermunt JD, van der Vleuten CP.
2005. Conditions for successful reflective use of portfolios in under-
graduate medical education. Med Educ 39(12):1230–1235.
Driessen E, van Tartwijk J, van der Vleuten C, Wass V. 2007. Portfolios in
medical education: Why do they meet with mixed success? A systematic
Review Med Educ 41:1224–1233.
duBoulay C. 2000. From CME to CPD: Getting better at getting better? BMJ
320(7332):393–394.
Ebell M. 1999. Information at the point of care: Answering clinical
questions. J Am Board Fam Pract 12:225–235.
Eva K, Regehr G. 2005. Self-assessment in the health professions: A
reformulation and research agenda. Acad Med 80:s46–s54.
Federation of Medical Regulatory Authorities of Canada. [Accessed 25
March 2013] Available from http://www.fmrac.ca/policy/revalidation_
eng.html
Finlay IG, Maughan TS, Webster DFT. 1998. A randomized controlled study
of portfolio learning in undergraduate cancer education. Med Educ
32:172–176.
Forster AJ, Clark HD, Menard A, Dupuis N, Chernish R, Chandok N. 2004.
Adverse events among medical patients after discharge from hospital.
CMAJ 170(3):345–349.
Galbraith RM, Hawkins RE, Holmboe ES. 2008. Making self-assessment
more effective. JCHEP 28(1):20–24.
Green M, Reddy SG, Holmboe ES. 2009. Teaching and evaluating point of
care learning with an internet-based clinical-question portfolio. JCEHP
29(4):209–219.
Grimshaw JM, Eccles MP, Walker AE, Thomas RE. 2002. Changing
physicians’ behaviour: What works and thoughts on getting more
things to work. JCEHP 22(4):237–243.
Grol R, Baker R, Moss F. 2002. Quality improvement research:
Understanding the science of change in health care. Qual Saf Health
Care 11(2):110–111.
Gurusamy K, Aggarwal R, Palanivelu L, Davidson BR. 2008. Systematic
review of randomized controlled trials on the effectiveness of virtual
reality training for laparoscopic surgery. Br J Surg 95:1088–1097.
Hall P, Byszewski A, Sutherland S, Stodel EJ. 2012. Developing a
sustainable electronic portfolio (ePortfolio) program that fosters
reflective practice and incorporates CanMEDS competencies into the
undergraduate medical curriculum. Acad Med 87(6):744–751.
Harris P, Snell L, Talbot M, Harden RM. 2010. Competency-based medical
education: Implications for undergraduate programs. Med Teach
32:646–650.
InfoPOEMs. 2012. accessed through the Canadian Medical Association at
http://www.cma.ca/clinicalresources/k4p
Iobst WF, Sherbino J, Cate OT, Richardson DL, Dath D, Swing SR, Harris P,
Mungroo R, Holmboe ES, Frank JR. 2010. Competency-based medical
education in postgraduate medical education. Med Teach 32:651–656.
Institute of Medicine Report. 1999. To Err is Human: Building a
Safer Health System. [Accessed 25 March 2013] Available from
http://iom.edu/Reports/1999/To-Err-is-Human-Building-A-Safer-Health-
System.aspx
Kardos RL, Cook JM, Butson RJ, Kardos TB. 2009. The development of an
ePortfolio for life-long reflective learning and auditable professional
certification. Eur J Den Educ 13(3):135–141.
ePortfolios for CPD
293
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Reg
ina
on 0
9/07
/13
For
pers
onal
use
onl
y.

Mann K, Gordon J, MacLeod A. 2007. Reflection and reflective practice in
health professions education: A systematic review. Adv Health Sci Educ
Theory Pract 14(4):595–621.
McGaghie MC, Issenberg AB, Petrusa ER, Scalese RJ. 2006. Effect of practice
on standardized learning outcomes in simulation-based medical
education. Med Educ 40:792–797.
McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristofaro A, Kerr EA.
2003. The quality of health care delivered to adults in the United States.
NEJM 348:2635–2645.
MedBiquitous. 2012. [Accessed 25 March 2013] Available from http://
www.medbiq.org/, and standards web page at http://www.medbi-
q.org/std_specs/standards/index.html#ActivityReport
Moon J. 2004. A handbook of reflective and experiential learning: Theory
and practice. London: Routledge-Falmer.
Moore DE, Green JS, Gallis HA. 2009. Achieved desired results and
improved outcomes: Integrating planning and assessment throughout
learning activities. JCEHP 29:1–15.
Overeem K, Faber M, Arah O, Elwyn G, Lombarts K, Wollersheim H, Grol R.
2007. Doctor performance assessment in daily practice: Does it help
doctors or not? A systematic review. Med Educ 41:1039–1049.
Parboosingh JT. 2002. Physician communities of practice: Where learning
and practice are inseparable. JCEHP 22(4):230–236.
Ross S, MacLachlan A, Cleland J. 2009. Students’ attitudes towards the
introduction of a Personal and Professional Development portfolio:
Potential barriers and facilitators. BMC Med Educ 9:69. doi:10.1186/
1472-6920-9-69.
Royal College of Physicians and Surgeons of Canada. [Accessed 25 March
2013] Available from www.royalcollege.ca
Scholes J, Webb C, Gray M, Endacott R, Miller C, Jasper M, McMullan M.
2004. Making portfolios work in practice. J Adv Nurs 46(6):595–603.
Schon D. 1987. Educating the reflective practitioner. San Francisco. Jossey-
Bass.
Sutherland S, Powell A. 2007. JISC InfoNet. http://www.jiscinfonet.ac.uk/
infokits/e-portfolios/; updated 14 November 2012.
Teunissen PW, Dornan T. 2008. Lifelong learning at work. BMJ
336:667–669.
Tochel C, Haig A, Hesketh A, Cadzow A, Beggs K, Colthart I, Peacock H.
2009. The effectiveness of portfolios for post-graduate assessment and
education: BEME Guide No. 12. Med Teach 31:299–318.
Tompkins M, Paquette-Frenette D. 2010. Learning portfolio models in
health regulatory colleges in Ontario, Canada. JCEHP 30(1):57–64.
van der Veer SN, de Keizer NF, Ravelli ACJ, Tenkink S, Jager KJ. 2010.
Improving quality of care. A systematic review of how medical
registries provide information feedback to health care providers. Int J
Med Inform 79(5):305–323.
van Tartwijk J, Driessen E. 2004. ePortfolio scenarios: Types of
ePortfolios. [Accessed 25 March 2013] Available from http://insight.
eun.org/ww/en/pub/insight/school_innovation/eportfolio_scenarios/
portfolios_types.htm
Wassef ME, Riza L, Maciag T, Worden C, Delaney A. 2012. Implementing a
competency-based electronic portfolio in a graduate nursing program.
Comput Inform Nurs 30(5):249–250.
Wilkinson TJ, Challis M, Hobma SO, Newble DI, Parboosingh JT, Sibbald
RG, Wakeford R. 2002. The use of portfolios for assessment of the
competence and performance of doctors in practice. Med Educ
36(10):918–924.
J. A. Gordon & C. M. Campbell
294
Med
Tea
ch D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Reg
ina
on 0
9/07
/13
For
pers
onal
use
onl
y.