Embed Size (px)
Citation preview

The Radiographic Pattern of Polyarthritis in Reiter’s Syndrome Stephen D. Sholkoff, Morton G. Glickman and Howard L. Steinbach
Roentgenographic and scintiphotographic studies of the arthritis of Reiter’s syndrome demonstrate concurrent involvement of various small joints of the lower extremities often associated with sacroiliitis. The most frequently affected sites are the heels, toes, sacroiliac joints, and ankles and tarsals. Simultaneous involvement of these sites is characteristic of this syndrome.
Previous articles have enumerated roent- genographic findings in Reiter’s syndrome (1-7). Predilection for involvement of the sacroiliac joints and the peripheral joints of the lower extremities has been noted; however, the tendency of these sites to be concurrently involved has not been em- phasized.
To determine the frequency of involve- ment of combinations of joints, we reviewed the roentgenograms and scintiphotographs of our large series of patients who had Reiter’s syndrome. If it can be shown that certain combinations of joint involvement are characteristic of Reiter’s syndrome, a presumptive diagnosis might then be justi- fied in the absence of classic clinical signs.
MATERIALS AND METHODS Between 1966 and 1969, 42 patients with Reiter’s
syndrome were examined in the Radiology Depart-
From the Department of Radiology, Universi ty of California school of Medicine, San Francisco, Calif.
Supported by NIH Grant GM 01272 from the National Institute of General Medical Sciences, and USPHS Grant AM 02589.
SI-JZPHEN D. SHOLKOFF, MD: USPHS Research Fel- low in Diagnostic Radiology: M O U ~ N c. CLICKMAN, MD; HOWARD L. WEINBACH, MD: Department of Radi- ology, University of California, School of Medicine, San Francisco, Calif.
Reprint requests should be addressed to S. D. Sholkoff, MD.
Submitted for publication July 1970; accepted Nov 18, 1970.
ment of the University of California Hospital. The methods of roentgenographic and scintiphotographic examinations, including positioning and technical details, were described elsewhere (1, 8). The diag- nosis of Reiter’s syndrome was established, using the criteria described by Engelman (9).
All 42 patients were examined roentgenograph- ically. In 17, roentgenograms of all joints were repeated at intervals of 1 4 3 months (median, 15 months). Roentgenographic signs of arthritis (effu- sion, tenosynovitis, erosions, periostitis and ankylo- sis) were judged as present or absent. Scintiphoto- graphs, using an Anger camera and 10 mCi of RmTc-pertechnetate, were taken in 7 patients. They were repeated in 3 patients at 2 weeks, 4% weeks and 2 months (8). None of the patients was younger than 10 years, 4 were 50 years or older, and only 2 were women (I).
RESULTS The most frequently affected sites were
the heels, toes, sacroiliac joints, and the ankles and tarsals. The ankles and tarsals were considered together in the tabulation. The frequency with which these four sites were affected simultaneously was as follows: all four sites in 5 patients, three in 7 pa- tients, two in 12 patients, and one in 7 patients. One patient had roentgen evi- dence of polyarthritis without involvement of any of these four sites, and in 10 pa- tients, the results of studies were normal. Of 32 patients with roentgenographically abnormal joints, more than one joint area was involved in 29.
Calcaneur. Roentgenograms demon-
Arthritis and Rheumatism, Vol. 14, No. 4 (July-August 1971) 551

fig
1.
Rei
teh
synd
rom
e in
you
ng m
an w
ho h
as s
hown
sym
ptom
s fo
r le
ss th
an 6
mon
ths.
(le
ft) R
ight
foot
. Pe
riarti
cula
r ero
sive
lesio
ns a
nd d
estru
ctio
n of
car
- til
age
are
wen
at
tad-
met
atar
sal
join
ts a
nd i
nter
met
atar
sal j
oint
s.
Perio
stiti
s th
icken
s sh
aft
of s
econ
d m
etat
arsa
l. (ri
ght)
Left
foot
. Ta
rsal
-met
atar
sal j
oint
s ar
e in
tact
. Th
ere
is m
ild s
oft
tissu
e sw
ellin
g Ov
er gr
eat t
oe,
and
slig
ht f
orm
atio
n of
per
iost
ial n
ew b
one
on s
haft
of d
ista
l pha
lanx
.

POLYARTHRITIS IN REITER’S SYNDROME
strated arthritis of the heels (19 plantar and 11 posterior, and 7 in both areas, simultaneously) in 23 patients. Associated sacroiliitis was observed in 9. Simultaneous disease of the ankles and tarsals, toes, or sacroiliac joints was evident in all but 4. Heel changes were not an isolated finding in any of the patients.
Sacroiliac. In only 2 of 17 patients with sacroiliitis was neither toe, tarsal, ankle or heel involved. In 1 of those pa- tients, effusion was present in the knee. Subsequent scintiphotography in this pa- tient demonstrated arthritis of the right ankle. Sacroiliitis was an isolated finding in 1 patient. Only 1 patient with roentgeno- graphically abnormal joints had neither sacroiliitis nor heel involvement.
Ankle, tarsus. In 13 of 15 patients
with ankle or tarsal involvement, arthritis was observed in at least one of the other three typical joints. In only 1 of 15 patients was the ankle or tarsus involved alone.
roes. Of 19 patients with toe involve- ment, 17 had disease in the heel as well, and 10 had sacroiliitis. I n all 19, either sacroiliac or heel disease was evident con- currently. Interestingly, in 14, the inter- phalangeal joint of the great toe was in- volved. In no patient was involvement of the toes the only abnormality.
Hands. Disease in the hand or wrist was seen in only 7 patients. It was associ- ated with sacroiliitis in 6, and with severe and extensive disease of the feet in 5.
Scintiphotography. Scintiphotography in 7 patients confirmed the distribution of
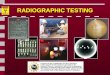
Fig 2. Scintiphotographs of feet in same patient on same day. In right foot, abnormal accumulation of activity corresponds to tarsal-metatarsal joint lesions seen in roentgenogram. In left foot, abnormal accumulation of activity corresponds to interphalangeal joint and metatarsal-phalangeal joint of great toe, indicating active inflammation of these joints. Tarsal-metatarsal joints and distal portion of tarsus are uninvolved. Symmetric accumulation of activity seen over proximal tarsus is due to superimposition of ankle joint in this view. Side view (not shown) demonstrated no abnormal accumulation in left tarsus.
Arthritis and Rheumatism, Vol. 14, No. 4 (July-August 1971) 553

Fig
3. Re
iter's
syn
drom
e in
you
ng m
an w
ith s
ympt
oms
of a
bout
3 m
onth
s' du
ratio
n.
(left)
Rig
ht h
eel. No
roen
tgen
ogra
phic
abno
rmal
ity.
(rig
ht) S
cintip
hoto
grap
h of
bot
h he
els. C
obal
t m
arke
r abo
ve t
anus
indi
cate
s rig
ht fo
ot.
Ther
e is
abn
orm
al a
ccum
ulat
ion
of a
ctiv
ity c
orre
spon
ding
to
plan
tar
surfa
ce o
f rig
ht c
alcan
eus.
Left
calca
neus
sho
rn n
o ab
norm
ality
. In
bot
h fe
et,
abno
rmal
acc
umul
atio
n of
act
ivity
is s
een
in m
etat
arsa
l-pha
lang
eal r
egio
ns.

POLYARTHRITIS IN REITER’S SYNDROME
active arthritis, as shown on roentgeno- grams (Fig 1, 2). In 5 of 7 patients, scinti- photography also demonstrated arthritic activity in joints that appeared normal on roentgenograms (Fig 3). In occasional joints, arthritic activity not suspected clinically or roentgenographically, was demonstrated by scintipho tography .
DISCUSS 10 N The most helpful observation in our
analysis of these cases of Reiter’s syndrome was the concurrent, usually asymmetric, in- volvement of the various small joints of the lower extremities accompanied with sacro- iliitis. In 26 of 33 patients, at least 2 of these joints were involved, and in 13 pa- tients, 3 or more joints were affected simul- taneously. This report emphasizes the fre- quency with which the heels, toes (particu- larly the interphalangeal joint of the great toe), sacroiliac joints, ankles and tarsals are affected concurrently in Reiter’s syndrome. For example, only I patient with abnormal joints had neither heel nor sacroiliac dis- ease. The joint structure can only respond to insult in a limited number of ways, re- gardless of etiology. Hence, a presumptive diagnosis may be inferred on the basis of the distribution of arthritis, rather than on characteristic articular changes.
The patterns of involvement, as modified by the scintiphotographs, were even more characteristic of this disease. Scintiphotog- raphy has not been used extensively in clinical evaluation of arthritis, and was performed in only a few of the patients
included in this report. I t is, however, a more sensitive indicator of early joint in- flammation than is roentgenography (6). Therefore, scintiphotography may be su- perior to roentgenography in depicting con- current involvement of several joints, with a pattern characteristic of Reiter’s syn- drome.
1.
2.
3.
4.
5.
6.
7.
8.
9.
REFERENCES Sholkoff SD, Glickman MG, Steinbach HL: Roentgenology of Reiter’s syndrome. Radi-
Csonka G Reiter’s syndrome. Ergebn Inn Med Kinderheilk 23:125-189, 1965 Mason RM, Murray RS, Oates JK, et al: A comparative radiological study of Reiter’s disease, rheumatoid arthritis and ankylos- ing spondylitis. J Bone Joint Surg (Lon- don) 41B:137-148, 1959 Murray RS, Oates JK, Young AC: Radio- logical changes in Reiter’s syndrome and arthritis associated with urethritis. J Fac Radiol 937-43, 1958 Peterson CC Jr, Silbiger M L Reiter’s syn- drome and psoriatic arthritis; their roent- gen spectra and some interesting similari- ties. Amer J Roentgen 101:860-871, 1967 Reynolds DF, Csonka GW: Radiological aspects of Reiter’s syndrome (‘venereal’ ar- thritis). J Fac Radiol 9:44-49, 1958 Weldon WV, Scalettar R: Roentgen changes in Reiter’s syndrome. Amer J Roentgen 86: 344-350, 1961 Sholkoff SD, Glickman M G Scintiphoto- graphic evaluation of arthritis activity. In- vest Radiol 4207-214, 1969 Engelman EP, Weber HM: Reiter’s syn- drome. Clin Orthop 57:19-29. 1968
ology 97~497-504, 1970
Mhritb 8d Rheumatism, Val. 14, NO. 4 (Juh-Aupd 1971) 555