Embed Size (px)
Citation preview
Brain (1994), 117, 1169-1181
The pathogenesis of gait hypokinesia inParkinson's diseaseMeg E. Morris,1-2 Robert Iansek,2 Thomas A. Matyas1 and Jeffery J. Summers3
department of Behavioural Health Sciences, La TrobeUniversity, Bundoora, the 2Geriatric Neurology Service andGeriatric Research Unit, Kingston Centre, Cheltenham andthe 3Department of Psychology, The University of SouthernQueensland, Toowoomba, Australia
Correspondence to: Meg Morris, Geriatric NeurologyResearch Unit, Kingston Centre, Warrigal Road,Cheltenham 3192, Australia
SummaryTo identify the fundamental deficit in gait hypokinesia inParkinson's disease (PD) we conducted a series ofexperiments that compared PD subjects with age- and height-matched controls in their capacity to regulate either stridelength, cadence (steps per minute) or both parameters tothree conditions. In the first condition the spatial and temporalparameters of gait were documented for slow, normal andfast walking. The second condition compared parkinsoniangait with the walking pattern of elderly controls whilstcontrolling for two movement speeds: fast (control preferred)speed and slow (PD preferred) speed. In the third conditionwe examined the ability of PD subjects to regulate oneparameter (e.g. stride length) when the other two parameters(e.g. velocity and cadence) were held at control values. Atotal of 34 PD subjects and 34 matched controls were testedusing a foolswitch stride analysis system that measured thespatial and temporal parameters of gait for a series of 10 mwalking trials. Parkinsonian subjects exhibited marked gaithypokinesia in each of the experiments. Although they retainedthe capacity to vary their gait velocity in a similar manner
Key words: gait; Parkinson's disease; movement disorders
to controls, their range of response was reduced. Within thelower velocity range, PD subjects could vary their speed ofwalking by adjusting cadence and, to a lesser extent, stridelength. However, when the speed of walking was controlled,the stride length was found to be shorter and the cadencehigher in PD subjects than in controls. Stride length couldnot be upgraded by internal control mechanisms in responseto a fixed cadence set for age and height-matched velocity.In contrast, cadence was readily modulated by external cuesand by internal control mechanisms when stride length wasfixed to the values obtained for age- and height-matchedcontrols. It was concluded that regulation of stride length isthe fundamental problem in gait hypokinesia and the relativeincrease in cadence exhibited by PD subjects is a compensatorymechanism for the difficulty in regulating stride length. Thesefindings are discussed in the context of the hypothesized roleof the basal ganglia in generating internal cues for themaintenance of the gait sequence and in relation to thestructuring of movement rehabilitation strategies.
IntroductionParkinson's disease (PD) is a chronic, progressiveneurological condition which affects approximately one inevery 100 people over the age of 65 years (Schoenberg,1987). Gait disorders are a hallmark of the condition and areassociated with a loss of independence (Schenkman et al.,1989) and an increased incidence of falls (Aita, 1982; Paulsonet al., 1986; Koller et al., 1989). The main approach to thetreatment of gait disorders in PD has been pharmacologicalintervention, most notably dopamine substitutes such aslevodopa. However, up to 50% of patients develop motorfluctuations and resistance to medication subsequent to thefirst 5 years of administration (Marsden etal., 1982; Klawans,1986). The cause of PD remains unknown and because no
cure for the condition has been found, patients face arelentless deterioration in mobility which can result in theeventual need for custodial care.
Despite the frequency of gait disorders in PD, there havebeen few attempts to quantify the locomotor pattern orto identify the fundamental motor control deficits inparkinsonian gait. This appears to be particularly the case inrelation to gait hypokinesia (slowness) which is one ofthe most frequently observed movement disorders in PD.Typically, slowness of walking is associated with a reducedstride length, decreased cadence (steps per minute) and anincrease in the proportion of the gait cycle spent in thedouble limb support phase of stance (DLS) (Knutsson and
Oxford University Press 1994
by guest on October 24, 2014
Dow
nloaded from

1170 M. E. Morris et al.
Martensson, 1971; Knutsson, 1972; Murray et al., 1978;Stern et al., 1983; Blin et al., 1990, 1991; Bowes et al.,1990; Brooks et al., 1990). However, clinical observationshave led some to suggest that when velocity is taken intoaccount, the walking cadence is in fact higher and the stridelength shorter in PD patients than elderly controls (e.g. Walland Turnbull, 1992). In contrast, investigations by Stern et al.(1983) and Blin et al. (1990) suggested that the normalrelationships between velocity, cadence and stride length arepreserved in PD.
Both Stern et al. (1983) and Blin et al. (1990) recordedstride length and cadence values from PD subjects walkingat their preferred velocity and compared the values withthose obtained for age-matched controls. They then plottedstride length against velocity for the two data sets and foundthat similar linear models could accommodate the results.Comparable linear models were also apparent for therelationship between cadence and velocity in PD subjectsand controls (Stern et al., 1983). From this it was concludedthat the relationships between velocity, stride length andcadence were not significantly different from normal.However, only a single set of coordinates for stride lengthand cadence was taken from each subject in these studies,those associated with the preferred walking speed. Thevelocity range encompassing the preferred speeds of fastnormals down to the slow speed of hypokinetic PD subjectsappears to be very large by comparison with the velocityrange than an individual PD subject is likely to exhibit. Itremains possible that substantially different slope coefficientscould occur within a limited velocity span for each individualwith PD without this effect becoming apparent in the contextof a population-wide model, constructed using only one pairof values from each subject. Because the within-subjectchanges in cadence or stride length with different velocitiesneed not follow the linear relationships shown by individualdifferences in preferred walking speeds and their associatedcadences or stride lengths, the clinical observations mightnot, in fact, be contradictory to the observations of Sternand Blin. However, resolution of this apparent discrepancyrequires further experimentation to compare within-subjectdifferences with individual differences in gait parameters fora range of walking speeds.
The inadequate documentation of the basic relationshipsbetween the spatial and temporal parameters of gait for arange of walking speeds in individuals with PD is mirrored bya lack of knowledge on the pathogenesis of gait hypokinesia. Itis currently not clear why basal ganglia dysfunction associatedwith PD leads to a slower walking pattern. Most knowledgeabout the underlying mechanisms of hypokinesia is derivedfrom studies on sequential movements of the upper limbs inprimates and in individuals with PD. A number of thesestudies have shown that normally the basal ganglia interactclosely with the supplementary motor area in the elaborationof well-learned, repetitive sequences of movement (Rolandet al., 1982; Seitz and Roland, 1992). For highly automaticmovements of this type, neurons in the globus pallidus of
the basal ganglia are seen to discharge phasically at the endof each movement in the sequence. It has been suggestedthat the phasic activity of globus pallidus turns off preparatoryor 'set-related' activity in the supplementary motor area andacts to trigger each submovement in the sequence, therebyallowing well-learned movements to run automatically (seeBrotchie et al., \99\a,b). There is growing evidence that inPD the basal ganglia cue is defective and leads to disorderedpreparation for each submovement in the sequence (seeGeorgiou et al., 1993; Martin et al., 1994). In addition, ifthe basal ganglia cue is smaller than normal or absent, thenthe switch between one movement and the next may beslower than average, with the whole sequence taking muchlonger to execute.
Given that locomotion is essentially an automatic move-ment sequence, similar deficits might be expected to underliegait hypokinesia in PD. Although animal experimentationsuggests that the stepping mechanisms for gait are largelycontrolled at spinal and brainstem levels (e.g. Grillner,1975) it is clear that supraspinal influences from the cortex,cerebellum and the basal ganglia can influence the excitationof spinal locomotor networks in order to alter the timing orsize of consecutive footsteps (Patla, 1991). The finding thatvelocity and stride length both increase when PD patientsare provided with floor makers to externally cue the steppingpattern (Martin, 1967; Forssberg et al., 1984; Richards et al.,1990; Bagley et al., 1991) lends support to the idea that gaithypokinesia results from a deficiency of the internal cueingmechanism of the basal ganglia, which in conjunction with thesupplementary motor area, normally regulates performance ofautomatic movement sequences.
Along with pharmacological intervention, physiotherapyhas been advocated for the management of gait disorders inPD (e.g. Palmer et al., 1984, 1986; Yekutiel et al., 1991).As yet the effectiveness of physiotherapy for PD has notbeen firmly established and the type of physiotherapy thatshould be used in gait training is unclear. Whereas controlledclinical trials by Gibberd et al. (1981) and Pederson et al.(1990) failed to identify significant benefits for gait training,studies by Palmer et al. (1984, 1986), Banks and Caird(1989), Hurwitz (1989) and Formisano et al. (1992) claimedthat exercise therapy had a positive effect on walking ability.However, none of these approaches provide clear guidelinesfor the management of gait hypokinesia in PD. The lack ofknowledge of underlying mechanisms of hypokinesia hasmade it difficult to structure physical therapies for thiscondition upon a rational basis.
In light of the need to establish a stronger theoretical basisfor the rehabilitation of PD gait, coupled with the inadequatedescription of the spatiotemporal parameters of gait for arange of walking speeds that currently exists, a detailedexamination of the underlying mechanisms of gait disturbancein PD was undertaken. We conducted a series of experimentsthat examined the capacity of PD patients to vary theirvelocity over a large range and investigated the manner inwhich stride length and cadence were regulated in order to
by guest on October 24, 2014
Dow
nloaded from

Gait hypokinesia in Parkinson's disease 1171
change velocity. We then analysed the relationships betweenthe temporal and spatial parameters of gait when the velocityof walking was controlled. Finally, we examined the abilityof PD patients to regulate one gait parameter (e.g. stridelength) when the other two parameters (e.g. velocity andcadence) were held at control values. These experimentsrevealed that PD subjects had the capacity to vary their gaitvelocity in a similar manner to controls although the rangeof response was diminished. However, when the speed ofwalking was controlled, the stride length was shorter and thecadence was higher in PD patients than controls. The resultsalso showed that gait hypokinesia was fundamentally due toan inability to regulate stride length using internal motorcontrol mechanisms. By contrast, cadence was easilyregulated by both external cues and internal controlmechanisms. The results provide convincing evidence thatthe relative increase in cadence seen in PD is a compensatorymechanism for difficulty in regulating stride length. Thesignificance of these results is discussed in relation to thepossible underlying mechanisms for the reduced stride lengthand the relevance of the findings for gait rehabilitationstrategies is considered.
MethodsSubjectsA total of 68 subjects were recruited for the series ofexperiments. The sample included 34 patients with idiopathicPD diagnosed by a neurologist and 34 age-, sex- and height-matched control subjects with no history of neurologicaldisorder. There were 22 PD subjects and 22 controls in Study1, 18 PD subjects and 18 controls in Study 2 and 12 PDsubjects and 12 controls in Study 3. Subjects in Study 2 hadalso participated in the first investigation.
To be included in the first study, subjects were required tobe >60 years of age, medically stable and able to walk10 m 10 times with only stand-by supervision from aphysiotherapist. The inclusion criteria for Study 2 were thesame with the exception that PD subjects needed to be ableto achieve gait velocity values comparable with normalswhen encouraged to walk faster. For Study 3, PD subjectswere included if they could perform up to 20 walks alonga 10 m walkway with only stand-by supervision from aphysiotherapist and if they demonstrated gait hypokinesia ongait analysis. To be included in Study 3 PD subjects alsoneeded to achieve gait velocity values which were comparablewith normals when encouraged to walk faster. Controlsubjects were included in Study 3 provided they couldperform up to 20 walks along a 10 m walkway with onlystand-by supervision from a physiotherapist. All subjectsprovided informed consent according to the declaration ofHelsinki (1964). Subjects were excluded if they had ahistory of neurological conditions other than PD; if they hadmusculoskeletal, cardiovascular or visual disturbances thataffected walking ability or dementia as indicated by a score<24 on the Short Test of Mental Status (Kokmen etai, 1987).
Tables 1 and 2 summarize the subject characteristics foreach of the investigations. Measures of age, height andweight were obtained for all subjects because these factorsare reported predictors of walking velocity (Grieve and Gear,1966; Du Chatinier et al., 1970). The walking pattern of PDsubjects was analysed in the interval 0.5-3 h followingadministration of their morning dose of PD medication. Themean interval between drug administration and gait analysiswas 1.5± 0.88 h. For PD subjects the level of functionaldisability was also determined by a neurologist by adminis-tration of the modified Webster scale (Webster, 1968) and theHoehn and Yahr scale (Hoehn and Yahr, 1967). Subjects in thefirst two studies exhibited mild to moderate levels of disabilityas indicated by a mean Webster score of 16.77 and a meanHoehn and Yahr score of 3.04, whereas subjects in Study 3were more mildly affected, with a mean score of 15.9 on theWebster scale and a mean score of 2.5 on the Hoehn andYahr scale.
ApparatusIn all three studies gait analyses were conducted on a 10 mwalkway using a commercially available clinical strideanalyser (B and L Engineering, Santa Fe Springs, California,USA). The system enables measurement of the spatial(distance) and temporal (timing) characteristics of the footsteppattern and consists of a set of foot switches, a start-stopcontroller and a data storage unit. Foot switches were wornas insoles in the subjects shoes and contained four sensorsfor detection of floor contact for the heel, first metatarsal,fifth metatarsal and great toe. The start-stop controller wasactivated by a light sensitive device, which was triggered bylights at the start and end of the 10 m walkway. The recordercollected data on the elapsed time of each run, the temporalcharacteristics of foot-switch patterns and the mean stridelength for the 10 m walk. The status of foot switches wassampled every 2 ms with data stored only when a changeoccurred and remained for at least 10 ms in one or moreswitches. An IBM compatible PC and 265k RAM runningDOS version 3.1 (C) was used for data transfer, analysis andstorage. The application software used was 'PCSA' version1.03 (C) (B and L Engineering, 1988).
In Study 3, a quartz electronic metronome (SuntechElectronics Corporation, Seoul, Korea) was used to set thecadence rate of PD subjects to that of controls. The metronomewas a small box, measuring 12.5X63X31 mm, and was wornon a waist belt. The metronome was calibrated at 40-208beats per min with an accuracy of 0.02% and the pitch wasset at 6E (82.41 Hz). In Study 3, visual cues were alsoutilized to match the stride length of PD subjects to that ofcontrols. These cues were floor markers made of laminatedstrips of white cardboard that measured 50X500X1 mm.Each marker was placed on the gait walkway, which wastiled in grey-green linoleum, at a distance equivalent to themean step length for the subjects matched control.
by guest on October 24, 2014
Dow
nloaded from
1172 M. E. Morris et al.
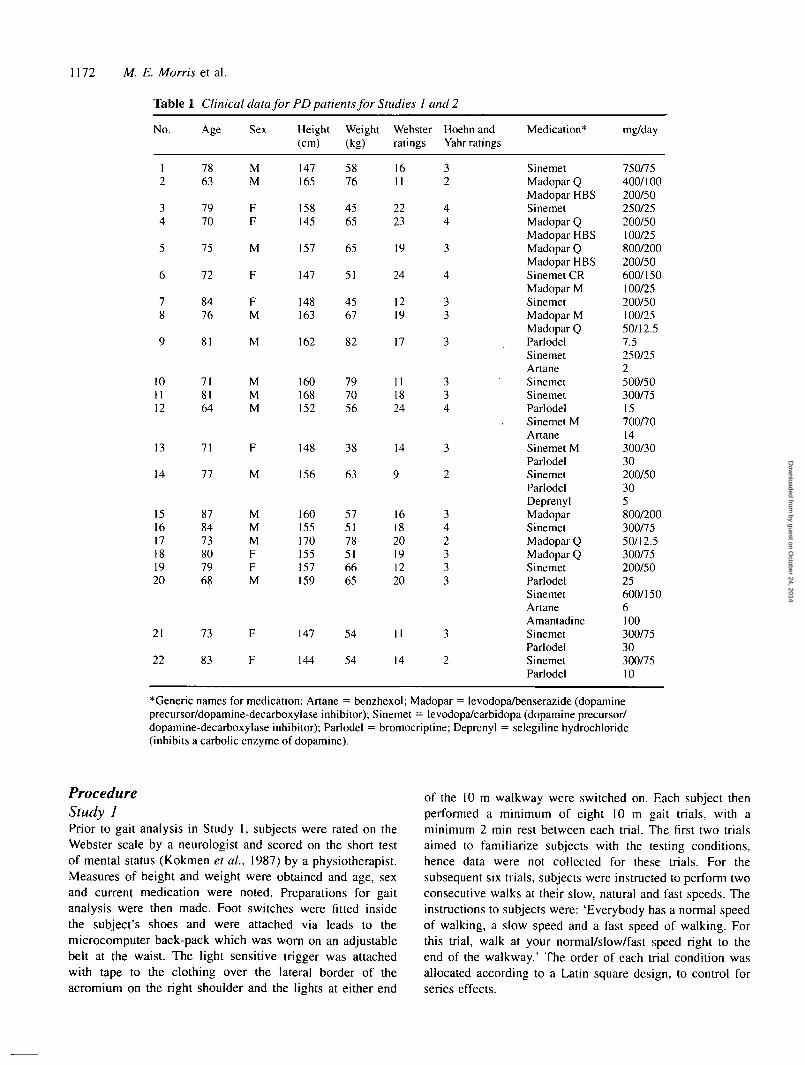
Table 1 Clinical data for PD patients for Studies 1 and 2
No. Age Sex Height Weight Webster Hoehn and Medication* mg/day(cm) (kg) ratings Yahr ratings
12
34
5
6
78
7863
7970
75
72
8476
MM
FF
M
F
FM
147165
158145
157
147
148163
5876
4565
65
51
4567
1611
2223
19
24
1219
32
44
3
4
33
81 M 162 82 17
101112
13
14
151617181920
21
22
718164
71
77
878473807968
73
83
MMM
F
M
MMMFFM
F
F
160168152
148
156
160155170155157159
147
144
797056
38
63
575178516665
54
54
111824
14
9
161820191220
II
14
334
3
2
342333
3
2
SinemetMadopar QMadopar HBSSinemetMadopar QMadopar HBSMadopar QMadopar HBSSinemet CRMadopar MSinemetMadopar MMadopar QParlodelSinemetArtaneSinemetSinemetParlodelSinemet MArtaneSinemet MParlodelSinemetParlodelDeprenylMadoparSinemetMadopar QMadopar QSinemetParlodelSinemetArtaneAmantadineSinemetParlodelSinemetParlodel
750/75400/100200/50250/25200/50100/25800/200200/50600/150100/25200/50100/2550/12.57.5250/252500/50300/7515700/7014300/3030200/50305800/200300/7550/12.5300/75200/5025600/1506100300/7530300/7510
*Generic names for medication: Artane = benzhexol; Madopar = levodopa/benserazide (dopamineprecursor/dopamine-decarboxylase inhibitor); Sinemet = levodopa/carbidopa (dopamine precursor/dopamine-decarboxylase inhibitor); Parlodel = bromocriptine; Deprenyl = selegiline hydrochloride(inhibits a carbolic enzyme of dopamine).
ProcedureStudy 1Prior to gait analysis in Study 1, subjects were rated on theWebster scale by a neurologist and scored on the short testof mental status (Kokmen et al., 1987) by a physiotherapist.Measures of height and weight were obtained and age, sexand current medication were noted. Preparations for gaitanalysis were then made. Foot switches were fitted insidethe subject's shoes and were attached via leads to themicrocomputer back-pack which was worn on an adjustablebelt at the waist. The light sensitive trigger was attachedwith tape to the clothing over the lateral border of theacromium on the right shoulder and the lights at either end
of the 10 m walkway were switched on. Each subject thenperformed a minimum of eight 10 m gait trials, with aminimum 2 min rest between each trial. The first two trialsaimed to familiarize subjects with the testing conditions,hence data were not collected for these trials. For thesubsequent six trials, subjects were instructed to perform twoconsecutive walks at their slow, natural and fast speeds. Theinstructions to subjects were: 'Everybody has a normal speedof walking, a slow speed and a fast speed of walking. Forthis trial, walk at your normal/slow/fast speed right to theend of the walkway.' The order of each trial condition wasallocated according to a Latin square design, to control forseries effects.
by guest on October 24, 2014
Dow
nloaded from
Gait hypokinesia in Parkinson's disease 1173
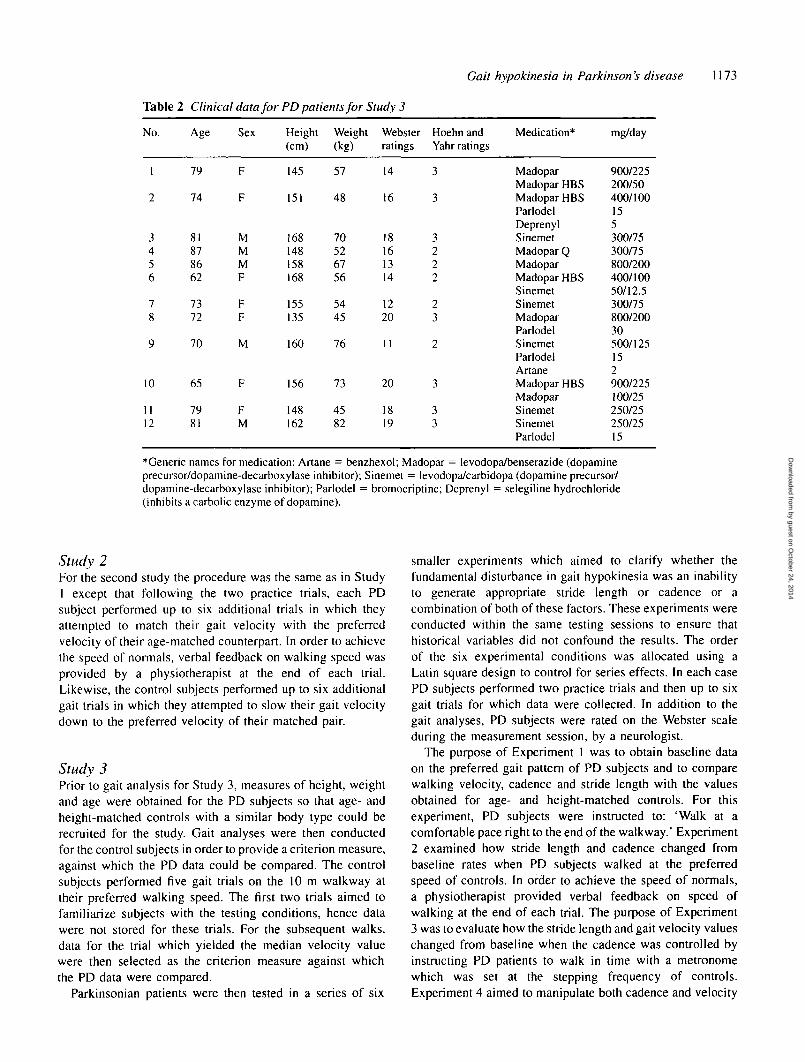
Table 2 Clinical data for PD patients for Study 3
No.
1
2
3456
78
9
10
1112
Age
79
74
81878662
7372
70
65
7981
Sex
F
F
MMMF
FF
M
F
FM
Height(cm)
145
151
168148158168
155135
160
156
148162
Weight(kg)
57
48
70526756
5445
76
73
4582
Websterratings
14
16
18161314
1220
11
20
1819
Hoehn andYahr ratings
3
3
3222
23
2
3
33
Medication*
MadoparMadopar HBSMadopar HBSParlodelDeprenylSinemetMadopar QMadoparMadopar HBSSinemetSinemetMadoparParlodelSinemetParlodelArtaneMadopar HBSMadoparSinemetSinemetParlodel
mg/day
900/225200/50400/100155300/75300/75800/200400/10050/12.5300/75800/20030500/125152900/225100/25250/25250/2515
*Generic names for medication: Artane = benzhexol; Madopar = levodopa/benserazide (dopamineprecursor/dopamine-decarboxylase inhibitor); Sinemet = levodopa/carbidopa (dopamine precursor/dopamine-decarboxylase inhibitor); Parlodel = bromocriptine; Deprenyl = selegiline hydrochloride(inhibits a carbolic enzyme of dopamine).
Study 2For the second study the procedure was the same as in StudyI except that following the two practice trials, each PDsubject performed up to six additional trials in which theyattempted to match their gait velocity with the preferredvelocity of their age-matched counterpart. In order to achievethe speed of normals, verbal feedback on walking speed wasprovided by a physiotherapist at the end of each trial.Likewise, the control subjects performed up to six additionalgait trials in which they attempted to slow their gait velocitydown to the preferred velocity of their matched pair.
Study 3Prior to gait analysis for Study 3, measures of height, weightand age were obtained for the PD subjects so that age- andheight-matched controls with a similar body type could berecruited for the study. Gait analyses were then conductedfor the control subjects in order to provide a criterion measure,against which the PD data could be compared. The controlsubjects performed five gait trials on the 10 m walkway attheir preferred walking speed. The first two trials aimed tofamiliarize subjects with the testing conditions, hence datawere not stored for these trials. For the subsequent walks,data for the trial which yielded the median velocity valuewere then selected as the criterion measure against whichthe PD data were compared.
Parkinsonian patients were then tested in a series of six
smaller experiments which aimed to clarify whether thefundamental disturbance in gait hypokinesia was an inabilityto generate appropriate stride length or cadence or acombination of both of these factors. These experiments wereconducted within the same testing sessions to ensure thathistorical variables did not confound the results. The orderof the six experimental conditions was allocated using aLatin square design to control for series effects. In each casePD subjects performed two practice trials and then up to sixgait trials for which data were collected. In addition to thegait analyses, PD subjects were rated on the Webster scaleduring the measurement session, by a neurologist.
The purpose of Experiment 1 was to obtain baseline dataon the preferred gait pattern of PD subjects and to comparewalking velocity, cadence and stride length with the valuesobtained for age- and height-matched controls. For thisexperiment, PD subjects were instructed to: 'Walk at acomfortable pace right to the end of the walkway.' Experiment2 examined how stride length and cadence changed frombaseline rates when PD subjects walked at the preferredspeed of controls. In order to achieve the speed of normals,a physiotherapist provided verbal feedback on speed ofwalking at the end of each trial. The purpose of Experiment3 was to evaluate how the stride length and gait velocity valueschanged from baseline when the cadence was controlled byinstructing PD patients to walk in time with a metronomewhich was set at the stepping frequency of controls.Experiment 4 aimed to manipulate both cadence and velocity
by guest on October 24, 2014
Dow
nloaded from
1174 M. E. Morris et al.
in order to evaluate how stride length changed or failed tochange from baseline rates. To achieve this aim PD subjectswere instructed: 'Keep in time with the metronome and walkfaster than your normal speed.' The purpose of Experiment5 was to examine whether cadence and velocity valueschanged from baseline levels when stride length was set tothe preferred step length of matched controls. The instructionsto the PD subjects for this experiment were: 'Walk at acomfortable pace over the markers on the floor, right to theend of the walkway.' Experiment 6 aimed to control boththe stride length and velocity in order to evaluate howcadence values responded or failed to respond. This wasachieved by instructing PD patients to walk faster than theirpreferred speed over white floor markers placed at thepreferred step length of controls.
For each of the six experiments in Study 3, tworepresentative gait trials were selected and the data fromthese trials were stored and later used in statistical analyses.The trials were chosen according to the aims of theexperiment. In Experiment I the two gait trials which yieldedthe closest velocity values were selected. In Experiments 2,4 and 6, PD subjects performed up to six trials until theirmean gait velocity was within 10% of the criterion value setby the age-matched controls. The data from two of the trialswhich most closely met this criterion were stored for furtheranalysis. For Experiment 3 PD subjects performed up to sixtrials until their mean cadence was within 10% of the criterionvalue set by the controls and in Experiment 5 they performedup to six trials until the means stride length was within 10%of the values set by age-matched controls. The data fromtwo of the trials which most closely met these criteria werestored for subsequent analyses.
ResultsStudy 1The first study used a two by three design with factors ofgroup (PD and age-matched controls) and walking speedcondition (slow, normal and fast). Velocity, cadence, stridelength and DLS phase duration values for each subject wereaveraged for the two trials sampled. A series of plannedcomparisons were then conducted to determine whether anyof these variables were significantly different in the PD groupcompared with the control group, for each of the threewalking speeds. Because the two groups were of equal samplesize and their data were normally distributed and showedsimilar variances, paired / tests were used for the family ofplanned comparisons.
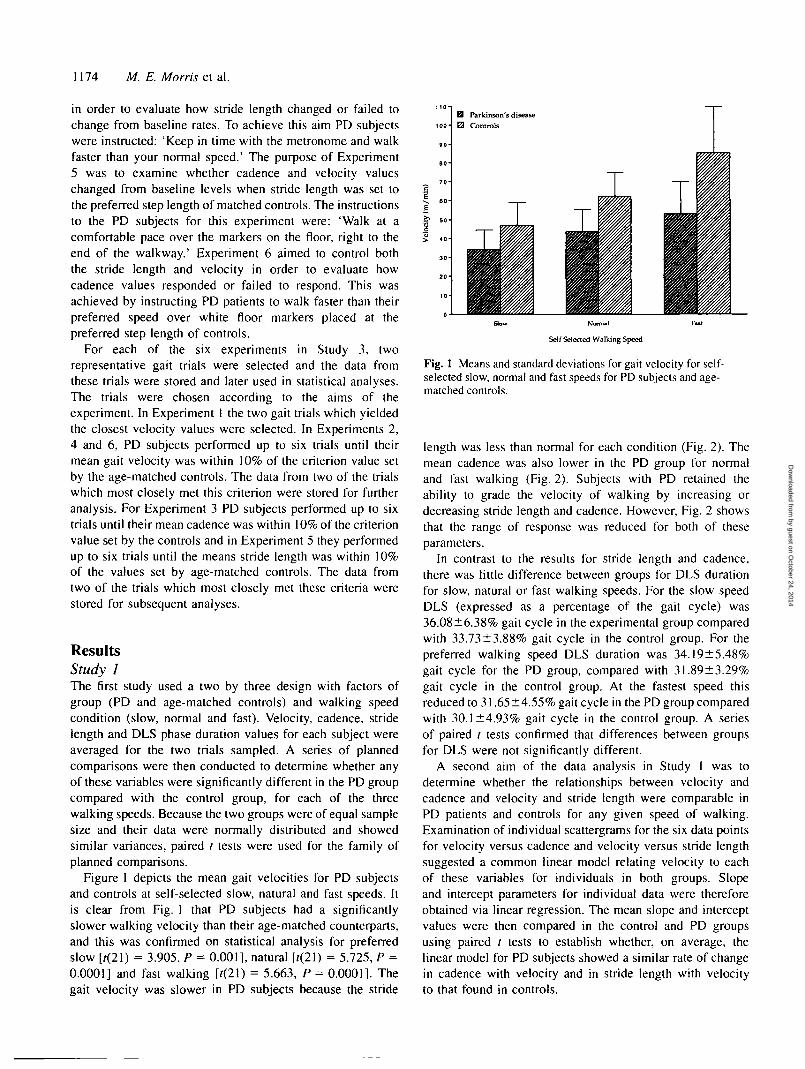
Figure 1 depicts the mean gait velocities for PD subjectsand controls at self-selected slow, natural and fast speeds. Itis clear from Fig. 1 that PD subjects had a significantlyslower walking velocity than their age-matched counterparts,and this was confirmed on statistical analysis for preferredslow [r(21) = 3.905, P = 0.001], natural [r(21) = 5.725, P =0.0001] and fast walking [f(21) = 5.663, P = 0.0001]. Thegait velocity was slower in PD subjects because the stride
Self Selected Walking Speed
Fig. 1 Means and standard deviations for gait velocity for self-selected slow, normal and fast speeds for PD subjects and age-matched controls.
length was less than normal for each condition (Fig. 2). Themean cadence was also lower in the PD group for normaland fast walking (Fig. 2). Subjects with PD retained theability to grade the velocity of walking by increasing ordecreasing stride length and cadence. However, Fig. 2 showsthat the range of response was reduced for both of theseparameters.
In contrast to the results for stride length and cadence,there was little difference between groups for DLS durationfor slow, natural or fast walking speeds. For the slow speedDLS (expressed as a percentage of the gait cycle) was36.08±6.38% gait cycle in the experimental group comparedwith 33.73±3.88% gait cycle in the control group. For thepreferred walking speed DLS duration was 34.19±5.48%gait cycle for the PD group, compared with 3I.89±3.29%gait cycle in the control group. At the fastest speed thisreduced to 31.65±4.55% gait cycle in the PD group comparedwith 30.1 ±4.93% gait cycle in the control group. A seriesof paired t tests confirmed that differences between groupsfor DLS were not significantly different.
A second aim of the data analysis in Study 1 was todetermine whether the relationships between velocity andcadence and velocity and stride length were comparable inPD patients and controls for any given speed of walking.Examination of individual scattergrams for the six data pointsfor velocity versus cadence and velocity versus stride lengthsuggested a common linear model relating velocity to eachof these variables for individuals in both groups. Slopeand intercept parameters for individual data were thereforeobtained via linear regression. The mean slope and interceptvalues were then compared in the control and PD groupsusing paired t tests to establish whether, on average, thelinear model for PD subjects showed a similar rate of changein cadence with velocity and in stride length with velocityto that found in controls.
by guest on October 24, 2014
Dow
nloaded from
Gait hypokinesia in Parkinson's disease 1175
Parkinson's diseaseControls
50 60 70
Velocity (m/min)
B
Parkinson's diseaseControls
Velocity (m/min)
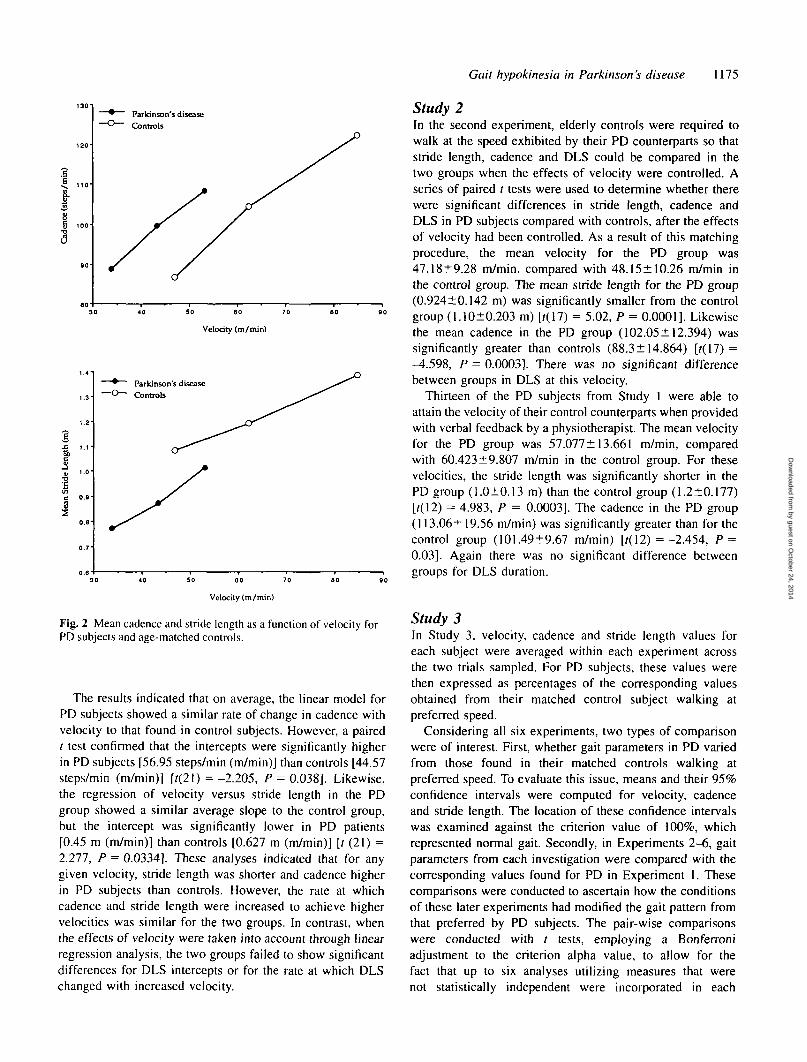
Fig. 2 Mean cadence and stride length as a function of velocity forPD subjects and age-matched controls.
The results indicated that on average, the linear model forPD subjects showed a similar rate of change in cadence withvelocity to that found in control subjects. However, a pairedt test confirmed that the intercepts were significantly higherin PD subjects [56.95 steps/min (m/min)] than controls [44.57steps/min (m/min)] [r(21) =-2.205, P = 0.038]. Likewise,the regression of velocity versus stride length in the PDgroup showed a similar average slope to the control group,but the intercept was significantly lower in PD patients[0.45 m (m/min)] than controls [0.627 m (m/min)] [t (21) =2.277, P = 0.0334]. These analyses indicated that for anygiven velocity, stride length was shorter and cadence higherin PD subjects than controls. However, the rate at whichcadence and stride length were increased to achieve highervelocities was similar for the two groups. In contrast, whenthe effects of velocity were taken into account through linearregression analysis, the two groups failed to show significantdifferences for DLS intercepts or for the rate at which DLSchanged with increased velocity.
Study 2In the second experiment, elderly controls were required towalk at the speed exhibited by their PD counterparts so thatstride length, cadence and DLS could be compared in thetwo groups when the effects of velocity were controlled. Aseries of paired t tests were used to determine whether therewere significant differences in stride length, cadence andDLS in PD subjects compared with controls, after the effectsof velocity had been controlled. As a result of this matchingprocedure, the mean velocity for the PD group was47.18±9.28 m/min. compared with 48.15± 10.26 m/min inthe control group. The mean stride length for the PD group(0.924±0.142 m) was significantly smaller from the controlgroup (1.10±0.203 m) [?(17) = 5.02, P = 0.0001]. Likewisethe mean cadence in the PD group (102.05±12.394) wassignificantly greater than controls (88.3± 14.864) [r(17) =-4.598, P = 0.0003]. There was no significant differencebetween groups in DLS at this velocity.
Thirteen of the PD subjects from Study 1 were able toattain the velocity of their control counterparts when providedwith verbal feedback by a physiotherapist. The mean velocityfor the PD group was 57.077± 13.661 m/min, comparedwith 60.423±9.807 m/min in the control group. For thesevelocities, the stride length was significantly shorter in thePD group (1.0±0.13 m) than the control group (1.2±0.177)[r(12) = 4.983, P = 0.0003]. The cadence in the PD group(113.06± 19.56 m/min) was significantly greater than for thecontrol group (101.49±9.67 m/min) [/(12) =-2.454, P =0.03]. Again there was no significant difference betweengroups for DLS duration.
Study 3In Study 3, velocity, cadence and stride length values foreach subject were averaged within each experiment acrossthe two trials sampled. For PD subjects, these values werethen expressed as percentages of the corresponding valuesobtained from their matched control subject walking atpreferred speed.
Considering all six experiments, two types of comparisonwere of interest. First, whether gait parameters in PD variedfrom those found in their matched controls walking atpreferred speed. To evaluate this issue, means and their 95%confidence intervals were computed for velocity, cadenceand stride length. The location of these confidence intervalswas examined against the criterion value of 100%, whichrepresented normal gait. Secondly, in Experiments 2-6, gaitparameters from each investigation were compared with thecorresponding values found for PD in Experiment 1. Thesecomparisons were conducted to ascertain how the conditionsof these later experiments had modified the gait pattern fromthat preferred by PD subjects. The pair-wise comparisonswere conducted with / tests, employing a Bonferroniadjustment to the criterion alpha value, to allow for thefact that up to six analyses utilizing measures that werenot statistically independent were incorporated in each
by guest on October 24, 2014
Dow
nloaded from
1176 M. E. Morris et al.
experiment (Keppel, 1982). The / test is robust when samplesizes are equivalent as in the present study (Keppel, 1982).However, as an additional check, we examined graphicallythe distributions of scores obtained for skew and heterogeneityof variance. Provision was made to check the result of thetheoretically more sensitive / test with a Wilcoxon matched-pairs signed-ranks test where deviation from the assumptionswere suggested by the distributions.
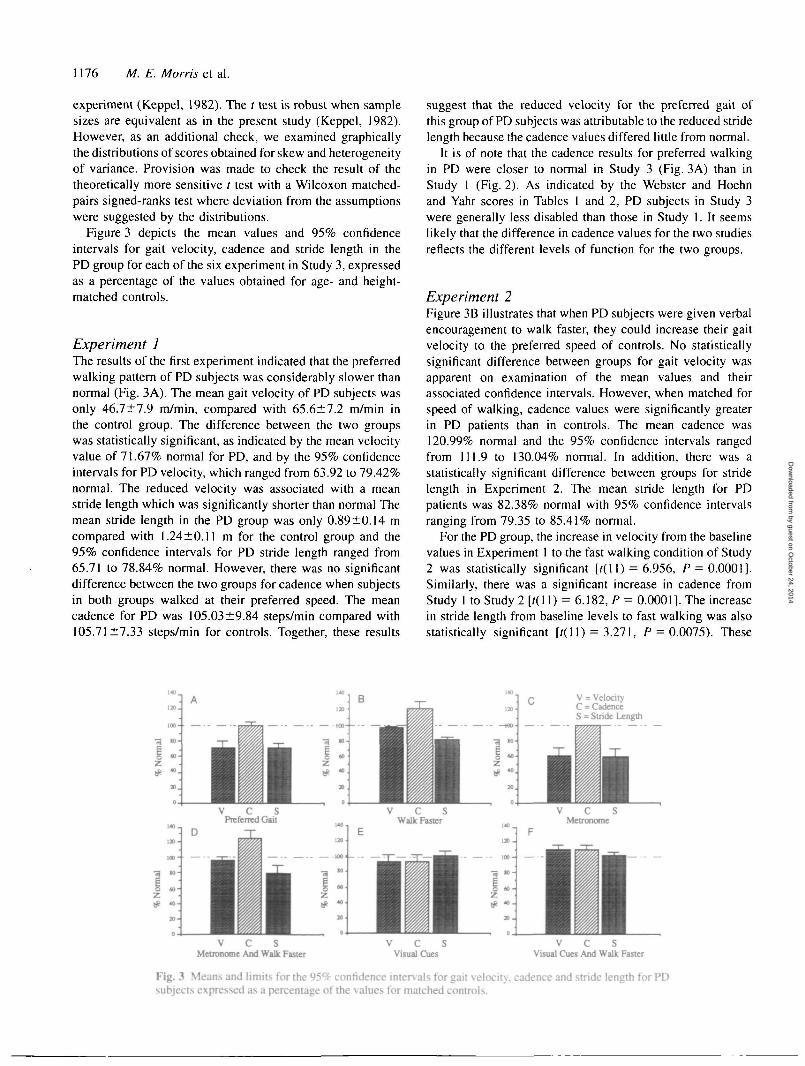
Figure 3 depicts the mean values and 95% confidenceintervals for gait velocity, cadence and stride length in thePD group for each of the six experiment in Study 3, expressedas a percentage of the values obtained for age- and height-matched controls.
Experiment 1The results of the first experiment indicated that the preferredwalking pattern of PD subjects was considerably slower thannormal (Fig. 3A). The mean gait velocity of PD subjects wasonly 46.7±7.9 m/min, compared with 65.6±7.2 m/min inthe control group. The difference between the two groupswas statistically significant, as indicated by the mean velocityvalue of 71.67% normal for PD, and by the 95% confidenceintervals for PD velocity, which ranged from 63.92 to 79.42%normal. The reduced velocity was associated with a meanstride length which was significantly shorter than normal Themean stride length in the PD group was only 0.89±0.14 mcompared with 1.24±0.11 m for the control group and the95% confidence intervals for PD stride length ranged from65.71 to 78.84% normal. However, there was no significantdifference between the two groups for cadence when subjectsin both groups walked at their preferred speed. The meancadence for PD was 105.03±9.84 steps/min compared with105.71 ±7.33 steps/min for controls. Together, these results
suggest that the reduced velocity for the preferred gait ofthis group of PD subjects was attributable to the reduced stridelength because the cadence values differed little from normal.
It is of note that the cadence results for preferred walkingin PD were closer to normal in Study 3 (Fig. 3A) than inStudy 1 (Fig. 2). As indicated by the Webster and Hoehnand Yahr scores in Tables 1 and 2, PD subjects in Study 3were generally less disabled than those in Study I. It seemslikely that the difference in cadence values for the two studiesreflects the different levels of function for the two groups.
Experiment 2Figure 3B illustrates that when PD subjects were given verbalencouragement to walk faster, they could increase their gaitvelocity to the preferred speed of controls. No statisticallysignificant difference between groups for gait velocity wasapparent on examination of the mean values and theirassociated confidence intervals. However, when matched forspeed of walking, cadence values were significantly greaterin PD patients than in controls. The mean cadence was120.99% normal and the 95% confidence intervals rangedfrom 111.9 to 130.04% normal. In addition, there was astatistically significant difference between groups for stridelength in Experiment 2. The mean stride length for PDpatients was 82.38% normal with 95% confidence intervalsranging from 79.35 to 85.41% normal.
For the PD group, the increase in velocity from the baselinevalues in Experiment 1 to the fast walking condition of Study2 was statistically significant [t(\ 1) = 6.956, P = 0.0001].Similarly, there was a significant increase in cadence fromStudy I to Study 2 [?(11) = 6.182, P = 0.0001]. The increasein stride length from baseline levels to fast walking was alsostatistically significant [t(\ 1) = 3.271, P = 0.0075). These
V = VelocityC = CadenceS = Stride Length
V C SMetronome And Walk Faster
V C SVisual Cues
V C SVisual Cues And Walk Faster
Fig. 3 Means and limits for the 95% confidence intervals for gait velocity, cadence and stride length for PDsubjects expressed as a percentage of the vaJues for matched controls.
by guest on October 24, 2014
Dow
nloaded from
Gait hypokinesia in Parkinson's disease 1177
results indicate that PD patients increased the velocity ofwalking by increasing both cadence and stride length althoughthe stride length values for fast walking still failed to reachnormal levels.
Experiment 3Figure 3C shows that subjects with PD could closely entraintheir cadence to that of controls when provided with auditorycues from an electronic metronome set at the desired gaitcycle frequency. The mean cadence was 100.89% normaland the 95% confidence intervals for PD cadence rangedfrom 99.77 to 102.01% normal. However, when PD patientswalked in time to the metronome the stride length wasonly -60% normal (95% confidence intervals: 52.64-71.06%normal). As a consequence of the reduced stride length thevelocity dropped to values that were significantly lower thancontrols. The mean velocity in Study 3 was 62.23% normalwith confidence intervals ranging from 53.17 to 71.29%normal.
A pair-wise comparison revealed that the reduction inmean stride length from the preferred walking speed of PDpatients to walking in time with the metronome did not quitereach statistical significance [/(11) =-2.12, P = 0.0576].Similarly, velocity and cadence values failed to changesignificantly from the baseline levels of Study 1 to theauditory cue condition of Experiment 3.
Experiment 4On instruction to walk faster whilst attending to themetronome, PD patients attained velocity values that did notsignificantly differ from normal (Fig. 3D). However, inattempting to walk as fast as controls the PD subjects failedto keep time with the metronome and increased their cadencein order to increase speed. The cadence reached a meanvalue of 124.94% normal with 95% confidence intervalsranging from 115.69 to 134.18% normal, hence wassignificantly higher than controls. In addition, under theseconditions the stride length was significantly less thancontrols. The mean stride length for PD patients was 77.89%normal and the 95% confidence intervals ranged from 72.86to 83.10% normal.
A paired t test showed that the mean cadence for PDsubjects in Study 4 was significantly greater than the pre-ferred cadence in Experiment 1 [r(l 1) = 5.297, P = 0.0003].Similarly the velocity values for the PD group in Study 4were significantly higher than baseline values of Study 1U(ll) = 6.083, P = 0.001). However, no significant differ-ence in stride length between the two experiments wasapparent on statistical analysis.
Experiment 5Visual cue walking produced near normal stride length,velocity and cadence values in the PD group (Fig. 3E).
Statistical analyses using means and 95% confidence intervalsfor the percentage normal scores failed to identify statisticallysignificant differences between PD patients and controls forany of the parameters in Experiment 5.
In contrast, there was a statistically significant differencebetween the preferred stride length of PD patients, asdetermined by Experiment 1, and their stride length whenwalking with visual cues [r(ll) = 8.591, P = 0.0001].Similarly there was a significant difference between thevelocity values obtained for the PD group in Experiment 1versus Experiment 5 [?(11) = 5.099, P = 0.0003]. In contrast,the cadence values failed to show a significant differencefrom the preferred walking condition to the visual cuecondition.
Experiment 6When PD patients were encouraged to walk as fast as controlswhilst stepping over the visual cues, they could maintaintheir stride length, velocity and cadence rates at levels thatwere equivalent to or greater than controls. The velocity ofPD patients in Experiment 6 was significantly higher thancontrols with mean velocity values at 108.42% normal and95% confidence intervals ranging from 101.79 to 114.39%normal. The mean cadence value for the PD group was alsosignificantly greater than normal. The mean cadence in Study6 was 108.417% normal and ranged from 100.31 to 116.52%normal. However, no statistically significant differencebetween the two groups could be identified for stride lengthin Experiment 6.
The difference in stride length from the preferred gait ofPD patients in Experiment 1 and the visual cues of Experiment6 was statistically significant [r(l 1) = 9.071, P = 0.0001).Likewise the increase in gait velocity from Experiment 1 toExperiment 6 was statistically significant [t(\ 1) = 2.482, P =0.0305). Cadence values, on the other hand, failed to showa significant difference across these conditions, possiblybecause the cadence values were already approximatelynormal in Experiment 1.
DiscussionThe results of this investigation provide considerable evidencethat PD patients walk more slowly than normal because theyhave a fundamental deficit in their ability to automaticallyregulate stride length. In so doing, this series of experimentsrepresents one of the first definitive attempts to documentthe relationships between the spatial and temporal parametersof gait for a range of walking speeds for individuals withPD compared with age- and height-matched controls, andto pinpoint the underlying motor control deficit in gaithypokinesia.
In the first study we found that for slow, natural and fastwalking speeds the velocity, stride length and cadence valueswere consistently lower in PD subjects than controls (Figs 1and 2). As indicated in Fig. 2, PD subjects could increase
by guest on October 24, 2014
Dow
nloaded from

1178 M. E. Morris et al.
and decrease their velocity of walking by grading both stridelength and cadence although the range of response wasreduced for both of these parameters. The reduced magnitudeof response in PD was not due to an inability to increase thestep size or step frequency at the same rate as controls.Linear regression analyses on the data from Study 1 indicatedthat, on average, PD subjects showed a similar rate of changein velocity with stride length and velocity with cadence tothat found in control subjects. Rather, the reduced magnitudeof response appeared to be an inherent characteristic of PDgait. The ability of PD subjects to grade movement amplitudeyet at the same time lack the ability to generate the requiredamplitude and velocity of movement has been demonstratedpreviously for the performance of upper limb ballisticmovements (e.g. Berardelli et al., 1986). As with our gaitresults, no explanation has yet been forthcoming in thiscontext.
One of the most important findings of this investigationwas that when the effects of walking speed were taken intoaccount, the stride length was shorter and the cadence higherin PD subjects than controls. This finding was consistentacross all three studies. The analyses in Study 1 highlightedthat, although the slopes for the regression of velocity againststride length and for velocity against cadence were notsignificantly different for the two groups, the intercept forstride length was lower in the PD group than the controlgroup and the intercept for cadence was higher in the PDgroup than the control group. Thus for any given velocity ofwalking the stride length was shorter and the cadence higherin the PD group than the control group. Study 2 yielded thesame findings using a different experimental approach. Inthe second study, control subjects were instructed to reducetheir speed of walking to the preferred velocity of their PDcounterparts and the PD subjects were instructed to walk asfast as their matched controls. When velocity was thusmatched for the two groups, the cadence was found to beproportionally higher and stride length smaller in the PDgroup than the control group. The same findings werereplicated in the second experiment of Study 3. Therefore,contrary to the conclusion drawn by Stern el al. (1983) that'. . . in parkinsonian patients the relative contributions ofpace-length and cadence to the velocity of walking are nodifferent from the elderly population at large', the results ofthis series of studies highlighted that for any given velocity,stride length is proportionally shorter and cadence higher inPD subjects compared with controls.
Also contrary to previous reports, this investigation foundno significant difference between PD subjects and controlsfor the period spent in the double support phase of the gaitcycle. The studies by Murray et al. (1969), Knutsson (1972),Stern et al. (1983) and Blin et al. (1991) showed an increasein DLS duration in PD gait. Our results indicated that forboth groups a reduction in walking velocity was associatedwith an elongation of the stance phase of the gait cycle, andin particular an increase in the period of DLS. Any increasein velocity was associated with a decrease in DLS duration in
both groups. However, the linear regression analyses forStudy 1 demonstrated that the rate of change in DLS withchange in velocity was comparable for the two groups. Theregression analyses also yielded similar intercept values forDLS for the PD and control groups which indicated that forany given velocity, the percentage of time spent in DLS wassimilar for the two groups. Furthermore, when matched forspeed of walking in Study 2, the duration of DLS wasnot significantly different for PD subjects compared withcontrols.
Both groups did, however, show DLS values well abovethe normal levels for non-geriatric adults. According toMurray (1967), DLS usually accounts for 20% of the gaitcycle in adults aged 21-65 years. In Study 1, our elderlycontrols spent 32% gait cycle in DLS for their preferredwalking speed and the PD subjects spent 34% gait cycle inDLS for their preferred gait. These values are similar tothose for the walking patterns of elderly people reported byMurray et al. (1978), O'Brien et al. (1983) and Wall et al.(1991). Gabell and Nayak (1984) made the point that frombiomechanical principles it can be assumed that an increasein DLS time will lead to greater stability of gait and thereforecould reflect a compensation for instability. That our studyfailed to identify a differential effect for DLS might suggestthat postural instability was not the major factor whichdiscriminated PD gait kinematics from the walking patternsof elderly controls. Nevertheless, the finding that PD subjectsalong with controls had higher than normal DLS valuesindicates that balance disturbance might have contributed tothe walking patterns of both groups. Further research isrequired to evaluate the relative contribution of balancedisturbance in the pathogenesis of gait hypokinesia in PD.
Determinants of gait hypokinesia in PDAlthough the results of Studies 1 and 2 yielded findings ofimportance for describing the kinematics of PD gait, they stillfailed to clarify the fundamental deficit in PD hypokinesia.In particular, it was not apparent whether the problem inregulating the velocity of walking was due to a problem ingenerating a large stride or a problem in modulating cadence.For these reasons we conducted Study 3 which aimed tohighlight which parameter (stride length or cadence) was atfault, and which parameter was used as a compensatorymechanism to help overcome hypokinesia.
The results of Study 3 clearly showed that in our sample ofPD subjects there was a problem in adjusting stride lengthby internal motor control mechanisms. Patients were able toincrease the size of their stride when they were asked to walkas fast as controls in Experiment 2, but the range of increasewas considerably reduced. When asked to walk in time with ametronome set at the normal cadence for controls, the stridelength values dropped to 60% of normal even though thecadence was closely synchronized with the metronome beat.It appeared as if the stride length defaulted to baseline levelswhen the PD subjects were required to shift their focus of
by guest on October 24, 2014
Dow
nloaded from

Gait hypokinesia in Parkinson's disease 1179
attention away from the step size to the timing of ambulation.In other words, when PD subjects were forced to rely oninternal motor control mechanisms to regulate stride length theamplitude of consecutive steps showed greatest deviation fromnormal. When asked to walk in time with the metronome at thesame time as walking as fast as controls, the stride length didincrease, but only to 80% of normal. Instead of adequatelyadjusting stride length for this experimental condition, PDsubjects increased their cadence rate in addition to stride lengthand therefore lost their synchronization with the metronomebeat. Nevertheless, it was possible for PD subjects to achievea normal stride length when using external visual cues to triggerthe stepping pattern. When white floor markers were providedfor the patients to step over, the stride length reached valuesthat were not significantly different from normal. At the sametime the cadence and velocity were not significantly differentfrom normal. This provides a strong indication that thefundamental deficit in gait hypokinesia is the internalregulation of stride length, because when the stride length wasnormalized using external cues the other gait variables werealso approximately equal to normal values.
By contrast with their difficulty in the internal regulation ofstride length, PD subjects showed no such deficit with theregulation of cadence. This parameter was easily controlled byinternal motor control mechanisms and external cueing. Forexample, when asked to walk faster with or without externalcues, PD subjects could easily increase their stepping rate.They could also very accurately entrain the timing of footstepsto the beat of the metronome. These findings, together with theresults of the visual cue experiment, which showed that whenthe stride length was normalized, the cadence values were alsoapproximately normal, suggest that the increase in cadence forany given velocity in PD is used as a compensation for difficultyin regulating stride length.
The pathophysiology of gait hypokinesia in PDIn this study, we demonstrated that walking sloweddramatically in PD hypokinesia when subjects were askedto perform a long gait sequence without resort to externalcues. The slowing of movement was primarily due to aninability to generate internally, steps of appropriate size, andwhen subjects were provided with visual cues both the spatialand temporal parameters of the foot step-pattern returned tonear normal values. This indicates that the motor controlmechanisms for gait are intact in PD and that a normal steppingresponse can be elicited under appropriate conditions.
The reason for the difficulty in regulating stride length isunclear although previous studies on PD hypokinesia suggestthat disturbed movement amplitude and velocity could resultfrom either impaired cue production in the basal ganglia ordisordered movement preparation (motor set). There is nowconsiderable evidence that the basal ganglia generate phasicinternal motor cues for predictable, well-learned movementsequences (e.g. Brotchie el ai, \99\a,b) and it has beensuggested that the phasic cue from the basal ganglia inter-
acts with the supplementary motor area to run movementsequences automatically. The interaction is thought to involvean abrupt cessation of premovement activity in thesupplementary motor area by phasic activity of the basalganglia and it is this abrupt cessation which enables thesubmovement to be executed normally (Brotchie et al.,\99\a,b). A disordered cue would not abruptly turn offpremovement activity in the supplementary motor area and thetiming of the movement that ensued would be abnormally slow.Georgiou et al. (1993) demonstrated that both the reaction timeand movement time of submovements performed in a learnedsequence are prolonged in PD patients compared with controls.They also showed that the longer movement time is due toprolonged preparation time. However, the provision of non-contingent auditory cues returned both reaction time andmovement time to normal, presumably because these cuessubstituted for the defective basal ganglia cue. The suggestionthat hypokinesia results from a disorder of phasic cuegeneration in the basal ganglia may, at first, seem contradictoryto the finding that cadence regulation (i.e. regulation of thefrequency of consecutive steps) is intact in PD patients.However, there are several lines of evidence which indicate thatspinal and brainstem mechanisms play a role in the regulationof locomotion, in addition to supraspinal mechanisms (e.g.Grillner, 1975; Pearson, 1993). In this regard it is possible thatcadence regulation is not under basal ganglia influence whereasstride length control is mediated by the basal ganglia.
An alternative explanation is that the reduced stride lengthin PD is due to inadequate preparatory processes involving theinteraction between the supplementary motor area and the basalganglia. Several studies on primates have demonstrated thatboth the globus pallidus and the striatum have a proportion ofneurons that exhibit set-related premovement activity (Brot-chie et al., \99\a,b; Kimura et al., 1992). Moreover, neuralnetwork modelling has led to the suggestion that the basalganglia need to generate sustained premovement activity inorder for movement sequences to be run by the supplementarymotor area (Brotchie et al., 1991c). The mechanism by whichdisturbed movement preparation leads to reduced movementamplitude and velocity is not well understood, althoughdisturbed motor set could affect the generation of forceindirectly by reducing the gain of spinal reflex mechanisms.Biomechanical analyses of gait (Winter, 1991) indicate that astep is generated mainly by a power burst from the triceps suraemuscles in the late phase of stance. If this power burst werediminished as a result of disturbed motor set, the length of thestride would be reduced. This hypothesis is consistent withthe decrease in stride length observed in the present studies.Nevertheless further research is needed to clarify the role ofthe basal ganglia in the control of human locomotion.
Significance for movement rehabilitationstrategiesThe findings of this investigation are potentially of benefit inthe development of optimal gait training strategies for PD. Our
by guest on October 24, 2014
Dow
nloaded from

1180 M. E. Morris et al.
results suggest that the fundamental deficit in gait hypokinesiais one of stride length regulation. However, the basic controlmechanisms for locomotion are intact and a normal steppingmechanism can be activated, given the appropriate conditions.In this light it seems possible that movement rehabilitationstrategies could have the potential to assist PD patients toachieve a more normal step size, perhaps by using visual cueingtechniques (Martin, 1967; Forssberge/a/., 1984; Dunne et al.,1987; Bagley et al., 1991; Weissenberg, 1993) or by teachingpatients to consciously focus their attention on the size ofconsecutive steps. Our results would suggest that use ofauditory cueing techniques to normalize cadence (e.g. useof an electronic metronome or verbal cueing) would not beeffective in normalizing walking speed. Although this studyhas clarified the nature of the basic deficit in gait hypokinesia,what is now required is elucidation of how to best activate theintact control mechanism to produce normal stride length.
AcknowledgmentsWe wish to thank Cameron Grant for technical assistance,members of MOREG for their comments and the PD patientswho gave so freely of their time.
ReferencesAita JF. Why patients with Parkinson's disease fall. JAMA 1982; 247:515-16.
Bagley S, Kelly B, Tunnicliffe N, Tumbull GI, Walker JM. The effectof visual cues on the gait of independently mobile Parkinson's diseasepatients. Physiotherapy 1991; 77: 415-20.
Banks MA, Caird FI. Physiotherapy benefits patients with Parkinson'sdisease. Clin Rehabil 1989; 3: 11-16.
Berardelli A, Dick JPR, Rothwell JC, Day BL, Marsden CD. Scalingof the size of the first agonist EMG burst during rapid wrist movementsin patients with Parkinson's disease. J Neurol Neurosurg Psychiatry1986; 49: 1273-9.
Blin O, Ferrandez AM, Serratrice G. Quantitative analysis of gait inParkinson patients: increased variability of stride length. J Neurol Sci1990; 98: 91-7.
Blin O, Ferrandez AM, Pailhous J, Serratrice G. Dopa-sensitive anddopa-resistant gait parameters in Parkinson's disease. J Neurol Sci1991; 103:51-^.
Bowes SG, Clark PK, Leeman AL, O'Neill CJA, Weller C, NicholsonPW, et al. Determinants of gait in the elderly parkinsonian onmaintenance levodopa/carbidopa therapy. Br J Clin Pharmacol 1990;30: 13-24.
Brooks DJ, Salmon EP, Mathias CJ, Quinn N, Leenders KL, BannisterR, et al. The relationship between locomotor disability, autonomicdysfunction, and the integrity of the striatal dopaminergic system inpatients with multiple system atrophy, pure autonomic failure, andParkinson's disease, studied with PET. Brain 1990; 113: 1539-52.
Brotchie P, Iansek R, Home MK. Motor function of the monkeyglobus pallidus: 1. Neuronal discharge and parameters of movement.Brain 1991a; 114: 1667-83.
Brotchie P, Iansek R, Home MK. Motor function of the monkeyglobus pallidus: 2. Cognitive aspects of movement and phasicneuronal activity. Brain 1991b; 114: 1685-702.
Brotchie P, Iansek R, Home MK. A neural network model of neuralactivity in the monkey globus pallidus. Neurosci Lett 1991c; 131:33-6.
Du Chatinier K, Molen NH, Rozendal RH. Step length, step frequencyand temporal factors of the stride in normal human walking. Proc KNed Akad Wet C 1970; 73: 214-27.
Dunne JW, Hankey GJ , Edis RH. Parkinsonism: upturned walkingstick as an aid to locomotion. Arch Phys Med Rehabil 1987; 68:380-1.
Formisano R, Pratesi L, Modarelli FT, Bonifati V, Meco G.Rehabilitation and Parkinson's disease. Scand J Rehabil Med 1992;24: 157-60.
Forssberg H, Johnels B, Steg G. Is parkinsonian gait caused by aregression to an immature walking pattern? Adv Neurol 1984; 40:375-9.
Gabell A, Nayak USL. The effect of age on variability in gait. JGerontol 1984; 39: 662-6.
Georgiou N, Iansek R, Bradshaw JL, Phillips JG, Mattingley JB,Bradshaw JA. An evaluation of the role of internal cues in thepathogenesis of parkinsonian hypokinesia. Brain 1993; 116: 1575-87.
Gibberd FB, Page NGR, Spencer KM, Kinnear E, Hawksworth JB.Controlled trial of physiotherapy and occupational therapy forParkinson's disease. BrMedJ 1981; 282: 1196.
Grieve DW, Gear RJ. The relationships between length of stride, stepfrequency, time of swing and speed of walking for children and adults.Ergonomics 1966; 9: 379-99.
Grillner S. Locomotion in vertebrates: central mechanisms and reflexinteraction. Physiol Rev 1975; 55: 247-304.
Hoehn MM, Yahr MD. Parkinsonism: onset, progression, andmortality. Neurology 1967; 17:427-442.
Hurwitz A. The benefit of a home exercise regimen for ambulatoryParkinson's disease patients. J Neurosci Nurs 1989; 21:180-4.
Keppel G. Design and analysis: a researcher's handbook. 2nd ed.Englewood Cliffs (NJ): Prentice-Hall, 1982.
Kimura M, Aosaki T, Hu Y, Ishida A, Watanabe K. Activity of primateputamen neurons is selective to the mode of voluntary movement:visually guided, self-initiated or memory-guided. Exp Brain Res 1992;89: 473-7.
Klawans HL. Individual manifestations of Parkinson's disease afterten or more years of levodopa. Mov Disord 1986; 1: 187-92.
Knutsson E. An analysis of parkinsonian gait. Brain 1972; 95:475-86.
Knutsson E, Martensson A. Quantitative effects of L-dopa on differenttypes of movements and muscle tone in parkinsonian patients. ScandJ Rehabil Med 1971; 3: 121-30.
Kokmen E, Naessens JM, Offord KP. A short test of mental status:description and preliminary results. Mayo Clin Proc 1987; 62: 281-9.
Koller WC, Glatt S, Vetere-Overfield B, Hassanein R. Falls andParkinson's disease. Clin Neuropharmacol 1989; 12:98-105.
Marsden CD, Parkes JD, Quinn N. Fluctuations of disability in
by guest on October 24, 2014
Dow
nloaded from

Gait hypokinesia in Parkinson's disease 1181
Parkinson's disease: clinical aspects. In: Marsden CD, Fahn S, editors.Movement disorders. London: Butterworth Scientific, 1982: 96-122.
Martin JP. The basal ganglia and posture. London: Pitman Medical,1967.
Martin KE, Phillips JG, Bradshaw JL, Iansek R. Could bradykinesiain Parkinson's disease simply be compensation? J Neurology 1994.241:439-447.
Murray MR Gait as a total pattern of movement. [Review]. AmJ PhysMed 1967; 46: 290-333.
Murray MP, Kory RC, Clarkson BH. Walking patterns in healthy oldmen. J Gerontol 1969; 24: 169-78.
Murray MP, Sepic SB, Gardner GM, Downs WJ. Walking patterns ofmen with parkinsonism. Am J Phys Med 1978; 57: 278-94.
O'Brien M, Power K, Sanford S, Smith K, Wall JC. Temporal gaitpatterns in healthy young and elderly females. Phys Can 1983; 35:323.
Palmer SS, Mortimer JA, Webster DD, Bistevins R, Dickinson GL.Comparison of stretch exercises and karate training as therapyfor Parkinson's disease [abstract]. Arch Phys Med Rehabil 1984;65: 626.
Palmer SS, Mortimer JA, Webster DD, Bistevins R, Dickinson GL.Exercise therapy for Parkinson's disease. Arch Phys Med Rehabil1986; 67: 741-5.
Patla AE. Understanding the control of human locomotion: a prologue.In: Patla AE, editor. Adaptability of human gait: implications for thecontrol of locomotion. Amsterdam: North-Holland, 1991: 3-17.
Paulson GW, Schafer K, Hallum B. Avoiding mental changes andfalls in older Parkinson's patients. Geriatrics 1986; 41: 59-62.
Pearson KG. Common principles of motor control in vertebrates andinvertebrates. [Review]. Annu Rev Neurosci 1993; 16: 265-97.
Pederson SW, Oberg B, Insulander A, Vretman M. Group trainingin parkinsonism: quantitative measurements of treatment. Scand JRehabil Med 1990; 22: 207-11.
Richards CL, Cioni M, Malouin F, Bedard PJ, Moffet H, Leieux R,et al. Changes in the gait of patients with Parkinson's disease inducedby sensory cues and L-dopa. Proceedings of the Sixth BiennialConference, Canadian Society for Biomechanics, 1990: 199-202.
Roland PE, Meyer E, Shibasaki T, Yamamoto YL, Thompson CJ.Regional cerebral blood flow changes in cortex and basal gangliaduring voluntary movements in normal human volunteers. JNeurophysiol 1982; 48: 467-80.
Schenkman M, Donovan J, Tsubota J, Kluss M, Stebbins P, ButlerRB. Management of individuals with Parkinson's disease: rationaleand case studies. Phys Ther 1989; 69: 944-55.
Schoenberg BS. Epidemiology of movement disorders. In: MarsdenCD, Fahn S, editors. Movement disorders 2. London: Butterworths,1987: 17-32.
Seitz RJ, Roland PE. Learning of sequential finger movements inman: a combined kinematic and positron emission tomography (PET)study. Eur J Neurosci 1992; 4: 154-65.
Stern GM, Franklyn SE, Imms FJ, Prestidge SP. Quantitativeassessments of gait and mobility in Parkinson's disease. J NeuralTransm 1983; Suppl 19: 201-14.
Wall JC, Turnbull GI. The kinematics of gait. In: Turnbull GI, editor.Physical therapy management of Parkinson's disease. New York:Churchill Livingstone, 1992: 49-67.
Wall JC, Hogan DB, Turnbull GI, Fox RA. The kinematics ofidiopathic gait disorder. A comparison with healthy young and elderlyfemales. Scand J Rehabil Med 1991; 23: 159-64.
Webster DD. Critical analysis of the disability in Parkinson's disease.Mod Treat 1968; 5: 257-82.
Weissenborn S. The effect of using a two-step verbal cue to a visualtarget above eye level on the parkinsonian gait: a case study.Physiotherapy 1993; 79: 26-31.
Winter DA. The biomechanics and motor control of human gait:normal, elderly and pathological. Ontario: University of WaterlooPress, 1991:45.
Yekutiel MP, Pinhasov A, Shahar G, Sroka H. A clinical trial of there-education of movement in patients with Parkinson's disease. ClinRehabil 1991; 5: 207-14.
Received January 12, 1994. Revised April 8, 1994.Accepted May 3, 1994
by guest on October 24, 2014
Dow
nloaded from





























