Embed Size (px)
Citation preview
THE LONGUS COLLI MUSCLE FLAP FORRECONSTRUCTION OF THE LATERALPHARYNGEAL WALL
Sharon L. Collins, MS, MD
Loyola University of Chicago Medical Center, 2160 S. First Avenue, Building 105, Room 1870,Maywood, Illinois 60153
Received 16 May 1994; accepted 17 December 1996
Abstract: Background. Full-thickness lateral pharyngeal wall(LPW) defects are difficult to reconstruct, whether the larynx ispreserved or removed (extended total laryngectomy). A simple,reliable reconstructive method using local tissue which optimizeswound healing and functional results would allow partial laryn-gectomy more often, without incurring the cost, donor site mor-bidity, and increased operative length of regional or free flaps.My objective was to propose use of the longus colli muscle as areconstructive flap for defects of the LPW.
Methods. Results of using the longus colli muscle flap(LCMF) in a series of 16 patients with primary tumors of thepharyngeal wall or pyriform sinus are presented. The majorityhad surgery and planned postoperative radiotherapy.
Results. There were no wound infections or fistulas. One of 2previously radiated patients had a transient wound-healing prob-lem. Although 88% of the patients were stage III and IV and 50%had T3–4 primary tumors, there were only 2 local failures, for alocal control rate of 88%. Corresponding cancer-free survival was69% (median follow-up of 22 months). Two thirds of the patientstook all or some food by mouth, and of the 12 with larynx pre-served, 58% were decannulated, and 11 had a good to normalvoice.
Conclusions. The reliability of wound healing and absence ofnegative impact on oncologic and functional results validate useof the LCMF as a reconstructive option for defects in the LPW at
both the oropharynx and hypopharynx levels. © 1997 John Wiley& Sons, Inc. Head Neck 19: 297–308, 1997.
Keywords: muscle flap; pharyngeal wall; longus colli flap
Resections which leave a full-thickness defect inthe lateral pharyngeal wall/pyriform sinus areahave been a perennial reconstructive challengefor the head and neck cancer surgeon, especiallywhen the larynx is preserved. Due to lack of asingle, reliable reconstructive method the prob-lem has been addressed with: (1) controlled phar-yngostomes and delayed reconstruction with cer-vical skin flaps, (2) performance of near-total ortotal laryngectomy to facilitate closure when notoncologically necessary, and (3) primary cancertreatment with radiation or, more recently, com-binations of chemotherapy and radiotherapy (RT)to avoid surgery altogether. The third strategysacrifices surgery, which is the best method tooptimize locoregional control for head and necksquamous cancer, to the potential detriment ofthe patient. Thus, if a simple, reliable methodcould be developed to reconstruct a full-thicknessdefect in the lateral pharyngeal wall (LPW), par-
Correspondence to: S. L. Collins
CCC 0148-6403/97/040297–12© 1997 John Wiley & Sons, Inc.
Longus Colli Muscle Flap HEAD & NECK July 1997 297
tial laryngectomy could be performed more often(when oncologically feasible), thereby maintain-ing surgery in the initial treatment with the po-tential to optimize oncological control and func-tional results without feeding tubes or stomas.
This paper redirects attention to the utility oflocal tissue to reconstruct defects in the LPW inan era when many surgeons consider that freeflap reconstruction of hypopharyngeal defects is‘‘state of the art.’’ Free flap technology is not uni-versally available, however, and results are op-erator-dependent. Simpler methods which are ac-cessible worldwide and in a more cost-consciousUSA should continue to be part of the head andneck surgeon’s armamentarium. This paper de-scribes for the first time a series of patients re-constructed with the longus colli muscle (LCM)used as a flap. The main context of use is for LPWdefects resulting from larynx-preserving pharyn-gectomy and from partial laryngectomies ex-tended to include resection of the pyriform sinus.The technique could also be used for repair of hy-popharyngeal fistulas and traumatic scarring orbenign strictures, when lining mucosa is defi-cient.
MATERIALS AND METHODS
Patient Population. Sixteen patients were recon-structed with the LCMF: 14 had primary surgerywith curative intent followed by planned postop-erative RT, 1 had salvage surgery following full-course RT, and 1 had salvage surgery followingsurgery plus postoperative RT. None of the pa-tients had chemotherapy as part of their initialtreatment. Thirteen patients were managed inthe Loyola University Medical Center practiceand 3 at the Hines VA Hospital.
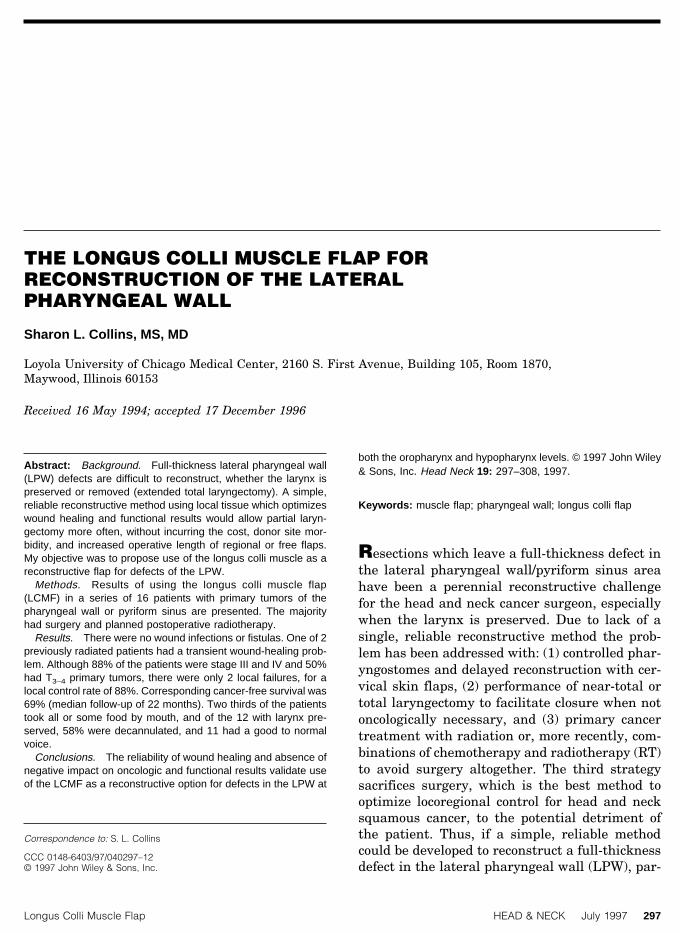
Primary tumor sites included the posteriorpharyngeal wall (PPW) in 13, pyriform sinus (n 42) and cervical esophagus (n 4 1). (This serieswas a subset of a larger group of patients withtumors in these sites who had other methods ofreconstruction; the LCMF was not necessary forall of the patients who underwent larynx-preserving pharyngectomy [LPP], because manyof them had adequate residual pyriform mucosato provide lateral tissue for primary reconstruc-tion.) In 12 patients, the larynx was preserved,and the flap was used to reconstruct a full-thickness defect in the LPW (Figure 1A). In 4 pa-tients, the LCMF was used for carotid artery pro-tection and to amplify neopharynx circumference
in reconstruction of a total laryngopharyngec-tomy (TLP) defect (Figure 1B). In the latter pa-tients, the LCMF provided the lateral aspect of areconstruction which consisted of the preverte-bral fascia (PVF) posteriorly and retained mu-cosa/submucosa from the postcricoid and pyri-form area used to reform an anterolateralneopharynx (‘‘mucosa-preserving’’ TLP). The de-tails of the patient series (tumor site, stage, treat-ment, outcome) are presented in Table 1.
Flap Anatomy and Technique. The LCMs arepaired neck flexors comprised of three portions(superior oblique, inferior oblique, vertical) whicharise from the anterior tubercles and transverseprocesses of the vertebral column spanning thearea from the arch of the atlas to the third tho-racic vertebra (Figure 2). The LCMs lie dorsal tothe pharyngeal constrictor muscles (deep to the
FIGURE 1. Use of the LCMF. (A) Reconstruction of lateral pha-ryngeal wall defect—larynx intact. Right longus colli muscle el-evated off anterior spinal ligaments (black dot) and sutured toresidual larynx (arrows). Omohyoid (overlying suture) and strapmuscles (in clamp) provide second and third closure layers. Chin(C).
298 Longus Colli Muscle Flap HEAD & NECK July 1997

PVF) and anterior to the ligaments of the cervicalspine (Figure 3). Innervation is from the cervicalplexus (C2–7), and the blood supply is from mus-cular perforators of the vertebral artery.
The vertebral artery (Figure 2) originates fromthe subclavian or innominate artery and entersthe transverse process of C6, above which level itis protected in bone. The extravertebral part ofthe artery (anterior to the transverse process ofC7, laterally) is short, about 4 cm from its subcla-vian origin to its entry into the vertebrae. Theartery runs superiorly between the long neckmuscles (longus colli, longus capitus) and the an-terior scalene muscle laterally, with the internaljugular vein, common carotid artery, and sterno-cleidomastoid muscle ventral to it. These relation-ships are shown in Figure 2 and on a magneticresonance imaging (MRI) scan (Figure 4). Thevertebral artery is of concern only low in the neckat the level of C7, where is it still in soft tissueanterior to the vertebrae. No attempt is made toidentify the artery in elevating the LCMF, and ithas not been visualized, encountered, or violatedin the author’s experience.
The thickness of the LCM ranges from one-eighth to one-half inch laterally. Medially, muscle‘‘slips’’ diminish, and fascial insertions predomi-nate. The length of the LCM allows it to be usedas a flap to close LPW defects from the level of theupper oropharynx to the cervical esophagus on
one or both sides. The lateral edge of the LCMF isdeveloped by dissecting bluntly through themuscle just medial to the carotid artery. Dissec-tion behind the artery is avoided, because thiscould damage the sympathetic chain,1 leading toHorner’s syndrome. Once the lateral edge of theflap is defined along the desired length, dissectioncontinues dorsal to the muscle—a bloodlessplane—and the flap is developed in a few moves.The width of the flap varies from 1 to 2 inches,depending on individual anatomy (Figure 1A).The LCM is not transected superiorly or inferi-orly; rather, it is turned anteriorly, forming a newLPW, and remains based medially on its attach-ments to the spine. The lateral aspect of themuscle is sutured to the antero-most laryngealremnant (anterior pyriform mucosa or laryngealframework), thereby reconstituting the LPW. Theprocedure takes 5–10 minutes.
This technique can be performed without neckdissection and does not preclude use of the levatorscapula muscle for carotid bulb coverage, if de-sired. The LCMF suture line can be reinforcedwith secondary and tertiary muscle layers pro-vided by the omohyoid and/or other residual strapmuscles, if available (Figure 1A). Detaching theomohyoid muscle from the hyoid decreases laryn-geal tethering which favors laryngeal elevation,and it can be used for additional coverage over theprimary LCMF suture line.
FIGURE 1. (Continued) Use of the LCMF. (B) Reconstruction of TLP defect. LCMF (in clamp) beingelevated medial to carotid artery (C). Intact prevertebral fascia (P), uvula (U).
Longus Colli Muscle Flap HEAD & NECK July 1997 299
CASE PRESENTATION
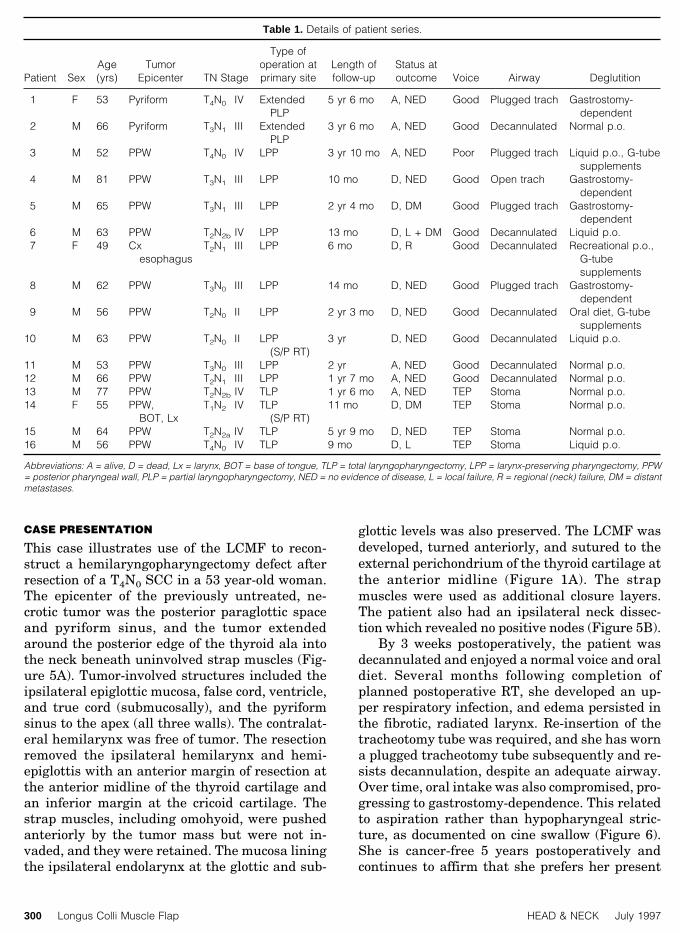
This case illustrates use of the LCMF to recon-struct a hemilaryngopharyngectomy defect afterresection of a T4N0 SCC in a 53 year-old woman.The epicenter of the previously untreated, ne-crotic tumor was the posterior paraglottic spaceand pyriform sinus, and the tumor extendedaround the posterior edge of the thyroid ala intothe neck beneath uninvolved strap muscles (Fig-ure 5A). Tumor-involved structures included theipsilateral epiglottic mucosa, false cord, ventricle,and true cord (submucosally), and the pyriformsinus to the apex (all three walls). The contralat-eral hemilarynx was free of tumor. The resectionremoved the ipsilateral hemilarynx and hemi-epiglottis with an anterior margin of resection atthe anterior midline of the thyroid cartilage andan inferior margin at the cricoid cartilage. Thestrap muscles, including omohyoid, were pushedanteriorly by the tumor mass but were not in-vaded, and they were retained. The mucosa liningthe ipsilateral endolarynx at the glottic and sub-
glottic levels was also preserved. The LCMF wasdeveloped, turned anteriorly, and sutured to theexternal perichondrium of the thyroid cartilage atthe anterior midline (Figure 1A). The strapmuscles were used as additional closure layers.The patient also had an ipsilateral neck dissec-tion which revealed no positive nodes (Figure 5B).
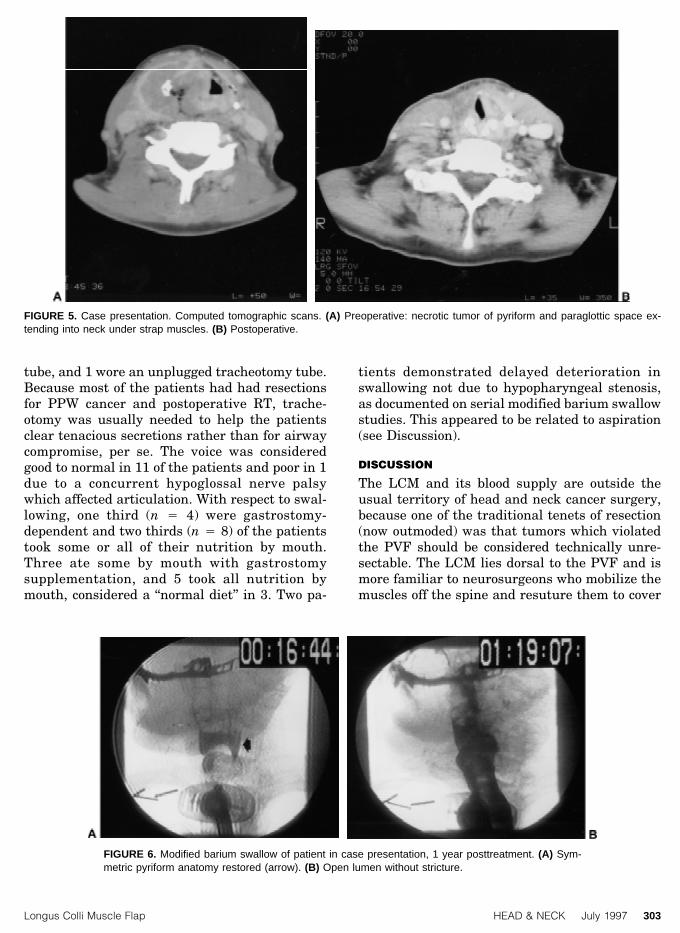
By 3 weeks postoperatively, the patient wasdecannulated and enjoyed a normal voice and oraldiet. Several months following completion ofplanned postoperative RT, she developed an up-per respiratory infection, and edema persisted inthe fibrotic, radiated larynx. Re-insertion of thetracheotomy tube was required, and she has worna plugged tracheotomy tube subsequently and re-sists decannulation, despite an adequate airway.Over time, oral intake was also compromised, pro-gressing to gastrostomy-dependence. This relatedto aspiration rather than hypopharyngeal stric-ture, as documented on cine swallow (Figure 6).She is cancer-free 5 years postoperatively andcontinues to affirm that she prefers her present
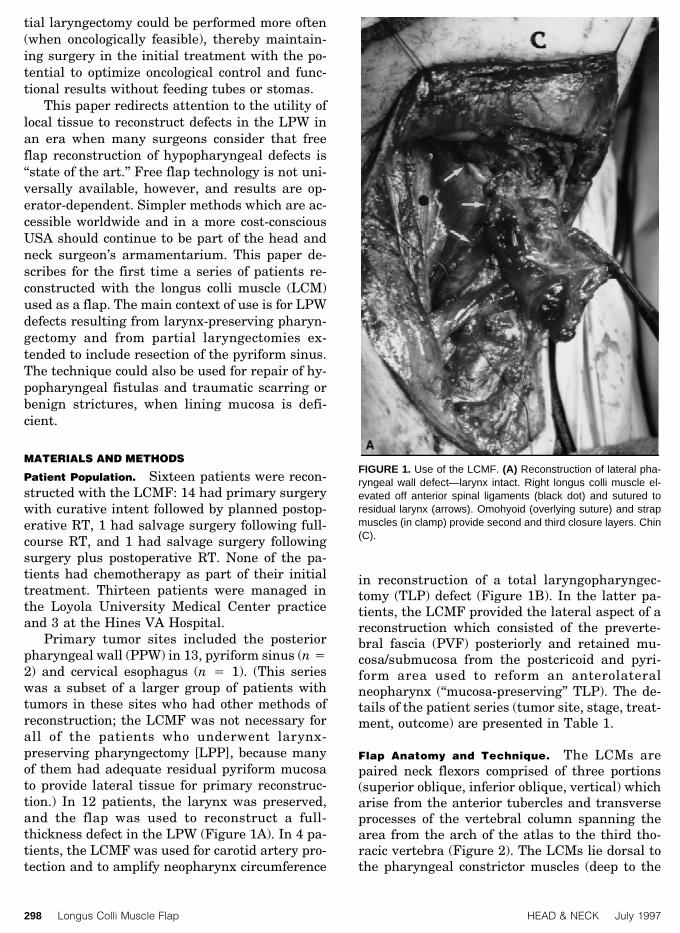
Table 1. Details of patient series.
Patient SexAge(yrs)
TumorEpicenter TN Stage
Type ofoperation atprimary site
Length offollow-up
Status atoutcome Voice Airway Deglutition
1 F 53 Pyriform T4N0 IV ExtendedPLP
5 yr 6 mo A, NED Good Plugged trach Gastrostomy-dependent
2 M 66 Pyriform T3N1 III ExtendedPLP
3 yr 6 mo A, NED Good Decannulated Normal p.o.
3 M 52 PPW T4N0 IV LPP 3 yr 10 mo A, NED Poor Plugged trach Liquid p.o., G-tubesupplements
4 M 81 PPW T3N1 III LPP 10 mo D, NED Good Open trach Gastrostomy-dependent
5 M 65 PPW T3N1 III LPP 2 yr 4 mo D, DM Good Plugged trach Gastrostomy-dependent
6 M 63 PPW T2N2b IV LPP 13 mo D, L + DM Good Decannulated Liquid p.o.7 F 49 Cx
esophagusT2N1 III LPP 6 mo D, R Good Decannulated Recreational p.o.,
G-tubesupplements
8 M 62 PPW T3N0 III LPP 14 mo D, NED Good Plugged trach Gastrostomy-dependent
9 M 56 PPW T2N0 II LPP 2 yr 3 mo D, NED Good Decannulated Oral diet, G-tubesupplements
10 M 63 PPW T2N0 II LPP(S/P RT)
3 yr D, NED Good Decannulated Liquid p.o.
11 M 53 PPW T3N0 III LPP 2 yr A, NED Good Decannulated Normal p.o.12 M 66 PPW T2N1 III LPP 1 yr 7 mo A, NED Good Decannulated Normal p.o.13 M 77 PPW T2N2b IV TLP 1 yr 6 mo A, NED TEP Stoma Normal p.o.14 F 55 PPW,
BOT, LxT1N2 IV TLP
(S/P RT)11 mo D, DM TEP Stoma Normal p.o.
15 M 64 PPW T2N2a IV TLP 5 yr 9 mo D, NED TEP Stoma Normal p.o.16 M 56 PPW T4N0 IV TLP 9 mo D, L TEP Stoma Liquid p.o.
Abbreviations: A = alive, D = dead, Lx = larynx, BOT = base of tongue, TLP = total laryngopharyngectomy, LPP = larynx-preserving pharyngectomy, PPW= posterior pharyngeal wall, PLP = partial laryngopharyngectomy, NED = no evidence of disease, L = local failure, R = regional (neck) failure, DM = distantmetastases.
300 Longus Colli Muscle Flap HEAD & NECK July 1997

functional situation to that of a total laryngecto-my with a stoma.
RESULTS
Wound-Healing Results. There were no neck in-fections or fistulas. Fourteen patients were previ-ously untreated, and 2 had been radiated, 1 withcurative intent and 1 postoperatively. Followingsalvage surgery, the latter patient had a break-down of the neck soft tissues, which healed with20 hyperbaric oxygen treatments, whereas theother radiated patient healed uneventfully.
There was no evidence of LCMF necrosis dueto compromise of its vascular supply, and nobleeding was encountered intraoperatively whileelevating the flap, indicating that the vertebralartery is easy to avoid. The hypopharynx remuco-salizes in about 3 weeks, at which time patients
typically commenced their planned postoperativeRT. There were no delays in instituting RT due towound-healing problems.
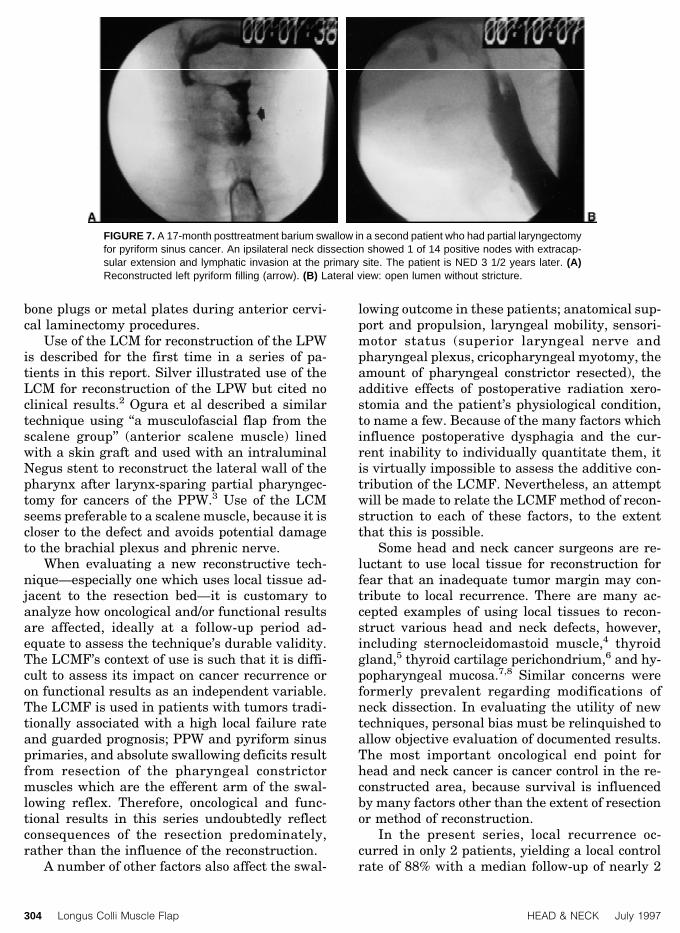
Figures 6 and 7 show modified barium swal-low results 1 and 1 1/2 years, respectively, follow-ing the completion of treatment in two represen-tative patients, documenting that it is possible torestore normal-appearing anatomy with thistechnique.
Neuromuscular Function. There was no impair-ment of neck flexion, probably because theremaining neck flexors (anterior, medial, and pos-terior scalenes, and usually the sternocleidomas-toid muscles) were left intact bilaterally. Interest-ingly, one patient had the opposite problem,difficulty with head extension requiring a cervicalcollar to help support his chin. Neurosurgical con-sultation failed to elucidate the cause.
FIGURE 2. Regional anatomy: deep neck muscles, vertebral artery, and sympathetic chain.
Longus Colli Muscle Flap HEAD & NECK July 1997 301

Three patients manifested Horner’s syndromepostoperatively. These patients all had PPW tu-mors abutting the skull base, and maneuvers inthe vicinity of the superior cervical ganglion werenecessary during resection. Horner’s syndromecan result from manipulation anywhere along thecourse of the cervical sympathetic chain and/organglia,1 so in patients with many primary tu-mors of the PPW it is not possible to differentiate
between tumor resection and mobilization of theLCMF as the cause of a postoperative Horner’ssyndrome.
Oncologic Results. The cancer-free survival ratewas 69% (11/16) with a median follow-up of 22months. Six patients are alive with no evidence ofdisease (NED), 5 have died NED, and 5 have diedwith cancer, 1 with local failure, 1 with neck fail-ure, 2 with distant metastases, and 1 with simul-taneous local and distant failure. Thus, the localcontrol rate was 88% (14/16) in a series of patientswith advanced tumors in unfavorable sites, 50%(8/16) T3 and T4 primaries and 88% (14/16) stageIII–IV.
Functional Results. Four of the patients operatedhad TLP, and their airway and voice results wereconsistent with the absence of the larynx: stomaand tracheoesophageal puncture speech. Three ofthese patients ate a normal diet by mouth, andone was restricted to a liquid diet, consistent withthe fact that even if the larynx is removed, pa-tients who have had an extensive resection of thepharyngeal constrictors (pharyngectomy) haveswallowing problems related to lack of bolus pro-pulsion. This also affects the ability of patientswith the larynx preserved to swallow their secre-tions.
Of the 12 patients who had the larynx pre-served—the main group of interest with respectto functional outcome—results were as follows: 7were decannulated, 4 wore a plugged tracheotomy
FIGURE 3. Cadaver dissection showing muscle layers of poste-rior pharynx. Larynx retracted medially (hook on posterior thyroidala). Pharyngeal constrictor muscle (1), longus colli muscle (2),anterior spinal ligaments (3). Chin (C).
FIGURE 4. MRI showing location of vertebral arteries (arrow) in low (A) and mid (B) neck.
302 Longus Colli Muscle Flap HEAD & NECK July 1997
tube, and 1 wore an unplugged tracheotomy tube.Because most of the patients had had resectionsfor PPW cancer and postoperative RT, trache-otomy was usually needed to help the patientsclear tenacious secretions rather than for airwaycompromise, per se. The voice was consideredgood to normal in 11 of the patients and poor in 1due to a concurrent hypoglossal nerve palsywhich affected articulation. With respect to swal-lowing, one third (n 4 4) were gastrostomy-dependent and two thirds (n 4 8) of the patientstook some or all of their nutrition by mouth.Three ate some by mouth with gastrostomysupplementation, and 5 took all nutrition bymouth, considered a ‘‘normal diet’’ in 3. Two pa-
tients demonstrated delayed deterioration inswallowing not due to hypopharyngeal stenosis,as documented on serial modified barium swallowstudies. This appeared to be related to aspiration(see Discussion).
DISCUSSION
The LCM and its blood supply are outside theusual territory of head and neck cancer surgery,because one of the traditional tenets of resection(now outmoded) was that tumors which violatedthe PVF should be considered technically unre-sectable. The LCM lies dorsal to the PVF and ismore familiar to neurosurgeons who mobilize themuscles off the spine and resuture them to cover
FIGURE 6. Modified barium swallow of patient in case presentation, 1 year posttreatment. (A) Sym-metric pyriform anatomy restored (arrow). (B) Open lumen without stricture.
FIGURE 5. Case presentation. Computed tomographic scans. (A) Preoperative: necrotic tumor of pyriform and paraglottic space ex-tending into neck under strap muscles. (B) Postoperative.
Longus Colli Muscle Flap HEAD & NECK July 1997 303
bone plugs or metal plates during anterior cervi-cal laminectomy procedures.
Use of the LCM for reconstruction of the LPWis described for the first time in a series of pa-tients in this report. Silver illustrated use of theLCM for reconstruction of the LPW but cited noclinical results.2 Ogura et al described a similartechnique using ‘‘a musculofascial flap from thescalene group’’ (anterior scalene muscle) linedwith a skin graft and used with an intraluminalNegus stent to reconstruct the lateral wall of thepharynx after larynx-sparing partial pharyngec-tomy for cancers of the PPW.3 Use of the LCMseems preferable to a scalene muscle, because it iscloser to the defect and avoids potential damageto the brachial plexus and phrenic nerve.
When evaluating a new reconstructive tech-nique—especially one which uses local tissue ad-jacent to the resection bed—it is customary toanalyze how oncological and/or functional resultsare affected, ideally at a follow-up period ad-equate to assess the technique’s durable validity.The LCMF’s context of use is such that it is diffi-cult to assess its impact on cancer recurrence oron functional results as an independent variable.The LCMF is used in patients with tumors tradi-tionally associated with a high local failure rateand guarded prognosis; PPW and pyriform sinusprimaries, and absolute swallowing deficits resultfrom resection of the pharyngeal constrictormuscles which are the efferent arm of the swal-lowing reflex. Therefore, oncological and func-tional results in this series undoubtedly reflectconsequences of the resection predominately,rather than the influence of the reconstruction.
A number of other factors also affect the swal-
lowing outcome in these patients; anatomical sup-port and propulsion, laryngeal mobility, sensori-motor status (superior laryngeal nerve andpharyngeal plexus, cricopharyngeal myotomy, theamount of pharyngeal constrictor resected), theadditive effects of postoperative radiation xero-stomia and the patient’s physiological condition,to name a few. Because of the many factors whichinfluence postoperative dysphagia and the cur-rent inability to individually quantitate them, itis virtually impossible to assess the additive con-tribution of the LCMF. Nevertheless, an attemptwill be made to relate the LCMF method of recon-struction to each of these factors, to the extentthat this is possible.
Some head and neck cancer surgeons are re-luctant to use local tissue for reconstruction forfear that an inadequate tumor margin may con-tribute to local recurrence. There are many ac-cepted examples of using local tissues to recon-struct various head and neck defects, however,including sternocleidomastoid muscle,4 thyroidgland,5 thyroid cartilage perichondrium,6 and hy-popharyngeal mucosa.7,8 Similar concerns wereformerly prevalent regarding modifications ofneck dissection. In evaluating the utility of newtechniques, personal bias must be relinquished toallow objective evaluation of documented results.The most important oncological end point forhead and neck cancer is cancer control in the re-constructed area, because survival is influencedby many factors other than the extent of resectionor method of reconstruction.
In the present series, local recurrence oc-curred in only 2 patients, yielding a local controlrate of 88% with a median follow-up of nearly 2
FIGURE 7. A 17-month posttreatment barium swallow in a second patient who had partial laryngectomyfor pyriform sinus cancer. An ipsilateral neck dissection showed 1 of 14 positive nodes with extracap-sular extension and lymphatic invasion at the primary site. The patient is NED 3 1/2 years later. (A)Reconstructed left pyriform filling (arrow). (B) Lateral view: open lumen without stricture.
304 Longus Colli Muscle Flap HEAD & NECK July 1997

years, and it is likely that the local recurrencesrelated more to the magnitude of the primary tu-mor than to the method of reconstruction. Of the2 patients who developed local recurrence, 1 had amassive PPW primary tumor abutting the skullbase measuring 11 cm at the level of the styloidprocesses. The second patient also had a verylarge PPW tumor filling the nasopharynx and apositive retropharyngeal node, both factors whichpredispose to local recurrence.
Oncologic concerns should be less for theLCMF than with reconstructions using someother tissue sources in the neck, because thismuscle is outside the territory traditionally re-sected in a head and neck cancer operation. Ofcourse, if tumor penetrates the PVF to involve theunderlying LCM, the muscle must be included inthe resection. In personal experience with opera-tions on 39 patients with primary cancers of thePPW, this situation was encountered only once inpreviously untreated patients.9 In that case, theLCM was included in the resection, and a pecto-ralis myofascial flap10 was used to form a newLPW (larynx preserved). That patient survivedfor 6 years to succumb to a second primary in thelung, free of cancer in the head and neck.
Thus, the rarity of local recurrence (2 of 16patients) suggests that use of the LCMF does notunduly compromise cancer control. Achieving lo-cal control rates comparable with those for glotticcancers is very favorable considering the prepon-derance of advanced stage and unfavorable pri-mary tumor characteristics which comprised thisseries.
It is possible to assess the most relevant earlyend point for a reconstructive method—woundhealing—and there were no wound-healing prob-lems (infections, fistulas) in previously untreatedpatients associated with the LCMF. The onlywound-healing problem occurred in 1 of the 2 pa-tients in which the technique was used followingRT. Silver stated that ‘‘for previously irradiatedpatients, closure with a regional skin flap or myo-cutaneous flap is preferred’’2 but gave no clinicaldata supporting this conclusion. In the absence ofevidence of flap necrosis or compromise of the ver-tebral artery by postoperative RT, there seems tobe no absolute contraindication provided by thisseries to use of the LCMF in previously radiatedpatients, and the present author will continue toinvestigate this context of flap use.
It is well-known that myofascial flaps contractover time, sometimes resulting in stricture forma-tion, and this contraindicates such a method of
reconstruction for a circumferential defect. Whenthe larynx is preserved, however, rigid supportcounteracts circumferential stenosis. The LCMFis not associated with problematic stricture for-mation, as documented in the modified bariumswallows presented in this paper (Figures 6 and7), which demonstrate that it is possible to dura-bly restore normal-appearing anatomy with thistechnique. Although the reconstructed pyriformis usually obliterated to some degree, and al-though some degree of contracture can be ex-pected to result from use of the LCMF, this maynot be a functional detriment. Especially in casesinvolving pharyngeal constrictor resection, a nar-rowed lumen may be better than one of normal oraugmented circumference, because it providesa nearby surface against which residual motoractivity in the pharynx can act; a narrowed hy-popharyngeal lumen may actually facilitateswallowing through a segment which lacks pro-pulsion. Similarly, if a reconstructive flap isinsensate, it may help to have a small lumenagainst which the opposite mobile laryngophar-ynx can appose.
Because sensation to the LCM is provided bythe redundant cervical plexus, it is likely thatsome sensation remains following elevation of theflap; however, this was not formally tested in thisseries. Documentation of hypopharyngeal sensa-tion with free flap reconstruction is also lackingdue to the difficulties of testing sensation in thisarea, so the proposition that other methods of‘‘sensate’’ flap reconstruction would be better isboth undocumented and based on a debatable as-sumption. The LCM has also been studied in re-construction of partial circumferential esophagealdefects in a canine model. No fistulas occurredand stricture tendency was decreased when a mu-cosal lining graft was used.11 A skin graft liningwas avoided in the present series, because itwould contribute to contraction, and the lack offistulization is evidence that additional lining isnot necessary.
Most reports of reconstructive techniques inthe head and neck literature include relativelyshort follow-up and few document changes overtime, although it is likely that such changes arenot rare. The airway and swallowing status dete-riorated in 2 patients in this series who had beendecannulated and were eating a normal diet bymouth, as described in the case presentation. Asecond patient who had LPP (T2N0 PPW cancer)and had normal functional results also developedincreasing dysphagia and supraglottic edema and
Longus Colli Muscle Flap HEAD & NECK July 1997 305

required retracheotomy 2 years following surgeryplus RT.
A stricture must be ruled out in any patientwith persistent, unexplained, posttreatment dys-phagia, but the negative effects of RT are alsoimportant. Neck fibrosis, which progresses overtime, and xerostomia are often overlooked causesof postoperative dysphagia. The contribution ofradiation to stricture formation has recently beennoted from our institution.12 Progressive, radia-tion-related, posttreatment neck fibrosis can po-tentially lead to laryngeal tethering (aggravatedby a tracheotomy tube when present), as mani-fested primarily in deteriorating swallowing re-sults with aspiration, and could be expected tohave a negative impact on any reconstructivetechnique over time. This pattern can be seen inany head and neck cancer patient with a pre-served larynx who has had RT as part of the treat-ment, and the negative impact of nonsurgicaltreatments on posttreatment swallowing functionis receiving increased attention in the recent lit-erature.13
The effect of postoperative RT on an operatedpharynx was also a factor in patients who re-quired prolonged tracheotomy; several patientsseemed to be dependent upon the easing sensa-tion of being able to clear their tenacious secre-tions via the tracheotomy, and airway obstructionwas seldom the main problem preventing decan-nulation. Nevertheless, of the patients with lar-ynx preserved, 58% (7/12) were decannulated.
With respect to the assessment of swallowing,it is important to take into account what is a base-line ‘‘normal’’ swallowing result for patients whohave had the larynx preserved but the pharyn-geal constrictors excised. In such patients, liquidsare handled much more easily than solids, and agood result is oral intake of a liquid/soft diet notrequiring feeding-tube supplementation. Whenthe patient is young and in good physical condi-tion, an essentially normal diet can sometimes beresumed. Based on this perspective, the swallow-ing result with LCMF reconstruction—all or someoral intake in 66% of the patients with the larynxpreserved—were consistent with other patientsundergoing similar cancer treatment but othermethods of reconstruction.
A potential critique is that local tissue recon-struction of the hypopharynx tethers laryngeal el-evation, which could negatively affect the swal-lowing result. Although the LCMF remainsattached to the spine posteromedially, the larynxitself (to which the flap is attached anterolater-
ally) remains mobile, especially if the surgical ap-proach is via a lateral or infrahyoid pharyn-gotomy which minimizes interference withsupport provided by the hyomandibular complex,in comparison with a transhyoid or suprahyoidapproach to a primary tumor of the PPW. Al-though possible, it is unlikely that the thin LCMFreconstruction would tether laryngeal elevationsignificantly; certainly no more so than would thebulk and weight of any other reconstructive flap,no matter how thin or well suspended. As notedabove, a major underestimated component of la-ryngeal tethering is undoubtedly progressive, ra-diation-related neck fibrosis.
A specific comparison with the sternocleido-mastoid myofascial flap (SCM-MFF) is in order,because it has been used to reconstruct similardefects. Alvi4 reported using the SCM-MFF withan extension of the SCM investing fascia in fourcases for laryngopharynx reconstruction. An en-dolaryngeal stent was left in place for 2–4 weeksand then removed endoscopically. One patient de-veloped a fistula ‘‘secondary to an oversizedstent,’’ which healed after removal of the stent.Whether or not stenosis occurred following stentremoval was not mentioned, the length of follow-up was not noted, and oncologic results were notreported in the small series. The flap was notused in patients with a prior history of neck irra-diation due to concern over its blood supply, al-though in other experience preoperative RT didnot appear to have a detrimental effect on SCMflap survival.14 Three of Alvi’s four patients wereradiated postoperatively, but the additive effect ofthis treatment was not discussed. The flap wasalso considered contraindicated in patients withimmobile nodal disease or when cancer involvedthe SCM.
The SCM-MFF is no longer used by the pres-ent author based on personal experience (unpub-lished) with this method to reconstruct a varietyof defects in the head and neck. Only 6 of 11 re-constructions healed without complications, de-spite careful elevation of the flap without compro-mising the superior blood supply above the levelof the spinal accessory nerve entrypoint, a nearly50% incidence of wound-healing complications.Three patients required additional surgery to cor-rect these problems, including 1 of the 2 caseswhere the flap was used to reconstruct a newLPW following partial laryngopharyngectomy.Immediate necrosis necessitated a return to theoperating room 12 hours later for debridment in
306 Longus Colli Muscle Flap HEAD & NECK July 1997

one patient, although the other healed unevent-fully.
Thus, the LCMF appears to have several ad-vantages over the SCM-MFF. The blood supply tothe LCMF—the vertebral artery—is less likely tobe compromised during flap elevation than that ofthe SCM-MFF. Alvi4 cited mobility as an advan-tage related to the SCM-MFF’s lack of bulk,which made it ‘‘ideal for reconstructing partialpharyngeal wall defects which allows for easyswallowing and minimal aspiration,’’ and theLCMF would be expected to be even more suitablebased on a ‘‘lack of bulk’’ criterion. The contrain-dication of immobile neck disease does not applyto the LCMF, and there is no absolute contrain-dication to use of the flap in patients who havehad prior RT, although experience with theLCMF in this context in this series was minimal.Also, no stent is required.
In this ‘‘high-tech’’ era of free flap reconstruc-tion, the literature reflects surgeon’s biases, andthere is a tendency to consider reconstructionwith local tissue as a lower form of endeavor.Such methods are sometimes derided as ‘‘fillers’’which plug a hole without any effort to restorenormal anatomy or function. The barium swal-lows evaluated in this series document the essen-tially normal reconstitution of anatomy which ispossible with the LCMF. Limitations to restoringhypopharyngeal function are common to all re-constructive flaps because of the inability to reli-ably restore sensation or mobility, among otherfactors. All flaps are ‘‘fillers’’ which are tailored tofit the defect, and many free flaps are quite small.Most flaps provide some degree of bulk which mayinterfere with deglutition. That more ‘‘sophisti-cated’’ methods of reconstruction reconstitute hy-popharyngeal anatomy and physiology betterthan reconstruction with local tissues is assumedrather than documented in the literature. The useof the LCMF also avoids the donor-site morbidityof myocutaneous, myofascial, or free flaps, whichhas been an issue with one of the most popularmethods of current reconstruction of hypopharyn-geal defects, the radial forearm free flap.15
In the absence of functional documentation inthe head and neck reconstructive literature as awhole, it is impossible to state the superiority ofany technique for hypopharyngeal reconstruction,but the LCMF has several advantages to recom-mend it: a reliable blood supply, technical ease,minimal additional operating time, and no re-quirement for a second reconstructive team or do-nor-site morbidity. Certainly, many surgeons will
continue to use other methods to reconstruct thisarea based on personal preference and training;however, this presentation adds another recon-structive option for LPW reconstruction: theLCMF. With compromise of neither oncologic norfunctional results, the LCMF emerges as a viablereconstructive option for full-thickness defects inthe lateral oropharynx and/or hypopharynx. Al-though the combination of extended partial lar-yngectomy or LPP with planned postoperative ir-radiation can result in functional problems whichmay increase over time, some motivated patientsmay prefer a surgical option with potential toachieve good voice and swallowing without astoma. This reconstructive method extends theindications for larynx preservation because thelarynx need no longer be resected simply to facili-tate closure. It also minimizes the need for freeflap or visceral interposition, decreases costs, andis within the capability of any head and neck sur-geon, factors which may help maintain surgery aspart of the initial treatment in patients with headand neck cancer, which is very important in opti-mizing their oncological outcome.16
REFERENCES1. Collins SL. The cervical sympathetics in surgery of the
neck. Otolaryngol Head Neck Surg 1991;105:544–55.2. Silver CE. In: Surgery for cancer of the larynx and related
structures. New York: Churchill Livingstone, 1981:177–178.
3. Ogura JH, Watson RK, Jurema AA. Partial pharyngecto-my and neck dissection for posterior hypopharyngeal can-cer. Immediate reconstruction with preservation of voice.Laryngoscope 1960;70:1523–1534.
4. Alvi A, Stegnjajac A. Sternocleidomastoid myofascial flapfor head and neck reconstruction. Head Neck 1994;16:326.
5. Kojima H, Omori K, Fugita A, et al. Thyroid gland flap forglottic reconstruction after vertical laryngectomy. Am JOtolaryngol 1990;11:328.
6. Stegnjajac A, Wenig BL, Guberina L, et al. Glottic recon-struction with thyroid perichondrium and investing cer-vical fascia. Arch Otolaryngol Head Neck Surg 1985;111:472.
7. Dumich PS, Pearson DW, Weiland LH. Suitability ofnear-total laryngopharyngectomy in pyriform carcinoma.Arch Otolaryngol 1984;110:664.
8. Salam MA, El-Kahky M, El-Mehary H. The use of pyri-form sinus mucosa for reconstruction after vertical partiallaryngectomy. J Laryngol Otol 1992;106:900.
9. Collins, SL. Cancer of the posterior pharyngeal wall: re-versing the poor prognosis in the head and neck. Triologi-cal thesis, 1996. Submitted for publication. Laryngoscope.
10. Smith PG, Collins SL. Repair of head and neck defectswith thin and double-lined pectoralis flaps. Arch Oto-laryngol Head Neck Surg 1984;110:468–473.
11. Bouayad H, Caywood DD, Alyakine H, et al. Surgical re-construction of partial circumferential esophageal defectsin the dog. J Invest Surg 1992;5:327–342.
12. Bastian RW, Taitz A. Post-radiation stenosis: an over-looked cause of dysphagia after partial laryngectomy. Ab-
Longus Colli Muscle Flap HEAD & NECK July 1997 307

stract. Am Acad Otolaryngol Head Neck Surgery, Wash-ington DC, September 29–October 2, 1996.
13. Lazarus CL, Logemann JA, Pauloski BR, et al. Swallow-ing disorders in head and neck cancer patients treatedwith radiotherapy and adjuvant chemotherapy. Laryngo-scope 1996;106:1157.
14. Tiwari R. Experiences with the sternocleidomastoidmuscle and myocutaneous flaps. J Laryngol Otol 1990;104:315.
15. Brown MT, Cheney ML, Gliklich RL, et al. Assessment offunctional morbidity in the radial forearm free flap donorsite. Arch Otolaryngol Head Neck Surg 1996;122:991–994.
16. Collins, SL. Controversies in multimodality therapy forhead and neck cancer: clinical & biological perspectives.In Thawley SE, Panje WR, Batsakis J, Lindberg R, Eds.Comprehensive management of head and neck tumors,2nd ed. W.B. Saunders: in press. 1997.
308 Longus Colli Muscle Flap HEAD & NECK July 1997





























