Embed Size (px)
Citation preview

Journal of Neurology, Neurosurgery, and Psychiatry 1985;48:297-301
Occasional review
The limbic system and the localisation of herpessimplex encephalitisANTONIO R DAMASIO,* GARY W VAN HOESEN*t
From the Departments ofNeurology* and Anatomyt, University ofIowa College of Medicine, Iowa City,Iowa, USA
SUMMARY The selective destruction of temporal and frontal lobe structures by herpes simplexencephalitis has been explained as a consequence of the proximity of those regions to the point ofentry of the virus in the encephalon, through olfactory pathways or meningeal branches of thetrigeminal nerves. An alternative hypothesis is presented: that the encephalitis is due to a specialaffinity of the herpes simplex Type 1 virus for the limbic cortices, that is, that distinctiveneuroanatomical, neurochemical and neuroimmunological properties of those cortices permit thevirus to manifest its destructive behaviour, regardless of the route of entry to the CNS, possiblyduring altered immunological states. The study of the neurochemical and neuroimmunologicalproperties of the limbic cortices may be a useful approach to the enigma of why and when herpessimplex Type 1 causes encephalitis.
Despite some advances in antiviral therapy, herpessimplex encephalitis is still a devastating and oftenfatal disease.' Patients who survive do so with majordefects of memory and affect, often incompatiblewith personal and social rehabilitation. The agent ofthe encephalitis, the herpes simplex virus Type 1,resides latent, possibly for many years, in the trigem-inal ganglia of its victims.2 4 But the reason why thevirus abandons its dormant state to invade and des-troy the central nervous system remains a mystery.It is also not known why the virus selectively dam-ages some neural structures of the temporal andfrontal lobes and spares most other cortices, graymatter nuclear masses and related white matter.Considering that infection with herpes simplex virusType 1 is highly prevalent in humans, it is importantto discover (a) why the virus turns from relativelybenign tenant to malignant invader, (b) the route
Address for reprint requests: Antonio R Damasio, MD PhD,Department of Neurology. University of Iowa Hospitals & Clinics,Iowa City, IA 52242, USA.
Received 8 June 1984 and in revised form 6 September 1984.Accepted 18 September 1984
This work was supported by NINCDS Grant P01 NS 19632-01.
taken to invade the central nervous system, and (c)the reasons why a specific set of neural structures isconsistently chosen as target. In this article weaddress the latter two issues.The first explanation proposed for the unique
localisation of herpes simplex encephalitis invokedintranasal inoculation and spread along the olfactorypathways into the nearby temporal and frontal cor-tices.5 More recently, Davis and Johnson advancedanother explanation.6 They postulated that from itslatent site in the trigeminal ganglia, the virus wouldtravel through the tentorial branches of the trigemi-nal nerve in the direction of the dura mater. Becausethe tentorial nerves supply the dura mater in boththe middle and anterior fossae, in and about theareas that the mesial and polar temporal lobes andthe inferior surface of the frontal lobes directly over-lie,' the virus would then travel in cell to cell contactacross the meninges and into the subjacent cortices.Both explanations are plausible but they do not
acknowledge (a) that the structures damaged byherpes simplex encephalitis are part of an anatomi-cal and functional neural unit, the limbic system; (b)that the boundaries of that anatomical system arerespected, often faithfully, by the destructive pro-cess; (c) that if the location of damage would be due
297

298
solely to proximity to the area of entry, then therewould be no explanation for why the process rarelytrespasses into other territories; (d) that althoughmeningeal branches of the ophthalmic divisions ofthe trigeminal nerve do innervate dura mater in reg-ions directly across from limbic cortices, they alsocontribute innervation to other areas of the dura inthe middle and anterior fossae,78 the overlying cor-tex of which is generally not involved.
Anatomical and pathological features of herpesencephalitis
Herpes encephalitis causes selective damage to thegray matter of the entire limbic system, for examplethe allocortices and the mesocortices (periallocortexand proisocortex). It severely involves hippocampalformation, including the subicular cortices (allocor-tical structures) and the amygdala, as well as theparahippocampal gyrus; the perirhinal cortex; theagranular insular cortex; the posterior orbitofrontalcortex; the paraolfactory gyrus of Broca; and theanterior cingulate cortex, structures that togetherconstitute the mesocortices. Cytoarchitecturally, the
Damasio, Van Hoesen
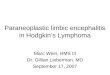
mesocortices are an intermediate structure, lesselaborate than the 6-layered isocortex (also knownas neocortex) which forms most of the telencepha-Ion but more complex than the allocortices whichconstitute the hippocampal formation and thesuperficial parts of the amygdala.9 Both allocorticesand mesocortices are relatively less myelinated andcontain neuronal types that are unique as well asmicrovascular patterns that are unlike those of othercortices.'° " Moreover, they contain a high concen-tration of opiate receptors,'2 abundant quantities oftrace metals, high concentrations of indoleamines,catecholamines, cholinergic enzymes and, in gen-eral, less oxidative enzymes than the isocortices.'3Finally, but perhaps of no lesser importance, is thefact that the mesocortices are powerfully intercon-nected via large association bundles such as the cin-gulum and the uncinate fasciculus'4 and that they arealso connected with the subicular allocortices'5 andwith the subcortical amygdaloid nuclei'617 (fig 1).The encephalitis consistently involves nearly thetotality of the limbic mesocortices as well as theamygdala and hippocampal formation. Only theposterior cingulate cortex, which is cytoarchitectur-ally different from the anterior, may escape its pil-
(Subicular projectionsLimbic lobe
tPoggrapjyy
Fig 1 Diagrams ofthe medial surface ofa higherprimate brain, depicting: A. the topography ofthe meso and allocorticesthat constitute the limbic lobe; B. two major pathways that interconnect various parts ofthe limbic lobe; C. the topographyofallocortical subicular projections to the limbic lobe; D. the topography ofamygdaloid projections to the limbic lobe. Notehow the distribution ofthese projections coincides with the areas destroyed by herpes simplex encephalitis.
~1

The limbic system and the localisation of herpes simplex encephalitis
lage. (A note should be made here of the fact thatthe anterior cingulate gyrus, Brodmann's area 24,although seldom mentioned as a damaged zone intextbook descriptions, was destroyed in nearly allpublished cases we reviewed and in all necropsycases personally observed; the concentration of viralantigen in the anterior cingulate was extremely high,of the same magnitude as that found in other limbiccortices.'8) Furthermore, the boundary between thelimbic cortices damaged by herpes simplexencephalitis and the nonlimbic cortices in the vicin-ity, is remarkably sharp, especially in the cingulategyrus and in the orbito-frontal region. For instance,necrosis of the cingulate is halted at the cingulatesulcus where the cytoarchitecture changes to giveway to the supplementary motor area. In the hori-zontal plane, necrosis stops at the boundary betweenBrodmann' s area 24 and 23 (the anterior and post-erior cingulate regions, respectively). The nearbygenu of the corpus callosum is commonly spared.This sharpness of boundaries is often less marked inthe temporal lobe component of the lesions wherenecrosis, haemorrhage and ischaemia caused by theencephalitis affect a wider group of cortical and sub-cortical structures; the destruction can be massive,with ensuing collapse of regions that extend beyondthe frontier of the limbic system. In other words,although it is true that both neurons and glia areinvolved in the process of herpes encephalitis, wedoubt that it would be possible to spare glia selec-tively considering the type of pathological processesset in motjon by the virus. On the other hand, atleast in adults, the encephalitis does prefer a specifictype and site of neural structure-the oldest cortexin phylogenetic evolution and one that isneuroanatomically and neurochemically dis-tinctive-while it refrains from destroying neuralstructures that do not belong to that particular type,namely all of the isocortex. The fact that herpessimplex encephalitis in infants fails to respect thesecytoarchitectonic boundaries further emphasises thepoint that, in adults, the response of limbic corticesto this agent is especially distinctive. It is possible,for instance, that the immunologic properties oflimbic and non-limbic neurons are different in theadult. The recent description of a monoclonal anti-body for membrane proteins which specificallylabels cells in the limbic cortices but leaves non-limbic elements unlabelled, is of special impor-tance."9
Hypothesis
Our hypothesis can be stated as follows: The initialmode of transport of the virus would be in a retro-
grade direction from cutaneous receptors to itslatent site in the trigeminal ganglion. From there, bymeans of transganglionic transport across the gang-lion cell soma, the virus would travel anterogradelyin the central root in the direction of the brainstemand of the trigeminal nuclei. The virus would thenspread transneuronally to limbic related nuclei, suchas the raphe and locus coeruleus. Those nuclei havewell known and widespread ascending projections tomesencephalic, diencephalic and telencephalicareas. Utilising these neural channels the viruswould be distributed almost everywhere in the cere-bral cortices but only in the limbic cortices of theadult would it find the proper terrain to multiply anddestroy nervous tissue, possibly in circumstances ofdisturbed immunity. The elaborate intrinsic connec-tivity of the limbic cortices would augment the"seeding' of the virus within that system, againthrough exclusively normal neural connections.The evidence in favour of this hypothesis is as
follows: (1) in both bilateral and unilateral cases ofadult herpes encephalitis, the lesions almost invari-ably fall, in a monotonous pattern, in the structuresof the limbic system reviewed above; (2) damage inthese structures is systematic, that is, it leaves noanatomical "gaps" and generally respects cytoar-chitectonic boundaries with non-limbic areas; inva-sion either through peripheral branches of thetrigeminal nerves or through the olfactory nerves,would be likely to cause patchier involvement, withislands of spared tissue, and it is difficult to acceptthat it might respect cytoarchitechtonic frontiers; (3)Esiri's immunohistological study of the distributionof viral antigen in the brains of herpes encephalitisvictims shows that the limbic cortices are the siteswhere viral antigen is concentrated;'8 the infection isheaviest in the granule cells of the dentate gyrus ofthe hippocampal formation; it is noteworthy that thelocus coeruleus and raphe nuclei project strongly tothe hilum of the dentate gyrus and thus their termi-nals are immediately adjacent to the granule cellsthat together form a hilum;202' (4) the mapping ofviral antigen in brains with herpes encephalitisstudied at different stages during the first threeweeks post-onset of the disease, suggests a 'wave"of infection spreading rapidly from limbic structureto limbic structure; the subacute progression of"limbic" symptomatology could be explained by anaccrual of limbic involvement due to this mode ofanatomical spread; all along the neural chain theaffinity of the virus for certain types of neuronswould be the determinant factor, (for example, viralantigen has been found throughout the telencepha-lon, including the isocortical motor strip, yet nec-rosis of that type of cortex is rarely reported at nec-ropsy nor are signs related to its dysfunction part of
299

300
the clinical picture of herpes encephalitis); (5) evi-dence from experimental studies in animals by Kris-tensson and associates,22 suggests that the virus maytravel the natural, CNS-bound route of the trigemi-nal nerve, and that it can infect the main sensory andspinal trigeminal nuclei and even continue alongthat neural system, transneuronally, toward thereticular formation, the raphe nuclei, the locuscoeruleus and sensory thalamus.A note should be made here of the fact that the
olfactory bulb receives input from some brainstemareas that do not receive olfactory bulb projectionsthemselves. Especially remarkable are the rapheand locus projections, which explain the abundantserotoninergic and noradrenergic terminals in thebulb.23 This means that the olfactory bulb could beinfected via a trigeminal mode of entry, instead ofdirectly, which might account for the inconsistentviral infection noted in the bulb.6
Although arguments for a trigeminal route ofentry appear, at the moment, more persuasive thanarguments for an olfactory route, the issue is farfrom settled. The bulb might be a conduit ratherthan a target, in much the same manner of thetrigeminal ganglion. The ganglion is only rarely des-troyed in herpes encephalitis in spite of its role as
reservoir. There is, thus, no reason why the bulbshould necessarily be destroyed.A comment should also be made about Kristens-
son's studies in animals sacrificed 3 to 4 days aftercutaneous inoculation of the virus. The virus had bythen travelled to brain stem-nuclei and to the con-
tralateral thalamus but no mention is made of viralpresence in cortical limbic system structures or sen-
sory cortex. Assuming that was specifically lookedfor and not encountered, and leaving aside speciesdifferences, we suspect that absence was to beexpected considering the time required forintralimbic anatomical spread to take place. In thisregard it is important to keep in mind that the con-
centration of viral antigens found in Esiri's studywas dependent upon the time after onset,'8 and thatclinical evidence clearly documents a subacute prog-
ression of signs compatible with gradual spread.In conclusion, we are persuaded that herpes simp-
lex encephalitis is the consequence of a specialaffinity of the herpes simplex Type 1 virus for theadult limbic cortices (allo, periallo and proisocor-tices) which permits the virus to manifest its destruc-tive behaviour. That behaviour is not manifested inthe phylogenetically newer cortices (isocortex)which the virus can also gain access to but tends notto destroy. The route of entry may be of secondaryimportance, though it appears that a trigeminalneural route is the most plausible. An alteredimmunological state may be an adjuvant factor. We
Damasio, Van Hoesen
suggest that the study of the neurochemical andneuroimmunological properties of the limbic cor-tices may be a useful approach to the matters ofwhy, when and how herpes simplex Type 1 willstrike its host.
Refemces
'Adams RA, Victor M. Principles ofNeurology, 2nd Edi-tion New York. McGraw-Hill Book Company, 1981.
2 Baringer JR. Herpes simplex virus infection of nervoustissue in animals and man. Prog Med Virol1975;20: 1-26.
3Baringer JR, Swoveland P. Recovery of herpes-simplexvirus from human trigeminal ganglions. N Engl J Med1973;288:648-50.
4Bastion FO, Rabson AS, Yee CL, et al. Herpes virushominis: isolation from human trigeminal ganglion.Science 1972; 178:306-7.
5 Johnson RT, Mims CA. Pathogenesis of viral infectionsof the nervous system. N Engl J Med 1968:278:23-38,84-92.
6 Davis LE, Johnson RT. An explanation for the localiza-tion of herpes simplex encephalitis. Ann Neurol1979;5:2-5.
Penfield W, McNaughton F. Dural headache and inner-vation of the dura mater. Arch Neurol Psychiat1940;44:43-75.
8 Feindel W, Penfield W, McNaughton F. The tentorialnerves and localization of intracranial pain in man.Neurology (Minneap) 1960; 10:555-63.
Filimonoff IN. A rational subdivision of the cerebral cor-tex. Arch Neurol Psychiat 1974;58:296-310.
'0 Lorente de No R. Studies on the structure of the cerebralcortex. I. The area entorhinalis, J Psychol Neurol1983;45: 381-438.
"Pfeifer RA. Die Angioarchitektonische areale Gliederundder Groshirnrinde. Leipzig Thieme, 1940.
12 LaMotte CC, Snowman A, Pert CB, Synder SH. Opiatereceptor binding in the rhesus monkey brain: associa-tion with limbic structures. Brain Res 1978; 155:374-9.
13 Friede RL. Topographic Brain Chemistry, New YorkAcademic Press, 1966.
14 Van Hoesen GW, Pandya DN, Butters N. Some connec-tions of the entorhinal (area 28) and perirhinal (area35) cortices of the rhesus monkey. II Frontal lobeafferents. Brain Res 1975;95:25-38.
Krettek JE, Price JL. Projections from the amygdaloidcomplex to the cerebral cortex and thalamus in the rat
and cat. J Comp Neurol 1977; 172:678-722.16 Rosene DL, Van Hoesen GW. Hippocampal efferents
reach widespread areas of cerebral cortex and amyg-dala in the rhesus monkey. Science 1977; 198:315-7.
7 Porrino LJ, Crane AM, Goldman-Rakic PS. Direct andindirect pathways from the amygdala to the frontallobe in the rhesus monkey. J Comp Neurol1981;198: 121-36.
8 Esiri MM. Herpes simplex encephalitis: An immunohis-tological study of the distribution of viral antigenwithin the brain. J Neurol Sci 1982;54:209-26.

The limbic system and the localisation ofherpes simplex encephalitis
9 Levitt P. A Monoclonal Antibody to Limbic SystemNeurons. Science 1984;223: 299-301.
20 Moore RY, Halaris AE. Hippocampal innervation byserotonin neurons of the midbrain raphe in the rat. JComp Neurol 1975;164:171-84.
21 Moore RY. Monoamine neurons innervating the hip-pocampal formation and septum. In: The Hippocam-pus. KH Pribram, RL Isaacson eds. New York,
Plenum Press, 1975.22 Kristensson K, Nennesmo I, Persson L, Lycke E.
Neuron to neuron transmission of herpes simplexvirus. J Neurol Sci 1982;54:149-56.
23 Broadwell RD. Society for Neuroscience Symposia III,
Aspects ofBehavioural Neurobiology, Neurotransmit-ter pathways in the olfactory system, Washington Soc-iety for Neurosciences 1978; 131-66.
301