Embed Size (px)
Citation preview

Eur J Hast Surg (1995) 18:115-117 European 1 ~ 1 • • J . . . . . Iof I~l~ii£I-Iilrb
Sur'g W" © Springer-Verlag 1995
The islanded V-Y advancement myocutaneous gluteus maximus flap: its use in three cases of late post-radiation soft tissue necrosis in the sacral area
B. Malavaud 1, K. Cohen 2, P. Martel 2
l Department of Urology and Transplantation CHU Purpan, 1 place du Dr. B aylac, F-31059 Toulouse Cedex, France 2 Centre Claudius Regaud, 20-24 rue du Pont Saint Pierre, F-31052 Toulouse Cedex, France
Abstract. Experience with the island V-Y advancement myocutaneous gluteus maximus flap is presented. The original description has been modified. The superior and inferior thirds of the muscle are preserved intact, the skin and muscle are excised in order to create a muscu- locutaneous island which can be moved to the midline with an inverting movement. There is no loss of function as assessed clinically in all cases and neurophysiologi- cally in one case.
Key words: Radionecrosis - Gluteus maximus - Myo- cutaneous flap
Radiation necrosis of the sacral area is no longer a com- mon long-term complication of pelvic radiotherapy. It is a painful and disabling condition, the surgical treatment of which has been with diverse myocutaneous flaps. Since 1987, three cases of extensive sacral radiation ne- crosis have been treated using an island V-Y advance- ment myocutaneous gluteus maximus flap. This differs from the technique described by Ramirez [1] in 1984 since distal muscle fibres are cut.
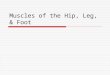
The gluteus maximus is a thick, superficial muscle, quadrangular in shape that originates from the ilium, sacrum, coccyx, the sacrosciatic and sacrotuberous liga- ments and inserts along the greater trochanter and the linea aspera. Its blood supply is rich and complex, and is summarized in Fig. 1. The superior gluteal artery enters the gluteal space above the piriformis muscle, 5 cm from the sacral edge [2] and runs along the deep surface of the muscle, supplying the upper half of the gluteus maximus and the gluteus medius while the inferior gluteal artery enters the gluteal space under the piriformis muscle and runs distally to the cruciate anastomosis, where is anas- tomoses with the femoral system [3]. Many flaps can be
Correspondence to: B. Malavaud
S "~ .?
S /
2
Fig. 1. Left gluteal area. 1 Gluteus maxlmus divided; 2 Gluteus medius m.; 3 Piriformis m.; 4 Superior gluteal artery; 5 Inferior gluteal artery; 6 Inferior gluteal nerve; 7 Sciatic nerve; 8 Greater trochander
planned on this blood supply whose richness is useful in covering areas with reduced vascularity such as paraple- gic ulcers, radiation necrosis, and lumbosacral meningo- myelocele defects [1, 3-6].
Case reports
This technique which will be described in detail later has been used successfully in three female patients (76, 68, and 66 years of age) treated 16, 18, and 20 years earlier by external beam therapy for carcinoma of the cervix, presenting sacral soft tissue necrosis (6x3 cm; 10×10 cm; 10x8 cm).
After an initial superficial wound excision, a twice daily hy- pertonic glucose dressing was applied until the wounds were clean and appeared vascular. Antibiotics were given according to the bacterial culture of tissue samples. No bowel preparation was em- ployed.
Under general anesthesia, the patients were placed in prone position, lying on a bolster placed under the lower part of the

116
Fig. 2. 1 Preservation of the arterial branches originating from the superior and inferior gluteal arteries. 2 Electrocautery division of the distal part of the flap
GLUTEUS MAXIMUS DISTAL DIVISION OF GLLrfEUS NLA.V~ML'S
\ \
MEDIAL ADVANCEMENT I
NNN
I N ' V t ~ R T I N G M O V E M I ~ N T ~ ~ Ill[[
Fig. 3. Schematic representation of the medial advancement (1) and of the inverting movement (2) that re-creates the natal cleft
chest and pubic area. The area of necrosis was excised by sharp dissection. Laterally it was necessary to resect beyond the field of irradiation as indicated by the original marker tattoos. Ultimately, the bed of the resected area were quadrangular in shape.
A superficial sacral osteotomy and a superficial carbon dioxide laser vaporization were then performed.
The flaps were drawn as triangles whose internal edges were marked by the excision margins. A line was then drawn between the posterior iliac spine and the summit of the greater trochanter. To mark the upper border of the flap, the skin and the subcutane- ous tissue along a 15 to 20 cm parallel line were sharply incised. The gluteus maximus muscular bundles run parallel to the incision and were easily split by blunt dissection. Two to three small branches of the superior gluteal artery needed ligation.
The dissection was completed at the inferior edge. The muscle was bluntly separated and the dissection carried distally to the summit of the triangle.
The gluteal space, between gluteus maximus and gluteus me- dius, was easy to locate and scissors were carefully inserted through the upper edge. The distal part of the flap was divided with electrocautery.
Therefore, a myocutaneous island was made, where skin and muscle were completely incised all the way through both layers, preserving the superior and inferior pedicles (Fig. 2) that were seen running along the deep surface of the flap. No attempt was made to locate the sciatic nerve, and the flap was advanced medi- ally and with an inverting movement that recreates the natal cleft (Fig. 3).
Four suction drains were inserted, one over each gluteus maxi- mus flap and two in the sacral area. Closure was performed in two layers.
For three days postoperatively, an attempt was made to de- crease the blood viscosity with low molecular weight dextran and low molecular weight heparin. For two days the patients rested prone on a normal hospital bed. On the third postoperative day they were mobilized to resume walking for short periods, sitting for meals was not allowed before the tenth postoperative day. The patients were discharged three weeks later with no specific treat- ment (Fig. 4).
D i s c u s s i o n
I r radia t ion m a y cause extens ive t issue necros is which can be repa i red with gluteus max imus flaps. This repor t shows that these ulcers can be repa i red with b i la tera l is- l anded s l iding myocu taneous gluteus max imus flaps. The dis ta l inc is ion o f some gluteus max imus fibres differs f rom Rami rez where the inser t ing fibres o f the il- io t ib ia l t ract and femur are left intact [1]. It is easy to pe r fo rm and does not requi re extens ive and pos s ib ly dangerous d i ssec t ion of the supply ing gluteal ar ter ies
Fig. 4. a Late post-radiation necrosis of the sacral area. b post-operative result (same patient)

117
[1]. As the muscle is divided all the way around the cir- cumference of the flap creating a musculocutaneous is- land, the closure with an inverting movement which recreates the natal cleft is easily done without tension even for large defects.
It does not impair running, jogging, or stable one- legged standing in our three cases. Neurophysiological testing was performed in one of our patients. It exhibited no difference between the superior and inferior parts of the glutens maximus on both sides that are left intact in our technique and control areas as tibialis anterior and quadriceps femoris.
These facts are not surprising since the superior part of the muscle inserted medially on the ilium which is functionally the most important segment of the muscle [7] and the inferior part inserted on the sacro sciatic and sacrotuberous ligaments where the motor innervation begins [1] are left intact.
Conclusion
This modified procedure lead to a gluteus maximus mus- culocutaneous island whose closure with an inverting
movement is easily performed and recreates the natal cleft. It preserves the function and allows the closure of sacral defects of reduced vascularity as post-radiation necrosis.
References
1. Ramirez OM, Orlando JC, Hurwitz DJ (1984) The sliding glu- teus maximus myocutaneus flap: its relevance in ambulatory patients. Plast Reconstr Surg 74:68
2. Mathes SJ, Nahai F (1979) Clinical atlas of muscle and muscu- locutaneous flaps. Mosby, St Louis
3. Becker H (1979) The distally-based glutens maximus muscle flap. Plast Reconstr Surg 63:653
4. Buchanan DL0 Agris J (1983) Gluteal plication closure of sac- ral pressure ulcers. Plast Reconstr Surg 72:49
5. Stevenson TR, Pollock RA, Rhorich RJ, VanderKolk CA (1987) The gluteus maximus musculocutaneous island flap: re- finements in design and application. Plast Reconstr Surg 79: 761
6. Ramirez OM, Ramasastry SS, Granick MS, Pang D, Futrell JW (1987) A new surgical approach to closure of large lumbosacral meningomyelocele defects. Plast Reconstr Surg 80:799
7. Stern JT (1972) Anatomical and functional specializations of the human gluteus maximus. Am J Phys Anthropol 36:315