Embed Size (px)
Citation preview

258
Although the influence of gender on the manage-ment of coronary artery disease1-4 is well established,there are few studies reporting the effect of gender onthe management of peripheral arterial disease. It hasbeen suggested that female gender not only mayadversely affect selection for abdominal aorticaneurysm (AAA) repair5,6 but also may be associatedwith significantly poorer outcome after surgery.5,7
The aim of the current study was to examine theeffect of gender on selection for surgery, periopera-
tive mortality, and long-term outcome after repair ofRAAA in a regional vascular surgery unit in Scotland.
METHODSThe Lothian Surgical Audit8 is a prospectively
gathered, computerized database in which demo-graphic, clinical, operative, and outcome details forall surgical admissions to hospitals within LothianRegion, Scotland, are recorded. Interrogation of thisdatabase resulted in the identification of 692 patients(542 men and 150 women) who were admitted tothe Edinburgh Regional Vascular Unit with RAAAbetween January 1, 1983, and December 31, 1995.A patient was defined as having had an operation ifan anesthetic was given with the intention of repair-ing the aneurysm, regardless of whether a graft wasinserted. In these patients, RAAA was defined as thepresence of retroperitoneal and/or intraperitonealblood in the absence of any identifiable cause otherthan an aortic aneurysm. In patients who were notoperated on, the presence of an aortic aneurysm wasconfirmed by means of ultrasonography in 29
The influence of gender on outcome afterruptured abdominal aortic aneurysmStephen M. Evans, BSc, FRCSEd, Donald J. Adam, FRCSEd, and Andrew W.Bradbury, MD, FRCSEd, Edinburgh, United Kingdom
Background: The influence of gender on the management of coronary artery disease iswell documented, but few reports exist regarding the influence of gender on the man-agement of peripheral arterial disease.Objective: The purpose of this study was to examine the influence of gender on selectionfor and short-term and long-term outcomes of repair of ruptured abdominal aorticaneurysm (RAAA) in a regional vascular surgery unit.Methods: Analysis of the prospectively gathered Lothian Surgical Audit database identi-fied 692 patients (542 male and 150 female) admitted with RAAA between January 1,1983, and December 31, 1995. Case notes were reviewed for patients who were admit-ted but not operated on. Operative mortality was defined as death within the same hos-pital admission. Long-term survival data were obtained from the General RegisterOffice (GRO1 records) through record linkage by the Information and StatisticsDivision of the National Health Service of Scotland.Results: A total of 542 men (78%; median age, 72 years; age range, 46-93 years) and 150women (22%; median age, 74 years; age range, 55-93 years) were admitted with RAAA(P = .12; Mann-Whitney U test). There was no significant difference in perioperativemortality between men and women. Although women who were not operated on (medi-an age, 81 years; age range, 68-93 years) were significantly (P = .005) older than menwho were not operated on (median age, 77 years; age range, 54-93 years), for any givenage group, women appeared less likely than men to be offered surgical repair. Long-termsurvival after successful repair was comparable for the genders.Conclusions: Gender has no influence on either short-term or long-term outcome forpatients undergoing operative repair of RAAA. However, women are less likely to beselected for operation than their male counterparts. (J Vasc Surg 2000;32:258-62.)
From the Vascular Surgery Unit, University Department ofClinical and Surgical Sciences, Royal Infirmary of Edinburgh.
Competition of interest: nil.Reprint requests: Mr Stephen M. Evans, Royal Infirmary of
Edinburgh, Vascular Studies Unit, 1 Lauriston Place,Edinburgh EH3 9YW, United Kingdom.
Copyright © 2000 by The Society for Vascular Surgery and TheAmerican Association for Vascular Surgery, a Chapter of theInternational Society for Cardiovascular Surgery.
0741-5214/2000/$12.00 + 0 24/1/106948doi:10.1067/mva.2000.106948
JOURNAL OF VASCULAR SURGERYVolume 32, Number 2 Evans, Adam, and Bradbury 259
patients (27%), and the diagnosis of rupture was con-firmed with computerized tomography in fivepatients (5%). Only six patients (6%) underwent post-mortem examination, which confirmed the diagnosisin each case. In all other cases, the diagnosis wasbased on clinical assessment by a vascular surgeon atthe time of admission. Discharge letters and casenotes for all nonoperated patients were scrutinized,and when the information was available, the reasoncited by the admitting surgical team for deciding notto operate was recorded. Operative mortality wasdefined as death during the same hospital admission.Long-term survival data were obtained from theGeneral Register Office (GRO1 records) throughrecord linkage by the Information and StatisticsDivision of the National Health Service of Scotland.
The χ2 test and Fisher exact test were used forstatistical analysis when appropriate, and the logrank test was used for comparison of survival curves.A probability value of less than .05 was regarded asstatistically significant.
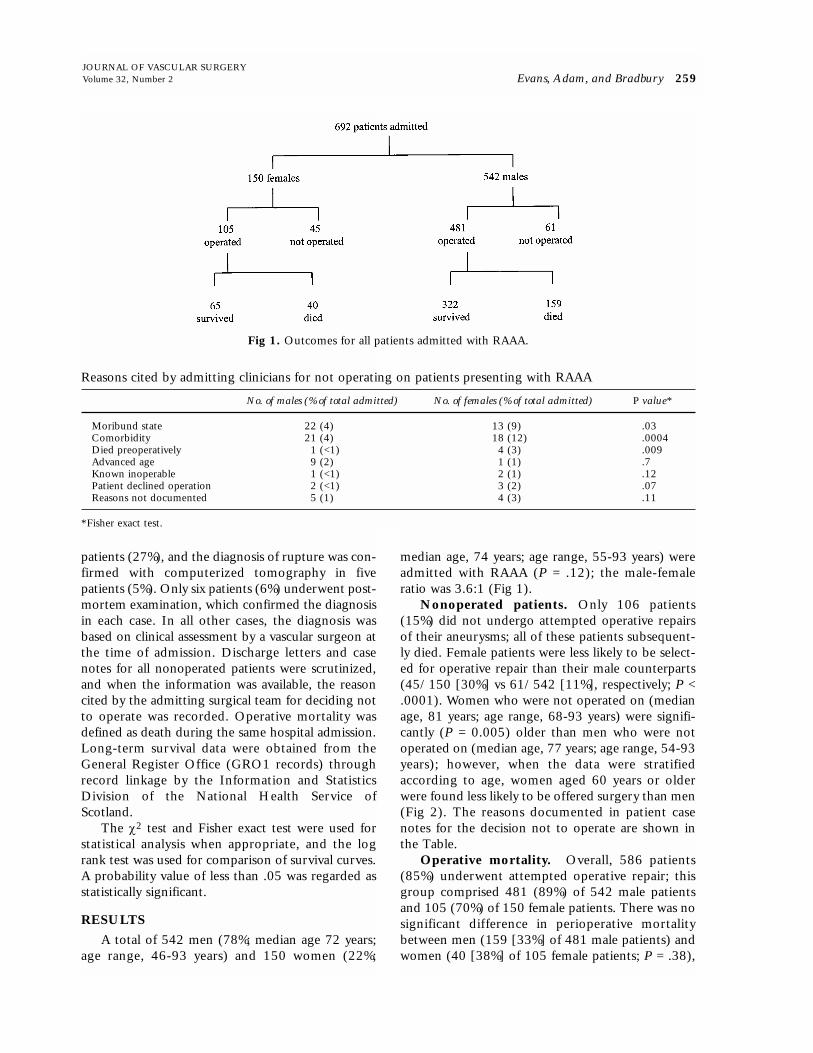
RESULTSA total of 542 men (78%; median age 72 years;
age range, 46-93 years) and 150 women (22%;
median age, 74 years; age range, 55-93 years) wereadmitted with RAAA (P = .12); the male-femaleratio was 3.6:1 (Fig 1).
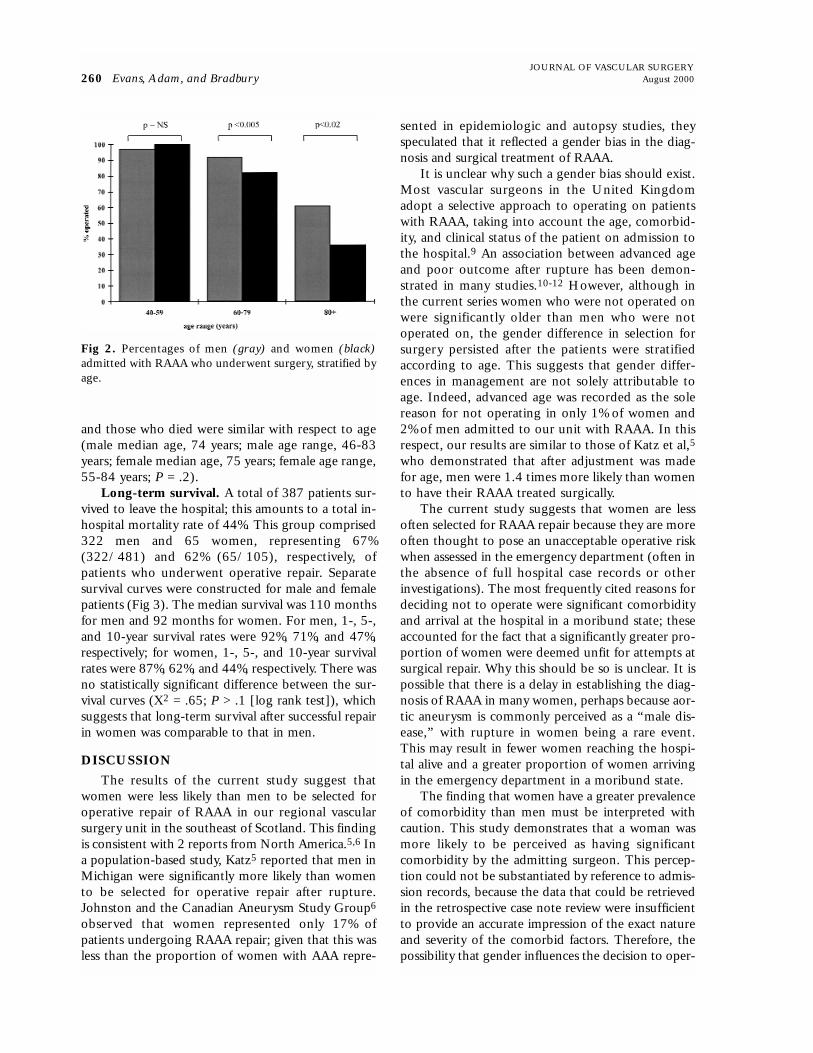
Nonoperated patients. Only 106 patients(15%) did not undergo attempted operative repairsof their aneurysms; all of these patients subsequent-ly died. Female patients were less likely to be select-ed for operative repair than their male counterparts(45/150 [30%] vs 61/542 [11%], respectively; P <.0001). Women who were not operated on (medianage, 81 years; age range, 68-93 years) were signifi-cantly (P = 0.005) older than men who were notoperated on (median age, 77 years; age range, 54-93years); however, when the data were stratifiedaccording to age, women aged 60 years or olderwere found less likely to be offered surgery than men(Fig 2). The reasons documented in patient casenotes for the decision not to operate are shown inthe Table.
Operative mortality. Overall, 586 patients(85%) underwent attempted operative repair; thisgroup comprised 481 (89%) of 542 male patientsand 105 (70%) of 150 female patients. There was nosignificant difference in perioperative mortalitybetween men (159 [33%] of 481 male patients) andwomen (40 [38%] of 105 female patients; P = .38),
Fig 1. Outcomes for all patients admitted with RAAA.
Reasons cited by admitting clinicians for not operating on patients presenting with RAAA
No. of males (% of total admitted) No. of females (% of total admitted) P value*
Moribund state 22 (4) 13 (9) .03Comorbidity 21 (4) 18 (12) .0004Died preoperatively 1 (<1) 4 (3) .009Advanced age 9 (2) 1 (1) .7Known inoperable 1 (<1) 2 (1) .12Patient declined operation 2 (<1) 3 (2) .07Reasons not documented 5 (1) 4 (3) .11
*Fisher exact test.
and those who died were similar with respect to age(male median age, 74 years; male age range, 46-83years; female median age, 75 years; female age range,55-84 years; P = .2).
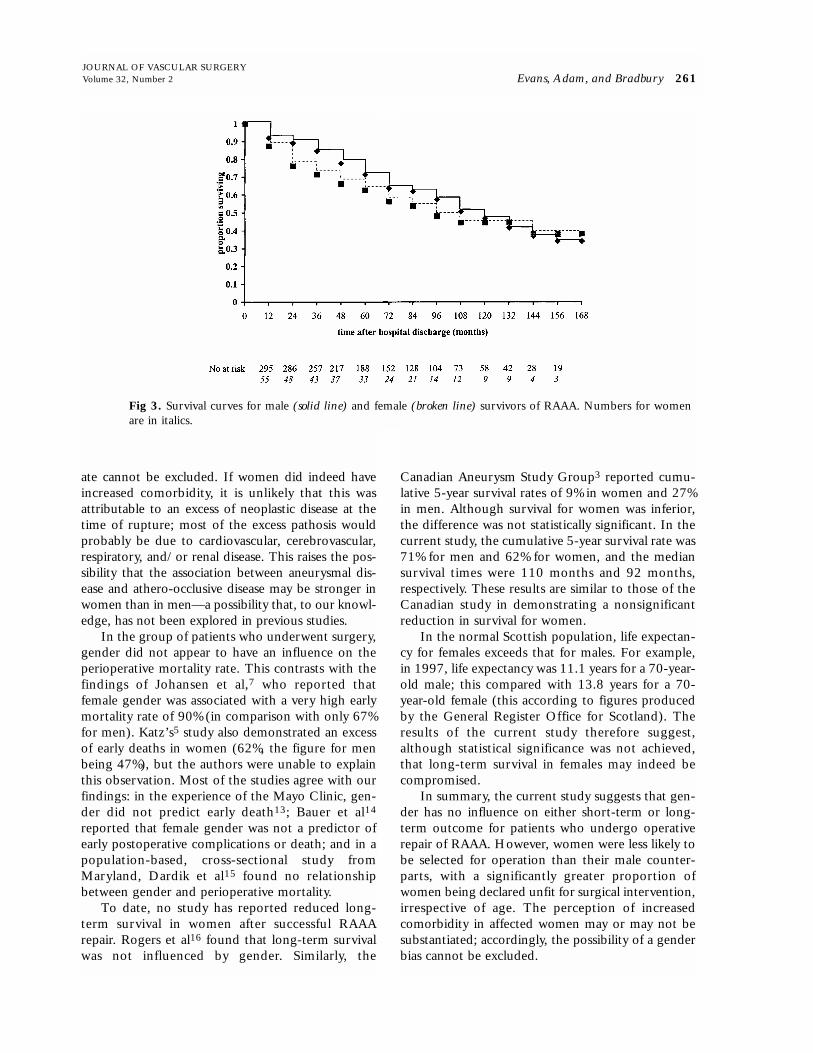
Long-term survival. A total of 387 patients sur-vived to leave the hospital; this amounts to a total in-hospital mortality rate of 44%. This group comprised322 men and 65 women, representing 67%(322/481) and 62% (65/105), respectively, ofpatients who underwent operative repair. Separatesurvival curves were constructed for male and femalepatients (Fig 3). The median survival was 110 monthsfor men and 92 months for women. For men, 1-, 5-,and 10-year survival rates were 92%, 71%, and 47%,respectively; for women, 1-, 5-, and 10-year survivalrates were 87%, 62%, and 44%, respectively. There wasno statistically significant difference between the sur-vival curves (Χ2 = .65; P > .1 [log rank test]), whichsuggests that long-term survival after successful repairin women was comparable to that in men.
DISCUSSIONThe results of the current study suggest that
women were less likely than men to be selected foroperative repair of RAAA in our regional vascularsurgery unit in the southeast of Scotland. This findingis consistent with 2 reports from North America.5,6 Ina population-based study, Katz5 reported that men inMichigan were significantly more likely than womento be selected for operative repair after rupture.Johnston and the Canadian Aneurysm Study Group6
observed that women represented only 17% ofpatients undergoing RAAA repair; given that this wasless than the proportion of women with AAA repre-
sented in epidemiologic and autopsy studies, theyspeculated that it reflected a gender bias in the diag-nosis and surgical treatment of RAAA.
It is unclear why such a gender bias should exist.Most vascular surgeons in the United Kingdomadopt a selective approach to operating on patientswith RAAA, taking into account the age, comorbid-ity, and clinical status of the patient on admission tothe hospital.9 An association between advanced ageand poor outcome after rupture has been demon-strated in many studies.10-12 However, although inthe current series women who were not operated onwere significantly older than men who were notoperated on, the gender difference in selection forsurgery persisted after the patients were stratifiedaccording to age. This suggests that gender differ-ences in management are not solely attributable toage. Indeed, advanced age was recorded as the solereason for not operating in only 1% of women and2% of men admitted to our unit with RAAA. In thisrespect, our results are similar to those of Katz et al,5who demonstrated that after adjustment was madefor age, men were 1.4 times more likely than womento have their RAAA treated surgically.
The current study suggests that women are lessoften selected for RAAA repair because they are moreoften thought to pose an unacceptable operative riskwhen assessed in the emergency department (often inthe absence of full hospital case records or otherinvestigations). The most frequently cited reasons fordeciding not to operate were significant comorbidityand arrival at the hospital in a moribund state; theseaccounted for the fact that a significantly greater pro-portion of women were deemed unfit for attempts atsurgical repair. Why this should be so is unclear. It ispossible that there is a delay in establishing the diag-nosis of RAAA in many women, perhaps because aor-tic aneurysm is commonly perceived as a “male dis-ease,” with rupture in women being a rare event.This may result in fewer women reaching the hospi-tal alive and a greater proportion of women arrivingin the emergency department in a moribund state.
The finding that women have a greater prevalenceof comorbidity than men must be interpreted withcaution. This study demonstrates that a woman wasmore likely to be perceived as having significantcomorbidity by the admitting surgeon. This percep-tion could not be substantiated by reference to admis-sion records, because the data that could be retrievedin the retrospective case note review were insufficientto provide an accurate impression of the exact natureand severity of the comorbid factors. Therefore, thepossibility that gender influences the decision to oper-
JOURNAL OF VASCULAR SURGERY260 Evans, Adam, and Bradbury August 2000
Fig 2. Percentages of men (gray) and women (black)admitted with RAAA who underwent surgery, stratified byage.
JOURNAL OF VASCULAR SURGERYVolume 32, Number 2 Evans, Adam, and Bradbury 261
ate cannot be excluded. If women did indeed haveincreased comorbidity, it is unlikely that this wasattributable to an excess of neoplastic disease at thetime of rupture; most of the excess pathosis wouldprobably be due to cardiovascular, cerebrovascular,respiratory, and/or renal disease. This raises the pos-sibility that the association between aneurysmal dis-ease and athero-occlusive disease may be stronger inwomen than in men—a possibility that, to our knowl-edge, has not been explored in previous studies.
In the group of patients who underwent surgery,gender did not appear to have an influence on theperioperative mortality rate. This contrasts with thefindings of Johansen et al,7 who reported thatfemale gender was associated with a very high earlymortality rate of 90% (in comparison with only 67%for men). Katz’s5 study also demonstrated an excessof early deaths in women (62%, the figure for menbeing 47%), but the authors were unable to explainthis observation. Most of the studies agree with ourfindings: in the experience of the Mayo Clinic, gen-der did not predict early death13; Bauer et al14
reported that female gender was not a predictor ofearly postoperative complications or death; and in apopulation-based, cross-sectional study fromMaryland, Dardik et al15 found no relationshipbetween gender and perioperative mortality.
To date, no study has reported reduced long-term survival in women after successful RAAArepair. Rogers et al16 found that long-term survivalwas not influenced by gender. Similarly, the
Canadian Aneurysm Study Group3 reported cumu-lative 5-year survival rates of 9% in women and 27%in men. Although survival for women was inferior,the difference was not statistically significant. In thecurrent study, the cumulative 5-year survival rate was71% for men and 62% for women, and the mediansurvival times were 110 months and 92 months,respectively. These results are similar to those of theCanadian study in demonstrating a nonsignificantreduction in survival for women.
In the normal Scottish population, life expectan-cy for females exceeds that for males. For example,in 1997, life expectancy was 11.1 years for a 70-year-old male; this compared with 13.8 years for a 70-year-old female (this according to figures producedby the General Register Office for Scotland). Theresults of the current study therefore suggest,although statistical significance was not achieved,that long-term survival in females may indeed becompromised.
In summary, the current study suggests that gen-der has no influence on either short-term or long-term outcome for patients who undergo operativerepair of RAAA. However, women were less likely tobe selected for operation than their male counter-parts, with a significantly greater proportion ofwomen being declared unfit for surgical intervention,irrespective of age. The perception of increasedcomorbidity in affected women may or may not besubstantiated; accordingly, the possibility of a genderbias cannot be excluded.
Fig 3. Survival curves for male (solid line) and female (broken line) survivors of RAAA. Numbers for womenare in italics.

JOURNAL OF VASCULAR SURGERY262 Evans, Adam, and Bradbury August 2000
REFERENCES
1. Steingart RM, Packer M, Hamm P, et al. Sex differences inthe management of coronary artery disease: survival and ventricular enlargement investigators. N Engl J Med1991;325:226-30.
2. Chiriboga DE, Yarzebski Y, Goldberg RJ, et al. A communi-ty-wide perspective of gender differences and temporal trendsin the use of diagnostic and revascularisation procedures foracute myocardial infarction. Am J Cardiol 1993;71:268-73.
3. Eysmann SB, Douglas PS. Reperfusion and revascularizationstrategies for coronary artery disease in women. JAMA1992;268:1903-7.
4. Petticrew M, McKee M, Jones J. Coronary artery surgery:are women discriminated against? BMJ 1993;306:1164-6.
5. Katz DJ, Stanley JC, Zelenock GB. Gender differences inabdominal aortic aneurysm prevalence, treatment, and out-come. J Vasc Surg 1997;25:561-8.
6. Johnston KW, Canadian Society for Vascular Surgery AneurysmStudy Group. Influence of sex on the results of abdominal aor-tic aneurysm repair. J Vasc Surg 1994;20:914-26.
7. Johansen K, Kohler TR, Nicholls SC, Zierler RE, ClowesAW, Kazmers A. Ruptured abdominal aortic aneurysm: theHarborview experience. J Vasc Surg 1991;13:240-7.
8. Aitken RJ, Nixon SJ, Ruckley CV. Lothian Surgical Audit; a15-year experience of improving surgical practice throughregional computerised audit. Lancet 1997;350:800-4.
9. Hewin DF, Campbell WB. Ruptured aortic aneurysm: the deci-sion not to operate. Ann R Coll Surg Engl 1998;80:221-5.
10. Shackleton CR, Schecter MT, Bianco R, Hildebrand HD.Preoperative predictors of mortality risk in ruptured abdom-inal aortic aneurysm. J Vasc Surg 1987;6:583-9.
11. Johnston KW, Canadian Society for Vascular SurgeryAneurysm Study Group. Ruptured abdominal aorticaneurysm: 6-year follow-up results of a multicenter prospec-tive study. J Vasc Surg 1994;19:888-900.
12. Hardman DTA, Fisher CM, Patel MI, et al. Rupturedabdominal aortic aneurysms: who should be offered surgery?J Vasc Surg 1996;23:123-9.
13. Gloviczki P, Pairolero PC, Mucha P Jr, et al. Rupturedabdominal aortic aneurysms: repair should not be denied. JVasc Surg 1992;15:851-9.
14. Bauer EP, Redaelli C, von Segesser LK, Turina MI. Rupturedabdominal aortic aneurysms: predictors for early complica-tions and death. Surgery 1993;114:31-5.
15. Dardik A, Burleyson GP, Bowman H, et al. Surgical repair ofruptured abdominal aortic aneurysms in the state ofMaryland: factors influencing outcome among 527 recentcases. J Vasc Surg 1998;28:413-21.
16. Roger VL, Ballard DJ, Hallett JW, Osmundson PJ, Puetz PA,Gersh BJ. Influence of coronary artery disease on morbidityand mortality after abdominal aortic aneurysmectomy: a pop-ulation based study, 1971-1987. J Am Coll Cardiol1989;14:1245-52.
Submitted Oct 12, 1999; accepted Jan 6, 2000.





























