Embed Size (px)
Citation preview

Journal of Audiovisual Media in Medicine 1986, 9, 4 4 4 9 Printed in Great Britain
The history of medical illustration GABRIEL DONALD
Keynote address from the IMBl Annual Conference at the University of Aberdeen (September 1985).
Over t h e years I have been very pri- vileged t o undertake a number o f tasks on behalf of our Institute, but this is one I never dreamt would come my way and I should like to thank the Conference Committee for the honour they have conferred o n me by their invitation to give the Keynote Address. As your guest. I am permitted to say what I like. itnd a s my hosts y o u must sit and suffer in silence. You are not permitted any p;irliamentary licence to shout 'Rub- bish' if y o u don't agree with what I have t o say. Now. having established our re- spective roles in this performance-let me get o n with the job.
The invitation suggested that my theme should be. the History of Medic- al Illustration. and it seemed to me that this was not an inappropriate time to take ii look at ou r past. Over the last two o r three years we have suffered a number of blows to o u r prestige and it would be surprising i f our morale were n o t ,just ii little dented. We have seen our protracted negotiations with the DHSS come to naught, after being almost on the point of resolution; we have been embroiled in the problems of trade unions (whose only interest is in the lowest common denominator); rejected by the Professions Supple- mentary to Medicine and the new tech- nology that is stalking the land has sent shock waves through all our thinking. And yet, we have a heritage of which to be proud. As St. Paul might have said. 'we are citizens of n o mean city'. So, I want to look at where we come from and consider some of the personalities and changes in technology that have in- fluenced our development. I n the pro- cess. I hope we shall see that we are fully justified in asserting our historic role in the professions allied to medicine.
Guhr-iel Doriuld MBE. / ) A . A T / ) . ARPS. FMAA. b/M/l/(/fo, ,) is /he former Direcror of Medical Illitsrruiiori u / rke Uiiiversiry 05 Glusgow.
Figure 1. Probably the first illustration (Roman).
Early records
I f we are looking for the earliest medic- al illustrations, ancient Egypt would appear to be the ideal place to find them. The Egyptians pictured their civi- lisation on papyrus rolls and sculptured reliefs and produced the world's first surgical textbook around the time of Tutankhamen-1700 BC. It describes in detail 48 cases of battle wounds and their treatment, 'when you examine a man with a gaping wound in his head- something in there which flutters under your fingers-then you must say a man with a gaping wound in his head is a sickness that cannot be treated', but i t contains no illustrations. However, a number of illustrations of medical in- terest are found mainly on sculptured reliefs on tombs of the 25th Century BC.
The Greek artists, like the Egyptians, used everyday themes in their decora- tive arts and most aspects of their cul- ture and medicine can be found in
of an outpatient c h i c dated 4UUBC
paintings on their black figure pottery, dating from 400 BC.
Aristotle, the Greek philosopher and scientist and founder of biological inves- tigation, is supposed to have used draw- ings in his teaching; but it was not until the end of the 4th and the beginning of the 3rd Century BC that diagrams to illustrate medicine were produced in Alexandria where the first Greek ana- tomists were at work. They are thought to have been a set of five schematic figures showing veins, arteries, nerves, bones and muscles.
When Alexandria was absorbed into the Roman Empire on the death of Cleopatra in 30BC. Greek scientific curiosity, which had already started to fade, was replaced by the practical approach of the Romans. It was not a time for new ideas; but for consolidat- ing knowledge from existing sources. Galen, the prince of physicians, who dominated medicine in the 2nd Century A D , did just that. He fused into one system all the medical ideas of his day. Human dissection was frowned upon in
J V
is C
omm
un M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
11/
24/1
4Fo
r pe
rson
al u
se o
nly.

2nd Century Greece and, although he wrote many books on anatomy and phy- siology and described his findings in great detail, he derived his facts from his dissection of pigs and monkeys. Galen died in 199AD and with the rise of Christianity and its emphasis on the soul and not the body. medical inves- tigation virtually came to a halt.
A new beginning
After the fall of the Roman Empire civilisation slipped into the so-called Dark Ages. Consequently, there are few medical manuscripts before the 10th Century and the illustrations with- in them are rare and crude. Neverthe- less, from the 1 Ith Century onwards, an increasing number of miniatures and an occasional full-page illustration began to appear. They are very similar in style to contemporary ecclesiastical art for the simple reason that the Church dominated the making of books, but they have left a record of the state of knowledge and practice of the period. They were not always purely decora- tive, but sometimes seem to have been deliberate attempts to illustrate a point in the text.
Until the 14th Century medicine was taught exclusively on the text of Galen who had died 1100 years before. His work, which had received the approval of the Church, was regarded as a can- on about which there could be no dis- pute.
When a mediaeval doctor was faced with a problem of diagnosis or treat- ment, the Prince of Physicians would be able to provide a satisfactory answer. In illustrations he is always shown gowned and dignified in robes trimmed with ermine; a very pillar of the establish- ment.
Universities were growing fast in the 14th and 15th Century, and the urgent need for books far outstripped the capacity of the scribes to produce them. There had already been a number of unsuccessful attempts to solve the tech- nical problems of printing, but in the middle of the 15th Century, Gutenberg succeeded brilliantly in solving them all-metal alloys, dies, paper. printing ink. printing press-and, at a stroke, originated a method of printing from movable type that was to be used with- out radical changes until the 20th Cen- tury.
With the invention of printing it was now possible to produce books with illustrations which could be printed in
Figure 2. Outpatient clinic at the time when the church dominated medical illustration. The style is similar to contemporary ecclesiastical art.
large numbers from wood-cut blocks instead of being laboriously and often wrongly copied by hand. It has been estimated that by the end of the 15th Century about eight million books had been printed. The first printed book to contain illustrations of medical interest was an Herbarius printed by Peter Schoeffer, at Mainz, in 1484. It con- tained a number of rather crude illustra- tions of herbs. The 15th Century was bursting with new ideas. Artists were throwing off the mediaeval traditions as they discovered the classical art of ancient Greece. Faced with these mas- terpieces they were stimulated to take an interest in the accurate representa- tion of the human body.
A bronze tablet by Donatello dated 1430 and known as the 'Anatomy of the Miser's Heart', shows the growing in- terest in dissection as a means of gaining first-hand knowledge of the body. The artists cared nothing for the divine Galen, but relied on their own observa- tions in their study of human pro- portions, surface anatomy and the mus- cles and their movement. Naturalism in art now came to maturity, and there is evidence that a long line of artists in- cluding Verrochio, Michelangelo and Raphael all performed dissections. To- wards the end of the 15th Century hu- man dissection was officially authorised by a Papal Bull of Sixtus IV. who had himself studied medicine at Padua. and this stimulated a new approach to the study of anatomy.
Leonardo de Vinci It was characteristic of the Renaissance, that it was the genius of Leonardo de Vinci that initiated the new era. One o f the greatest artists of all time. architect, geologist and mechanical engineer, he seemed capable of understanding every- thing. 'A good painter', he said, 'has two objects to paint-man and the in- tention of his soul; the former is easy. the latter hard because he has to repre- sent it by attitudes and movements of his limbs'.
I f Leonardo went to academic de- monstrations he must have been bitterly disappointed for he had a stinging re- buke for the established method of teaching by wordy discourse. 'When you speak of the representation of any- thing that possesses substance and is surrounded by surface. I counsel you not to cumber yourself with words un- less you are speaking to the blind. Do not busy yourself in making enter by the ears things that have to d o with the eyes for in that y o u will be surpassed by the artist.' This was the revolutionary prin- ciple that altered the whole course of anatomy and established the artist as an indispensable partner in research.
As with every project to which he put his mind. Leonardo was soon deeply involved in fundamental research. Laborious dissection and meticulous illustration formed the contents of his book, Of /he Human Figure referred to as early a 1489. 'This plan of mine will be unfolded to y o u as though you had
The Journal of Audiovisual Media in Medicine (1986) Vol. 9INo.2 45
J V
is C
omm
un M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
11/
24/1
4Fo
r pe
rson
al u
se o
nly.

the natui-iil m;in before you. Begin your iinatoniy with ;I nian fully grown: then show him elderly and less muscular: then go on t o strip him stage by stage right down to the bones. And ofter- wards. you should make the child SO its
to show the womb.' Independent sources have confirmed that Leonardo dissected personiilly over 30 bodies of males and females. He spoke of the natural repugnance with which these studies could be regarded and the fear of passing the night hours in the coni- p i n y o f corpses. quartered and Hayed and horrible t o behold.
Nevertheless. because of his great skill ;is ; i n artist he was able to present his findings in ways that had never been thought of before. He wiis able t o use techniques thxt were fitmiliar to him in architecture by drawing plans and sec- tions; in engineering by making ex- ploded drawings of parts that were closely related to each other; and he could visualise what was happening in depth atid create ;I three dimension;d triiiisparent figure. All this was com- pl e t e 1 y new 11 n d revolution ii ry .
Of over 7000 sheets contained in the 120 books o f his drawings and notes o n iinatomy o n l y 200 sheets remain. Although the work was never pub- lished, the anatomical researches of Leonardo were well known to his con- temporaries. His approach to anatomy was the beginning of modern scientific method. with carefully controlled inves- tigation. detailed recording and accu- rate illustrntion of the findings. It soon bore f ru i t in the Medical Schools; from this time onward illustrated anatomical textbooks began to appear.
Vesalius
The University of Padua was the centre o f the scientific renaissance when Andreas Vesalius had the degree of Doctor o f Medicine conferred on him on 5 December. 1537. O n the following day he wiis appointed Professor of Sur- gical Anatomy. H e was just 23 years of age. Like Leonardo. 50 years before him. he soon recognised that the estab- lished system of teaching anatomy was wrong. To quote his own words. 'the detestable procedure now in vogue is that one man has to carry out the dissec- tion while the lecturer is perched up aloft in ii pulpit like a jackdaw and drones out information about facts he never approaches at first hand.' Vesa- lius began his own dissections. At the request of his students he made a draw- ing of the veins which as he said,
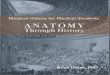
Figure 3. The bones from the human body presented from the posterior aspect by Andreas Vesalius 7 543.
'proved to be s o pleasing that they urged me to supply a description of the arteries and nerves'. In 1538, he puh- lished six anatomical tables. the first three of which he had drawn himself. These unbound fugitive sheets or post- ers, a s we would call them, were hand coloured. The skeletons that made up the other three tables of the set were the work of Stephanus or Calcar as he is more commonly called. These were the first reasonably accurate skeletons to be published. Accurate study of Galen's text finally brought Vesalius to the con- viction that Galen had never dissected a human body. He had been cheated by his monkeys. The whole study of ana- tomy had to begin anew. Vesalius col- lected his findings for his great book The Fuhricu. It was the first complete and systematic description of the human body. The Fuhricu is a large volunie (670 pages and 186 plates). Vesalius himself said that the text was of secon- dary importance to the illustrations and he made certain that they were not only scientifically accurate, but artistically superb and reproduced by the highest art form available-the woodcut. Some of the wood-cuts measure over 20 inches high. The illustrations show liv- ing anatomy. The drawings have been attributed to Calcar. but these master- pieces are more likely to have been the
work of :I group o f well trained artists from the studio of Titian who found ;inatomical illustration ;in exciting chal- lenge. However, the study was fraught with frustrations since bodies were dif- ficult to obtain. Usually they were of criminals who had been executed by hanging or bodies stolen from graves by his enthusiastic assistants but. in one case. when Vesnlius was studying the optic nerves. be was presented with ;I
head still warm from the executioner's axe. Vesalius also h;id problems with the ii rt is t ic t e m pe ra in e n t d u ri ng the course of the work. When i t was all over he wrote. ' N o longer shall I have to put up with the bad temper o f artists and engravers who made me more miser- able than the bodies I was dissecting.'
Although the drawings were m x l e i t , Venice. and the wood blocks cut there, the book was printed i n Bask . in 1533. by Oporinus who was the master printer of the day. Vesalius spent almost ii
whole year at Bask supervising every stage of the printing
The learned Galenists were now alarmed at the dun ge ro us1 y explosive nature of his research and his own teacher. Sylvius of Paris. poured scorn on the new fangled use of figures f o r the illustration of anatomical facts and c;iI- led upon him, ' t o renounce his heretical statements. to confess his mistakes and publicly to declare his faults lest by his pestilent breath he poison the rest of Europe'. In 1544, when still only ;I
young man of 30, Vesalius decided that he had had enough and determined to leave Padua. He Hung his unpublicised manuscript into the fire and so ended his brilliant academic c x e e r which had lasted barely five years. Nevertheless. in that short time he had revolutionised the study of anatomy. initiated the era of scientific investigation in medicine: produced what is still acknowledged to be one of the tinest medical textbooks and a supreme example of the art o f printing; and established the future role of medical illustration a s an indispensi- ble partner in medical research. Indeed, Leonardo can be described as the father of medical art and the work of Vesalius as the first real partnership between the artist and the doctor. Ironically. Vesa- lius had scarcely given up his research in despair before his work was being blatantly stolen all over Europe.
In 1533, Thomas Geminus. who had been commanded by Henry Vll l to bring English medicine up-to-date. pub- lished a plagiarised version of the Fuhri- cu. However. instead of using wood- cuts, he used copper-plate engravings.
46 Donald
J V
is C
omm
un M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
11/
24/1
4Fo
r pe
rson
al u
se o
nly.

These were the first copper-plate en- gravings of any consequence produced in England.
After Vesalius had shown the way many famous teachers followed in his footsteps and the tinest illustrations were produced by Continental artists particularly from Holland and Ger- many. The tables of skeletons and mus- cles of Albinus are the finest produced in the 18th Century. Albinus in his in- troduction to the book writes. 'to this end 1 employed an artist very skilful in drawing and engraving and I encour- aged him by giving him whatever he demanded for his trouble' Jan Wande- lar was guided by the Professor in all the work. Not a single picture was drawn free-hand; everything was measured and brought down to scale.
I n Glasgow the name of William Hunter is enshrined in the Hunterian Museum which contains the treasures that he bequeathed to the University. In addition to unique examples of the works of Vesalius there is a copy of his own famous book on the gravid uterus which contains some magnificent en- gravings. The original drawings were by ;I Dutch artist Van Rymsdyk working in England in the 18th Century and Hun- ter's instructions to him are very in- teresting. 'I asked him to see that the figures were well finished for in ana- tomy where the subject is imperfectly known. the smaller parts must be stu- died with as much care as the larger masses'. There is a collection of Ryms- dyk drawings in Glasgow which shows that Hunter's instructions were carried out to the letter. They are in red chalk, beautifully modelled and show subtle- ties of form that were not always trans- lated into the engravings. Van Rymsdyk also produced a set of anatomical draw- ings known as the Fothergill Collection which became the nucleus of the teaching collections of John Hopkins Medical School in the USA.
From art to photography
I have concentrated mainly on anato- mical illustration because it presented a fairly continuous theme. But, research in medicine was not confined to ana- tomy. With the rapid growth of patholo- gical anatomy and the medical special- ties there was an increasing need to describe and record all the fine changes of disease. Skin diseases, for example, were difficult to describe in words and wax models or water-colour drawings that could be turned into coloured en- gravings or lithographs meant that dis-
eases could be pictured in atlases and made available for study. And what the physician was seeing through the micro- scope and all the other diagnostic tools that were being invented had to be pic- tured and published and made available for teaching.
The rapidly expanding field of opera- tive surgery could only be illustrated by artists who could understand the medic- al problems and bring an informed mind and a skilled hand to their portrayal. As Michelangelo had said, 'an artist draws with his brains and not his hands'. Thus, a new type of artist was needed. one who would specialise in illustrating the whole range of medicine, not just anatomy-the forerunner of the mod- ern medical artist. Medicine looked in- creasingly to the artist for help in re- cording its research and in the presenta- tion of its results and he ruled supreme as the eyes of medicine until Niepce and Daguerre unlocked the treasure chest of photographic images and art was shaken to its very foundations. Af- ter it had recovered its senses, the reac- tion of established art to photography was twofold. On one hand, it was viewed with dismay and led to that fatuous and oft quoted remark, 'from today painting is dead'. On the other, it was seen as a cleansing fire which would turn art away from the superficial real- ism into which it had sunk. Many artists hoped that photography would function as a servant to art. but it was so much in tune with the mechanical achievements of the age that it could not be held in check.
By the 1860's photographers had con- vincingly broken through the quaran- tine imposed on them. Anxiety about photography grew to a new pitch. 'Art's mortal enemy', it was now called. The love-hate relationship between art and photography was well and truly estab- lished. In 1840, immediately following the Daguerrotype and the development of Fox Talbot's calotype process, the craft of the miniature painter was the first to suffer. Those who wanted minia- tures found that a photograph could guarantee a perfect likeness a t a frac- tion of the cost. Next to fall were the second-rate portrait painters. They were no great loss to art, but they were an asset to photography; many of them turned to it for a living and brought to it more than mere technical skill. Other artists turned to photography for help. One of these was David Octavius Hill who, together with Robert Adamson, an Edinburgh photographer, produced hundreds of photographs for a huge
Figure 4. Early medical photograph of a patient with a sarcoma of the lower femur 7889. (This photograph is from the Pringle Collection). With acknowledgements to the Greater Glasgow Health Board Archived Department of Medical Illustration Glasgow Royal Infirmary.
portrait group he was painting. The pic- ture, which was commissioned to com- memorate the first general assembly of the new Church of Scotland contains 474 likenesses and is a disaster; but the photographs are among the finest photographic portraits ever produced. The most frequent use of photographs by artists was in portrait painting. A good photograph helped to reduce the interminable sittings. G . F. Watts who was famous for his subject pictures des- paired of the difficulty of painting likenesses. 'It has cost me more labour to paint a portrait than a subject pic- ture'. H e was full of admiration for the soft portraits of Julia Cameron. ' I wish I could paint such a picture as this', he said, on seeing one of her studies; but some artists were not so kindly disposed to photography. When Yvon was paint- ing the Battle of Solferino he wanted to portray Louis Napoleon mounted on a horse and he engaged a photographer to take a photograph in the Tuileries as a study. H e was dismayed to find that while his picture was hanging proudly in the Salon, the photographer was selling prints to the public on the streets of Paris. H e had thought that by hiring the photographer he had acquired the rights
The Journal of Audiovisual Media in Medicine (1986) Vol.9tNo.2 47
J V
is C
omm
un M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
11/
24/1
4Fo
r pe
rson
al u
se o
nly.

to the photograph which. of course. he wanted to suppress.
A frequent cause of misunderstand- ing between artist and photographer is the belief t h a t the camera sees nature as the artist sees it. This is far from the case. Indeed, when we get into the realms of how we see things we get into deep psychological waters. It was Oscar Wilde who said, ‘things are because we see them, and how we see them de- pends on the art that has influenced us.’ The important difference between the camera and the artist is how the image is recorded. The camera sees a whole ob- ject a t once while the human eye can focus on only a small area at a time. Consequently, we observe an object by letting our eyes scan over i t ; the images being transmitted to the brain which edits them. discarding some and emph- asising others. The work of the artist is the result of this interaction between himself and the subject over a period of time. Like a composer of music an artist works note by note. It is this dimension of time that is the vital difference be- tween the artist and the camera. l t means that the work of the artist, n o matter how hard he tries to be objec- tive, is always an interpretation in which he brings to bear his knowledge. his skill and above all his temperament. Thus, if you ask ten artists to paint the same subject you will get ten recognis- able, but different results. Although art and photography literally do not see eye-to-eye there is no doubt that photo- graphy served to heighten the artist’s perception of both nature and art. The young impressionist painters appeared in Paris in the early 1860’s in the thick of the battle between photography and art. In their paintings are found the effects of the non-panchromatic emul- sions. of halation, the blurring of move- ment, the foliage of trees reduced to shimmering masses. Monet’s painting of city streets, with the blurred images of pedestrians swarming like ants on the crowded pavements show features com- mon in photographs before the develop- ment of more sensitive plates and faster shutters. Degas, loved and appreciated photography. His frequent use of loom- ing objects in the foreground and the dwarfing of objects slightly further in depth spring from the aberrations of the photographic image. After 1862, he be- gan to use the cut-off effect of snapshot photography in the composition of his pictures to great effect. The arrival in Paris, in 1875. of the instantaneous photographs of Eadweard Muybridge revealed the mistakes that all artists had
made in the representation of move- ment and from that date figures of the horse in the conventional gallop no lon- ger appear in the work of Degas. Never- theless, the ability to freeze movement created problems for the artists. Should they accept the evidence of the camera or paint only what they could see. Struggle as they might, they could not escape from the influence of photogra- phy on every aspect of their work and the need for personal expression in art increased i n proportion to the growth of photography.
I n the field of medical illustration the conflict of interest between the artist and the photographer is a futile one. When art was the only means of record- ing, artists struggled to remain objec- tive. but whether i t was an operation sequence, or a view through an ophthalmoscope the artist could not escape fom his own personality which imprinted itself on his work. I t is just as easy to tell which artist produced a clin- ical picture as it is to tell a Rembrandt from a Frans Hals; not that the work has necessarily the same artistic con- tent. While photography does not tell the whole truth, its limitations can be quantified and the all-seeing camera can record clinical situations better and quicker and, what is more important, repeat the recording again and again. Indeed, many of the modern clinical investigations, such as fluorescein angiography, would not be possible without photography. It is in straight- forward recording that we see the camera’s unique quality. Here is the power and appeal of the camera’s im- age. By substituting the camera for the human eye a new order of objectivity is possible. Far below the threshold of direct experience states of matter, frac- tions of movement and particles even beyond the range of the optical micro- scope are made visible by the camera.
From the patient’s point of view it must be a great relief to keep the artist away from clinical recording. When I t h i n k back on my career in ophthalmol- ogy I blush for the amount of discom- fort I must have caused as I relentlessly extracted the minutest details froin a patient’s retina. I t is. therefore, no loss to the artist to be relieved of the necessity to produce a picture from ev- ery clinical situation. He has been re- leased to do what he alone can do, that is, produce illustrations in which under- standing of the subject and selection of the elements that go to make the illus- tration are more important than literal truth.
The future
The invention of photography threw the artists into confusion from which they have emerged with a clearer under- standing of their unassailable position. but new technical developments are now undermining the position of the photographers. When Daguerre announced his new invention he claimed that it could be used without any understanding of the chemical pro- cesses. This was very far from the case and un t i l recently the Inysteries o f photography were mainly tied up with the chemical and technical processes that went on behind the scenes. Now. thanks to new technology. electronic cameras with automatic focusing, built- in light meters and calibrated light sources have brought wi th in the reach of the unenlightened public, :I standard of photographic excellence, in colour. that would have been unthinkable not so many years ago.
Here is the photographer’s dilemma. Just as he killed off the second-rate artist and displaced the medical artist from the clinical field, so the second- rate photographer, in his t u r n , is being killed off by the enthusiastic amateur. Gone are the studios churning out photographs of the family. I t seems tha t even the photographer in the clinical field is being threatened. I t has been suggested by our masters in the Health Service, that there is no reason why doctors and nurses should not be able to use a camera as and when it is required. In my view they should be so busy with their own work that they should have no time for such activities. If an instant photograph is all that is needed anyone could take i t , but a clinical photograph should be more than that. I t is not enough to produce a photograph that barely meets the minimum requirement of the doctor; i t must extract the max- imum information from the clinical situation and the photographer must train the doctor to appreciate the differ- ence.
When I was an art student, I had an instructor who used to say, ‘if your granny likes your picture tear i t up’. That is what being a professional is about. It is not a matter of fulfilling an order like a grocer, but of creating an appreciation of higher standards. However, medical photography is no longer concerned only with clinical photography; television and other electronic imaging is providing it with means to explore new horizons. Thus, in order to compete in the rapidly
48 Donuld
J V
is C
omm
un M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
11/
24/1
4Fo
r pe
rson
al u
se o
nly.

changing world of medicine, it will be necessary to ensure that our own stan- dards are truly professional and are set and maintained at levels high enough to protect the interests of our profes- sion. To do this i t will be necessary to look again at training. There is still too much emphasis placed on technique and not enough on understanding why it should be done. Above all, we must realise that we are not in this profession to produce 'High Art' and 'Salon' photography. We have one basic objec- tive, whether we are artists or photo- graphers, and that is to communicate and our knowledge and skills must be directed towards that end. I t may be, like the artists who illustrated for Vesa- lius. that something special will come out of ou r efforts, but that will be a bonus and not an end in itself. Com- munication will unlock doors that, as yet, we have scarcely identified and we should be in the ideal situation t o meet every emerging need of the Health Sci- ences. One of our most difficult tasks will be to open the eyes of our masters, to see the potential and scope, of the service we can and should provide. far beyond the narrow confines of their in- terpretation of medical illustration. This was one of the intractable problems we had to face i n our negotiations with the DHSS. We have not only to convince our masters of the changing horizon of medical illustration, we have to con- vince ourselves. I have spoken to photo- graphers whose only desire is to go on producing pure clinical photography. I have spoken to artists who want to be left alone to create the hand work for which they have been trained. And I have spoken to both artists and photo- graphers who want nothing to do with television or any computer process.
We are living in rapidly changing times and over-specialisation will not meet the needs of the future. The dino- saur is dead. Professional flexibility will be the keynote for survival and success. Photography and computer imaging are wonderful tools and their application to man's contemplation of his universe has only just begun. Computer technology will have an effect on mankind far greater than the invention of printing. It will place in the hands of man tools of unprecedented power to create and manipulate images.
We have already witnessed its tenta- tive application to photography; and, for the first time in history, it has pre- sented to the artists an entirely new medium in which to express their crea- tive concepts with freedom and flexibil-
ity hitherto unknown. However, science and electronics are expanding so rapidly and the images they are producing are so complex that the future will need the active co-ordination of the skills of both artists and photographers to meet the technical challenges that will arise. Together they will have to learn new languages. It will not be enough that they should merely exist side-by-side. This is not a time for amateurs or semi-
professionals, nor a time t o he inhibited by the dark mysteries of technology. I t i s a time to follow the example of those who have gone before us in this profes- sion and meet the challenges head on. A time to fight for o u r rightful place in medicine.
1 have one regret. I shall not be able to join you in this adventure. I can only wish you success.
A range of diazochrome printers and processors
ci] Tecnifax Diazochrome Film - range of 20 colours 0 G-VAS de luxe combined printer/ rocessor
kl G-VA3 versatile low cost two part printer/processor for D G-VSC flat bed processor - fume P ree operation
small volume user
Gordon Audio Visual Ltd. Symes Mews37 Camden High St. London NWl 7JE Telephone 01 -387 3399 Telex. 26441 3 Greshrn G
The Journal of Audiovisital Media in Medicine (1986) Vol. 9INo.2 49
J V
is C
omm
un M
ed D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y N
yu M
edic
al C
ente
r on
11/
24/1
4Fo
r pe
rson
al u
se o
nly.