Embed Size (px)
Citation preview

The Gracilis Sling for Fecal Incontinence
By John Raffensperger
Chicago, I l l inois
�9 During the past 20 yr, we have transplanted the gracilis muscle to the perianal position for use as a sphincter to achieve continence in 7 completely incontinent children, ages 7 to 16 yr. Complete continence was achieved in three, three were improved and one transplant became infected and failed completely. The procedure has been per- formed as originally described by Pickrell. The bowel must be impeccably clean prior to the operation and the muscle must be sutured as tightly as possible about the anus. These two details, in addition to postoperative training, are essential for a successful result.
INDEX WORDS: Anal incontinence; gracilis muscle transplant.
C HILDREN with fecal incontinence are ridi- culed by siblings, shunned by school mates
and on occasion abandoned by their parents. Despite improvements in the management of children with imperforate anus and meningo- myelocele, there is still a hard core of older children who remain incontinent despite re- peated operations and various medical regimes.
The gracilis muscle transplant offers an opportunity for these children to become conti- nent. Seven children have had a gracilis trans- plant during the past 20 yr at the Cook County and Children's Memorial Hospitals in Chicago. Five of these children were incontinent because of an imperforate anus and one had a meningo- myelocele which caused both fecal and urinary incontinence, but spared the legs. One boy's sphincters were totally destroyed by pelvic sepsis following a pull-through operation for Hirsch- prung's disease. Their ages at operation ranged from 7 to 16 yr. The period of follow-up has been one to 15 yr.
The gracilis muscle originates from the lower half of the pubic symphysis and the upper half of
From the Children's Memorial Hospital, Chicago, Ill. Presented before the lOth Annual Meeting o f the Ameri-
can Pediatric Surgical Association, Los Angeles, California, March 25-28, 1979.
Address reprint requests to John Raffensperger, M.D., Children's Memorial Hospital, 2300 Children's Plaza, Chicago, Ill. 60614.
~) 1979 by Grune & Stratton, Inc. 0022-3468/79/1406-003250l .00/0
the pubic arch, traverses the thigh medial to the adductor longus, curves around the medial condyle of the tibia and inserts as a flat tendon into the tuberosity of the tibia. The gracilis is a narrow flat muscle which becomes tendinous. Innervation is derived from L2, 3, 4 through the obturator nerve. The nerves and blood supply enter the lateral side just above the mid portion of the muscle belly. Normally, the gracilis adducts, flexes and rotates the thigh inward.
MATERIALS AND METHODS
The child is admitted to the hospital 3 or 4 days prior to operation for an extensive mechanical intestinal cleansing. He is given a clear liquid and elemental diet together with laxatives by mouth and rectal irrigations. Twenty-four hours prior to the operation 100 mg/kg of neomycin is given in 4 divided doses. The bowel must be impeccably clean.
During this period, the child is also given twice daily tub baths. After the patient is anaesthetized, the surgeon irri- gates the rectum with povidone-iodine and finally swabs the rectal mucosa with a sponge soaked in the same solution. The legs, perineum, and lower abdomen are scrubbed and painted with povidonc-iodine. As originally described, the muscle was mobilized with the patient supine; the legs were then placed in the lithotomy position for the perineal portion of the operation. It is simpler, however, to suspend the legs from supports beneath the calf so the patient is in the lithotomy position during the entire operation (Fig. 1A). The initial incision is made in the distal third of the thigh over the tendon of the gracilis. The incision must be deepened through the skin, subcutaneous tissue and the fascia to enter the muscular compartment. The muscle is isolated at this point and encircled with a soft penrose drain. The tendon is then dissected as far distally as possible by applying traction to the tendon and by dividing its loose attachments under direct vision with a long pair of scissors. A second, curving incision is made at the knee. The tendon is dissected both proximally and distally until the flattened tendon is isolated directly on the periosteum of the tibia. The freed end of the gracilis is next brought out through the first incision in the thigh. The muscle is mobilized proximally up to its mid portion with both sharp and blunt dissection. A third incision is then made directly over the muscle in the upper portion of the thigh. It is possible to free more of the muscle distally through this incision until the muscle with its tendon can be delivered and wrapped in a moist pad. The remaining proxi- mal dissection to free the muscle must be done cautiously to avoid injury to the neurovascular bundle. A nerve stimulator is extremely helpful at this point. When the neurovascular bundle has been identified, it may be dissected for several centimeters in order to gain more proximal muscle length, h may be necessary to divide one distal nerve and artery in
794 Journal of Pediatric Surgery, Vol. 14, No. 6 (December), 1979
THE GRACILIS SLING 795
B.
A' I
C.
Penrose drain " " . " : , ' .... ~.:. ~d~2~;;,,,"i
- .:~--.. ~-~,4'>. ~ >//// .... .~ ,,
~xy.-~j ~;W ~J'l i'~\ \ " Gra~,hs mu~c~ ~,..,',.,r~dto
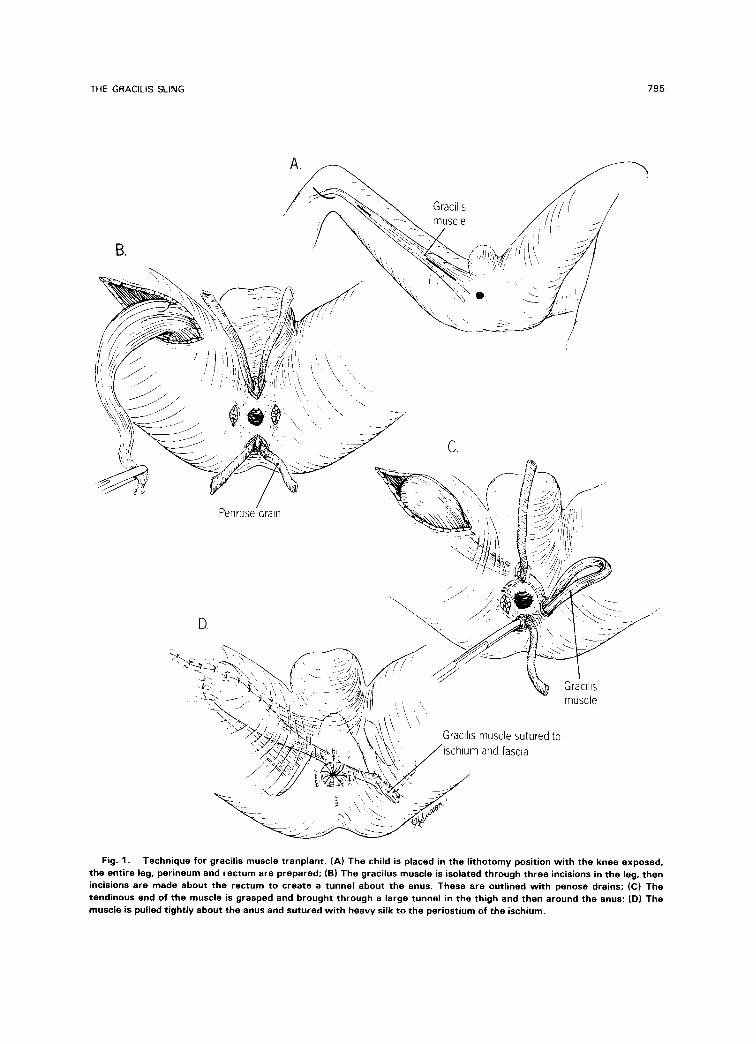
Fig. 1. Technique for gracilis muscle tranplant. (A) The child is placed in the l i thotomy position w i th the knee exposed, the entire leg, perineum and rectum are prepared; (B) The gracilus muscle is isolated through three incisions in the leg, then incisions are made about the rectum to create a tunnel about the anus. These are outl ined w i th penose drains; (C) The tendinous end of the muscle is grasped and brought through a large tunnel in the thigh and then around the anus; (D) The muscle is pulled t ight ly about the anus and sutured w i th heavy silk to the periostium of the ischium.

796 JOHN RAFFENSPERGfiR
order to gain sufficient length. The next incision is made in the midline anterior to the anus and is connected by subcuta- neous dissection to a small incision posterior to the anus. Penrose drains are drawn through these tunnels to guide the gracilis tendon (Fig. 1B). When tunnelling about the anal canal is completed, a large subcutaneous tract is created between the incision anterior to the anus and the most proximal thigh incision. This must be roomy enough to accomodate two fingers so the muscle will slide easily and not be constricted. A forceps is then passed from the anal incision to grasp and pull through the gracilis (Fig. 1C). The tendon is passed about the anus until it emerges from the anterior incision. Another incision is then made over the tuberosity of the ischium. This incision must be deepened through muscle fibers until the periosteum of the bone has been exposed. The end of the gracilis tendon is then led down to this incision where it is sutured to the periosteum of the ischium with heavy nonabsorbable sutures (Fig. 1D). Addi- tional anchoring sutures are taken between the tendon and adjacent fascia. The gracilis must be pulled so tightly that it is impossible to insert an index finger into the anus. Unfortu- nately, we have erred on the side of making the sling too loose, rather than too tight. All incisions are closed with subcuticular absorbable sutures and a compression dressing is applied to the thigh.
Postoperatively, the child is given a low residue diet and paregoric to prevent a bowel movement for several days. When he complains of a full feeling in the lower abdomen, he is placed on the toilet, with his legs abducted, a position which relaxes the gracilis muscle. Then he strains and hopefully has a bowel movement. If the gracilis is too tight, it may he necessary to pass a catheter and give a small enema to initiate a stool. It is always bette r to have the transplanted muscle too snug rather than too loose. The child is contin- ually encouraged to adduct his thighs to tighten the muscle because exercise is necessary for continued function. The occlusion of the rectum, however depends on making the encircling tendon and muscle tight, then it may be loosened with the leg abducted.
RESULTS
O u r first pa t i en t was opera ted upon in 1959. She has r e m a i n e d co n t i n en t of stool since her
opera t ion bu t requ i red an ileal condu i t because of a neu rogen i c b ladder . The second pa t i en t developed a severe wound infect ion an d was a
total fai lure. In all, t h ree pa t ien ts have nea r
perfect con t inence ; however, it was necessary to
t i g h t e n the t r a n s p l a n t in one . T h r e e a r e
improved, bu t a re still i n con t i nen t of loose stool.
Thus , of the 7 pa t ien ts , 1 was a fai lure, 3 have
essent ia l ly no rma l con t inence , and 3 c o n t i n u e to have acc idents and soiling.
DISCUSSION
Pickrel l and his associates, in a series of ar t ic les be tween 1952 and 1959 descr ibed the
t echn ique for the graci l is musc le t r ansp l an t . He
opera ted upon 50 ch i ldren f rom 3 to 14 yr of age;
most suffered f rom neurogen ic i n c o n t i n e n c e ] 3
Al l e i ther achieved comple te fecal control or
were improved. Pickrel l also used the graci l is muscle t r a n s p l a n t to correct u r i n a r y incont i -
nence in six boys. 4 Others have also repor ted good r e s u l t s . 5 7 R e c e n t l y , B r a n d e s k y a n d
Holschne ide r repor ted i m p r o v e m e n t in 21 of 24 pa t ients who had graci l is t r ansp lan t s , s All of
these au thors have ut i l ized the or ig inal tech-
n ique descr ibed by Pickrel l and his associates.
Har t l , however, has modif ied the opera t ion by
us ing the proximal por t ions of both graci l i i t ha t
are wrapped abou t the ana l cana l and su tu red to one ano ther . 9
W e have looked upon the graci l is musc le t r an -
p lan t as a " las t resor t" for ch i ld ren who have been u n a b l e to develop con t inence af ter reopera-
t ions upon their levator sl ing and who are fail- ures on medica l m a n a g e m e n t inc lud ing supposi-
tories, d ie ta ry res t r ic t ions , enemas , and d rugs tha t suppress peristalsis. N o n e of our pa t i en t s has had any d e m o n s t r a b l e sph inc te r func t ion
and most were old enough to have reached the age when chi ldren with imper fo ra t e anus sponta-
neously improve. A pro longed period of bowel
c leans ing is necessary prior to opera t ion to avoid
infect ion. The most i m p o r t a n t t echnica l de ta i l is to m a k e the t r a n s p l a n t e d musc le as snug as possible abou t the ana l canal . C o n t i n u e d postop- erat ive t r a in ing and supervis ion is necessary for
a successful result .
REFERENCES
1. Pickrell K, Broadbent TR, Masters FW, et al: Construction of a rectal sphincter and restoration of anal continence by transplanting the gracilis muscle. Ann Surg 135:853-862, 1952
2. Pickrell K, Georgiade N, Maquire C, et al: Gracilis muscle transplant for rectal incontinence. Surgery 40:349- 363, 1956
3. Pickrell K, Georgiade N, Richard ER, et al: Gracilis muscle transplant for the correction of neurogenic inconti- nence. Surg Clin North Am 39:1405-1415, 1959
4. Pickrell K, Georgiade N, Crawford H, et al: Gracilis muscle transplant for correction of urinary incontinence of male children. Ann Surg 143:764-779, 1956

THE GRACILIS SLING 797
5. Jacob ET, Shapira Z, Bar Natan Berent M: Total ano rectal reconstruction following congenital ano rectal anoma- ly. Dis Colon Rectum 19:172 176, 1976
6. Curmon ML: Gracilis muscle transposition. Contemp Surg13:9 16,1978
7. Pohl V, Schnierer M, Tergtianka G, et al: K Prob- lemom Rie~,enia [nkontinencie Alvae Pomocou Sfinktero-
plastiky PodFs Pickrella Rozhledy V. Chirurgii XLV 9 t966, pp 6t6-6t3
8. Bradensky G, Holschneider A: Operations for improve- ment of faecal continence. Prog Pediatr Surg 9:105-114, 1976
9. Hard, H: Modifiziert gracilis plastik. P~idiatr U P~dol 2:99-106, 1972 (suppl)





























