Embed Size (px)
Citation preview

THE FREE ANTEROLATERAL THIGH MUSCULOCUTANEOUS FLAPFOR HEAD AND NECK RECONSTRUCTION: ONE SURGEON’SEXPERIENCE IN 92 CASES
BERNARDO BIANCHI, M.D.,1 ANDREA FERRI, M.D.,1* SILVANO FERRARI, M.D.,1 CHIARA COPELLI, M.D.,1 PIETRO BONI, M.D.,1
TEORE FERRI, M.D.,2 and ENRICO SESENNA, M.D.1
Background: Applications of the free anterolateral thigh (ALT) musculocutaneous flap have been largely underestimated compared withindications for fasciocutaneous or perforator flaps. In this article, the authors critically review the experience of a single surgeon with thefree ALT musculocutaneous flap for head and neck reconstruction, focusing on its applications in different cephalic areas and on advan-tages and disadvantages of this technique. Patients and methods: Ninety-two patients were treated using a free ALT musculocutaneousflap. Reconstructed areas included tongue, oropharynx, mandible, maxilla, hypopharynx, cheek, and skull base. Results: Flap survivalrate was 97.8%. Donor site morbidity consisted in two cases of partial necrosis of the skin graft used its closure with a final donor sitecomplication rate of 2.2%. Overall results showed an 89% of patients returned to a normal or a soft diet. Speech was good or intelli-gible in 88% and cosmesis resulted good or acceptable in 89% of cases. Conclusion: The free ALT musculocutaneous flap offersunique advantages in head and neck reconstructions including adequate bulk when needed, obliteration of dead space, support for thesoft tissues of the face, low donor-site morbidity, and harvesting without needing for perforators dissection, allowing for optimal patientoutcome. Excessive bulky and thickness of subcutaneous tissue, especially in occidental population, have to be considered as the maindisadvantages of this technique, finally the high incidence of hairy skin in thigh area in male patients and donor site scars associatedwith the use of skin grafts have to be considered as supplementary minor drawbacks. VVC 2012 Wiley Periodicals, Inc. Microsurgery32:87–95, 2012.
The reconstruction of head and neck defects represents a
challenge because of the critical role of this area both
esthetically and functionally. In the past, attempts were
made to achieve functional restoration of resected head
and neck areas with acceptable cosmesis using local and
locoregional flaps.1,2 Free flap techniques represented a
revolution in reconstructive surgery as they enabled the
harvesting of a large amount of revascularized tissue; it
could be tailored to the defect and allowed for more
complex reconstructive procedures, while simultaneously
permitting more extensive head and neck resections.3 Pro-
gresses in microsurgery led to the possibility of recon-
structing virtually all defects of the head and neck by
harvesting soft tissue or bone-containing free flaps. The
choice of the flap to use is key to the reconstructive pro-
cedure. The ideal soft tissue free flap should be reliable
and pliable, with low donor-site morbidity and should
provide sufficient tissue for the reconstruction. Further-
more, it should have a long vascular pedicle containing
vessels of a diameter suitable for vascular anastomosis.
Finally, it should be easy and fast to harvest, and allow
two teams to work simultaneously.4 Over the last 30
years, several attempts have been made to find the ideal
soft tissue free flap: the rectus abdominis free flap has
long been the workhorse of many surgeons, especially for
reconstructing wide defects that require bulk and vol-
ume5; the radial forearm free flap is the flap of choice
for all defects when pliability and reliability are the goals
of the procedure.6
Song et al.7 introduced the anterolateral thigh (ALT)
flap in 1984, and it immediately attained worldwide ac-
ceptance. It has unique features that allow for the har-
vesting of different kinds of flap from the same donor
site. It can be harvested as a perforator,8 fasciocutane-
ous,9 musculocutaneous,10 adipofascial,11 or chimeric
flap,12 and this versatility makes this flap suitable for
reconstructing almost all defects of the head and neck.
Given these features, the ALT flap has been advo-
cated as the ideal soft tissue free flap for cervicofacial
reconstruction, especially in the Asian international liter-
ature.13 However, the applications of the free ALT mus-
culocutaneous flap have been largely underestimated
compared with the well-recognized indications for fas-
ciocutaneous or perforator flaps. Furthermore, few stud-
ies have reported on large case series involving occiden-
tal populations.14 Finally, a ‘‘one-surgeon experience’’
ensures more critical comprehension of the free ALT
musculocutaneous flap applications in the head and neck
area.
In this article, the authors critically review the expe-
rience of a single surgeon (B. Bianchi) with the free
ALT musculocutaneous flap for head and neck recon-
struction, focusing on its applications in different ce-
phalic area and on the advantages and disadvantages of
this technique.
1Maxillo-Facial Surgery Division, Head and Neck Department, UniversityHospital of Parma, Parma, Italia2Otolaryngology Head Neck Surgery Division, Head and Neck Department,University Hospital of Parma, Parma, Italia
*Correspondence to: Andrea Ferri, M.D., via Gramsci 14, 43100 Parma,Italia. E-mail: [email protected]
Received 30 May 2011; Accepted 1 August 2011
Published online 20 January 2012 in Wiley Online Library (wileyonlinelibrary.com). DOI 10.1002/micr.20952
VVC 2012 Wiley Periodicals, Inc.

PATIENTS AND METHODS
From 1 January 2003 to 31 December 2009, 92
patients were treated for head and neck malignancies or
secondary reconstruction using a free ALT musculocuta-
neous flap at the Maxillo-Facial Surgery Division, Head
and Neck Department, University and Hospital of Parma,
Italy. Data concerning patients’ population are summar-
ized in Table 1. All of the flaps were harvested by the
first author, B.B. The patients were evaluated retrospec-
tively after follow-up ranging from 12 to 84 months
(mean, 34.6 months).
The subjects consisted of 58 males and 34 females
ranging in age from 12 to 82 years, with a mean age of
69.4 years. The patients were treated for secondary recon-
struction in three cases: in two patients, an ALT muscu-
locutaneous flap was used to correct trismus that devel-
oped after surgery and radiation therapy for oral cavity
malignancies, while the ALT musculocutaneous flap was
used to reconstruct a facial contour defect in the third
patient who was treated for a mandibular malignancy. In
the other 89 cases, the patients were treated for head and
neck malignancies. The histology was squamous cell car-
cinoma in 79 patients, basal cell carcinoma in seven
patients, sarcoma in two patients, and undifferentiated
carcinoma of the submandibular gland in one patient. The
primary tumor was located in the tongue in 26 cases, the
oropharynx in 18 (including the soft palate, tonsil, retro-
molar trigon, and pharyngeal wall), the mandible in 17,
the maxilla in 10, hypopharynx in six, cheek and skull
base in five cases each, and inferior lip and submandibu-
lar gland in one case each.
Twenty-eight patients were treated previously with
surgery alone (n 5 14), radiation therapy alone (n 5 6),
surgery and radiotherapy (n 5 5), or chemoradiation ther-
apy (n 5 3).
Surgical Technique
The design of the skin paddle was based on the size
and three-dimensional features of the defect. When
needed, we preferred to delay the de-epithelialization
until after transplanting the flap to maximize the custom-
ization of the flap, so we designed the skin paddle in an
elliptical or bilobed shape.
Working with a second team to resect the tumor and
prepare the recipient site simultaneously, the dissection
began in the medial border of the flap, incising only 5 to
6 cm of skin initially and the underlying superficial fas-
cia. After identifying the rectus femoris, we followed the
intermuscular septum until the pedicle of the flap (the de-
scending branch of the lateral circumflex femoral artery
with its two venae comitantes and the anterior branch of
the lateral cutaneous nerve) was identified (Fig. 1).
At this point, independent of the presence of a septo-
cutaneous perforator, which may be suitable for harvest-
ing a septocutaneous perforator flap, we completed the
medial skin incision and dissected the vascular pedicle,
distally to proximally. After incising the fascia lata, the
vastus lateralis muscle were transected distally, and the
distal part of the pedicle was isolated, ligated, and cut.
The dissection proceeded distally to proximally. The flap
was taken in the hand of the first operator and the vastus
lateralis muscle was harvested based on the need for
reconstruction. At this point, the anterior branch of the
lateral cutaneous nerve was dissected and preserved in 62
cases, transected in 18, and transected and repaired in the
remaining 12. The entire procedure took 30 to 40
minutes.
The donor site was usually closed directly after plac-
ing a drain. In our experience, a skin graft was needed
only when the minor axis (oriented perpendicular to the
septum) of the flap was larger than 10 to 13 cm.
The free ALT musculocutaneous flap was harvested
from the right thigh in 89 cases; the left thigh was used
in the remaining three because anomalies were detected
during the preoperative mapping of the skin perforators.
The skin paddle measured from 4 3 5 to 12 3 23
cm2, and the amount of muscle harvested ranged from a
minimum of 4 cm in length and 2 cm in width to the
entire muscular belly (12 3 6 cm2). Muscular cuff played
a major role in tongue reconstruction, when it was placed
with the skin component to restore an adequate bulk into
the oral cavity (Fig. 2). When used for neck vessels and
anastomosis protection, the muscle was placed in the
neck and fixed with resorbable sutures to sternocleido-
mastoid muscle (when present) and supra-hyoid muscles.
In case of hypopharyngeal reconstruction after total laryn-
gectomy, muscle component was spread over the tracheal
stoma creating a muscular layer between the tubulized
skin of the flap used for the reconstruction of hypophar-
ynx and the stoma, ensuring a good fixation to surround-
ing tissues and obliteration of dead spaces. When oro-
mandibular reconstruction was performed, the muscular
cuff was placed in the submandibular area fixing it to the
periostium of the residual mandible and to the oral cavity
residual soft tissues, taking care to roll the muscle around
the reconstructive plate when it was used to restore the
mandibular arch defect (Fig. 3). For maxillary defect
reconstruction, the muscle was placed into the maxillary
defect to fill it completely and sutured to the periostium
of preserved bone structures (zygoma, nasal bone, and or-
bital rim); if bone grafts or alloplastic prosthesis were
used, muscle was positioned taking care to ensure a good
contact with grafts reducing dead spaces and providing
well vascularized tissue for integration of grafts and pros-
thesis, thus preventing infections and reabsorption
(Fig. 4). Finally, when used for skull base reconstruction,
88 Bianchi et al.
Microsurgery DOI 10.1002/micr
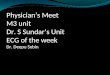
Table
1.Patients:Population,Treatm
ents,andComplications
Location
No.
Previous
treatm
ents
Associatedtechnique
Donorsite
directclosure
Postoperative
treatm
ents
Complications
Tongue
26
Surgery:7
None
21(80%)
RT:7
Flaplost:1(3.8%)
Surgery
þRT:2
Marginalnecrosis:1(3.8%)
RT:2
RTþ
CT:8
Dehiscence:3(11.5%)
RTþ
CT:1
Donorsiteskin
graftnecrosis:0
Oropharynx
18
Surgery:2
None
15(83%)
RT:4
Flaplost:0
Surgery
þRT:2
Marginalnecrosis:2(11.1%)
RT:4
RTþ
CT:7
Dehiscence:3(16.6%)
RTþ
CT:1
Donorsiteskin
graftnecrosis:0
Oromandibulararea
17
Surgery:2
Plate:12
15(88%)
RT:5
Flaplost:0
Surgery
þRT:1
Fibula:4
Marginalnecrosis:1(5.8%)
RT:0
Cervicopectoralflap:2
RTþ
CT:6
Dehiscence:3(17.6%)
RTþ
CT:0
Donorsiteskin
graftnecrosis:0
Maxilla
10
Surgery:1
Bonegrafts:8
7(70%)
RT:5
Flaplost:1(10%)
Surgery
þRT:0
Marginalnecrosis:0
RT:0
RTþ
CT:3
Dehiscence:2(20%)
RTþ
CT:0
Donorsiteskin
graftnecrosis:1(10%)
Hypopharynx
6Surgery:0
None
4(67%)
RT:2
Flaplost:0
Surgery
þRT:0
Marginalnecrosis:0
RT:0
RTþ
CT:3
Dehiscence:0
RTþ
CT:1
Donorsiteskin
graftnecrosis:0
Cheek
5Surgery:1
Cervicopectoralflap:1
3(60%)
RT:2
Flaplost:0
Surgery
þRT:0
Marginalnecrosis:0
RT:0
RTþ
CT:3
Dehiscence:1(20%)
RTþ
CT:0
Donorsiteskin
graftnecrosis:0
SkullBase
5Surgery:0
None
1(20%)
RT:1
Flaplost:0
Surgery
þRT:0
Marginalnecrosis:0
RT:0
RTþ
CT:2
Dehiscence:0
RTþ
CT:0
Donorsiteskin
graftnecrosis:1(20%)
Trism
usrelease
2Surgery:0
None
0RT:0
Flaplost:0
Surgery
þRT:2
Marginalnecrosis:0
RT:0
RTþ
CT:0
Dehiscence:0
RTþ
CT:0
Donorsiteskin
graftnecrosis:0
Facialcontourdefect
1Surgery:0
None
0RT:0
Flaplost:0
Surgery
þRT:0
Marginalnecrosis:0
RT:0
RTþ
CT:0
Dehiscence:0
RTþ
CT:0
Donorsiteskin
graftnecrosis:0
RT:radiotherapy;
CT:chemotherapy;RTþ
CT:chemo-radiationtherapy.
ALT Musculocutaneous Flap 89
Microsurgery DOI 10.1002/micr

muscular cuff was placed over the defect filling all the
surgical gap and suturing it to surrounding bone and peri-
ostium to prevent ptosis and dehiscences (Fig. 5).
Direct closure of the donor site was achieved in 71
patients, while in the other 21, a partial-thickness free
skin graft was harvested from the contralateral internal
side of the thigh and used for donor site closure.
In 27 patients, the flap was associated with another
reconstructive technique: with a titanium plate in 12
patients, free bone grafts in eight, a fibula osteocutaneous
free flap in four, and a locoregional cervicopectoral flap
in the other three patients.
The microvascular anastomosis was performed by the
same surgeon (first author, B.B.) using the artery and
only one vein. The superior thyroid artery was chosen as
the recipient artery 42 times (contralateral to the defect
five times), the facial artery 29 times (contralateral to the
defect 10 times), the lingual artery 12 times, and the
external carotid artery nine times (contralateral to the
defect twice). The internal jugular vein was the preferred
recipient vein and was used 74 times: in 48 cases, an
end-to-side anastomosis was performed (contralateral to
Figure 1. Intraoperative picture showing flap harvesting. (A) Muscu-
lar anatomy. RF: rectus femori muscle; VL: vastus lateralis muscle;
the painted blue line between the two muscles represents the inter-
muscular septum. (B) The neurovascular pedicle. (C) The final har-
vesting of the free ALT musculocutaneous flap. [Color figure can be
viewed in the online issue, which is available at wileyonlinelibrary.
com.]
Figure 2. Musculocutaneous ALT flap for tongue reconstruction.
(A) Intraoperative picture of the surgical defect following a subtotal
glossectomy. (B) Postoperative results after adjuvant radiation ther-
apy. The bulk of the flap enable patient’s oral cavity functions as
speech and swallow. [Color figure can be viewed in the online
issue, which is available at wileyonlinelibrary.com.]
90 Bianchi et al.
Microsurgery DOI 10.1002/micr

the defect 12 times), and in 26 cases, an end-to-end anas-
tomosis to a proximal affluent trunk was used (contralat-
eral to the defect five times). The facial vein was used
10 times, while the external jugular vein was used eight
times.
RESULTS
Of the 92 free ALT musculocutaneous flaps harvested
and transplanted, major complications resulted in the loss
of two flaps due to venous thrombosis: one occurred in-
traoperatively during the reconstruction of a submandibu-
lar gland tumor resection and the second on the second
postoperative day after the reconstruction of an inferior
lip tumor resection. The final survival rate was 97.8%
(90 of 92). Minor complications included marginal necro-
sis of the skin paddle (4.3%; n 5 4), dehiscence of the
suture (13%; n 5 12), and partial necrosis of the skin
graft used for donor site closure (2.2%; n 5 2). All these
minor complications were managed with wound dressing
or suture replacement under local anesthesia and required
no further surgical procedure. No major donor site com-
plication occurred, and all the patients returned to their
daily activities in around 4 weeks without limitation due
to donor-site morbidity.
In all cases, excess bulk was present in the first post-
operative weeks, but a large part of the muscular compo-
nent atrophied, optimizing the result in a few months.
This time was reduced drastically if adjuvant radiotherapy
was performed.
The length of hospitalization ranged from 6 to 31
days (mean, 12 days).
Postoperative adjuvant radiation therapy was per-
formed in 58 patients, 32 of whom also received concom-
itant chemotherapy (cisplatin in all cases).
Follow-up ranged from 12 to 84 months, with a mean
of 34.6 months. Of the 92 patients, 29 died of their dis-
ease, 10 are alive with disease (four local recurrences on
palliative chemotherapy and six distant metastases on
chemotherapy), and 53 show no evidence of disease.
Patient’s postoperative functions were evaluated on alive
patients by medical examination, and questionnaire and
results are summarized in Table 2. Deglutition was
assessed by the patient diet that was classified as normal,
soft, or gastrostomy tube-dependent. Speech evaluation
was based on the capability of the patient to be under-
stood, and the results were classified as good, intelligible,
or unintelligible. Aesthetic outcome was valued by the
Figure 4. Musculocutaneous ALT flap for maxillary reconstruction.
Intraoperative picture showing flap insetting: the skin is used for
palatal and nasal mucosal lining reconstruction; the muscle and a
portion of de-epithelializated skin paddle is used for maxillary
defect filling providing adequate bulk and enrolling bone grafts used
for floor of the orbit reconstruction. [Color figure can be viewed in
the online issue, which is available at wileyonlinelibrary.com.]
Figure 3. Musculocutaneous ALT flap and titanium plate for oro-
mandibular reconstruction. Intraoperative picture showing the role
of the different flap components: the skin is used for oral mucosa
defect reconstruction; fascia lata is used for plate enrollment and
flap suspension; muscular component is placed in the submandibu-
lar area obliterating dead spaces and preventing oro-cervical fistu-
las and infections. [Color figure can be viewed in the online issue,
which is available at wileyonlinelibrary.com.]
ALT Musculocutaneous Flap 91
Microsurgery DOI 10.1002/micr
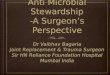
Figure 5. Musculocutaneous ALT flap for skull base reconstruction. (A) Skull base defect after tumor resection. (B) Reconstruction of the through
and through defect using the ALT flap: the muscular component is used to fill all the defect preventing fistulas and infections obliterating all the
dead areas of the surgical gap, while the skin is placed externally to reconstruct the cutaneous defect. [Color figure can be viewed in the online
issue, which is available at wileyonlinelibrary.com.]
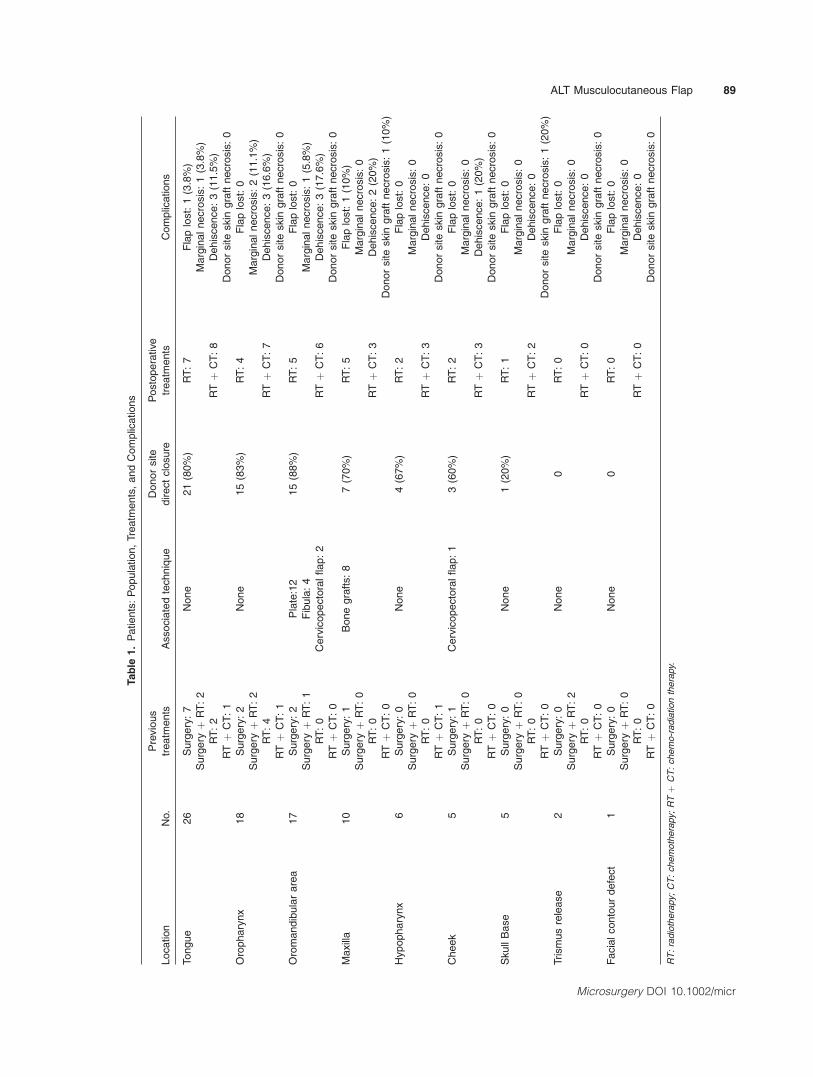
Table 2. Functional and Esthetic Results
Location No. Diet Speech Cosmesis
Tongue 16 Normal: 19% (n 5 3) Good: 31% (n 5 5) Excellent: 37% (n 5 6))
Soft: 62% (n 5 10) Intelligible: 50% (n 5 8) Acceptable: 50% (n 5 8)
GT dependant: 19% (n 5 3) Unintelligible:19% (n 5 3) Poor: 13% (n 5 2
Oropharynx 13 Normal: 31% (n 5 4) Good: 54% (n 5 7) Excellent: 38% (n 5 5)
Soft: 54% (n 5 7) Intelligible: 38% (n 5 5) Acceptable: 47% (n 5 6)
GT dependant: 15% (n 5 2) Unintelligible: 8% (n 5 1) Poor: 15% (n 5 2)
Oromandibular area 11 Normal: 64% (n 5 6) Good: 36% (n 5 5) Excellent: 18% (n 5 2)
Soft: 36% (n 5 5) Intelligible: 64% (n 5 6) Acceptable: 73% (n 5 8)
GT dependant: 0 Unintelligible: 0 Poor: 9% (n 5 1)
Maxilla 9 Normal: 44% (n 5 4) Good: 67% (n 5 6) Excellent: 44% (n 5 4)
Soft: 56% (n 5 5) Intelligible: 33% (n 5 3) Acceptable: 56% (n 5 5)
GT dependant: 0 Unintelligible: 0 Poor: 0
Hypopharynx 4 Normal: 0 Good: 0 Excellent: 0
Soft: 50% (n 5 2) Intelligible: 0 Acceptable: 75% (n 5 3)
GT dependant: 50% (n 5 2) Unintelligible: 25% (n 5 1)
Laryngectomy: 75%(n 5 3)
Poor: 25% (n 5 1)
Cheek 5 Normal: 80% (n 5 4) Good: 100% (n 5 5) Excellent: 60% (n 5 3)
Soft: 20% (n 5 1) Intelligible: 0 Acceptable: 40% (n 5 2)
GT dependant: 0 Unintelligible: 0 Poor: 0
Skull base 2 Normal: 100% (n 5 2) Good: 100% (n 5 2) Excellent: 0
Soft: 0 Intelligible: 0 Acceptable: 50% (n 5 1)
GT dependant: 0 Unintelligible: 0 Poor: 50% (n 5 1)
Trismus release 2 Normal: 50% (n 5 1) Good: 100% (n 5 2) Excellent: 50% (n 5 1)
Soft: 50% (n 5 1) Intelligible: 0 Acceptable: 50% (n 5 1)
GT dependant: 0 Unintelligible: 0 Poor: 0
Facial contour defect 1 Normal: 100% (n 5 1) Good: 100% (n 5 1) Excellent: 100% (n 5 1)
Soft: 0 Intelligible: 0 Acceptable: 0
GT dependant: 0 Unintelligible: 0 Poor: 0
Overall results 63 Normal: 39% (n 5 25) Good: 52% (n 5 33) Excellent: 36% (n 5 22)
Soft: 50% (n 5 32) Intelligible: 36% (n 5 22) Acceptable: 53% (n 5 34)
GT dependant: 11% (n 5 7) Unintelligible: 12% (n 5 8) Poor: 11% (n 5 7)
GT dependant: gastrostomy tube dependant.
92 Bianchi et al.
Microsurgery DOI 10.1002/micr

surgeon and by the patient’s own perception as excellent,
acceptable, or poor. Overall results showed an 89% of
patients that returned to a normal or a soft diet and only
11% that are gastrostomy tube dependant. Speech was
good or intelligible in 88% of patients and unintelligible
in the remaining 12% (three of these patients—5%—were
submitted to a total laryngectomy during tumor resec-
tion). Concerning cosmetic results, good or acceptable
cosmesis was achieved in 89% of cases.
DISCUSSION
The advantages of the ALT free flap and its applica-
tions are well documented. Wong and Wei15 reported
their experience in head and neck reconstruction with the
ALT flap, emphasizing the use of this flap with perforator
harvesting. Kimata et al.16 described the advantages of
the perforator ALT free flap in the reconstruction of post-
oncologic cervicofacial defects. Although the advantages
of the perforator technique are well documented, only a
few studies have reported on free ALT musculocutaneous
flap applications, and none of them dealt with Western
populations. Wei et al.13 reported a large case series deal-
ing with 672 ALT flaps harvesting; however, only 95 of
these (14%) were musculocutaneous flaps, and protection
of musculocutaneous perforators was advocated as the
main advantage of muscle harvesting. Demirkan et al.10
were the first in 2000 to emphasize the versatility of the
ALT musculocutaneous flap underlining the advantage of
a safe flap harvesting without needing for perforators dis-
section and independently from anatomic vascular varia-
tions and the usefulness of muscle component for volume
restoration and dead space obliteration. The same
approach was proposed 1 year later by Kuo et al.17 that
used the musculocutaneous version of the ALT flap in
62.1% of their reported patients, describing the advan-
tages of this technique when bulky flap was needed.
Wong et al.18 described in 2009 a technical note for the
ALT musculocutaneous flap harvesting, underlining the
importance of musculocutaneous perforators identification
and preservation at the beginning of the dissection that
has to be performed opening the intermuscular septum
and unroofing the musculocutaneous perforators. We
recently described the use of the free ALT musculocuta-
neous flap and bone grafts association for maxillary
reconstruction;19 however, as far as we know, other
articles dedicated specifically to free ALT musculocutane-
ous flap patients series were published only in the last
year and only in Chinese literature. Xia et al.20 reported
their experience with ALT musculocutaneous flap for
tongue and mouth floor reconstruction in 14 cases, while
Liu et al.21 reported a series of 109 free ALT musculocu-
taneous flaps for reconstruction of soft tissue defects fol-
lowing en block resection of tongue cancer. In both
articles, a detailed description of ALT musculocutaneous
flap advantages was performed, focusing on bulky and
obliteration of dead space provided with the technique.
However, both articles dealt only with tongue defects
without considering other areas of head and neck.
Following the international literature, in our first
experiences with the ALT free flap, we started with the
use of the perforator variant, which requires a long oper-
ating time and tedious, difficult intramuscular dissection
of the perforator vessels in cases when a septocutaneous
perforator is not present22 (70 to 80% of the literature
reported cases). Although optimal results were obtained
with this flap, we started to modify our approach by har-
vesting a cuff of vastus lateralis muscle in almost all
cases. This has at least two great advantages: the dissec-
tion time decreases from 2 to 3 hours for the perforator
flap to between 30 and 40 minutes for the musculocuta-
neous flap, and the harvested muscle can be used in the
reconstruction in several ways, depending on the site of
the defect and the need for bulk in its reconstruction.
The free ALT musculocutaneous flap is now our first-
choice flap for reconstructing almost all soft tissues
defects of the head and neck, replacing the rectus abdom-
inis free flap and radial forearm fasciocutaneous free flap
(RFFF). Several discussions exist in the literature about
replacing the RFFF with the ALT flap.23 We use the
RFFF only for the smallest oral cavity defects, and only
when extreme pliability and thinning are critical for the
patient’s functional outcome (e.g., for small defects of
the cheek, floor of the mouth, or soft palate), preferring it
to a perforator ALT flap; for all other defects, the free
ALT musculocutaneous flap is used.
When we deal with hypopharyngeal defects recon-
struction, the main goal is restoring the digestive tract by
tubularizing the flap used.24 In three patients of the
reported list, the skin component of the ALT musculocu-
taneous flap was used for pharyngeal mucosal defect
reconstruction, and only a small amount of muscle was
harvested, to avoid compressing the tubularized skin,
which increases the risk of stenosis. The muscular cuff
was placed in the neck to protect the great vessels and
anastomosis. In the remaining three patients, a larger
hypopharyngeal defect associated with a laryngectomy
was present, and the muscular component was used to
separate the airway from the digestive tract to prevent
pharyngo-stomal or neck-pharyngeal fistulas.
When the resection involves the tongue, reconstruction
of partial or total glossectomies is one of the best indica-
tions for the use of a free ALT musculocutaneous flap.
Given the physiology of speech and deglutition, one of the
main objectives of such reconstructions is to restore
adequate bulk, which should not be excessive to allow mo-
bility of the flap together with the residual structures.
Enough bulk should exist to permit the lingual-palatal con-
ALT Musculocutaneous Flap 93
Microsurgery DOI 10.1002/micr

tact that represents the first and most important step in the
oral phase of deglutition. The muscular component of the
ALT musculocutaneous flap is very useful for this purpose,
especially when the tongue base is involved in the resec-
tion, as in 19 of the 26 reported patients. Furthermore, the
muscle can be used to obliterate any submandibular dead
spaces, ensuring optimal separation between the oral cavity
and neck, thereby preventing fistulas and infections.
For oromandibular defects, we usually use bone-con-
taining free flaps to optimize the esthetic and functional
outcome.25 When bone reconstruction is not indicated,
we prefer a free ALT musculocutaneous flap, alone or in
association with a titanium reconstructive plate.26 In such
cases, the muscular component of the flap plays a major
role, it protects the plate with a large amount of well
revascularized tissue, thereby preventing plate infections
and exposure, while simultaneously providing bulky
reconstruction of the defect and reducing the asymmetry
of the oral cavity resulting from the mandibular resection.
In the patients list reported here, any of the 12 plates
used in association with the flap underwent exposure and
esthetically, the bulk of the flap allowed an adequate fa-
cial contour restoration also when the flap was used alone
(n 5 5).
Also maxillary reconstruction is usually performed
using bone-containing free flaps;27 however, in elderly
patients or those with a poor prognosis, a free ALT mus-
culocutaneous flap can be useful. When a wide residual
cavity is present, muscle harvesting permits filling of the
entire space, thereby preventing air communication and
providing cheek soft tissue support. In eight of our
patients, the large amount of revascularized muscle was
rolled around bone grafts or alloplastic prosthesis for the
floor of the orbit or zygoma reconstruction, avoiding
infections and resorption also after radiation therapy. Fur-
thermore, the ALT flap can be harvested with two skin
paddles as in two of the reported patients, when recon-
struction of the external coverage of the cheek is needed.
Finally, the fascia lata may be used for flap suspension,
preventing ptosis of the flap in the oral cavity and ensur-
ing adequate functional reconstruction of the soft palate.
In the reconstruction of the skull base, the free ALT
musculocutaneous flap offers unique advantages over the
perforator ALT flap and other musculocutaneous flaps.28
It provides a large amount of revascularized muscle,
which is essential for obliterating the space in the skull
base, preventing fistulas and infections. The pedicle is
long enough to reach the recipient vessels in the neck;
also, the large amount of skin included can be used for
cutaneous defects, and the fascia lata can be used for flap
suspension preventing ptosis of the flap typical when this
area is approached.
Independently on the area to reconstruct, the low
donor-site morbidity and the possibility of harvesting the
flap simultaneously with the resection have been recog-
nized worldwide as the main advantages of the ALT
flap.29 With the musculocutaneous version of the flap, the
harvesting of the muscular component does not increase
the donor-site morbidity; the cutaneous defect can usually
be closed primarily when a skin paddle of up to between
12 and 13 cm is harvested, and the functional outcome is
usually optimal without interfering with the patient’s
daily activities, even when a large amount of vastus later-
alis is harvested as recently described by Hanasono
et al.30 These authors reported only an 8% of weakness
after muscle harvesting that was not associated with the
degree of muscle harvested or motor nerve transection,
probably because the synergistic effect of the remaining
three muscle bellies of the quadriceps.
Despite the great advantages of the free ALT muscu-
locutaneous flap, excessive bulky may result if redundant
amount of muscle is harvested, thus requiring a careful
planning of the reconstruction and a harvesting tailored
on the size of the defect and on the reconstructive need-
ing. This disadvantage may be particularly significant in
occidental population because of the major thickness of
the subcutaneous fat tissue, when compared with oriental
one and become critical in obese patients. Finally, the
high incidence of hairy skin in thigh area in male patients
and donor site scars associated with the use of skin grafts
in large defects have to be considered as supplementary
minor drawbacks of this technique.
CONCLUSIONS
The free ALT musculocutaneous flap offers unique
advantages in head and neck reconstruction, including
adequate bulk when needed, obliteration of dead space
thus preventing fistulas and infections, protection of
plates and bone grafts, support for the soft tissues of the
face allowing for optimal patient outcome. Based on our
experience, we would like to emphasize the major role
played by the free ALT musculocutaneous flap that is
nowadays largely underestimated.
REFERENCES
1. Crow ML, Crow FJ. Resurfacing large cheek defects with rotationflaps from the neck. Plast Reconstr Surg 1976;58:196–200.
2. Bianchi B, Ferri A, Ferrari S, Copelli C, Poli T, Sesenna E. Freeand locoregional flap associations in the reconstruction of extensivehead and neck defects. Int J Oral Maxillofac Surg 2008;37:723–729.
3. Futran ND, Mendez E. Developments in reconstruction of midfaceand maxilla. Lancet Oncol 2006;7:249–258.
4. Blackwell KE, Buchbinder D, Biller H, Urken ML. Reconstructionof massive defects in the head and neck: The role of simultaneousdistant and regional flaps. Head Neck 1997;19:620–628.
5. Bianchi B, Bertolini F, Ferrari S, Sesenna E. Maxillary reconstruc-tion using rectus abdominis free flap and bone grafts. Br J OralMaxillofac Surg 2006;44:526–530.
94 Bianchi et al.
Microsurgery DOI 10.1002/micr

6. Soutar DS, Scheker LR, Tanner NS, McGregor IA. The radial fore-arm flap: A versatile method for intra-oral reconstruction. Br J PlastSurg 1983;36:1–8.
7. Song YG, Chen GZ, Song YL. The free thigh flap: A new free flap conceptbased on the septocutaneous artery. Br J Plast Surg 1984;37:149–159.
8. Makitie AA, Beasley NJP, Neligan PC, Lipa J, Gullane PJ, GilbertRW. Head and neck reconstruction with anterolateral thigh flap. Oto-laryngol Head Neck Surg 2003;129:547–555.
9. Koshima I. Free anterolateral thigh flap for reconstruction of headand neck defects following cancer ablation. Plast Reconstr Surg2000;105:2348–2357.
10. Demirkan F, Chen HC, Wei FC, Chen HH, Jung SG, Hau SP, Liao CT.The versatile anterolateral thigh flap: A musculocutaneous flap in dis-guise in head and neck reconstruction. Br J Plast Surg 2000;53:30–36.
11. Ao M, Uno K, Maeta M, Nakagawa F, Saito R, Nagase Y. De-epi-thelialised anterior (anterolatera and anteromedial) thigh flaps fordead space filling and contour correction in head and neck recon-struction. Br J Plast Surg 1999;52:261–267.
12. Koshima I, Yamamoto H, Hosoda M, Moriguchi T, Orita Y,Nagayama H. Free combined composite flaps using the lateral cir-cumflex femoral system for repair of massive defects of the headand neck regions: an introduction to the chimeric flap principle. PlastReconstr Surg 1993;92:411–420.
13. Wei FC, Jain V, Celik N, Chen HC, Chuang DC, Lin CH. Have wefound an ideal soft-tissue flap? An experience with 672 anterolateralthigh flaps. Plast Reconstr Surg 2002;109:2219–2226.
14. Wolff KD, Kesting M, Thurmuller P, Bockmann R, Holzle F. The an-terolateral thigh as a universal donor site for soft tissue reconstructionin maxillofacial surgery. J Craniomaxillofac Surg 2006;34:323–331.
15. Wong CH, Wei FC. Anterolateral thigh flap. Head Neck 2010;32:529–540.
16. Kimata Y, Uchiyama K, Ebihara S, Yoshizumi T, Asai M, SaikawaM, Hayashi R, Jitsuiki Y, Majima K, Ohyama W, Haneda T, Nakat-suka T, Harii K. Versatility of the free anterolateral thigh flap forreconstruction of head and neck defects. Arch Otolaryngol HeadNeck Surg 1997;123:1325–1331.
17. Kuo YR, Jeng SF, Kuo MH, Liu YT, Lai PW. Versatility of the freeanterolateral thigh flap for reconstruction of soft-tissue defects:review of 140 cases. Ann Plast Surg 2002;48:161–166.
18. Wong CH, Kao HK, Fu B, Lin JY. A cautionary point in the har-vesting of the anterolateral thigh myocutaneous flap. Ann Plast Surg2009;62:637–639.
19. Bianchi B, Ferri A, Ferrari S, Copelli C, Sesenna E. Maxillaryreconstruction using anterolateral thigh flap and bone grafts. Micro-surgery 2009;29:430–436.
20. Xia DL, Fu GX, Ma Z, Chen JL, Zhou HY, Jia J. Application of an-terolateral thigh myocutaneous flap in the reconstruction of tongueand mouth floor defect after tongue carcinoma. Zhonghua ZhengXing Wai Ke Za Zhi 2011;27:8–11.
21. Liu J, Wu H, Zhu Z, Wu X, Tan H, Wang K. Free anterolateralthigh myocutaneous flap for reconstruction of soft tissue defects fol-lowing en block resection of tongue cancer. Zhingguo Xiu Fu ChongJian Wai Ke Za Zhi 2010;24:82–86.
22. Koshima I, Fukuda K, Utunomiya R, Soeda S. The anterolateralthigh flap; variations in its vascular pedicle. Br J Plast Surg1989;42:260–262.
23. Valentini V, Cassoni A, Marianetti TM, Battisti A, Terenzi V, Ian-netti G. Anterolateral thigh flap for the reconstruction of head andneck defects: Alternative or replacement of the radial forearm flap?J Craniofac Surg 2008;19:1148–1153.
24. Genden EM, Jacobson AS. The role of the anterolateral thigh flapfor pharyngoesophageal reconstruction. Arch Otolaryngol Head NeckSurg 2005;131:796–799.
25. Bianchi B, Ferri A, Ferrari S, Copelli C, Boni P, Sesenna E.Reconstruction of anterior through and through oromandibulardefects following oncological resections. Microsurgery 2010;30:97–104.
26. Bianchi B, Ferri A, Ferrari S, Copelli C, Boni P, Baj A; SesennaE. Reconstruction of lateral through and through oromandibulardefects following oncological resections. Microsurgery 2010;30:517–525.
27. Cordeiro PG; Santamaria E. A classification system and algorithmfor reconstruction of maxillectomy and midfacial defects. PlastReconstr Surg 2000;105:2331–2346.
28. Hanasono MM, Sacks JM, Goel N, Ayad M, Skoracki RJ. The an-terolateral thigh free flap for skull base reconstruction. OtolaryngolHead Neck Surg 2009;140:855–860.
29. Kimata Y, Uchiyama K, Ebihara S, Sakuraba M, Ida H, NakatsukaT, Harii K. Anterolateral thigh flap donor-site complications andmorbidity. Plast Reconstr Surg 2000;106:584–589.
30. Hanasono MM, Skoracki RJ, Yu P. A prospective study of donor-sitemorbidity after anterolateral thigh fasciocutaneous and myocutaneousfree flap harvest in 220 patients. Plast Reconstr Surg 2010;125:209–214.
ALT Musculocutaneous Flap 95
Microsurgery DOI 10.1002/micr